Back to Journals » Psychology Research and Behavior Management » Volume 17
Diabetes Distress Among Patients Undergoing Surgery for Diabetic Retinopathy and Associated Factors: A Cross-Sectional Survey
Authors Zhang M ![]() , Zhang X
, Zhang X ![]() , Yang Y, Weng Y
, Yang Y, Weng Y ![]() , Chen X
, Chen X ![]() , Chen Y
, Chen Y ![]() , Shi Y
, Shi Y ![]()
Received 20 December 2023
Accepted for publication 14 March 2024
Published 2 April 2024 Volume 2024:17 Pages 1451—1461
DOI https://doi.org/10.2147/PRBM.S455535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Mengyue Zhang,1 Xiaoxian Zhang,1 Yingrui Yang,2 Yu Weng,3 Xiaojun Chen,1 Yanyan Chen,3 Yinghui Shi3
1School of Ophthalmology and Optometry, Wenzhou Medical University, Wenzhou, People’s Republic of China; 2Department of Nursing, Henan Provincial People’s Hospital, Zhengzhou, People’s Republic of China; 3Department of Nursing, The Eye Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China
Correspondence: Yanyan Chen; Yinghui Shi, The Eye Hospital, School of Ophthalmology and Optometry, Wenzhou Medical University, 270 West Xueyuan Road, Wenzhou, Zhejiang, 325027, People’s Republic of China, Tel +86 138 5885 5689 ; +86 138 6844 0966, Email [email protected]; [email protected]
Background: Diabetes distress (DD) is a negative emotion related to diabetes management and a predictor of depression; it affects diabetic retinopathy (DR) patients’ quality of life and disease outcomes. The prevalence of DD was higher in patients undergoing surgery for DR. However, few studies have been conducted on DD in DR surgery patients. The present study aims to investigate the status of DD in DR surgery patients and identify factors associated with DD.
Methods: Using a convenience sampling method, 210 DR surgery patients who were admitted to 2 tertiary-level hospitals in Wenzhou City (Zhejiang Province) and Zhengzhou City (Henan Province) from February to June 2023 were selected as research subjects. A questionnaire collecting demographic and disease-related information, the Diabetes Distress Scale, the Summary of Diabetes Self-Management Activities, the Family Care Index Scale, and the Social Support Rating Scale were used to collect data. Statistical analyses included descriptive statistics, t tests, ANOVAs, Pearson’s correlation analyses and stepwise multiple linear regression. This study is reported according to the STROBE guidelines.
Results: In total, 156 out of 210 (74.29%) DR surgery patients experienced DD, with an average score of 2.13± 0.63. The results of the stepwise multiple regression analysis showed that residential location, employment status, self-management level, family support, and social support were significantly associated with DD. These variables accounted for 30.6% of the total variation in DD.
Conclusions: DR surgery patients exhibit moderate levels of distress. Health care professionals should pay attention to DD in DR surgery patients and develop targeted interventions to improve the self-management ability of these patients, increase their family support and social support to reduce their DD levels.
Keywords: diabetic retinopathy, diabetes distress, self-management, family support, social support
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Wang has been published for this article.
Introduction
Diabetic retinopathy (DR) is the leading cause of vision loss in working-age adults.1 As the most common microvascular complication from diabetes, blindness and low vision from DR has become a major public health challenge.2 Vitrectomy is one of the mainstays of DR treatment. However, patients are only able to partially recover or retain vision after surgery, and most patients continue to experience psychological, emotional, and social problems.3 Meanwhile, visual impairment due to DR has an enormous impact on the quality of life of patients.4 Impaired vision can result in limited mobility, restricted activities and limited socialization, which can lead to concern and emotional distress for the patient.5
Diabetic distress (DD) is a negative emotional response due to worries about diabetes-related disease management, disease support, treatment pathways and emotional burdens.6 It accompanies emotional disturbances, stress, guilt feelings, and avoidance of treatment.7 DD is a psychological disturbance that differs from depression and a predictor of depression.8 DD is more prevalent than depression in patients with diabetes and is more closely associated with diabetes self-management and glycaemic control.9,10 The results of a meta-analysis including 55 studies from high- and middle-income countries showed that more than one-third of patients with type 2 diabetes experienced DD.11 A study conducted in 17 countries, including India and China, showed that 45% of patients with diabetes experienced DD.12 Current standards of medical care recommend routine monitoring of DD in patients.13 These sobering statistics and clinical recommendations indicate that DD has become one of the important mental health issues in diabetic patients.
Some studies have suggested that the prevalence of DD may be higher in DR patients treated with Vitrectomy surgery.14 Due to the filling of gas and silicone oil, DR patients will not experience a significant change in vision immediately after surgery compared to pre-surgery; those who have had silicone oil injected require a second surgery to remove the silicone oil; the patient often requires to maintain the head-down position and side-lying position alternately after surgery. The uncertainty of the disease prognosis, the uncertainty of the time of the second surgery, and the discomfort of the special position all increase negative emotions such as anxiety, depression, and psychological distress.15 However, at present, the studies related to DD have mostly focused on diabetic patients, with only a few focusing on DR surgery patients, especially on DD at discharge of DR surgery patients, and these studies have limitations such as narrow sampling regions and small sample sizes.8,14
Diabetic patients need more support, including family support and social support. Indeed, people with diabetes who report more adequate family support are more motivated to engage in self-management behaviours such as diet, exercise, glucose monitoring, medication, and foot care and have lower levels of DD.10,16,17 Self-management behaviours largely occur within the social contexts of individuals.16 Therefore, the social context impacts DD. For this reason, assessments of DD explicitly include social components. For example, the Diabetes Distress Scale contains an interpersonal distress dimension that involves asking if family/friends understand the difficulties experienced by diabetic patients.18 Therefore, self-management, family support, and social support are expected to have a significant impact on DD among diabetic patients. In addition, DD is associated with age, gender, education level, residential location, family income, diabetes treatment modality, diabetes duration and complications.19–23 However, the impact of the above factors on DD in DR surgery patients needs to be further explored.
