Back to Journals » Risk Management and Healthcare Policy » Volume 16
Experience Sharing on Continuity of Healthcare Services in Internally Displaced Peoples: The Case of Tigray War Crisis
Authors Haftu H ![]() , Weledegebriel MG
, Weledegebriel MG ![]() , Gebre-egziabher A
, Gebre-egziabher A ![]() , Gebrehiwot T
, Gebrehiwot T ![]() , Zenebe D, Berhe B, Gebremeskel H, Melese F, Gebretsadik S
, Zenebe D, Berhe B, Gebremeskel H, Melese F, Gebretsadik S
Received 19 July 2023
Accepted for publication 12 October 2023
Published 20 October 2023 Volume 2023:16 Pages 2197—2208
DOI https://doi.org/10.2147/RMHP.S426627
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Hansa Haftu,1 Migbnesh Gebremedhin Weledegebriel,2 Abraha Gebre-egziabher,1 Teklu Gebrehiwot,3 Dawit Zenebe,4 Bereket Berhe,1 Hailay Gebremeskel,2 Freweini Melese,5 Simon Gebretsadik6
1Department of Pediatrics and Child Health, College of Health Sciences, Mekelle University, Tigray, Ethiopia; 2Department of Internal Medicine, College of Health Sciences, Mekelle University, Tigray, Ethiopia; 3Department of Clinical Pharmacy, College of Health Sciences, Mekelle University, Tigray, Ethiopia; 4Department of Epidemiology, College of Health Sciences, Mekelle University, Tigray, Ethiopia; 5Department of Gynaecology and Obstetrics, College of Health Sciences, Mekelle University, Tigray, Ethiopia; 6Department of Treatment Division, Tigray Regional Health Bureau, Tigray, Ethiopia
Correspondence: Hansa Haftu, Mekelle University, Tigray, Ethiopia, Tel +251-948-487-877, Email [email protected]
Abstract: The war and siege in Tigray led millions to displace internally. More than three-fourths of the health facilities were either destroyed or not functional as the equipment and other resources were stolen. Furthermore, the remaining functioning health facilities were flooded beyond their capacity, resulting in many patients received treatment late, and ending with complications including life loss. Mekelle City is one of the largest towns with many internally displaced people from different areas of Tigray. To provide services for the most vulnerable populations, 11 IDP clinics were opened for internally displaced people and the surrounding host community in Mekelle. A total of 6732 patients received clinical services, of which 3465 were males. The age of the patients was in ranged of 24 days to 95 years. A total of 364 patients were emergency cases and 428 outbreaks were seen. A total of 722 patients with chronic illnesses received follow-up services, the most common being hypertension (112), diabetes (79), and asthma (70). Overall, 1198 investigations were done and 1339 were referred to higher-level healthcare facilities. Upper respiratory infection (n = 976), acute gastroenteritis (n = 667), and pneumonia (n = 612) were the most common disease conditions in IDP clinics. Antibiotics were the most commonly prescribed medication for 2468 patients, followed by anti-pain/pyretic (1402). This community engagement showed us that, it is possible to continue healthcare services when health facilities get collapsed during crisis owing to the relocation and mobilization of available resources.
