Back to Journals » Clinical Ophthalmology » Volume 20
Exposure to and Comfort with Toric and Presbyopia-Correcting Intraocular Lenses: A Survey of Ophthalmology Residents
Authors Devireddy N, Scruggs K, Lehman E, Longenecker A, Pantanelli SM ![]()
Received 19 April 2026
Accepted for publication 23 June 2026
Published 9 July 2026 Volume 2026:20 615011
DOI https://doi.org/10.2147/OPTH.S615011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Nitya Devireddy,1 Kathleen Scruggs,1 Erik Lehman,2 Amy Longenecker,1 Seth M Pantanelli1
1Department of Ophthalmology, Penn State College of Medicine, Hershey, PA, USA; 2Department of Public Health Sciences, Penn State College of Medicine, Hershey, PA, USA
Correspondence: Seth M Pantanelli, Department of Ophthalmology, Penn State College of Medicine, 500 University Drive, HU19, Hershey, PA, 17033-0850, USA, Tel +1 717-531-5690, Fax +1 717-531-5009, Email [email protected]
Purpose: To investigate exposure to and comfort with advanced technology intraocular lenses (ATIOLs) and ascertain residency program characteristics predictive of increased exposure and comfort.
Patients and Methods: A survey was created in REDCap and distributed to fourth-year (PGY-4) ophthalmology residents across the United States through the Association of University Professors in Ophthalmology (AUPO). The survey included questions on characteristics of ophthalmology residency training programs, understanding of preoperative counseling, intraoperative steps, and postoperative management pertinent to ATIOL implantation. Continuous and ordinal outcomes were analyzed using Kruskal Wallis or Wilcoxon Rank Sum Test and ordinal logistic regression, respectively.
Results: There were 72 residents who completed the survey. Programs with multiple faculty offering ATIOLs provided greater opportunity for residents to observe preoperative counseling for presbyopia-correcting IOLs (OR 9.49 [1.70– 52.8]; p=0.010) and practice preoperative toric IOL counseling themselves (OR 9.89 [1.70– 57.6]; p=0.011). These residents also reported greater comfort with patient selection for presbyopia-correcting IOLs (OR 5.15 [1.05– 25.3]; p=0.044). Programs with 10– 25 faculty offered greater opportunity for residents to observe pre-op toric IOL (OR 4.98 [1.17– 21.13]; p=0.03) and presbyopia-correcting IOL counseling (OR 8.98 [1.98– 40.84]; p=0.004) compared to those with 0– 10 faculty. Programs with industry-subsidized ATIOL programs had greater number of resident cataract cases as primary surgeon (Mean 184 vs. 137; p=0.014).
Conclusion: Incorporating exposure to ATIOLs into residency training curricula will equip trainees to be proficient with options that align with patients’ expectations. This can be achieved by supporting clinician-educator faculty that use ATIOLs themselves and permitting industry representatives to interact with trainees.
Keywords: cataract surgery, education, toric, multifocal, resident
Introduction
Advanced technology intraocular lenses (ATIOLs) include toric IOLs, which can correct astigmatism, and presbyopia-correcting IOLs (PC-IOLs), which reduce bifocal and trifocal dependence by extending depth of field or providing multifocality.1,2 These IOLs offer positive visual and refractive outcomes and less reliance on corrective glasses after surgery, but may also be associated with photopsias (eg. glare, halos, and starbursts) or loss of contrast in some patients. As such, working with this technology requires that the surgeon develop a skill-set that includes being discerning with patient selection, providing proper education, maintaining best practices for IOL power calculations, being technically proficient with orienting and centering these lenses intraoperatively, and being in a position to help the patient with surface enhancements or IOL exchange in the event of postoperative complications.
Despite the obvious benefits ATIOLs confer, surveys conducted by the American Society of Cataract and Refractive Surgery (ASCRS) in both 2016 and 2019 demonstrated limited exposure to and confidence with these lenses among ophthalmologists-in-training and those less than 5 years out of practice. In the 2016 survey, 61% of respondents had never implanted a PC-IOL and 70% rated their residency experience with PC-IOLs as somewhat or very inadequate, while in 2019, 34.7% had still never implanted one.3,4 In 2016, only 15% stated they were very comfortable and 31% were somewhat comfortable with patient selection for these IOLs.3 Similarly, in the 2019 survey, only 25% of young ophthalmologists stated they were very confident and 39.1% were somewhat confident in preoperative evaluation, implantation, and management of PC-IOLs.4
While there are many factors that might contribute to the statistics above, one possible explanation is that residents are not acquiring the unique skills required to feel comfortable with this technology in the course of their training. It is not known how widespread structured ATIOL curricula are among US ophthalmology residency training programs. While the Accreditation Council for Graduate Medical Education (ACGME) requires that residents perform a minimum of 86 cataract surgeries to graduate, there is no mandated curriculum for ATIOL education. Furthermore, International Council of Ophthalmology Surgical Competency Assessment Rubric (OSCAR) and ACGME ophthalmology program requirements do not specifically mention ATIOLs.5,6 Despite this, academic ophthalmologists recognize that ATIOL education is important. In a survey of U.S. ophthalmology program directors, toric IOL selection and implantation was recognized as the third most important cataract surgery technique for residents to learn and master before graduating.7
The purpose of this study was to assess current ophthalmology residents’ exposure to and comfort with ATIOLs, and correlate these findings with residency program characteristics, with a goal of identifying program features associated with resident education in this domain.