Therefore, this study investigated DD among DR surgery patients in 2 provinces in China with a cross-sectional design and identified factors associated with DD, which is expected to inform the development of measures to safeguard the psychological health of DR surgery patients and inform patient-centered design of technology solutions.
Materials and Methods
Design
This study was a cross-sectional and descriptive study. Simultaneously, the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist was used to report the findings (See Table S1 for details).24
Participants
Convenience sampling was used to recruit 214 DR surgery patients from 2 tertiary-level hospitals in Wenzhou City (Zhejiang Province) and Zhengzhou City (Henan Province), China. The inclusion criteria were as follows, (1) met the relevant diagnostic criteria for DR in the Clinical Diagnosis and Treatment Guidelines for DR in China,25 (2) underwent vitrectomy, (3) aged ≥18 years and (4) had normal verbal communication skills. The exclusion criteria were as follows, (1) cognitive impairment or mental disorder, or (2) receiving or having received psychological interventions.
The necessary sample size for the stepwise regression analysis was calculated using G*Power 3.1.26 With six predictive variables, a significance level of 0.05, statistical power (1 − β) of 0.85, and effect size of 0.15, a minimum sample size of 109 patients was estimated. Considering a rate of invalid data of 20%, a total of 131 patients were needed; more than this number of patients were recruited.
Data Collection
Data were collected with a questionnaire administered by the researcher of the present study from February to June 2023. Demographic and disease-related information was obtained from electronic medical records and electronic nursing record data. Before completing the questionnaire, patients were informed about the questionnaire by the researcher. Then, the patients completed the questionnaire. Questionnaire completion occurred before the patient was discharged from the hospital. If patients had low vision or questions about the questionnaire, the researcher provided nonleading explanations to assist the patient. Immediately after the patient completed the questionnaire, the researcher checked the questionnaire. If any values were missing, the patient was reminded to complete the items to improve the quality of the collected data.
Outcomes and Measurements
Demographic and Disease-Related Information
A custom-designed questionnaire was used to collect the demographic and disease-related information of participants. It included items on demographic characteristics (gender, age, marital status, education level, employment status, residential location, mode of residence, and monthly per person household income) and disease-related items (duration of the disease, diabetes medication type, comorbid chronic diseases, other complications, glycosylated haemoglobin A1c (HbA1c) levels and the best-corrected visual acuity (VA)).
The VA of all patients was examined using an international standardized visual acuity chart. For the purpose of analysis, the decimal VA was converted to logMAR. In addition, VA was stratified into three categories, good vison (<0.3 logMAR), moderate vision loss (0.3–1.0 logMAR), and severe vision loss (>1.0 logMAR).27 In this study, visual acuity that enabled counting fingers, detecting hand motions, perceiving light and the inability to perceive light corresponded to logMAR values of 2.6, 2.7, 2.8 and 2.9, respectively.28
Diabetes Distress
Diabetes distress was measured using the Diabetes Distress Scale (DDS), which was developed by American scholars Polonsky18 in 2005. The scale consists of 4 subscales, emotional burden (EB), regimen-related distress (RD), physician-related distress (PD) and interpersonal distress (ID). It has a total of 17 items, which are rated on a 6-point Likert scale, ranging from 1 (not a problem) to 6 (a very serious problem). A mean score of less than 2 indicates no to low distress, 2 to 2.9 indicates moderate distress, and 3 or higher indicates severe distress. The scale was translated into Chinese by Yang and Liu in 2010.29 Cronbach’s α coefficient was 0.842 to 0.951.
Self-Management
Self-management was measured by the Summary of Diabetes Self-Care Activities (SDSCA), which was developed by Toobert30 in 2000 and translated into Chinese by Wan31 in 2008. It reflects diabetes patients’ self-management behaviours in the recent week. The scale consists of 5 subscales, including healthy diet, physical activity, blood glucose testing, foot care and medication taking, with a total of 11 items. Items are scored on an 8-point Likert scale, ranging from 0 to 7, with higher scores indicating greater self-management behaviours. The Cronbach’s α coefficient of the scale was 0.918.
Family Support
Family support was measured using the Family Care Index Scale (APGAR), which was developed by Smilkstein32 in 1978 and translated into Chinese by Lu and Gu33 in 1995. The questionnaire consists of five items, adaptation, partnership, growth, affection, and resolve. Items are scored on a 3-point Likert scale, 0 = rarely, 1 = sometimes, and 2 = always. The total score ranges from 0 to 10. A total score of 0~3 indicates severe family dysfunction; 4~6 indicates moderate family dysfunction; and 7~10 indicates good family functioning. The Cronbach’s α coefficient of the scale was 0.790.
Social Support
Social support was measured using the Social Support Rating Scale (SSRS), which was developed by a Chinese scholar Xiao34 in 1994. It is used to assess the social support of individuals. It contains 3 dimensions, subjective support, objective support, and utilization of support. It has a total of 10 items. The total score ranges from 12 to 66, and the higher the score is, the better the social support. Total scores of ≤22, 23~44, and 45~66 indicate low, medium, and high levels of social support, respectively. The Cronbach’s α coefficient of the scale was 0.92.
Data Analysis
Data entry and verification were performed by two people in Epidata version 3.1. IBM SPSS Statistics version 26.0 was used to analyse the data. Before the analysis was performed, the data were checked for missing values, outliers and normality. No outliers were found in the data, and 4 questionnaires with missing values were excluded. To determine whether the data had a normal distribution, kurtosis and skewness coefficients were calculated and a histogram was examined. In addition, the Kolmogorov–Smirnov and Shapiro–Wilk tests were performed. Frequencies, percentages, means and standard deviations are used to describe the demographic and disease-related data of DR patients in the present study. Student’s t tests and one-way ANOVAs were used to compare the differences between DDS scores and demographic and disease-related data. The relationship between DD and related factors was examined with Pearson correlation analysis. Stepwise multiple linear regression was used to analyse the factors affecting DD. In this study, P<0.05 was taken to indicate a significant difference.
