Back to Journals » Patient Related Outcome Measures » Volume 14
Exploring Effective Communication Strategies Employed by Physicians in Delivering Bad News in Ethiopian State Hospitals
Authors Gessesse AG ![]() , Haile JM, Woldearegay AG
, Haile JM, Woldearegay AG ![]()
Received 20 July 2023
Accepted for publication 12 December 2023
Published 20 December 2023 Volume 2023:14 Pages 409—425
DOI https://doi.org/10.2147/PROM.S390164
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lynne Nemeth
Alebel Guangul Gessesse,1 Jemal Mohammed Haile,2 Amanuel Gebru Woldearegay3
1Department of Journalism and Communication, Dilla University, Dilla, Ethiopia; 2Departments of Journalism and Communication, Bahir Dar University, Bahir Dar, Ethiopia; 3School of Journalism and Communication, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Alebel Guangul Gessesse, Tel +251-910922903, Email [email protected]
Introduction: Delivering Bad News (DBN) presents a highly challenging situation in physician-patient communication. This study aims to gain insight into the various communication strategies employed by physicians when DBN.
Methods: This qualitative study conducted thematic analysis of in-depth interviews. Physicians from two comprehensive hospitals with large patient populations were selected purposively based on their engagement in delivering bad news to patients. Thematic analysis was made.
Results: Thematic analysis of the data revealed several communication strategies physicians use when delivering bad news. These communication strategies include. Jointly Initiated Physician-Patient Communication Strategies: ((i) Discussing with patient family/caregivers, (ii) Collaborating with other physicians and specialists), Patient-Engaged/Led Communication Strategies: ((iii) Investigating with adolescents alone or without the family, (iv) Helping patients predict what the news is, (v) Identifying patients’ emotions related to bad news, (vi) Assessing patients’ level of understanding, (vii) Minimizing patient anxiety), Physician-Related Communication Strategies: ((viii) Making sure diagnostic results are accurate, (xi) Identifying causes for rejection, (x) deliveringbad news using clear and simple communication).
Conclusion: Delivering bad news to patients can be challenging for physicians. It is important to be clear and accurate, and to prepare patients for the news. Patients may feel more comfortable and open when they are unaccompanied and with their healthcare provider. The study concluded that physicians need to be prepared to deliver bad news in a sensitive and effective manner.
Keywords: bad news, communication strategies, communication, patient, physicians
Introduction
One of the highly challenging situations for physicians when communicating with patients is breaking bad news. There are many difficulties that doctors have in breaking bad news because of their fear of causing their patients’ damage or pain and their fear of being blamed for or having to deal with their patients’ feelings. According to Ptacek, Fries, Eberhardt & Ptacek,1 the term “bad news” means any information that is given to patients and their families that directly or indirectly involves a negative change in their lives. Similarly, the most recent edition of the Medical Ethics Manual: stats that physicians have a crucial role in delivering bad news, particularly regarding impending death. It emphasizes the importance of considering both cultural and personal factors in the communication process.2
Likewise, for both patients and their families delivering bad news is a challenging task that primarily falls under the responsibilities of physicians. It demands a range of professional skills to effectively handle the communication situation. These skills encompass the ability to communicate potentially distressing information, assess the recipients’ level of understanding, acknowledge and address the emotional repercussions of the news on everyone involved, and facilitate a collaborative approach to decision-making.3 The way these encounters are handled is crucial and has a big impact on how patients make decisions and deal with their disease.
Several previous studies have focused on identifying the communication strategies used by physicians when delivering bad news. For instance, a study conducted by Baile et al4 explored the specific communication techniques utilized by oncologists in breaking bad news to patients with cancer. The study highlighted the importance of strategies such as preparing the patient, addressing emotions, providing clear information, and allowing sufficient time for questions and discussion.
Although studies have shown that patients want integrity, kindness, treatment, and affectivity and that their doctors explain their doubts, they also demand not only professionalism and competence in clinical skills but also communication effectiveness.1 However, this should not be done coldly or recklessly. In light of this, breaking bad news is a difficult task that requires communication skills.
The present study was designed to find out the communication strategies that physicians use to deliver bad news. The way the diagnosis of a serious illness such as cancer is conveyed may have a major effect not just on patients’ perception of their illness, but also on the prognosis and their partnership with their doctor.5 In all cases, the need for good communication skills is essential.
Recent research indicates delivering bad news in Ethiopian state hospitals does not meet recommendatios by authorities in the field. For instance, a study conducted at the Chemotherapy and Radiotherapy Center of Tikur Anbessa (Black Lion) Specialized Hospital in Addis Ababa, the sole facility offering radiotherapy services in Ethiopia, has revealed a common practice of withholding health-related information, particularly bad news, from patients. In many cases, this withholding is done at the request of the patient’s family. Additionally, the clinic’s staff expressed a need for more guidance on how to deliver distressing information and manage family involvement in such situations.6 Abraha Woldemariam et al7 report that the desires of patients to receive information clash with the preferences of their family caregivers, leading to an ethical dilemma for healthcare professionals regarding the extent to which they involve patients in making clinical decisions. Patients themselves emphasize that they do not want information to be kept from them. From them, effective communication involves full disclosure of information about their medical condition. It is therefore necessary to understand that effective communication between healthcare providers and patients is a fundamental element in delivering exceptional medical care.8
Similarly, physicians inability to effectively break bad news to patients and their family due to a lack of communication skills results in long-lasting effects on the patients’ and family caregivers’ lives.9 Patients and relatives who receive negative news have higher levels of emotional distress, which hinders their ability to take in and remember information.10
Indisputably, effective communication in delivering bad news is crucial in healthcare settings. However, there is inadequate research exploring the communication strategies employed by physicians in delivering bad news specifically in the Ethiopian context. It is therefore necessary to investigate the specific communication strategies utilized by physicians in Ethiopian state hospitals when delivering bad news. By identifying these strategies, healthcare providers can enhance their communication skills and tailor their approaches to meet the cultural, linguistic, and contextual needs of Ethiopian patients, ultimately improving the overall patient experience and satisfaction.
The specific objective of the present study was to identify the communication strategies physicians employ in delivering bad news.
Materials and Methods
A qualitative approach was used in this study to identify the communication strategies that physicians employ in delivering bad news in specialized comprehensive hospitals in the study region. In-depth interviews were conducted with physicians to gather their insights on delivering bad news.
Study Site
The participants of the study were selected from Dessie and Felege-Hiwot comprehensive hospitals purposively. Dessie Referral Hospital is a public hospital located in the city of Dessie, in the Amhara region of Ethiopia. It is one of the major hospitals in the North East Ethiopia, offering a wide range of medical services to the local population of the surrounding areas.11
The second study site is Felege Hiwot Hospital, which is a referral hospital located in the city of Bahir Dar, Ethiopia. It serves as the primary referral hospital for the North West Ethiopia, which has a population of approximately 20 million people.
The reason behind the selection of two hospitals was their higher patient load compared with the other six comprehensive specialized hospitals found in the Amhara region. In addition, the two hospitals serve out-of-state patients from the adjusent Afar region, the Oromo special zone, and the Benishangul-Gumuz region, due to the lack of access to specialized medical services in the areas.
