Back to Journals » Patient Preference and Adherence » Volume 20
Factors Associated with Adherence to the Atrial Fibrillation Better Care (ABC) Pathway Among Rural Patients with Atrial Fibrillation: A Path Analysis Based on the Integrated Theory of Health Behavior Change (ITHBC)
Authors Huang J ![]() , Chen J
, Chen J ![]() , Ye Q, Cai X, Feng Y, Lai X, Diao X, Dai Q, Zhang X, Li K
, Ye Q, Cai X, Feng Y, Lai X, Diao X, Dai Q, Zhang X, Li K
Received 15 August 2025
Accepted for publication 30 December 2025
Published 20 January 2026 Volume 2026:20 556835
DOI https://doi.org/10.2147/PPA.S556835
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jun Huang,1,* Jing Chen,2,* Qirao Ye,3 Xiaomei Cai,4 Yuanchun Feng,4 Xinwei Lai,3 Xiulin Diao,3 Qingxiang Dai,5 Xiaomin Zhang,2,6 Kun Li2
1Department of Geriatrics, Guangdong Provincial Geriatrics Institute, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China; 2School of Nursing, Sun Yat-sen University, Guangzhou, People’s Republic of China; 3Department of Cardiology, People’s Hospital of Shangyou County, Ganzhou, People’s Republic of China; 4Chronic Disease Management Center, People’s Hospital of Shangyou County, Ganzhou, People’s Republic of China; 5Electrocardiogram Room, People’s Hospital of Shangyou County, Ganzhou, People’s Republic of China; 6Department of Medical Oncology, Sun Yat-Sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaomin Zhang, Department of Medical Oncology, Sun Yat-Sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, People’s Republic of China, Tel +86 18811332158, Email [email protected] Kun Li, School of Nursing, Sun Yat-sen University, No. 74 Zhong Shan second Road, Guangzhou, 510080, People’s Republic of China, Tel +86 13822206519, Email [email protected]
Background: The atrial fibrillation better care (ABC) pathway is an effective strategy for the integrated management of atrial fibrillation (AF). However, the adherence rate of ABC pathway in rural Chinese patients with AF is extremely low.
Aim: To explore the factors and mechanisms of adherence to the ABC pathway based on the integrated theory of health behavior change (ITHBC) among rural patients with AF.
Methods: In this cross-sectional study, we recruited 940 patients with AF from rural areas in China from July 2022 to September 2023. Patients completed a questionnaire covering AF-related demographic and clinical characteristics, AF knowledge, AF health beliefs, AF self-management ability, and social support. Adherence to ABC pathway was assessed based on AF-demographic and clinical characteristics. Path analysis was used to explore the relationship between variables.
Results: Adherence to ABC pathway among rural patients with AF was extremely low (5.7%). AF self-management ability (β = 0.449; P< 0.001) and social support (β = 0.429; P< 0.001) directly and positively affected adherence to ABC pathway. Additionally, AF knowledge (β = 0.211; P< 0.001), AF health beliefs (β = 0.350; P< 0.001) and social support (β = 0.085; P< 0.001) can also indirectly and positively affect adherence to ABC pathway through AF self-management ability. AF knowledge (β = 0.121; P< 0.001) can indirectly affect adherence to the ABC pathway through a series of mediations via AF health beliefs and AF self-management ability.
Conclusion: AF knowledge, AF health beliefs, and social support are important intervention components that should be closely integrated with AF self-management ability.
Keywords: atrial fibrillation, guideline adherence, rural population, knowledge, health belief, self-management, social support
Introduction
Atrial fibrillation (AF) is the most common arrhythmia.1 In China, there are approximately 7.9 million patients with AF.2 AF can lead to a range of complications, the most serious of which is stroke.1 Patients with AF have a 4–5 times higher risk of stroke than those without AF, and AF-related ischemic strokes are almost twice as fatal as those without AF.1,3 The main symptoms of AF are palpitations, chest tightness, fatigue, and dyspnea, which impair the quality of life of more than 60% of patients.1 Additionally, AF is often accompanied by cardiovascular diseases such as heart failure (HF), coronary artery disease (CAD), hypertension, diabetes, hyperlipidemia, and peripheral arterial disease (PAD).1 In China, 73–90% of patients with AF have two or more cardiovascular diseases, and approximately 72% of deaths in patients with AF are attributed to cardiovascular disease.4–7
Therefore, Lip8 proposed the atrial fibrillation better care (ABC) pathway in 2017 to guide the integrated management of AF. Moreover, the ABC pathway was also strongly recommended by the 2020 European Society of Cardiology (ESC) and 2021 Asia Pacific Heart Rhythm Society (APHRS) guidelines.1,9 The ABC pathway refers to “A, anticoagulation or stroke avoidance”, “B, better control of symptoms through heart rate or rhythm control”, and “C, optimal management of cardiovascular comorbidities and risk factors”.1,8,9 Adherence to the ABC pathway significantly reduces the risk of ischemic stroke, cardiovascular disease, and all-cause mortality (45%, 63%, and 58%, respectively).10 However, Since AF patients are primarily elderly and often have multiple comorbidities, this results in generally very low adherence to the ABC pathway. Improving adherence to the ABC pathway in AF patients is a challenging task worldwide. A study of 285,000 AF patients across developed countries showed that the adherence rate to the ABC pathway was 21%.10 In rural areas of China, where social economy and medical resources are relatively backward, only 5.75% of AF patients adhered to the ABC pathway.5 Improving adherence to the ABC pathway among rural patients with AF is an urgent need.
The integrated theory of health behavior change (ITHBC) has been widely used to guide health behavior change in patients with chronic diseases.11 Based on multiple theories and a large body of empirical research, the ITHBC incorporates three constructs: knowledge and beliefs, self-regulation abilities, and social support.11 (Figure 1). The ITHBC proposed that patients’ knowledge, beliefs, and social support can influence self-regulation ability and consequently change their health behavior.11
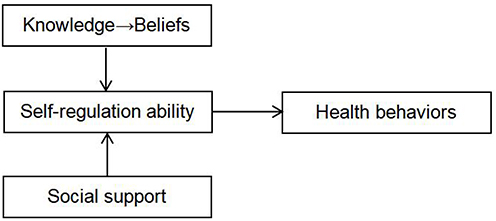 |
Figure 1 The integrated theory of Health Behaviour Change (ITHBC). |
Several studies have validated the relationship between some of the concepts in ITHBC and their effects on health behavior change in patients with AF. A study of patients with AF in high-altitude areas showed that patients’ knowledge and attitude could influence practice.12 Ding et al ’s13 study of patients with AF within 3 months after radiofrequency catheter ablation (RFCA) showed that patients” knowledge of AF, self-management beliefs, and social support were associated with their self-management behavior of AF. A study by Li et al14 showed that knowledge of oral anticoagulants (OACs) in patients with AF was independently associated with attitude and practice. To date, no study has explored the variables of health behavior change that affect adherence to the ABC pathway among rural patients with AF.