Keywords: health care, emergency, crisis, war, internally displaced peoples
Introduction
War is a manmade enemy of the health system with both direct and indirect consequences. The conflict not only destroys the health system but also shunts all the limited resources to weaken health facilities. In addition to the immediate casualties and injury of individuals in the battlefield, it also breaks down the family, society, and culture of the community, causing significant health burden and increased mortality. Data from previous conflict-affected countries showed that, due to displacements, overcrowding, and a shortage of prevention mechanisms, communicable diseases have alarmingly increased with significant mortality.1,2
Tigray is one of the states in Ethiopia found in the northern part and had the better health system before the war.3,4 Since the war and siege broke out in November 2020, thousands of deaths, rapes, and millions were displaced by Ethiopian forces and allies (Eritrean forces, Amhara militia, Amhara fano, and others).5 Hundreds of civilian’s deaths related to direct shelling, air/drone strikes, armed men attack, blasts and landmines were being reported by our clients that were fortunate enough to come to Ayder Comprehensive Specialized Hospital (ACSH) for treatment. Tegaru was displaced in every corner of Tigray; more than 2.5 million were reported to be internally displaced and 5.2 (91%) of the people needed emergency humanitarian assistance.6 Internally displaced people (IDP) were among the most vulnerable; all were at risk of hunger, lack of shelter, lack of access to clean and potable water, lack of basic medical care, risk of gender-based violence, and other forms of violence (repeated reports of attempted sexual abuse by armed men), and lack of hygiene and sanitation.1
More than three-fourths (70–80%) of the health facility were destroyed and looted by the Ethiopian National Defence Forces and their allies (Eritrean Forces, Amhara Fano, and Militia). Due to deliberate health facility destruction and looting, Tigray remained with very limited space to provide health services.4 Mekelle accommodated more than 150,000 internally displaced people (IDPs), including community-hosted.7 Many were sheltered in approximately 26 government and private schools. Functioning health facilities which were limited around Mekelle were flooded with critical patients from every corner of the state including from internally displaced people (IDP) and overwhelmingly burdened beyond the hospital’s capacity. Patients get treatment late and becoming complicated end up with death.
Therefore, alternative service areas, such as clinics, are important to provide the minimum service for the most in need. Thus, Mekelle University (MU), in collaboration with the Tigray Regional Health Bureau and Individual Voluntary Health Professionals, opened 11 IDP-Clinics for both displaced and community-hosted people, which were selected based on health demands and total population size. The team leaders of this project had regular meetings and discussions to set and plan how to run the clinic services (Figure 1). The main objectives of each clinic were emergency services, outpatient treatment that included follow-up of patients with chronic illness, referral linkage to higher medical services, active surveillance of outbreaks, telehealth and specialist on-site and phone consultations, antenatal care, and family planning.
 |
Figure 1 Sample photos of the members of the community intervention in meeting and discussion. |
Experience Sharing on the Establishment of Local IDP-Clinics During War Crisis
Volunteering healthcare professionals (MDs, nurses, midwives, etc.) in collaboration with the Tigray Regional Health Bureau (TRHB) visited the areas and produced relevant preliminary data via snapshot assessment to help stakeholders procure assistance. The assessment focused on under five children, pregnant and lactating mothers, the vaccination status of children, chronic medical illnesses, and disabilities.
Under five children were recorded 1420 of which 446 were evaluated; 19 had moderate acute malnutrition, and two had severe acute malnutrition (SAM). Of the 116 pregnant mothers assessed, three were found to be malnourished. Of the 214 lactating mothers, 41 were malnourished. The vaccination status of the children was assessed, and 152 children were eligible. Of these, 42 required catch-up, 63 not up to date, and 82 in the right timeline for vaccination. Gross assessment was performed for chronic medical illnesses. There were 222 patients with chronic medical illness; of these 39-hypertension, 31-HIV/AIDS, 31-Diabetes Mellitus, 27-Bronchial asthmas, 6-Tuberculosis and others. The patients were evaluated for disabilities and mental health conditions: 23 had visual related impairments, 18-mental illnesses, 6-hearing difficulties, and 61-musculoskeletal and congenital deformations. This baseline data assessment indicated a high demand for establishing clinics at all IDP sites to provide minimum medical care.
Based on the above assessment, 11 clinics were established in 11 of the 26 IDP schools that were selected based on health demand from preliminary surveys and population size of each IDP. The study sites were Adishimdhun, Adihaki, Ethio-China, Meserete, Kesate, Kisanet, Momona, Elala, Yekatit 11, Gerebtsedo, and Myweyni. More than 35,000 people lived inside and outside the selected IPD sites (Table 1).