Sampling Techniques
The participants of the study were selected from Dessie and Felege-Hiwot comprehensive hospitals purposively. Creswell12 argues that purposefully selected sites or individuals are vital and that cases are selected based on whether they possess certain desired contextual characteristics. A purposive sample includes respondents, subjects, or elements selected for specific characteristics or qualities and eliminates those who fail to meet these criteria.13
The purposive sampling method was used to select participants who had experience in delivering bad news. The purpose of utilizing purposive sampling method was to ensure that the participants had the necessary knowledge and experience to provide insights into the communication strategies used in delivering bad news. The purposive sampling method also allowed the researchers to select participants who were willing to share their experiences and insights. As a result, experienced physicians with over five years of experience were deliberately chosen to handle the task of delivering bad news.
Sample Size and Sampling Frame
The study focused on physicians who engage in regular patient communication and handle the responsibility of delivering difficult or distressing news. In total, the study included a diverse group of twenty four physicians, drawn from two different hospitals. These participants were selected for interviews, forming a representative sample that would contribute valuable insights to the study’s objectives. Focusing on physician’s allowed the study to delve into the nuances of these strategies, potentially leading to tailored interventions or guidelines for improving communication skills.
Inclusion and Exclusion Criteria of Participants
The following inclusion criteria were used for physicians to participate in the research: (1) physicians who are currently following outpatients, (2) physicians who have delivered bad news, (3) physicians who are willing to sign the informed consent form to indicate their willingness to participate in the research, and (4) physicians who have at least five years of working experience, as they will have had sufficient exposure to various patient populations and clinical scenarios to provide valuable insights into physician-patient communication. These criteria ensured that the study’s results were based on a representative sample of physicians with relevant experience and commitment to the research process.
On the contrary, the following criteria were applied to exclude physicians who were not eligible to participate in the study: (1) physicians who were handling inpatient departments and (2) physicians who were not engaged in delivering bad news. By limiting the inclusion criteria to this specific population, the study’s results would be more accurate and applicable to the intended audience. Physicians may employ distinct communication strategies when delivering bad news in outpatient settings. Focusing on this subset allows researchers to delve into the nuances of these strategies, potentially leading to tailored interventions or guidelines for improving communication skills.
Data Collection Method
In-Depth Interview
For this research, in-depth interviews were conducted with physicians who delivered bad news. The aim of interviewing physicians involved in the delivery of bad news was to identify their communication strategies related to breaking bad news. Physicians were selected purposively, mainly based on the inclusion and exclusion criteria stated above. The interviews were carried out during the months of May and June in 2022, the place was located in the hospitals. The study included the Interview Guide in the Supplementary Materials. No repeat interviews were carried out.
Whaley14 argues that an in-depth interview is one of the best methods for investigating health communication processes that are not readily observable in other ways. During the interview, we sat down with physicians in a comfortable setting at the study hospitals. We provided the participants with the necessary information including objectives of the study and the permission to publish their anonymized responses during the written informed oonsent process, allowing them the opportunity to ask any questions they had, all of which we answered to their satisfaction. Once they voluntarily agreed to participate in the study, we proceeded to record the information and conduct the interview. The interview took place with only the participants and researchers present.
Transcription and Translation
The researchers meticulously transcribed Amharic language audio recording. The process of transcription involved listening to the audio recordings multiple times to ensure accuracy and completeness. The researchers paid close attention to the nuances of the Amharic language, including dialects and colloquialisms used by the participants. The transcription was done with the utmost care and attention to detail to capture the essence of the conversations accurately. By transcribing the recording audios, the researchers were able to analyze the data effectively and draw meaningful conclusions from the interviews with physicians. The resulting data provided valuable insights into the experiences and perspectives of the participants, which could inform future research and healthcare interventions.
After the meticulous transcription of the recorded audio of interviews with physicians, the researchers proceeded to translate the transcriptions. The translation process involved accurately rendering the Amharic text into English, while preserving the meaning, intent, and tone of the original speech. The researchers were proficient in both languages, and could capture the nuances and subtleties of the Amharic language and convey them in English. The translation process was critical in ensuring that the data was accessible to a wider audience and could be used to inform policy and practice. The translated transcripts were an essential tool for analyzing the qualitative data and drawing meaningful conclusions from the interviews. The resulting insights could be used to improve healthcare interventions and address the needs of the physicians in the study. Overall, the translation of the Amharic transcriptions was a crucial step in producing high-quality qualitative data and ensuring the validity and reliability of the research findings.
Analytical Strategy
Thematic analysis of qualitative data was performed using Braun and Clarke’s15 steps. Meaningful and holistic categories were combined to form themes. The themes were given under different subheadings in the findings and interpretations.
The study used three detailed steps for data analysis. The first step was creating and using code; in this step, coding was the major activity performed. It was necessary to give each code a title that could makesense. Events, behaviors, actions, meanings, and a variety of other non-quantifiable components can all be coded.
Secondly, the study employed finding themes and connections. When analyzing data for qualitative investigations, the researchers’ analytical and critical thinking skills are crucial due to lack of procedures that can be used to obtain results in qualitative data analysis. As a result, no qualitative study can have the same results when repeated. However, there are a number of strategies employed to find common themes, patterns, and links in the sample group members’ responses with respect to the codes that were defined in the earlier step. The study employed most popular and effective methods of qualitative data interpretation including scanning the primary data for words and phrases most commonly used by respondents, comparing the findings of the interview with the findings of the literature review and discussing differences between them, and discussions about which aspects of the issue were not mentioned by respondents.
Thirdly, presentation data summary was acomplished. At this final step, the researcher connects research findings to the study’s objectives. It also emphasized key findings and potential conflicts in a data analysis chapter by citing relevant passages from the transcript.
The study ultimately employed the COREQ (Consolidated Criteria for Reporting Qualitative Research Checklist) found in the Supplementary Material.
Ethical Consideration
The study was approved by the Ethics Review Board of the Amhara Public Health Institute (APHI) (Reference number NoH/R/T/T/D/5/23 issued on March 11, 2022). Informed consent was obtained from the respondents prior to the questionnaires and interview administration.
Theoretical Framework
The SPIKES Model
The study used the SPIKES model developed by Baile et al4 as a six-step framework for delivering bad news. The acronym stands for Setting, Perception, Invitation, Knowledge, Empathy, and Summary. The protocol emphasizes the importance of preparing for the conversation, assessing the patient’s understanding of their condition, inviting them to participate in decision-making, providing clear information about their diagnosis and prognosis, expressing empathy and support, and summarizing the key points of the conversation.
Several studies have evaluated the effectiveness of the SPIKES protocol in delivering bad news. In a randomized controlled trial conducted by Fujimori et al,16 oncologists who received training in using the SPIKES protocol reported higher levels of confidence and satisfaction in delivering bad news compared to those who did not receive training.
In another study conducted by Ptacek et al,1 patients who received bad news using the SPIKES protocol reported higher levels of satisfaction with communication compared to those who did not receive such information. The use of the SPIKES protocol has been associated with positive patient outcomes such as improved understanding of their condition, increased satisfaction with communication, reduced anxiety and depression levels, and improved quality of life.16
The structured frameworks of SPIKES can help healthcare professionals deliver bad news in a compassionate manner while ensuring that patients understand their condition accurately. Several studies have demonstrated that using this protocol can lead to positive patient outcomes such as improved understanding, increased satisfaction with communication, reduced anxiety levels, and improved quality of life.
