Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Evolving Research Hotspots and Emerging Trends in Atopic Dermatitis and Inflammatory Bowel Disease: A Bibliometric Analysis
Authors Li Z ![]() , Deng C, Lu B, Chen F, Cao X, Fan J, Song Y
, Deng C, Lu B, Chen F, Cao X, Fan J, Song Y
Received 14 April 2026
Accepted for publication 12 June 2026
Published 26 June 2026 Volume 2026:19 616722
DOI https://doi.org/10.2147/CCID.S616722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Monica K. Li
Zhiquan Li,1 Chenwei Deng,1 Bingxuan Lu,2 Foling Chen,2 Xiyuan Cao,2 Jiwen Fan,1 Yu Song2
1Clinical Medical College, Jiangxi University of Chinese Medicine, Nanchang, Jiangxi, People’s Republic of China; 2Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
Correspondence: Yu Song, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, No. 725, Wanping South Road, Xuhui District, Shanghai, 200032, People’s Republic of China, Email [email protected]
Background: The number of people affected by atopic dermatitis (AD) and inflammatory bowel disease (IBD) continues to rise, increasing the disease burden. These conditions are epidemiologically linked and share features related to barrier dysfunction, immune dysregulation, and microbial dysbiosis, making them an important focus of integrated research. However, systematic bibliometric analysis of this field remains lacking. This study aimed to characterize the publication landscape, knowledge structure, evolving hotspots, and emerging translational trends in AD–IBD research.
Methods: English-language articles and reviews on the intersection of AD and IBD published between 2000 and 2025 were retrieved from the Web of Science Core Collection and Scopus. After merging, deduplication, and data standardization, CiteSpace, VOSviewer, and Scimago Graphica were used to analyze publication trends, country/region and institutional contributions, author and journal profiles, keyword co-occurrence, and co-cited references.
Results: A total of 1,542 publications were included. Annual publication output increased steadily, with a marked acceleration after 2020. The United States ranked first in publication volume, total citations, and international collaboration strength, while Harvard University occupied a central position in the institutional collaboration network. The Journal of Allergy and Clinical Immunology ranked first in both citation and co-citation counts. Keyword clustering and co-cited reference burst analyses identified four major directions: gut microecology and immune regulation, shared inflammatory pathways and immune-mediated comorbidities, therapeutic strategies involving biologics and JAK inhibitors, and genetic susceptibility and causal inference. The field has gradually shifted from epidemiological associations and inflammatory mechanism exploration toward clinical translation and safety evaluation.
Conclusion: AD–IBD research has evolved into a multidisciplinary field centered mainly in North America and Europe, with rapidly expanding contributions from Asia. Future studies should strengthen interdisciplinary and cross-regional collaboration and prioritize gut–skin axis mechanisms, stratified management of comorbid populations, and long-term risk–benefit assessment of targeted therapies.
Keywords: atopic dermatitis, inflammatory bowel disease, bibliometrics, visual analysis, gut–skin axis, JAK inhibitors
Introduction
Atopic dermatitis (AD) is a common chronic, relapsing inflammatory skin disease characterized by recurrent eczematous lesions and intense pruritus, with its pathogenesis closely linked to impaired skin barrier function and immune dysregulation.1 Inflammatory bowel disease (IBD), encompassing Crohn’s disease (CD) and ulcerative colitis (UC), represents a group of immune-mediated disorders characterized by chronic intestinal inflammation, similarly marked by a protracted and relapsing clinical course and substantial disease burden; its pathological processes involve disruption of the intestinal mucosal barrier, dysregulated immune responses, and persistent inflammation.2,3 In recent years, the global number of individuals affected by AD and IBD has continued to increase, with growing disease burden and long-term management needs, making both conditions important public health concerns.4,5 Although AD and IBD primarily affect the skin and intestinal mucosal epithelium, respectively, both are characterized by epithelial barrier dysfunction, chronic immune-inflammatory activation, and microbial dysbiosis, providing a biological rationale for investigating their potential association.6
The potential association between AD and IBD has attracted increasing attention. A systematic review and meta-analysis revealed a bidirectional epidemiological association between AD and IBD,7 and a large-scale population-based cohort study in the United Kingdom further confirmed that patients with AD have a significantly elevated risk of developing incident IBD, with this risk increasing in proportion to AD severity.8 Beyond epidemiological evidence, previous studies have explored the potential link between AD and IBD from multiple perspectives, including the gut–skin axis, Mendelian randomization-based causal inference, comparative molecular analyses, and shared therapeutic targets.9–12 Collectively, these findings indicate that cross-disciplinary research on AD and IBD is evolving from epidemiological observations toward mechanistic elucidation and therapeutic strategy development; however, the overall research landscape of this field has yet to be systematically characterized.
However, the aforementioned studies have largely focused on specific scientific questions and are dispersed across diverse disciplines, including dermatology, gastroenterology, microbial ecology, and genetic epidemiology. Consequently, a comprehensive, panoramic understanding of the overall research landscape, evolving hotspots, and emerging frontiers within this interdisciplinary field remains lacking.
Bibliometric analysis combined with visualization is a quantitative approach for elucidating the knowledge structure, evolutionary trajectory, collaboration networks, and emerging trends within a given research domain at the macroscopic level, and has been extensively applied to assess research landscapes in interdisciplinary medical fields.13,14 Accordingly, the present study retrieved English-language publications (articles and reviews) on the AD–IBD nexus from 2000 to 2025, using the Web of Science Core Collection and Scopus as data sources. Leveraging visualization tools such as CiteSpace and VOSviewer, we conducted analyses across multiple dimensions, including publication trends, country/region and institutional distributions, prolific authors and journals, keyword co-occurrence, and co-cited references. This study aims to systematically delineate the research landscape of this field, identify hotspot topics and frontier directions, and provide a reference framework for future mechanistic investigations, clinical translation, and interdisciplinary collaboration.
Materials and Methods
Data Sources and Search Strategy
In bibliometric research, the selection of data sources is critical to the reliability and completeness of the findings. WoSCC offers distinct advantages through its rigorous journal selection criteria and well-established citation indexing system, while Scopus complements it with broader disciplinary coverage and robust cross-domain retrieval capabilities. As any single database is subject to inherent coverage limitations, integrating both helps balance depth of indexing with breadth of disciplinary scope, minimizes potential retrieval omissions, and thereby provides a more robust data foundation for the present study.
The literature search and data collection were completed in WoSCC and Scopus on March 27, 2026. The publication period was set from January 1, 2000, to December 31, 2025. In WoSCC, the Topic field was searched using the following complete search string: TS=((“atopic dermatitis” OR “atopic eczema” OR “atopic neurodermatitis” OR “atopic dermatit*” OR “atopic eczem*”) AND (“inflammatory bowel disease*” OR “Crohn’s disease” OR “Crohn disease” OR “ulcerative colitis”)). In Scopus, the TITLE-ABS-KEY field was searched using the following complete search string: TITLE-ABS-KEY((“atopic dermatitis” OR “atopic eczema” OR “atopic neurodermatitis” OR “atopic dermatit*” OR “atopic eczem*”) AND (“inflammatory bowel disease*” OR “Crohn’s disease” OR “Crohn disease” OR “ulcerative colitis”)). By applying the Boolean operator AND, this strategy required AD-related and IBD-related terms to co-occur in the title, abstract, or keyword fields. The strategy was designed to retrieve studies directly focused on the AD–IBD association, as well as studies that addressed both diseases in the context of shared pathogenic mechanisms.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: publications related to atopic dermatitis and inflammatory bowel disease; English-language articles with complete bibliographic information; and document types limited to original articles and review articles. The exclusion criteria encompassed conference papers, book chapters, early access articles, editorials, articles in press, book series, conference abstracts, letters, duplicate publications, and retracted articles. Following cross-database retrieval, Python was employed to merge and deduplicate the search results from WoSCC and Scopus. After this screening process, a total of 1542 publications—comprising 753 original research articles and 789 reviews—were retained for subsequent analysis (Figure 1).
