Back to Journals » Patient Preference and Adherence » Volume 20
Exploring Changes in Family Functioning: A Qualitative Study of Patients with Rheumatoid Arthritis
Authors Sadeghnezhad H ![]() , Sabeghi H, Vagharseyyedin SA
, Sabeghi H, Vagharseyyedin SA
Received 7 January 2026
Accepted for publication 25 February 2026
Published 27 February 2026 Volume 2026:20 594313
DOI https://doi.org/10.2147/PPA.S594313
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Hossein Sadeghnezhad,* Hakimeh Sabeghi, Seyyed Abolfazl Vagharseyyedin*
Department of Nursing, Faculty of Nursing and Midwifery, Birjand University of Medical Sciences, Birjand, Iran
*These authors contributed equally to this work
Correspondence: Seyyed Abolfazl Vagharseyyedin, Department of Nursing, Faculty of Nursing and Midwifery, Birjand University of Medical Sciences, Birjand, Iran, Email [email protected]
Purpose: Rheumatoid arthritis (RA) is a chronic inflammatory disease that affects not only patients’ physical and psychological health but also their families’ functioning. Despite the central role of families in providing care, particularly in cultures with strong family bonds, little is known about the specific changes that RA causes in family functioning. This study aimed to explore patients’ experiences and perceptions of changes in family functioning associated with with RA.
Patients and Methods: This conventional content analysis study was performed on 19 participants who were purposively selected from Birjand and Kashmar cities in Iran from February 2025 to July 2025. Face-to-face, semi-structured, in-depth interviews were conducted to collect data. The interviews continued until no new experiential meanings emerged, indicating data saturation. The data were analyzed using the conventional content analysis approach of Graneheim and Lundman using MAXQDA version 2020.
Results: Six main categories emerged, reflecting extensive changes in family functioning: 1) reduced functional independence in daily life activities, 2) compromised marital affairs, 3) limitations in parenting, 4) Imposing additional financial burden on the family, 5) restrictions in social activities, and 6) deprivation of psychological comfort within the family.
Conclusion: Patients reported that RA disrupts their family functioning. In contexts such as Iran, where families are deeply involved in caregiving, these challenges are intensified. The findings highlight the need for family centered interventions, psychosocial support, and health policies that address patient care and family well-being.
Keywords: chronic disease, family, qualitative research, rheumatoid arthritis
Introduction
Rheumatoid arthritis (RA) is a common chronic inflammatory disease that affected 17.6 million people globally in 2020.1 At the individual level, RA not only reduces the quality of life but also leads to psychological problems, such as depression and anxiety.2 However, the impact of this disease on family functioning has received less attention.3,4
Family functioning includes effective communication, problem-solving, fulfilling responsibilities, and mutual support.5 The dimensions influencing family functioning include tasks and roles, communication patterns, emotional expression, level of involvement and participation, behaviors, values, and rules.6 In many societies, the family is considered the primary and most important source of social, emotional, and economic support for patients.7 Proper family functioning can have positive outcomes, such as better adaptation to the disease, improved treatment adherence, enhanced quality of life, reduced feelings of loneliness, and increased motivation for self-care.8 Proper family functioning can lead to higher levels of motivation and self-confidence in patients with RA.9,10 In contrast, poor family functioning may lead to increased stress, feelings of frustration, decreased motivation for treatment adherence, exacerbation of psychological symptoms such as depression and anxiety, and even social isolation of patients.11
Although positive family functioning has a significant impact on adaptation to and management of RA,12 a systematic review showed that when a family member develops a chronic illness, all family members are likely to be affected by the symptoms, treatment, limitations, and complications of the disease.13 Studies conducted in Singapore and Turkey have confirmed that RA affects not only an individual’s physical and mental health but also impacts relationships, family roles, and responsibilities, leading to an increased burden on caregivers and negative effects on their health and finances.14,15
The existing literature often focuses on the clinical aspects of RA or assesses family burden from an external viewpoint. However, there is a gap in understanding how patients themselves experience and perceive the changes within their families. Therefore, the aim of this study was to deeply explore the lived experiences and perceptions of patients with RA regarding the changes in their family functioning.
Materials and Methods
Study Design
This study employed a qualitative content analysis using a conventional approach. Nineteen participants were selected for this study. To be eligible for this study, participants were required to meet several criteria, including adults who were 18 years old and above, diagnosed with RA over 1 year ago by a rheumatologist based on the criteria set by the American College of Rheumatology (ACR), and able to speak Persian. The exclusion criteria included patients with visual, hearing, and/or cognitive impairments, mental disorders, and/or a lack of willingness to continue participating in the study. Maximum variation sampling was used as the purposive sampling method. This sampling approach aimed to select participants with diverse experiences (in terms of age, gender, disease duration, marital status, education, employment, etc). Eligible participants were recruited from two outpatient clinics in Birjand and Kashmar, Iran.