Communication Accommodation Theory
The study is mainly guided by communication accommodation theory (CAT) which is a social cognitive approach that was first developed by Giles and associates in 1973.17,18 CAT posits that when people interact, they often attempt to meet the other person’s needs and abilities by adjusting their communication and focuses on the ways individuals modify their communicative behavior as a result of their communication with each other.
In the study of healthcare communication, CAT helps to the researcher to anticipate and clarify nonverbal and verbal behavioral changes made by caregivers and patients to establish, maintain or minimize social distance in interaction.19 CAT focuses on the ways individuals modify their communicative behavior as a result of their communication with each other and helps to comprehend when and how patients and physicians adjust their communication to one another.
As a result, CAT offers a helpful framework for predicting and explaining the various modifications and adjustments that patients and physicians could make in order to create maintain or lessen social distance during medical encounter. Furthermore, Street20 strengthens the idea that understanding how patients perceive physicians accommodating behavior in influencing patients’ satisfaction with the clinical encounter through various accommodation strategies is extremely useful, in the present study, CAT could be helpful in evaluating the effect of accommodation on these communicative outcomes because various accommodation tactics may affect patient centered outcomes, such as patient satisfaction.
In summary, the thematic analysis would use the SPIKES model to categorize findings based on the key steps in delivering bad news, while CAT was applied to examine how physicians accommodate their communication style to enhance understanding and emotional support. By integrating these theoretical frameworks, the analysis aimed to provide a comprehensive understanding of the communication strategies employed by physicians in challenging conversations.
Results
Demographic Characteristics of Physicians
Twenty-four (18 male and 6 female, mean age 33.7 Years) were employed in various outpatient departments (0PD) within the selected hospitals. These departments included Orthopedics, Psychiatry, Pediatrics, ICU, Military, Maternity, Ophthalmology, Emergency, Medical, Surgical, and Oncology. No one refused to participate.
Communication Strategies to Deliver Bad News
Delivering bad news is always a challenging task for providers. However certain communication techniques can make the experience less difficult for the patient and family. In the study, the identified themes were categorized into major themes and subthemes. The major themes were Physician-Patient Jointly Initiated Communication Strategies, Patient-Engaged/Led Communication Strategies and Physician-Related Communication Strategies. To enhance clarity, all major themes and subthemes are presented in Table 1.
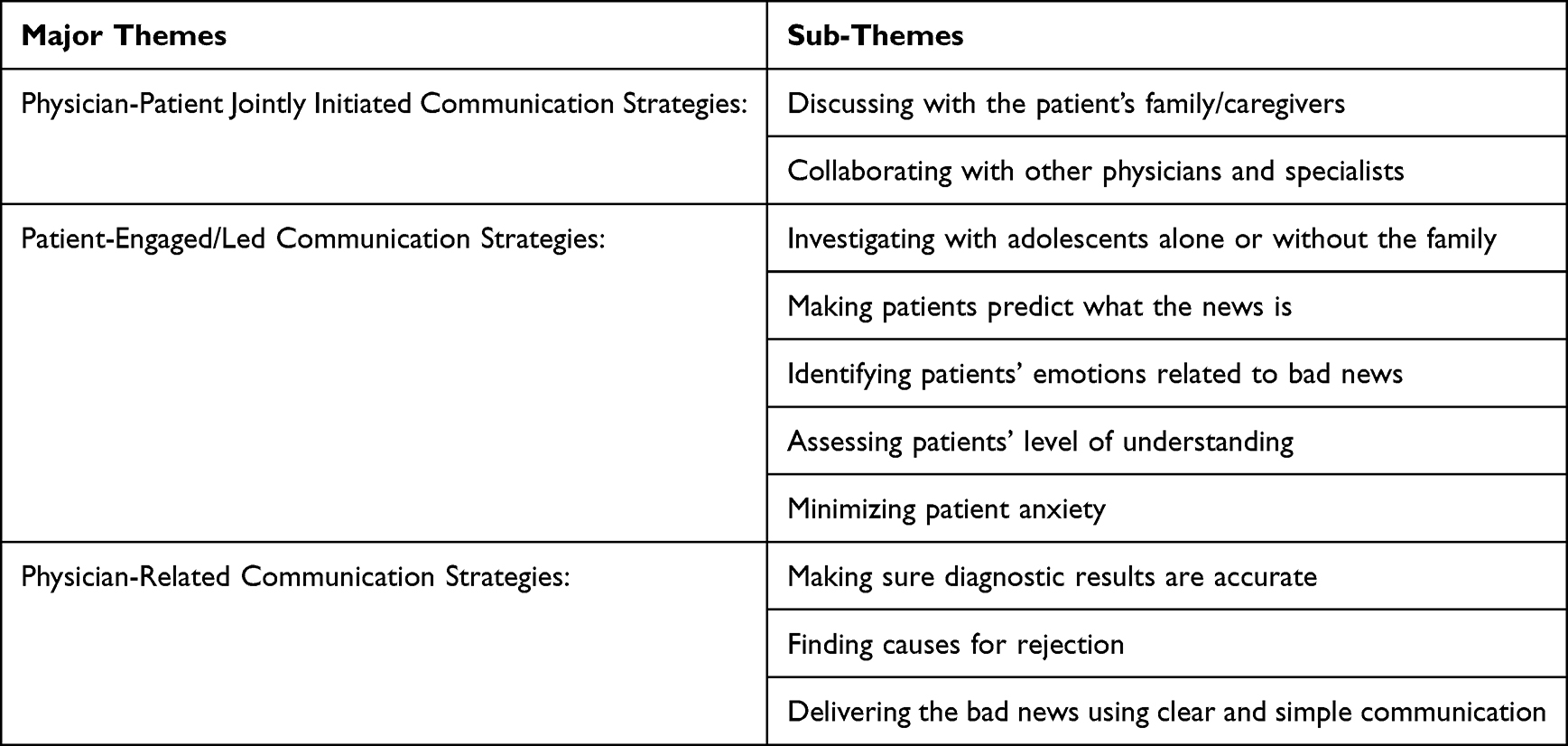 |
Table 1 Key Themes That Physicians Employ When Delivering Bad News |
Physician-Patient Jointly Initiated Communication Strategies
Discussing with Their Families or Caregivers
When physicians deliver bad news to a family member or their parents, it might be particularly difficult. It is essential to communicate clearly at all times. Of course, providers must be considerate of the recipient’s needs and move slowly if necessary. This is particularly valid when talking about death in the family. They need to assure them that they will be there for them by using comforting language and encouraging words. As one interviewee put it:
Yes, you can get some results after diagnosing a patient. Despite this fact, the challenge is how to deliver the results. For example, if I just sit down to report the results of the test for liver cancer, it’s easy for me to explain that the test is over and it shows liver cancer. However, telling the patient right away is not a good idea because he or she expects a simple illness and believes he or she will recover soon, but liver cancer is difficult to treat, so if the level is high and I say “You may die in the next 6 months”, if I kill him right away. He will be in a bad situation. And what is recommended is that the communication should be, first of all, with the people who came with the patient before delivering the bad news . For example, if the patient’s wife or husband comes with him or her, the physician should call and consult with her or him before informing the patient. (PYI1-personal interview on May 12, 2022)
The aforementioned excerpt signifies that having a strong support network can help with treatment. When family or friends are aware of the patient’s struggles, they can offer the most support, particularly after the patient is discharged. Many health-related concerns are caused by family customs, and problems that a physician can also address are another factor. There is a time to tell the family and make them take the medicine. When their health improves and physicians see a change, they will be ready to receive the news. However, physicians do this for inpatients with serious illnesses. Giving patients the news directly will hurt them, not help them. One key informant supports the idea:
Sometimes advanced cases go unreported. Let’s say we have a patient with advanced cancer. It’s lung cancer that has spread throughout the body, and if we say it’s hopeless, it can further shorten the patient’s chances of survival . But, when we have a problem like this, we tell the family or caregivers, even if we don’t tell the patient directly. The situation is like this, there is no hope of recovery, but in the meantime, we recommend; keeping an eye on him by feeding him/her well and giving him sedation so that he does not feel pain. (PYI 4-personal interview on May 15, 2022)
Hence, as shown in the above excerpts, physicians do not speak directly to the patient. Instead, they can just give medicine to the patient and send him or her away without telling him anything about the disease. However, the patient has the right to know the results, and the doctor must inform them.