Based on the ITHBC, this study aimed to explore the relationship between AF knowledge, AF health beliefs, AF self-management ability, and social support and adherence to the ABC pathway in rural patients with AF in China, to provide supportive evidence and identify intervention targets for improving adherence to the ABC pathway in rural patients with AF.
Methods
Design and Patients
This was a cross-sectional study involving a total of 940 rural patients with AF. The inclusion criteria were patients with an age ≥18 years, diagnosed with AF based on a 24-hour Holter, standard 12-lead ECG recording, or ≥30 second single-lead ECG tracing. All patients had to be able to communicate, understand the content and purpose of the study, and agree to participate in the study. The exclusion criteria were transient AF due to reversible causes (eg, temporary AF induced by surgery, hyperthyroidism, or pulmonary embolism) and terminal stage of malignant cancer or serious mental disorder. The patient inclusion flowchart was presented in Figure 2.
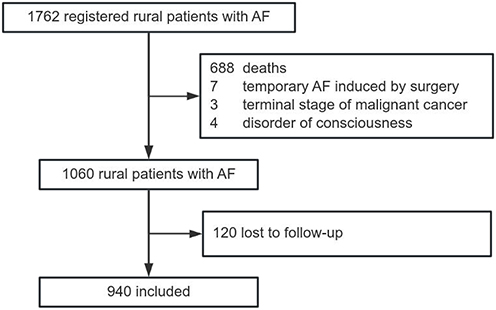 |
Figure 2 Flowchart of AF patients’ selection. |
Sample Size
Because the study explored factors affecting adherence to the ABC pathway based on ITHBC, which is a model with two independent variables and two mediating variables, the sample size requirements of a complex mediating model were referred to when determining the sample size.15 There are no reports on the effect size of this complex mediation model in patients with AF; therefore, we used the sample size of the partial mediation effect and the average effect size model to determine the sample size. The minimum required sample sizes for models with two independent variables and two mediating variables are 480 and 360, respectively.15 Considering a 20% non-response rate, a minimum of 600 patients with AF were required for this study.
Data Collection
Convenience sampling was used in this study. Since all ECG machines in Shangyou County, Ganzhou City, Jiangxi Province, China, were connected to a local general hospital, the medical record system of the general hospital had a list of all patients with a previous diagnosis of AF. After obtaining authorization from the local health management department, we retrieved the list of all patients with AF diagnosed from the general hospital from 2015 to 2022. Then, we selected those registered as permanent residents in local rural areas according to the official household registration system. After excluding patients who had died, were in the terminal stage of malignant tumors, or had disorder of consciousness, we sent a recruitment text message or placed a call to all surviving patients with AF. Patients were invited to attend a local general hospital to complete a data collection form. They were verified by specialist nurses in the chronic disease management center. Missing data were supplemented by interviewing patients on the spot or by reviewing the medical record system. For patients who could not be contacted or had mobility barriers, data were collected by village doctors at home.
Variables and Measurements
Demographic and Clinical Variables
Demographic characteristics included sex, age, education level, marital status, occupation, type of medical insurance, and monthly household income per capita. Clinical characteristics included the type of AF, the duration of AF, history of previous hospitalization for AF, history of previous hospitalization in a department of cardiology or neurology, the CHA2DS2-VASc stroke risk score, the HAS-BLED bleeding risk score, RFCA, left atrial appendage closure (LAAC), pacemaker implantation, the presence of chronic comorbidities, and the medications being used. Multimorbidity was defined as patients having ≥2 chronic conditions in addition to AF.16 Polypharmacy was defined as patients being administered ≥5 medications.17 The medication information was collected based on the patient’s self-reported current medications being taken.
AF Knowledge
AF knowledge was measured using the AF knowledge scale developed by Xu et al18. The questionnaire has five dimensions and 25 items: knowledge of AF, anticoagulation, healthy lifestyle, RFCA, and self-monitoring. A score of 1 was assigned to a correct answer, or “known,” and 0 to an incorrect answer, or “unknown.” The total scores range from 0 to 25. The content validity index of the scale was 0.946. The Cronbach’s α value was 0.835 in this study.
AF Health Beliefs
According to the health belief model, health beliefs include six dimensions: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy.19 AF health beliefs were measured using the Atrial Fibrillation Health Belief Scale (AFHBS) developed by Xu et al18 and the six-item Chinese version of the Chronic Disease Self-Efficacy Scale (CDSES) developed by Lorig20 and translated by Chow et al.21 Because AFHBS and CDSES measured different dimensions of AF health beliefs, the scores of these two scales were summed to obtain the total score of AF health beliefs. The total scores range from 23 to 145.
The AFHBS has five dimensions and 17 items: perceived severity, perceived susceptibility, perceived benefits, perceived barriers, and motivation to maintain health. A 5-point Likert scale was used to score from strongly disagree to strongly agree. The total scores range from 17 to 85. The content validity index of the scale was 0.921.The Cronbach’s α value was 0.840 in this study.
The 6-item CDSES was used to measure self-efficacy. It reflects patients’ confidence in overcoming fatigue, pain management, emotion management, symptom management, activity management, and medication management. Each item was scored from 1 to 10 points. A score of 1 indicated no confidence, and a score of 10 indicated high confidence. The Cronbach’s α value was 0.791 in this study.
AF Self-Management Ability
AF self-management ability was measured using the Self-Management Ability Scale for patients with AF (SMAS-AF), developed by Wen.22 SMAS-AF has five dimensions and 22 items: compliance behavior management, bad habits management, emotional and social management, anticoagulant drug management, and disease prevention and monitoring management. A 5-point Likert scale was used, with each item ranging from “not done” (1 point) to “always done” (5 points). The total scores range from 22 to 110. The content validity index of the scale was 0.926. The Cronbach’s α value was 0.891 in this study.
Social Support
Social support was measured using the Social Support Rating Scale (SSRS) developed by Xiao.23 The SSRS has three dimensions and 10 items: objective support, subjective support, and utilization of social support. The total score of the scale was the sum of the scores of each item, with higher scores indicating better social support. The total scores range from 12 to 66. The Cronbach’s α value was 0.784 in this study.