Material and Methods
This survey study received approval from the Penn State College of Medicine Institutional Review Board and was carried out in compliance with the tenets of the Declaration of Helsinki. Survey participants were able to indicate online implied consent prior to beginning the online survey and all participants’ data was maintained confidentially throughout the study. The survey was developed by the primary authors, which includes a full-time academic ophthalmologist involved in residency cataract surgery education and a medical student pursuing ophthalmology. The survey included demographic questions, questions about respondents’ respective residency programs and level of involvement with ATIOLs, respondents’ cataract surgery numbers using ATIOLs, and level of comfort and exposure to monofocal toric and PC-IOLs. Respondents were surveyed on their comfort with preoperative counseling, intraoperative steps, and postoperative management of patients with these IOLs. The survey was prepared and administered using the Research Electronic Data Capture (REDCap) platform and is provided as Supplemental Figure 1.
All PGY-4 ophthalmology residents at Accreditation Council for Graduate Medical Education (ACGME) accredited ophthalmology training programs in the U.S. were eligible to complete the survey. Residents with no experience performing cataract surgery as primary surgeon were excluded from the study.
After review and approval by the Association of University Professors of Ophthalmology (AUPO) Data Resource Committee, the survey link was sent to the program directors and program coordinators of all U.S. ophthalmology residency programs to distribute among their fourth-year residents. An incentive of a $10 gift card was offered to residents who completed the survey. The survey remained open for approximately 3 weeks from April 3, 2025 to April 26, 2025 with a reminder Email sent to residency programs 2 weeks after the initial recruitment Email to encourage completion of the survey.
Descriptive statistics were used to characterize participants’ demographic information, cataract surgery numbers, and residency program characteristics. Continuous outcomes surveying resident cataract numbers were analyzed using either Kruskal Wallis or Wilcoxon Rank Sum tests to determine if the residency program factors queried in the survey were associated with these outcome variables. Nonparametric data for multiple pairwise group comparisons between each residency program factor was adjusted for with Dwass, Steel, Critchlow-Fligner method. Spearman correlation was used to determine association between frequency of observing or practicing with ATIOLs and ordinal outcomes measuring level of comfort using these IOLs and managing patients with them. Chi-square was used for the survey variable measuring comfort with lens centration using intraoperative purkinje images as the response options represented distinct categories of experience and knowledge rather than ordinal Likert scale options. Ordinal logistic regression models were used to analyze the residency program characteristics significantly associated with resident experience and comfort, which are ordinal outcomes with Likert scale response options. All statistical analyses were performed in SAS (V9, SAS Institute Inc, Cary, NC). P values <0.05 were considered statistically significant.
Results
The survey was sent to all 121 ACGME-certified ophthalmology residency training programs which were instructed to distribute the survey among fourth-year residents. There were 72 fourth-year ophthalmology residents who met the inclusion criteria, responded to the survey, and were included in the analysis. Thirty-five residents were between the ages 26–30 (48%), 34 (47.2%) were between the ages 31–35, and there was an approximately even distribution of women and men respondents (Table 1). The majority of respondents were training in the Midwest (25, 34.7%) or South (23, 31.9%), followed by Northeast (16, 22.2%), West (7, 9.7%), and 1 (1.4%) chose not to answer.
