Back to Journals » Patient Preference and Adherence » Volume 17
Chinese Community Home-Based Aging Institution Elders’ Self-Management of Chronic Non-Communicable Diseases and Its Interrelationships with Social Support, E-Health Literacy, and Self Efficacy: A Serial Multiple Mediation Model
Authors Wu Y, Wen J, Wang X, Wang Q, Wang W, Wang X, Xie J, Cong L ![]()
Received 11 March 2023
Accepted for publication 15 May 2023
Published 25 May 2023 Volume 2023:17 Pages 1311—1321
DOI https://doi.org/10.2147/PPA.S412125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ying Wu,1 Jing Wen,1 Xiaohui Wang,1 Qingyao Wang,1 Wen Wang,2 Xiangjia Wang,1 Jiang Xie,1 Li Cong1
1School of Medicine, Hunan Normal University, Changsha, 410013, People’s Republic of China; 2Teaching and Research Section of Clinical Nursing, Xiangya Hospital of Central South University, Changsha, 41008, People’s Republic of China
Correspondence: Li Cong, School of Medicine, Hunan Normal University, Changsha, People’s Republic of China, Tel +86-0731-88912446, Fax +86-0731-88912478, Email [email protected]
Background: The Chinese population is aging, and chronic non-communicable diseases (NCDs) prevalence is correspondingly increasing, along with associated disability and healthcare costs. Although self-management has been associated with social support and is a recognized priority, its mediating variables have not been studied in detail, particularly among old people with chronic diseases.
Purpose: To examine the mediating role of e-health literacy and general self-efficacy in the relationship between social support and self-management of chronic NCDs in Chinese community home-based aging institution residents.
Patients and Methods: A random sample of 289 community home-based aging institution elders (≥ 60 years) with chronic NCDs in China was recruited. Questionnaire data were recorded on self-reported socio-demographics, self-management, social support, e-health literacy, and general self-efficacy. Pearson’s correlation analysis identified the relationship between these factors and self-management. Serial multiple mediation model was used to test the hypothesized relationships.
Results: The self-management mean (±SD) score was 29.39 ± 9.60, and the level of self-management was medium. Social support (r = 0.283; P < 0.001), e-health literacy (r = 0.566; P < 0.001), and general self-efficacy (r = 0.477; P < 0.001) were positively associated with self-management. Furthermore, social support indirectly influenced self-management through three pathways: independent mediation of e-health literacy (effect = 0.234, P < 0.001), independent mediation of general self-efficacy (effect = 0.515, P < 0.001), and chain mediation of e-health literacy and general self-efficacy (effect = 0.075, P < 0.001).
Conclusion: In Chinese community home-based aging institution elders, the relationship between self-reported self-management and social support is positively affected by the independent mediating effect of e-health literacy and general self-efficacy and the serial mediating effect of e-health literacy and general self-efficacy. Targeted self-management programs for elders with chronic NCDs have theoretical support, which could improve the health status and quality of life in this population.
Keywords: chronic non-communicable disease, self-management, social support, e-health literacy, general self-efficacy, serial multiple mediation analysis
Introduction
Chronic non-communicable diseases (NCDs) including cardiovascular and cerebrovascular diseases, cancer, chronic respiratory diseases, and type 2 diabetes form the largest percentage of the Chinese burden of morbidity and mortality.1 The available estimates suggest that by 2025, chronic NCDs will impose a disease burden of nearly $7 trillion on low- and middle-income countries.2 The healthcare costs for chronic diseases account for 70% of China’s total public expenditure on diseases.3 Currently, there are approximately 300 million Chinese people with one or more NCDs, and this number is rising with the aging of the population.4 There are 180 million old people aged 60 and above in China who suffer from chronic diseases, with more than three-fourths of the old people population suffering from the coexistence of multiple chronic NCDs.5 Importantly, as China is an aging society, the population base of patients with chronic NCDs is large, the average life expectancy is longer, and the public health resources are more limited.6 Moreover, these patients bring greater financial and emotional burdens to their family caregivers.7 All of this poses a huge challenge to the public health and primary healthcare systems of China.8 A current top priority in China’s public health industry is actively promoting healthy aging and strengthening the prevention and management of old people with chronic NCDs.
China’s Elderly Care Development Plan recommends creating a multi-level old-age service system based on home care, assisted by community care, and supported by professional nursing homes.9 The plan focuses on the need to develop and create community home-based aging institutions, completely use community resources, meet the needs of old people, and improve their health status.9 Community home-based aging institutions use the family as the core, depending on the community, and utilize community resources to provide places for free entertainment, learning, and exercise, as well as paid food supply, rehabilitation guidance, and simple care for old people in the community.10 Old people voluntarily choose to come to community home-based aging institutions for activities, learning, and socializing, and still go home to rest. This method of old people care meets the traditional Chinese desire of old people to care for at home and also considers the requirements of old people for healthy and high-quality care.11 However, community home-based aging institutions only provide relatively simple services for the old people, the daily care, medication, and disease management of old people with chronic NCDs still mostly depend on old people and their family caregivers.12
According to China’s Long-Term Plan for Chronic Disease Prevention and Treatment (2017–2025), the basis for the prevention and treatment of chronic diseases should be to improve patients’ self-management ability.13 Self-management refers to maintaining and improving health and monitoring and managing diseases based on the patient’s behavior.14 Self-management of chronic NCDs has been widely studied and applied in many countries with good results and has become a research hotspot in the field of chronic disease treatment.15,16 Although the introduction of the self-management model in China was relatively short, considerable research and development has been performed.17 The self-management of chronic NCDs can efficiently promote rehabilitation, control progress, and prevent the complications of chronic diseases.18 Self-management is a sustainable health behavior that can decrease the effect of diseases on the social functioning, emotions, and interpersonal relationships of the patients, particularly the burden on family caregivers.19,20 Therefore, to reduce the burden on caregivers, improve the efficiency of long-term family care, lessen the burden on social nursing homes, and achieve a healthy China, it is important to encourage self-management in old people with chronic NCDs.21
As an available external resource, social support is a realistic, practical, and important way to improve patient self-management and lessen the burden on primary family caregivers. Social support refers to the care, respect, and assistance that individuals feel from their close partners or social network.22 People with chronic NCDs learn how to take care of themselves and stay healthy from others who also have chronic diseases.23 Furthermore, receiving support from doctors can positively affect self-management in patients with chronic NCDs.24 However, some old people with chronic NCDs depend on social support and have a reduced sense of responsibility for self-management.25 Therefore, no consensus on the effect of social support on patient self-management in old people with chronic NCDs and its underlying mechanisms has been achieved yet.