And another commented
When we deliver negative news to patients, it is important to involve their families in the conversation as they offer crucial support to the patient. (PYI1-personal interview on May 12, 2022)
This strategy shows that physicians need to anticipate the presence of a family member when a serious diagnosis is delivered because it is common. This can be achieved by acknowledging the family member as an excellent source of support for the patient. In addition, it can be done by integrating the family members into the conversation after breaking the bad news. Although the patient’s needs are the most significant consideration when breaking bad news, physicians can build trust and understanding with family members. This is done by actively engaging them in the dialogue as it occurs. Practicing in advance how to talk to the patient without involving a family member in the discussion can be unrealistic.
Collaborating with Other Physicians and Specialists
According to key informants, patients receive news from a team of medical professionals, including physicians, nurses, psychologists, and social workers. Communicating as a team with the patient and with each other helps avoid mistakes and reassures patients and their families that they will be receiving proper care. In one case, the participant thought that.
Once we have received the results, we will contact patients and make an appointment for them to come with their immediate family 3 days later. If it’s something simple, we’ll the patient right away. If it is difficult, we will have a preparation period. Occasionally, we are disappointed. There is a problem that is beyond one’s ability, and there are often multiple problems. At times I call a friend, and the two of us will sit there and explain to the patient the reality of thier illness. If it is too difficult, there are specialists who are better than us, and we can link the patient to specialists. (PYI3 personal interview on May 13, 2022)
The above extract reveals that physicians may take several steps to deliver bad news. It is possible to deliver bad news to a team and to refer the issue to a specialist as one of the methods of delivering it.
Physicians also indicate that there is a common problem with some of their patients. Sometimes it can be due to a cultural influence, which creates a problem of misunderstanding. During such time of difficult communication, physicians come to understand limits of their communication competence; as a result, they try to use their full potential to persuade the patient, as well as their colleagues who may have superior communication skills, and finally refer the matter to specialists. Talking about this issue, an interviewee said:
What we realize now is that persuasive resources vary from person to person, so I will use all of my communicative abilities to persuade the patientregarding their illness, as well as, my colleagues who have stronger exprssive abilities. (PYI4-personal interview on May 15, 2022)
Patient-Engaged/Led Communication Strategies
Investigating Adolescents Alone or Without Their Families
A few people are present during the physical examination and evidence-collection processes. The examining medical team should be the attending personnel. Under no circumstances should the examination be held in the presence of a parent or guardian suspected of perpetrating the abuse.
Based on the findings, physicians give a child or adolescent a choice regarding the presence of a family memebr during medical treatment. However, before being given that choice, physicians need to decide whether the presence of a family during the medical examination is desirable. Ideally, the parent or guardian should be supportive of the child or adolescent and help decrease anxiety. There are, however, certain situations when the presence of a caregiver may be detrimental to the examination. One informant reported that:
When adults are admitted to the examination room and we inquire about their history, we do not allow their family to attend. I follow this strategy because there is something I have gained from experience. Some young people arrived here after making a sexual mistake. Those youths are women, and a woman says ‘I feel sick in my stomach’, I will ask probing questions like, Do you feel nauseous when you wake up in the morning? And I will do HCG internally. I will explain a medical result to the women themselves. Have you ever dealt with this kind of pregnancy issue before? They don’t hide. Now, when I’m alone with them, they rarely hide anything from me. Since I keep them alone, I freely consider their secret to be my own. I only do it so that the patient herself can be informed. Occasionally, it means that there are some worrying things to be aware of. (PYI2-personal interview on June 10, 2022)
In summary, these results show that, if physicians decide that the parent should not be present, a member of the medical team should take the child/adolescent to a private area, provide support and comfort, and explain why the examination is being conducted and what it will include.
Getting Patients to Forecast
The study found that physicians making patients forecast bad news as a strategy while delivering bad news, rather than delivering news either by way of stalling or by being blunt, is the most effective way of eliciting realization on the part of recipients. That is, physicians prepare their patients for the coming news by indicating what it is. In light of this, compared with stalling and being blunt, forecasting allows recipients to predict the news in the second sense. This allows recipients to expect what the news will be, such that when the news arrives, it does so in a prepared social and psychological environment. Thus, while forecasting is a deliverer’s strategy for conveying bad news, it ultimately facilitates realization by involving the recipient in a relational structure of anticipation and understanding.
During the diagnosis process, we inform the patient that the lab-based diagnosis will be made based on our suspicions and that the next test will be discussed after the test. This method helps them think about the next step. Most of the time, we understand this method and what we are trying to convey when we say this. When we announce a test result we say a diagnosis shows a particular illnessand indicates the meaning and implication of the illness. (PYI6-personal interview on June 17, 2022)
The above quoted material indicates that forecasting induces the recipient to anticipate and predict the bad news to come, which is evident when recipients guess the bad news correctly.
Identifying Patients’ Emotions Related to Bad News
The other communication strategy physicians used in the study was to identify patients’ emotions related to bad news. Identifying patients’ emotions related to bad news can be challenging, as people react differently to difficult news depending on a variety of factors, such as their personality, past experiences, and coping mechanisms. By exploring patients’ perspectives, physicians can tailor the news to the patient’s current emotions. This is a vital step because it helps physicians determine if the patient is in a state of denial or has unrealistic expectations of treatment. One participant commented:
To determine the patient’s emotional level, we first look at the patient’s physical condition. When we look at it, the nature of the illness puts them in a state of stress, and we can see and feel how much stress there is in their mood. If they are completely exhausted, it means that stress has affected them more than the pain. For example, when we ask them, they do not explain and are not ready to answer, which means that they are under pressure due to their illness. We understand that they are under a lot of stress. (PAI12-Personal interview on May 18, 2022)
The above excerpt reveals that physicians also give patients psychotherapy. One of the physicians’ duties is not only to give treatment when the patient comes to the hospital; counseling a patient is also a priority. Moreover, physicians have to look at the patients emotional state, and there is a way for them to describe the level of pain; their breathing may be irregular; and physicians can feel the heartbeat. These are methods for determining the level of pain.