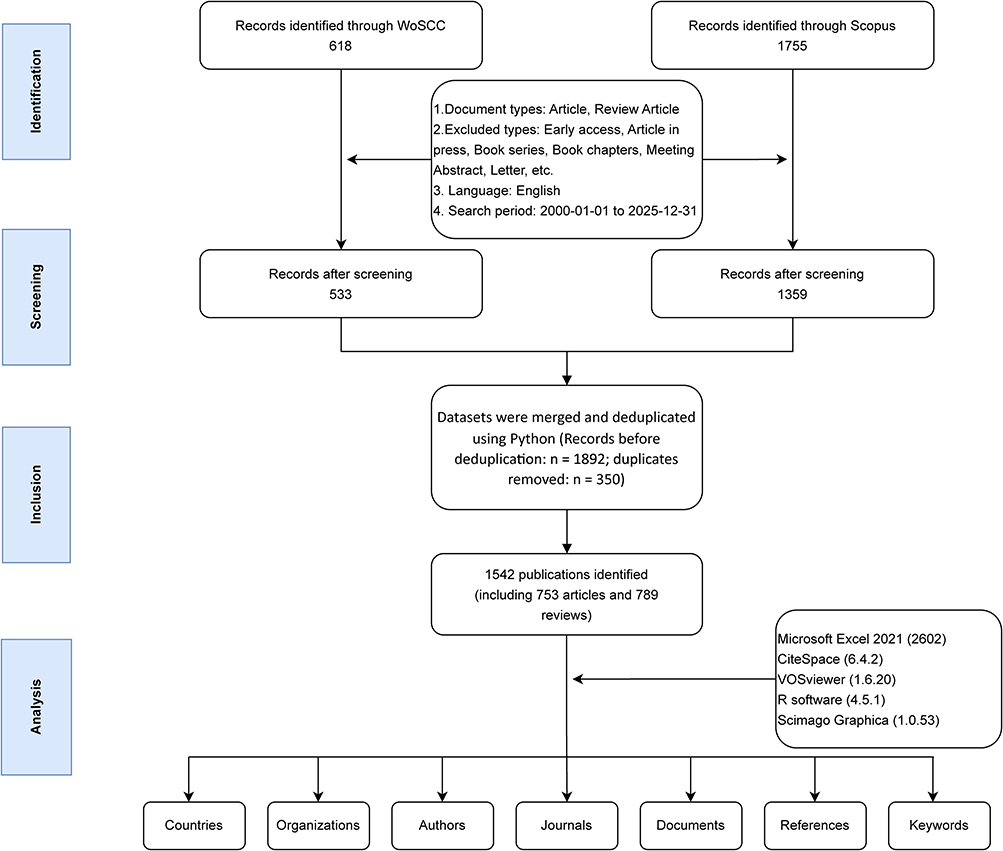 |
Figure 1 Flowchart of the literature search and screening process. |
Data Analysis
Records exported from WoSCC were saved as plain-text files containing full records and cited references, whereas records from Scopus were exported as CSV files using the same criteria. The Scopus data were subsequently converted into plain-text format in Python 3.10.18, merged with the WoSCC data, and deduplicated to generate a unified text-format dataset. During preprocessing, special symbols and redundant spaces were removed. Countries/regions were harmonized according to author affiliation addresses recorded in the databases. Authors, institutions, journals, and keywords were also standardized; the keyword standardization rules are provided in Supplementary Table S1. The cleaned data were then reformatted using the import/export function in CiteSpace to meet the requirements for subsequent analyses. Two researchers independently extracted the following fields into a structured framework: publication year, country/region, institution, journal, author, references, and keywords.
Bibliometric visualization methods were used to systematically characterize research hotspots, knowledge structures, and temporal evolution in AD–IBD research. The analyses were performed using VOSviewer 1.6.20, CiteSpace 6.4.2, Scimago Graphica 1.0.53, R 4.5.1, and Microsoft Excel 2021. Publication data exported from CiteSpace were organized in Excel; cumulative publication output was presented as a bar chart, and annual publication output was displayed as a line chart to show temporal trends. Country/region geographic distribution maps were generated by converting VOSviewer outputs into GML format and visualizing them in Scimago Graphica. Country/region collaboration chord diagrams were created using R. Author collaboration networks, institutional distributions, journal sources, and keyword co-occurrence networks were generated using VOSviewer; journal and author data were additionally exported as txt files for further processing. Keyword timeline analysis and co-cited reference burst detection were conducted in CiteSpace. Details of data cleaning, deduplication procedures, parameter settings, and screening thresholds are provided in Supplementary Table S2.
Results
Publication Trends
To delineate the evolutionary trajectory of research at the intersection of AD and IBD, we analyzed annual and cumulative publication output from 2000 to 2025 (Figure 2). Publication output in this field showed a sustained upward trend and could be broadly divided into three phases. The first phase, from 2000 to 2010, represented an initial accumulation period, during which annual output remained low and increased slowly, indicating that the field was still in its foundational stage. The second phase, from 2011 to 2019, was characterized by steady growth, with annual publications increasing from 36 in 2011 to 67 in 2018, reflecting sustained scholarly attention to AD–IBD research. The third phase, from 2020 to 2025, showed rapid growth, with annual output rising to 152 publications in 2021 and peaking at 179 in 2024. Cumulative publication output also increased continuously over time, further indicating the progressive accumulation of knowledge in this field.
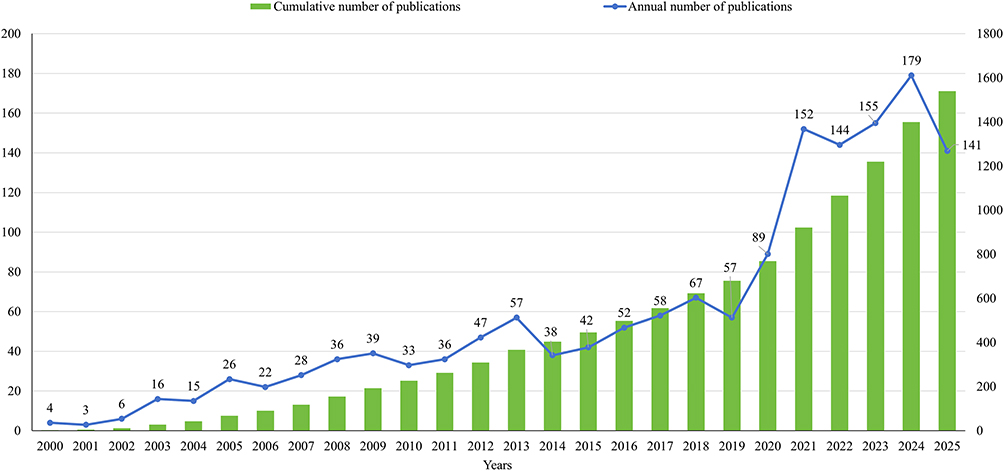 |
Figure 2 Annual and cumulative publication output of AD–IBD-related research from 2000 to 2025. The green bars indicate the cumulative number of publications and correspond to the right y-axis. The blue line with circular markers indicates the annual number of publications and corresponds to the left y-axis. The numbers above the markers indicate the annual publication counts. |
National Collaboration Network