With the ongoing transition toward a more digital world, emerging digital technologies and smart health devices have transformed the way old people manage their health conditions.26 The combination of chronic disease self-management and the 5G internet has become unavoidable.27 However, old people with chronic NCDs still lack the opportunity and ability to get health information from the internet28 and are unable to make good use of smart health devices to manage diseases.29 A systematic review indicated low e-health literacy of old Chinese, and it can be affected by a number of influencing factors at the individual, interpersonal, and social/community levels.30 E-health literacy is defined as the ability to find, understand, and assess health information from electronic resources and use it to resolve one’s health problems.31 An improvement in e-health literacy leads to an increase in patients’ knowledge and confidence in disease management and encourages them to take positive health management measures.32 Informational and emotional support can contribute to e-health literacy in old people with chronic NCDs.33 Therefore, e-health literacy may be an essential mediating variable between social support and self-management.
Lorig designed the Chronic Diseases Self-Management Program using general self-efficacy theory as the theoretical framework.14 General self-efficacy refers to an individual’s overall confidence in dealing with the difficulties of various environments and facing new things.34 An important requirement for self-management and a key factor for people to change their behaviors and maintain healthy functioning is a high sense of general self-efficacy.35 In patients with multiple chronic conditions, self-efficacy in performing self-management mediated the relationships between sociodemographic characteristics and adherence.36 Peer support can encourage general self-efficacy,37 and social support indirectly affects self-management behaviors through general self-efficacy.38 Furthermore, e-health literacy indirectly affects health promotion behaviors via general self-efficacy.39 Therefore, general self-efficacy may be an essential mediating variable in the effect of social support on self-management in old people with chronic NCDs and may also indirectly affect self-management via e-health literacy.
Many existing studies have shown relationships between self-management, social support, e-health literacy, and general self-efficacy or relationships among the three. We have demonstrated a significant correlation between social support and self-management; however, no path relationship was found through the structural equation model between social support and self-management.40 Meanwhile, few studies have considered the relationship between social support, e-health literacy, general self-efficacy, and self-management in old people with chronic NCDs. Based on the literature review and our previous study findings, we created a model to test the following hypotheses: Hypothesis 1: social support positively directly affects self-management, e-health literacy, and general self-efficacy; Hypothesis 2: e-health literacy mediates the indirect relationship between self-management and social support; Hypothesis 3: general self-efficacy mediates the indirect relationship between self-management and social support; Hypothesis 4: e-health literacy and general self-efficacy serially mediate the relationship between social support and self-management.
In conclusion, this study aims to construct a series multiple mediation model to explore the potential mechanisms between self-management, social support, e-health literacy, and general self-efficacy in old people with chronic NCDs. This may provide a theoretical basis for clinical intervention and improve the health status and quality of life of old people with chronic NCDs.
Materials and Methods
Study Design and Participants
From July 2021 to November 2021, a cross-sectional study was conducted. We selected old people with chronic NCDs from four community home-based aging institutions in four random districts of Changsha City (Yuelu District, Yuhua District, Kaifu District, and Furong District). Old people with at least one chronic NCD diagnosed by a professional physician, who were aged 60 or older, and who participated voluntarily are included. Old people with mental or communication impairments that make it difficult to understand the questionnaire are excluded. All investigators (three graduate nursing students and two undergraduate nursing students) were uniformly trained before the study to ensure that each investigator used a unified guiding language. A one-to-one survey was conducted in an independent quiet room of each community home-based aging institution. Before the survey, the researchers explained the purpose, significance, and precautions of the survey to old people with chronic CNDs. During the survey, for some old people with difficulty in reading or writing, the investigators explained each item one by one or helped them complete the questionnaire by taking their oral responses. All eligible patients included in the study provided a signed consent form before participation. All paper-based questionnaires completed by patients were collected on the spot and checked for missing items to ensure data integrity. In total, 300 questionnaires were distributed, of which 289 valid questionnaires were returned; the response rate was 96.33%. The study was approved by the Ethics Committee of Hunan Normal University (No: 2021291) and complied with the Declaration of Helsinki.
Instruments
General Information Questionnaire
Our research group designed the general questionnaire to obtain the sociodemographic characteristics and health-related information, including gender, age, education status, living situation, main caregiver, family history of the disease, years of chronic NCDs, number of chronic NCDs, frequency of daily dosing, and whether they use smart health devices, of old people with chronic NCDs.
