Back to Journals » Clinical Ophthalmology » Volume 18
A Modular Cataract Surgery Training Model Incorporating Human Factors and a Pedagogical Theory
Authors Mansoor Q, Qurashi N, Chen Y
Received 17 December 2023
Accepted for publication 11 April 2024
Published 1 May 2024 Volume 2024:18 Pages 1171—1180
DOI https://doi.org/10.2147/OPTH.S451594
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Qasim Mansoor,1,2 Neda Qurashi,1 Yunzi Chen1
1Department of Ophthalmology, James Cook University Hospital, Middlesbrough, UK; 2Teesside Newmedica Eye Health Clinic & Surgical Centre, Middlesbrough, UK
Correspondence: Qasim Mansoor, James Cook University Hospital, Marton Road, Middlesbrough, Cleveland, TS4 3BW, UK, Email [email protected]
Synopsis: High volume cataract lists are cost-effective, reduce waiting times, and facilitate surgical teaching. We propose a stepwise training model that incorporates human factor principles and a reflective pedagogical approach, which has not been documented previously.
Background/Aims: Surgical training in ophthalmology is effective when a modular approach is utilised. High volume lists further enhance training by increasing exposure to a newer way of learning and working. We evaluated the efficiency and safety of trainee-assisted cataract surgery across a single NHS eye unit and an independent sector (IS) provider.
Methods: We examined results from audits of surgical efficiency and safety in trainee-assisted high-volume lists, including a single-centre comparative evaluation of consultant-only and trainee lists. The quantitative and qualitative information gained from these projects helped us to implement a modular, structured training programme that utilises a reflective cycle of pedagogy, suitable for any grade of trainee.
Results: Our projects included an audit following cataract surgery performed by a surgical trainee over a 5-month period, which showed excellent post-op refractive results and no cases of intra-operative and post-operative complications. A single-centre observational study demonstrated comparable surgical throughput and safety results for trainee and solo consultant high volume lists. Systemic and ocular complication rates were reported to be similar for low and medium risk cataract surgery among trainee supervised IS and NHS lists.
Conclusion: Cataract surgery outcomes and patient feedback support the effectiveness of the surgical training model. Combining Gibbs’ reflective cycle of critical reflection with the International Council of Ophthalmology’s principles helped us to develop the QM Model of modular teaching for cataract surgery, which we believe is suitable for utilisation in all surgical centres in the NHS and IS settings, for both low volume and high-volume surgical lists regardless of trainee experience.
Plain Language Summary:
What Is Already Known on This Topic
- High volume lists are increasingly popular for cataract surgery; however, trainee exposure to high flow cataract surgery lists is limited.
What This Study Adds
- A modular approach to training via high volume training lists is possible. Origination and implementation of a stepwise cataract surgery training model that incorporates human factors and a pedagogical learning approach within high volume lists in the independent sector and NHS setting.
How This Study Might Affect Research, Practice, or Policy
- Promote the widespread adoption of the QM model which integrates modular-based experiential learning approaches for surgical training in both NHS and independent sector settings, applicable to low and high volume surgical lists, irrespective of trainee experience.
Keywords: Cataract, surgery, training, education, teaching, pedagogy
Introduction
The independent sector, in collaboration with Health Education England (HEE), the Royal College of Ophthalmologists (RCOphth) and NHS England, play an important role in promoting excellence in ophthalmic education and training. Human factors training and application of its principles in routine surgical activity are crucial to achieving the General Medical Council (GMC) standards for education and training, while effective teamwork and communication are essential components in patient-centred safer surgery.
In March 2021 RCOphth and GIRFT (Getting It Right First Time) established guidelines to set up high volume surgical hubs for several subspecialities.1 Over time, it became evident that “mixed” lists with a combination of low complexity and high complexity cases were suitable for the high volume standardised processes without adversely affecting productivity or efficiency.2 In order to make the high flow pathway effective, it is important that a consistent process is established with trained professionals who are equipped with the necessary skills and knowledge. By doing so, both experience and expertise are concentrated where it is needed, leading to better outcomes.