Data Collection
Data were collected through in-person interviews. A total of 20 interviews were conducted (one participant was interviewed twice). At the beginning of the interviews, participants were asked introductory questions such as, “Please introduce yourself.” Subsequently, a semi-structured interview guide was used, consisting of open-ended key questions such as: “How has RA affected the different aspects of your life?”, “How has RA affected your and your family’s roles and responsibilities?” and “How has RA affected your relationship with your family members?” The interviews continued with follow-up questions such as, “Can you provide an example?” Finally, the interviews concluded with an open-ended question like, “Is there anything you feel is important regarding your family functioning and your illness that we haven’t asked about?” The interviews were conducted in a quiet and private setting and were audio-recorded. On average, the interviews lasted for 42 min. Data collection was guided by the principle of data saturation. Data saturation was reached after the 16th interview, when no new information emerged in subsequent interviews, the codes became repetitive, and no new concepts were added to the findings.16 Four additional interviews were conducted to confirm saturation had been achieved. Data collection and analysis began in February 2025 and concluded in July 2025.
Data Analysis
For data analysis in this study, we used the qualitative content analysis approach by Graneheim and Lundman.17 In the first stage, the text of all the recorded interviews was transcribed using Microsoft Word and then imported into MAXQDA 2020 software to facilitate systematic data management and analysis. In the second stage, the interview texts were read multiple times to gain a comprehensive understanding of their contents. In the third stage, the texts were read word by word and semantic units were identified. These semantic units were then coded as initial codes. In the fourth stage, the codes were classified into subcategories based on their similarities. In the final stage, the subcategories were grouped into main categories based on their semantic relationships, which were more abstract and conceptual. An example of the analysis process related to the category of “Compromised Marital Affairs” is presented in Table 1. Data analysis was conducted concurrently with data collection.
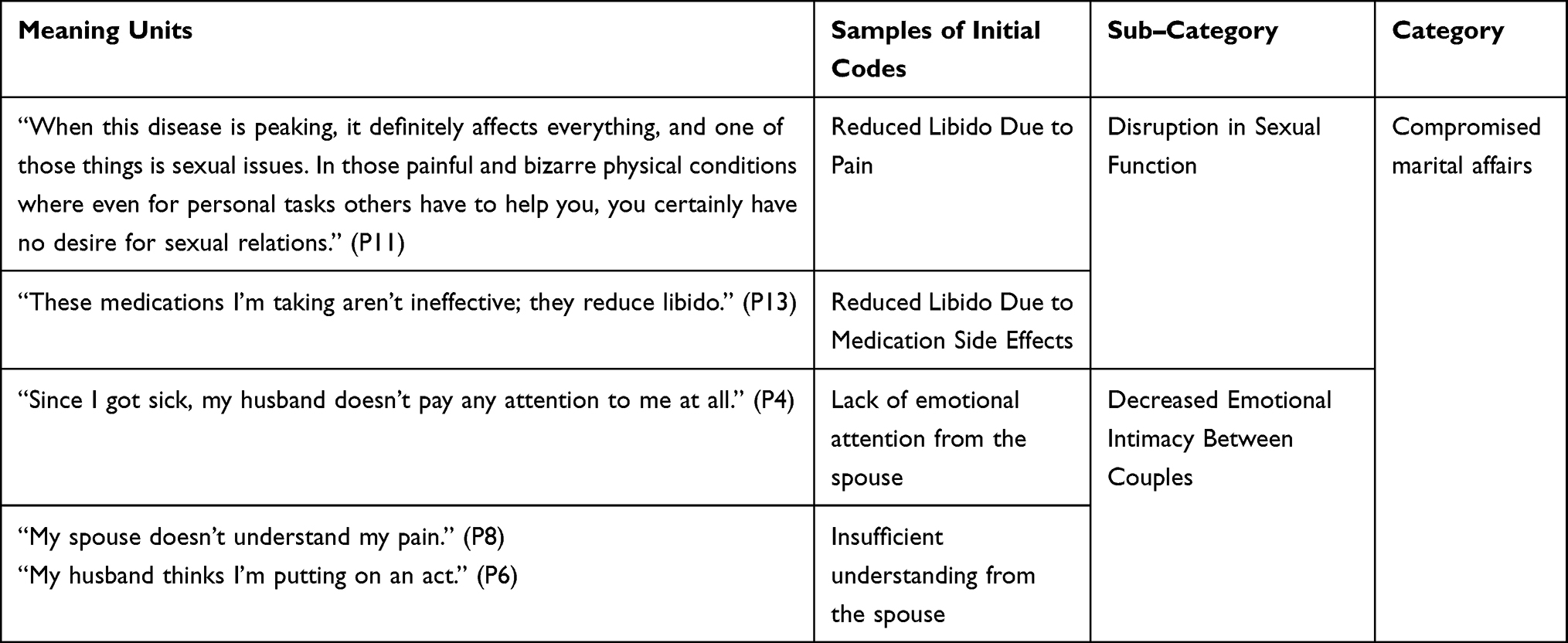 |
Table 1 Example of the Analysis, from a Meaning Unit to a Category |
Trustworthiness and Rigor of the Study
To ensure the trustworthiness of the data, the criteria proposed by Lincoln and Guba18 were applied in this study. Credibility was achieved through prolonged engagement with participants, sufficient time allocation for data collection, maximum variation sampling to capture diverse experiences, and member checking by seeking participants’ confirmation of coded data. Dependability was enhanced through repeated data analyses and peer debriefing with the supervisor and advisor to ensure the consistency of findings. Transferability was supported by providing participants’ characteristics, and all stages of the study, enabling the readers to determine the applicability of the findings to other contexts. Confirmability was established by maintaining an audit trail, sharing transcripts, codes, and categories with other research team members, and obtaining their agreement on the coding process.