Ethical Considerations
The study was approved by the ethics committee of each hospital (No, 2022–045-K-30-01 and HNEEC-2023(33)). The investigators explained the study to all participants. Patients who volunteered to participate in the study signed an informed consent form. Patients understood that they could refuse to participate at any time and that their decision would not affect their further treatment.
Results
Participant Characteristics
A total of 214 patients were recruited and questionnaires were distributed. A total of 210 valid questionnaires were recovered. The effective recovery rate was 98.13%. Among the DR patients, 61.90% (n=130) were male, 82.38% (n=173) were married, 56.67% (n=119) were from urban areas, and 58.57% (n=123) had an HbA1c >7%. Other characteristics of the DR patients are shown in Table 1.
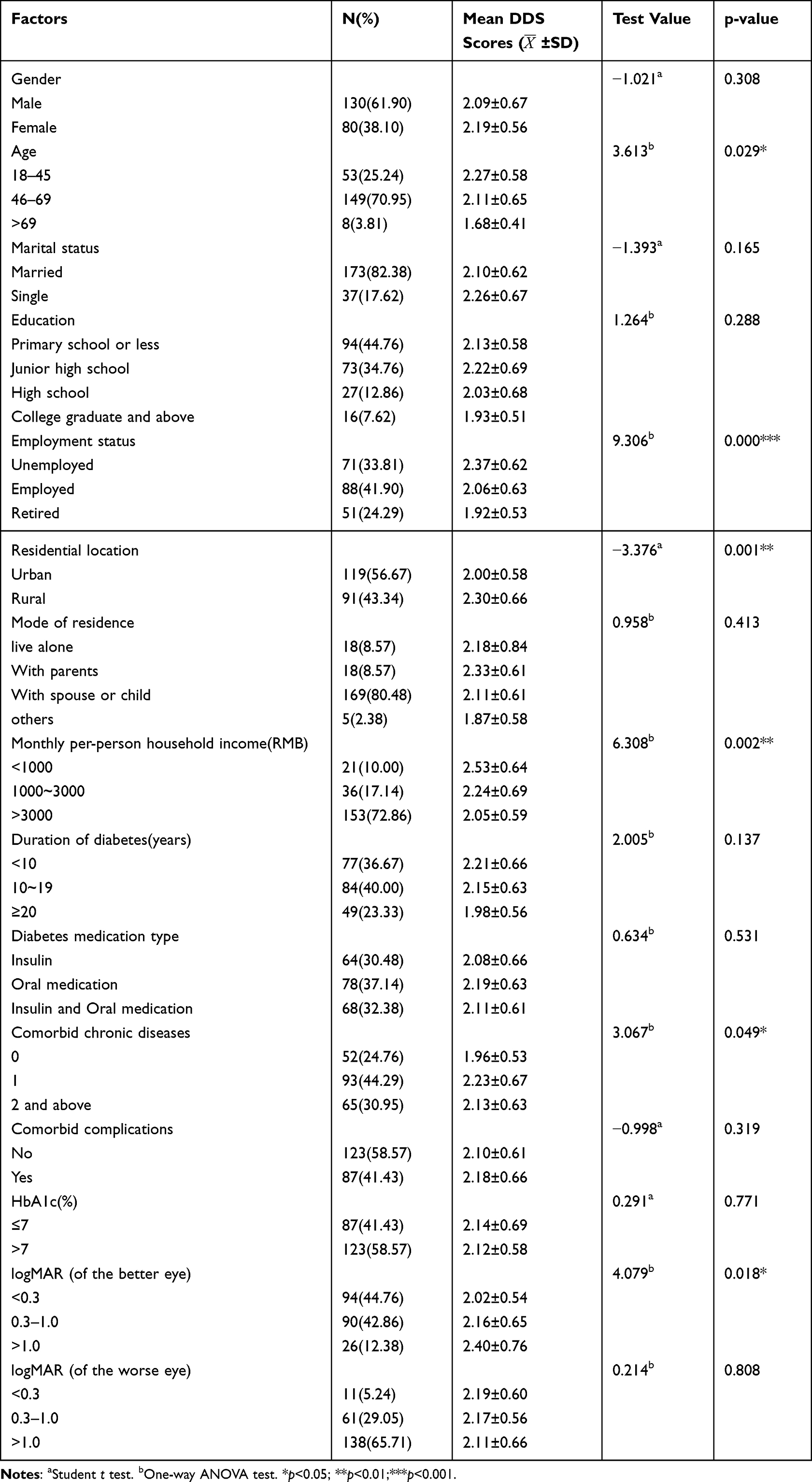 |
Table 1 Participants’ Characteristics and Univariate Analyses of the Factors Associated with DDS Scores of the Participants (N=210) |
Levels of Diabetes Distress Among DR Surgery Patients and Other Outcomes
The DDS total score of the DR surgery patients was 36.24±10.71, and the mean entry score on the DDS was 2.13±0.63. Diabetes distress was exhibited by 156 individuals (ie, the mean score of the entries was >2.0), and the prevalence of diabetes distress was 74.29% (95% CI:0.684~0.802). The DR patients’ mean scores were 33.34±12.35 for self-management, 8.11±2.56 for family support, and 38.84±7.33 for social support. See Table 2 for details.