During and after the Covid-19 pandemic, trainees reported limited access to surgery and reduced cataract surgery numbers for their portfolios.3,4 Identifying which trainee is suitable for training in the independent sector is reviewed regularly by the educational supervisors from ST1 level. The blueprint for cataract training 2022 guidance recommends that trainees need to complete around 100 cases per year from ST2-ST6 and if the NHS training unit is not able to provide this, then the trainee should be placed in the independent sector.5 It is thought that once a trainee has completed around 500 cases, the complication rate reduces by 50%.
In line with this notion, trainee exposure to high volume lists is limited and to date there is no stepwise model that incorporates principles of human factors with pedagogy in high volume cataract surgery training.
With this in mind, we sought to find a model that puts consistency at the core of teaching. Guidelines recommend a stepwise modular approach to cataract surgical training in high volume cataract settings, aiming for 8 cases per theatre list for a trainee who is not yet able to complete a cataract operation within 20 minutes to receive supervised training and 10 cases per list for more experienced trainees who are able to consistently complete a cataract operation within 20 minutes.6 A transparent log of performance and progress should also be maintained.
Experience of Surgical Training in the Independent Sector in the UK
The authors reported results from the first regional UK study to evaluate trainees’ perception and experience of cataract surgery training in the independent sector.7 Overall, most trainees did not receive any training on managing high volume cataract lists and had inadequate or insufficient training on human factors and ergonomics, which are crucial elements in securing a safe and efficient surgical list.
Currently, ophthalmic trainees face challenges in undertaking the required number of cataract procedures, due partly to a lack of training opportunities in the independent sector. An overview of training opportunities currently available to ophthalmology trainees in the UK reported that independent sector providers operate in all 18 regions of the UK.8 Seven of these 18 regions reported trainees as being able to access cataract surgery training opportunities. Among trainees who had an opportunity to access training opportunities in the independent sector, most but not all considered the experience to be positive overall.
Human Factors Principles
Most clinicians are aware of potential safety concerns as illustrated in James Reason’s Swiss cheese model of accident causation.9–11 Preventable surgical adverse events are often linked to human factors, such as communication breakdowns, environmental factors, and operating room design. Failure to apply human factors principles is a key aspect of most adverse events in health care.12 Human factors research examines the relationship between human beings and the systems with which they interact by focusing on improving efficiency, creativity, productivity, and job satisfaction, with the goal of minimising errors.
Both James Cook University Hospital, Middlesbrough and Newmedica Eye Hospital, Middlesbrough have GMC recognition and registration for provision of cataract surgery training, with four trainee candidates enrolled to date in the independent sector. The Newmedica Eye Hospital, Middlesbrough provides services for both NHS and private patients, predominantly in high volume cataract surgery lists.
It is important from the training perspective to recognise that high volume and high turnover cataract surgeries increase the potential risk for errors or mishaps, such as never events. Implantation of an incorrect intraocular lens (IOL) leading to unplanned refractive error was noted by Kelly et al as one of the most frequent causes of litigation in ophthalmic care, the most common reason being poor patient-doctor communication.13,14 Most commonly, cataract surgery is performed under local anaesthetic, and therefore special attention to verbal communication among team members in the operative environment is needed.
Non-Technical Skills Complement Surgical Know-How and Competence in Theatre
The underlying causes of adverse events in surgery commonly originate from behavioural or non-technical aspects of performance (eg, communication failures) rather than a lack of technical expertise alone.15 Surgical training needs to focus on non-technical skills, such as team working, leadership, situation awareness, decision-making, and communication to increase the likelihood of maintaining high levels of performance over time.15
The Non-Technical Skills for Surgeons (NOTSS) system is a behavioural rating system, incorporating 4 skill categories and 12 elements.15 The NOTSS system is adapted according to the level of experience of the trainee: for junior trainees, the NOTSS system can be used for general discussion of non-technical skills and their importance to clinical practice. For more senior trainees, the NOTSS system can be used to rate skills and provide feedback during increasingly challenging cases. Towards completion of training it can also be used to help senior trainees learn how to observe and assess non-technical skills in others.
The new ophthalmic specialist training (OST) programme from the RCOphth is set to be introduced at the start of the 2024–25 training year.16 The draft cataract surgery syllabus on patient management notes that a level 4 trainee should be an effective supervisor, teacher, and trainer of cataract surgery. This includes participating in the education and training of medical students and junior trainees, and allied health professionals in cataract surgery. They should also supervise and accredit trainees to Level 3 in cataract surgery.