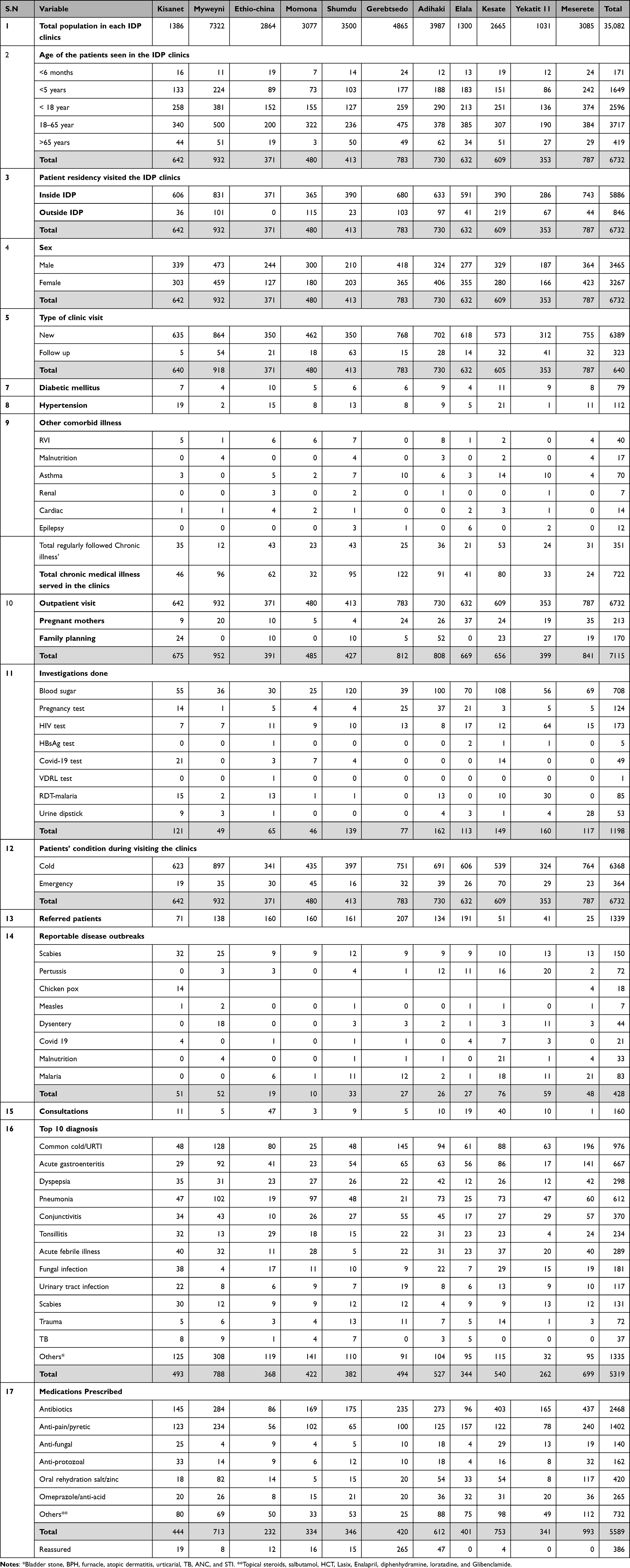 |
Table 1 Descriptive Results of the Intervention of Community Service in Each IDP Clinic Sites |
This project was run by the Mekelle University College of Health Sciences, Ayder Comprehensive Specialized Hospital (MU-CHS-ACSH), in collaboration with TRHB and UNICEF (emergency kits) for continuous supply. The duration of this project strengthens over a total course of the six months. First, clinics were established at the six IDP sites. After one month, clinical services were expanded to five additional sites, resulting in a total of 11 IDP clinics because of the high demand. Each clinic was fully furnished with furniture and sanitary (Figure 2) and stationery materials like registration books and prepared medical sheets (prescription sheets, patient cards, etc.) were distributed (SI-1). Guideline to detect disease outbreaks was also distributed to each clinic for early detection and management (SI-2).