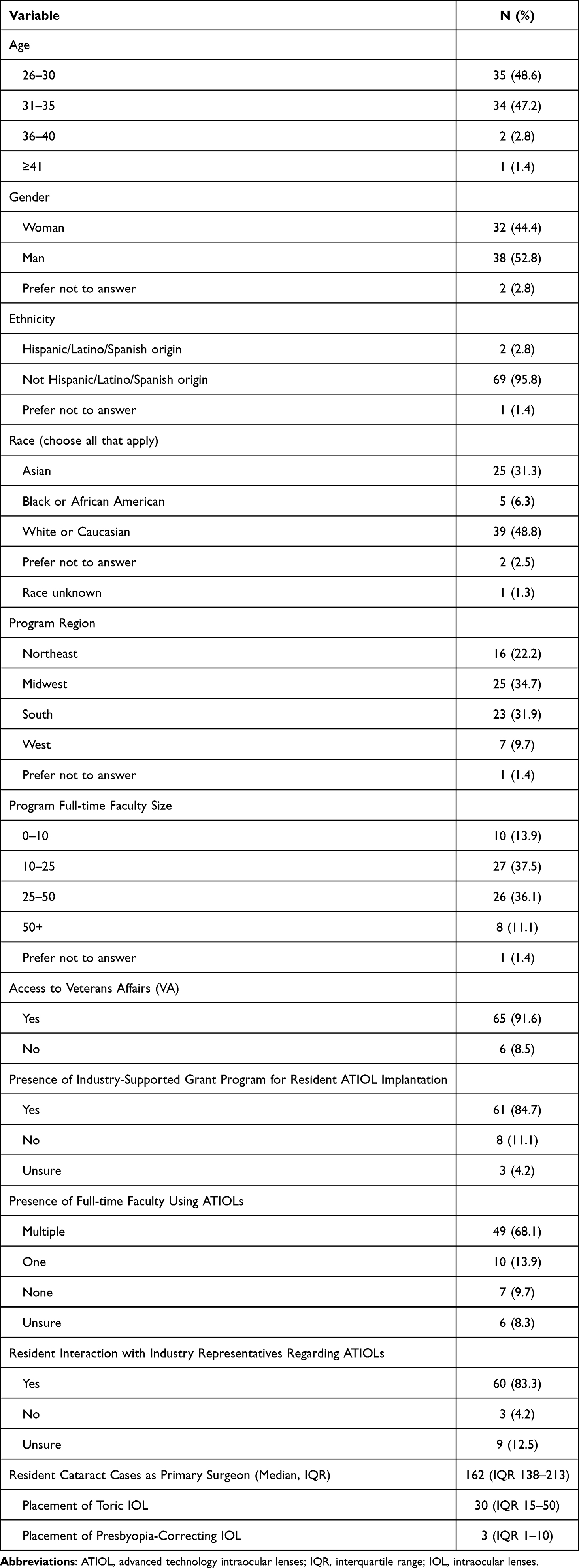 |
Table 1 Respondent Demographics and Residency Program Characteristics |
Regarding program size, 27 (37.5%) residents were at programs with between 10–25 full-time faculty, 26 (36.1%) at programs with between 25–50 faculty, 10 (13.9%) at programs with 0–10 faculty, 8 (11.1%) at programs with 50+ faculty, and 1 (1.4%) chose not to answer. Forty-nine (68.1%) residents were training at programs where there were multiple full-time faculty routinely offering ATIOLs to patients, 10 (13.9%) were at programs where only 1 faculty member offered ATIOLs, 7 (9.7%) did not have faculty members using these IOLs, and 6 (8.3%) were unsure. Sixty-five (91.6%) had access to a Veterans Affairs (VA) facility for cataract surgery training, 69 (83.3%) were permitted to interact with industry representatives selling ATIOLs, and 61 (84.7%) disclosed that their programs offered the opportunity to participate in industry-supported grant programs, allowing them to gain exposure to implanting ATIOLs at a reduced/no cost to the patient. The median number of cataract surgery cases performed as primary surgeon was 162 (IQR 138–213). Of these, the median number of cases involving placement of toric IOLs was 30 (IQR 15–50) and those involving PC-IOLs was 3 (IQR 1–10).
Table 2 outlines residency program characteristics as predictors of survey respondents’ number of cataract surgery cases and ATIOLs. Regional variation in cataract numbers was minimal, except for the number of toric IOLs implanted, where residents in the Midwest (median [IQR] = 30 [20–50]) reported significantly more cases than those in the Northeast (median = 10 [3–30]; p = 0.03). Access to a Veterans Affairs (VA) hospital was associated with significantly higher number of toric IOLs implanted (p=0.007) but did not significantly impact cataract surgical volume (p=0.063) or the number of presbyopia-correcting IOLs implanted (p=0.298). Participation in industry-supported grant programs for ATIOLs were associated with significantly higher overall cataract surgical volume (p=0.014) but did not significantly influence the number of toric or PC-IOLs implanted. Full-time faculty size, presence of attending faculty offering ATIOLs, or access to industry representatives were not associated with significant differences in cataract numbers.