Adherence to the ABC Pathway
Adherence to the ABC pathway in patients with AF was assessed based on the 2020 ESC guideline criteria.1 A - adherence was defined as patients at a high risk of stroke (CHA2DS2-VASc scores ≥ 2 in males or ≥3 in females) being administered an OAC or LAAC or not at high risk of stroke. Otherwise, patients were classified as A-non-adherence. B - adherence was defined as having European Heart Rhythm Association (EHRA) scores of I (asymptomatic) or II (mild symptoms not affecting daily activities). Otherwise, patients were classified as B-non-adherence. C - adherence was defined as cardiovascular risk or other comorbidities associated with AF that have been treated with appropriate medications or have achieved control standards as follows: (1) Effective control of hypertension defined as baseline blood pressure ≤140/90 mmHg; (2) The treatment for HF included the use of Angiotensin Receptor-Neprilysin Inhibitors (ARNI)/angiotensin converting enzyme inhibitors (ACEI)/angiotensin receptor blockers (ARB) and β-blockers; (3) Treatment for CAD involved the use of ACEI/ARB, β-blockers, and lipid-lowering drugs (LLD); (4) PAD treated with LLD; (5) Stroke/TIA treated with LLD; (6) Diabetes treated with insulin or oral hypoglycaemic drugs; (7) Hyperlipemia treated with LLDs; and (8) A body mass index (BMI)<24.0 kg/m2. Individuals were classified into the C-adherent group when all these diseases were properly medicated or well-controlled, or when individuals were not accompanied by any of these diseases. Otherwise, patients were classified as C-non-adherence. Adherence to the ABC pathway was defined as meeting all three components of the guideline criteria.
Data Analysis
Data analysis was performed using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA) and Mplus version 8.0.24 Categorical variables are reported as frequencies (percentages), while continuous variables are reported as means (standard deviations [SD]). Chi-square tests, t-test and analyses of variance were used to compare sociodemographic characteristics, clinical characteristics, and variables in the ITHBC between ABC-adherent and ABC-non-adherent patients with AF. A correlation analysis was used to analyze the correlation between variables. After controlling for sociodemographic and clinical characteristics that were significant in the univariate analysis, path analysis using bootstrapping with 5000 sample draws was used to explore the mediating hypothesis of the model. P-values < 0.05 (two-sided) were considered statistically significant.
Results
Sample Description
Among the 940 rural patients with AF, 50.7% were male, 79.3% were ≥65 years of age, 56.3% had a primary or lower level of education, 51.9% had a family per capita income of <1000 Renminbi Yuan (RMB), 77.2% were married, 44.5% were farmers, and 30.1% were unemployed. In terms of clinical characteristics, 78.2% had paroxysmal AF, 89.7% had a CHA2DS2-VASc score ≥2 in males or ≥3 in females, 93.1% had a HAS-BLED score ≤2, and 47.8% had a disease duration of ≤1 year. Regarding multimorbidity and polypharmacy, 89.1% patients had ≥2 chronic diseases, and 37.8% were being administered ≥5 medications (Table 1).
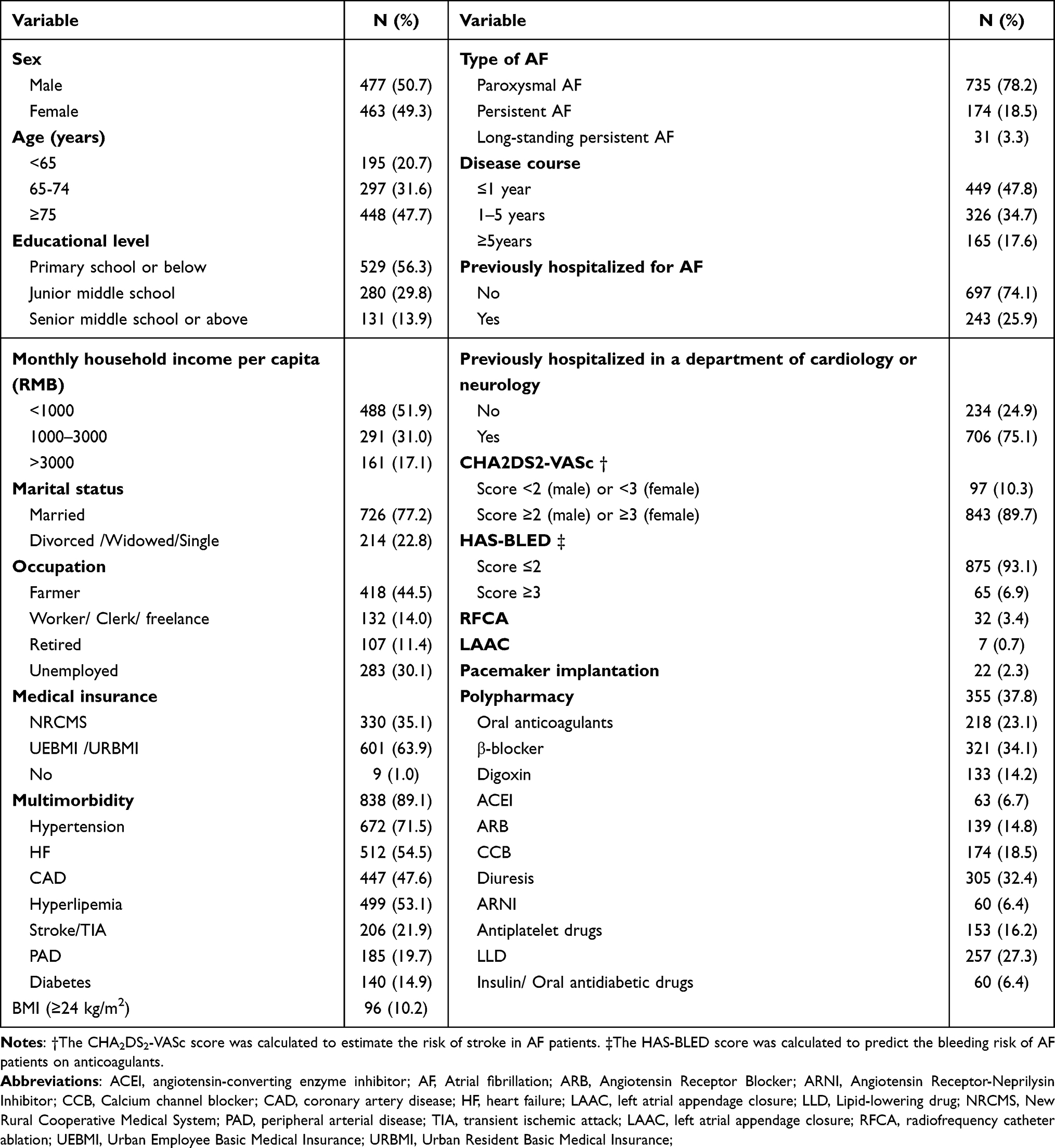 |
Table 1 Sociodemographic and Clinical Characteristics in Rural Patients with AF (N=940) |
Adherence to the ABC Pathway in Rural Patients with AF
In this study, only 5.7% of rural patients with AF adhered to the ABC pathway. Of the three components, component C (management of cardiovascular comorbidities and risk factors) had the lowest adherence rate (19.8%), followed by component A (anticoagulation or stroke avoidance, 32.2%). Approximately half (54.1%) of the patients adhered to component B (control of symptoms) (Table 2).
