Back to Journals » Journal of Pain Research » Volume 19
Exploring the Influence of Testosterone on Pain Perception and Modulation Among Men with Low and Normal Testosterone Concentrations
Authors Vincenot M ![]() , Bordeleau M, le Blanc F
, Bordeleau M, le Blanc F ![]() , Pagé C, Gaumond I
, Pagé C, Gaumond I ![]() , Léonard G
, Léonard G ![]() , Marchand S
, Marchand S
Received 4 November 2025
Accepted for publication 16 February 2026
Published 27 March 2026 Volume 2026:19 571741
DOI https://doi.org/10.2147/JPR.S571741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Wendy Imlach
Matthieu Vincenot,1,2,* Martine Bordeleau,1,2,* Flore le Blanc,1,2 Catherine Pagé,1 Isabelle Gaumond,3 Guillaume Léonard,1,2 Serge Marchand4
1Research Centre on Aging, Centre intégré universitaire de santé et de services sociaux de l’Estrie - Centre hospitalier universitaire de Sherbrooke, Sherbrooke, QC, Canada; 2School of Rehabilitation, Faculty of Medicine and Health Sciences, Université de Sherbrooke, Sherbrooke, QC, Canada; 3Department of Medicine, Faculty of Medicine and Health Sciences, Université de Sherbrooke, Sherbrooke, QC, Canada; 4Department of Surgery, Faculty of Medicine and Health Sciences, Université de Sherbrooke, Sherbrooke, QC, Canada
*These authors contributed equally to this work
Correspondence: Guillaume Léonard, Research Centre on Aging, Centre intégré universitaire de santé et de services sociaux de l’Estrie - Centre hospitalier universitaire de Sherbrooke, School of Rehabilitation, Faculty of Medicine and Health Sciences, Université de Sherbrooke, 1036 rue Belvédère Sud, Sherbrooke, QC, J1H4C4, Canada, Email [email protected] Serge Marchand, Department of Surgery, Faculty of Medicine and Health Sciences, Université de Sherbrooke, 3001 12e Avenue Nord, Sherbrooke, QC, J1H5H3, Canada, Email [email protected]
Background: Pain perception varies considerably between individuals, with sex differences likely contributing to this variability. These differences appear to involve multiple factors, including sex hormones, although the underlying mechanisms of modulation remain unclear.
Purpose: To explore how variations in free testosterone influence pain perception and modulation mechanisms in men.
Patients and Methods: A non-probabilistic convenience sampling was used to recruit a total of 12 men with low testosterone and 16 controls for this cross-sectional experimental study. Pain sensitivity was evaluated via heat pain threshold (HPT) and heat pain tolerance (HPTol) using a contact thermode placed on the left forearm. Pain modulation was assessed through conditioned pain modulation (CPM) responses using a counter-irritation protocol with heat pain stimulation as test stimuli applied before and after a cold pressor test serving as the conditioning stimulus. Temporal summation of pain (TSP) was assessed using 2 minutes constant heat pain stimulation.
Results: Pain perception (HPT and HPTol) was significantly lower in low testosterone compared to controls (p = 0.02). Free testosterone levels were positively correlated with HPTol (r = 0.40, p = 0.03). Pain modulation responses were similar in low-testosterone and those in the control group. No significant between-groups differences were observed for CPM and TSP responses (all p > 0.90).
Conclusion: Control men showed lower pain sensitivity than low-testosterone participants, supporting an antinociceptive effect of testosterone that may partly contribute to sex differences in pain.
Keywords: pain perception, pain threshold, pain modulation, conditioned pain modulation, temporal summation, sex hormones, testosterone, men
Introduction
Testosterone is an androgen sex hormone involved in multiple physiological systems, including pain processing, where it is thought to exert a modulatory effect.1 Evidence from animal models suggests that testosterone generally has antinociceptive effects, influencing both pain perception and pain-related behaviors.2–8 For instance, it could be observed that diminished testosterone levels post-gonadectomy in male rats was associated with increased nociceptive responses, whereas testosterone administration in female rats led to reduced nociceptive responses.3,8,9
Conversely, in humans, study findings are less consistent and sometimes conflicting.8 While some investigations support the antinociceptive role of testosterone observed in animal models – reporting, for example, significant positive correlations between free testosterone levels and thermal pain thresholds10–13 – others have found no such association.14 Moreover, recent placebo-controlled data suggest that exogenous testosterone administration in healthy men may paradoxically increase pain perception during exposure to painful electric stimuli,1 further highlighting the complexity of testosterone’s role in pain processing.
A better understanding of the impact of testosterone on endogenous pain modulation mechanisms could potentially shed some light on these contradictory findings. These mechanisms can be assessed non-invasively in humans, notably through the evaluation of temporal summation of pain (TSP), reflecting excitatory processes,15 and conditioned pain modulation (CPM), reflecting inhibitory control.16 Scientific evidence suggests that human men typically exhibit more efficient inhibitory pain mechanisms and lower temporal summation than women.17 These differences suggest that testosterone, the predominant sex hormone in men, may play a role in modulating these mechanisms. However, few studies have directly examined the relationship between testosterone levels and specific pain modulation processes in humans.8
A study conducted by Rezaii and colleagues18 examined CPM responses during the early follicular phase in healthy women, and found no association between CPM effects and salivary testosterone levels. In contrast, a neuroimaging study conducted in women with low testosterone levels showed that activity in two major areas involved in descending pain modulation (rostral ventromedial medulla and periaqueductal gray) was significantly reduced compared to a group of women with normal testosterone levels.13 These results highlight a potential link between testosterone and pain modulation; however, despite these areas being involved in pain modulation, it is not possible to directly infer a causal relationship between the PAG and RVM and the psychophysical response of CPMs as this study did not assess CPM. To this effect, a recent study conducted by Vollert and colleagues19 showed that plasma testosterone levels explain a negligible level (around 5%) of variance in the CPM response in healthy individuals.