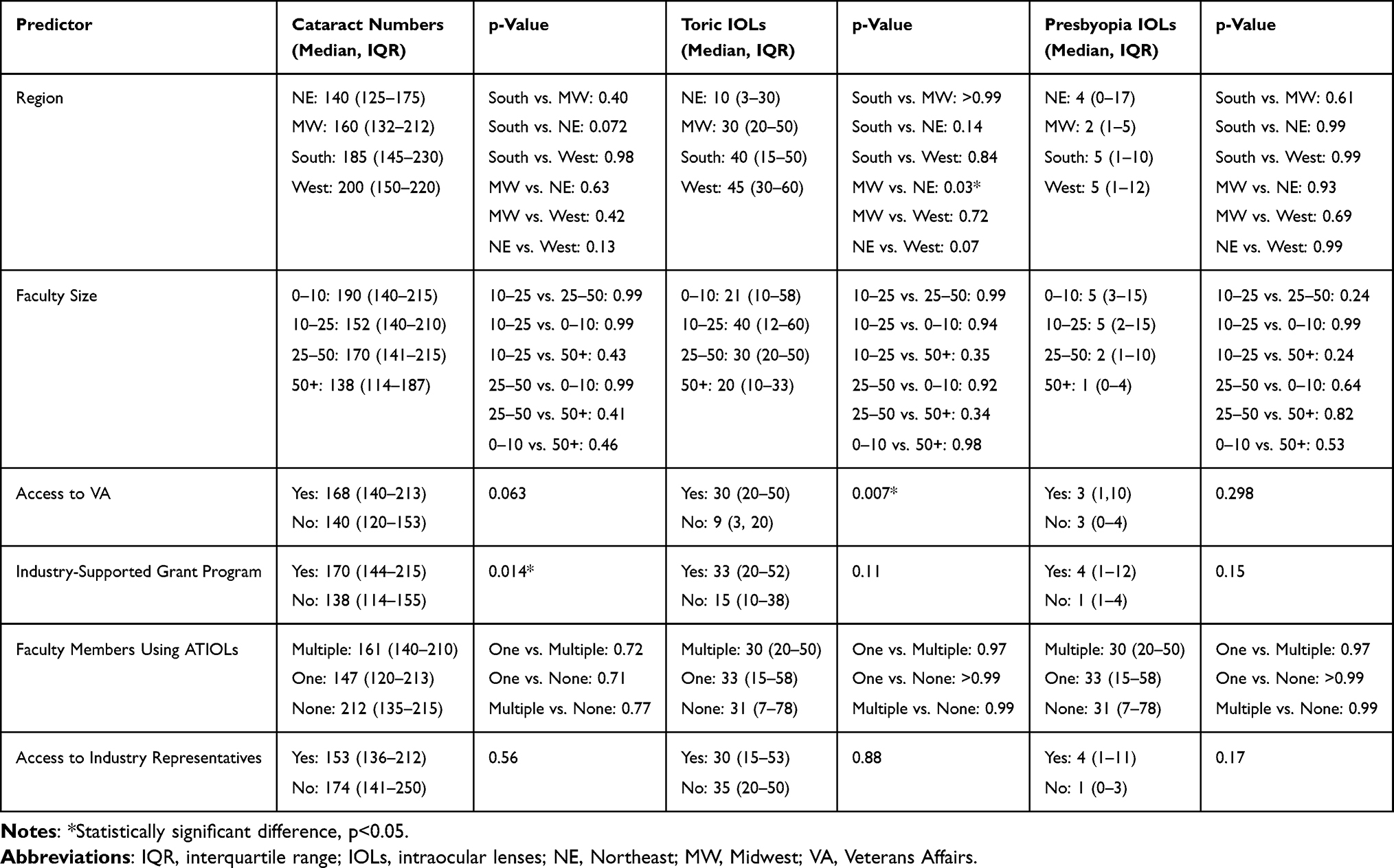 |
Table 2 Residency Program Characteristics as Predictors of Respondent Cataract and Advanced Technology Intraocular Lens Numbers |
Toric Intraocular Lenses
Among residency program characteristics, several factors were significantly associated with exposure to and comfort with toric IOLs (Table 3). Regional variation was noted, as residents in the Midwest were more likely to report observing preoperative counseling regarding risks and benefits of toric IOLs (OR 3.93 [1.14–13.46], p=0.03) and to feel comfortable with postoperative evaluation and management of residual refractive error/blurry vision (OR 4.66 [1.38–15.84], p=0.014). Similarly, residents in the South were more likely than those in the Northeast to observe preoperative counseling (OR 3.94 [1.13–13.46], p=0.032). Faculty size also influenced toric IOL exposure, with programs of 10–25 faculty compared to 0–10 associated with increased odds of observing preoperative counseling (OR 4.98 [1.17–21.13], p=0.030). The presence of multiple attending “champions” routinely offering ATIOLs was associated with higher odds of residents actively practicing preoperative counseling (OR 9.89 [1.70–57.57], p=0.011) regarding astigmatism and risks and benefits of toric IOLs. No significant associations were found with access to industry representatives or participation in industry-supported ATIOL grant programs.