All data utilised in our study originate from service evaluation audits and trainee data, which do not necessitate formal ethical approval, as determined by the NHS Health Research Authority. Furthermore, the tenets of the Declaration of Helsinki protocol were diligently adhered to throughout the collection and analysis of the data.
In this article, the authors discuss their experiences and pathways of high flow cataract surgery training in the independent sector and NHS facility, that utilise the NOTSS and ICO principles, human factors and combine this with a pedagogical approach.
Methods and Results
Evaluations of Surgical Training Model
Assessment of trainees’ performance is based on the International Council of Ophthalmology’s Surgical Competency Assessment Rubric for phacoemulsification (ICO-OSCAR: phaco). This provides a key tool for both teaching and assessing competence in performing cataract surgery and specific steps of the procedure including capsulorrhexis, hydrodelineation, and IOL implantation.17
A structured comprehensive training programme was followed for the independent sector high volume list, which consists of 12 patients per session of varying complexity. Trainees are led through modular cataract training with gradual progression to more complex full cases, with regular feedback and assessment using the ICO competency assessment framework. Training on all aspects of cataract surgery, including surgical ergonomics, was incorporated.
Case Complexity in Trainee Involved High-Volume Cataract Surgery Similar in the NHS and Independent Sector
We undertook a comparative study of systemic and ocular characteristics between NHS and independent sector centre cataract patients undergoing trainee-involved cataract surgery.18 Data were collected from theatre lists across 4 weeks involving a trainee cataract surgery list in the NHS and in the independent sector on an NHS list. The consultant supervisor was the same in both cohorts (n = 37 in each cohort, with 9–12 patients per list). No statistically significant difference was found in the complexity grading between cohorts (p = 0.92). Similar levels of low and medium-risk cataracts were observed in both the NHS and independent sector cohorts, although NHS centre patients were more likely to have multiple risk factors. The study suggests that trainees can expect to face a broad and similar range of complex cases whether training in the NHS or the independent sector (Table 1).
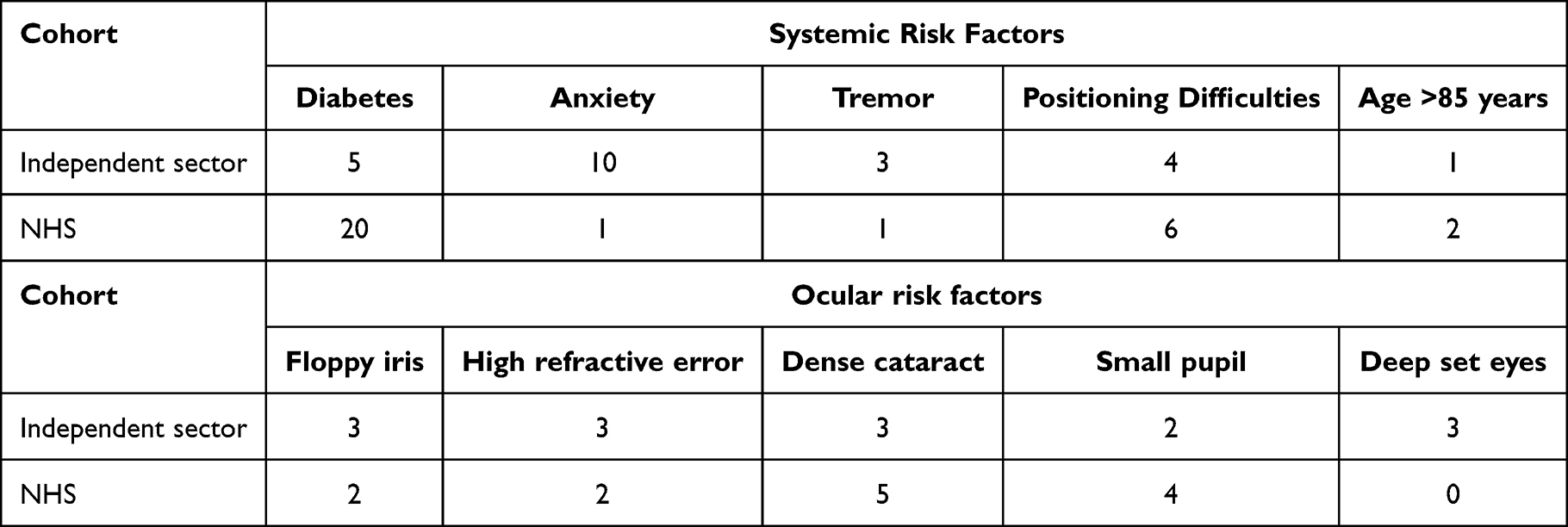 |
Table 1 Baseline Systemic and Ocular Risk Factors of Cataract Surgery Cohorts in a NHS Eye Unit and Independent Sector Centre |
A separate comparative study of outcomes amongst trainees performing cataract surgery in the independent sector and NHS showed no intraoperative and postoperative complication rates in both settings.7 Trainees gained exposure to many cases with varying complexity whilst ensuring patient safety and maintaining surgical efficiency, all comparable to NHS training lists. Anonymised patient feedback survey results, conducted immediately postoperatively for a total of 20 patients from both trainees’ lists, showed that all patients agreed that it was a positive experience.
Comparative Evaluation of Surgical Throughput in High Volume Lists