Results
A total of 19 participants (11 women and 8 men) were included. Participant characteristics are shown in Table 2. Data analysis yielded 516 initial codes, resulting in six categories and 15 subcategories (Table 3).
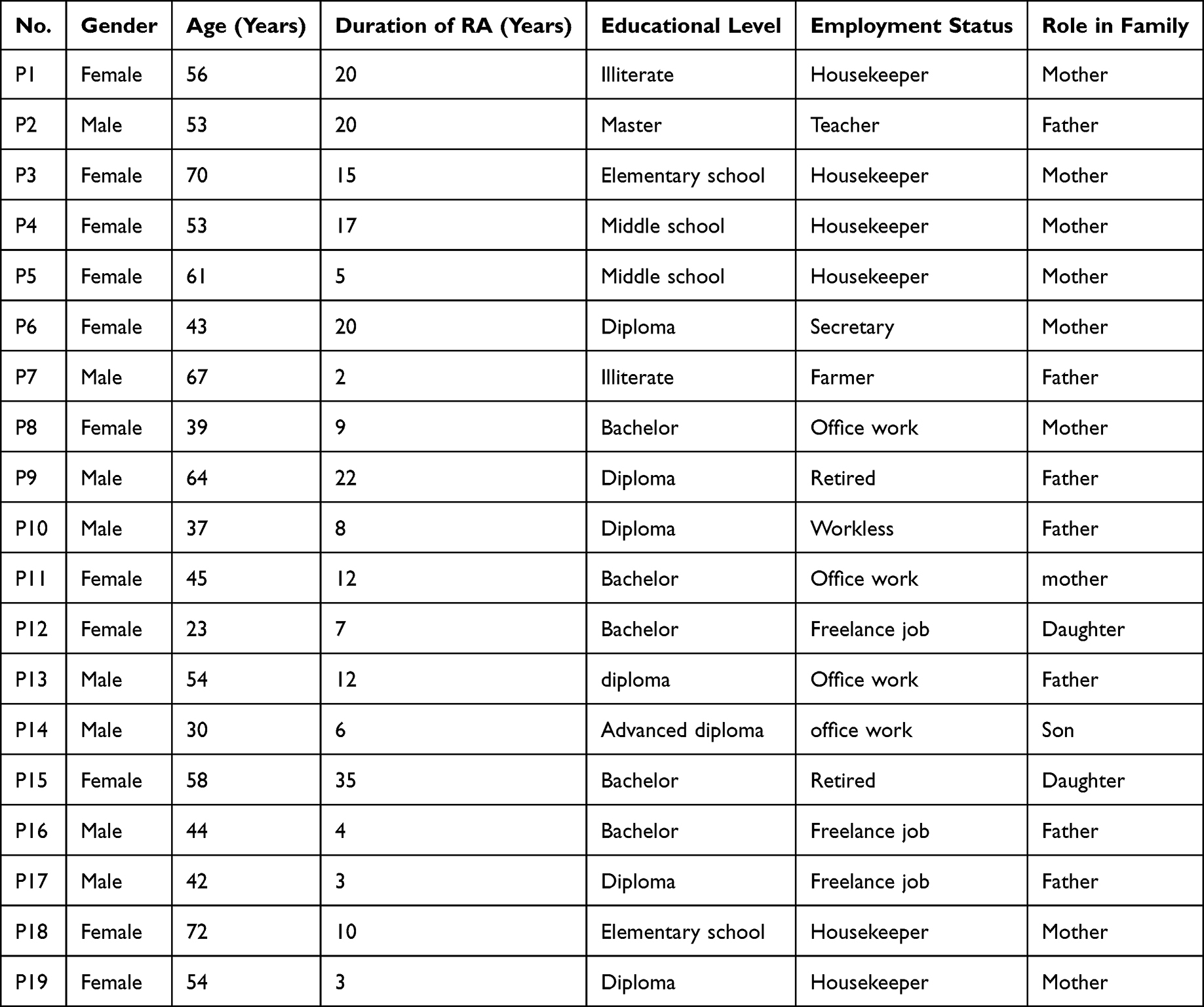 |
Table 2 RA Participants’ Characteristics |
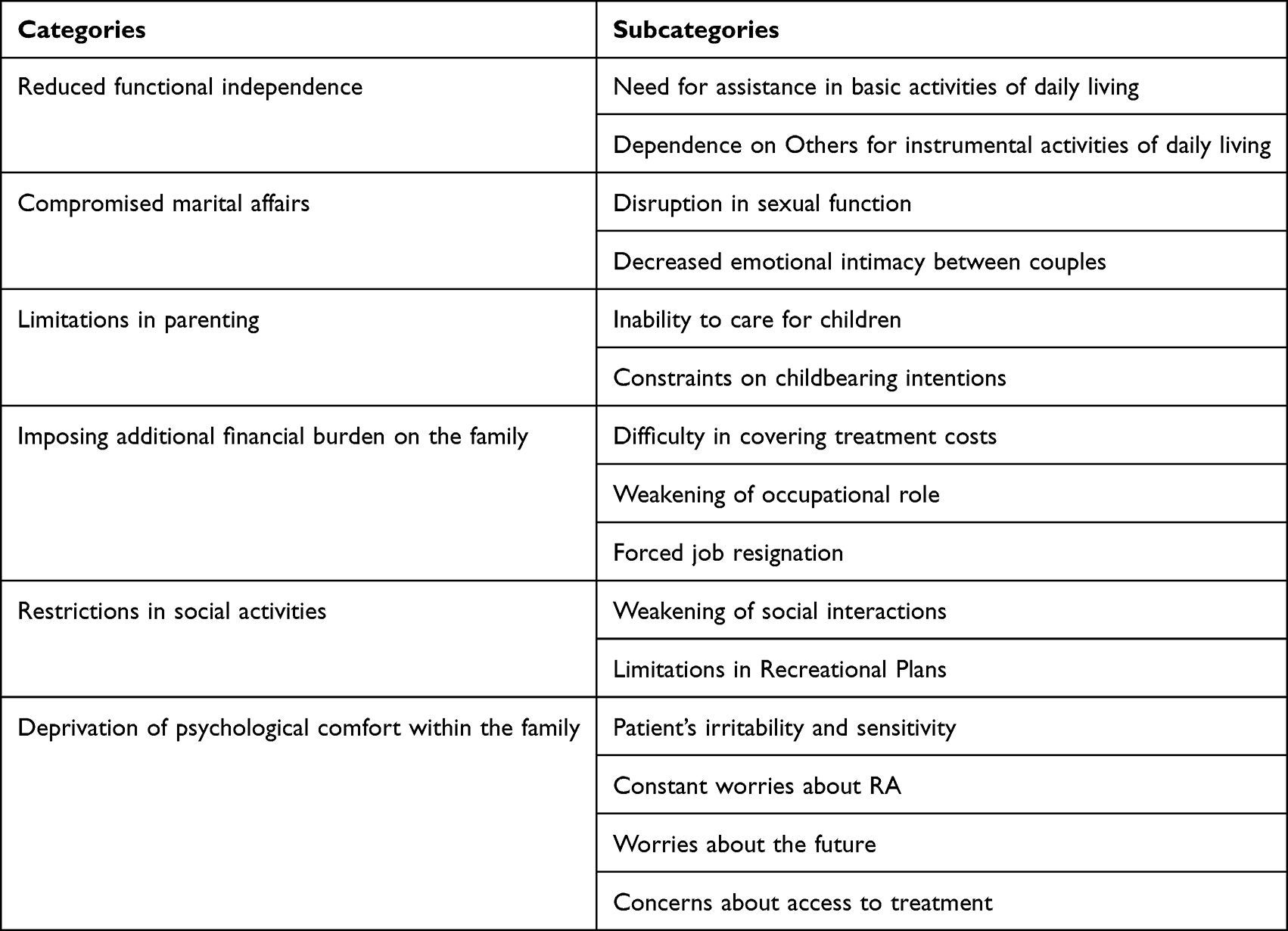 |
Table 3 The Categories and Subcategories Emerging from the Findings |
Although standardized clinical metrics, such as disease activity scores, were not formally collected, the participants’ narratives consistently indicated a high level of clinical severity. Most participants experienced daily, debilitating pain and significant joint stiffness that limited their mobility. Several individuals spoke of visible joint deformities in their hands and feet, and a substantial portion were receiving biologic therapies, which are typically prescribed for moderate-to-severe RA cases. This indicates that the sample was largely composed of individuals with significant and long-standing disease burdens.
Participants’ family compositions varied but predominantly involved nuclear households (spouse and/or children), with substantial practical and emotional contributions from extended family members in most cases. For example, adult children or in-laws often assisted with activities of daily living, transportation, or financial support for treatment purposes.
Reduced Functional Independence
Most participants faced challenges in basic or instrumental daily activities due to disease limitations, increasing dependence on others. Subcategories: “Need for Assistance in Basic Activities of Daily Living” and “Dependence on Others for Instrumental Activities of Daily Living.”
Need for Assistance in Basic Activities of Daily Living
Participants with chronic pain, limited mobility, and fatigue required help for tasks like bathing or moving at home.
Example: “Because my legs were in so much pain, my sons would carry me up and down stairs.” (P 7)
Another: “Now someone has to hold my hand to help me walk. I cannot get up alone.” (P 3)
Dependence on Others for Instrumental Activities of Daily Living
Many could not perform complex tasks like housekeeping or errands independently, relying on family. Female participants in traditional homemaker roles described acute disruption in household tasks, whereas male participants emphasized mobility limitations affecting outdoor duties.