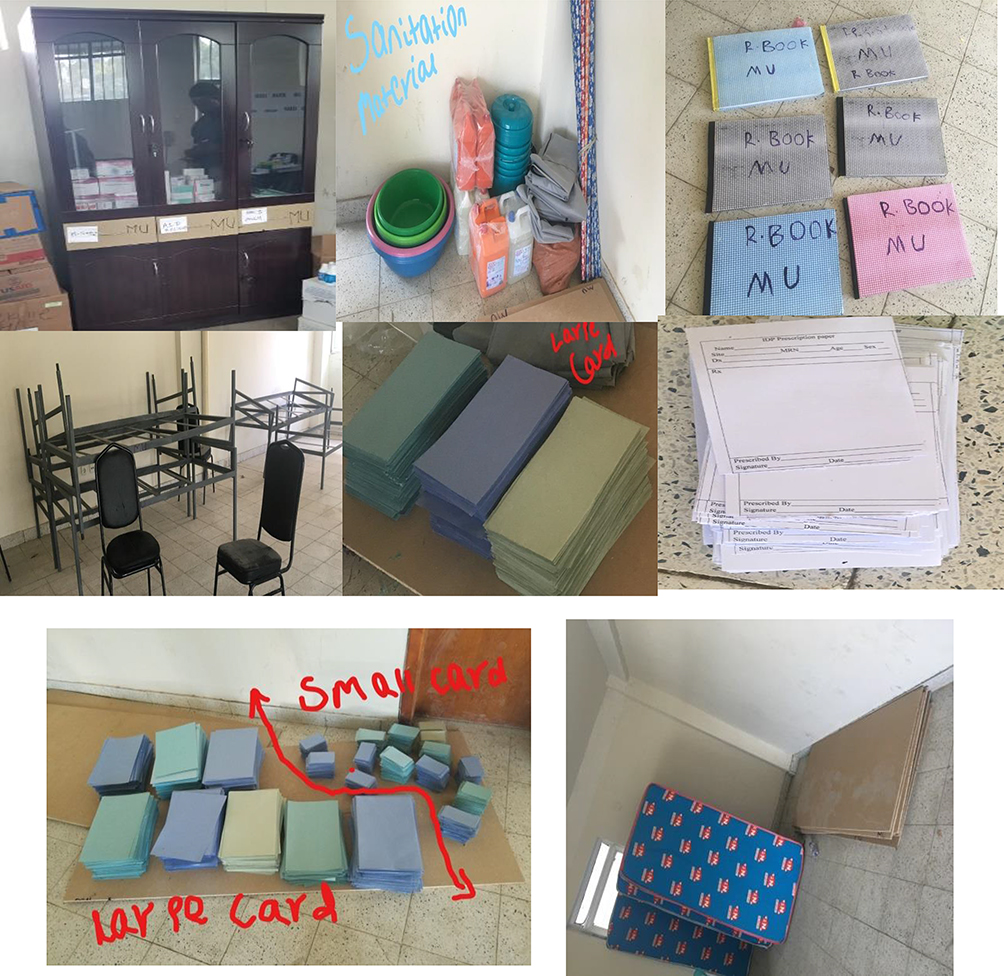 |
Figure 2 Sample distribution of sanitation materials, medical sheets, beds and registration books, medication shelf. |
Medication and medical equipment were also mobilized from MU and TRHB and distributed to different IDP clinics (Figure 3 and Tables S1–S5). All IDPs were also given a laminated a guideline about the definition of different disease outbreaks and reportable disease (SI-2). Different levels of health professionals were deployed to each IDP clinic from the MU and TRHB. Each clinic had one general practitioner and a clinical nurse who were mobilized from the TRHB. These health professionals were active on a regular basis helping their patients (Figure 4) while volunteering specialist physicians working in Ayder Comprehensive Specialized Hospital (ACSH) were participating with daily phone consultations and onsite clinical services once per week when a patient was appointed (Figure 5).