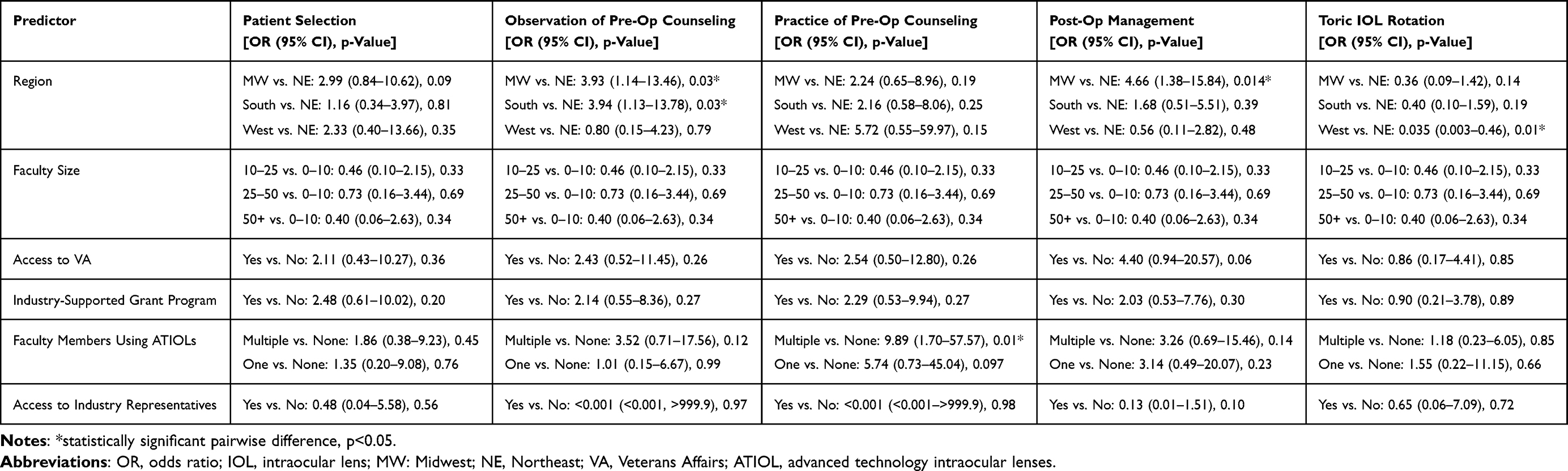 |
Table 3 Respondent Exposure to and Comfort with Toric Intraocular Lenses |
Presbyopia-Correcting Intraocular Lenses
For PC-IOLs, full-time faculty size, presence of industry-supported ATIOL grant programs, and faculty members routinely offering ATIOLs were significantly associated with exposure and comfort (Table 4). Programs with 10–25 faculty compared to 0–10 were associated with higher odds of observing preoperative counseling (OR 8.98 [1.98–40.84], p=0.004). Participation in industry-supported grant programs was associated with increased experience with lens centration using intraoperative Purkinje images (OR 4.70 [1.21–18.26], p=0.026). Those who participated in these programs reported having experience performing lens centration using purkinje images 1–5 times, whereas those who did not participate in these programs had only read about lens centration, but never performed it. Having multiple attending champions was associated with higher odds of comfort with patient selection (OR 5.14 [1.05–25.32], p=0.044) and increased observation of preoperative counseling (OR 9.49 [1.70–52.84], p=0.010). No significant associations were found with resident comfort in postoperative management, IOL power calculations for exchange, or IOL exchange in the setting of an intact bag. Access to industry representatives was also not significantly associated with residents’ exposure to PC-IOLs.