Example: “... After washing two dishes, I have to rest for ten minutes.” (P 6)
Another: “I mostly go shopping with my wife to avoid joint pressure.” (P 2)
Compromised Marital Affairs
RA caused emotional, psychological, and physical changes affecting spouses. Subcategories: “Disruption in Sexual Function” and “Decreased Emotional Intimacy Between Couples.”
Disruption in Sexual Function
Participants reported reduced desire, pain during/after intercourse, and unsatisfactory relations.
Example: “After sexual intercourse, it feels like my hands and feet are going to break.” (P 10)
Another: “When in pain, my sexual desire decreases due to mental preoccupation.” (P 8)
Decreased Emotional Intimacy Between Couples
Female participants more often highlighted emotional intimacy gaps, such as their spouses’ lack of understanding.
Example: “My spouse sometimes understands me, but there are also many times when he does not. For example, regarding the pain I have, he says, ‘Well, what can I do? How long do I have to endure this?” (P 12)
Limitations in Parenting
Concerns about parenting and childbearing emerged. Subcategories: “Inability to Care for Children” and “Constraints on Childbearing Intentions.”
Inability to Care for Children
Many were dissatisfied with inability to perform their children’s caregiving tasks due to RA limitations. Concerns about parenting were expressed more frequently by women.
Example: “I couldn’t take my child to kindergarten in the mornings due to pain, so my husband did it.” (P 11)
Constraints on Childbearing Intentions
Disease and medications influenced reluctance to conceive, fearing complications or inability to parent. Younger mothers expressed guilt over their inability to care for their children and childbearing constraints, intensified by societal pressures on women for reproduction.
Example: “My family kept saying, ‘Have another child,’ but I was afraid I could not take care of it. I did not want to have a child who would feel deprived. So, I decided to give up on it altogether.” (P 8)
Imposing Additional Financial Burden on the Family
Ongoing treatment costs, reduced income, and job loss created financial pressure. Subcategories: “Difficulty in Covering Treatment Costs,” “Weakening of Occupational Role,” and “Forced Job Resignation.”
Difficulty in Covering Treatment Costs
High costs distressed families. Female participants who were not primary earners more often expressed feelings of guilt and of being a financial liability to their spouses or children.
Example: “My husband is a worker and spends his earnings on my illness; I get upset.” (P 1)
Weakening of Occupational Role
Limitations hindered work tasks.
Example: “As a teacher, I can’t play with kids or move much.” (P 2)
Another: “Working with a keyboard makes my fingers lose sensation.” (P 6)
Forced Job Resignation
Severe symptoms led to temporary or permanent resignation.
Example: “I used to farm daily, but now if I go one day, I rest for two.” (P 7)
Restrictions in Social Activities
RA reduced social roles and participation in events. Subcategories: “Weakening of Social Interactions” and “Limitations in Recreational Plans.”
Weakening of Social Interactions
Consequences limited communication and relationships.
Example: “I wait until the day before a party to decide based on my condition.” (P 6)
Another: “I can only sit briefly at parties, so I skip many.” (P 2)
Limitations in Recreational Plans
Pain and fatigue reduced family outings.
Example: “Going Mountaineering with my family on weekends is beyond my capacity.” (P 2)
Deprivation of Psychological Comfort Within the Family
Participants described how the constant presence of RA, through its physical symptoms and uncertainties, contributed to a pervasive atmosphere of psychological distress that undermined the family’s role as a source of comfort and security for the patients. This deprivation of psychological comfort was not a single feeling but a complex phenomenon resulting from a cascade of stressors that were interrelated. It encompassed the patient’s irritability and sensitivity, Constant worries about RA, Worries about the future and Concerns about access to treatment. As reflected in the participants’ accounts, these elements collectively contributed to an environment of tension and worry that affected the entire family, as detailed in the following subcategories.
Patient’s Irritability and Sensitivity
Participants reported that their tolerance for daily stressors had decreased, which they primarily attributed to persistent pain, fatigue, and the overall burden of living with RA. This reduced tolerance, they felt, led to emotional reactions and contributed to tensions within the family.
Example: “I get very nervous (accompanied by crying). (My family members) cannot really talk to me much. Before the illness, I was the calmest person in my family, but now I get upset and fall apart with the slightest conversation.” (P 13)
Constant Worries About RA
Uncertainties about cause and cure caused anxiety. Younger participants expressed more shock, uncertainty, and concerns about RA.
Example: “I am still amazed at why I got sick. What is the root cause of the disease that causes this to occur in the body? Well, I still think this is very undiscovered.” (P 11)
Another: “I always think about how long this illness is going to last. Isn’t there a cure for this illness? I mean, isn’t there any doctor who can completely heal this disease with a specific medication?” (P 14)
This internal preoccupation with the disease often translated into a tense family atmosphere, as patients either withdrew emotionally or required constant reassurance, straining the family’s ability to maintain a sense of normalcy in their lives.
Worries About the Future
Fears of worsening symptoms and frailty persisted. Concerns about the future were greater among younger participants.