More importantly, the possibility of the patient expressing strong emotions, including denial, anger, anxiety, shock, sadness, or blame, is relatively high. Usually, these outbursts make physicians uncomfortable However, it may be necessary to give the patient and family some time to respond and express their emotions rather than attempting to control them right away. Acknowledging and dealing with their feelings as they emerge is a requirement of empathy. Key informants also articulated that to identify patients’ emotions, physicians ask probing questions. One intreviewee stated that:
When we do the examination, we may ask questions in the manner of an HIV/AIDS examination: “What would you do if your result might be unexpected?” And then, if the patient is willing, if it doesn’t hurt his feelings, and if it doesn’t cause problems in his situation, we will do the examination and then let them know the results. (PYI8-personal interview on June 18, 2022)
And another commented:
Before delivering bad news, we ask a question like, ‘Do you think you have had this disease before, or has anyone ever told you that you have it? “to which the patient might reply, ‘I have never heard of it”. Then we can tell him that the tests results are in and show a particular medical condition and explain the nature of the disease. (PYI9-personal interview on June 19, 2022)
The above two excerpts show that physicians confirm the patient’s emotions by asking probing questions. The findings also indicate that physicians investigate the patients’ perceptions before delivering bad news.
Assessing the Level of Patients’ Understanding
When delivering bad news to a patient, it is important to assess their level of understanding to ensure effective communication and support. This involves evaluating the patient’s comprehension of the information, their emotional reactions, and their ability to make informed decisions regarding their care. Therefore, healthcare providers need to prioritize assessing a patient’s understanding when delivering bad news.
Before breaking the news to a patient, physicians should assess their level of comprehension. This step helps physicians learn what the patient already knows about the disease and their level of understanding. Before providing information, it may be necessary to find out what the patient already knows about their condition. Talking about this issue an interviewee said:
If I have to deliver bad news to patients, I ask certain questions to assess their level of understanding. There are times when patients answer based on their understanding. If they do not seem to understand adequately we attempt to explain in different ways. Finally, I ask them, “Do you understand me?” and check their level of understanding of the issue. (PYI 5-personal interview on May 16, 2022)
As shown in the above excerpts, physicians assess their patients’ prior knowledge of the diagnosis they will deliver. In many instances, the patient has previously received information from other healthcare professionals. Different media platforms might color the patient’s thoughts and perhaps make them confused when updated information is provided. In light of this, physicians should be aware that patients will arrive at their offices with preconceived assumptions about a specific ailment. These assumptions may be based on sources that are not entirely reliable. As a result, determining what a patient already understands or misunderstands at the outset is crucial.
Minimizing the Patient’s Anxiety
Delivering bad news can increase anxiety and elicit a shock-induced acute stress response. Hence, physicians try to avoid such negative feelings. Talking about this issue, an interviewee said:
Sometimes, if you treat patients like family, they feel more liberated. They will be happy. There is something I learned from my university teacher. There is not much that he has done, but something that he has done to his patients. This has made many people say that if he touches them, they will feel happy and all the pain will be gone. I sometimes joke about why a patient is fat while she is actually thin and a fat woman why she is skinny. Some like it when you tell simple family jokes, touch their bodies, and do a physical exam for their pain. I try things that help patients minimize their anxiety. (PYI2- personal interview on June 10, 2022)
As shown in the above excerpts, these results show that physicians can minimize the patient’s anxiety in a variety of ways.
Physician-Related Communication Strategies
Making Sure Diagnostic Results are Accurate
Physicians often struggle with how to deliver bad news. They do not want to deny the patient hope. They might be worried about how the patient or their family will respond to the news or become unsure of how to handle a strong emotional reaction. In doing so, it is often necessary to break bad news with confirmed results. The outcome of the diagnosis affects the physician’s way of delivering bad news. One informant reported that…
There are two types in this regard. One senario is the illness is simple. Or if the disease has been treated and cured, which presents little difficulty to talk about. We will tell them the result if they ask for it, and we will tell them what the test shows. However, you used to be certain if the disease is very serious, such as cancer, high blood pressure, heart disease, diabetes, and so on before releasing the results.These: diseases becouse they are chronic and require lifelong care and oftent trigger significant concern. The severity of the illness requiers you first confirm the diagnosis 100 percent. (PYI3-personal interview on May 13, 2022)
In sum, the findings revealed that there will be a problem with physicians, and there may be a problems with the nurses and laboratory technicians who work with them. There are some unpleasant things about imaging. Physicians do not know whether the results are unpleasant because of the professional’s neglegence or lack of knowledge. Many patients are now treated based on a physical and history examination. As one interviewee put it;
Sometimes, when we have a hard time with a decision, we send them outside again. Let’s send it to the experts we trust again.” (PYI2-personal interview on June 10, 2022)
There are professional interpretatives differences in the results that physicians obtain from the laboratory. At times, rather than stating that particular result is incorrect, physicians may choose to use delay tactics.
Finding the Cause of Rejection
According to the findings of the other section of the study, a patient deny or rejected the results of the diagnosis. Despite the fact that physicians are often advised not to confront denial at the first interview, they should also understand that denial is an unconscious mechanism that may facilitate coping and should be treated gently over several interviews. As a result, physicians who identify the causes of denial at an early stage will most likely just treat the patient’s anxiety. One participant commented:
For example, while we tell the patient s/he has HIV/AIDS, they may not want to accept the result, and we ask ourselves, “Why did they not accept it?” We think it might be because of an abnormality or the fear of being stigmatized and discriminated against by society. We will try to find out the reason behind the denial. (PYI2-personal interview on June 10, 2022)
The above excerpt indicates that physicians, when delivering bad news and facing denial from patients, try to find out the reason behind the rejection or denial. Often, how to get through denial depends on the issue at hand. Given enough time and encouragement, people often accept the truth of a situation on their own, and support groups or psychotherapy may also be beneficial.
Delivering the Bad News Using Clear and Simple Communication
It’s essential to communicate clearly at all times. Of course, physicians must be considerate of the recipient’s needs and move slowly if necessary. This is especially true when talking about a death in the family. It may be necessary using comforting language and encouraging words.
When physicians deliver news to patients, slow, deliberate information gives patients the time they need to process the newly acquired knowledge. Other strategies physicians employ to give patients time include taking regular breaks and utilizing proper body language to reinforce silence according to their response. The listener has more time to ask questions with a slow delivery and suitable pauses, which the doctor can use to provide more precise information. So, a conversation with pauses helps both parties understand the other party better. For example, one interviewee said:
We make patients adhere by saying the result has been reached and we have already discussed it. In light of this, we advise them to take the action they need to take. For example, if a patient is diagnosed with diabetes, we don’t say that you have diabetes; instead, the results show that the level of sugar in your blood is increasing. On the other hand, there will be an opportunity for us to speak smoothly. I tell the patient gently that, according to what they told me and based on the results of our analysis, particular complaints will show will show. You don’t say that this is the disease you have at the same time. (PYI 6-personal interview on June 17, 2022)
As shown in the above quotes, physicians should take their time to inform the patient. It is not advisable to be in a position where professionals feel like lightning all at once. After physicians explain to the people close to the patient that this is how professional conduct is, they should make them gradually aware of it. The physician should think about how to say it. Can his feelings be hurt? It means that they will talk to the caregivers, and then they will gradually inform them in a way that will not hurt them. But when they announce, the truth must be told, and there must be a clear line. It should not be covered. And when they tell the truth, for example, if it is a serious illness, without saying that you will die after 6 months, it means that you are being killed on the spot.