In a single-centre observational study, we evaluated surgical throughput in high volume cataract lists with mixed case complexity, comparing solo consultant lists vs surgical trainee lists carried out in the independent sector.19 Direct consultant supervision was provided with assessment on each case applying the ICO-OSCAR rubric and Gibbs’ reflective cycle.
In the anaesthetic room, only anaesthetic drops are instilled, with no mydriatic drops. The surgeon consents and marks the patient and selects the IOL. In theatre, intracameral Mydrane (Laboratoires THEA),20 a preservative-free ophthalmic combination of tropicamide 0.02%, phenylephrine 0.31%, and lidocaine 1% is injected after the initial incision is made, with pupil size measured at 30 seconds and at the end of surgery. Intraoperative data collected included pupil size 30 seconds after injection of Mydrane, pupil size at the end of surgery, intraoperative complication rate, systemic adverse effects, and pain score rated by patient (0 = no pain, 10 = maximum pain). Duration of stay at all stages of the high flow cataract surgery care pathway were recorded.
A total of 302 patients were included in the final analysis: 232 patients from the consultant lists and 70 patients from the surgical trainee lists. Demographics and clinical characteristics of patients in each study arm were generally similar. The consultant lists had a higher proportion of patients with systemic risk factors namely diabetes, whereas the trainee lists had a slightly greater proportion of patients with higher cataract grade.
Intracameral mydriasis simplifies pre-operative routines and facilitates efficient high volume cataract surgery.21 Rapid and effective mydriasis was achieved by Mydrane injection with a mean pupil size of 6.7 mm at 30 seconds. This effect was maintained in both cataract surgery lists with a mean pupil size of 6.6 mm at the end of surgery. Good intraocular anaesthesia was achieved with a mean pain score of 0.5. No intraoperative complications or systemic adverse effects were observed in both groups. All lists were completed within 4 hours, with a significant but expected difference in the mean overall patient stay between consultant list and trainee (31 mins vs 49 mins; p < 0.001). Demographics and summary results are consolidated in Table 2.
 |
Table 2 Comparative Evaluation of Surgical Throughput in Consultant and Trainee High Volume Cataract Lists: Baseline Demographics and Clinical Characteristics, Intraoperative Outcomes, and Patient Duration of Stay During Pathway |
Successful training was delivered with excellent results on length of patient stay, patient experience, and complication rates, all of which were comparable to results observed for a solo consultant high volume list. Overall, the study demonstrated an efficient and safe model for training ophthalmology trainees on high volume cataract surgeries.
Discussion
Overview of Training Model
We implemented the Royal College of Surgeons Edinburgh NOTSS module into the surgical training programme. The trainee was asked to complete the NOTSS e-learning course. This was further complemented by the trainer and trainee’s discussion around non-technical skills in different scenarios. This was documented as a part of the trainee’s continuous professional development.