Taken together, these findings point to the potential but inconsistent role of testosterone in pain modulation and emphasize the difficulty with which generalizations about the role of testosterone in human pain responses can be made. Notably, to the best of our knowledge, no study has focused on comparing healthy men with men presenting low testosterone concentration. Most studies have compared men and women or women alone, the latter in whom other sex hormones may influence pain assessment. The comparison with a group of men with lower testosterone concentration therefore represents an interesting model in this regard. Furthermore, excitatory mechanisms, such as TSP, remain largely unexplored in the context of testosterone levels. Hence, the objective of this study was to evaluate the influence of testosterone concentration on pain perception and modulation by comparing men with lower testosterone levels to male control participants using standardized quantitative sensory testing (QST), including TSP and CPM protocols. We hypothesize that low testosterone men would be more likely to demonstrate a pro-nociceptive profile (lower pain and tolerance thresholds, greater TSP and enhanced CPM) compared to controls, and that testosterone levels would be associated with pain perception and modulation.
Materials and Methods
Participants
The experiments were conducted between 2009 and 2010 at the Centre de recherche du Centre hospitalier universitaire de Sherbrooke (Sherbrooke, Quebec, Canada). This study adhered to the Helsinki Declaration. Ethics approval was granted by the institutional review board of the Centre intégré universitaire de santé et de services sociaux de l’Estrie – Centre hospitalier universitaire de Sherbrooke, Sherbrooke, Canada (project #09-024). Informed consent was obtained from all participants prior to all experimental procedures. This cross-sectional study involved healthy men aged between 45 and 65 years with normal or low testosterone levels. The study consisted of a single experimental session lasting approximately 90 minutes. Exclusion criteria were as follow: (1) use of antidepressants or other drugs with an action on autonomic nervous system activities ; (2) use of anticoagulants; (3) presence of chronic pain; (4) presence of carcinoma of the prostate or breast; (5) presence of edema or cardiac, hepatic or renal insufficiency, or (6) presence of sleep apnea. A non-probabilistic convenience sampling strategy was used.
Questionnaires
In order to ensure that the two groups were comparable, a number of psychological characteristics were measured. Height and weight were measured to estimate the body mass index. Psychological functioning was assessed using a series of questionnaires including the validated French versions of the Beck Depression Inventory (BDI),20 the Social Readjustment Rating Scale (SRRS)21 and the State-Trait Anxiety Inventory – Forms Y1 and Y2 (STAI-Y1/Y2),22 measuring depression, stress and anxiety symptoms, respectively.
Dosage of Sex Hormones
A venous blood sample was collected at the beginning of the experimental session and placed in serum separator tubes. Blood collection tubes were immediately refrigerated at 4°C for one hour, and centrifuged (1500 rpm, 4 °C) for 10 minutes. The serum collected was then transferred into aliquots, and frozen at −80 °C. Serum levels of free testosterone were analyzed using competitive chemiluminescent methods (Siemens Medical Solutions Diagnostics, Los Angeles, CA) by the biochemistry and hematology laboratories of the Centre hospitalier universitaire de Sherbrooke. Low testosterone was defined as a concentration falling at least one standard deviation below the control group mean,13 corresponding to values below 217 pmol/L (control mean mean = 305 pmol/L; SD = 88 pmol/L). To ensure that potential between-group differences were not due to other hormones, we also analyzed the concentrations of estradiol, hormone-binding globulin, dehydroepiandrosterone sulphate (DHEA), follicle-stimulating hormone, luteinizing hormone and cortisol.
Experimental Pain Procedure
The experimental pain procedure was split into different steps. First, pain perception and pain tolerance thresholds were evaluated. Then, to assess pain modulation mechanisms, three thermal stimulations were administered: two identical test stimuli applied by a heating plate before and after a cold-water bath (cold pressor test; CPT) serving as the conditioning stimulus. Detailed descriptions of each procedure are provided in the following subsections, and Figure 1 presents an overview of the experimental protocol.
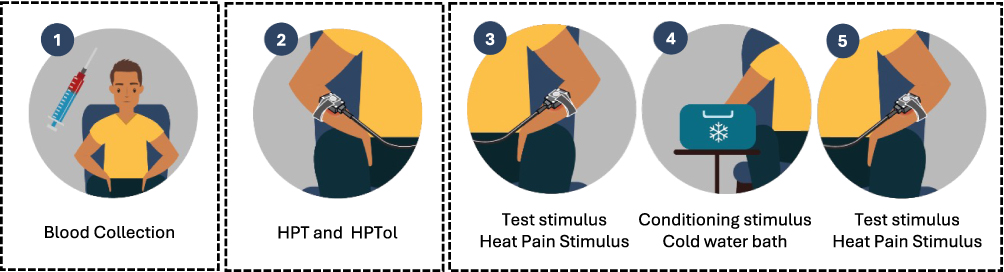 |
Figure 1 Timeline of the experimental procedure. |
Pain Assessment
Pain perception was assessed throughout the experimental procedure using a computerized visual analogue scale (CoVAS, Medoc, Ramat Yishai, Israel). CoVAS offers a computerized, real-time, continuous visual analogue scale (VAS) evaluation ranging from 0 (absolutely no pain) to 100 (worst pain imaginable).