On the other hand, physicians need to use easy-to-understand language that explains the information or decision with clarity. They should not not use medical jargon or reframe the news so that it seems less severe. Physicians should be honest and direct when delivering the news, or make sure patients understand the information they are sharing.
Discussion
Delivering bad news is an inevitable part of a physician’s job, yet it remains one of the most challenging tasks they face. The way physicians communicate bad news can have a significant impact on patients’ emotional well-being and their ability to cope with the diagnosis.21 The following are some of the major strategies that physicians employ in delivering bad news to patients.
Engaging in discussions with Their Families
The results of this study indicate that physicians commonly discuss the delivery of bad news with their patients’ families or caregivers. This finding is consistent with previous research that has highlighted the important role that family members and caregivers can play in the healthcare decision-making process.22 By involving family members and caregivers in the discussion of bad news, physicians can ensure that patients receive the emotional and practical support they need to cope with their illness.
The involvement of family members and caregivers in the discussion of bad news is also consistent with CAT. According to this theory, individuals adapt their communication style to match the expectations and norms of their social group.18 When physicians involve family members and caregivers in the discussion of bad news, they adapt their communication style to match the expectations and norms of these individuals, which can help to facilitate effective communication and support.
On the contrary, the findings shows that physicians give children and adolescents a choice regarding the presence of parents or other support persons during medical treatment, which is consistent with the principles of patient-centered care, which emphasizes the importance of involving patients in their care decisions.23 The finding that physicians give children and adolescents a choice regarding the presence of parents or other support persons during medical treatment aligns with the principles of patient-centered care and can promote patient autonomy, relatedness, and improved outcomes.24 Physicians should continue to prioritize patient-centered care in their practice and consider the potential benefits of involving parents or other support persons in medical treatment decisions.
Accurate Diagnosis in Communication
The findings of this study highlight the importance of effectively communicating confirmed results, even if they are negative or unfavorable. According to the American Medical Association Code of Medical Ethics, physicians have a professional responsibility to ensure the accuracy of the diagnosis and communicate the diagnosis to the patient in a compassionate and sensitive manner.25 However, the finding of this study confirmed that one strategy to ensure the accuracy of the diagnosis is to review the results of diagnostic tests and seek second opinion when necessary.
One potential protocol for breaking bad news in research is the SPIKES protocol developed by Baile et al,4 emphasizes the importance of preparing for the conversation, assessing the patient’s understanding and emotional state, delivering information clearly and empathetically, addressing any concerns or questions, and summarizing next steps.
The study findings indicate potential issues with physicians, nurses, and laboratory technicians who collaborate with them. Imaging can be a challenging area, as physicians may not always be able to determine if unpleasant results are due to professional negligence or lack of knowledge. Some patients are now being treated through physical examinations and medical history assessments, but when decisions become difficult, physicians may refer them to trusted experts for further evaluation. As one interviewee put it;
We sometimes send them outside once more when we are having trouble making a decision. We say the results return to the professionals we acknowledged. (PYI2-personal interview on June 10, 2022)
Additionally, there may be discrepancies in the results that physicians obtain from the laboratory, leading to delays in communicating incorrect diagnosis.
The National Comprehensive Cancer Network recommends obtaining a second opinion from a qualified healthcare professional when the diagnosis is uncertain or when there is a lack of consensus among physicians.26 The NCCN also recommends that physicians consider the patient’s preferences and values when making treatment decisions based on the diagnosis.19 In conclusion, effectively communicating confirmed results is an important aspect of research ethics and requires careful consideration of communication strategies and theories.
On the other hand, enabling patients to anticipate the news (predicting unfavorable outcomes) with greater accuracy by providing enough information can help them to anticipate unfavorable outcomes with greater accuracy. In a study conducted by Fried et al,27 patients were provided with detailed information about their prognosis using a prognostic index tool. The study found that physicians enable patients to anticipate the news (predicting unfavorable outcomes) with greater accuracy by providing enough information.
This finding is consistent with the concept of informed decision-making, which emphasizes the importance of providing patients with the information they need to make informed decisions about their healthcare is widely recognized in healthcare literature. Informed decision-making has been shown to be associated with improved patient outcomes, increased patient satisfaction, and reduced healthcare costs,28 when patients are well-informed about their prognosis, they are better able to understand the potential risks and benefits of different treatment options.
This can help them to make decisions that are aligned with their personal values and preferences and can improve their overall satisfaction with their healthcare experience. In turn, this can lead to better health outcomes and improved quality of life.
Empathizing the Communication
The results of this study indicate that empathic communication is a communication strategy that physicians commonly employ when delivering bad news to their patients. This finding is consistent with previous research that has demonstrated the importance of empathy in medical practice.29 The use of empathic communication allows physicians to demonstrate an understanding of their patients’ emotional experiences, which can help to build trust and rapport between the physician and patient.
Previous studies have explored the effectiveness of this strategy in improving patient outcomes and satisfaction. One study by Buckman30 found that empathic communication was associated with higher levels of patient satisfaction and reduced anxiety in patients receiving bad news. The study also found that physicians who used empathic communication were perceived as more caring and supportive by their patients. A more recent study by Kim et al,31 investigated the role of physician empathy in improving patient satisfaction with end-of-life care and found that physicians who demonstrated high levels of empathy were more likely to engage in effective communication with their patients and families, leading to higher levels of satisfaction with end-of-life care.
In addition to the use of empathic communication, this study also found that the delivery of bad news should be slow and deliberate to allow patients the time they need to process the newly acquired knowledge. This finding is consistent with the “SPIKES” protocol, which emphasizes the importance of taking the time to deliver bad news in a structured and deliberate manner.4 When physicians deliver bad news quickly or in a rushed manner, patients may feel overwhelmed and may not fully comprehend the information being provided to them.
Emotional Identification and Assessment of Patient Understanding
The ability of physicians to accurately identify patients’ emotions while delivering bad news is crucial for patient-centered care and effective communication.32 The study found communication strategy physicians used was to identify patients’ emotions related to bad news.
Physicians have to look at the mood, and there is a way for them to describe the level of emotion. These findings are consistent with previous studies that have explored physician-patient communication in the context of delivering bad news. For example, a study by Ptacek et al,1 found that physicians who were more empathetic and provided emotional support during the delivery of bad news were perceived as more competent and trustworthy by their patients. Similarly, a study by Back et al,32 found that patients who received more emotional support from their physicians during the delivery of bad news reported lower levels of anxiety and depression.