Over the 8-week modular surgical training programme (Box 1), there was a gradual increase in the number of cases operated, depending on the complexity of case mix. Complexity of case mix increased as case experience increased, involving patients with small pupils, brunescent cataract, white cataract, posterior polar, high myope, shallow anterior chamber, phacodonesis, difficult position, or a combination of these. The surgical trainee assisted with use of different surgical materials, instruments, and devices. Over 3 months, the number of supervised trainee operated cases increased progressively. Total ICO-OSCAR competency score in performing cataract surgery, reflecting intraoperative technical skill, progressed steadily in conjunction with case experience.
 |
Box 1 Outline of Eight-Week Modular Cataract Surgical Training Schedule |
Trainees had previous experience in hands-on cataract surgery and simulation, all trainees had less than the required surgical numbers for cataract surgery. Our projects included trainees of various levels, two ST3 Level, one ST4, and one ST6.
As the trainee progressed through each week, every step was repeated in each successive case so that there was a sequential learning pattern. This cyclical nature reinforced the Gibbs’ reflective cycle as each step was reflected upon (Figure 1).22
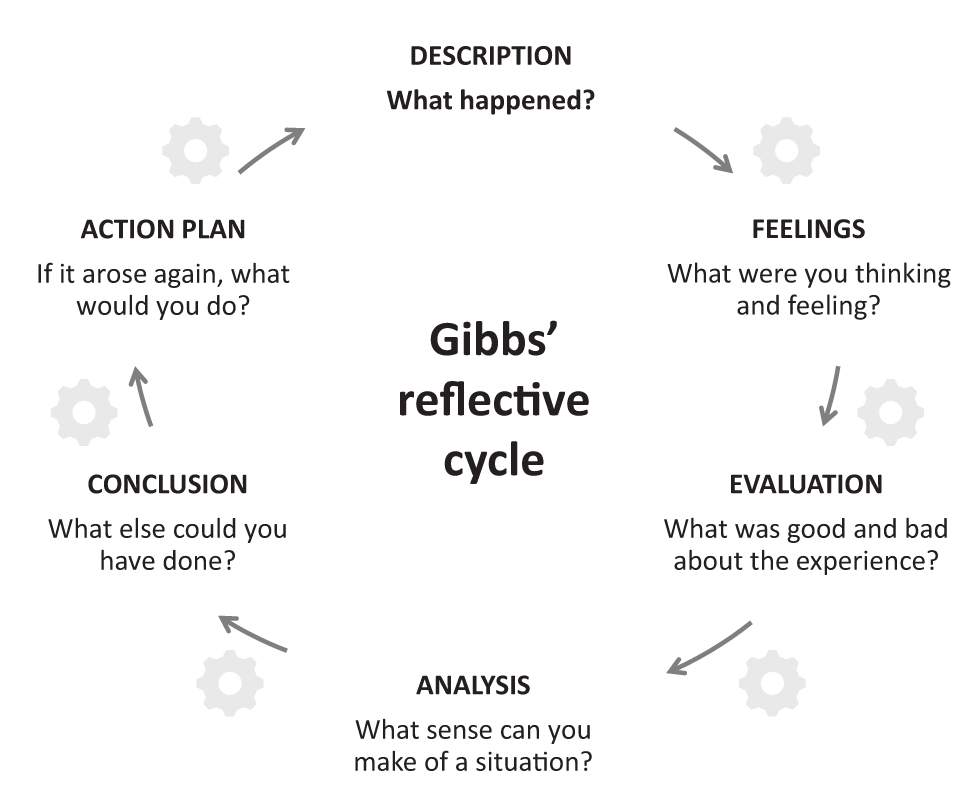 |
Figure 1 Schematic illustration of Gibbs’ reflective cycle. Notes: Adapted from Gibbs G. Learning by doing; a guide to teaching and learning methods. London: Further Education Unit, Oxford Polytechnic; 1988. Creative Commons.22 |
Cataract Audit of Vision Outcomes
A surgical trainee undertook a total of 98 phaco cases over a period of 5 months. Of these, 58 patients were included in an audit of vision outcomes, with other patients excluded due to lack of postoperative vision/refractive outcomes, typically second eye patients involving telephone follow-up. Visual acuity was better than 6/12 in most patients (98%, 55/58). All patients with vision worse than 6/12 had pre-existing ocular comorbidities, such as age-related macular degeneration. Most patients (94%) had spherical equivalent <1 dioptre from the refractive aim. There were no cases of intra-operative and post-operative complications.