Heat Pain Threshold and Tolerance
Heat pain threshold (HPT) and heat pain tolerance (HPTol) were assessed with a continuous thermal stimulation applied on the right-side anterior forearm using a 3cm2 thermode (TSA II, Thermal Sensory Analyzer, Medoc, Ramat Yishai, Israel). The temperature was gradually increased from a baseline temperature of 32°C to a maximum of 51°C, at a rate of 0.3°C/s. This procedure23,24 was carried out twice: participants indicated the moment at which they experienced the very first sensation of pain (heat pain threshold, CoVAS score > 0/100) and the moment when pain was no longer tolerable (heat pain tolerance threshold, CoVAS score = 100/100). Using individuals’ pain perception recordings with the CoVAS, we extracted the average pain-inducing temperature of 50/100 (target temperature) for each participant, which was later used in the pain modulation assessment procedure described below.
Pain Modulation
After a 10-minute rest period following the heat threshold determination procedure, pain modulation mechanisms were evaluated using a counter-irritation paradigm involving a test stimulus performed before and after a conditioning stimulus following the protocol developed by Tousignant-Laflamme and colleagues.25–27 The test stimulus (a 2-minute tonic pain test) was performed on the left-side anterior forearm. After a constant rise (0.3 °C/sec) from baseline (32 °C) to the individually predetermined temperature (target temperature), the temperature remained constant throughout 120s. To avoid generating an expectation effect and bias in pain ratings, participants were advised that the temperature was controlled by the computer setup and could vary randomly. Participants were instructed to evaluate their pain level with the CoVAS during the 2-minute test. This first test gave us two parameters: the first was the temporal summation amplitude, calculated by measuring the difference in pain perception between the beginning of the stimulation (when the thermode reached the target temperature) and the end of stimulation (ie at 120 seconds). The second parameter was the baseline perception level of pain based on the average pain perception throughout the stimulation, which was used to calculate the effect of CPM.
Immediately after the test stimulus, participants were subjected to a CPT (conditioning stimulus) inducing a heavy and sustained pain sensation to trigger top-down inhibitory mechanisms. Participants were asked to immerse their right arm (up to their elbow) in cold water maintained at 10 °C for 2 minutes. Pain ratings were assessed every 15 seconds with a verbal numeric rating scale (NRS). To measure CPM amplitude, a second identical test stimulus was performed with the thermode on the left forearm, immediately after the CPT. The CPM amplitude was measured by the difference in pain intensity before and after the CPT. A negative score, indicating a reduction in pain perception following the CPT was interpreted as an efficient CPM response.