Between 2000 and 2025, researchers from 81 countries/regions published studies on the association between AD and IBD. Figure 3A illustrates the geographic distribution of publications by country, with the USA leading in output (491 articles), followed by China (180) and Italy (156). The chord diagram in Figure 3B depicts international collaboration networks, revealing that the USA maintained the strongest collaborative ties (collaboration strength = 445), while the UK (collaboration strength = 333) and Germany (collaboration strength = 314) also served as key collaboration hubs. Table 1 presents the top 10 most productive countries along with their collaboration strength, total citations, and average citations per publication. In terms of total citations, the USA ranked first (39,863), followed by the UK (15,888) and Germany (11,625). Notably, Spain (128.75), France (127.62), and the Netherlands (112.76) achieved the highest average citations per publication, indicating substantial scholarly attention to their research output. The geographic distribution of publications and associated citation profiles suggest that AD–IBD cross-disciplinary research has garnered widespread global interest and established considerable academic impact.
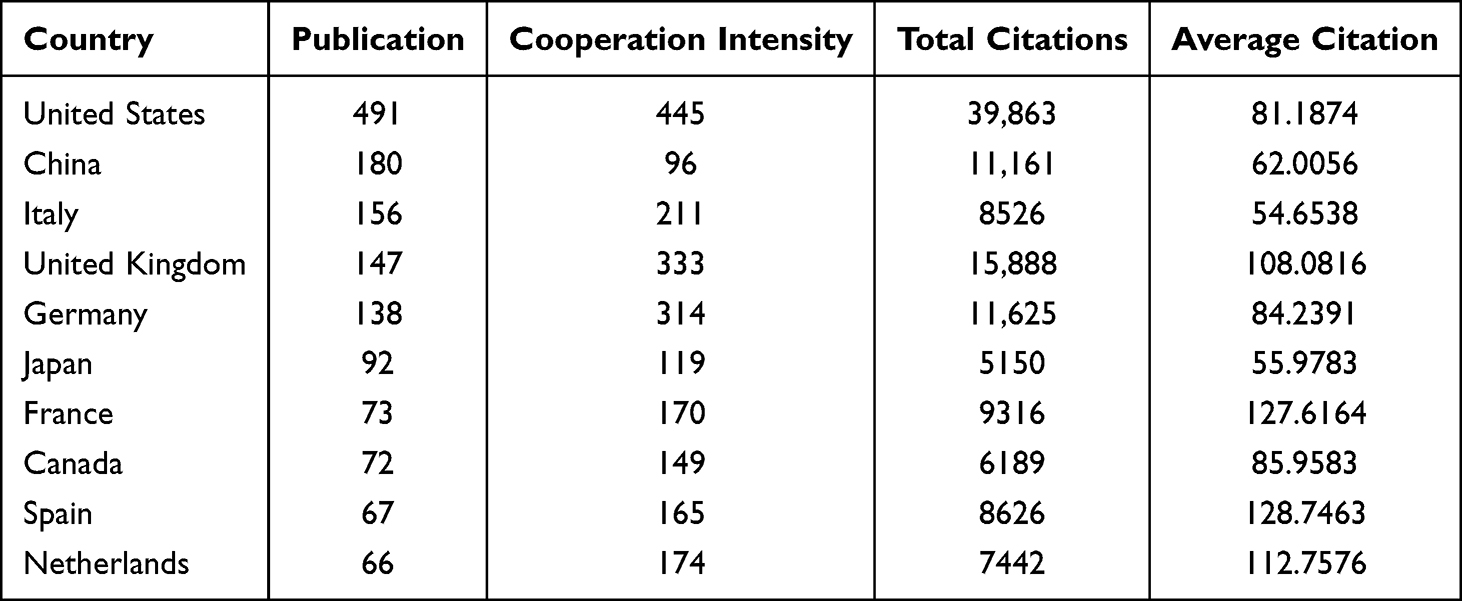 |
Table 1 Top 10 Countries by Total Publication Volume from 2000 to 2025 |
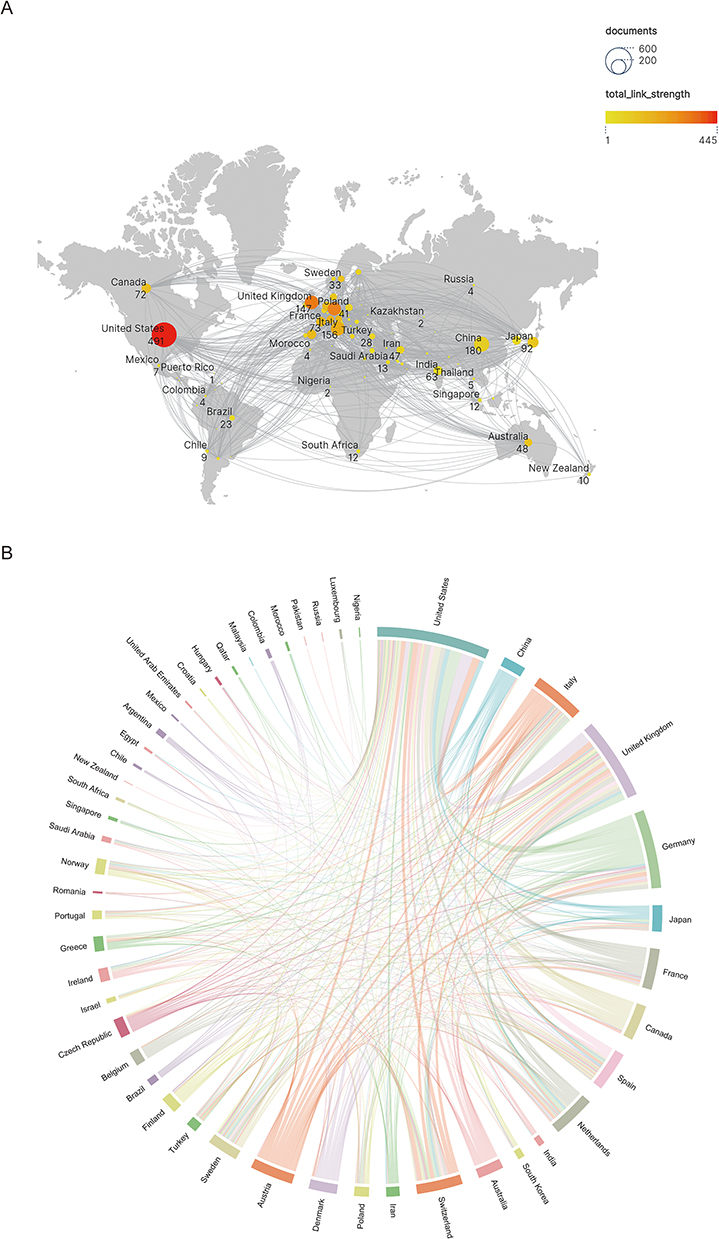 |
Figure 3 Country/region-level visualization of AD–IBD research. (A) Global geographic visualization; circle size represents publication volume, and the color gradient indicates total link strength. (B) Global collaboration chord diagram; node size represents publication volume, and line thickness indicates collaboration strength. |
Author and Institutional Collaboration Networks
Collaboration network analyses were performed using VOSviewer, including institutions with more than 11 publications and authors with more than 3 publications. The author collaboration network (Figure 4A) revealed several distinct research teams, among which those led by Li Jicui, Peyrin-Biroulet Laurent, and McInnes Iain B. were particularly prominent. However, inter-team connections remained limited, indicating that overall collaboration among research groups requires further strengthening. The institutional collaboration network (Figure 4B) showed that Harvard Univ occupied a central position, maintaining close ties with Johns Hopkins Univ, Univ Calif San Francisco, and Rockefeller Univ, suggesting its strong role as a hub in institutional collaboration within this field. Different colored clusters indicated the formation of several collaborative subgroups among institutions. Nevertheless, certain institutions, such as Univ Glasgow, were located at the periphery of the network with relatively limited connections to core institutions, suggesting room for enhanced inter-institutional collaboration. Overall, the collaborative landscape in this field has yet to be fully optimized, and future efforts should focus on strengthening cross-team and cross-institutional cooperation to facilitate sustained advancement in this domain.
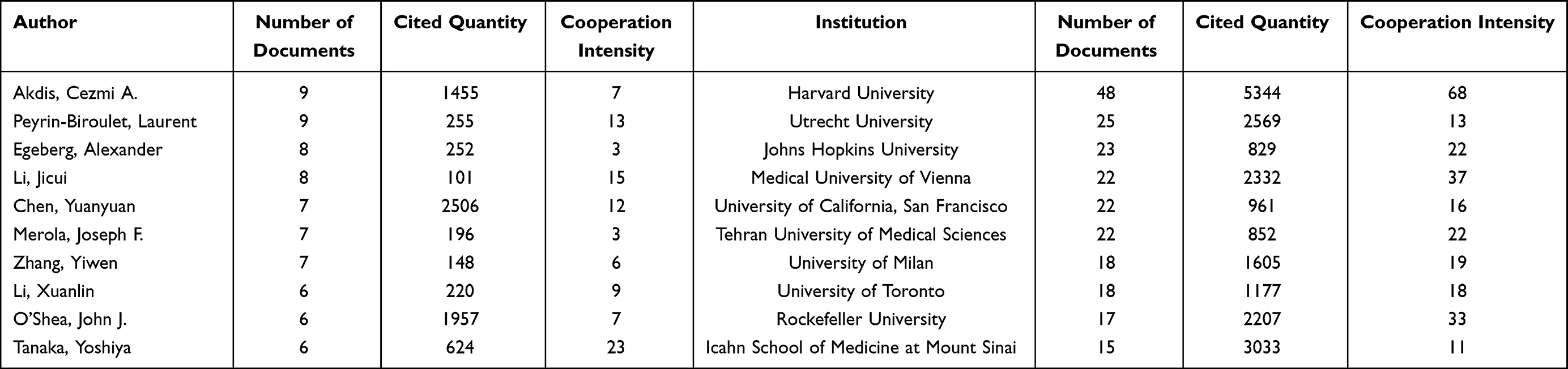 |
Table 2 Top 10 Authors and Institutions by Contribution to AD and IBD Research From 2000 to 2025 |
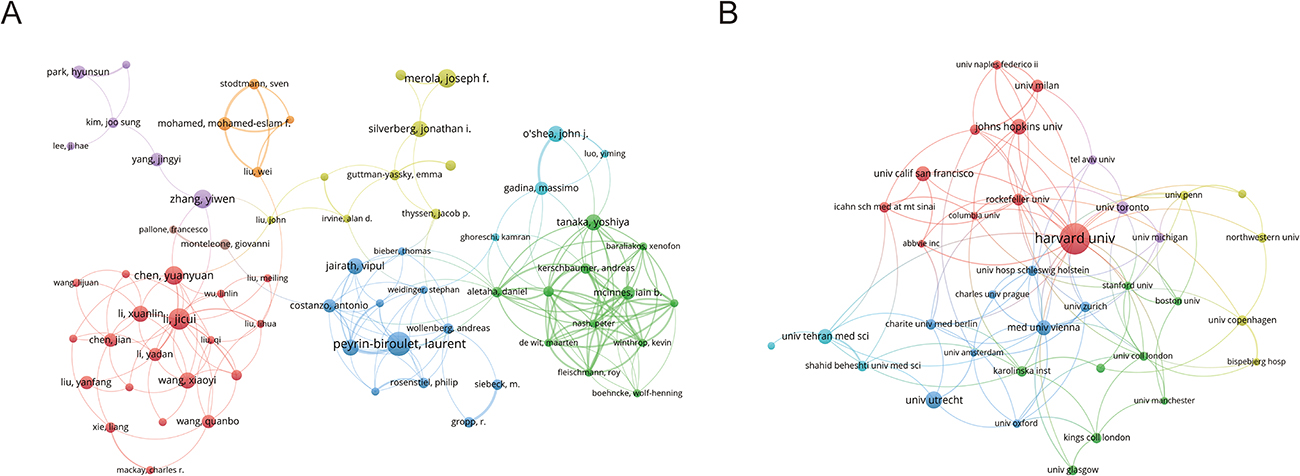 |
Figure 4 Author and institutional collaboration networks in AD–IBD research. (A) Author collaboration network; (B) institutional collaboration network. In both panels, node size represents publication output, line thickness indicates collaboration strength, and colors denote collaboration clusters identified by VOSviewer. |
Table 2 summarizes the leading authors and institutions contributing to the intersection of AD and IBD research. Akdis CA and Peyrin-Biroulet L were the most prolific authors, each with nine publications, indicating their active engagement in this field. Chen Yuanyuan received the highest total citation count (2,506), suggesting considerable scholarly attention to their work. Tanaka Yoshiya exhibited the greatest collaboration strength (23), reflecting extensive participation in co-authorship networks. At the institutional level, Harvard University ranked first in publication output, total citations, and collaboration strength, demonstrating a distinct advantage in both academic influence and collaborative capacity. Utrecht University, Johns Hopkins University, and the Medical University of Vienna also emerged as significant contributors. Together, these highly productive authors and core institutions constitute the principal academic forces driving research in this field.