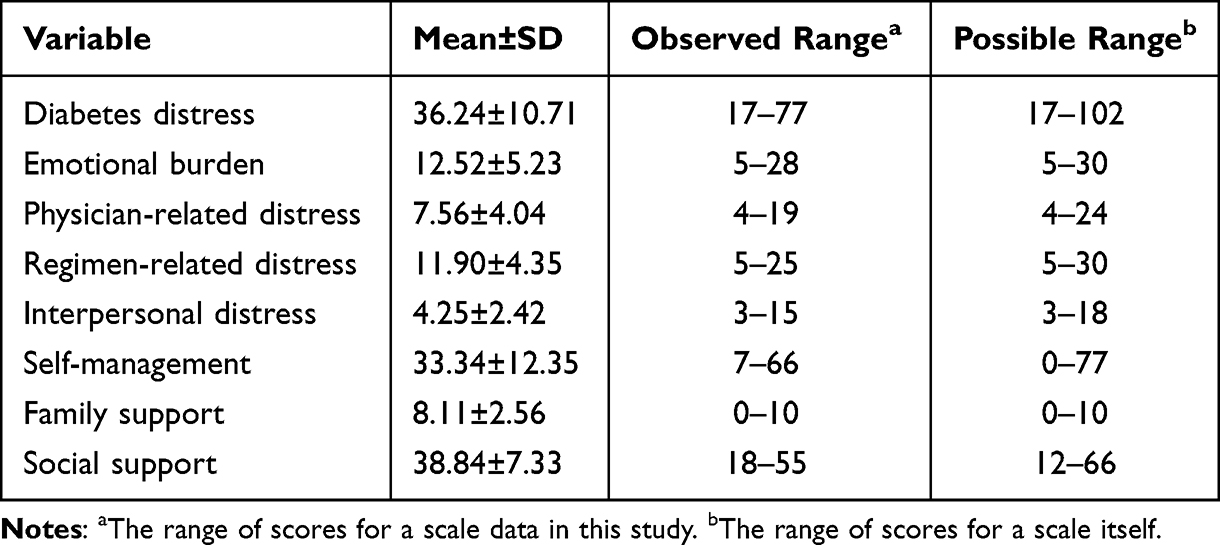 |
Table 2 Levels of Diabetes Distress Among DR Surgery Patients and Other Outcomes |
Univariate Analysis of Diabetes Distress in DR Surgery Patients
The results of univariate analysis showed that DDS scores significantly differed among DR surgery patients of different ages (F=3.613, p<0.05), employment status (F=9.306, p<0.001), residential location (t=−3.376, p<0.01), monthly per-person household income (F=6.308, p<0.01), comorbid chronic diseases (F=3.067, p<0.05) and logMAR (of the better eye), (F=4.079, p<0.05), as shown in Table 1.
Relationships Between Diabetes Distress and Related Outcomes
The results of the correlation analysis showed that self-management (r=−0.215, p<0.01), family support (r=−0.422, p<0.001) and social support (r=−0.410, p<0.001) were significantly associated with diabetic distress, as shown in Table 3.
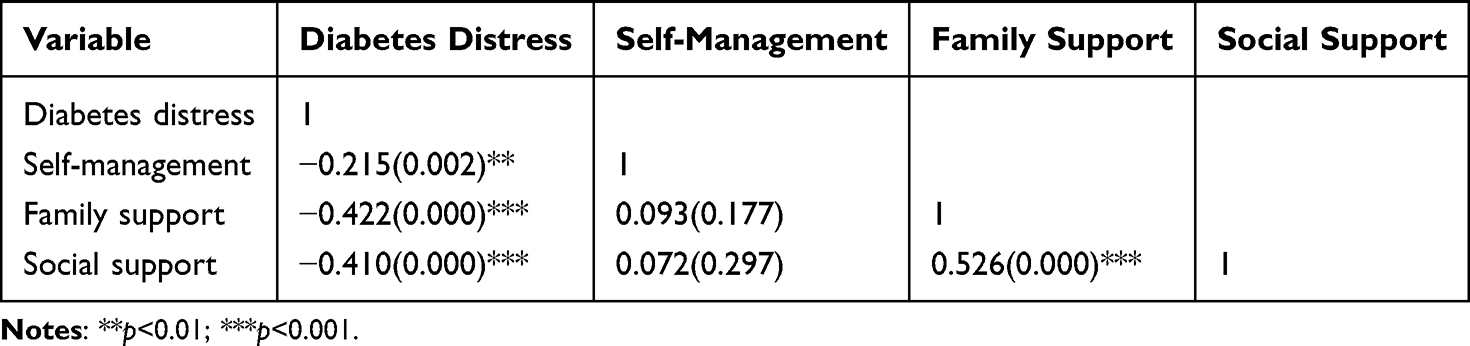 |
Table 3 Relationships Between Diabetes Distress and Related Outcomes(N=210) |
Multiple Linear Regression of Diabetes Distress in DR Surgery Patients
Multiple linear regression models (αin = 0.05, αout = 0.10) were constructed with DD as the dependent variable and 9 variables identified as statistically significant in the univariate and correlation analyses were the independent variables. The results of regression analysis showed that the DD regression model for DR surgery patients was significant (F= 16.359, p<0.001) and that residential location (t=2.989 p<0.01), employment status, self-management (t=−3.001, p<0.01), family support (t=−3.662, p<0.001), and social support (t=−3.162, p< 0.01) were significant factors influencing DD. Family support was the factor with the strongest influence (β = −0.25), followed by social support (β = −0.219), residential location (β = 0.177), self-management (β = −0.174), and employment status; these factors explained 30.6% of the variance in DD of DR surgery patients. See Table 4 for details.