Statistical Analyses
Descriptive analyses were performed to illustrate the sample characteristics. Normality test and visual inspection did not support the assumption of normally distributed data. Consequently, Mann–Whitney tests were applied to compare pain perception and modulation responses between men with low testosterone and controls. Spearman correlation analyses were also performed to examine the associations between free testosterone concentration (as a continuous variable) and pain threshold and modulation responses. A p-value < 0.05 was considered statistically significant. All tests were performed using Prism 10 (version 10, GraphPad Software, Boston, Massachusetts USA).
Results
Characteristics of the Participants
Twenty-eight male participants were recruited. Twelve individuals were classified as low testosterone, while the remaining 16 were classified as controls, ensuring 82% statistical power with an alpha level of 0.05 (based on HPT as primary outcome). Clinical, biochemical, and psychophysical characteristics of the participants are presented in Table 1. Age, body mass index, resting heart rate, and emotional functioning (depression, anxiety and stress symptoms) were comparable between the 2 groups. The concentrations of other hormones are presented in Table S1. Only estradiol appeared significantly different between the two groups and additional analysis was conducted for this purpose (see results section).
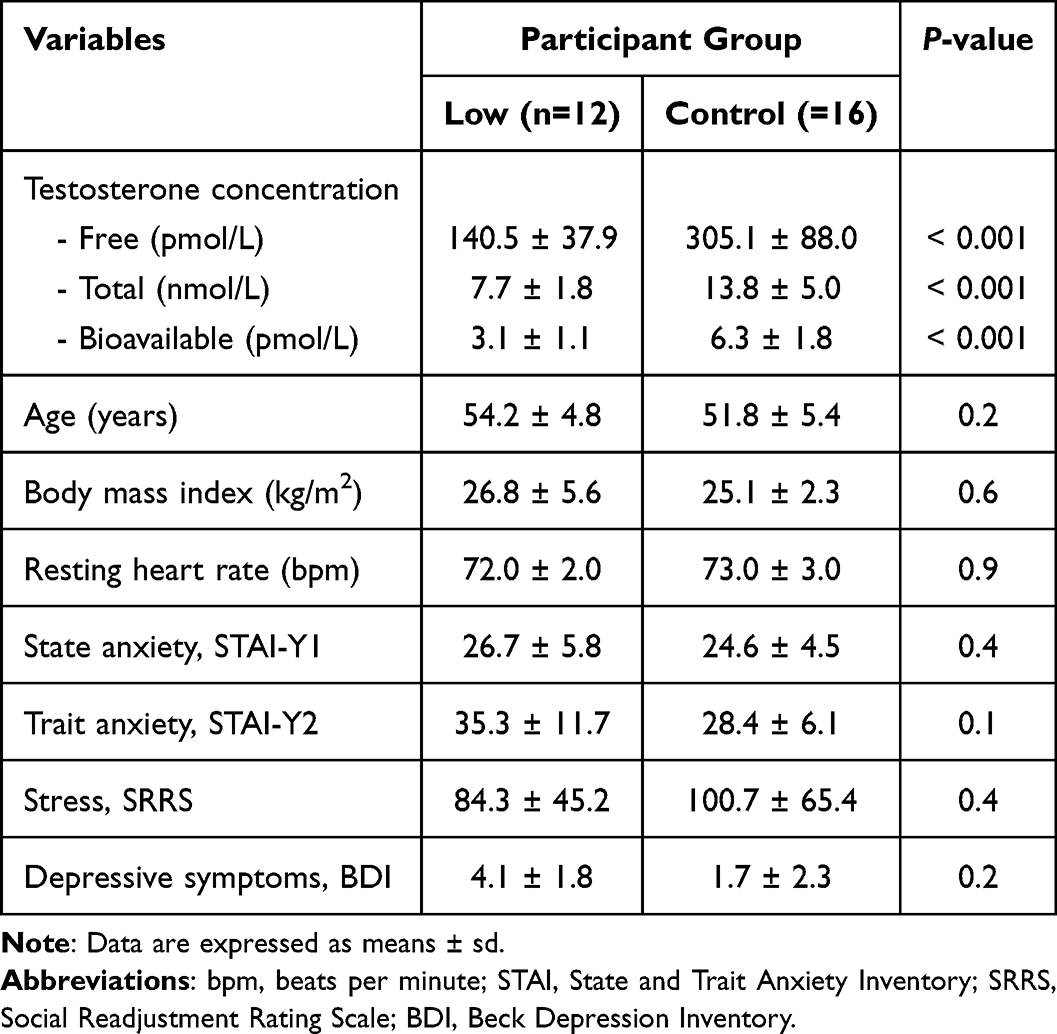 |
Table 1 Characteristics of the Participants |
Baseline Thermode Measures and Immersion-Induced Pain
Means and standard deviations for pain perception before, during and after the CPT are presented in Table 2. Whether before, during or after the CPT, the control group tended to report lower pain intensity than the low testosterone group; however, these differences were not statistically significant (all p-values > 0.3).
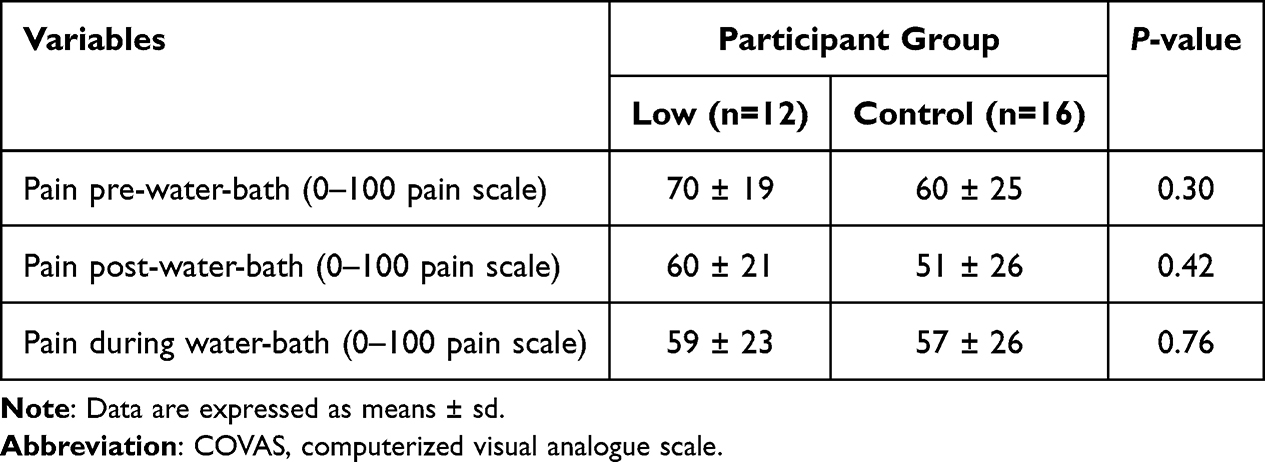 |
Table 2 Pain Perception COVAS Scores During Tests and Conditioning Stimuli |
Heat Pain Threshold and Tolerance
Mann–Whitney tests revealed that low testosterone men had statistically lower HPT (Figure 2A) and HPTol (Figure 2B) compared to controls (all p-values < 0.05). Spearman correlation analyses revealed a trend correlation between HPT and free testosterone (p = 0.08, Figure 3A) and a positive correlation between HPTol and free testosterone levels (p = 0.03, Figure 3B). Correlation analyses considering total and bioavailable testosterone concentrations appeared relatively similar to those for free testosterone (see Table S2). Given that the concentration of estradiol differed between the two groups, we performed correlation analyses between estradiol concentration and pain outcomes; none of these correlations were statistically significant (all p values ≥ 0.2) (see Table S3).