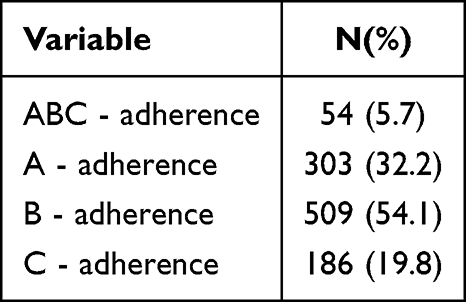 |
Table 2 Adherence to ABC Pathway in Rural Patients with AF. (N=940) |
Descriptions and Correlation Between Study Variables
The level of AF knowledge, AF health beliefs, AF self-management ability and social support of rural patients with AF were extremely low. The total scores were 4.15 ± 3.13, 73.79 ± 14.56, 53.05 ± 10.94 and 27.7 ± 4.80 respectively, which were less than or close to half of the total scores on the scale. There were moderately or highly significant positive correlations between these variables, with correlation coefficients ranging from 0.611 to 0.843. (Table 3).
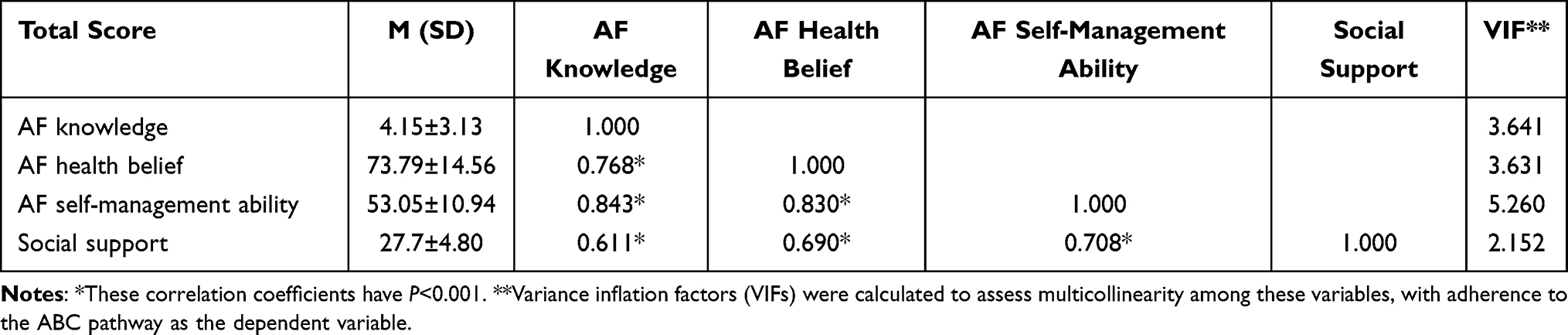 |
Table 3 Descriptions and Correlation Between Study Variables. (N=940) |
Univariate Analysis of Adherence to the ABC Pathway in Rural Patients with AF
Univariate analysis showed that patients with older age, lower education level, no employment or farming as their occupation, low income, persistent AF, and multimorbidity were more likely to be in the ABC-non-adherent group. Patients in the ABC-non-adherent group had lower levels of AF knowledge, AF health beliefs, AF self-management ability, and social support than those in the ABC-adherent group. (Table 4).
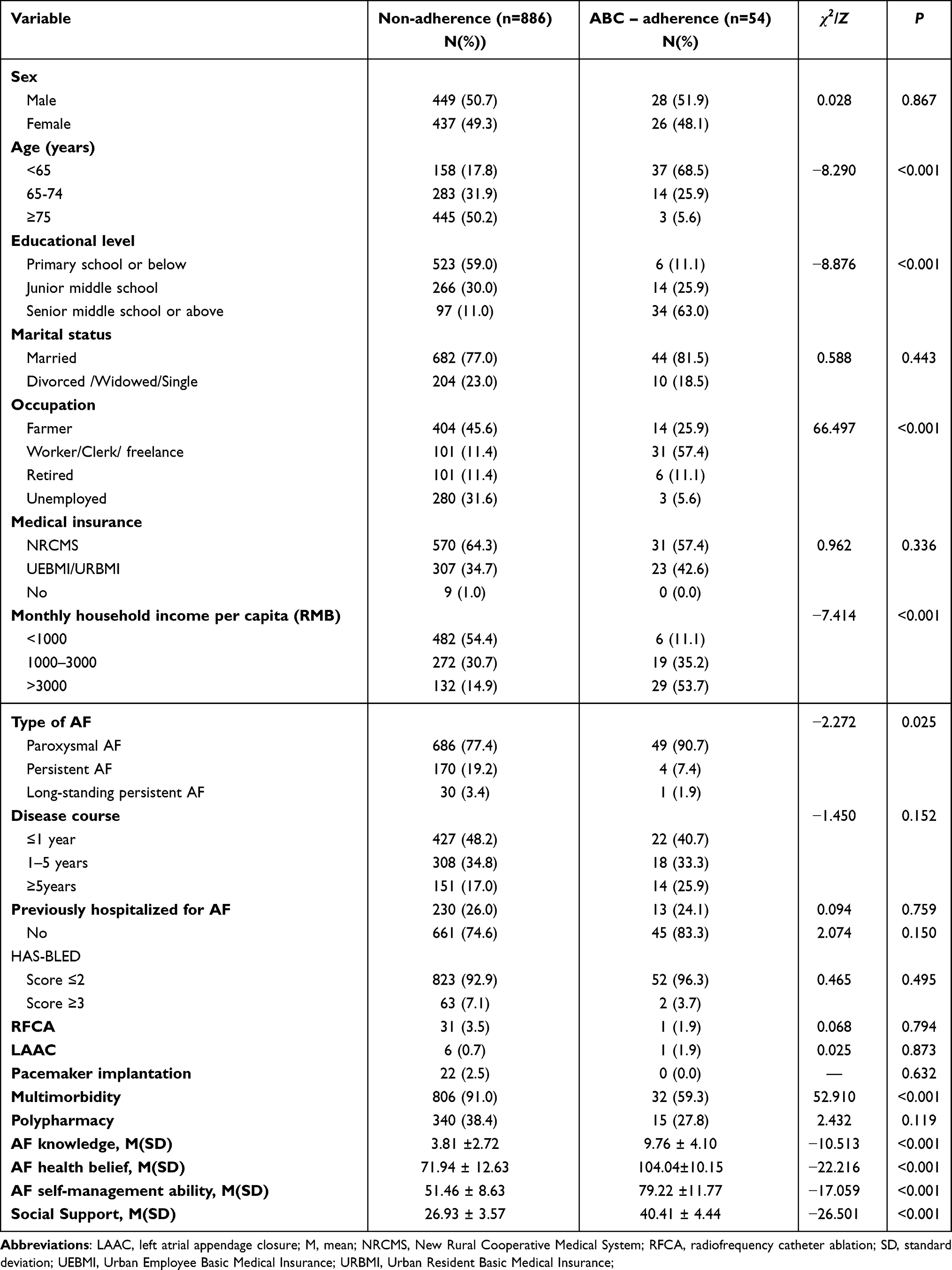 |
Table 4 Univariate Analysis of Adherence to ABC Pathway in Rural Patients with AF. (N=940) |
Test of the Hypothesized Path Models
ITHBC includes three constructs: knowledge and beliefs, self-regulation abilities, and social support. Therefore, path model tests were performed step by step for each construct and the overall construct of ITHBC, respectively (Figure 3). The fit measures for path Models 1 and 2 indicated a good fit (Model 1: χ2/dƒ = 58.603/14=4.186 < 5, RMSEA = 0.058 < 0.08, CFI = 0.984 > 0.9, TLI = 0.970 > 0.9, SRMR = 0.027 < 0.05. Model 2: χ2/dƒ = 34.540/7 = 4.934 < 5, RMSEA = 0.065 < 0.08, CFI = 0.979 > 0.9, TLI = 0.948 > 0.9, SRMR = 0.017 < 0.05). The fit measure for path Model 3 indicated an acceptable overall fit (Model 3: χ2/dƒ = 210.896/15=14.060 > 5, RMSEA = 0.118 > 0.08, CFI = 0.937 > 0.9, TLI = 0.878 > 0.8, SRMR = 0.034 < 0.05). This may mainly be caused by the complexity of the model paths. The R2 values for Models 1, 2 and 3 were 40.7%, 48.9% and 48.0% respectively.
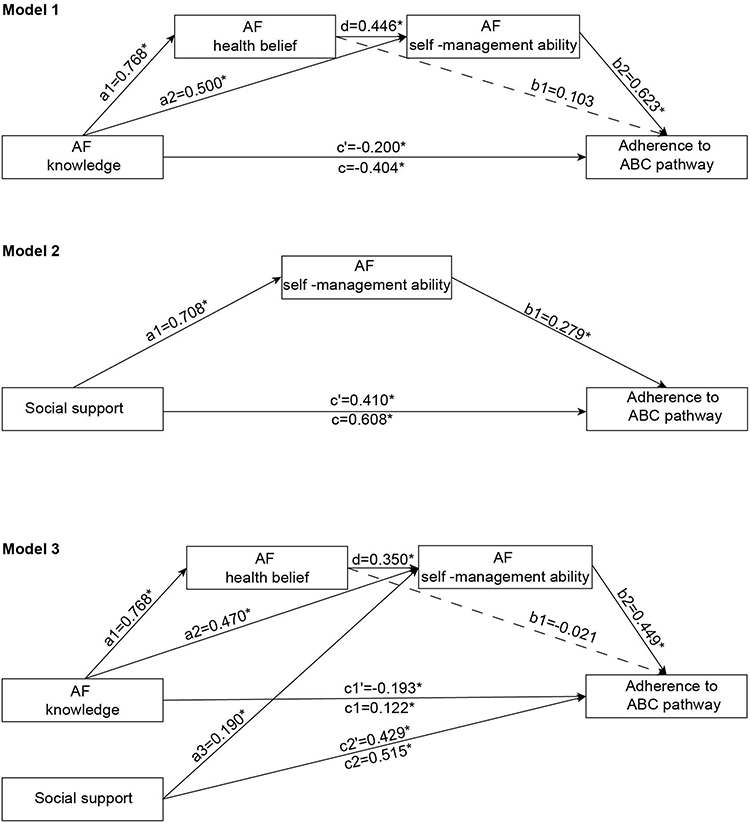 |
Figure 3 Test of the hypothesized model. *:The symbol indicates that the path coefficient has statistical significance (P < 0.05). |
Stepwise path model tests showed stable and consistent results. (Figure 3) Regarding the overall path structure of ITHBC (Model 3), AF self-management ability (β = 0.449, P < 0.001) and social support (β = 0.429, P < 0.001) directly and positively affected adherence to the ABC pathway. Social support also indirectly positively affected adherence to the ABC pathway through AF self-management ability (β = 0.085, P < 0.001, relative mediating effect = 16.5%). AF health beliefs had no direct effect on adherence to the ABC pathway, but they indirectly positively affected adherence to the ABC pathway through AF self-management ability. Possibly due to a masking effect, AF knowledge had a direct negative effect on adherence to the ABC pathway. However, it indirectly positively affected adherence to the ABC pathway through AF self-management ability (β = 0.211, P < 0.001, relative mediating effect = 41.5%). AF knowledge also indirectly positively affected adherence to the ABC pathway through a series of mediations via AF health beliefs and AF self-management ability (β = 0.121, P < 0.001, relative mediating effect = 23.8%). (Table 5).