Example: “I’m terrified of turning 50 and becoming frail without help.” (P 8)
This fear of future dependence was a significant source of personal anxiety that cast a shadow over the family, creating a shared sense of dread about what was to come.
Concerns About Access to Treatment
The logistical and systemic challenges of securing consistent treatment served as a major external shock to the families’ psychological well-being. The uncertainty of obtaining necessary medications, as one participant described, created acute periods of anxiety and helplessness that rippled through their household.
Example: “A few weeks ago, the Remicade drug was not available; no pharmacy had it. It had become strangely scarce. I was unsure whether I would be able to find the drug. Until finally the drug reached me, my left knee had become severely swollen and painful.” (P 11)
Another: “One of the other dilemmas we have is that our doctors, as soon as they complete their service years, they get a transfer and leave here. The next novice doctor takes a lot of time to get up to speed on the course of my disease.” (P 2)
Discussion
The findings of the present study indicate that patients with RA perceive extensive and predominantly negative changes in their family functioning. These changes were categorized into six main categories: Reduced functional independence, compromised marital affairs, limitations in parenting, imposing an additional financial burden on the family, Restrictions in social activities, and deprivation of psychological comfort within the family. These results are consistent with previous studies that demonstrated the impact of chronic diseases on various dimensions of family life.13,14 As these results were derived from a specific cultural setting, they are most applicable to societies with strong family based caregiving cultures, such as Iran. Indeed, the focus of this study on the cultural context of Iran, where families have traditional structures and high dependency,19 highlights localized aspects that are less addressed in other studies.
The findings of this study, which exclusively focused on the perspectives of patients with RA, provide a deep insight into their experience of altered family functioning. The overarching theme from the patients’ narratives is a profound sense of loss and disruption across multiple domains, from daily activities to intimate relationships. Our finding that patients perceive a significant loss of functional independence aligns with previous research,14,15 however, our study adds that from the patient’s viewpoint, this loss is primarily interpreted through the lens of becoming a burden on their family. Women more frequently described intense disruptions in instrumental daily activities, such as performing housekeeping, reflecting traditional Iranian gender expectations, where women predominantly manage domestic responsibilities.20 The challenges reported by patients suggest that educational programs aimed at training family caregivers may be beneficial, and these could potentially be delivered by healthcare providers.
Compromised marital affairs and limitations in parenting were other findings. Our findings revealed that compromised marital affairs, characterized by decreased emotional and sexual intimacy, were significant sources of distress for patients. This aligns with the literature documenting the negative impact of chronic pain and disability on marital relationships.3,14 However, this trajectory of compromised marital affairs is not universal in the literature. For instance, research on dyadic coping has shown that collaborative coping and mutual support between partners are significant sources of resilience. A study by Mittinty et al (2024) demonstrated that supportive dyadic coping in couples with RA was associated with higher relationship quality and better psychological well-being for both the patient and spouse.21
Women more often framed limitations in parenting and marital intimacy as personal failures within traditional Iranian gender norms, consistent with a narrative review highlighting intensified caregiving expectations for women in Middle Eastern contexts.22 In Iranian culture, where marriage and childbearing hold high value, these limitations may lead to deeper emotional pressures and threaten family stability.23 The concern about medication effects on the fetus aligns with global recommendations to avoid pregnancy while taking drugs like methotrexate.24 The distress surrounding marital affairs and fertility suggests that incorporating sexual and fertility counseling into routine treatment discussions is a potential area for practice development that may help manage challenges and improve marital satisfaction.
From the patients’ viewpoint, imposing an additional financial burden on the family involved difficulties in treatment costs, weakened occupational roles, and forced job resignations. Men more frequently connected occupational weakening to diminished family provider status. These nuances align with the broader literature on the gendered impacts of chronic illness in patriarchal settings, where role disruptions challenge culturally valued identities differently.25,26 While economic hardship is a well-documented consequence of RA globally,27,28 the severity and nature of the burden described in our study appear distinct. For example, studies conducted in European nations with universal healthcare and robust social safety nets tend to focus on indirect costs.29 However, this pressure takes on more complex dimensions within the economic context of Iran, which grapples with chronic inflation and limitations from international sanctions. As one participant noted the difficulty of obtaining foreign medications, these challenges transcend personal costs and become a structural issue that directly impacts the family’s ability to manage the disease. One potential approach could be the routine assessment of financial burden in clinics and the creation of clearer referral pathways for subsidized treatments.
Limitations in social activities indicate challenges in maintaining social relationships and participating in leisure activities. These findings are consistent with studies where RA patients report reduced social participation, leading to isolation and negative impact on quality of life.30,31 In Iranian families, where collective recreation is cultural, these limitations can cause collective deprivation and weaken emotional support. The profound impact on social participation found in our study implies that policymakers should consider the development of accessible recreational facilities as a potential means of reducing social deprivation and improving well-being in this patient group.