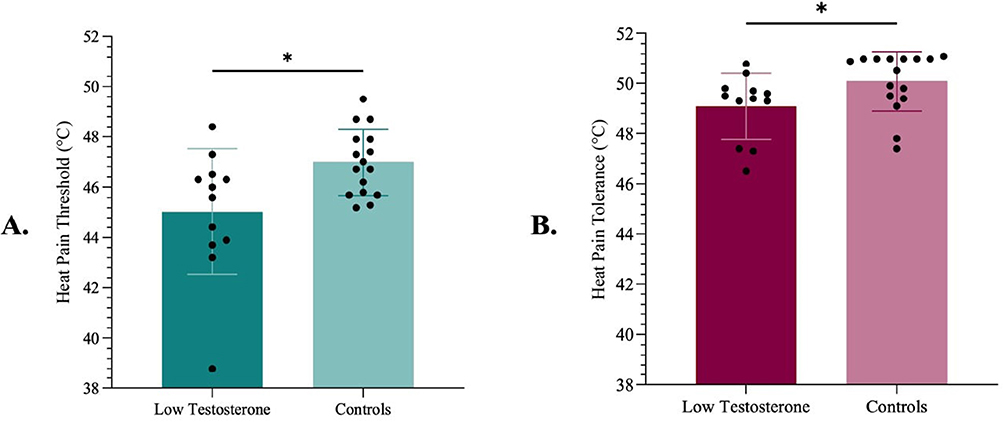 |
Figure 2 Difference in pain perception between the low testosterone group and controls. (A) Pain perception threshold. (B) Pain tolerance threshold. *Indicates a statistically significant difference. |
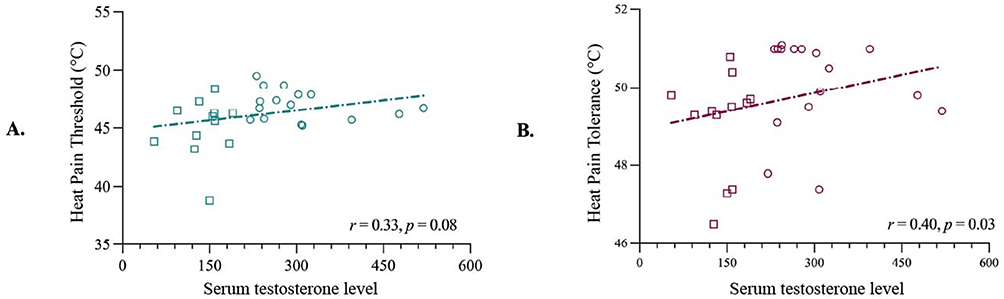 |
Figure 3 Correlation analysis between testosterone concentrations and pain thresholds. (A) Pain perception threshold. (B) Pain tolerance threshold. |
Temporal Summation and Conditioned Pain Modulation
As presented in Table 3, neither the TSP nor the CPM effects were statistically different between the two groups, and no correlations were found between testosterone concentration and TSP/CPM (all p values > 0.6). Furthermore, no correlation was found between TSP or CPM measures and total or bioavailable testosterone concentrations (see Table S2), nor estradiol levels (all p values ≥ 0.2) (see Table S3).
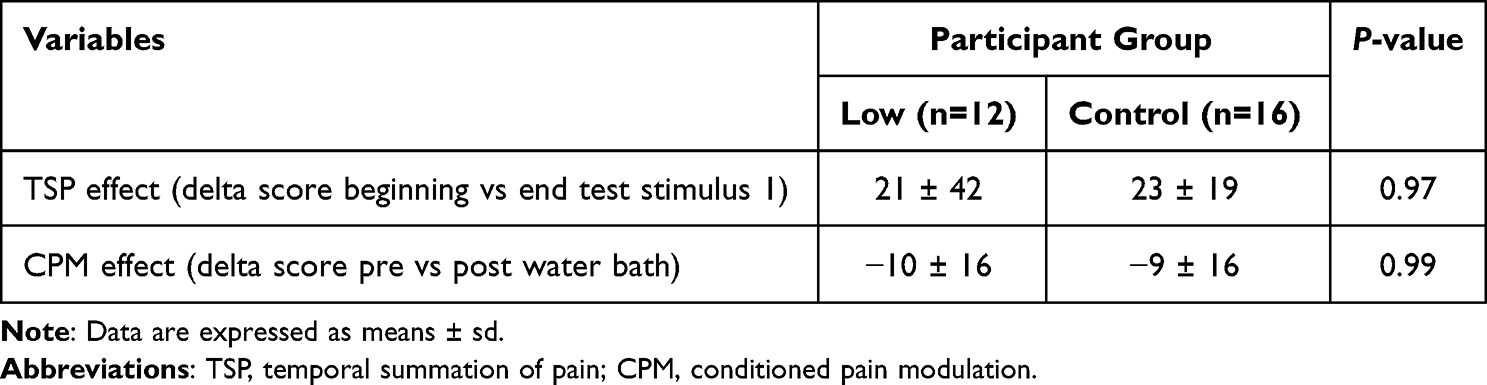 |
Table 3 TSP and CPM Amplitude for Both Groups |
Discussion
This study aimed to investigate how testosterone levels affect pain processing by comparing sensory thresholds (HPT and HPTol) and modulatory responses (TSP and CPM) between men with low testosterone and male control participants. Our results suggest that men with lower testosterone levels exhibit reduced HPT and HPTol. Notably, a positive relationship was observed between free testosterone level and HPTol, suggesting that higher testosterone levels may be associated with greater tolerance to heat pain. A similar trend was noted between testosterone levels and HPT of participants.
Past research using rodent models has shown that castrated rats exhibit increased sensitivity to nociceptive stimuli compared to the non-castrated control group in different pain experimental context.2,3,28–30 Altogether, these studies suggest a protective role of testosterone on pain perception.
In human studies, a recent investigation in the context of heat pain conducted in a cohort of 88 healthy participants found no correlation between HPT and free testosterone concentrations in either men or women.14 However, in this study, testosterone levels were measured using salivary samples. Although salivary testosterone assays are less invasive and easier to collect, they are more sensitive to external factors that can influence the validity of the measurements.31 Other studies have reported a positive correlation between salivary testosterone concentration and electrical pain threshold,11 as well as between serum testosterone concentration and heat- and cold-10 pain thresholds, aligning with our findings and suggesting a protective role of testosterone.