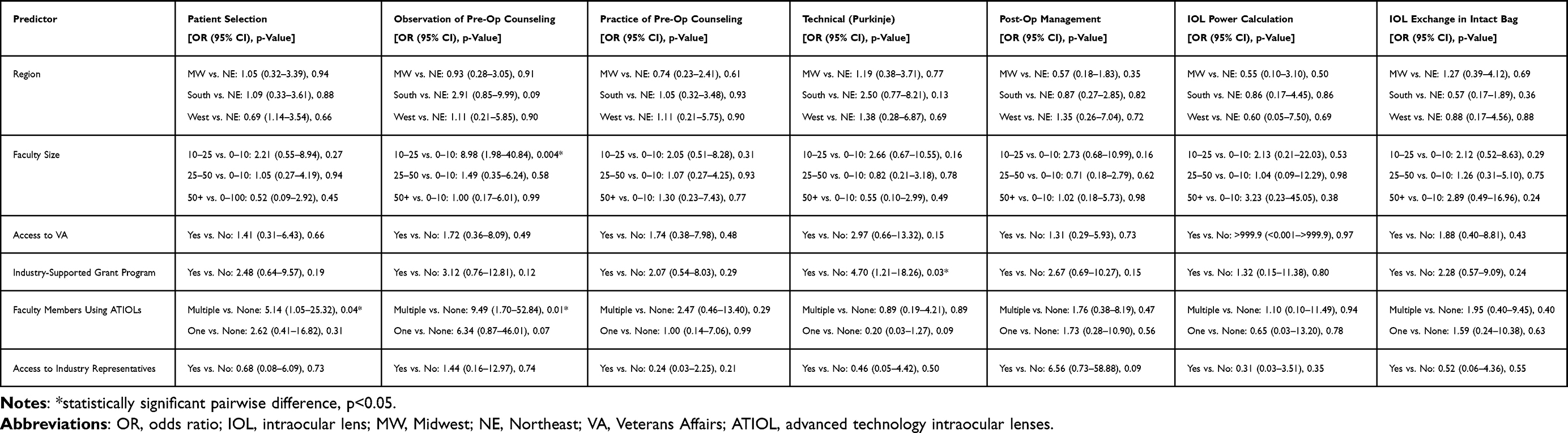 |
Table 4 Respondent Exposure to and Comfort with Presbyopia-Correcting Intraocular Lenses |
Discussion
Exposure to ATIOLs in residency positively influences resident knowledge about them and may impact future practice patterns.8 Despite this, our national survey of US PGY-4 ophthalmology residents found considerable variability in exposure to these technologies. While all respondents’ cataract case numbers exceeded ACGME requirements, experience with PC-IOLs was limited. The median number of PC-IOLs implanted per resident in the present study was only 3 (IQR 1–10). This is consistent with the 2016 report from Schallhorn et al, in which 61% of ophthalmology trainees and recent graduates had never implanted a PC-IOL and only 29% reported being comfortable with patient selection for these lenses.3 Despite nearly a decade of innovation in IOL design and expanded adoption in clinical practice, our results suggest that resident training in PC-IOLs has not substantially changed. Although PC-IOLs are increasingly used, the limited exposure to these technologies among trainees suggests that related educational opportunities are not expanding at the same pace as clinical adoption. This may have important implications for future practice as young ophthalmologists could enter independent practice underprepared to manage these lenses.
There may be discrepancies in perceived and actual comfort with PC-IOLs among faculty and residents. In a prior study, program directors reported that 59.9 ± 36.1% (range 0–100%) of graduating residents were competent in selecting and implanting multifocal IOLs.7 This is in contrast to our findings, and those of others,3 where trainees expressed low comfort with handling PC-IOLs.
In contrast to PC-IOLs, exposure to toric IOLs was found to be more common, with residents reporting a median of 30 (IQR 15–50) cases. This aligns with the ASCRS Young Eye Surgeons Clinical Surveys where respondents from the 2016 and 2019 surveys had more experience and greater comfort using toric IOLs compared to PC-IOLs.3,4 The greater exposure to toric IOLs might be explained by the perceived safety profile of toric over PC-IOLs. Research has found that residents using toric IOLs in cataract surgery achieve positive refractive and safety outcomes, with outcomes comparable to those of experienced surgeons.8–11 A second reason for the increased toric IOL exposure might be the value program directors place on their incorporation into training curricula. In a prior survey of program directors, toric IOL implantation was identified as the third most important cataract surgery skill for residents to master before graduation.7 Our study extends the above findings by identifying specific program-level factors associated with increased toric IOL exposure, including faculty size, regional variation, and the presence of attending “champions” routinely offering ATIOLs to their patients.
We found that residents in the Midwest implanted significantly more toric IOLs compared to those in the Northeast. The reasons underlying this regional variation are unclear and may be explained by variations in patient demographics, faculty practice patterns, institutional resources, institutional relationships with industry, reimbursement patterns, or regional adoption of ATIOLs. The training background of faculty across regions and their comfort with using ATIOLs can also influence resident exposure to these technologies. However, this survey instrument did not assess these factors, and future studies are required to evaluate regional variation in ATIOL training.