Finally, deprivation of psychological comfort within the family, while conceptually broad, accurately reflects the lived realities of patients and their families. Our findings suggest that the erosion of psychological well-being is not caused by a single factor but by a cascade of interconnected stressors. External pressures, such as inconsistent access to treatment, fuel internal patient anxieties about the disease and its progression. These worries can manifest as irritability and emotional distress, creating tension in family interactions. As a further implication for policy, the experiences of irritability and family tension described by the participants suggest that strategies aimed at helping families manage psychological stress could be beneficial. Similarly, the widespread concern over treatment access highlights that a continued focus on improving the availability and consistency of care is critical for health policy.
The strengths of this study include its use of a qualitative approach to capture the in-depth lived experiences of patients with RA. However, this study has several limitations. First, the findings are based on a sample of 19 participants from a limited geographic area within Iran, which may influence their transferability to other cultural contexts. Second, this study explored family functioning exclusively from the patient’s perspective. Family functioning is inherently interactive, and reliance on a single viewpoint may introduce information bias. Therefore, the findings should be understood as a reflection of the patients’ personal experiences and perceptions of change rather than a comprehensive, objective assessment of family functioning. Future research would benefit greatly from employing a dyadic or family systems approach that includes interviews with spouses, children, or other family members to provide a more holistic understanding.
Conclusion
Within the Iranian cultural context, characterized by strong family based caregiving, patients with RA perceived that the disease significantly impacted family functioning across the physical, psychological, social, and economic domains. These findings underscore the potential value of a family centered approach in community-oriented care, where nurses and midwives consider the family as a broader unit of care. The results indicate that interventions focused on education, counseling, and psychosocial support could be promising avenues for future research aimed at helping patients and their families adapt to the disease and maintain their well-being.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
Approval was obtained from the Ethics Committee of Birjand University of Medical Sciences (Ethics No: IR.BUMS.REC.1403.041) prior to the investigation. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Consent for Publication
All participants provided written informed consent, including permission to publish anonymous responses and direct quotes.
Acknowledgments
The authors thank all participants for their valuable time and insights.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Black RJ, Cross M, Haile LM. GBD. 2021 rheumatoid arthritis collaborators. global, regional, and national burden of rheumatoid arthritis, 1990–2020, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 2023;5:e594–10. doi:10.1016/s2665-9913(23)00211-4.
2. Sadawy Salim A, Elsayed Mahdy N, Mohamed Khorais A, et al. Quality of life for patients with rheumatoid arthritis. Egy J Health Care. 2024;15(1):250–262. doi:10.21608/ejhc.2024.339292
3. Hamdi O, Jemmali S, Boussaid S, et al. POS1515-HPR conjugal relationships in married patients with chronic inflammatory rheumatisms. Ann Rheumatic Dis. 2022;81(1):1102–1103. doi:10.1136/annrheumdis-2022-eular.428
4. Unif DS, Sitiawari W. Family support and rheumatoid arthritis management in Lamongan: a mixed-methods study. Indonesian Nurs J. 2025;2(2):65–71. doi:10.31962/inj.v2i2.296
5. Bennich BB, Munch L, Overgaard D, et al. Experience of family function, family involvement, and self-management in adult patients with type 2 diabetes: a thematic analysis. J Adv Nurs. 2020;76(2):621–631. doi:10.1111/jan.14256
6. Dai L, Wang L. Differences in family functioning before and during the COVID-19 pandemic: an observational study in Peruvian families. PeerJ. 2023;8(11):e16269. doi:10.7717/peerj.16269
7. Hejazi SS, Hosseini M, Ebadi A, et al. Family caregiver: the forgotten savior. Int J Comm Based Nurs Midwifery. 2021;9(4):346–347. doi:10.30476/ijcbnm.2021.90118.1673
8. Zhang Y. Family functioning in the context of an adult family member with illness: a concept analysis. J Clin Nurs. 2018;27(16):3205–3224. doi:10.1111/jocn.14500
9. Hansen CW, Nørgaard MW, de Thurah A, et al. Significant others in inflammatory arthritis: roles, influences, and challenges-a scoping review. Rheumatol Int. 2024;44(10):1849–1859. doi:10.1007/s00296-024-05639-9
10. Whitehead L, Jacob E, Towell A, et al. The role of the family in supporting the self-management of chronic conditions: a qualitative systematic review. J Clin Nurs. 2018;27(1–2):22–30. doi:10.1111/jocn.13775