In the context of continuous thermal stimulation, a study by Choi et al using a 30-second finger immersion test in 50°C water found that men with low testosterone levels reported greater pain compared to those with higher levels.32 These findings are partially consistent with our results, as both studies indicate that lower testosterone concentrations are associated with increased sensitivity to thermal stimulation. However, unlike Choi et al, our study did not reveal any group-level differences for tonic pain measures, likely due to differences in stimulation protocols. The younger age of participants in Choi’s study (around 23 years) compared to our sample (mean age 53) could also partly explain the discrepancies, as previous research suggests that age may influence thermal perception thresholds,33,34 although this remains a subject of debate.35
No differences in pain modulation were observed between our two groups for either TSP (excitatory) or CPM (inhibitory) responses. Few studies have examined the influence of testosterone on CPM responses. One study by Vollert and colleagues19 found no association between testosterone levels and CPM magnitude when using a sequential protocol (ie the second test stimulus applied after the conditioning stimulus) mirroring our methodology and supporting our results. Surprisingly, this relationship reached statistical significance when CPM was assessed by Vollert and colleagues under a parallel protocol (ie where the conditioning and test stimuli were delivered concurrently to the conditioning stimulus) with testosterone accounting for around 6% of the variance.19 The way in which CPMs are induced and measured therefore seems to be an important factor to consider.36 It should also be noted that Vollert and colleagues collected blood samples immediately after the CPM protocol, rather than beforehand, as in our study – a difference in timing that may influence the results.
Concerning TSP, the current body of literature remains too limited to draw firm conclusions about the influence of testosterone on excitatory pain modulation response. A recent study conducted by our team found that testosterone level did not predict the amplitude of TSP in a large cohort of chronic pain and healthy individuals, further suggesting that TSP is not associated with testosterone.23 Clearly, further research is needed to clarify the potential role of testosterone in excitatory pain mechanisms. Besides sex hormones, various factors such as pain catastrophizing are thought to influence pain sensitivity and pain modulation.16,37
Although our results show a more obvious effect of testosterone on pain perception compared to pain modulation, its effect on the brain structures involved in pain processing remains to be clarified. A recent electroencephalography study demonstrated that testosterone administration, compared to a placebo, was associated with increased pain ratings and greater N1 component amplitudes in response to both nociceptive and non-nociceptive stimuli, suggesting that testosterone may broadly affect sensory processing beyond pain-specific mechanisms.1 Another study conducted by Stanton et al (2009) found that individuals with higher testosterone levels showed increased ventromedial prefrontal cortex (vmPFC) activity in response to threat-related stimuli.38 These findings laid the groundwork for the investigation of the relationship between testosterone levels and pain processing given that pain is processed as a form of threat.39 In another study, Girard-Tremblay et al (2014) demonstrated that, in a matched pain perception paradigm where painful stimulus intensity was equal among participants, men who reported the highest subjective levels of pain also exhibited significant deactivation of the vmPFC.40 A positive association between endogenous testosterone levels and vmPFC activity regulating the subjective pain experience would align with our observations of increased pain sensitivity in men with low testosterone levels. The involvement of the vmPFC and its relationship with testosterone levels supports the idea that pain processing is deeply intertwined with emotional and hormonal regulation, and that individual variability in these systems may shape how pain is experienced and managed.
It is important to acknowledge certain limitations of this study. First, the sample size is modest, which limits the generalizability of our findings and increases the risk of a type II error, meaning that a true effect might have gone undetected. Also, the fact that testosterone concentration was only collected before the protocol limits the interpretability of the results, as levels may vary throughout the different stages of the pain protocols. Given the modality-dependent nature of the pain processes observed in this study, the results should be interpreted within the context of our protocol. Despite these limitations, the study also presents several notable strengths. The protocol used follows a standardized structure based on expert recommendations.41 Our free testosterone concentrations were measured using a blood sample, providing measurements that were less prone to external confounds than saliva samples. Moreover, although we emphasize the analyses for free blood testosterone, as this is the most common metric, we have also shared the analyses for the other forms of testosterone (see Table S2).
Conclusion
In conclusion, this study confirmed our original hypotheses, supporting that testosterone can exert a hypoalgesic effect on heat pain sensitivity. While free testosterone levels did not significantly influence CPM and TSP responses, our findings suggest that testosterone contributes to pain perception in men, likely through mechanisms independent of endogenous inhibitory and excitatory pain pathways. These findings may partially explain sex differences in pain sensitivity. Given that men generally have higher testosterone levels than women, hypoalgesic effect of testosterone on heat pain sensitivity could contribute to lower pain sensitivity in men. However, the absence of significant effects of testosterone on CPM or TSP responses highlights the complex and likely multifactorial nature of sex differences, underscoring the need for further research. Pain research would benefit from the systematic assessment of hormonal influences, given the well-established role of sex hormones in modulating nociceptive processing. Studies directly comparing hormonal influences between sexes or using human models associated with testosterone disorders (eg, polycystic ovary syndrome and hypogonadal men, women, and children) would also help clarify whether differences in pain sensitivity and analgesic responses stem from testosterone levels rather than other biological or psychosocial factors, and how sustained hormonal deficiency can shape pain processing and treatment outcomes. Future clinical directions may also emphasize the systematic consideration of hormonal status in both experimental and clinical pain models. Whereas experimental paradigms capture acute and highly controlled nociceptive processes, clinical pain is inherently multifactorial and shaped by rich biopsychosocial interactions. Addressing hormonal influences across both experimental and clinical pain protocols will enhance our ability to determine whether controlled laboratory effects translate to everyday pain.