Chronic Disease Self-Management Study Measures
The chronic disease self-management study measures created by Lorig at the Stanford University Patient Education Research Center in 199914 were sinicized by Chinese scholar Fu Dongbo in 2003 to evaluate patients’ self-management behavior.41 The scale assessed the self-management behavior of old people with chronic NCDs from the following three dimensions: The exercise dimension has six entries, each of which asks how much time the patient has spent walking, swimming, or doing other aerobic exercises in the past week. The communication dimension has three items, wherein each item describes the patient’s habits when seeing a doctor (eg, making a list of questions to ask in advance). The cognitive symptom management dimension has six items, each reflecting the patient’s attitude toward pain or other uncomfortable symptoms (eg, trying to ignore the discomfort). Each item was scored on a 5-point Likert scale, with an overall score ranging from 0 to 75 (low level: 0–25, medium level: 25–50, and high level: 50–75), with higher scores indicating better self-management skills. The Chinese version had high sensitivity and validity in old people with chronic NCDs. Cronbach’s α for internal consistency was 0.79–0.85.41
Social Support Rate Scale
The social support rate scale was proposed by the Chinese researcher Xiao in 1995 and contains 10 entries in three dimensions.42 The objective support dimension comprises three items (eg, “Who will comfort and care for you in emergencies?”). The subjective support dimension includes four items (eg, “Which family member can you rely on for support and care?”). The supported utilization dimension has three items (eg, “Do you turn to others for help when you are in trouble?”). The total score ranges from 10 to 66, with a higher score indicating higher levels of social support. The scale had good internal consistency (Cronbach’s α = 0.89) and test–retest reliability (Cronbach’s α = 0.92).38
E-Health Literacy Scale
The e-health literacy scale was developed by Norman and Skinner in 2006 and comprises three dimensions with eight entries.31 In 2013, Peking University sinicized the e-health literacy scale and verified its reliability and validity in the Chinese population.43 The application dimension was measured using five items (eg, I know how to obtain health resource information from the internet). The discrimination dimension was measured using two items (eg, the ability to evaluate good and bad information on network health resources). The decision dimension included whether people were confident that they could use online information to make decisions, with each response ranging from 1 (ie, totally disagree) to 5 (ie, totally agree). The total scores ranged from 8 to 40, with higher scores reflecting higher e-health literacy. The Chinese version showed good reliability among old people in the community. Cronbach’s α for internal consistency was 0.98.44
General Self‑efficacy Scale
Schwarzer compiled the general self-efficacy scale in 1994.34 The Chinese version of the general self-efficacy scale was translated and revised by Wang Caikang in 2001.45 This scale consists of 10 items (eg, “When things get tough, I always find a way to solve them”.), with responses ranging from 1 (ie, totally incorrect) to 4 (ie, correct). The total score of the scale was the sum of the 10 items divided by 10, with a higher score representing greater general self-efficacy. The reliability and validity have already been demonstrated in 26 countries.46 The Chinese version also had high sensitivity and validity; Cronbach’s α for internal consistency was 0.85.47
Statistical Analysis
The data were analyzed using SPSS 22.0 (IBM Corporation, Armonk, NY, USA) and double-entered independently to avoid input errors. The numerical variables were presented as means and standard deviations, whereas the categorical variables were presented as percentages and numbers. Descriptive, univariable, and multi-factor regression analyses were used. Pearson correlation was used to test for the relationship between continuous variables. Based on the significant relationships and hypothesis model, we used Hayes’s48 PROCESS macro (Model 6) to conduct mediation analyses using social support as the independent variable, e-health literacy, and general self-efficacy as the mediating variables, and self-management as the dependent variable; statistically significant variables in the univariate analysis were included in the mediating model as the covariates. We used a bias-corrected non-parametric percentage Bootstrap test, and after 5000 repeated samples, a 95% confidence interval was calculated to test each indirect effect. If the 95% confidence interval did not include 0, it indicated that the indirect effect was significant. P < 0.05 was considered statistically significant.
Results
Participant Characteristics
Table 1 presents the self-reported sociodemographic characteristics of old people with chronic NCDs. Among the 289 participants, there were 108 (37.4%) females and 181 (62.6%) males. The mean age was 68.61 ± 5.36 (range: 60–86) years. Moreover, 176 (60.9%) old people had hypertension and 106 (38.2%) had diabetes; 246 old people needed to take medication more than twice a day. Moreover, the majority (79.2%) of old people with chronic NCDs had been ill for more than 5 years, and 78.2% had multiple chronic diseases. A univariate analysis was conducted to evaluate the effects of sociodemographic characteristics on the self-reported self-management of old people with chronic NCDs in community home-based aging institutions. The use of smart health devices and age were significantly associated with self-management in old people with chronic NCDs.
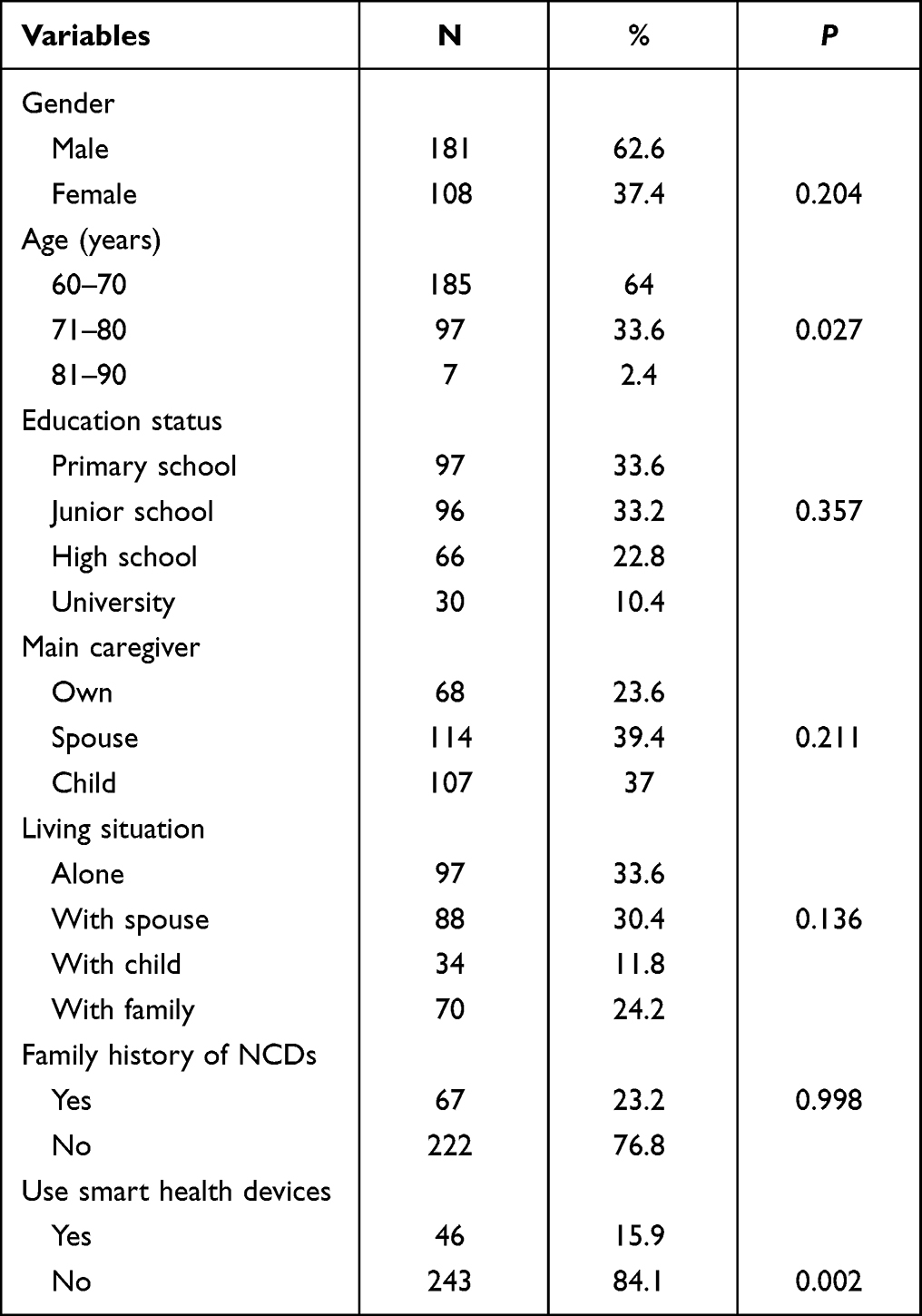 |
Table 1 Demographic Characteristics of the Study Participants (n = 289) |
Bivariate Analyses
Table 2 shows the descriptive statistics and correlation analysis of self-reported research variables of old people with chronic NCDs. Self-management was significantly positively related to e-health literacy (r = 0.566; P < 0.01), general self-efficacy (r = 0.477; P < 0.01), and social support (r = 0.283; P < 0.01) in old people with chronic NCDs. E-health literacy was positively associated with general self-efficacy (r = 0.404; P < 0.01) and social support (r = 0.307; P < 0.01), and general self-efficacy was significantly positively associated with social support (r = 0.499; P < 0.01).
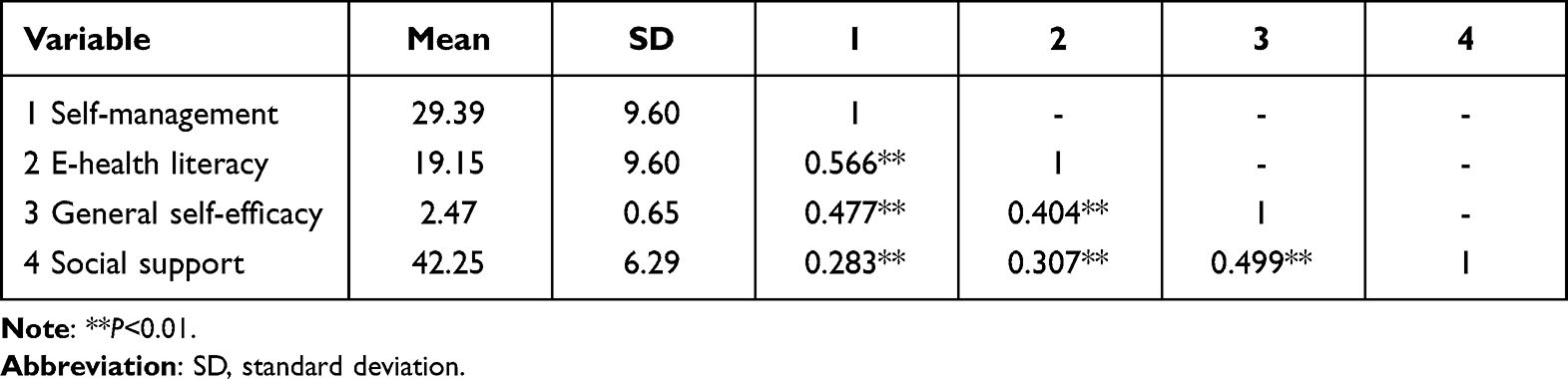 |
Table 2 Mean Scores and Pearson Correlation Coefficients of Main Variables (n = 289) |
Serial Mediating Effect Tests for E-Health Literacy and General Self-Efficacy
The mediating role of e-health literacy and general self-efficacy between self-management and social support in chronically ill old people was analyzed, controlling for sex and the use of smart healthdevices. The regression analysis revealed that social support was a direct positive predictor of e-health literacy (β = 0.223, P < 0.001) and general self-efficacy (β = 0.423, P < 0.001); e-health literacy was a direct positive predictor of general self-efficacy (β = 0.184, P < 0.001); e-health literacy (β = 0.376, P < 0.001) and general self-efficacy (β = 0.448, P < 0.001) were significantly positively related to self-management. The results of the regression analysis are shown in Table 3. Figure 1 shows the path coefficients of the mediation model.
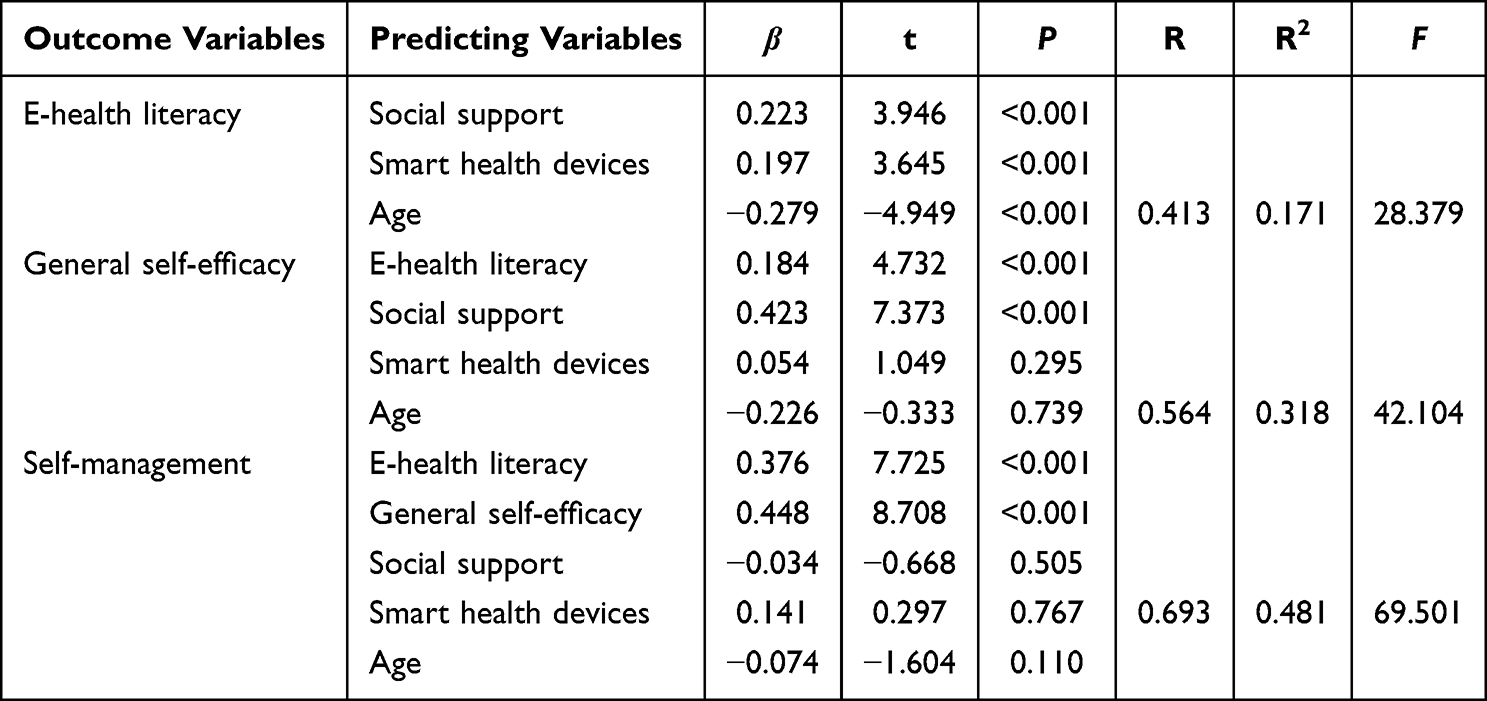 |
Table 3 Multiple Linear Regression Analysis for e-Health Literacy, General Self-Efficacy, and Self-Management (n = 289) |
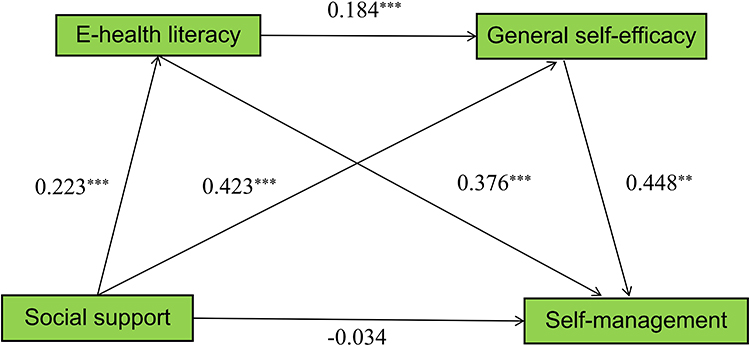 |
Figure 1 Serial mediation of e-health literacy and general self-efficacy on the relationship between social support and self-management. The coefficients shown are standardized path coefficients, ***P < 0.001. |
Table 4 shows the indirect effects. The results show that e-health literacy and general self-efficacy have a significant mediated effect between social support and self-management, with a totally mediated effect value of 0.824. The total mediated effect consists of three indirect effect paths, which accounted for 28.4%, 62.5%, and 9.1% of the total mediated effect, respectively.
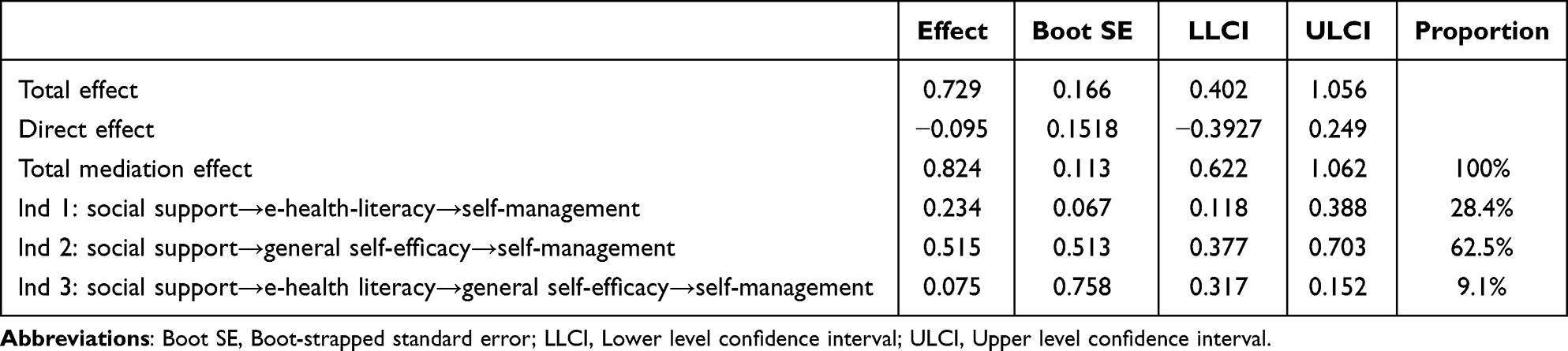 |
Table 4 Indirect Effects of e-Health Literacy and General Self-Efficacy (n = 289) |
Discussion
Our study findings revealed that old people with chronic NCDs have lower levels of self-management and e-health literacy, moderate levels of general self-efficacy, and high levels of social support, which are consistent with the findings of previous studies.25,32,38,49 We also assessed the effect and mechanism of social support on old people with chronic NCDs. The study findings revealed that social support directly positively affects e-health literacy and general self-efficacy but negatively affects self-management; therefore, Hypothesis 1 was not fully supported. In our study, old people with chronic NCDs received higher social support, but it had no positive promoting effect on the self-management of the old people in the community home-based aging institutions. This may be because too much social support may encourage the patient’s sense of dependence, such as the weakening of self-management responsibility in the aspects of diet, medication, and emotional management.25 The declining self-management ability of old people leads to an increase in the burden on caregivers. Furthermore, the negative emotions associated with long-term care, the medical costs associated with the treatment of the disease, and the complications caused by improper management all place a great burden on family caregivers, creating a vicious cycle.50 Therefore, community home-based aging institutions can provide more opportunities for old people with chronic NCDs to participate in society and learn and use various electronic media such as health platforms, WeChat official account, TikTok, community radio to popularize knowledge about diseases, reasonable diet, mental health, physical exercise, medication matters, emergency disposal and other knowledge, to improve the e-health literacy and disease self-management ability of old people.
As shown by the serial multiple mediation model, e-health literacy indirectly mediates the relationship between social support and self-management in old people, supporting Hypothesis 2. The e-health literacy level of Chinese old people with chronic NCDs is lower than the international level.51 Improving the level of e-health literacy is beneficial for old people with chronic diseases to correctly seek, evaluate, and apply online health information, thereby actively participating in disease self-management.52 Hence, community home-based aging institutions should conduct customized internet health information education and guidance activities for old people with chronic NCDs. Social media platforms and regulatory authorities should be responsible for establishing an account credit system, alerting about false information prompts, providing information protection for old people, compressing the space for false information dissemination, and cleaning the platform environment. Family members should encourage old people with chronic diseases to build confidence, help them access multiple information channels, guide them to identify false information, inform them about official health websites or WeChat official accounts, and improve their ability to identify online health information. Only 15.9% of old people in our study used smart health devices. In the future, the design of intelligent health products for old people should have simple operation functions, high efficiency, and strong practicability, which will increase the usage rate of smart health devices and also improve patients’ confidence in using the devices, thereby promoting the application of intelligent health products in the self-management of chronic NCDs in the old people.
General self-efficacy mediated the relationship between social support and self-management, thus supporting Hypothesis 3, which is also consistent with the finding of a previous study.38 General self-efficacy is an essential belief factor in self-management, that is, the stronger the sense of general self-efficacy, the stronger the confidence in disease management.53 Serial multiple mediation models have demonstrated that e-health literacy and general self-efficacy serially mediate the relationship between social support and self-management, thus supporting Hypothesis 4, which has similarities and differences with the findings of previous studies.39,54 To fully encourage patients’ behavioral motivation and achieve self-empowerment, the use of e-health literacy to increase patients’ self-management ability should also pay more attention to patients’ general self-efficacy. Moreover, medical workers and caregivers should pay attention to the psychological state of patients, provide targeted counseling when necessary, promote the correct management of diseases, strengthen patients’ confidence in self-management, and ensure the continuity of self-management. The combination of internet information technology and community home-based aging institutions can lead to more intelligent and efficient old people care services, improve the level of community pension security, and reduce the burden of social public guidance.55 It can also simultaneously promote the self-management of patients, lessen the burden of care of family members, and improve the quality of life and long-term prognosis of old people with chronic diseases.
Nonetheless, our study has some limitations. First, the subjects of the study were only recruited from Changsha City. In the future, the sample scope should be expanded to more comprehensively analyze the self-management status of old people with chronic NCDs in community home-based aging institutions of different levels and regions. Second, this study was based on a self-reported questionnaire survey of old people. When answering the questionnaire, the respondents might have estimated their responses or incorrectly judged their abilities, thus affecting the accuracy of the information to some extent. Therefore, future research could be combined with other assessment, qualitative, observational, and experimental studies to obtain a deeper information of self-management and e-health literacy in old people with chronic NCDs.
Conclusion
Our study identified some factors associated with the self-management of old people with chronic NCDs in China, clarified the multiple chain-mediated effects of e-health literacy and general self-efficacy in the relationship between self-management and social support, and provided a reference for the intervention programs aimed at improving self-management of old people. Our findings provide a new perspective and theoretical basis for reducing the burden on family caregivers and national old people care, and improving the long-term quality of life and rehabilitation effect of old people with chronic NCDs.
Data Sharing Statement
The original contributions presented in this study are included in the article, which can be further queried by the corresponding authors.
Ethics Approval and Participate
All experimental protocols in this study were approved by the Ethics Committee of Hunan Normal University (No: 2021291) and complied with the Declaration of Helsinki. Informed consent was obtained from all old people.
Acknowledgments
Acknowledgments to all the old people who participated in the study and to the community home-based aging institutions.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that the study was conducted without any business or financial relationship that could be interpreted as potential conflicts of interest.
References
1. GBD 2019 Diseases and Injuries Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/s0140-6736(18)32279-7
2. Chowdhury SR, Chandra Das D, Sunna TC, Beyene J, Hossain A. Global and regional prevalence of multimorbidity in the adult population in community settings: a systematic review and meta-analysis. EClinicalMedicine. 2023;57:101860. doi:10.1016/j.eclinm.2023.101860
3. Wang LM, Chen ZH, Zhang M, et al. 中国老年人群慢性病患病状况和疾病负担研究 [Study of the prevalence and disease burden of chronic disease in the elderly in China]. Chin J Epidemiol. 2019;40(3):277–283. Chinese. doi:10.3760/cma.j.issn.0254-6450.2019.03.005
4. Chen X, Giles J, Yao Y, et al. The path to healthy ageing in China: a Peking University-Lancet commission. Lancet. 2022;400(10367):1967–2006. doi:10.1016/S0140-6736(22)01546-X
5. Jiang Q, Feng Q. Editorial: aging and health in China. Front Public Health. 2022;10:998769. doi:10.3389/fpubh.2022.998769
6. Shilian H, Jing W, Cui C, Xinchun W. Analysis of epidemiological trends in chronic diseases of Chinese residents. Aging Med. 2020;3(4):226–233. doi:10.1002/agm2.12134
7. Ivziku D, Clari M, Piredda M, et al. Anxiety, depression and quality of life in chronic obstructive pulmonary disease patients and caregivers: an actor-partner interdependence model analysis. Qual Life Res. 2019;28(2):461–472. doi:10.1007/s11136-018-2024-z
8. Bao J, Zhou L, Liu G, et al. Current state of care for the elderly in China in the context of an aging population. Biosci Trends. 2022;16(2):107–118. doi:10.5582/bst.2022.01068
9. Ministry of health of the people’s republic china. National plan for the development of elderly care and the elderly care service system during the 14th five year plan period. Available from: http://www.gov.cn/zhengce/content/2022-02/21/content_5674844.htm.
10. Jiang H, Liu Z. Community home elderly care services, multidimensional health and social participation of chronically ill elderly-Empirical analysis based on propensity score matching and multiple mediation analysis. Front Public Health. 2023;11:1121909. doi:10.3389/fpubh.2023.1121909
11. Zhang L, Zeng Y, Wang L, Fang Y. Urban-Rural Differences in Long-Term Care Service Status and Needs Among Home-Based Elderly People in China. Int J Environ Res Public Health. 2020;17(5):1701. doi:10.3390/ijerph17051701
12. Yue Z, Xiang N, Li H, Liu E. The evolution trend of availability of China’s community-based care services and its impact on the cognitive function of elderly people: 2008–2018. Int J Equity Health. 2021;20(1):203. doi:10.1186/s12939-021-01544-w
13. Kong LZ. China’s medium-to-long term plan for the prevention and treatment of chronic diseases (2017–2025) under the healthy China initiative. Chronic Dis Transl Med. 2017;3(3):135–137. doi:10.1016/j.cdtm.2017.06.004
14. Lorig KR, Sobel DS, Stewart AL, et al. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: a randomized trial. Med Care. 1999;37(1):5–14. doi:10.1097/00005650-199901000-00003
15. Billany RE, Thopte A, Adenwalla SF, March DS, Burton JO, Graham-Brown MPM. Associations of health literacy with self-management behaviours and health outcomes in chronic kidney disease: a systematic review. J Nephrol. 2023. doi:10.1007/s40620-022-01537-0
16. Magny-Normilus C, Hassan S, Sanders J, Longhurst C, Lee CS, Jurgens CY. Implications for self-management among African Caribbean adults with noncommunicable diseases and mental health disorders: a systematic review. Biomedicines. 2022;10(11):2735. doi:10.3390/biomedicines10112735
17. Yu S, Wan R, Bai L, et al. Transformation of chronic disease management: before and after the COVID-19 outbreak. Front Public Health. 2023;11:1074364. doi:10.3389/fpubh.2023.1074364
18. Corbett T, Cummings A, Calman L, et al. Self-management in older people living with cancer and multi-morbidity: a systematic review and synthesis of qualitative studies. Psychooncology. 2020;29(10):1452–1463. doi:10.1002/pon.5453
19. Reed RL, Roeger L, Howard S, et al. A self-management support program for older Australians with multiple chronic conditions: a randomised controlled trial. Med J Aust. 2018;208(2):69–74. doi:10.5694/mja17.00127
20. He X, Wang Y, Feng C, et al. Preferring self-management behavior of patients with chronic kidney disease. Front Public Health. 2022;10:973488. doi:10.3389/fpubh.2022.973488
21. Zhu XL, Luo JS, Zhang XC, Zhai Y, Wu J. China’s efforts on management, surveillance, and research of noncommunicable diseases: NCD scorecard project. Ann Glob Health. 2017;83(3–4):489–500. doi:10.1016/j.aogh.2017.10.025
22. Behrendt D, Spieker S, Sumngern C, Wendschuh V. Integrating social support into interventions among the elderly in nursing homes: a scoping review. BMJ Open. 2023;13(4):e071962. doi:10.1136/bmjopen-2023-071962
23. Thompson DM, Booth L, Moore D, Mathers J. Peer support for people with chronic conditions: a systematic review of reviews. BMC Health Serv Res. 2022;22(1):427. doi:10.1186/s12913-022-07816-7
24. Prat Vigué G, Cano Prieto I, Del Río Sáez R, Vilanova Masana R, Simó Algado S. Training peer support workers in mental health care: a mixed methods study in Central Catalonia. Front Psychiatry. 2022;13:791724. doi:10.3389/fpsyt.2022.791724
25. Yangyang M, Min L, Jiantao L. Correlation analysis of self⁃management and social support for hypertensive patients in rural areas of Shanxi. Chin Nurs Res. 2022;36(21):3845–3849.
26. Parker S, Prince A, Thomas L, Song H, Milosevic D, Harris MF; IMPACT Study Group. Electronic, mobile and telehealth tools for vulnerable patients with chronic disease: a systematic review and realist synthesis. BMJ Open. 2018;8(8):e019192. doi:10.1136/bmjopen-2017-019192
27. Taylor ML, Thomas EE, Vitangcol K, et al. Digital health experiences reported in chronic disease management: an umbrella review of qualitative studies. J Telemed Telecare. 2022;28(10):705–717. PMID: 36346938. doi:10.1177/1357633X221119620
28. Ding X, Wen Y, Tian Z, et al. Effect of e-health intervention on disease management in patients with chronic heart failure: a meta-analysis. Front Cardiovasc Med. 2023;9:1053765. doi:10.3389/fcvm.2022.1053765
29. Cilli E, Ranieri J, Guerra F, Ferri C, Di Giacomo D. Naturalizing digital and quality of life in chronic diseases: systematic review to research perspective into technological advancing and personalized medicine. Digit Health. 2022;8:20552076221144857. doi:10.1177/20552076221144857
30. Shi Y, Ma D, Zhang J, Chen B. In the digital age: a systematic literature review of the e-health literacy and influencing factors among Chinese older adults. Z Gesundh Wiss. 2023;31(5):679–687. doi:10.1007/s10389-021-01604
31. Norman CD, Skinner HA. eHealth literacy: essential skills for consumer health in a networked world. J Med Internet Res. 2006;8(2):e9. doi:10.2196/jmir.8.2.e9
32. Madrigal L, Escoffery C. Electronic health behaviors among us adults with chronic disease: cross-sectional survey. J Med Internet Res. 2019;21(3):e11240. doi:10.2196/1124
33. Zhao YC, Zhao M, Song S. Online health information seeking among patients with chronic conditions: integrating the health belief model and social support theory. J Med Internet Res. 2022;24(11):e42447. doi:10.2196/42447
34. Schwarzerr A. Optimistic self-beliefs assessment of general perceived self-efficacy in thirteen cultures. World Psychol. 1997;3(12):177–190.