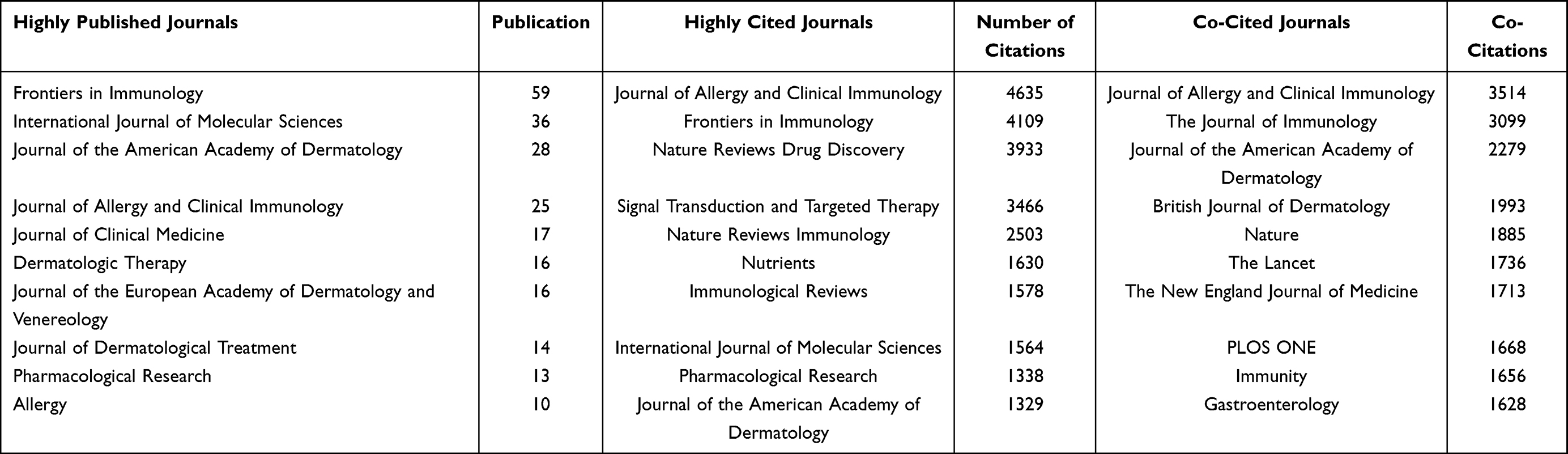 |
Table 3 Top 10 Journals and Co-Cited Journals in AD and IBD Research from 2000 to 2025 |
Journal Analysis
Figure 5A presents the network visualization of publishing journals, and Figure 5B displays the network visualization of co-cited journals. Table 3 lists the top 10 journals ranked by publication count, citation frequency, and co-citation frequency. In terms of publication output, Frontiers in Immunology (n = 59) ranked first, followed by International Journal of Molecular Sciences (n = 36) and Journal of the American Academy of Dermatology (n = 28), indicating that immunology and dermatology journals serve as the primary publication venues in this field. Regarding citation frequency, Journal of Allergy and Clinical Immunology (n = 4,635) ranked first, followed by Frontiers in Immunology (n = 4,109) and Nature Reviews Drug Discovery (n = 3,933). Notably, Frontiers in Immunology ranked among the top journals in both publication output and citation frequency, demonstrating both high productivity and high impact. In the co-citation analysis, Journal of Allergy and Clinical Immunology (n = 3,514) again ranked first, followed by The Journal of Immunology (n = 3,099) and Journal of the American Academy of Dermatology (n = 2,279). The journal co-citation network exhibited distinct clustering patterns, primarily encompassing immunology, allergy and clinical immunology, dermatology, and gastroenterology, reflecting the multidisciplinary nature of this field. These journals collectively provide essential platforms for knowledge dissemination and scholarly exchange in this research domain.
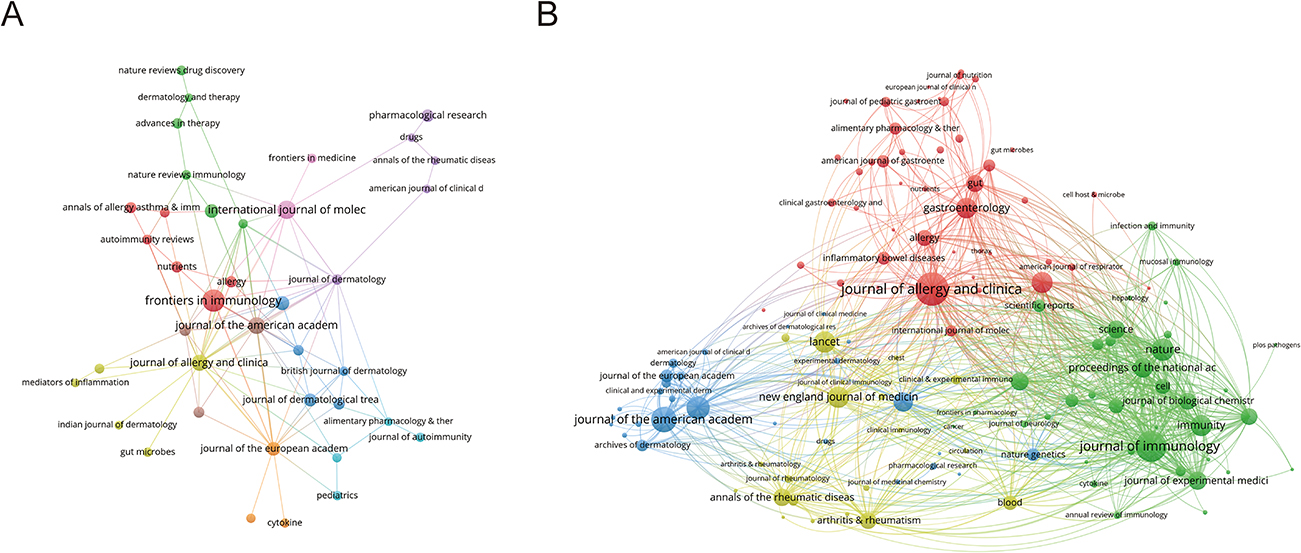 |
Figure 5 Visualization analysis of journals in AD–IBD research. (A) Journal publication network. Node size represents publication output, line thickness indicates citation link strength, and node color denotes citation-based journal clusters. (B) Journal co-citation network. Node size represents co-citation frequency, line thickness indicates co-citation link strength, and node color denotes co-cited journal clusters. |
Keyword Analysis
Keyword co-occurrence analysis identified four distinct clusters (Figure 6A). The red cluster, centered on gut microbiota, probiotics, dysbiosis, cytokines, and T cells, reflects research on intestinal microecology and immune regulation. The green cluster, anchored by AD and IBD, encompasses clinical treatment themes including biologics, JAK inhibitors, efficacy, and safety. The blue cluster involves innate lymphoid cells, Th17 cells, tumor necrosis factor-alpha (TNF-α), and immunotherapy, pointing toward autoimmune-related inflammatory pathways. The yellow cluster focuses on asthma, food allergy, allergic rhinitis, genetics, and susceptibility loci, corresponding to research on allergic comorbidities and genetic predisposition.
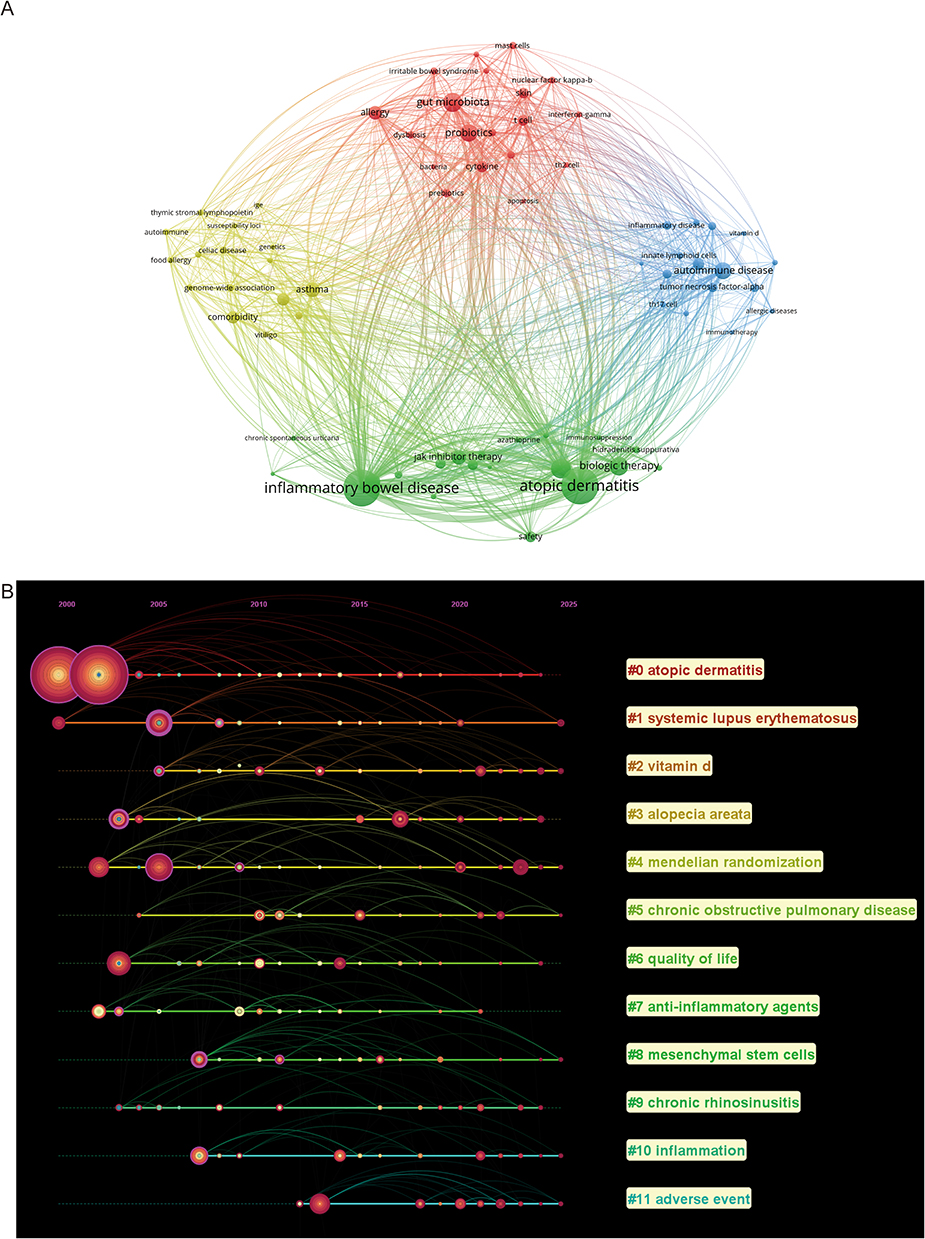 |
Figure 6 Keyword visualization analysis of AD–IBD research. (A) Keyword co-occurrence network. Node size represents keyword frequency, line thickness indicates co-occurrence strength, and colors denote keyword clusters. (B) Keyword cluster timeline map. The horizontal timeline indicates publication year; each horizontal line represents a keyword cluster, with the cluster number and label shown on the right. Nodes on each line represent keywords within the cluster; larger nodes indicate higher keyword frequency, and links indicate associations between keywords. To maintain readability and avoid overcrowding, keyword labels for individual nodes are omitted. |
To further delineate the evolutionary trajectory of this field, Figure 6B presents a timeline of major research clusters from 2000 to 2025. A total of 12 clusters were identified, encompassing multiple core research directions at the intersection of AD and IBD.