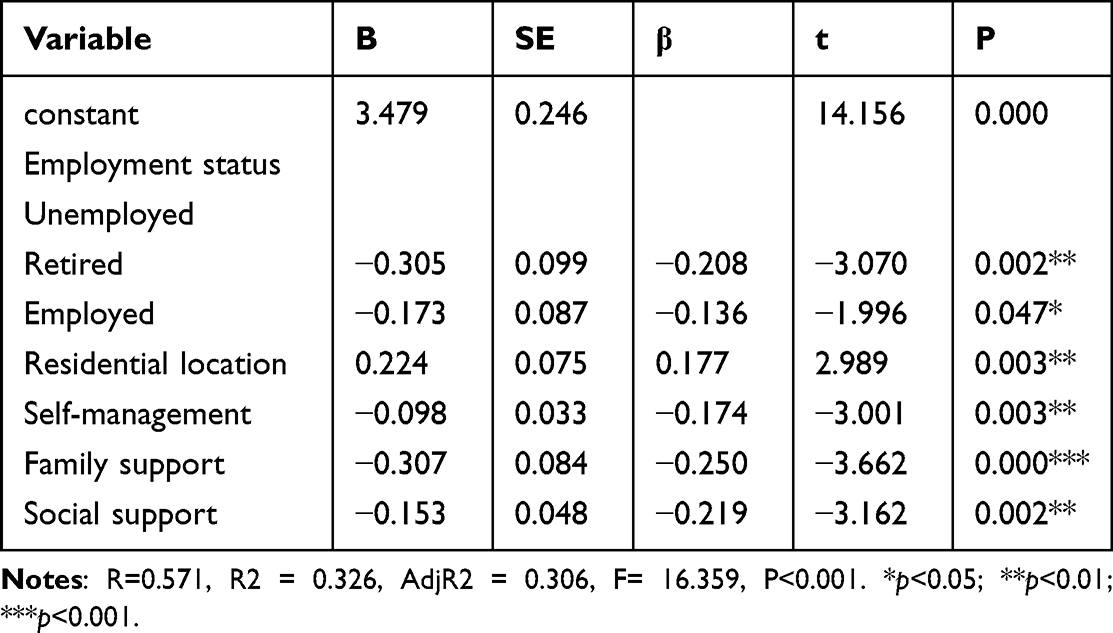 |
Table 4 Multiple Linear Regression of Diabetes Distress in DR Surgery Patients(n=210) |
Discussion
Moderate Levels of Diabetes Distress in Diabetic Retinopathy Surgery Patients
In the present study, 74.29% of DR surgery patients had DD, with a DDS score of 2.13±0.63, which indicates a moderate level of distress. In a study by Liu14 conducted in China, the prevalence of DD in 86 patients undergoing DR surgery was 65%, which is lower than that in the present findings. In addition, the prevalence of DD in this study was higher than that in diabetic patients without complications. Among diabetic patients, the prevalence rates of DD according to the same tool (DDS) were 51.3% in the USA, 39% in Canada, and 29.4% in Vietnam,35–37 differences may be related to vision limitations and the surgical treatment of DR patients. Vitrectomy is a large surgical procedure in ophthalmology. Most patients undergoing vitrectomy are in the proliferative phase. The disease prognosis is uncertain. DR patients undergoing surgery suffer from both visual impairment and diabetes mellitus, coupled with an uncertain prognosis for surgery. As a result, they may experience greater social and emotional strain. Meanwhile, Zhang15 showed that DR surgery patients have strong emotional responses both before and after surgery, such as pre-surgery fear and worry, regret and self-blame, shadows and daunt, and post-surgery uncertainty about the disease, all of which exacerbate their psychological distress. In conclusion, DD is a serious behavioural-psychological condition and should receive attention from health care professionals, especially in patients undergoing surgery for DR.
Factors Influencing Diabetic Distress in Diabetic Retinopathy Surgery Patients
Residential Location
The results of the present study showed that patients living in rural areas had higher DD levels than those living in urban areas, which is consistent with the findings of Kamrul-Hasan.23 The reason may be related to the uneven distribution of medical resources. Compared with rural areas, urban areas have more advanced medical equipment and more abundant medical resources. In addition, some studies have pointed out21 that the psychological state of diabetic patients is related to socioeconomic status. Urban areas are relatively economically developed, and individuals in these areas have relatively high average per-person incomes, which may reduce the level of distress in DR patients. Therefore, the results suggest that medical professionals should pay more attention to DR surgery patients from rural areas.
Employment Status
The results of the study showed that unemployed patients undergoing DR surgery had the highest levels of DD, followed by employed and retired patients. This may be related to economic and social pressures. The course of DR is long, and the condition often recurs. Patients need to receive a combination of treatment modalities. Treatment requires tremendous energy and financial resources, which imposes heavy care and financial burdens on patients and their families.15 In addition, most of the study participants were young or middle-aged. The social roles of DR patients in this age group are more complex, as they are both sons and daughters and parents. Their multiple roles impose a heavy caregiving burden. Multiple pressures exacerbate the DD levels of employed and unemployed DR patients. Therefore, health care professionals should pay attention to the psychological state of DR patients, especially those who are unemployed, in clinical practice and provide them with timely psychological counselling if distress is observed.
Self-Management
The results of the study showed that DD levels in DR surgery patients were negatively correlated with self-management ability. This indicates that patients with better self-management ability have lower levels of DD, consistent with Hu’s20 findings. Self-management, as an important and modifiable factor in the care process, is of critical importance to patients’ health outcomes.38 Man39 suggested that perceived barriers to diabetes self-management are closely related to the occurrence and severity of DR. In addition, poor self-management behaviours lead to psychological distress, which in turn reduces patients’ willingness and motivation to engage in health management. Ultimately, a vicious cycle of poor self-management behaviours, increased distress, and poor quality of life occurs.40 Therefore, in clinical practice, health care professionals should pay attention to improving patients’ self-management ability, such as providing educational interventions with message framing41 to provide patients with health-related information and support, thus promoting patient behaviour changes, enabling them to maintain healthy behaviours, thereby improving their psychological and physiological health.