In the study key informants also articulated that to identify patients’ emotions, physicians ask probing questions. One individual stated that: “When we do the examination, let’s ask questions in the manner of an HIV/AIDS examination, like this:
What would you do if your result might be unexpected? “and others.” (PYI8-personal interview on June 18, 2022)
Similarly, these findings are consistent with those of Stewart et al33 which showed that physicians who were able to accurately identify patients’ emotions while delivering bad news were perceived as more empathetic by patients and were associated with improved patient outcomes, such as increased patient trust and satisfaction with care.
As previously stated in the findings section, one strategy physicians used while delivering bad news is assessing the patient’s level of understanding. One way that physicians can assess the patient’s level of understanding is by using open-ended questions. Open-ended questions encourage patients to provide more detailed responses and can help physicians understand the patient’s perspective.34
Physicians could ask patients how they feel about the news they have received or if they have any questions. Open-ended questions have been shown to be an effective way to assess patients’ emotional state and understanding of medical information.35
The CAT suggests that communication should be tailored to the individual and that successful communication involves both accommodation and convergence.18 Accommodation involves adjusting one’s communication style to match the other person, while convergence involves the other person adjusting their communication style to match that of the speaker. By assessing a patient’s level of comprehension before breaking news, physicians can tailor their communication to the individual patient, accommodating their needs and improving the likelihood of successful communication.
A study by Hagerty et al,36 examined the communication strategies used by oncologists when delivering bad news to patients. The study found that assessing the patient’s level of understanding was a crucial strategy that helped physicians tailors their communication to the patient’s needs and concerns. This approach was also associated with increased patient satisfaction and lower levels of emotional distress.
Similarly, a study by Khoramshahi et al,37 found that assessing the patient’s understanding was a critical component of effective communication when delivering bad news. The study highlighted the importance of using clear and simple language, avoiding medical jargon, and checking for comprehension throughout the conversation.
Other studies have also emphasized the importance of assessing the patient’s level of understanding when delivering bad news. For example, a systematic review by Ptacek et al,1 found that patients who reported feeling well-informed and understood during the conversation had better emotional outcomes and were more satisfied with their care.
Promoting Collaborative Care
Based on input from key informants, it was found that physicians deliver news in a collaborative team of medical professionals comprising physicians, nurses, psychiatrists, psychologists, and social workers. This team-based approach to communication enables effective coordination and reduces the likelihood of errors, thereby instilling a sense of reassurance in patients and their families that they will receive optimal care. Physicians rely on the support of colleagues or specialists to help explain the situation to the patient. As one interviewee stated,
If it’s too difficult, we can call in a friend who is better equipped to handle the situation, and we can sit together with the patient and explain things. Alternatively, we may also referred the patient to specialist. (PYI3 personal interview on May 13, 2022)
Physicians have reported encountering a common issue with some of their patients, which is often related to cultural influences leading to misunderstandings. In such situations, physicians acknowledge that their persuasiveness and communication skills may differ from one physician to another. To overcome this challenge, they make use of their full potential to persuade the patient, as well as seek the support of colleagues who possess higher communication skills and may be better equipped to engage with patients from diverse backgrounds. According to one interviewee,
Given that our persuasiveness can vary from person to person, I try to use all of my persuasive abilities to convince the patient, and I also rely on my colleagues who have stronger persuasive skills. (PYI4-personal interview on May 15, 2022)
The finding is consistent with the concept of inter professional collaboration in healthcare. The importance of inter professional collaboration is further supported by the Institute of Medicine’s report on the future of nursing, which emphasizes the need for healthcare providers to work together in a collaborative, interdisciplinary manner to achieve optimal patient outcomes.23
Alleviating Patient Anxiety
The findings of this study reveal that patients may deny or reject the information about their medical condition, which poses a significant challenge for physicians in delivering proper care. Denial is a common coping mechanism that individuals use to avoid the distress associated with a diagnosis, and it is essential for physicians to understand the reasons for denial before confronting patients. One participant commented:
For example, while we break the news that the patient has HIV/AIDS, he or she may not want to accept it, and we may ask ourselves, “Why did they reject it?” We think it might be because of an abnormality or the fear of being stigmatized and discriminated against by society. We often try to find out the reason behind the rejection . (PYI2-personal interview on June 10, 2022)
Physicians are often advised not to confront denial during the first interview, as this may exacerbate the patient’s anxiety and lead to a breakdown in communication. However, they must also be mindful of the potential negative consequences of allowing denial to persist. By doing so, they can facilitate the patient’s acceptance of the diagnosis and improve the patient’s overall well-being.
The finding that physicians can identify the cause of rejection and minimize the patient’s anxiety in various ways aligns with the E4 communication model. The E4 model emphasizes empathy, empowerment, and encouragement to promote effective communication between healthcare providers and patients.31 When patients reject or deny the results of a study, physicians can use the E4 model to approach the situation and identify the underlying cause of rejection.
Conclusion
DBN is an integral part of a physician’s role, and it holds great significance for patients’ emotional well-being and their ability to cope with a diagnosis. The findings highlight that some young people may feel more comfortable and open when they are alone with their healthcare provider. This can allow for more honest communication and a better understanding of their medical history and concerns. By keeping them alone, healthcare providers can create an environment where patients feel safe to share sensitive information. However, healthcare providers need to handle this information responsibly and ensure patient confidentiality.
The fear of denying hope concerns about emotional reactions, and uncertainty on how to handle such situations make it difficult for physicians to effectively communicate bad news. However, physicians must break bad news with confirmed results, especially in cases of serious diseases like cancer or chronic conditions. The study also suggests that there may be issues not only with physicians but also with nurses and laboratory technicians involved in the diagnostic process. Overall, these findings emphasize the importance of clear and accurate communication in delivering bad news to patients.
The findings of this study also suggest that the strategy of forecasting bad news, rather than stalling or being blunt, is the most effective approach in eliciting realization and understanding from patients. By giving patients an indication of what the news will be, physicians can prepare them for the impending information and create a social and psychological environment that facilitates acceptance and comprehension. This method allows patients to anticipate and predict the news, enabling them to mentally prepare for it. Additionally, informing patients during the diagnosis process about the basis of lab-based diagnosis and discussing future tests helps them understand the next steps in their treatment journey.
Limitations of the Study
One potential limitation of this study is its exclusive focus on verbal communication within physician-patient interactions. While verbal communication is undoubtedly crucial for communication strategies physicians employ in delivering bad news, it is essential to recognize that nonverbal communication also plays a significant role in delivering bad news. Nonverbal cues such as body language, facial expressions, and tone of voice can convey empathy, understanding, and reassurance, which can greatly impact patient satisfaction and trust.
Therefore, future research should consider incorporating a comprehensive analysis of both verbal and nonverbal communication in physician-patient communication to obtain a more holistic understanding of communication strategies physicians employ in delivering bad news. This would allow for a more comprehensive exploration of the various communication strategies and techniques that can optimize patient care and improve overall healthcare outcomes.