Residents training alongside multiple faculty members who routinely offered ATIOLs were more likely to report comfort with patient selection, observation of preoperative counseling, and active practice of counseling skills. This highlights that even in the absence of formal curricular requirements, faculty engagement and prioritization of ATIOL education can markedly influence the quality of resident training. Prior studies on medical education and other specialties have demonstrated that local faculty expertise and a “champion” can influence the implementation of new techniques and technologies, underscoring the critical role of engaged mentors in shaping resident competence and skills.12,13
Importantly, our data reveal that structured exposure to ATIOLs is not uniform across training programs. Participation in industry-supported programs was associated with increased odds of intraoperative experience with Purkinje images for PC-IOL centration, an essential step in optimizing postoperative outcomes. However, reliance on industry-supported programs raises concerns about sustainability and equity. Programs without such partnerships may leave residents under-exposed, which could perpetuate disparities in readiness for independent practice. Similar concerns have been raised in prior literature on surgical device training, where industry involvement can augment exposure but should not replace standardized curricula.14 To increase exposure to ATIOLs when industry-supported initiatives are not available, there must be an emphasis on ATIOL education in the residency curriculum. This could include simulation-based training, wet-lab opportunities, ATIOL-specific cases in education lectures, a formal didactics curriculum, and institutional support to encourage ATIOL exposure. These strategies require support from residency program leadership to provide consistent exposure to ATIOLs while reducing dependence on industry-sponsored initiatives.
The implications of these findings are significant for both training and patient care. As cataract surgery increasingly functions as a refractive procedure, patient expectations for spectacle independence continue to rise. Trainees unexposed to ATIOLs during residency may enter independent practice without adequate skills to counsel patients on refractive options or manage postoperative concerns. A lack of preparedness in these areas could limit new graduates’ ability to meet patient expectations and may delay adoption of new technologies in clinical practice. These results underscore the need for structured, standardized ATIOL curricula within U.S. residency programs. Currently, ACGME program requirements and the ICO OSCAR rubric do not mention ATIOLs, leaving training highly program-dependent.5,6 At the University of Chicago, faculty created a stepwise surgical curriculum introducing ATIOLs to residents.15 The success of this curriculum offers a blueprint for other residency programs to incorporate ATIOL education into didactics, simulation-based training, and wet lab experiences to provide residents with foundational knowledge and technical practice. Collaborative efforts by national organizations such as AUPO, AAO, and ASCRS to design an ATIOL didactic and wet lab curriculum may help establish minimum benchmarks for ATIOL exposure, ensuring equitable and comprehensive education across programs.
Our study has several limitations, most notably due to the inherent nature of a survey study. As it is a voluntary survey, there is response bias, and not all programs were represented. Case numbers were self-reported, which may introduce recall error. Additionally, this study only surveyed PGY-4 residents, and we did not capture earlier exposure that may occur during residency. The survey instrument was developed by the authors and reviewed and approved by the AUPO Data Resource Committee, but was not formally pilot tested or validated before being distributed, which did not allow for assessing the clarity and reliability of the survey. Despite these limitations, this study provides one of the most up-to-date assessments of ATIOL training in U.S. ophthalmology residency programs and highlights specific factors associated with meaningful exposure.
Conclusion
This study demonstrates substantial variability in ATIOL training among U.S. ophthalmology residency programs. While toric IOL exposure has improved relative to prior reports, PC-IOL experience remains limited despite their growing role in modern cataract surgery. Faculty engagement, program size, and industry-supported opportunities influence resident preparedness, but broader curricular reform will be necessary to ensure consistent training in these increasingly important technologies. Future research should investigate the impact of ATIOL training on graduates’ early-practice patterns and patient outcomes, as well as barriers to implementing standardized curricula. Longitudinal evaluation of exposure across all years of residency would also help identify the most effective timing and methods for ATIOL education in residency curricula. We advocate for greater ATIOL exposure and practical application of surgical techniques for ophthalmology trainees. Utilizing multiple education modalities such as journal clubs, active resident participation in during cataract evaluations, industry-sponsored wet labs, didactics, and standardized benchmarks can help achieve greater exposure to ATIOLs for trainees.
Acknowledgments
The paper was presented in part at the American Society of Cataract and Refractive Society (ASCRS) 2026 annual conference in Washington, DC as a poster.
Funding
The authors received funding support from the Penn State College of Medicine Woodward Center (Hershey, Pennsylvania, USA) for Excellence in Health Sciences Education Grant. The funding source had no role in the collection, analysis, interpretation of data, report writing, or decision to submit the article for publication.