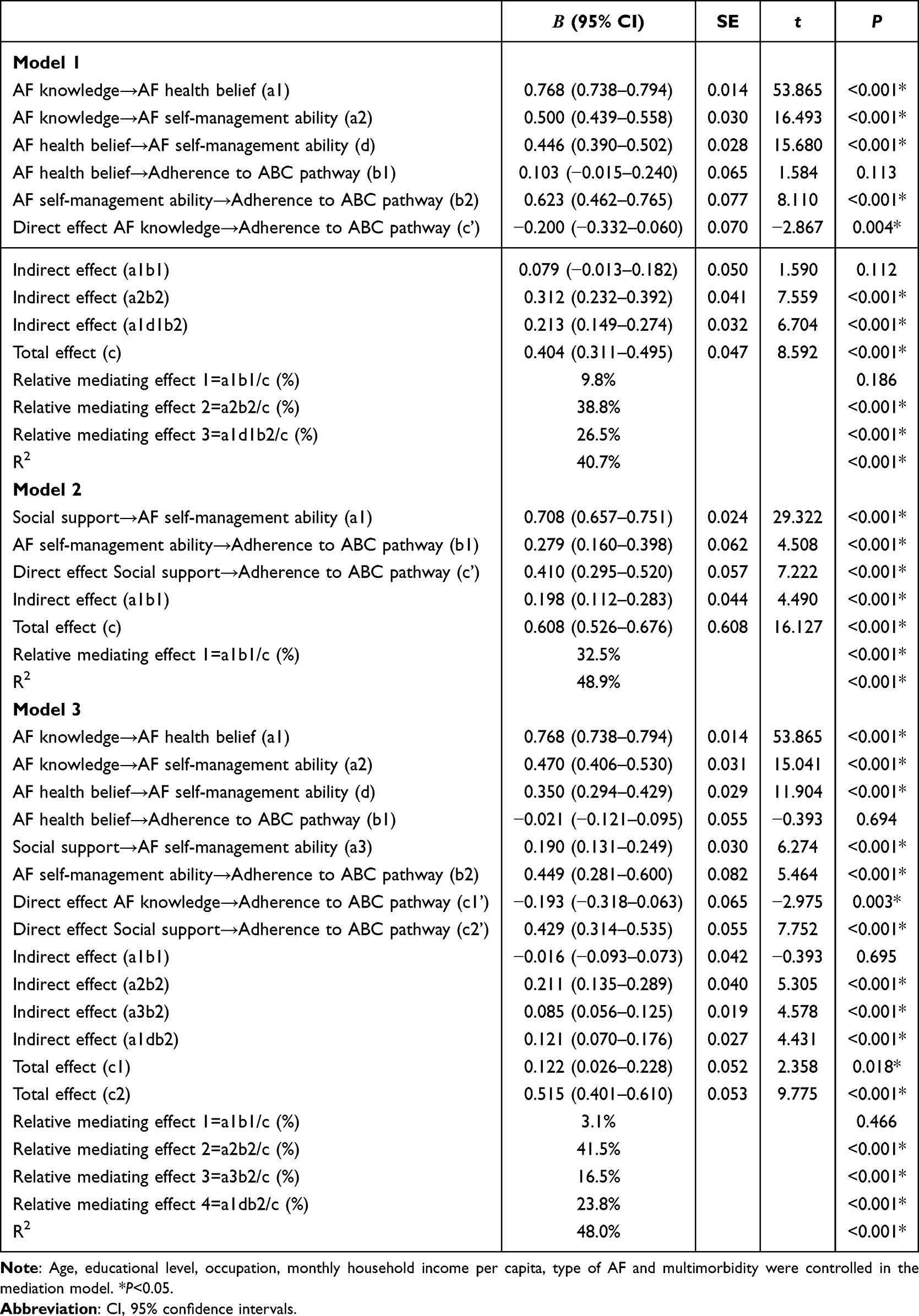 |
Table 5 Mediation Effects Between Study Variables. (N=940) |
Discussion
The study shows that the ITHBC-based pathway model can effectively predict adherence to the ABC pathway in rural patients with AF. Four findings were explored and validated in the study: (1) Adherence to the ABC pathway in rural patients with AF was extremely low (5.7%). (2) AF self-management ability and social support can directly and positively affect adherence to the ABC pathway. (3) AF knowledge, AF health beliefs, and social support can indirectly positively affect adherence to the ABC pathway through AF self-management ability. (4) Although AF health beliefs have no direct effect on adherence to the ABC pathway, the serial mediating effects of AF health beliefs and AF self-management ability also played an important role in the relationship between AF knowledge and adherence to the ABC pathway.
It seems that education and economic status in rural areas are associated with few patients (5.7%) being treated according the ABC pathway in this study, which was much lower than that in developed countries (21%) and urban areas in China (22.8%).10,25,26 Furthermore, considering that 39.5% (688/1762) of the patients died and 11.3% (120/1060) of the patients were lost to follow-up in the medical registration system, the rate of adherence to the ABC pathway for rural patients with AF in the real world might be even lower. Similarly, rural patients also had relatively lower levels of AF knowledge, AF health beliefs, AF self-management ability, and social support. AF knowledge (4.15 ± 3.13 vs 11.79 ± 5.58), AF health beliefs (AFHBS: 59.63 ± 15.67 vs 71.23 ± 6.64; CDSES: 14.16 ± 5.67 vs 32.13 ± 1.50), AF self-management ability (53.05 ± 10.94 vs 76.73 ± 17.54) and social support [27.7 ± 4.80 (total score 66) vs 63.84 ± 10.01, (total score 85)] scores of rural patients with AF were much lower than those of urban patients in China.18,27–29 Furthermore, compared with urban areas, medical resources and quality in rural areas are relatively insufficient.30 It lead to a decrease in the utilization of health care resources in rural patients with AF.31 Therefore, clarify the prediction of adherence to the ABC pathway by AF knowledge, AF health beliefs, social support, and AF self-management ability and elucidating the mechanisms involved based on the ITHBC, and maximizing the accessibility and utilization of medical resources, is of crucial importance for the construction of a targeted and effective integrated management program for rural patients with AF.
In this study, AF self-management ability and social support had a direct positive effect on adherence to the ABC pathway. Although the path analysis showed a negative direct effect of AF knowledge on adherence to the ABC pathway, this may be due to a masking effect. The indirect effect of AF knowledge on adherence to the ABC pathway through AF health beliefs and AF self-management ability was positive. This result is consistent with theories on health behavior change, such as cognitive behavioral theory, the theory of reasoned action, and social cognitive theory. The effect of improving the level of AF knowledge, AF self-management ability, and social support on improving adherence to “A” (ie, anticoagulation) has been widely verified.32,33
AF knowledge, AF health beliefs, and social support also had indirect positive effects on adherence to the ABC pathway through AF self-management ability in the study. The same result was shown in a study predicting lymphedema self-management behavior in patients with breast cancer that was based on the ITHBC.34 AF self-management ability is an important mediating variable for improving adherence to the ABC pathway. Model 3 showed that AF self-management ability had the largest positive direct effect on adherence to the ABC pathway. The indirect positive effects of AF knowledge and social support on adherence to the ABC pathway through AF self-management ability accounted for 41.5% and 16.5% of the total effect, respectively. The serial mediating effect of AF health beliefs and AF self-management ability between AF knowledge and adherence to the ABC pathway accounted for 23.8% of the total effect. A study showed that the activation of self-management ability was positively associated with health outcomes in patients with AF.35 It suggests that future intervention strategies should focus more on strengthening AF self-management ability and consider AF knowledge, AF health beliefs, and social support as important components of self-management interventions.