 |
Figure 3 Sample arranging medication and medical equipment’s to distribute to each IDP clinics. |
 |
Figure 4 Sample interactions with IDP site responsible bodies, professionals providing services to clients in some of the IDP clinics like “May weyni”, “Elala” and “Ya katit II clinic”. |
 |
Figure 5 Specialist doctors evaluating patients in the IDP clinic. |
The beneficiaries of this service were the IDP community sheltered in selected schools in Mekelle City and the community-hosted IDP. All necessary working document preparations and availability were performed to provide the following services in each IDP clinic: emergency and outpatient medical care, referral linkage to higher health facilities, antenatal care, family planning, follow-up of patients with chronic illness, passive and active surveillance of disease outbreaks, bedside laboratory investigations (urine dipstick, RBS, HBsAg, HCAB, pregnancy test, PICT, malaria kit, and VDRL), necessary medication, and medical equipment. Data was collected from registration book which includes sociodemographic, clinical diagnosis, and investigation done and the treatment received by the patients.
Outcome Services Provision in the IDP-Clinics
Before the clinical service started, the team members (Figure 1) discussed it in consecutive meetings and prepared different medical sheets for the IDP clinics, such as registration books, patient cards, investigation sheets, history sheets, prescription sheets, referral sheets, and case definitions of disease outbreaks for early reporting, isolation, and early management. Training was provided to doctors hired for the IDP clinic. Furniture, stationery, sanitation materials, medication, and medical equipment were partially mobilized from Mekelle University, TRHB, and UNICEF. The remaining equipment and medications necessary for the clinic were purchased from the limited budget of the Mekelle University. The clinic was open for clients seven days a week and emergency ambulances at night. Accordingly, from the 11 IDP clinics, 6732 patients were observed at 11 IDP clinics. Among those, 3465 were male, and the age ranged from 24 days to 95 years, with 1649 (47%) around fifty percent were under five children. Of these patients, 364 were emergency cases and 1339 were referred to higher facilities. A total of 722 patients had chronic illnesses and received clinical services. The most common chronic illnesses were hypertension (n = 112), diabetes (n = 79) and asthma (n = 70). In addition to providing treatment for acute illnesses and follow-up for chronic illnesses, the clinics provided antenatal care to 213 mothers. 170-Family planning for clients of both sexes (male and female). A total of 428 patients were diagnosed with reportable disease outbreaks, with the highest burden of scabies (150), malaria (83), pertussis (72), and dysentery (44). In all the IDP clinics, 160 specialty consultations were conducted. The most common diagnoses in clinics were upper respiratory infection (URTI), acute gastroenteritis (AGE), and pneumonia, with frequencies of (976, 667, and 612), respectively (Table 1).
Basic investigation services were provided by all established clinics. A total of 1198 investigations were performed, of which blood sugar determination (708) was followed by HIV (173) and pregnancy (124) tests. Antibiotics were prescribed to 2468 patients, followed by anti-pain/pyretics (1402), and 386 were reassured. Table 1 summarizes the major services provided by clinics at each IDP site. The service provided helped us divert the burden of functional health facilities, mainly ACSH, to some extent, as patients were retained there. This experience may also guide the continuation of medical care until the destroyed health facilities are completely restored and the relocations of IDPs to where they want to live. It also provides early detection and appropriate treatment for outbreaks. Since the total duration of these clinics was six months, the clinics were handed over to the TRHB.
Conclusion and Recommendation
This project provided clinical services for more than 35,000 people (those who were living in the 11 Mekelle IDP sites), including free access to medication for those who had chronic medical illnesses, such as diabetes and hypertension, and onsite specialty services. Emergency cases and different disease outbreaks were identified, reported, and managed or referred early to the appropriate institutions. There was a smooth referral system between IDP clinics and health facility institutions. These timely services averted further morbidities and mortalities, with minimal expenses. In addition, there was a significant decrease in the patient load of the overburdened nearby institutions in Mekelle like ACSH, relieving the financial concerns of the displaced people as they have received the medications free, and nearby without transportation inside their camps, including specialty services.