Implication and Recommendation
By understanding effective communication techniques for delivering difficult news, physicians can improve patient understanding, emotional support, and coping mechanisms during challenging situations. State hospitals should invest in communication skills training for physicians to enhance their ability to communicate effectively with patients. This training should focus on techniques for delivering bad news in a compassionate and empathetic manner, as well as strategies for building rapport and trust with patients during routine interactions. This includes training in empathy, active listening, and effective communication techniques to improve patient experiences during difficult conversations.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ptacek JT, Fries EA, Eberhardt TL, Ptacek JJ. Breaking bad news to patients: physicians’ perceptions of the process. Support Care Cancer. 1999;7(3):113–120. doi:10.1007/s005200050240
2. The World Medical Association. Medical Ethics Manual. World Medical Association. Ferney-Voltaire Cedex; 2015.
3. Beach WA, Easter DW, Good JS, Pigeron E. Disclosing and responding to cancer “fears” during oncology interviews. Soc Sci Med. 2005;60(4):893–910. doi:10.1016/j.socscimed.2004.06.031
4. Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5(4):302–311. doi:10.1634/theoncologist.5-4-302
5. Maguire P. Breaking bad news. Eur J Surg Oncol. 1998;24:188–191. doi:10.1016/S0748-7983(98)92929-8
6. Kebede BG, Abraha A, Andersson R, et al. Exploring communicative challenges in Ethiopian cancer care: a qualitative study. PLoS One. 2018;15:e0230309.
7. Abraha Woldemariam A, Andersson R, Munthe C, Linderholm B, Berbyuk Lindström N. Breaking bad news in cancer care: Ethiopian patients want more information than what family and the public want them to have. JCO Glob Oncol. 2021;7:1341–1348. doi:10.1200/GO.21.00190
8. Gessesse AG, Mohammed Haile J, Woldearegay AG. The nexus between physician-patient communication and health outcomes: level of patient communication satisfaction and its impact on adherence in Ethiopian comprehensive specialized hospitals. Patient Preference Adherence. 2022;16:2509–2519. doi:10.2147/ppa.s381937
9. Barclay JS, Blackhall LJ, Tulsky JA. Communication strategies and cultural issues in the delivery of Bad News. J Palliat Med. 2007;10(4):958–977. doi:10.1089/jpm.2007.9929
10. AlMohaimeed AA, Sharaf FK. Breaking bad news issues: a survey among physicians. Oman Med J. 2013;28(1):20–25. doi:10.5001/omj.2013.05
11. Sewagegn N. Evaluation of ceftriaxone use for hospitalized patients in Ethiopia: the case of a referral hospital. Int J Pharm Sci. 2017;3(2):26–31. doi:10.25141/2471-6782-2017-2.0026
12. Creswell JW. Research Design: Qualitative, Quantitative and Approaches. Thousand Oaks, CA: Sage; 2014.
13. Wimmer RD, Dominick JR. Mass Media Research: An Introduction.
14. Whaley BB. Research Methods in Health Communication: Principles and Application. Routledge; 2014.
15. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
16. Fujimori M, Shirai Y, Asai M, Kubota K, Katsumata N, Uchitomi Y. Effect of communication skills training program for oncologists based on patient preferences for communication when receiving bad news: a randomized controlled trial. J Clin Oncol. 2014;32(20):2166–2172. doi:10.1200/jco.2013.51.2756
17. Giles H. Accent Mobility: A Model and Some Data. Anthropological Linguistics; 1973.
18. Giles H, Taylor DM, Bourhis RY. Towards a theory of interpersonal accommodation through language: some Canadian data. Lang Soc. 1973;2:177–192. doi:10.1017/S0047404500000701
19. Giles H. Communication Accommodation Theory. Engag Theor Interpers Communic. 2008;2008:161–173.
20. Street RL. Accommodation in medical consultations. Cont Accommod. 1991;131–156. doi:10.1017/cbo9780511663673.004
21. Adebayo PB, Abayomi O, Johnson PO, Oloyede T, Oyelekan AAA. Breaking bad news in clinical setting - health professionals′ experience and perceived competence in southwestern Nigeria: a cross sectional study. Ann Afr Med. 2013;12(4):205. doi:10.4103/1596-3519.122687
22. Tang VL, Hannon B, Johnson N, Krzyzanowska MK, Mahendran R. Shared decision-making for individuals with cancer: evolving contributions of family caregivers. Support Care Cancer. 2015;23(12):3403–3408. doi:10.1007/s00520-015-2920-5
23. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. National Academy Press; 2001.
24. Bernabeo E, Holmboe ES. Patients, providers, and systems need to acquire a specific set of competencies to achieve truly patient-centered care. Health Affairs. 2013;32(2):250–258. doi:10.1377/hlthaff.2012.1120
25. American Medical Association. Telemedicine: what it is and how it works; 2021. Available from: https://www.ama-assn.org/practice-management/digital/telemedicine-what-it-and-how-it-works.
26. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: second opinion pathology review; 2021. Available from: https://www.nccn.org/professionals/physician_gls/pdf/second_opinion.pdf.
27. Fried TR, Bradley EH, O’Leary JR, Canavan M, Cherlin E, Bradley E. Prognosis communication in serious illness: perceptions of older patients, caregivers, and clinicians. J Am Geriatr Soc. 2017;65(7):1406–1412. doi:10.1111/jgs.14891
28. Stiggelbout AM, Van der Weijden T, De Wit MPT, et al. Shared decision making: really putting patients at the centre of healthcare. BMJ. 2012;344:e256. doi:10.1136/bmj.e256
29. Decety J, Jackson PL. The functional architecture of human empathy. Behav Cognit Neurosci Rev. 2004;3(2):71–100. doi:10.1177/1534582304267187
30. Buckman R. Communicating difficult news supportively. Support Oncol. 2011;485–492. doi:10.1016/b978-1-4377-1015-1.00047-3
31. Kim SS, Kaplowitz S, Johnston MV. Factors associated with patient satisfaction in university hospitals in Korea: a national cross-sectional study. Int J Qual Health Care. 2018;30(7):527–533.
32. Back AL, Arnold RM, Baile WF, et al. Efficacy of communication skills training for giving bad news and discussing transitions to palliative care. Arch Intern Med. 2005;165(6):697–703.
33. Stewart M, Meredith L, Brown JB, Galajda J. The influence of older patient-physician communication on health and health-related outcomes. Clin Geriatr Med. 2000;16(1):25–36. doi:10.1016/s0749-0690(05)70005-7
34. Kripalani S, Weiss BD, Teaching TB. Teaching about health literacy and clear communication. J Gen Intern Med. 2008;23(4):467–470.
35. Clayton JM, Butow PN, Waters A, et al. Evaluation of a novel individualised communication-skills training intervention to improve doctors’ confidence and skills in end-of-life communication. Palliat Med. 2013;27(3):236–243. doi:10.1177/0269216312449683
36. Hagerty RG, Butow PN, Ellis PM, et al. Communicating with realism and hope: incurable cancer patients’ views on the disclosure of prognosis. J Clin Oncol. 2016;24(20):4209–4213. doi:10.1200/JCO.2006.06.9479
37. Khoramshahi F, Ehsani SR, Dastpak M, Fallahi-Khoshknab M. The effect of communicating bad news using a blended teaching method on the communication skills of oncology nurses. Cancer Nurs. 2019;42(4):E1–E7. doi:10.1097/NCC.0000000000000635
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.