Family Support
The results of the study showed that DD levels in DR surgery patients were negatively correlated with family support. A meta-analysis that included 23 studies indicated that family-based interventions can increase family support and self-efficacy and reduce the level of DD in diabetic patients,42 consistent with the results of this study. Compared with diabetic patients, DR patients are more likely to rely partially or completely on family for support in their daily lives due to varying degrees of vision loss and limitations of self-care ability. Family members can provide instrumental support, such as helping with insulin injections, preparing healthy meals, or reminding patients to take their medications, as well as providing social or emotional support, which can help them cope with the disease. Beneficial family involvement can improve the physical and mental health of diabetic patients, enhance their self-management ability and improve their glycaemic control.43 Therefore, health care professionals should pay attention to patients’ family support, improve family health education, help solve problems regarding family management, and promote good family function.
Social Support
The results of the study showed that DD levels in DR surgery patients were negatively correlated with social support. The results of an observational study suggested that perceived social support is more important than visual acuity for predicting mental health in DR patients.44 Positive social support plays a protective role in mental health. It can increase the level of adaptation and promote positive coping with the disease in DR patients. In contrast, negative social support, such as lack of concern for patients by health care professionals and blaming of patients by family members, can cause DD, which ultimately leads to a decrease in patients’ autonomy and motivation for disease management.45 Therefore, health care professionals, as an important source of social support, need to help patients face and manage the disease. For example, online support groups should be set up to promote patients’ communication with each other to provide peer support and alleviate their negative emotions. At the same time, government departments should advocate all aspects of society to actively integrate into maintaining the health of DR patients and advocate them to actively play their roles so that DR patients can be respected, understood and concerned.
Other Factors
In the univariate and correlation analyses, we identified 9 factors affecting the occurrence of DD in DR patients. However, the results of stepwise multiple linear regression showed that only residential location, employment status, self-management, family support and social support were independent risk factors for the occurrence of DD in DR patients after excluding the effects of confounding factors. One reason for this discrepancy may be the small sample size for some of the factors. Additionally, the confounding variables in the multiple linear regression analysis may have masked the effects of age, monthly per-person household income, comorbid chronic diseases and VA.
DR patients have varying degrees of visual impairment, and the relationship between VA and mental health (eg, anxiety, depression) is debated.46,47 The results of multivariate analysis in this study showed that vision was not an independent risk factor for DD. This may be related to the fact that family support and social support partially mediated the relationship between VA and DD, consistent with the findings of Hernández-Moreno.44 However, the correlation between VA and mental health needs to be further explored in the further.
Limitations
The study has several limitations. First, this study had a cross-sectional design and participants were recruited from only 2 hospitals in the same country. Therefore, the results should be interpreted with caution. Future longitudinal, large-sample, multi-country, multi-centre studies are needed to explore the DD in DR surgery patients before surgery and DD in DR surgery patients at 1 month, 3 months, 6 months and 1 year after surgery, to draw dynamic trajectory. Thereby elucidating the causality and targeting the timing and measures of core interventions. Second, the regression model predicted 30.6% DD which means there are other factors influencing DD in DR surgery patient that were not captured in this study. Therefore, other factors that may influence DD in DR surgery patient, such as psychological or physiological factors, need to be included in future studies.
Conclusion
The results of this study showed that DR surgery patients exhibited moderate levels of distress. Living in rural areas, being unemployed, having poor self-management ability, having low family support, and having insufficient social support are risk factors for increased DD in DR surgery patients. Regarding clinical applications, health care professionals should develop targeted health education programs and interventions based on these factors, especially after the patients are discharged from the hospital. The aim is to improve patients’ self-management ability, family support and social support to help patients actively cope with the disease, thereby reducing DD and improving their health-related quality of life. Meanwhile, in developing technology applications for DD in DR patients, technicians can refer to the factors related to DD to develop application boards to better realise the patient-centred concept and reduce the level of DD in DR patients.
Abbreviations
DR, Diabetic retinopathy; DD, Diabetes distress; HbA1c, Glycosylated haemoglobin A1c; VA, Visual acuity; DDS, Diabetes Distress Scale.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding authors on reasonable request.
Ethics Approval and Informed Consent
The study clung to the tenets of the Declaration of Helsinki. This study was granted by the Ethic Committee of Eye Hospital of Wenzhou Medical University (No, 2022-045-K-30-01) and Hennan Provincial People’ Hospital (No, HNEEC-2023(33)). Informed consent was provided and obtained from all participants before the study commenced.
Acknowledgments
We would like to thank all the patients who participated in this study and the experts who helped us in the data analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, writing, revising or critically reviewing the article; have agreed on the journal to which the article has been submitted; gave final approval of the version to be published; and agree to take responsibility and be accountable for the contents of the article.