First, immune-mediated diseases and their comorbidity associations (core clusters: #0 atopic dermatitis, #1 systemic lupus erythematosus(SLE), #3 alopecia areata, #9 chronic rhinosinusitis) constitute a fundamental research foundation in this field. The sustained activity of clusters such as atopic dermatitis (#0), SLE (#1), alopecia areata (#3), and chronic rhinosinusitis (#9) indicates that the research scope has progressively expanded beyond AD and IBD themselves to encompass immune-related comorbidities and multi-organ involvement. Collectively, these thematic clusters suggest that AD and IBD research is increasingly oriented toward disease associations within the broader context of systemic immune dysregulation.
Second, inflammatory mechanisms and immune regulatory pathways (core clusters: #10 Inflammation, #7 Anti-inflammatory Agents, #8 Mesenchymal Stem Cells) represent a key research direction in this field. Clusters #10 (Inflammation) and #7 (Anti-inflammatory Agents) have persisted over an extended period, indicating that inflammatory pathways and their intervention strategies have remained central to AD and IBD research. Cluster #8 (Mesenchymal Stem Cells), an emerging topic in recent years, reflects growing interest in regenerative medicine and immunomodulation. Studies have demonstrated that mesenchymal stem cells (MSCs) exert therapeutic potential in both cutaneous inflammation control in AD and intestinal mucosal repair in IBD through paracrine secretion of anti-inflammatory factors, modulation of T-cell differentiation, and restoration of damaged epithelial barriers. Collectively, these thematic clusters suggest that AD–IBD research is progressively expanding from the elucidation of inflammatory mechanisms toward the development of novel intervention strategies.
Third, the identification of risk factors and methodological innovation (core clusters: #2 Vitamin D, #4 Mendelian Randomization, #5 Chronic Obstructive Pulmonary Disease) have broadened the research horizon of this field. Cluster #2 (Vitamin D) focuses on the regulatory role of nutritional and metabolic factors in immune function. Evidence suggests that vitamin D deficiency may exacerbate intestinal barrier disruption and cutaneous immune dysregulation, highlighting the potential contribution of environmental factors such as diet and sunlight exposure to AD and IBD susceptibility. The emergence of Mendelian randomization (Cluster #4) has provided a robust analytical framework for delineating causal relationships between exposure factors and disease outcomes. Cluster #5 (chronic obstructive pulmonary disease) further suggests that systemic inflammation may exert cross-organ effects spanning the skin, gut, and respiratory systems, thereby enriching the understanding of the AD–IBD comorbidity network.
Finally, clinical translation and patient outcome evaluation (core clusters: #6 quality of life, #11 adverse events) represent an important expanding direction in this field. The emergence of keywords related to quality of life (#6) and adverse events (#11) indicates that the research focus has progressively shifted beyond basic mechanistic exploration toward patient-reported outcomes and treatment safety assessment.
In summary, keyword co-occurrence analysis revealed that research in this field is organized around four major themes: gut microecology and immune regulation, clinical therapeutic strategies, autoimmune inflammatory pathways, and allergic comorbidities with genetic predisposition. Timeline visualization of keyword clusters further indicated a progressive shift in research focus from early exploration of immune-inflammatory mechanisms toward risk factor identification, methodological innovation, and clinical translation assessment. Together, these findings suggest that the AD and IBD research landscape has evolved into a relatively comprehensive framework spanning from fundamental mechanisms to clinical applications.
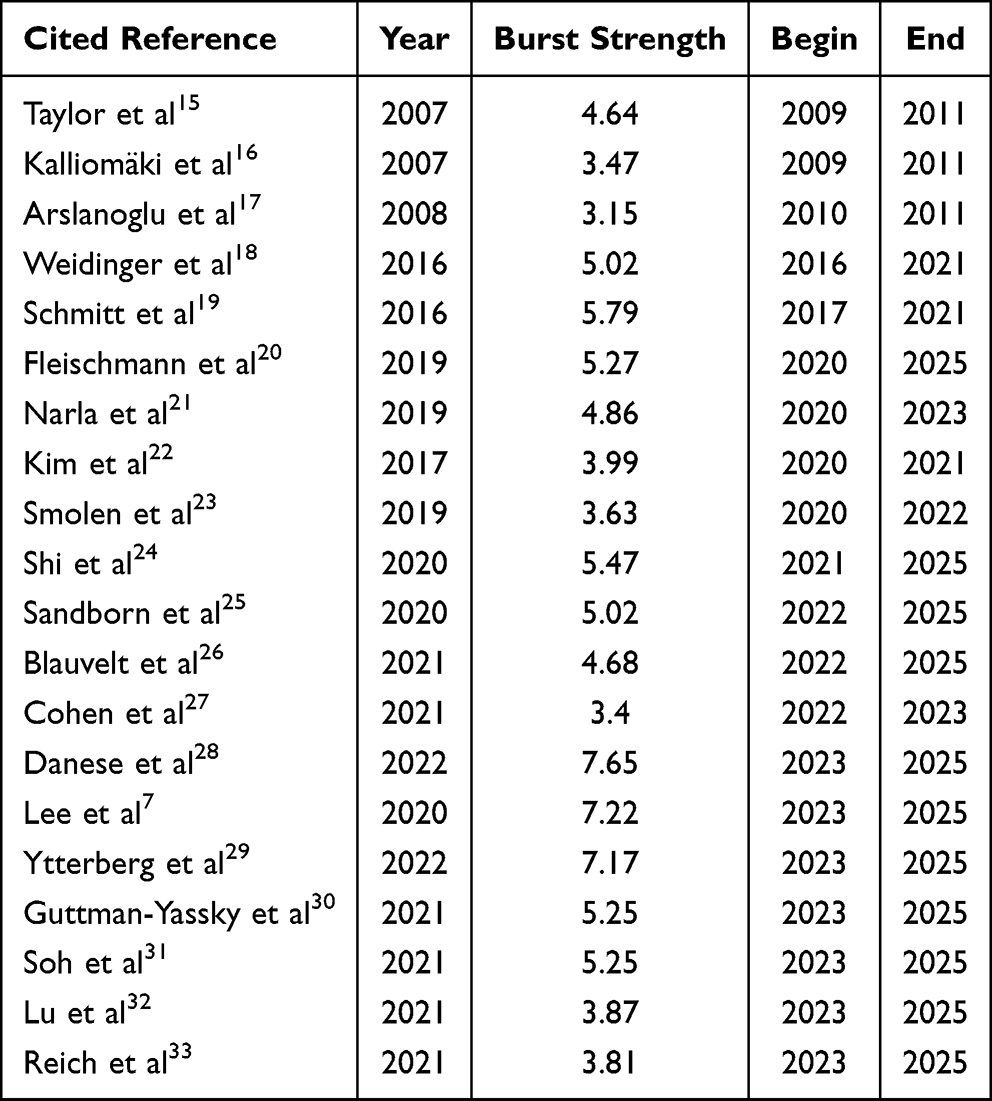 |
Table 4 Top 20 Co-Cited References with the Strongest Citation Bursts in AD–IBD Research |
Burst Detection Analysis of Co-Cited References
Analysis of highly cited references with citation bursts helps reveal key trends and recent focal points in the intersection of atopic dermatitis (AD) and inflammatory bowel disease (IBD). Table 4 highlights three pivotal publications—Danese (burst strength = 7.65), Lee (burst strength = 7.22), and Ytterberg (burst strength = 7.17)—all exhibiting sustained citation bursts from 2023 through 2025, reflecting the most active research frontiers in this field. Danese et al28 published a Phase III clinical trial in The Lancet in 2022, demonstrating that upadacitinib, a selective Janus kinase 1 (JAK1) inhibitor, effectively induced and maintained clinical remission in moderate-to-severe ulcerative colitis, with significant endoscopic and histological improvements. The sustained citation burst of this study underscores the growing recognition of JAK inhibitors as a promising therapeutic strategy at the AD–IBD interface, given their pharmacological capacity to simultaneously target cutaneous and intestinal inflammatory pathways. Lee et al7 conducted a systematic review and meta-analysis published in 2020, encompassing 10 studies with over 95 million participants, which established a bidirectional epidemiological association between AD and IBD at the prevalence level, providing robust evidence for understanding their comorbid relationship and shared immune dysregulation mechanisms.