Notably, there was no direct effect of AF health beliefs on adherence to the ABC pathway in the current study. This is inconsistent with the findings in other studies, which showed that health beliefs directly influence health behaviors.14 In the current study, the effect of AF health beliefs on adherence to the ABC pathway was fully mediated by AF self-management ability. This may be mainly due to the poor AF self-management abilities of rural patients with AF. Consequently, patients do not have the corresponding skills and abilities for self-management, even if they are confident enough to actively change their health behaviors. However, this does not mean that AF health beliefs are not important for adherence to the ABC pathway in rural patients with AF. The serial mediation of AF health beliefs and AF self-management ability between AF knowledge and adherence to the ABC pathway was the second largest mediating effect. AF health belief is also a key component of intervention strategies for rural patients with AF, and it should be closely integrated with the components of AF knowledge and AF self-management ability.
Limitations
This study has some limitations. Firstly, this is a cross-sectional study. Although path analysis can explain complex relationships between variables, its application to inferring causal relationships is limited. In the future, prospective longitudinal studies or empirical studies are needed to further verify the effects and mechanism of the variable model based on ITHBC on adherence to the ABC pathway in rural patients with AF. Secondly, the risk factors assessed in the C component of this study were not comprehensive enough, and future research should further consider lifestyle-related factors. Thirdly, the integrated management of patients with AF requires the cooperation of patients and medical multidisciplinary teams. The study only explored patient-related factors. Further exploration of the influencing factors and perceptions of other stakeholders on patients’ adherence to the ABC pathway is required. Fourth, although Models 1 and 2 have good fits, some of the fit indicators of Model 3 were only close to the fit criteria. Therefore, Model 3 was mainly used to test the path relationships and conclusion reliability based on the complete ITHBC model in the study, rather than as an accurate effect estimation model. Finally, the study was conducted among rural patients with AF from only one county in China. Therefore, the conclusions of the study need to be extrapolated with caution.
Conclusions
Adherence to the ABC pathway by rural patients with AF in China is extremely low. In the current study, the path analysis based on ITHBC elucidated the effects and mechanisms of AF knowledge, AF health beliefs, AF self-management ability, and social support on adherence to the ABC pathway among rural patients with AF. AF self-management ability has the greatest direct positive effect and an important mediating effect on adherence to the ABC pathway. AF knowledge, AF health beliefs, and social support have indirect positive effects on adherence to the ABC pathway through AF self-management ability. We suggest that effective interventions to strengthen AF self-management ability should be explored among rural patients with AF in the future, and that AF knowledge, AF health beliefs, and social support should be closely combined with AF self-management ability as important intervention components.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, Xiaomin Zhang or Kun Li.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and has been approved by the Medical Ethics Committee of the People’s Hospital of Shangyou, China (approval number:SYRY-20220716-002). Confidentiality of patients personal information was ensured, and informed consent was obtained from all patients.
Acknowledgment
Thanks to Xu wenhua et al, Wen xiu, Xiao shuiyuan, lorig et al, and Chow et al, for the development and authorization of the relevant scales. Thanks for the support of all the doctors, nurses and patients in the study.
Funding
This study was supported by the Guangdong Provincial Science and Technology Planning Project (Grant No. 2023B110009).
Disclosure
The authors report no conflicts of interests in this work.
References
1. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373–13. doi:10.1093/eurheartj/ehaa612
2. Du X, Guo L, Xia S, et al. Atrial fibrillation prevalence, awareness and management in a nationwide survey of adults in China. Heart. 2021;107(7):535–541. doi:10.1136/heartjnl-2020-317915
3. Choi SE, Sagris D, Hill A, Lip GYH, Abdul-Rahim AH. Atrial fibrillation and stroke. Expert Rev Cardiovasc Ther. 2023;21(1):35–56. doi:10.1080/14779072.2023.2160319
4. Kotalczyk A, Guo Y, Stefil M, Wang Y, Lip GYH. ChiOTEAF Registry Investigators. Effects of the atrial fibrillation better care pathway on outcomes among clinically complex chinese patients with atrial fibrillation with multimorbidity and polypharmacy: a report from the ChiOTEAF registry. J Am Heart Assoc. 2022;11(7):e24319. doi:10.1161/JAHA.121.024319
5. Zhang X, Wang W, Zeng J, et al. Adherence to the atrial fibrillation better care pathway and its associated factors among rural patients with atrial fibrillation in China: a cross-sectional study. Heart Lung. 2024;66:23–30. doi:10.1016/j.hrtlng.2024.03.002
6. Zhang X, Huang J, Weng F, et al. Adherence to Atrial Fibrillation Better Care (ABC) pathway management of Chinese Community elderly patients with atrial fibrillation: a cross-sectional study. Patient Prefer Adherence. 2023;17:1813–1823. doi:10.2147/PPA.S417384
7. Pokorney SD, Piccini JP, Stevens SR, et al. Cause of death and predictors of all-cause mortality in anticoagulated patients with nonvalvular atrial fibrillation: data from ROCKET AF. J Am Heart Assoc. 2016;5(3):e2197. doi:10.1161/JAHA.115.002197
8. Lip GYH. The ABC pathway: an integrated approach to improve AF management. Nat Rev Cardiol. 2017;14(11):627–628. doi:10.1038/nrcardio.2017.153
9. Chao TF, Joung B, Takahashi Y, et al. 2021 focused update consensus guidelines of the Asia Pacific Heart Rhythm Society on stroke prevention in atrial fibrillation: executive summary. Thromb Haemost. 2022;122(1):20–47. doi:10.1055/s-0041-1739411
10. Romiti GF, Pastori D, Rivera-Caravaca JM, et al. Adherence to the ‘atrial fibrillation better care’ pathway in patients with atrial fibrillation: impact on clinical outcomes–A systematic review and meta-analysis of 285,000 patients. Thromb Haemost. 2022;122(3):406–414. doi:10.1055/a-1515-9630
11. Ryan P. Integrated theory of health behavior change: background and intervention development. Clin Nurse Spec. 2009;23(3):161–170,171–2. doi:10.1097/NUR.0b013e3181a42373
12. Li K, Liu J, Zhu Y. Knowledge, attitude, and practice of atrial fibrillation in high altitude areas. Front Public Health. 2024;12:1322366. doi:10.3389/fpubh.2024.1322366
13. Ding Y, Li F, Fan Z, et al. Factors influencing self-management behavior during the “Blanking Period” in patients with atrial fibrillation: a cross-sectional study based on the information-motivation-behavioral skills model. Heart Lung. 2023;58:62–68. doi:10.1016/j.hrtlng.2022.11.006
14. Li C, Meng Y, Meng X, Song Y. Knowledge, attitude and practice toward oral anticoagulants among patients with atrial fibrillation. Front Cardiovasc Med. 2023;10:1301442. doi:10.3389/fcvm.2023.1301442
15. Sim M, Kim SY, Suh Y. Sample size requirements for simple and complex mediation models. Educ Psychol Meas. 2022;82(1):76–106. doi:10.1177/00131644211003261
16. Diederichs C, Berger K, Bartels DB. The measurement of multiple chronic diseases--a systematic review on existing multimorbidity indices. J Gerontol a Biol Sci Med Sci. 2011;66(3):301–311. doi:10.1093/gerona/glq208
17. Viktil KK, Blix HS, Moger TA, Reikvam A. Polypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problems. Br J Clin Pharmacol. 2007;63(2):187–195. doi:10.1111/j.1365-2125.2006.02744.x
18. Xu W, Sun G, Lin Z, et al. Knowledge, attitude, and behavior in patients with atrial fibrillation undergoing radiofrequency catheter ablation. J Interv Card Electrophysiol. 2010;28(3):199–207. doi:10.1007/s10840-010-9496-2
19. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. 1984;11(1):1–47. doi:10.1177/109019818401100101
20. Lorig KR, Sobel DS, Ritter PL, Laurent D, Hobbs M. Effect of a self-management program on patients with chronic disease. Eff Clin Pract. 2001;4(6):256–262.