Funding
This work was funded in part by SM’s and GL's research grants from the Natural Sciences and Engineering Research Council of Canada Discovery Grant [grant number: 323767 and 04585]. MV and MB each received a scholarship from the Fonds de recherche du Québec Santé (FRQ-S). GL received salary support from the Fonds de recherche du Québec – Santé (FRQS). The funders had no role in any of the processes involved in this study, including study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors have no conflicts of interest to declare regarding this manuscript.
References
1. Zhuo S, Zhang Y, Lin C, Peng W. Testosterone administration enhances the expectation and perception of painful and non-painful somatosensory stimuli. Psychoneuroendocrinology. 2023;152:106081. doi:10.1016/j.psyneuen.2023.106081
2. Gaumond I, Arsenault P, Marchand S. The role of sex hormones on formalin-induced nociceptive responses. Brain Res. 2002;958(1):139–10. doi:10.1016/S0006-8993(02)03661-2
3. Gaumond I, Arsenault P, Marchand S. Specificity of female and male sex hormones on excitatory and inhibitory phases of formalin-induced nociceptive responses. Brain Res. 2005;1052(1):105–111. doi:10.1016/j.brainres.2005.06.011
4. Gaumond I, Spooner M-F, Marchand S. Sex differences in opioid-mediated pain inhibitory mechanisms during the interphase in the formalin test. Neuroscience. 2007;146(1):366–374. doi:10.1016/j.neuroscience.2007.01.002
5. Hagiwara H, Funabashi T, Mitsushima D, Kimura F. Effects of neonatal testosterone treatment on sex differences in formalin-induced nociceptive behavior in rats. Neurosci Lett. 2007;412(3):264–267. doi:10.1016/j.neulet.2006.11.020
6. Hau M, Dominguez OA, Evrard HC. Testosterone reduces responsiveness to nociceptive stimuli in a wild bird. Hormones Behav. 2004;46(2):165–170. doi:10.1016/j.yhbeh.2004.02.007
7. Pepino L, Malapert P, Saurin AJ, Moqrich A, Reynders A. Formalin-evoked pain triggers sex-specific behavior and spinal immune response. Sci Rep. 2023;13(1):9515. doi:10.1038/s41598-023-36245-7
8. Wu-Chen E, Banerjee G, Requadt E, et al. The role of androgens on experimental pain sensitivity: a systemic review and meta-analysis. Pain Rep. 2025;10(2):e1263. doi:10.1097/PR9.0000000000001263
9. Stoffel EC, Ulibarri CM, Craft RM. Gonadal steroid hormone modulation of nociception, morphine antinociception and reproductive indices in male and female rats. Pain. 2003;103(3):285–302. doi:10.1016/s0304-3959(02)00457-8
10. Apkhazava M, Kvachadze I, Tsagareli M, Mzhavanadze D, Chakhnashvili M. The relationship between thermal pain sensation, free testosterone, trpv1, mor levels and various degrees of hostility in young healthy males. Georgian Med News. 2018;(283):109–114.
11. Choi JC, Chung MI, Lee YD. Modulation of pain sensation by stress-related testosterone and cortisol. Anaesthesia. 2012;67(10):1146–1151. doi:10.1111/j.1365-2044.2012.07267.x
12. Choi JC, Kim J, Kang E, et al. Brain mechanisms of pain relief by transcutaneous electrical nerve stimulation: a functional magnetic resonance imaging study. Eur J Pain. 2016;20(1):92–105. doi:10.1002/ejp.696
13. Vincent K, Warnaby C, Stagg CJ, Moore J, Kennedy S, Tracey I. Brain imaging reveals that engagement of descending inhibitory pain pathways in healthy women in a low endogenous estradiol state varies with testosterone. Pain. 2013;154(4):515–524. doi:10.1016/j.pain.2012.11.016
14. Pan -L-LH, Chen S-P, Ling Y-H, et al. Salivary testosterone levels and pain perception exhibit sex-specific association in healthy adults but not in patients with migraine. J Pain. 2024;25(9):104575. doi:10.1016/j.jpain.2024.104575
15. Mendell LM. The path to discovery of windup and central sensitization. Front Pain Res. 2022;3. doi:10.3389/fpain.2022.833104
16. Ramaswamy S, Wodehouse T. Conditioned pain modulation—A comprehensive review. Neurophysiol Clin. 2021;51(3):197–208. doi:10.1016/j.neucli.2020.11.002
17. Popescu A, LeResche L, Truelove EL, Drangsholt MT. Gender differences in pain modulation by diffuse noxious inhibitory controls: a systematic review. Pain. 2010;150(2):309–318. doi:10.1016/j.pain.2010.05.013
18. Rezaii T, Hirschberg AL, Carlström K, Ernberg M. The influence of menstrual phases on pain modulation in healthy women. J Pain. 2012;13(7):646–655. doi:10.1016/j.jpain.2012.04.002
19. Vollert J, Trewartha N, Kemkowski D, et al. Conditioned pain modulation and offset analgesia: influence of sex, sex hormone levels and menstrual cycle on the magnitude and retest reliability in healthy participants. Eur J Pain. 2022;26(9):1938–1949. doi:10.1002/ejp.2014
20. Bourque P, Beaudette D. Étude psychometrique du questionnaire de dépression de Beck auprès d’un échantillon d’étudiants universitaires francophones. [Psychometric study of the Beck depression inventory on a sample of French-speaking university students.]. Canadian J Behav. 1982;14(3):211–218. doi:10.1037/h0081254