Licensed doctors are expected to seek feedback from patients to help inform their future development. Patient feedback surveys involving a 10-item questionnaire following trainee-involved cataract surgery were collected over a period of 3 weeks and were conducted immediately after surgery in the recovery area. Of nineteen responses collected in total, 89% said that they did not feel significant pain during surgery and the majority agreed that they would be happy to be treated by the same doctor again, reflecting that the training model worked well.
Trainer Perspective
Providing effective training in high volume lists is dependent on securing surgical efficiency in a safe environment. A systematic training protocol is essential to minimise the risk of avoidable errors and patient harm. This builds on a comprehensive training programme covering all aspects of cataract surgery: human factors training, phacodynamics, and instrument knowledge, and biometry. Intensive modular cataract training is provided to perfect each step, combined with exposure to a wide variety of case scenarios. Regular feedback and assessment form an integral part of surgical training and learning, underpinned by application of the ICO-OSCAR competency framework, video presentations, and small group discussions. Ongoing audit of outcomes, safety, and efficiency provides essential benchmarking of performance and results.
Sufficient staffing, preoperative briefing, precise planning, and the ethos of surgery ergonomics play a pivotal role in the seamless completion of high-volume cataract lists without complications. Overall, good communication and a good skill mix amongst the multidisciplinary team assures a smooth-running process for all patients. Comparative evaluations confirm that regular high-volume lists are highly cost effective, reduce waiting times, and facilitate surgical teaching in a stepwise, modular manner.
Our findings demonstrated an efficient and safe model for training of ophthalmology trainees in high volume cataract surgeries, can be adopted in NHS eye units and independent sector centres. Study results, supported by clinical experience, show that use of a standardised intracameral combination of mydriatics and anaesthetic in high volume training lists induces rapid, intense, and stable mydriasis during cataract surgery with minimal systemic side effects. This has resulted in successful training being delivered with excellent results on patient length of stay, patient experience, and complication rates, all of which were comparable to those observed for a solo consultant high volume list.
The reported audits involved operative performance assessments that were rigorous and comparative but were nonetheless limited by single consultant surgeon oversight.
QM Model for Cataract Training
Our work to date inspired us to propose a model of teaching that encapsulates our research and incorporates integral aspects of training from the ICO-OSCAR framework and the new ophthalmic specialist training Curriculum 2024. Each of the trainees was trained using a pedagogical approach that involved reflection and experiential learning, specifically the Gibbs’ reflective cycle (Figure 1). This model uses cyclical reflection, which in turn provides a structural framework for learning experiences. It encourages the learner to critically analyse the learning experience and transform this into a valuable learning opportunity. The cyclical nature of this method of pedagogy was suitable for trainees in cataract surgery as the weekly surgical steps were repeated for every patient on the list for that week, performance was then critically analysed subsequently providing a platform for constructive feedback, enabling trainees to enhance their competencies and skills preparing for real-life situations when they operate independently.
Experiential learning supports performance improvement, learning, and development and we felt it was the ideal educational theory to align our surgical teaching framework with. This method of meaningful learning ensures that the learner takes an active role in understanding and applying the concepts that are being taught. It requires that the learner, in our case the trainee, utilises new knowledge and processes it in a cognitive manner which is both constructive and enduring.
Limitations
It would be helpful to carry out large-scale projects similar to ours so that meaningful statistical data can be extracted and analysed to improve the generalisability. We recognise that the projects were supervised by a single consultant, and so we recommend that future projects could encapsulate wider involvement to assess any discrepancies. Future projects could also include visual acuity outcomes, these were not included in our studies as we focused on teaching methodology.