This gave us insight into how to fill the gaps in basic health services during complex emergencies. During crises, the mobilization of local expertise, resources, and coordination can effectively and efficiently tackle health crises. This also teaches us how to utilize local resource allocation, including manpower, which should be started from the available assets.
This experience complements the available evidence that it is possible to continue clinical services in conflict-affected areas, where civilians are not the main targets of conflict. This was not true in Tigray, as many were massacred and forcefully displaced from different parts of Tigray. This makes it more difficult to expand services outside Mekelle, where the health dire is imminent. Therefore, to continue healthcare services in war-torn areas like Tigray, it is up to the international community to protect civilians from getting their rights, including healthcare. This highlights the need for authorities, health experts, institutions, and policymakers to continue such small clinics and mobile clinics to reach the health issue of our community and until relocation of displaced people as a bridge until destroyed health facilities are constructed and services resumed. Still, Tigray is under a worse health crisis, and nearly all the population is in terrible need of help; hence, government and non-government must think and mobilize small and mobile clinics to address the health deficit in every corner of Tigray until the destroyed health system reconstructs and resumes its function.
Strength and Limitation
This involved teamwork among MU, TRHB, and other partners and was supplemented by each other smoothly and in a timely manner. This is a practical problem-solving task with successful patient care that creates a strong referral system. There was also a significant shortage of medications, owing to budget limitations and subsidies. The project members were equally involved in their routine clinical and teaching activities, which overstretched them. Our main limitations were the communication blackout in the middle (after six months of implementation) of the project and the siege, which made it very difficult to continue services such as specialist phone consultations, continued provision of medication as transactions, and other services were cut off, and there was no transportation, which made continuous monitoring difficult. There was a significant problem in the documentation of the daily activities of the clinic, which underestimated the clinical work when expressed in numbers.
Abbreviations
IDP, Internally Displaced people, AGE, Acute gastroenteritis, CD, Communicable disease; TRHB, Tigray Regional Health Bureau; NCD, Non-Communicable disease; MUAC, Mid upper Arm Circumference; HIV, Human Immunodeficiency Virus; ACSH, Ayder Comprehensive Specialized Hospital; RBS, Random Blood Sugar; HBsAg, Hepatitis Surface Antigen; HCAB, Hepatitis C Antibody; PICT, Provider-initiated counselling and testing; VDRL, Venereal Disease Research Laboratory test.
Ethical Considerations and Consent for Publication
The study was approved by ethical review board of College of Health Sciences, Mekelle University, and informed consent was taken from each participant including to publish their image by blurring out identifiable faces and confidentiality was maintained. Our intervention and study were complied with Declaration of Helsinki.
Acknowledgment
I would like to thank Mekelle University, College of Health Science (all specialty departments for their willingness and services without hesitation) for their administration, pharmacy, and all project coordinators. I would like to thank the Tigray Regional Health Bureau and voluntary health professionals working in the IDPs.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No specific funding was found for publication.
Disclosure
No conflicts of interest in all the authors.
References
1. Debarre A. Hard to reach: providing healthcare in armed conflict. International Peace Institute; 2018.
2. Benjamin D. Healthy generation. War Public Health. 2007;7(3):1–16.
3. Central Statistical Agency. Ethiopian demographic health survey 2016. Addis Ababa and Calverton: Central Statistical Agency (Ethiopia) and ICF International; 2018.
4. Gesesew H, Berhane K, Siraj ES, et al. The impact of war on the health system of the Tigray region in Ethiopia: an assessment. BMJ Global Health. 2021;6(11):1–7. doi:10.1136/bmjgh-2021-007328
5. omnatigray.org, OMNA Tigray. Medical crisis in Tigray Destruction of Tigray’s helath care system November 2020-April 2021.
6. Plaut M. The International community struggles to address the Ethiopian conflict. RUSI News brief RUSI; 2021.
7. Briefing by Bureau of Labor and Social Affairs. Regional Health Bureau of Tigray; 2021.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.