21. Harmon DK, Masuda M, Holmes TH. The social readjustment rating scale: a cross-cultural study of Western Europeans and Americans. J Psychosomatic Res. 1970;14(4):391–400. doi:10.1016/0022-3999(70)90007-3
22. Gauthier J, Bouchard S. Adaptation canadienne-française de la forme révisée du state–trait anxiety inventory de spielberger. [A French-Canadian adaptation of the revised version of Spielberger’s State–Trait Anxiety Inventory]. Canadian J Behav Sci. 1993;25(4):559–578. doi:10.1037/h0078881
23. Vincenot M, Lévesque S, Gendron L, Camirand Lemyre F, Marchand S, Léonard G. Modeling temporal summation and conditioned pain modulation in individuals with and without chronic pain. Clin J Pain. 2025;41(11):e1320. doi:10.1097/AJP.0000000000001320
24. Potvin S, Vincenot M, Haroune L, et al. Data-driven dynamic profiles of tonic heat pain perception in pain-free volunteers are associated with differences in anandamide levels. Sci Rep. 2024;14(1):17238. doi:10.1038/s41598-024-67401-2
25. Tousignant-Laflamme Y, Pagé S, Goffaux P, Marchand S. An experimental model to measure excitatory and inhibitory pain mechanisms in humans. Brain Res. 2008;1230:73–79. doi:10.1016/j.brainres.2008.06.120
26. Vincenot M, Beaulieu L-D, Gendron L, Marchand S, Léonard G, Karshikoff B. Reliability and minimal detectable change of dynamic temporal summation and conditioned pain modulation using a single experimental paradigm. PLoS One. 2024;19(7):e0307556. doi:10.1371/journal.pone.0307556
27. Vincenot M, Léonard G, Cloutier‐Langevin C, et al. Exploring the spectrum of temporal summation and conditioned pain modulation responses in pain-free individuals using a tonic heat pain and cold pressor test paradigms. Euro J Pain. 2025;29(5):e70019. doi:10.1002/ejp.70019
28. Pednekar JR, Mulgaonker VK. Role of testosterone on pain threshold in rats. Indian J Physiol Pharmacol. 1995;39(4):423–424.
29. Saika F, Uta D, Fukazawa Y, et al. Androgen receptors expressed in the primary sensory neurons regulate mechanical pain sensitivity. bioRxiv. 2025. doi:10.1101/2025.03.13.642983
30. Lesnak JB, Inoue S, Lima L, Rasmussen L, Sluka KA. Testosterone protects against the development of widespread muscle pain in mice. Pain. 2020;161(12):2898–2908. doi:10.1097/j.pain.0000000000001985
31. Goldman AL, Bhasin S, Wu FC, Krishna M, Matsumoto AM, Jasuja R. A reappraisal of testosterone’s binding in circulation: physiological and clinical implications. Endocr Rev. 2017;38(4):302–324. doi:10.1210/er.2017-00025
32. Choi JC, Park Y-H, Park SK, et al. Testosterone effects on pain and brain activation patterns. Acta Anaesthesiol Scand. 2017;61(6):668–675. doi:10.1111/aas.12908
33. Lautenbacher S, Peters JH, Heesen M, Scheel J, Kunz M. Age changes in pain perception: a systematic-review and meta-analysis of age effects on pain and tolerance thresholds. Neurosci Biobehav Rev. 2017;75:104–113. doi:10.1016/j.neubiorev.2017.01.039
34. Zhi Y, Zhang Y, Zhang Y, Zhang M, Kong Y. Age-associated changes in multimodal pain perception. Age Ageing. 2024;53(5):afae107. doi:10.1093/ageing/afae107
35. El Tumi H, Johnson MI, Dantas PBF, Maynard MJ, Tashani OA. Age-related changes in pain sensitivity in healthy humans: a systematic review with meta-analysis. Eur J Pain. 2017;21(6):955–964. doi:10.1002/ejp.1011
36. Nuwailati R, Curatolo M, LeResche L, Ramsay DS, Spiekerman C, Drangsholt M. Reliability of the conditioned pain modulation paradigm across three anatomical sites. Scand J Pain. 2020;20(2):283–296. doi:10.1515/sjpain-2019-0080
37. van der Meulen M, Rischer KM, González Roldán AM, et al. Age-related differences in functional connectivity associated with pain modulation. Neurobiol Aging. 2024;140:1–11. doi:10.1016/j.neurobiolaging.2024.04.008
38. Stanton SJ, Wirth MM, Waugh CE, Schultheiss OC. Endogenous testosterone levels are associated with amygdala and ventromedial prefrontal cortex responses to anger faces in men but not women. Biolog Psychol. 2009;81(2):118–122. doi:10.1016/j.biopsycho.2009.03.004
39. Lim M, O’Grady C, Cane D, et al. Threat prediction from schemas as a source of bias in pain perception. J Neurosci. 2020;40(7):1538–1548. doi:10.1523/JNEUROSCI.2104-19.2019
40. Girard-Tremblay L, Auclair V, Daigle K, Léonard G, Whittingstall K, Goffaux P. Sex differences in the neural representation of pain unpleasantness. J Pain. 2014;15(8):867–877. doi:10.1016/j.jpain.2014.05.004
41. Yarnitsky D, Bouhassira D, Drewes AM, et al. Recommendations on practice of conditioned pain modulation (CPM) testing. Euro J Pain. 2015;19(6):805–806. doi:10.1002/ejp.605
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.