Conclusion
With this in mind, we propose the QM Model for cataract training that captures all key elements necessary for trainee surgeons to be taught in a structured, modular manner where both the trainee and educator share responsibilities in the learning experience (Figure 2). The model is based on the ICO principles and the RCOphth curriculum where the trainee is introduced to the modular training mentioned above. Every week, the trainee uses Gibbs’ cycle of reflective learning to master the skill required. This is discussed with the educator and an action plan devised before the next set of skills are acquired. This positive reinforcement ensures that the concrete experience of learning and abstract conceptualisation provided meaningful value that was converted into active experimentation to further reinforce the learning experience. The authors propose that the QM Model for cataract training is suitable for utilisation in all surgical centres in the NHS and independent sector settings for both low volume and high volume surgical lists across all trainee grades.
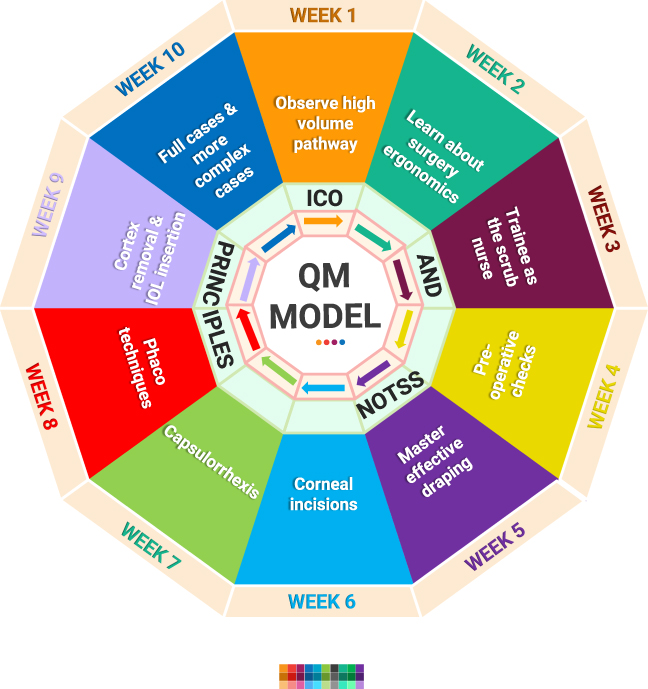 |
Figure 2 QM Model for Cataract Training. Abbreviations: ICO, International Council of Ophthalmology; IOL, intraocular lens; NOTSS, Non-Technical Skills for Surgeons; QM, Qasim Mansoor. |
Acknowledgments
The authors gratefully acknowledge third-party editorial assistance provided by Rod McNeil Associates, which was funded by Thea Pharmaceuticals Ltd.
Disclosure
Dr Qasim Mansoor is a consultant advisor for Thea Pharmaceuticals, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. The Royal College of Ophthalmologists. Cataract hubs and high flow cataract lists. Ophthalmic Services Document; 2021: Available from: https://www.rcophth.ac.uk/wp-content/uploads/2021/09/Cataract-Hubs-and-High-Flow-Cataract-Lists.pdf.
2. The Royal College of Ophthalmologists. High flow cataract surgery. Ophthalmic Service Document. Version 2.0: VS January; 2022: Available from: https://www.rcophth.ac.uk/wp-content/uploads/2022/02/High-Flow-Cataract-Surgery_V2.pdf.
3. General Medical Council. National training survey 2022 results; 2022: Available from: https://www.gmc-uk.org/-/media/documents/national-training-survey-summary-report-2022-final_pdf-91826501.pdf.
4. The Royal College of Ophthalmologists. RCOphth survey of ophthalmologists in training in 2020. Available from: https://www.rcophth.ac.uk/news-views/gmc-report-highlights-pressure-on-ophthalmologists-in-training/.
5. The Royal College of Ophthalmologists. Training guidance. Blueprint for cataract training in the independent sector: guidance for providers and trainers; 2022. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2022/10/Blueprint-for-cataract-training-2022_v2.pdf.
6. The Royal College of Ophthalmologists. Training Guidance. Cataract surgical training in high volume cataract settings; 2021. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2021/12/Cataract-Surgical-Training-in-High-Volume-Cataract-Settings.pdf.
7. Chen Y, Crothers O, Ting D, et al. Outcomes of cataract surgery training amongst trainees between NHS and independent sector: a comparative study.
8. Ophthalmologists Training Group. The current state of cataract surgery training in the independent sector. Eye. 2023;2023:1.