Funding
This study was supported by General Research Project of Zhejiang Provincial Education Department (Y202250278), Wenzhou Basic Scientific Research Project (Y20210496) and Nursing Specialization Subjects of The Eye Hospital of Wenzhou Medical University (YNHL1202001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Leasher JL, Bourne RRA, Flaxman SR, et al. Global estimates on the number of people blind or visually impaired by diabetic retinopathy, a meta-analysis from 1990 to 2010. Diabetes Care. 2016;39(9):1643–1649. doi:10.2337/dc15-2171
2. Sabanayagam C, Banu R, Chee ML, et al. Incidence and progression of diabetic retinopathy, a systematic review. Lancet Diabetes Endocrinol. 2019;7(2):140–149. doi:10.1016/S2213-8587(18)30128-1
3. Berrocal MH, Acaba-Berrocal L. Early pars plana vitrectomy for proliferative diabetic retinopathy, update and review of current literature. Curr Opin Ophthalmol. 2021;32(3):203–208. doi:10.1097/ICU.0000000000000760
4. Assi L, Chamseddine F, Ibrahim P, et al. A global assessment of eye health and quality of life, a systematic review of systematic reviews. JAMA Ophthalmol. 2021;139(5):526–541. doi:10.1001/jamaophthalmol.2021.0146
5. Fenwick EK, Cheng GHL, Man REK, et al. Inter-relationship between visual symptoms, activity limitation and psychological functioning in patients with diabetic retinopathy. Br J Ophthalmol. 2018;102(7):948–953. doi:10.1136/bjophthalmol-2017-310915
6. Fisher L, Glasgow RE, Mullan JT, Skaff MM, Polonsky WH. Development of a brief diabetes distress screening instrument. Annals of Family Med. 2008;6(3):246–252. doi:10.1370/afm.842
7. Fisher L, Polonsky WH, Hessler D. Addressing diabetes distress in clinical care, a practical guide. Diabetic Med. 2019;36(7):803–812. doi:10.1111/dme.13967
8. Zhou H, Zhu J, Liu L, et al. Diabetes-related distress and its associated factors among patients with type 2 diabetes mellitus in China. Psychiatry Res. 2017;252:45–50. doi:10.1016/j.psychres.2017.02.049
9. Fisher L, Mullan JT, Arean P, Glasgow RE, Hessler D, Masharani U. Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care. 2010;33(1):23–28. doi:10.2337/dc09-1238
10. Khan A, Choudhary P. Investigating the association between diabetes distress and self-management behaviors. J Diabetes Sci Tech. 2018;12(6):1116–1124. doi:10.1177/1932296818789721
11. Perrin NE, Davies MJ, Robertson N, Snoek FJ, Khunti K. The prevalence of diabetes-specific emotional distress in people with Type 2 diabetes, a systematic review and meta-analysis. Diabetic Med. 2017;34(11):1508–1520. doi:10.1111/dme.13448
12. Nicolucci A, Kovacs Burns K, Holt RIG, et al. Diabetes attitudes, wishes and needs second study (DAWN2™), cross-national benchmarking of diabetes-related psychosocial outcomes for people with diabetes. Diabetic Med. 2013;30(7):767–777. doi:10.1111/dme.12245
13. Care D. 5. Lifestyle management, standards of medical care in diabetes-2019. Diabetes Care. 2019;42(Suppl 1):S46–S60. doi:10.2337/dc19-S005
14. Liu Y, Gao J, Yang X. Analysis on psychology status of patients with diabetic retinopathy during preoperative period and its influencing factors. Chin J Dias Contr Prevent. 2018;22(7):717–720.
15. Zhang M, Zhang C, Chen C, et al. The experience of diabetic retinopathy patients during hospital-to-home full-cycle care, A qualitative study. BMC Nurs. 2023;22(1):58. doi:10.1186/s12912-023-01206-y
16. Roddy MK, Nelson LA, Spieker AJ, Greevy RA, Mayberry LS. Family involvement and diabetes distress across dyads for adults with type 2 diabetes. Patient Educ Couns. 2023;112:107719. doi:10.1016/j.pec.2023.107719
17. Jingjing Y, Haipeng W, Xiaomin H, Qi L, Qiang S. Association between family support and self-management behavior among patients with type 2 diabetes mellitus in China. Chin J Dias Contr Prevent. 2019;23(5):573–577.
18. Polonsky WH, Fisher L, Earles J, et al. Assessing psychosocial distress in diabetes, development of the diabetes distress scale. Diabetes Care. 2005;28(3):626–631. doi:10.2337/diacare.28.3.626
19. Batais MA, Alfraiji AF, Alyahya AA, et al. Assessing the prevalence of diabetes distress and determining its psychosocial predictors among Saudi adults with type 2 diabetes, a cross-sectional study. Frontiers in Psychology. 2021;12:759454. doi:10.3389/fpsyg.2021.759454
20. Hu Y, Li L, Zhang J. Diabetes distress in young adults with type 2 diabetes, a cross-sectional survey in China. J Diabetes Res. 2020;2020:4814378. doi:10.1155/2020/4814378
21. Qiu S, Sun H, Liu Y, et al. Prevalence and correlates of psychological distress among diabetes mellitus adults in the Jilin province in China, a cross-sectional study. PeerJ. 2017;5:e2869. doi:10.7717/peerj.2869
22. Thi DK, Xuan BN, Le Duc C, et al. Unmet needs for social support and diabetes-related distress among people living with type 2 diabetes in Thai Binh, Vietnam, a cross-sectional study. BMC Public Health. 2021;21(1):1532. doi:10.1186/s12889-021-11562-6
23. Kamrul-Hasan ABM, Hannan MA, Asaduzzaman M, et al. Prevalence and predictors of diabetes distress among adults with type 2 diabetes mellitus, a facility-based cross-sectional study of Bangladesh. BMC Endocr Disord. 2022;22(1):28. doi:10.1186/s12902-022-00938-3
24. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The STRENGTHENING THE REPORTING of Observational Studies in Epidemiology (STROBE) statement, guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
25. Ophthalmology Society of Chinese Medical Association. Clinical guidelines for diagnosis and treatment of diabetic retinopathy in China. Chin J Ophthalmol. 2014;(11):851–865.
26. Faul F, Erdfelder E, Buchner A, Lang A-G. Statistical power analyses using G*Power 3.1, tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
27. Ostrovsky M, Rosenblatt A, Hollander N, Habot-Wilner Z. Online support group for patients with inflammatory eye disease, characterisation of members and assessment of benefits. Clin Exp Ophthalmol. 2023;51(7):704–713. doi:10.1111/ceo.14287
28. Fujikawa A, Mohamed YH, Kinoshita H, et al. Visual outcomes and prognostic factors in open-globe injuries. BMC Ophthalmol. 2018;18(1):138. doi:10.1186/s12886-018-0804-4
29. Yang Q, Liu X. Reliability and validity of the diabetes distress scale. J Nurs. 2010;17(12):8–10.
30. Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure, results from 7 studies and a revised scale. Diabetes Care. 2000;23(7):943–950. doi:10.2337/diacare.23.7.943
31. Wan Q, Shang S, Lai X, Jie P. Study on the reliability and validity of summary of diabetes self-care activities for type 2 diabetes patients. Chin J Pract Nurs. 2008;24(07):26–27.