The ORAL Surveillance trial published by Ytterberg et al29 in 2022 demonstrated that tofacitinib was associated with higher risks of major adverse cardiovascular events and malignancies compared with TNF inhibitors in rheumatoid arthritis patients with cardiovascular risk factors, failing to meet the prespecified non-inferiority criteria. The sustained citation burst of this publication suggests that, as JAK inhibitors are increasingly applied across a broad spectrum of immune-mediated diseases such as AD and IBD, their long-term safety profile and benefit–risk balance have emerged as critical concerns in the field.
Discussion
Overall Landscape and Knowledge Base of Cross-Disciplinary Research Between AD and IBD
Our analysis revealed a sustained increase in publication output on AD–IBD cross-disciplinary research from 2000 to 2025, with a notable acceleration since 2020, indicating that the field has transitioned from sporadic early exploration to a phase of rapid and sustained expansion. Regarding the distribution of research capacity, the USA dominated in terms of publication volume, international collaboration intensity, and total citation count, serving as the primary driver of progress in this field. China has demonstrated strong growth potential with a rapid rise in publications in recent years, while several European countries—including the UK, France, Spain, and the Netherlands—exhibited relatively high citations per publication, reflecting considerable academic influence. Author and institutional collaboration network analyses further revealed that leading institutions such as Harvard University functioned as key hubs within the collaborative network. The field has thus formed a research landscape anchored in North America and Europe, with Asia emerging as a rapidly growing contributor. Nevertheless, linkages among certain author groups and between peripheral and core institutions remain relatively limited, suggesting room for strengthening cross-team and cross-institutional collaboration. Meanwhile, the most prolific and highly cited journals were concentrated in the domains of immunology, allergy and clinical immunology, dermatology, and gastroenterology, underscoring that the knowledge base of this field rests on substantial multidisciplinary convergence.
Key Research Hotspots in AD–IBD Cross-Disciplinary Research
Gut Microbiota and Immune Regulation
Keyword clustering analysis showed that terms such as gut microbiota, probiotics, dysbiosis, cytokines, and T cells converged within the red cluster, suggesting that gut microecology and immune regulation have emerged as important themes in AD–IBD cross-disciplinary research. In the AD field, Rios-Carlos et al34 systematically reviewed the pathways through which gut microbial metabolites influence cutaneous inflammation, noting that short-chain fatty acids can modulate immune responses by promoting regulatory T cell differentiation while enhancing epidermal barrier function and reducing transepidermal water loss. Additionally, tryptophan-derived indole metabolites activate the aryl hydrocarbon receptor, thereby downregulating the expression of pro-inflammatory mediators such as thymic stromal lymphopoietin (TSLP) and IL-4, while simultaneously upregulating filaggrin expression — thus exerting dual effects on immune regulation and barrier repair. In the IBD field, Iliev et al35 reviewed the roles of intestinal bacteria, fungi, and their metabolites in mucosal immune dysregulation and epithelial barrier disruption, emphasizing the regulatory significance of metabolites such as short-chain fatty acids and bile acids in maintaining the Treg/Th17 balance. Studies in both fields implicate shared elements, including gut microecology, barrier function, and immune responses, which may provide a plausible biological context for interpreting the bibliometric hotspots identified at the AD–IBD interface.
The value of this topic lies in revealing a potential positive feedback loop between dysbiosis and impaired barrier function. Research has demonstrated that the gut microbiota of AD patients exhibits intraspecies compositional shifts in Faecalibacterium prausnitzii, characterized by enrichment of the low-butyrate-producing L2-6 phylotype alongside reduced fecal butyrate and propionate levels, suggesting a feedback loop between F. prausnitzii subspecies imbalance and intestinal epithelial inflammation that may ultimately influence cutaneous immune responses through increased intestinal permeability.36 Notably, Dokoshi et al employed murine skin wounding and epidermal hyaluronidase overexpression models to demonstrate that skin injury alters gut microbiota composition and upregulates colonic host defense genes, including Reg3 and Muc2. Furthermore, fecal microbiota transplantation experiments confirmed that this altered microbiota enhances susceptibility to colitis in recipient mice, providing direct experimental evidence for the existence of a skin–gut axis.37 Collectively, these findings indicate that microbiota–immune crosstalk between the skin and the gut may be bidirectional, offering a novel perspective for understanding the comorbidity between AD and inflammatory bowel diseases.
Regarding immune regulation, probiotic research has provided relatively clear mechanistic insights. Smits et al38 demonstrated that L. reuteri and L. casei modulate dendritic cell function by engaging the dendritic cell-specific intercellular adhesion molecule-3-grabbing non-integrin receptor on the dendritic cell surface, thereby promoting the differentiation of IL-10-producing regulatory T cells. Kwon et al39 further reported that a defined mixture of five probiotic strains (IRT5) induces the generation of regulatory dendritic cells, which in turn drive the differentiation of CD4⁺Foxp3⁺ Tregs from CD4⁺CD25− precursors while suppressing Th1, Th2, and Th17-associated cytokine expression, yielding significant disease amelioration in experimental models of IBD, AD, and RA. Additionally, a comprehensive review has delineated, from the perspective of the dietary fiber–gut microbiota–short-chain fatty acid axis, the multifaceted mechanisms through which short-chain fatty acids maintain immune homeostasis—namely, reinforcing intestinal epithelial barrier integrity, inhibiting histone deacetylases, and activating metabolite-sensing G protein-coupled receptors—thereby establishing a theoretical framework for dietary intervention in inflammatory diseases.40
Overall, our bibliometric analysis indicates that gut microbiota and immune regulation are major themes in research at the AD–IBD interface. In light of previous studies, dysbiosis may contribute to the development and progression of AD–IBD comorbidity by disrupting intestinal barrier integrity and modulating local and systemic immune responses. Viewing the AD–IBD association through the lens of the gut–skin axis may provide a theoretical basis for microbiota-targeted interventions, including probiotics and dietary strategies. However, the present study cannot establish causal directionality. Future longitudinal, mechanistic, and interventional studies are needed to clarify causal relationships and evaluate the clinical value of microbiota-targeted interventions.
Shared Inflammatory Pathways and Immune-Mediated Comorbidity
At the disease level, keywords such as “allergic diseases,” “autoimmune disease,” and “SLE” converged within the blue cluster in our analysis, while the keyword clustering timeline revealed that topics including SLE, alopecia areata, and inflammation have remained persistently active. These findings indicate that the research scope in the AD–IBD field has expanded beyond single-organ disorders to encompass cross-organ immune-mediated comorbidities. Recent systematic reviews have demonstrated that patients with AD face an elevated risk of developing multiple autoimmune conditions, including alopecia areata, celiac disease, Crohn’s disease, SLE, ulcerative colitis, and rheumatoid arthritis.32 At the genetic level, Qi et al41 leveraged large-scale genome-wide association study (GWAS) data to systematically examine the shared genetic architecture between allergic and gastrointestinal diseases. They identified genome-wide genetic correlations between asthma and related phenotypes and irritable bowel syndrome, whereas correlations with CD, UC, and celiac disease were driven by specific genomic regions. Although the patterns of genetic correlation varied across disease pairs, integration of single-cell transcriptomic and single-cell eQTL data revealed that the associated genetic signals were consistently enriched in CD4⁺ T cells across multiple tissues. Collectively, this evidence suggests that the co-occurrence of AD and IBD may be partly rooted in a shared immune-genetic basis rather than being solely driven by environmental exposures or therapeutic factors.
From a mechanistic perspective, the recurrent emergence of Th17, tumor necrosis factor (TNF)-related pathways, and innate lymphoid cells (ILCs) provides important clues for understanding the association between AD and IBD. Lopata et al11 constructed and systematically compared disease atlases of AD and UC, identifying 131 shared HGNC-standardized gene identifiers. Significant overlap was observed in signaling pathways including NF-κB, JAK-STAT, and MEK-ERK, along with 28 common drug targets, suggesting that despite affecting different organs, these two diseases share comparable inflammatory mechanisms at the molecular network level. At the innate immune level, group 2 innate lymphoid cells (ILC2s) represent the most critical ILC subset in AD pathogenesis. Upon activation by epithelium-derived TSLP, IL-33, and IL-25, ILC2s secrete IL-5 and IL-13 to drive type 2 inflammation. Meanwhile, group 3 innate lymphoid cells (ILC3s) contribute to AD pathology through secretion of IL-17A and IL-22, indicating multidimensional regulatory roles of ILCs in AD.42 Epithelial barrier studies have further demonstrated that IL-4 and IL-13 downregulate the expression of tight junction proteins and keratinization-associated proteins via the JAK-STAT6 pathway—a mechanism operative across the skin barrier in AD, the airway barrier in asthma, and the gastrointestinal barrier in eosinophilic esophagitis. These findings support the notion that type 2 inflammation-driven barrier dysfunction is a cross-organ phenomenon and provide a barrier-level explanation for the comorbidity between AD and other epithelial inflammatory diseases.43 Additionally, Hisamoto et al44 reported elevated serum TNF-like ligand 1A (TL1A) levels in AD patients, which positively correlated with IgE, lactate dehydrogenase (LDH) levels, and eosinophil counts. The TL1A–death receptor 3 axis has been implicated in the inflammatory processes of IBD, rheumatoid arthritis, and psoriasis; moreover, TL1A can simultaneously promote both Th2 and Th17 responses, suggesting that this TNF superfamily member may participate in the inflammatory cascade of multiple immune-mediated diseases. However, its precise mechanistic role in AD remains to be elucidated.
Overall, the comorbidity between AD and IBD may not be incidental. Our findings indicate that shared inflammatory pathways and comorbidity-related themes have remained persistent research hotspots in this field. Existing epidemiological, genetic, and mechanistic evidence suggests that the two diseases may partly share immunogenetic foundations and inflammatory regulatory networks. However, current evidence is mainly derived from observational association studies, genetic analyses, and bioinformatics investigations. The specific roles of shared pathways in each disease and the potential direction of causality remain unclear and require further clarification through prospective cohort studies and disease-specific functional validation.
Evolution of Therapeutic Strategies: Biologics and JAK Inhibitors
Based on keyword clustering and burst citation analyses in this study, the green cluster centered on atopic dermatitis, inflammatory bowel disease, biologic therapy, JAK inhibitor therapy, efficacy, and safety, while recent burst references primarily involved agents such as upadacitinib and tofacitinib. These findings suggest that the research focus at the AD–IBD intersection is shifting from comorbidity characterization toward risk–benefit evaluation of shared therapeutic targets. This trend is closely linked to therapeutic advances in each field: in AD, biologics exemplified by dupilumab and JAK inhibitors including baricitinib, upadacitinib, and abrocitinib now constitute the mainstay of systemic therapy;45 in IBD, tofacitinib and upadacitinib have been approved for moderate-to-severe ulcerative colitis and demonstrate favorable efficacy in patients with prior biologic failure.46 As the JAK-STAT pathway represents a shared intervention target for both diseases, cross-disease comparisons of efficacy and safety have emerged as a key research direction within this interdisciplinary field.
At the therapeutic level, biologics first ushered the field into the era of targeted therapy, while selective JAK1 inhibitors have further expanded the treatment armamentarium. In AD, upadacitinib significantly improved skin lesions and pruritus in moderate-to-severe patients in the Measure Up 1 and Measure Up 2 trials;30 the AD Up study confirmed comparable efficacy when combined with topical corticosteroids;33 and in a head-to-head trial against dupilumab, upadacitinib demonstrated superiority in high-threshold skin clearance (EASI-90, EASI-100) and early itch relief.26 In IBD, a phase IIb study by Sandborn et al25 first indicated that upadacitinib improved clinical remission rates and endoscopic outcomes in patients with active UC; Danese et al28 subsequently confirmed its superiority over placebo for both induction and maintenance therapy in moderate-to-severe UC in a phase III program; and phase III trials in Crohn’s disease showed consistent efficacy trends.47 Overall, JAK1 inhibitors such as upadacitinib have shown clinical benefits in both AD and IBD; however, parallel therapeutic benefits do not necessarily indicate a shared pathophysiological mechanism. The precise biological roles and disease-specific relevance of the JAK–STAT pathway in these two diseases remain to be further clarified.
Meanwhile, the safety profile of JAK inhibitors has attracted increasing scrutiny. An integrated analysis of upadacitinib encompassing over 27,000 patient-years across seven indications demonstrated that the incidence of adverse events remained stable over long-term follow-up; however, rates of herpes zoster, non-melanoma skin cancer, and creatine kinase (CK) elevation were higher than those observed with active comparators, and the risks of herpes zoster and venous thromboembolism were notably pronounced among patients with UC relative to other indications.48 In the AD population, a meta-analysis revealed that major adverse cardiovascular events remained rare during JAK inhibitor therapy, with no significant difference compared with placebo or dupilumab, although the certainty of evidence was limited and insufficient to exclude long-term cardiovascular risk.49 Furthermore, a network meta-analysis corroborated a consistent dose–response relationship between JAK inhibitors and elevated herpes zoster risk, with AD patients exhibiting the highest incidence of herpes zoster among all immune-mediated inflammatory diseases.50 Accordingly, future research should focus not only on validating the cross-disease therapeutic potential of JAK inhibitors but also on delineating appropriate patient populations for each indication, optimizing safety monitoring protocols, and establishing long-term risk management strategies.
Overall, biologics have laid the foundation for targeted therapy research in AD and IBD, while the introduction of JAK inhibitors has further shifted the research focus from disease-level associations toward mechanistic exploration of shared signaling pathways. Concurrently, long-term safety and risk–benefit analyses have become increasingly central to clinical therapeutic decision-making.
Genetic Susceptibility, Environmental Factors, and Causal Inference
The emergence of topics such as vitamin D, Mendelian randomization, and chronic obstructive pulmonary disease within the yellow cluster—encompassing genetics and susceptibility loci—and in the keyword clustering timeline, indicates that this field has progressively expanded from comorbidity research to investigations of genetic susceptibility, environmental exposure, and causal inference. The concentrated co-occurrence of keywords such as allergic rhinitis, asthma, food allergy, GWAS, and susceptibility loci suggests that the association between AD and IBD is increasingly being understood within the framework of a shared genetic architecture. Both AD and IBD are polygenic complex diseases, and previous GWAS have independently identified numerous risk loci for each condition.51,52 Lazanas et al53 identified 70 pleiotropic loci shared between AD and IBD; although genome-wide genetic correlation was limited, these shared loci were enriched in immuno-inflammatory pathways involving T-cell differentiation and leukocyte activation, suggesting that localized genetic overlap may mediate their comorbidity through specific inflammatory pathways.
However, this comorbid association is not uniform across atopic phenotypes. A genetically informed study from Sweden confirmed individual-level comorbidity between IBD and asthma, allergic rhinitis, and eczema, yet multiple genetic analytic approaches detected only a weak signal of shared genetic and unique environmental contributions between IBD and eczema, with insufficient evidence for a common genetic origin linking IBD to the remaining allergic diseases.54 Clinical data further indicate that children with AD at age 3 have a significantly elevated risk of subsequent IBD, whereas asthma, food-related allergic symptoms, and allergic rhinitis show no significant association with IBD.55 A large UK population-based cohort similarly demonstrated that both children and adults with AD carry a significantly increased risk of incident IBD, with the risk escalating in a severity-dependent manner; notably, however, the association between childhood AD and UC reached statistical significance only among patients with severe AD.8 Taken together, the available evidence suggests that AD may be the atopic phenotype most closely linked to IBD, although their shared genetic basis appears limited.
Environmental and nutritional factors represent another important thread within this cluster. The persistent appearance of vitamin D as a high-frequency keyword suggests that the research focus has shifted from immune phenotyping toward the interplay between mucosal barrier integrity and environmental exposures. The epithelial barrier hypothesis posits that barrier-disrupting agents pervasive in industrialized and modern lifestyles may serve as a common driver underlying the rising prevalence of allergic, autoimmune, and other chronic inflammatory diseases, thereby providing a unifying pathophysiological framework for the cross-organ association between AD and IBD.56 Consistent with this notion, vitamin D/VDR signaling has been shown to regulate tight junction proteins in both the skin and the intestinal epithelium and to modulate innate immune responses, exerting potentially protective effects in barrier-dysfunction disorders such as AD, IBD, and celiac disease.57 Nevertheless, a causal role for vitamin D remains unestablished. Previous Mendelian randomization studies have found no significant association between genetically determined low 25-hydroxyvitamin D levels and the risk of AD, asthma, or elevated serum IgE, suggesting that the positive associations reported in earlier observational studies may be attributable to residual confounding or reverse causation.58
At the methodological level, the application of MR represents a significant advance in this field. A bidirectional two-sample MR study revealed a causal association between genetic susceptibility to AD and increased IBD risk (pooled OR = 1.11, 95% CI: 1.04–1.18), with subtype analysis suggesting a directional association between AD and UC, although the reverse effect was not supported.59 Subsequently, Li et al extended their analysis to multiple allergic diseases and found that IBD—particularly CD—increased the risk of AD, allergic asthma, and allergic rhinitis, whereas no significant reverse causation was observed.60 These two studies diverge regarding causal directionality: the former supports a causal pathway from AD to UC, while the latter primarily supports a direction from CD to AD. This discrepancy may stem from differences in instrumental variables, GWAS datasets, and sample sizes, and further suggests that UC and CD may be fundamentally distinct in their genetic associations with AD. From a systems biology perspective, Lopata et al11 constructed a disease map of UC and AD, identifying 131 shared genes and 19 similar molecular interaction modules, and proposed that shared pathways such as NF-κB and JAK-STAT could serve as common therapeutic targets for both diseases, with potential for drug repositioning. Such integrative studies provide molecular-level explanations for the AD–IBD association and lay the groundwork for mechanism-driven therapeutic strategies.
Emerging Trends and Future Directions in AD–IBD Cross-Disciplinary Research
As indicated by the keyword timeline in this study—where topics such as “quality of life” and “adverse event” have gained prominence—the research focus at the AD–IBD intersection has expanded from elucidating shared pathogenic mechanisms to identifying high-risk populations and evaluating clinical burden. A recent meta-analysis demonstrated that AD exposure was associated with a significantly elevated risk of IBD (OR = 1.37), a finding consistent across both Crohn’s disease (OR = 1.51) and ulcerative colitis (OR = 1.33) subtypes.61 A specialty clinic-based study further indicated that this association was predominantly driven by moderate-to-severe AD (adjusted OR = 4.45), whereas no significant association was observed for mild AD, suggesting that disease severity may serve as a critical stratification factor.62 Moreover, a retrospective study of IBD patients revealed the substantial clinical burden imposed by comorbidity: 79.8% of IBD patients with concomitant immune-mediated diseases exhibited an aggressive disease course, compared with only 8.1% of those without such comorbidities, with a dose–response relationship between the number of comorbidities and disease aggressiveness (OR = 1.6).63 Collectively, these findings underscore the need for future studies to incorporate stratified analyses based on AD severity and the comorbidity spectrum, thereby enabling more precise identification of high-risk populations and informing long-term management strategies.
“Mesenchymal stem cells,” as an emerging frontier topic in recent years, reflects growing interest in cell-based therapeutic strategies at the intersection of AD and IBD. In the context of AD, umbilical cord-derived MSCs have been shown to attenuate lesion severity in AD-like dermatitis models by suppressing JAK-STAT signaling and the expression of multiple inflammatory cytokine receptors, while partially restoring transcription of epidermal barrier-related genes.64 In the context of IBD, Tak et al65 demonstrated that SOD3-transduced MSCs inhibited MAPK signaling activation and preserved epithelial tight junction protein expression in DSS-induced murine colitis, and mitigated TNF-α-mediated inflammatory injury in intestinal organoids. Furthermore, a small-sample Phase I clinical trial showed that intravenous infusion of umbilical cord-derived MSCs for active UC exhibited a favorable safety profile, with sustained improvement in Mayo scores observed in a subset of patients.66 Overall, existing experimental studies and early clinical evidence suggest that MSCs may have immunomodulatory and barrier-protective effects. In the present study, the emergence of “mesenchymal stem cells” should be interpreted as an emerging research theme; their long-term efficacy, safety, and optimal therapeutic regimens require validation in larger-scale, disease-specific clinical and mechanistic studies.
Based on recent co-citation bursts, the long-term safety and benefit–risk assessment of pharmacotherapies has emerged as a prominent theme in this field. In AD, the 52-week follow-up data from the Measure Up 1 and Measure Up 2 trials demonstrated that the efficacy of upadacitinib at both 15 mg and 30 mg was sustained over time, with an overall safety profile consistent with earlier observations; however, the 30 mg group exhibited higher rates of certain infections and laboratory-related adverse events.67 The Heads Up head-to-head trial further showed that upadacitinib 30 mg was superior to dupilumab in skin clearance and itch relief, albeit with elevated rates of serious infections, eczema herpeticum, herpes zoster, and laboratory abnormalities.68 In the IBD setting, clinical follow-up of tofacitinib in ulcerative colitis indicated that the incidence of herpes zoster remained generally stable over time, with most episodes being non-serious and confined to one or two dermatomes; nevertheless, advanced age and prior TNF inhibitor failure were identified as independent risk factors.69 At a broader safety level, a cross-indication meta-analysis by Russell et al70 found no significant difference in malignancy risk between JAK inhibitors and placebo or methotrexate, yet a significantly higher risk compared with TNF inhibitors. Notably, this difference was largely driven by the ORAL Surveillance trial, which enrolled an elderly RA population enriched for cardiovascular risk factors;29 whether these findings can be extrapolated to comorbid populations with distinct immunological backgrounds and baseline risk profiles, such as patients with concomitant AD and IBD, warrants further investigation. As the indications for JAK inhibitors continue to expand, how to balance efficacy and safety in light of the specific risk profiles of patients with co-existing AD and IBD remains a critical question for future clinical research.
Limitations
This study has several limitations. First, only original articles and reviews published in English were included, which may have resulted in the omission of non-English literature and other study types. Second, although the combined search of WoSCC and Scopus helped improve coverage, differences between the two databases in journal indexing scope and citation update frequency make retrieval gaps unavoidable. Third, although the search strategy required the co-occurrence of AD- and IBD-related terms, some included records may have addressed both conditions within a broader context of immune- or inflammation-related diseases. Therefore, terms such as systemic lupus erythematosus, alopecia areata, and chronic obstructive pulmonary disease should be interpreted as reflecting broader shared inflammatory pathways or interdisciplinary contexts. Future studies could apply stricter record-level relevance validation to further improve dataset specificity. Fourth, recently published studies, particularly those from 2025, may be affected by delays in database indexing and citation accumulation, which could lead to underestimation of the importance of emerging topics. Fifth, open-access articles generally have greater visibility and are more likely to be cited; therefore, citation and co-citation frequencies should be interpreted as indicators of scholarly attention rather than direct measures of scientific quality.
Conclusion
This study conducted a systematic bibliometric analysis of the research literature at the intersection of AD and IBD. The results revealed a sustained upward trend in publication output, with a notably accelerated growth since 2020. Research activity has been predominantly driven by North America and Europe, while Asia has emerged as a rapidly growing contributor in recent years. The field has evolved into a multidisciplinary landscape anchored in immunology, allergy and clinical immunology, dermatology, and gastroenterology. Current research priorities center on gut microbiota and immune regulation, shared inflammatory pathways and immune-mediated comorbidities, therapeutic strategies involving biologics and JAK inhibitors, as well as genetic susceptibility and causal inference. The research focus has progressively shifted from epidemiological associations and inflammatory mechanism exploration toward clinical translation and safety evaluation.
Current evidence suggests that the association between AD and IBD may be underpinned by a shared pathological basis, including epithelial barrier dysfunction, immune dysregulation, microbial dysbiosis, and partially overlapping signaling pathways, rather than by simple comorbid co-occurrence. However, the bibliometric findings of the present study reflect only the distribution of research hotspots; whether AD and IBD share common pathogenic mechanisms remains to be confirmed by mechanistic studies. Several key issues remain unresolved, including inconsistencies in the direction and magnitude of causal associations, insufficient validation of the long-term safety of JAK inhibitors in comorbid populations, and a lack of high-quality clinical evidence for emerging interventions. Moreover, as this study was based on bibliometric analysis, its conclusions may be influenced by the search strategy, literature deduplication, and delayed citation accumulation for recent publications, and should therefore be interpreted in conjunction with future mechanistic and clinical evidence. Future research should further focus on validating gut–skin axis mechanisms, refining precision stratification of comorbid populations, and evaluating the long-term risk–benefit profiles of targeted therapies. Strengthening interdisciplinary, inter-institutional, and international collaboration will be essential to advance this field from associative description toward mechanistic investigation and clinical translation.
Abbreviations
AD, atopic dermatitis; IBD, inflammatory bowel disease; CD, Crohn’s disease; UC, ulcerative colitis; JAK, Janus kinase; JAK1, Janus kinase 1; GWAS, genome-wide association study; SLE, systemic lupus erythematosus; MSCs, mesenchymal stem cells; TSLP, thymic stromal lymphopoietin; TNF, tumor necrosis factor; TNF-α, tumor necrosis factor-alpha; TL1A, TNF-like ligand 1A; LDH, lactate dehydrogenase; ILCs, innate lymphoid cells; ILC2s, group 2 innate lymphoid cells; ILC3s, group 3 innate lymphoid cells; CK, creatine kinase.
Ethics Approval and Consent to Participate
This study employed bibliometric methods, with all data retrieved exclusively from publicly accessible and authorized academic databases. It was a non-interventional study and did not include human participants, animals, biological samples, or any personally identifiable information. Therefore, no ethical issues were involved, and approval from an institutional review board or ethics committee was not required in accordance with relevant regulations and international ethical principles. Since no individuals were enrolled as research subjects, informed consent was not applicable.
Acknowledgments
We would like to express our gratitude to the teams responsible for maintaining and developing the databases and software employed in this research.
Funding
The authors declare that financial support was received for the research, and/or publication of this article. This study was supported by the “Science and Technology Innovation Action Plan” of Shanghai (Grant No. 23Y31920300), the SPH-SHUTCM Joint Research Institute (Grant No. E4-H200210399), the Shanghai Shenkang Hospital Development Center (Grant No. SHDC2025CCS013), the Jiangxi Provincial Administration of Traditional Chinese Medicine (Grant No. 2025020707), the Shanghai Municipal Administration of Traditional Chinese Medicine (Grant No. 2025CXGZS-14), and the Yu Song Famous Traditional Chinese Medicine Doctor Studio Fund (Jiangxi Hospital of Shanghai Longhua Hospital).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Guttman-Yassky E, Renert-Yuval Y, Brunner PM. Atopic dermatitis. Lancet. 2025;405(10478):583–23. doi:10.1016/S0140-6736(24)02519-4
2. Hashash JG, Limdi JK, Shapiro JM, Shah SA. Medical management of inflammatory bowel diseases. BMJ. 2025;391:e079050. doi:10.1136/bmj-2025-079050
3. Neurath MF, Artis D, Becker C. The intestinal barrier: a pivotal role in health, inflammation, and cancer. Lancet Gastroenterol Hepatol. 2025;10(6):573–592. doi:10.1016/S2468-1253(24)00390-X
4. Oh J, Kim S, Kim MS, et al. Global, regional, and national burden of asthma and atopic dermatitis, 1990–2021, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Respir Med. 2025;13(5):425–446. doi:10.1016/S2213-2600(25)00003-7
5. Lin D, Jin Y, Shao X, et al. Global, regional, and national burden of inflammatory bowel disease, 1990–2021: insights from the global burden of disease 2021. Int J Colorectal Dis. 2024;39(1):139. doi:10.1007/s00384-024-04711-x
6. Sun N, Ogulur I, Mitamura Y, et al. The epithelial barrier theory and its associated diseases. Allergy. 2024;79(12):3192–3237. doi:10.1111/all.16318
7. Lee H, Lee JH, Koh SJ, Park H. Bidirectional relationship between atopic dermatitis and inflammatory bowel disease: a systematic review and meta-analysis. J Am Acad Dermatol. 2020;83(5):1385–1394. doi:10.1016/j.jaad.2020.05.130
8. Chiesa Fuxench ZC, Wan J, Wang S, et al. