Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 18
Facilitators and Barriers to Implementation of WHO HEARTS Strategy for Hypertension and Diabetes Among People Living with HIV in Eastern Uganda: A COM-B Analysis
Authors Katuramu R ![]() , Li Y
, Li Y ![]() , Namugaya M, Muwanga SN, Kibuuka R
, Namugaya M, Muwanga SN, Kibuuka R ![]() , Mawejje F, Obakiro SB
, Mawejje F, Obakiro SB ![]() , Kanyike AM
, Kanyike AM ![]() , Li Z
, Li Z
Received 22 March 2026
Accepted for publication 25 June 2026
Published 9 July 2026 Volume 2026:18 611133
DOI https://doi.org/10.2147/HIV.S611133
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Richard Katuramu,1,2 Yueyun Li,3 Maureen Namugaya,4 Steven Nsereko Muwanga,4 Ronald Kibuuka,4 Francis Mawejje,4 Samuel Baker Obakiro,4,5 Andrew Marvin Kanyike,4,6 Zhihui Li3
1Department of Internal Medicine, Faculty of Health Sciences, Busitema University, Mbale, Uganda; 2Department of Internal Medicine, College of Health Sciences, Makerere University, Kampala, Uganda; 3Vanke School of Public Health, Tsinghua University, Beijing, People’s Republic of China; 4Department of Pharmacology and Therapeutics, Faculty of Health Sciences, Busitema University, Mbale, Uganda; 5Natural Products Research and Innovation Centre, Faculty of Health Sciences, Busitema University, Mbale, Uganda; 6Department of Clinical and Biomedical Sciences, University of Exeter, Exeter, UK
Correspondence: Richard Katuramu, Department of Internal Medicine, Faculty of Health Sciences, Busitema University, Mbale, Uganda, Email [email protected]
Background: The World Health Organization’s HEARTS technical package aims to improve the management of hypertension (HTN) and diabetes (DM) in primary health care at the population level. This study explored the barriers and facilitators of implementing this strategy among People Living with HIV (PLHIV) with Hypertension and/or Diabetes in Eastern Uganda.
Methods: This was a descriptive qualitative study that used a semi-structured interview guide. We conducted in-depth interviews with healthcare workers (HCWs). We adopted the Capability, Opportunity, and Motivation (COM-B) model of behavior change to guide both study design and data analysis.
Results: Twelve HCWs with a mean age of 36 years were interviewed. Within the capability domain, inadequate training on HTN and DM management was identified as a barrier, while existing skills in blood pressure measurement and management served as a facilitator. Social opportunity barriers included the absence of community-based support groups for integrated HIV-NCD co-management and the inability to track outcomes for patients on concurrent ART and NCD medications. Physical opportunity barriers encompassed frequent stock-outs of essential antihypertensive and antidiabetic medications, shortages of glucometer test strips and blood pressure machines, and understaffing at HIV clinics. Conversely, opportunity facilitators included collaboration with implementing partners for material support, adherence to standard treatment guidelines, and availability of lifestyle counselling sessions. Within the motivation domain, patient-centred follow-up and strong therapeutic rapport between healthcare workers and patients were identified as facilitators, with no motivational barriers reported.
Conclusion: Implementation of the WHO HEARTS strategy in HIV clinics is influenced by some of the COM-B domains. Building on these findings, a stakeholder-informed foundation can support the design of contextually appropriate, behaviorally targeted interventions to improve outcomes in similar settings.
Keywords: HIV, hypertension, diabetes, HEARTS, WHO, implementation
Background
Chronic non-communicable diseases (NCDs) are a major global health concern. They cause over 17 million premature deaths annually.1,2 Cardiovascular diseases (CVDs) are the leading cause, primarily due to hypertension (HTN) and diabetes mellitus (DM).2 People living with HIV (PLHIV) are currently more affected by CVDs than by advanced HIV or opportunistic infections.3 PLHIV face twice the risk of CVD morbidity and mortality compared to uninfected counterparts.4 This is concerning in countries like Uganda, where HIV prevalence stands at 5.8%, with 54,000 new infections per year.5 There is also a high, rapidly increasing prevalence of HTN (26.4%) and DM (1.4%) in Uganda.6
The World Health Organization’s (WHO) HEARTS program provides a robust framework for managing HTN and DM in primary healthcare settings. This program is built upon six evidence-based, pragmatic components: Healthy lifestyle counselling, Evidence-based protocols, Access to essential medicines and technology, Risk-based CVD management, Team-based care, and Systems for monitoring.2 Given the shared risk factors for HTN and DM, the HEARTS approach provides a suitable framework to improve outcomes among PLHIV with HTN and/or DM.7 Although the HEARTS program has demonstrated a significant impact on improving HTN and DM outcomes in the general population,8,9 its effectiveness within the HIV clinical setting remains underexplored. It is not clear whether those results translate to routine HIV clinical care, where patient complexity with co-morbid ART use and multiple co-morbidities differ from general outpatient settings. This study is exploring the WHO HEARTS strategy implementation within public-sector regional referral HIV clinics among PHLIV with HTN and /DM comorbidity.
One study from a large HIV clinic in central Uganda reported improved HTN control among people living with HIV following an adapted HEARTS strategy;10 however, the study was conducted in a specialized HIV care centre staffed by specialist HIV physicians—resources that are typically absent in public-sector health facilities and also evaluated only HTN rather than integrated HTN/DM care.
There is a need to understand the barriers and facilitators of this approach in typical public-sector HIV clinics using a combined HTN/DM model. Several patient-, provider-, and system-level barriers have been identified as impeding optimal integration of HTN and DM services into HIV care.10 Building on these findings, we conducted a formative assessment to identify the facilitators and barriers to implementing the WHO HEARTS strategy at the HIV clinic of Mbale Regional Referral Hospital (MRRH). We recently reported a high prevalence of HTN (37.5%) and DM (12%) among PLHIV at this clinic.11,12 Such evidence is essential to guide the development of a contextually appropriate strategy.
We used the Capability, Opportunity and Motivation for Behavioral Change (COM-B) model to examine the facilitators and barriers to implementing the WHO HEARTS strategy in an HIV ART Clinic. The COM-B model was chosen to understand the capabilities, opportunities, and motivations that influence HCWs’ behavior in adopting the strategy. Capability includes both psychological aspects (knowledge and skills) and physical aspects (resources and equipment) that enable individuals to act in specific ways. Opportunities encompass social factors (peer acceptance, social norms) and biological factors (resource availability and access to facilities) that affect behavior. Motivation covers psychological drivers, including automatic (instinctive), reflective (conscious decisions), and personal (values and beliefs) influences. According to the COM-B model, capability and opportunity shape motivation, and engaging in a behavior can also alter capability, opportunity, and motivation.13 These factors operate at multiple levels: the individual (knowledge, skills, and motivation), the interpersonal (social relationships and peer influence), and the contextual (environmental, societal, and structural factors), as shown in Figure 1 below. Analyzing these levels helps identify barriers and facilitators to behavior, providing a structured framework for designing effective interventions.14
 |
Figure 1 Illustration of how Capability, Opportunity, and Motivation (COM) influence behavior. (Adapted from Michie et al 2014). |
Methods
Study Design
We conducted a descriptive qualitative study using in-depth interviews (IDIs) in December 2024 to January 2025 involving healthcare workers (HCWs) at the HIV ART Clinic. To understand barriers and facilitators to implementing the WHO HEARTS protocol among adult PLHIV with HTN and/or DM comorbidities, we interviewed twelve HCWs. The study was reported using the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.15
Study Setting
The study was conducted at Mbale Regional Referral Hospital’s (MRRH) HIV ART Clinic, a government-funded facility that offers free services. It is located in the Eastern part of Uganda, within Mbale city. MRRH is located approximately 222 km east of Kampala in Mbale City, Eastern Uganda. MRRH is one of 16 regional referral hospitals in the Ugandan public health system and serves as the tertiary care center for a catchment area encompassing 16 districts across four sub-regions: Bugisu, Sebei, Teso, and Busoga. The estimated population within this catchment is approximately 4.5 million. The HIV ART clinic runs every Wednesday and Thursday, attending to about 200–250 patients per clinic day. The clinic is staffed by a multidisciplinary team comprising medical and clinical officers, nurses, and social workers.
Sample Size and Study Participants
We conducted in-depth interviews with 12 health care workers (nurses, counsellors, and clinicians) working in the HIV ART clinic. We included all staff who were 18 years old and had worked in the ART clinic for more than 12 months, as we anticipated that this duration would ensure sufficient experience to provide informed perspectives. We believe that this sample size attained saturation basing on the recent systematic review, which showed that a sample size of between 9 to 17 individual participants in a study can be enough to reach saturation.16
Data Collection Procedures
Data collection occurred between December 2024 and January 2025. It was conducted by a team comprising the first author, a male doctor with training in implementation science research (R.K.), a female graduate doctor (MN), and a social scientist (YL). All obtained on-the-job training in conducting qualitative interviews by the social scientist before the study began. Data were collected through face-to-face semi-structured interviews conducted in private, quiet settings within the ART clinic or other confidential spaces in the facility, ensuring participant privacy, comfort, and trust. Before each interview, participants received a full briefing on the study’s objectives, risks, and benefits, and provided both verbal and written informed consent. Research assistants were trained on the study tools and interview guides, including a piloting phase to assess question clarity, interpretation, and flow. Interviewers were specifically oriented to avoid leading questions, thereby minimising social desirability bias and encouraging candid responses. Each interview lasted approximately 35–45 minutes, was conducted in English, and audio-recorded with participants’ consent. Recordings were transcribed verbatim and stored securely to maintain confidentiality.
Data Collection Instruments
Data were collected through semi-structured face-to-face IDIs with HCWs to explore their perceived barriers and facilitators to implementing the WHO HEARTS strategy among PLHIV with HTN and/or DM. The interview questions focused on HCWs’ knowledge of the HEARTS strategy, their attitudes toward patient care informed by its components, and how these components were being integrated into the ART clinic’s patient management. These included how the care for PLHIV with HTN and DM are integrated with HIV care, any protocols or guidelines that are currently followed for managing HTN and DM in HIV patients, If they are aware of the HEARTS protocol and its components, challenges they face in managing patients with comorbid HIV, HTN, and DM, how these challenges could be addressed, are they comfortable to manage HTN or DM among PLHIV, are there tools to manage HTN/DM effectively at the clinic, What kind of motivation is needed you to ensure effective management of HIV patients with HTN/DM. The interview guides were designed based on the components of the COM-B model (Supplementary 1).
Data Analysis
Data were analysed using inductive thematic analysis, following Braun and Clarke’s six-phase framework and guided theoretically by the COM-B model.17 The process began with repeated reading of transcripts to achieve deep familiarisation with the data, attending closely to both content and context. Initial codes were then systematically generated to label conceptually significant features across the dataset. These codes were subsequently grouped into candidate subthemes by identifying recurring patterns relevant to the barriers and facilitators of implementing the WHO HEARTS strategy. Through an iterative process of review and refinement, subthemes were merged, split, or discontinued where necessary to enhance analytical rigour and ensure faithful representation of participants’ perspectives. Refined subthemes were then interrogated to produce overarching themes, which were validated against their coded extracts and assigned clear, descriptive names reflecting their meaning and scope. The resultant themes were finally organised within the COM-B framework and categorised as either facilitators—those positively influencing implementation—or barriers—those negatively influencing implementation of the HEARTS strategy.
Data Trustworthiness
Trustworthiness was reinforced through two principal strategies. First, independent dual coding was conducted, whereby RK and MN each coded all transcripts separately, then convened to compare, discuss, and resolve discrepancies, thereby strengthening the consistency and rigour of the coding framework. Second, peer debriefing was undertaken with an independent qualitative researcher (MK), who critically reviewed the codes, themes, and interpretations to provide an external analytical check and mitigate potential researcher bias. Together, these measures substantially enhanced the credibility and dependability of the study findings.
Reflexivity
Throughout the research process, the team maintained a deliberate reflexive stance, critically examining their positionality and its potential influence on data collection and interpretation. RK is a clinician practising within the study facility who participated solely in conducting interviews with healthcare workers, thereby limiting his clinical role during the research period. MN is a medical doctor engaged exclusively by the research project; although primarily research-focused, she occasionally joined the clinical team for patient reviews, a dual role that was explicitly acknowledged and managed. The team remained acutely aware that power asymmetries—inherent in both the researcher-participant relationship and the broader socio-structural context of HIV care—could shape participants’ responses and influence analytical interpretations. Accordingly, deliberate efforts were made to cultivate a respectful, open, and non-coercive environment that encouraged participants to share their experiences freely. Ongoing critical reflection on the team’s own perspectives, assumptions, and disciplinary backgrounds facilitated a more nuanced and contextually situated interpretation of the findings.
Rigor
To ensure methodological rigour, we applied Lincoln and Guba’s four trustworthiness criteria18—credibility, dependability, confirmability, and transferability—throughout all phases of the study.
Credibility was strengthened through regular reflexive team discussions that fostered consensus-building, inclusive analytical decision-making, and critical interrogation of emerging interpretations. The diverse disciplinary backgrounds of the research team enriched the analytical process, while explicit attention to researcher positionality ensured that potential biases were systematically identified and addressed during both data collection and analysis.
Dependability was enhanced through the conduct of in-depth individual interviews within a safe, confidential, and non-judgmental environment, designed to encourage candid disclosure of participants’ experiences. Open-ended questions and probing techniques were deliberately employed to avoid premature interpretive closure, allowing participants to direct the flow of discussion organically. Interviews were intentionally framed as reciprocal dialogues to build rapport, minimise power asymmetries between researcher and participant, and promote authentic engagement with the research process.
Confirmability was established through member checking, whereby the collected data were returned to participants for verification of accurate representation of their experiences and interview responses. Together, these rigorous measures substantially strengthened the credibility and trustworthiness of the study, thereby enhancing its potential transferability to similar healthcare settings.
Results
Description of the Study Participants
A total of 12 health care workers were enrolled in the study. The mean age was 36 years. The sample included an equal number of male and female participants. All HCWs approached for enrollment consented to participate (Table 1).
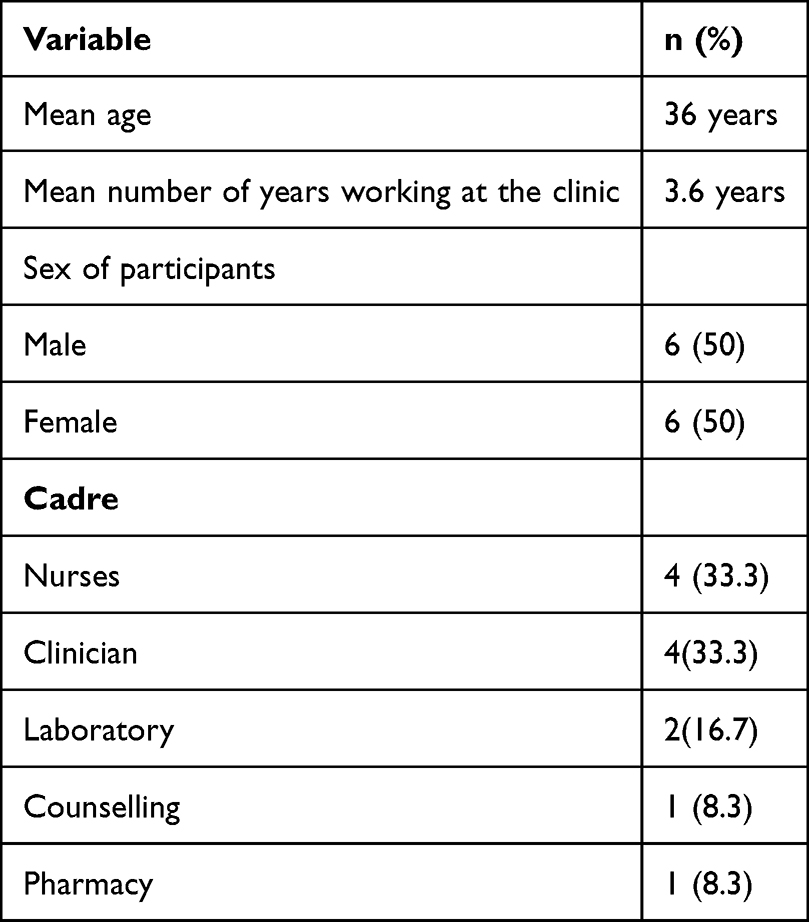 |
Table 1 The Distribution of the Health Care Workers Who Were Involved in the in-Depth Interviews to Determine the Facilitators and Barriers to the Implementation of the WHO-HEARTS Strategy Among Adult PLHIV in MRRH Eastern Uganda |
Perceived Barriers to the Implementation of the WHO HEARTS Strategy in the Management of Adult PLHIV with HTN and DM Comorbidities
In their efforts to manage HTN and DM care among PLHIV in Mbale RRH HI clinic, HCWs encountered several barriers in implementing the six components of the WHO HEARTS implementation strategy. These barriers map to the Psychological capability and the Social and Physical opportunity domains of the COM-B model. They include: lack of community-based support groups for integrated HIV-NCD care; inadequate outcome tracking for patients receiving both ART and HTN/DM medications; frequent stockouts of essential drugs that disrupt treatment continuity; shortage of blood-glucose test strips for people with DM; and limited availability of blood-pressure monitors at the clinic (Table 2).
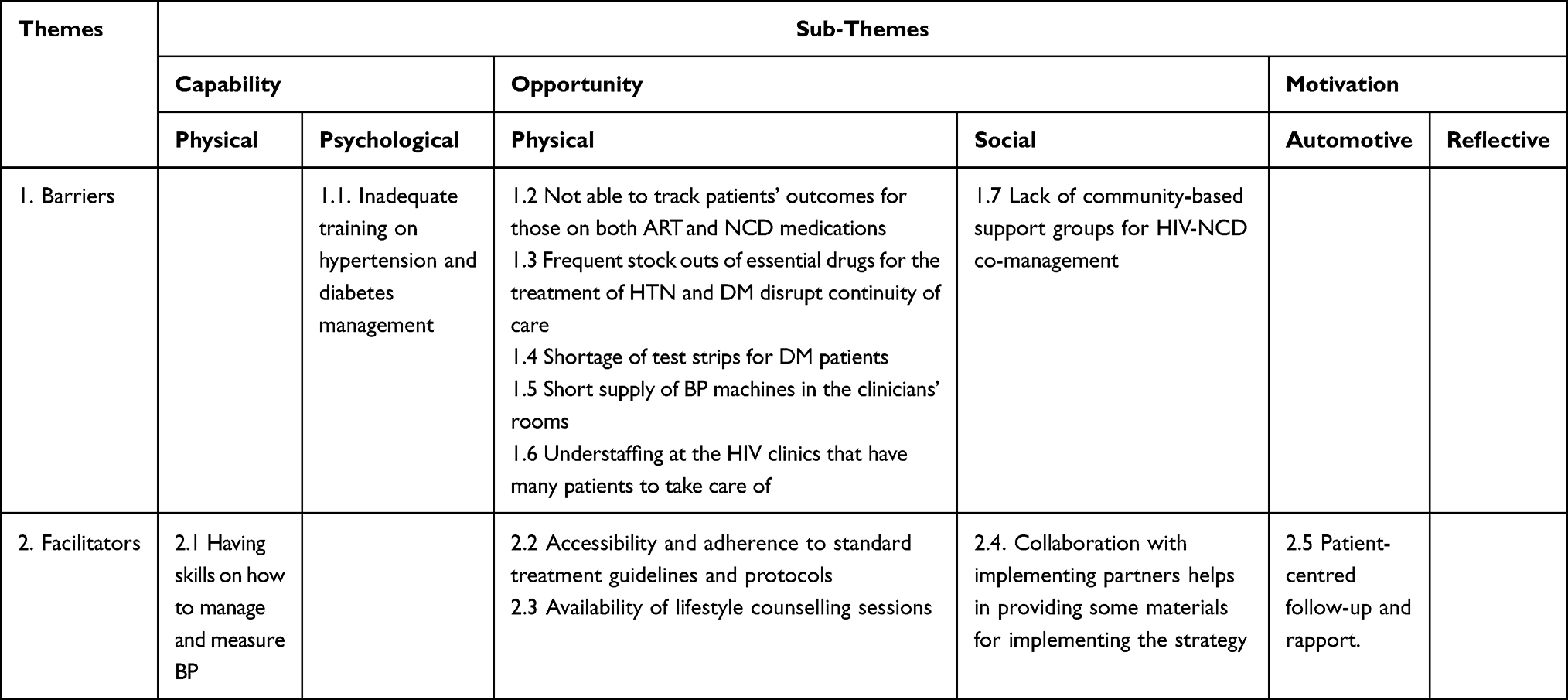 |
Table 2 Facilitators and Barriers to Implementation of the WHO HEARTS Protocol Among Adult PLHIV with HTN and DM Co-Morbidities in MRRH HIV ART Clinic as Related to the COM-B Model Domains |
Capability
In assessing the psychological capability, most HCW reported having not been trained in managing HTN and DM, and hence have knowledge gaps in managing these patients, yet they were well trained to manage HIV. Secondly, they believed that managing both diseases among the PLHIV may require special training.
As a social worker, I haven’t received any training apart from being trained by my fellow workers, like the clinicians. However, I have never attended any specific training in that regard. Female social worker. Interview-007
Have I received any training on how to care for HIV patients who have hypertension or diabetes? No. And definitely, I need it. Male enrolled nurse interview-008.
Opportunity
Under physical opportunity, although the government provides free medicines for both NCDs and HIV, the majority of HCWs reported frequent stock-outs of HTN and DM medications. This significantly undermines the quality of care delivered to patients. Most patients visit the hospital with the expectation of receiving free drugs; however, when these medicines are unavailable, many cannot afford to purchase them independently. As a result, patients miss their medication doses, leading to poor adherence and, consequently, poor treatment outcomes. This situation poses a considerable barrier to the implementation of the “essential commodities” component of the HEARTS strategy.
Amlodipine, which is the most preferred hypertensive drug, has been hard to obtain in large quantities. NMS (National Medical Stores) has been issuing small quantities, which are finished within one or two weeks. So, most of our clients have to buy them if they get money. Female P/T, Interview_004
The inconsistent supply of laboratory consumables—including glucose strips for blood glucose testing and glucometers—has contributed to a reduced willingness among HCWs to screen patients for HTN and DM during routine visits, as recommended by clinical guidelines. Consequently, a significant proportion of patients are discharged without being screened for these chronic conditions. This critical gap in routine screening represents a substantial barrier to the effective implementation of the HEARTS strategy.
It’s only the side of RBS (Random Blood Sugar) testing where we normally have stock-outs of the test strips. It can even go for a month so we cannot screen these patients. Male NO interview_005
The BP machines are there, at least we have somewhere to begin from, but for diabetes, we have limited screening kits, that is to say, the glucometers test strips that are insufficient in supply. (Male M/O interview_011)
HCWs also reported a significantly increased workload in the context of existing understaffing challenges. Previously, their role was limited to reviewing patients’ progress in HIV management, after which referrals were made to other HCWs for the management of HTN and DM. However, with the integration of care, HCWs are now required to manage both conditions concurrently, a practice that is considerably more time-intensive and places additional strain on an already overburdened workforce.
One of the main challenges is the increase in workload in treating patients’ HIV condition and HTN and or DM condition…. Yeah, this takes some time, and patients spend a lot of time at the clinic. We are a few clinicians at this clinic. (Female Medical Clinical Officer_001)
HCWs reported an inability to adequately monitor treatment outcomes among patients receiving care for NCDs. This deficiency makes it considerably difficult to track patients’ progress over time. Furthermore, data management is predominantly conducted using paper-based records, with no electronic or software-based data management systems in place. The absence of a digital data management infrastructure further compounds the challenges associated with patient follow-up and longitudinal monitoring of treatment outcomes.
…we are still struggling with bulk documentation for each patient that has to be managed, and recently there was another bigger tool that was introduced for the PLHIV, which has DM and HIV indicators (Female MCO, Interview_001)
Under social opportunity, several HCWs reported the absence of community-based support groups dedicated to educating patients about the management of DM and HTN among PLHIV. Such groups play a vital role in delivering tailored lifestyle education, reinforcing medication adherence, and facilitating the sharing of lived experiences—functions similar to those performed by existing HIV-specific support groups. However, the absence of equivalent structures for integrated NCD and HIV care renders patient education and peer experience sharing considerably more difficult, thereby limiting the social support available to this population.
Patient engagement as ‘expert clients’ would do a lot. They should be identified and trained just like those for PLHIV without comorbidities. So that they know they are teaching their fellow friends who have the same illness, they can provide more care than a random assignment of health workers. Also, these experts can help identify many others in communities seeking care. The Village Health Teams we always refer to, which were recruited into HIV service, only concentrate there, and are even less knowledgeable about NCDs. We need full-time expert client community involvement for the management of PLHIV with HTN and DM. (Male SNO, Interview_012)
Perceived Facilitators to the Implementation of the WHO HEARTS Strategy in the Management of Adult PLHIV with HTN and DM Comorbidities
We observed key strengths across various domains of the COM-B model that could aid HCWs’ efforts to implement this strategy to improve patients’ outcomes. These strengths demonstrate the HCWs’ opportunity and motivation to implement the strategy in providing care to these patients, as shown in Table 2 above.
Capability
The health care workers reported that the available blood pressure machines make measurements quick and easy, thereby simplifying their workflow
We are required to measure BP at every visit in the triage, and we have some BP machines which are automated, which make the measurement fast; within no time, you can determine the patient’s BP results. (Female social worker_007)
Opportunity
Health care workers had physical opportunities to support standardized care: treatment guidelines and protocols were displayed in examination rooms and accessible digitally, facilitating consistent, efficient patient screening and management and promoting adherence to clinical standards.
We mostly follow protocols/ guidelines; we pin them out in the examination rooms. …we also have soft copies of the guidelines on the phone for reference. These are meant to ease patient screening and management. (Female MCO, Interview_001)
At the facility, there exist lifestyle counselling sessions to curb the NCDs, which are largely lifestyle-based.
We do lifestyle counseling on a case-by-case basis; we do it as part of routine care. (Clinical Officer, Interview_002)
Under social opportunity, collaborations with external partners (eg, USAID, UHA) have played a key role in initiating and supporting the integration of NCD and HIV services, which help implement best practices for managing DM and HTN.
These collaborations really helped a big deal… we started a collaboration with the UHA, which is a USAID-funded organization, on the integration I mentioned about, and these helped bring in some materials and awareness on the WHO guidelines for managing HTN and DM, which is the HEARTs strategy you are talking about. Male M/O interview_011
Motivation
The HCWs are motivated to improve care quality by building strong patient relationships and ensuring the clinic environment encourages regular attendance.
We have a robust follow-up system by phone, creating rapport as well as creating a conducive environment at the clinic to induce their desire to always come to the clinic. Female social worker. Interview-007
Discussion
The World Health Organization WHO HEARTS Technical Package is a critical global strategy designed to enhance the primary care management of HTN, DM, and other CVD risk factors within low- and middle-income countries (LMICs). We identified key facilitators and barriers to the practical implementation of the HEARTS components by HCWs within HIV clinics caring for PLHIV who have HTN and/or DM comorbidities in the MRRH HIV ART Clinic in Eastern Uganda. The facilitators included the availability of standardized MOH treatment guidelines, free HTN and DM medications within the clinic pharmacy, the capacity for patient counselling and rapport, and the presence of automated BP machines. Conversely, implementation was significantly challenged by several critical barriers: a lack of dedicated in-service/Continuing Medical Education (CME) training for HTN and DM management, the absence of community-based support groups for integrated HIV-NCD co-management, difficulties in patient outcome tracking, frequent stock-outs of essential NCD medications leading to continuity-of-care disruptions, a shortage of DM test strips and few clinical BP machines, and chronic HCW understaffing at the ART clinics, which compounds the high patient load. These findings are crucial for developing a tailored implementation science approach to improve co-management and subsequent clinical outcomes among PLHIV with HTN and DM comorbidities in similar resource-limited settings.
HCWs in this study reported a deficit in the fundamental knowledge required to implement the HEARTS protocol for managing HTN and DM. This finding highlights a critical need for targeted training to enhance their competency in managing these two chronic diseases within the HIV clinic setting. Continuous Medical Education (CME) is a well-established mechanism for improving HCW knowledge, skills, performance, confidence, and self-efficacy.19 Our results are consistent with reports from other Sub-Saharan African countries, which similarly document that HCWs operating in HIV clinics possess limited knowledge regarding the management of NCDs among PLHIV.10,20 Consequently, improving HCW knowledge is essential for optimizing the quality of integrated care and enhancing patient outcomes in this co-morbid population.
The successful implementation of the HEARTS technical package was limited by a significant shortage of essential monitoring equipment. Specifically, healthcare workers reported a lack of basic tools, including a limited number of Blood Pressure (BP) monitors and glucose test strips, which are vital for accurate diagnosis and continuous patient monitoring. Without reliable monitoring tools, clinicians cannot precisely evaluate patients’ hypertensive status or blood glucose levels, hindering evidence-based management. This shortage of essential supplies for management and monitoring within the ART clinic aligns with similar findings from a previous study conducted in Kampala.21
Frequent stock-outs of essential HTN and DM medicines emerged as one of the most important barriers to sustained implementation of the WHO HEARTS package. Although NCD medicines are intended to be provided free of charge in Ugandan government facilities, the medicines are inconsistently available. In this context, the main implementation challenge is continuity and reliability of supply. Stock-outs can interrupt treatment, shift costs to patients who must purchase medicines privately, reduce adherence, and undermine confidence in integrated HIV-NCD care. This finding is consistent with evidence from Central Uganda, where medication availability was also identified as a key constraint to integrated hypertension care in HIV clinics.10 However, the existing policy of free public-sector medication provision provides a foundation on which implementation strategies can build. Rather than requiring entirely new service models, strengthening HEARTS implementation may require practical supply-chain interventions, including improved quantification and forecasting, routine stock monitoring, buffer stocks for essential HTN and DM medicines, and better alignment of NCD commodities with existing HIV clinic supply and dispensing systems.
The absence of structured community-based support groups was also cited as a barrier to WHO HEARTS implementation. This challenge is particularly acute in resource-limited settings, where the global health worker crisis necessitates strategies such as task-sharing.22 Task-sharing, defined as the delegation of clinical tasks to non-specialist or mid-level health workers, is an effective and affordable approach to improving access to NCD care.21 A model for this already exists in ART clinics, where “expert patients” successfully engage in screening and community follow-up for PLHIV. Leveraging this existing community-level infrastructure for NCD co-management represents a significant, yet currently unrealized, opportunity.
Finally, a further systemic barrier was the reported lack of simple, standardized monitoring tools to track NCD patient outcomes. The inability to use straightforward instruments to track patient progress complicates monitoring and evaluation for HCWs, potentially contributing to demotivation and reduced enthusiasm for integrated care. This finding mirrors observations from a study in Ethiopia, which highlighted the apparent lack of standardized patient- and program-monitoring instruments to support integrated NCD care among PLHIV.23
Despite the reported barriers, several key factors facilitated the implementation of the technical package. Foremost among these was the availability of standard treatment guidelines from the MOH. HCWs frequently consulted these guidelines when providing patient care, thereby enhancing their knowledge and improving patient management. HCWs’ ability to reference these materials increased the likelihood of adherence to evidence-based protocols.
A crucial ongoing facilitation activity was consistent counselling for PLHIV on healthy lifestyles. This educational component is vital for increasing awareness among PLHIV, empowering them to actively pursue screening for the early detection of co-morbidities or complications. Moreover, effective counselling helped to establish and strengthen the therapeutic rapport between HCWs and PLHIV, making consistent follow-up care and adherence monitoring more straightforward and effective.
Our study identified multiple barriers and several facilitators to implementing the WHO HEARTS strategy in the MRRH HIV ART clinic. The facilitators provide points of leverage, while the barriers can be addressed using targeted functions from the COM-B/Behavior Change Wheel framework.24 For example, inadequate training in hypertension and diabetes management can be remedied through education and training interventions; absence of community-based support for integrated HIV–NCD care may be addressed by social restructuring that engages peer support groups; and the inability to track outcomes for patients receiving both ART and NCD medications can be mitigated through enablement and environmental restructuring (for example, improved record systems and data workflows) and shortage of DM test strips and short supply of BP machines in clinical rooms could be addressed through Environmental restructuring by address supply chain gaps through ensuring consistent stock of drugs, test strips and BP equipment through quantification, forecasting and buffer stock strategies.
Limitations and Strengths
This study has several limitations. The timing of data collection, which coincided with an organizational transition from a vertical to a horizontal chronic care model following the closure of a USAID project, might have influenced participants’ views. Specifically, HCWs interviewed could have expressed especially strong opinions about the importance of integrating HTN and HIV care. Additionally, the study was conducted at a single public Antiretroviral Therapy clinic within a regional referral hospital, which may provide better care than standard facilities in the region. Nonetheless, as a government-operated institution, the reported system-level challenges, such as resource constraints and structural issues, are likely applicable to other regional referral centers across the country.
The study captures only healthcare worker perspectives; we acknowledge that including patients, caregivers, community health workers, and health-system managers would strengthen the findings and provide additional insights for future intervention design.
Despite these limitations, the study possesses several notable strengths. Our focus on NCD care, especially for PLHIV with HTN and DM, provides crucial, context-specific insights into implementation strategies and challenges in this underrepresented area of the health literature. Additionally, the analytical approach, using the Comprehensive Behavioral Change Model, provides a robust, systematic framework for understanding and addressing the contextual barriers and facilitators to effective implementation of interventions in this field.
Conclusions and Recommendations
The WHO HEARTS technical package represents a straightforward, protocol-driven implementation strategy that may support the management of the rapidly rising burden of CVDs, such as HTN and DM, in Sub-Saharan African healthcare settings. However, for successful deployment within established HIV Antiretroviral Therapy clinics, the strategy must be rigorously contextualized to address local constraints. This study identified perceived barriers and facilitators to implementation, including deficits in healthcare worker training, chronic resource shortages such as essential commodities and monitoring tools, and societal misconceptions about integrated care. These findings may inform future context-specific implementation strategies, including providing continuous and comprehensive HCW training, ensuring clinics are equipped with essential supplies such as test strips and are fully stocked with medication, and implementing robust tools for longitudinal patient monitoring.
Abbreviations
ART, Antiretroviral Therapy; BCW, Behavioral Change Wheel; CVD, Cardiovascular Diseases; COM–B, Capability Opportunity and Motivation for Behavior; DM, Diabetes Mellitus; HTN, Hypertension; LMIC, Low-middle income countries; PLHIV, People Living with HIV; MOH, Ministry of Health; SSA, Sub-Saharan Africa; WHO, World Health Organization.
Data Sharing Statement
The raw data supporting the findings of this study can be obtained from the corresponding author upon request.
Ethical Considerations
This study received approval from the Busitema University Faculty of Health Sciences Research Ethics Committee (approval number BUFHS-2024-227) and from the Uganda National Council of Science and Technology (approval number HS5399ES). We also obtained administrative permission from the Mbale Regional Referral Hospital, and all participants provided written informed consent to participate in the study. The participants’ informed consent included publication of anonymized responses/direct quotes. The study complies with the Declaration of Helsinki.
Acknowledgments
The authors are grateful to all the participants who took part in this study. Special thanks go to the clinical in-charge of Mbale regional referral hospital Chronic Care clinic, who supported the team during data collection.
Author Contributions
All authors made a significant contribution to the work reported, in the conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This publication was prepared under a Grant to Kanyike Marvin Andrew, funded by the Research Fund, Vanke School of Public Health, Tsinghua University.
Disclosure
Mr Steven Muwanga reports Grants or contracts from BRIGHT NETWORK Tsinghua University, outside the submitted work. The authors confirm that there is no conflict of interest related to the publication of this paper.
References
1. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–12. doi:10.1016/S0140-6736(20)30925-9
2. World Health Organization. HEARTS Technical package for cardiovascular disease management in primary health care. Geneva, Switzerland; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
3. Dimala CA, Blencowe H, Choukem SP. The association between antiretroviral therapy and selected cardiovascular disease risk factors in sub-Saharan Africa: a systematic review and meta-analysis. PLoS One. 2018;13(7):e0201404. doi:10.1371/journal.pone.0201404
4. Cerrato E, D’Ascenzo F, Biondi-Zoccai G, et al. Cardiac dysfunction in pauci symptomatic human immunodeficiency virus patients: a meta-analysis in the highly active antiretroviral therapy era. Eur Heart J. 2013;34(19):1432–1436. doi:10.1093/eurheartj/ehs471
5. Uganda Ministry of Health. Population-based HIV Impact Assessment. Kampala; 2022. Available from: https://phia.icap.columbia.edu/wp-content/uploads/2022/08/UPHIA-Summary-Sheet-2020.pdf.
6. Uganda MoHUN-CDRFBS. Non-Communicable Disease Risk Factor Baseline Survey Uganda 2014 REPORT. Kampala; 2014. Available from: https://www.health.go.ug/cause/non-communicable-disease-risk-factor-baseline-survey/.
7. Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol. 2018;34(5):575–584. doi:10.1016/j.cjca.2017.12.005
8. DiPette DJ, Goughnour K, Zuniga E, et al. Standardized treatment to improve hypertension control in primary health care: the HEARTS in the Americas Initiative. J Clin Hypertens. 2020;22(12):2285–2295. doi:10.1111/jch.14072
9. Flood D, Edwards EW, Giovannini D, et al. Integrando o manejo da hipertensão e do diabetes na atenção primária à saúde: uso do HEARTS como instrumento [Integrating hypertension and diabetes management in primary health care settings: HEARTS as a tool]. Rev Panam Salud Publica. 2022;46:e213. Spanish. doi:10.26633/rpsp.2022.213
10. Muddu M, Ssinabulya I, Kigozi SP, et al. Hypertension care cascade at a large urban HIV clinic in Uganda: a mixed methods study using the Capability, Opportunity, Motivation for Behavior change (COM-B) model. Implement Sci Commun. 2021;2(1):121. doi:10.1186/s43058-021-00223-9
11. Richard K, Raymond K, Winfred NA, et al. Prevalence of hyperglycaemia and associated factors among people living with HIV in Eastern Uganda: a descriptive cross-sectional study. SN Compreh Clin Med. 2024;6. doi:10.1007/s42399-024-01737-8
12. Kanyike AM, Nakawuki AW, Akech GM, et al. Prevalence, awareness, and factors associated with hypertension among people living with HIV in Eastern Uganda. A multicentre cross-sectional study. HIV AIDS. 2024;16:325–335. doi:10.2147/hiv.S477809
13. Owuor M, Wamuti B, Katz DA, et al. Factors influencing community demand for assisted partner services for HIV in western Kenya: a multilevel qualitative analysis. BMJ Open. 2025;15(3):e088436. doi:10.1136/bmjopen-2024-088436
14. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
15. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
16. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523. doi:10.1016/j.socscimed.2021.114523
17. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
18. Lincoln YSG, Egon G. Establishing depilndability and confirmability in naturalistic inquiry through an audit. 1982.
19. Chaker R, Hajj-Hassan M, Ozanne S. The effects of online continuing education for healthcare professionals: a systematic scoping review. Open Educ Stud. 2024;6(1). doi:10.1515/edu-2022-0226
20. Masupe T, Mashalla Y, Seloilwe E, Jibril H, Medhin H. Integrated management of HIV/NCDs: knowledge, attitudes, and practices of health care workers in Gaborone, Botswana. Afr Health Sci. 2019;19(3):2312–2323. doi:10.4314/ahs.v19i3.3
21. Joshi R, Alim M, Kengne AP, et al. Task shifting for non-communicable disease management in low and middle income countries--a systematic review. PLoS One. 2014;9(8):e103754. doi:10.1371/journal.pone.0103754
22. World Health Organization. World Health Report 2006: working together for health. Geneva: World Health Organization; 2006.
23. Letebo M, Shiferaw F. Adapting HIV patient and program monitoring tools for chronic non-communicable diseases in Ethiopia. Glob Health. 2016;12(1):26. doi:10.1186/s12992-016-0163-y
24. Michie S, Atkins L, West R. The Behaviour Change Wheel. A Guide to Designing Interventions. London: Silverback Publishing; 2014.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Independent Association of 25[OH]D Level on Reduced Glutathione and TNF-α in Patients with Diabetes and/or Hypertension
AlRadini FA, El-Sheikh AAK, Al Shahrani AS, Alzamil NM, Fayed AA, Alsayed E, Alharbi SS, Altulihee MA, Andijani SA, AlShaiddi WK, Alamri FA
International Journal of General Medicine 2022, 15:7065-7075
Published Date: 5 September 2022
Interventions Incorporating Therapeutic Alliance to Improve Medication Adherence in Black Patients with Diabetes, Hypertension and Kidney Disease: A Systematic Review
Desta R, Blumrosen C, Laferriere HE, Saluja A, Bruce MA, Elasy TA, Griffith DM, Norris KC, Cavanaugh KL, Umeukeje EM
Patient Preference and Adherence 2022, 16:3095-3110
Published Date: 14 November 2022
Prevalence of and Factors Associated with Hypertension Among Adults on Dolutegravir-Based Antiretroviral Therapy in Uganda: A Cross Sectional Study
Kasoma Mutebi R, Weil Semulimi A, Mukisa J, Namusobya M, Namirembe JC, Nalugga EA, Batte C, Mukunya D, Kirenga B, Kalyesubula R, Byakika-Kibwika P
Integrated Blood Pressure Control 2023, 16:11-21
Published Date: 19 April 2023
Knowledge of Cardiovascular Disease Risk Factors and Its Primary Prevention Practices Among the Saudi Public – A Questionnaire-Based Cross-Sectional Study
Bashatah A, Syed W, Al-Rawi MBA
International Journal of General Medicine 2023, 16:4745-4756
Published Date: 20 October 2023
Correlation Between Anthropometric Measurements with Cardiometabolic Biomarkers and Ten-Year Cardiovascular Risk Score Among People with HIV in Uganda
Baluku JB, Mutinye Kwesiga J, Adzemovic T, Nabwana M, Olum R, Bongomin F, Rhein J
HIV/AIDS - Research and Palliative Care 2025, 17:287-296
Published Date: 6 September 2025