32. Smilkstein G, Ashworth C, Montano D. Validity and reliability of the family APGAR as a test of family function. J Family Pract. 1982;15(2):303–311.
33. Lu F, Gu Y. Family APGAR questionnaire and its clinical application. Hos Manage Forum. 1995;2:56–59.
34. Xiao S. Theoretical basis and research applications of the Social Support Rating Scale (SSRS). J Clin Psychiatry. 1994;02:98–100.
35. Fisher L, Glasgow RE, Strycker LA. The relationship between diabetes distress and clinical depression with glycemic control among patients with type 2 diabetes. Diabetes Care. 2010;33(5):1034–1036. doi:10.2337/dc09-2175
36. Huynh G, Tran TT, Tht D, et al. Diabetes-related distress among people with type 2 diabetes in Ho Chi Minh City, Vietnam, prevalence and associated factors. Diabetes Metab Syndr Obes. 2021;14:683–690. doi:10.2147/DMSO.S297315
37. Wong EM, Afshar R, Qian H, Zhang M, Elliott TG, Tang TS. Diabetes distress, depression and glycemic control in a Canadian-based specialty care setting. Can J Diabetes. 2017;41(4):362–365. doi:10.1016/j.jcjd.2016.11.006
38. RuiTong G. An Intervention Programme Based on the Message Framing Effect on Self-Management Behaviour in Patients Living with Type 2 Diabetes. Jilin University; 2022.
39. Man REK, Fenwick EK, Gan ATL, et al. Association between perceived barriers to diabetes self-management and diabetic retinopathy in Asian patients with type 2 diabetes. JAMA Ophthalmol. 2017;135(12):1387–1393. doi:10.1001/jamaophthalmol.2017.4888
40. Strandberg RB, Graue M, Wentzel-Larsen T, Peyrot M, Rokne B. Relationships of diabetes-specific emotional distress, depression, anxiety, and overall well-being with HbA1c in adult persons with type 1 diabetes. J Psychosomatic Res. 2014;77(3):174–179. doi:10.1016/j.jpsychores.2014.06.015
41. Gao R, Guo H, Liu Y, et al. The effects of message framing on self-management behavior among people with type 2 diabetes, A randomized controlled trial. Int J Nurs Stud. 2023;142:104491. doi:10.1016/j.ijnurstu.2023.104491
42. Zhang H, Zhang Q, Luo D, et al. The effect of family-based intervention for adults with diabetes on HbA1c and other health-related outcomes, Systematic review and meta-analysis. J Clin Nurs. 2022;31(11–12):1488–1501. doi:10.1111/jocn.16082
43. Leukel PJ, Kollin SR, Lewis BR, Lee AA. The influence of emotion regulation and family involvement on diabetes distress among adults with type 2 diabetes. J Behav Med. 2022;45(6):904–913. doi:10.1007/s10865-022-00351-0
44. Hernández-Moreno L, Senra H, Moreno N, Macedo AF. Is perceived social support more important than visual acuity for clinical depression and anxiety in patients with age-related macular degeneration and diabetic retinopathy? Clin Rehabil. 2021;35(9):1341–1347. doi:10.1177/0269215521997991
45. Yufeng C, Shennan Y, Qingqing L. Advances in the study of diabetes-related psychological distress. Chin J Nurs. 2015;50(3):354–359.
46. Yang Y, Wu J, Jiang J, Dong J. Associations of self-reported vision impairment with depression symptoms among middle-aged and older Chinese. Aging Clin Exp Res. 2022;34(9):2117–2128. doi:10.1007/s40520-022-02158-0
47. Seong HJ, Kim J, Yook TM, Lee D, Chung EJ. Association between vision impairment and depression, a 9-year, longitudinal, nationwide, population-based cohort study in South Korea. Br J Ophthalmol. 2023;107(9):1390–1394. doi:10.1136/bjophthalmol-2021-320970
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Chinese Community Home-Based Aging Institution Elders’ Self-Management of Chronic Non-Communicable Diseases and Its Interrelationships with Social Support, E-Health Literacy, and Self Efficacy: A Serial Multiple Mediation Model
Wu Y, Wen J, Wang X, Wang Q, Wang W, Wang X, Xie J, Cong L
Patient Preference and Adherence 2023, 17:1311-1321
Published Date: 25 May 2023
Comparison of Metabolic, Lifestyle and Mental Health Parameters in People with Diabetes and Relatives with and without Family Support
García-Ulloa AC, Miranda-Gil V, Díaz-Pineda M, Garnica-Carrillo MF, Serrano-Pérez NH, Tron-Gomez MS, Colorado Báez GP, Cruz Madrigal CA, Hernández-Jiménez S
Diabetes, Metabolic Syndrome and Obesity 2024, 17:239-245
Published Date: 18 January 2024
Non-Linear Relationship Between Fasting C-Peptide and Retinopathy in Patients with Type 2 Diabetes Mellitus - A Retrospective Study
Ma J, Han C, Lv Y, Cai H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1035-1045
Published Date: 7 April 2025
Network Analysis of Depressive Symptoms, Social Support, and Diabetes Distress Among Patients with Type 2 Diabetes: A Cross-Sectional Study
Chen H, Dong X, Chen S, Chen X, Lu X, He J, Ji W, Hou C, Bai D, Gao J
Patient Preference and Adherence 2025, 19:1951-1964
Published Date: 8 July 2025
Factors Associated with Adherence to the Atrial Fibrillation Better Care (ABC) Pathway Among Rural Patients with Atrial Fibrillation: A Path Analysis Based on the Integrated Theory of Health Behavior Change (ITHBC)
Huang J, Chen J, Ye Q, Cai X, Feng Y, Lai X, Diao X, Dai Q, Zhang X, Li K
Patient Preference and Adherence 2026, 20:556835
Published Date: 20 January 2026