35. Huang X, Xu N, Wang Y, Sun Y, Guo A. The effects of motivational interviewing on hypertension management: a systematic review and meta-analysis. Patient Educ Couns. 2023;112:107760. doi:10.1016/j.pec.2023.107760
36. Xie Z, Liu K, Or C, Chen J, Yan M, Wang H. An examination of the socio-demographic correlates of patient adherence to self-management behaviors and the mediating roles of health attitudes and self-efficacy among patients with coexisting type 2 diabetes and hypertension. BMC Public Health. 2020;20(1):1227. doi:10.1186/s12889-020-09274-4
37. Nair P, Walters K, Aw S, et al. Self-management of depression and anxiety amongst frail older adults in the United Kingdom: a qualitative study. PLoS One. 2022;17(12):e0264603. doi:10.1371/journal.pone.0264603
38. Kong LN, Zhu WF, Li L, Lei QS, Wang T, Li YL. Self-management behaviors in adults with chronic hepatitis B: a structural equation model. Int J Nurs Stud. 2021;116:103382. doi:10.1016/j.ijnurstu.2019.06.013
39. Wang Y, Song Y, Zhu Y, Ji H, Wang A. Association of eHealth literacy with health promotion behaviors of community-dwelling older people: the Chain mediating role of self-efficacy and self-care ability. Int J Environ Res Public Health. 2022;19(10):6092. doi:10.3390/ijerph19106092
40. Wu Y, Wen J, Wang X, et al. Associations between e-health literacy and chronic disease self-management in older Chinese patients with chronic non-communicable diseases: a mediation analysis. BMC Public Health. 2022;22(1):2226. doi:10.1186/s12889-022-14695-4
41. Dongbo F, Ding Y, Mcgowan P, Fu H. Qualitative evaluation of chronic disease self-management program (CDSMP) in Shanghai. Patient Educ Couns. 2006;61(3):389–396. doi:10.1016/j.pec.2005.05.002
42. Sy X. The theoretical basis and application of social support scale. J Clin. 1994;4(02):98–100. Chinese.
43. Shua G, Yu S. Adaptation and evaluation of Chinese version of eHEALS and its usage among senior high school students. Chin J Health Educ. 2013;29(2):106–123. Chinese . doi:10.16168/j.cnki.issn.1002-9982.2013.02.019
44. Zhang X, Zhang R, Lu X. Exploring the effects of patient activation in online health communities on patient compliance. Telemed J E Health. 2020;26(11):1373–1382. doi:10.1089/tmj.2019.0258
45. Wang CK, Hu, ZF, Liu, Y. 一般自我效能感量表的信度和效度研究 [Evidences for reliability and validity of the Chinese version of general self-efficacy scale]. Chin Journal of Applied Psychology. 2001;01:37–40. Chinese.
46. Villegas Barahona G, González García N, Sánchez-García AB, Sánchez Barba M, Galindo-Villardón MP. Seven methods to determine the dimensionality of tests: application to the general self-efficacy scale in twenty-six countries. Psicothema. 2018;30(4):442–448. doi:10.7334/psicothema2018.113
47. Zhang X, Zhan Y, Liu J, et al. Chinese translation and psychometric testing of the cardiac self-efficacy scale in patients with coronary heart disease in mainland China. Health Qual Life Outcomes. 2018;16(1):43. doi:10.1186/s12955-018-0872-4
48. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. Guilford publications; 2017.
49. Chen J, Tian Y, Yin M, et al. Relationship between self-efficacy and adherence to self-management and medication among patients with chronic diseases in China: a multicentre cross-sectional study. J Psychosom Res. 2023;164:111105. doi:10.1016/j.jpsychores.2022.111105
50. Phetsitong R, Vapattanawong P, Mayston R, Prince M, Chua KC. In caring for older people in low- and middle-income countries, do older caregivers have a high level of care burden and psychological morbidity compared to younger caregivers? Int J Environ Res Public Health. 2022;19(24):16405. doi:10.3390/ijerph192416405
51. Jung S, Son Y, Choi E. E-health literacy in older adults: an evolutionary concept analysis. BMC Med Inform Decis Mak. 2022;22(1):28. doi:10.1186/s12911-022-01761-5
52. Labrique A, Agarwal S, Tamrat T, Mehl G. WHO digital health guidelines: a milestone for global health. NPJ Digit Med. 2020;3:120. doi:10.1038/s41746-020-00330-2
53. Korenhof SA, Rouwet EV, Elstgeest LEM, et al. Evaluation of an intervention to promote self-management regarding cardiovascular disease: the social engagement framework for addressing the chronic-disease-challenge (SEFAC). Int J Environ Res Public Health. 2022;19(20):13145. doi:10.3390/ijerph192013145
54. Nagao-Sato S, Akamatsu R, Karasawa M, et al. Associations between patterns of participation in community activities and social support, self-efficacy, self-rated health among community-dwelling older adults. J Psychiatr Res. 2023;157:82–87. doi:10.1016/j.jpsychires.2022.11.023
55. Meng Q, Hong Z, Li Z, et al. Opportunities and challenges for Chinese elderly care industry in smart environment based on occupants’ needs and preferences. Front Psychol. 2020;11:1029. doi:10.3389/fpsyg.2020.01029
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
How Does Social Support and Emotional Intelligence Enhance Life Satisfaction Among Adolescents? A Mediational Analysis Study
Azpiazu L, Antonio-Agirre I, Fernández-Zabala A, Escalante N
Psychology Research and Behavior Management 2023, 16:2341-2351
Published Date: 27 June 2023
Diabetes Distress Among Patients Undergoing Surgery for Diabetic Retinopathy and Associated Factors: A Cross-Sectional Survey
Zhang M, Zhang X, Yang Y, Weng Y, Chen X, Chen Y, Shi Y
Psychology Research and Behavior Management 2024, 17:1451-1461
Published Date: 2 April 2024
Factors Associated with Adherence to the Atrial Fibrillation Better Care (ABC) Pathway Among Rural Patients with Atrial Fibrillation: A Path Analysis Based on the Integrated Theory of Health Behavior Change (ITHBC)
Huang J, Chen J, Ye Q, Cai X, Feng Y, Lai X, Diao X, Dai Q, Zhang X, Li K
Patient Preference and Adherence 2026, 20:556835
Published Date: 20 January 2026
The Mediating Roles of Self-Efficacy, Resilience, and Social Support in the Relationship Between Clinical Factors and Adaptation to Chronic Disease
Laza R, Lustrea A, Lazureanu EV, Oancea CI, Dehelean L, Poplicean EI, Bătrîn AD, Romosan RS, Romosan AM
Journal of Multidisciplinary Healthcare 2026, 19:576275
Published Date: 20 February 2026