Disclosure
SMP is a consultant for Bausch & Lomb and Carl Zeiss Meditec, and has received research support from Bausch & Lomb, and Carl Zeiss Meditec, unrelated to the present work. He also reports travel support from RxSight. The remaining authors have no proprietary interest or financial relationships to disclose for this work.
References
1. Chen SP, Woreta F, Chang DF. Cataracts: a Review. JAMA. 2025;333(23):2093–10. doi:10.1001/jama.2025.1597
2. Amesbury EC, Miller KM. Correction of astigmatism at the time of cataract surgery. Curr Opin Ophthalmol. 2009;20(1):19–24. doi:10.1097/ICU.0b013e328319c27a
3. Schallhorn JM, Ciralsky JB, Yeu E. Resident and young physician experience with complex cataract surgery and new cataract and refractive technology: results of the ASCRS 2016 Young Eye Surgeons survey. J Cataract Refract Surg. 2017;43(5):687–694. doi:10.1016/j.jcrs.2017.04.022
4. Eyeworld. ASCRS Clinical Survey 2019 - YES. EyeWorld Supplement. Available from: https://supplements.eyeworld.org/eyeworld-supplements/september-2020-yes-clinical-survey.
5. Accreditation Council for Graduate Medical Education. ACGME Program Requirements for Graduate Medical Education in Ophthalmology. 2016.
6. International Council of Ophthalmology. Ophthalmic Educators. 2021. Available from: https://icoph.org/education/ophthalmic-educators/.
7. Yen AJ, Ramanathan S. Advanced cataract learning experience in United States ophthalmology residency programs. J Cataract Refract Surg. 2017;43(10):1350–1355. doi:10.1016/j.jcrs.2017.10.014
8. Roensch MA, Charton JW, Blomquist PH, Aggarwal NK, McCulley JP. Resident experience with toric and multifocal intraocular lenses in a public county hospital system. J Cataract Refract Surg. 2012;38(5):793–798. doi:10.1016/j.jcrs.2011.11.043
9. Moreira HR, Hatch KM, Greenberg PB. Benchmarking outcomes in resident-performed cataract surgery with toric intraocular lenses. Clin Experiment Ophthalmol. 2013;41(6):624–626. doi:10.1111/ceo.12054
10. Tran EM, Tang KS, Chen AJ, et al. Refractive Outcomes for Cataract Surgery With Toric Intraocular Lenses at a Veterans Affairs Medical Center. Fed Pract Health Care Prof VA DoD PHS. 2020;37(3):138–142.
11. Sundy M, McKnight D, Eck C, Rieger F. Visual Acuity Outcomes of Toric Lens Implantation in Patients Undergoing Cataract Surgery at a Residency Training Program. Mo Med. 2016;113(1):40–43.
12. Kraleti S, Gibson-Oliver L, Jarrett DM. The Importance of a Champion in Leading Major Improvements in Residency Programs. Fam Med. 2024;56(10):659–662. doi:10.22454/FamMed.2024.937126
13. Elder KG, Frederick EK, Raake S, Stephens BC. Faculty Doing More with Less: a Technology Initiative Realized Through a Structured Process. Innov Pharm. 2022;13(2):4469. doi:10.24926/iip.v13i2.4469
14. He B, de Smet MD, Sodhi M, Etminan M, Maberley D. A review of robotic surgical training: establishing a curriculum and credentialing process in ophthalmology. Eye. 2021;35(12):3192–3201. doi:10.1038/s41433-021-01599-7
15. Riaz KM, Williams BL, Farooq AV, Kloek CE. Surgical Curriculum for Presbyopia-Correcting Intraocular Lenses: resident Experiences and Surgical Outcomes. Clin Ophthalmol. 2020;14:2441–2451. doi:10.2147/OPTH.S263249
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Visual and Refractive Outcomes of a New Hydrophobic Trifocal Toric Intraocular Lens
Daya S, Espinosa Lagana M
Clinical Ophthalmology 2024, 18:997-1007
Published Date: 3 April 2024
A Modular Cataract Surgery Training Model Incorporating Human Factors and a Pedagogical Theory
Mansoor Q, Qurashi N, Chen Y
Clinical Ophthalmology 2024, 18:1171-1180
Published Date: 1 May 2024
Impact of Simulation-Based Surgical Training in Laparoscopy on Satisfaction Level and Proficiency in Surgical Skills
Mukhtar F, Shaheen MF, Alhabeeb AY, Zafar M, Alkattan K
Advances in Medical Education and Practice 2025, 16:357-366
Published Date: 27 February 2025