21. Chow SK, Wong FK. The reliability and validity of the Chinese version of the Short-form chronic disease self-efficacy scales for older adults. J Clin Nurs. 2014;23(7–8):1095–1104. doi:10.1111/jocn.12298
22. Wen X. Development, reliability and validity of the self management ability scale for atrial fibrillation patients. Eur J Cardiovasc Nurs. 2021. doi:10.27235/d.cnki.gnjiu.2020.000718
23. Xiao S. Theoretical basis and research application of social support rating scale. J Clin Psychiatry. 1994;(02):98–100.
24. Muthen LK, Muthen BO. Mplus user’s guide (eighth); 1998.
25. Guo Y, Imberti JF, Kotalczyk A, Wang Y, Lip GYH. ChiOTEAF Registry Investigators. 4S-AF scheme and ABC pathway guided management improves outcomes in atrial fibrillation patients. Eur J Clin Invest. 2022;52(6):e13751. doi:10.1111/eci.13751
26. Wang YF, Jiang C, He L, et al. Integrated care of atrial fibrillation using the ABC (Atrial fibrillation Better Care) pathway improves clinical outcomes in Chinese population: an analysis from the Chinese atrial fibrillation registry. Front Cardiovasc Med. 2021;8:762245. doi:10.3389/fcvm.2021.762245
27. Song T, Xin X, Cui P, Zong M, Li X. Factors associated with anticoagulation adherence in Chinese Patients with non-valvular atrial fibrillation. Patient Prefer Adherence. 2021;15:493–500. doi:10.2147/PPA.S285020
28. Ding YM. Investigation on the status quo and influencing factors of self-management behavior in patients with atrial fibrillation based on IMB model. Patient Prefer Adherence. 2023. doi:10.27262/d.cnki.gqdau.2023.000464
29. Ding YM, Liu CP, Xu HX, et al. Effect of social support on illness perception in patients with atrial fibrillation during “Blanking Period”: mediating role of sense of mastery. Nurs Open. 2023;10(1):115–122. doi:10.1002/nop2.1284
30. Zhu Y, Wang Y, Shrikant B, et al. Socioeconomic disparity in mortality and the burden of cardiovascular disease: analysis of the Prospective Urban Rural Epidemiology (PURE)-China cohort study. Lancet Public Health. 2023;8(12):e968–e977. doi:10.1016/S2468-2667(23)00244-X
31. Jiang S, Seslar SP, Sloan LA, Hansen RN. Health care resource utilization and costs associated with atrial fibrillation and rural-urban disparities. J Manag Care Spec Pharm. 2022;28(11):1321–1330. doi:10.18553/jmcp.2022.28.11.1321
32. Magon A, Hendriks JM, Conte G, Caruso R. Description of self-care behaviours in patients with non-valvular atrial fibrillation on oral anticoagulant therapy: a scoping review. Eur J Cardiovasc Nurs. 2024;zvae007. doi:10.1093/eurjcn/zvae007
33. Schwanda M, Gruber R. Increased knowledge of oral anticoagulants and treatment satisfaction leads to better adherence to oral anticoagulants in patients with atrial fibrillation. Evid Based Nurs. 2020;23(2):48. doi:10.1136/ebnurs-2018-103013
34. Shen A, Wu P, Qiang W, et al. Predicting lymphedema self-management behaviours in breast cancer patients: a structural equation model with the integrated theory of health behaviour change. J Adv Nurs. 2023;79(12):4778–4790. doi:10.1111/jan.15759
35. McCabe PJ, Stuart-Mullen LG, McLeod CJ, et al. Patient activation for self-management is associated with health status in patients with atrial fibrillation. Patient Prefer Adherence. 2018;12:1907–1916. doi:10.2147/PPA.S172970
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Parental Acceptance of Human Papillomavirus (HPV) Vaccination in Districts with High Prevalence of Cervical Cancer in West Java, Indonesia
Frianto D, Setiawan D, Diantini A, Suwantika AA
Patient Preference and Adherence 2022, 16:2709-2720
Published Date: 29 September 2022
Chinese Community Home-Based Aging Institution Elders’ Self-Management of Chronic Non-Communicable Diseases and Its Interrelationships with Social Support, E-Health Literacy, and Self Efficacy: A Serial Multiple Mediation Model
Wu Y, Wen J, Wang X, Wang Q, Wang W, Wang X, Xie J, Cong L
Patient Preference and Adherence 2023, 17:1311-1321
Published Date: 25 May 2023
Diabetes Distress Among Patients Undergoing Surgery for Diabetic Retinopathy and Associated Factors: A Cross-Sectional Survey
Zhang M, Zhang X, Yang Y, Weng Y, Chen X, Chen Y, Shi Y
Psychology Research and Behavior Management 2024, 17:1451-1461
Published Date: 2 April 2024
Knowledge, Attitude, and Practice Toward Hyperuricemia Among Patients Diagnosed with Hyperuricemia
Xiang D, Yuan L, Wu Y, Yuan Y, Liao S, Chen W, Zhang M, Zhang Q, Ding L, Wang Y
Journal of Multidisciplinary Healthcare 2025, 18:2845-2858
Published Date: 22 May 2025
A Cross-Sectional Study on Chinese Geriatricians’ Knowledge, Attitudes, and Practices Regarding Oral Anticoagulants for Atrial Fibrillation Patients
Chen Y, Liang Y, Qin M, Liu Q
Journal of Multidisciplinary Healthcare 2025, 18:4739-4747
Published Date: 6 August 2025