9. Reason J. Safety in the operating theatre - Part 2: human error and organisational failure. Qual Saf Health Care. 2005;14(1):56–60.
10. Reason J. The contribution of latent human failures to the breakdown of complex systems. Philos Trans R Soc Lond B Biol Sci. 1990;327(1241):475–484.
11. Suliburk JW, Buck QM, Pirko CJ, et al. Analysis of human performance deficiencies associated with surgical adverse events. JAMA Network Open. 2019;2(7):e198067. doi:10.1001/jamanetworkopen.2019.8067
12. Urban D, Burian BK, Patel K, et al. Surgical teams’ attitudes about surgical safety and the surgical safety checklist at 10 years: a multinational survey. Ann Surg Open. 2021;2(3):e075. doi:10.1097/AS9.0000000000000075
13. Kelly SP, Steeples LR, Smith R, et al. Surgical checklist for cataract surgery: progress with the initiative by the royal college of ophthalmologists to improve patient safety. Eye. 2013;27(7):878–882. doi:10.1038/eye.2013.101
14. The Royal College of Ophthalmologists. Correct IOL implantation in cataract surgery. Quality Standard; 2018. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2021/12/Correct-IOL-implantation-in-cataract-surgery-quality-standard-1.pdf.
15. The Royal College of Surgeons of Edinburgh. The Non-Technical Skills for Surgeons (NOTSS) System Handbook v2.0. Available from: https://www.rcsed.ac.uk/media/682516/notss-system-handbook-v20.pdf.
16. The Royal College of Ophthalmologists. Postgraduate medical training. Cataract surgery syllabus: patient management domain. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2021/12/Cataract-Surgery-syllabus.pdf.
17. Golnik KC, Beaver H, Gauba V, et al. Cataract surgical skill assessment. Ophthalmology. 2011;118(2):427.e1–5. doi:10.1016/j.ophtha.2010.09.023
18. Crothers O, Jacob DA, Qurashi N, et al. Comparison of patients systemic and ocular characteristics between NHS & Independent sector (independent sector) in the trainee involved high-volume cataract surgery.
19. Chen Y, Ting D, Mansoor Q. Improving the surgical efficiency and throughput of high volume cataract training lists with the use of intracameral Mydrane.
20. Thea Pharmaceuticals, Mydrane Patient Information; 2023. Available from: https://www.thea-pharmaceuticals.co.uk/products/mydrane.
21. Intracameral Mydrane (ICMA) and Ethics Group, Chiambaretta F, Pleyer U, Behndig A, et al. Pupil dilation dynamics with an intracameral fixed combination of mydriatics and anesthetic during cataract surgery. J Cataract Refract Surg. 2018;44(3):341–347. doi:10.1016/j.jcrs.2017.12.025
22. Gibbs G. Learning by Doing; a Guide to Teaching and Learning Methods. London: Further Education Unit, Oxford Polytechnic; 1988.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Paramedics Satisfaction with Simulation Experience for Career Development and Skills Maintenance
Alshibani A, Alburaidi AS, Alsukait MA, Albadr R, Alsubaie BK, Almutairi A, Almutairi S, AlHussaini Z
Advances in Medical Education and Practice 2025, 16:245-253
Published Date: 19 February 2025
Impact of Simulation-Based Surgical Training in Laparoscopy on Satisfaction Level and Proficiency in Surgical Skills
Mukhtar F, Shaheen MF, Alhabeeb AY, Zafar M, Alkattan K
Advances in Medical Education and Practice 2025, 16:357-366
Published Date: 27 February 2025
Pulmonary and Critical Care Medicine Trainees’ Educational Experiences and Well-Being During the COVID-19 Pandemic
Murali S, Velapati SR, Kaul P, Cohen RI
Advances in Medical Education and Practice 2025, 16:1717-1730
Published Date: 24 September 2025
Exposure to and Comfort with Toric and Presbyopia-Correcting Intraocular Lenses: A Survey of Ophthalmology Residents
Devireddy N, Scruggs K, Lehman E, Longenecker A, Pantanelli SM
Clinical Ophthalmology 2026, 20:615011
Published Date: 9 July 2026