11. Li J, Kong X, Wang J, et al. Family functioning and patients’ depressive symptoms: comparison in perceived family function between patients who had an acute ischaemic stroke and their primary family caregivers - a cross-sectional study. BMJ Open. 2023;13(11):68794. doi:10.1136/bmjopen-2022-068794
12. Jahani S, Haghighi S, Ansari S, et al. The lived experiences of iranian patients with rheumatoid arthritis: a qualitative research. Iran J Nurs Midwifery Res. 2022;27(3):204–210. doi:10.4103/ijnmr.ijnmr_84_21
13. Madani FS, Zarani f, zarani F. Managing chronic illness in the family: a systematic review. J Family Res. 2022;18(1):57–73. doi:10.52547/JFR.18.1.57
14. Poh LW, He HG, Chan WCS, et al. Experiences of patients with rheumatoid arthritis: a qualitative study. Clin Nurs Res. 2017;26(3):373–393. doi:10.1177/1054773816629897
15. Sabaz Karakeci E, Çetintaş D, Kaya A. Association of the commitments and responsibilities of the caregiver within the family to the disease activity in patients with rheumatoid arthritis: a report from Turkey. Arch Rheumatol. 2018;33(2):213–220. doi:10.5606/archrheumatol.2018.6427
16. Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. 2018;52(4):1893–1907. doi:10.1007/s11135-017-0574-8
17. Graneheim UH, Lindgren BM, Lundman B. Methodological challenges in qualitative content analysis: a discussion paper. Nurse Educ Today. 2017;56:29–34. doi:10.1016/j.nedt.2017.06.002
18. Amin MEK, Nørgaard LS, Cavaco AM, et al. Establishing trustworthiness and authenticity in qualitative pharmacy research. Res Social Administrative Pharm. 2020;16(10):1472–1482. doi:10.1016/j.sapharm.2020.02.005
19. Lohrasbi F, Maghsoudi J, Alavi M, et al. Care Bermuda, families of the patients with chronic mental disorders in Iran surrounded by psychosocial problems and needs: a qualitative study. Ann Med Surg Lond. 2024;86(6):3357–3366. doi:10.1097/ms9.0000000000000626
20. Yoosefi Lebni J, Mohammadi Gharehghani MA, Soofizad G, et al. Challenges and opportunities confronting female-headed households in Iran: a qualitative study. BMC Womens Health. 2020;20(1):183. doi:10.1186/s12905-020-01046-x
21. Mittinty MM, Mittinty MN, Buchbinder R, et al. Interpersonal process of dyadic coping in rheumatoid arthritis: a perspective from the australian rheumatology association database. J Rheumatol. 2024;51(9):862–869. doi:10.3899/jrheum.2023-0664
22. Al-Namla M, Mahboob A, Radwan E, et al. A narrative review of challenges faced by informal caregivers of people with dementia in the Middle East and North Africa. Front Med. 2025;12:1610957. doi:10.3389/fmed.2025.1610957
23. Behjati-Ardakani Z, Navabakhsh M, Hosseini SH. Sociological study on the transformation of fertility and childbearing concept in Iran. J Reprod Infertil. 2017;18(1):153–161.
24. Birru Talabi M, Clowse MEB. Antirheumatic medications in pregnancy and breastfeeding. Curr Opin Rheumatol. 2020;32(3):238–246. doi:10.1097/bor.0000000000000710
25. Peiró AM, Carracedo P, Agulló L, et al. Gendered dimension of chronic pain patients with low and middle income: a text mining analysis. PLoS One. 2024;19(12):e0311292. doi:10.1371/journal.pone.0311292
26. Flurey C, White A, Rodham K, Kirwan J, Noddings R, Hewlett S. et al’Everyone assumes a man to be quite strong’: men, masculinity and rheumatoid arthritis: a case-study approach. Sociol Health Illness. 2018;40(1):115–129. doi:10.1111/1467-9566.12628
27. Huang Y, Li J, Agarwal SK. Economic and humanistic burden of rheumatoid arthritis: results from the us national survey data 2018-2020. ACR Open Rheumatol. 2024;6(11):746–754. doi:10.1002/acr2.11728
28. Rezaee M, Lotfi F, Gholami A, et al. Economic burden of rheumatoid arthritis in Iran: a societal perspective economic burden of R.A. Res Square. 2022. doi:10.21203/rs.3.rs-1257689/v1
29. Bowman SJ, Guest L. The national clinical audit for rheumatoid and early inflammatory arthritis. Clin Med. 2016;16(6):500–501. doi:10.7861/clinmedicine.16-6-500
30. Suh CH, Lee K, Kim JW, et al. Factors affecting quality of life in patients with rheumatoid arthritis in South Korea: a cross-sectional study. Clin Rheumatol. 2022;41(2):367–375. doi:10.1007/s10067-021-05944-9
31. Cano-García L, Mena-Vázquez N, Manrique-Arija S, et al. Ability to participate in social activities of rheumatoid arthritis patients compared with other rheumatic diseases: a cross-sectional observational study. Diagnostics. 2021;11(12):2258. doi:10.3390/diagnostics11122258
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Expectations and Experiences of a Group of Patients Enrolled in an Educational Program for Rheumatoid Arthritis at a Specialized Care Center in Colombia
Castiblanco-Montañez RA, Buitrago-Garcia D, Arévalo Velandia A, Garzón-Cepeda JD, Rodríguez-Florido F, Sánchez Vanegas G, Santos-Moreno P
Journal of Multidisciplinary Healthcare 2023, 16:483-492
Published Date: 22 February 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Exploring Information Needs and Perspectives on a Patient Decision Aid for Biologic Therapy: A Qualitative Interview Study Among Individuals with Rheumatoid Arthritis
Rai SK, McCormick N, Yokose C, De Vera MA, Li LC, Choi HK
Patient Preference and Adherence 2026, 20:565490
Published Date: 23 June 2026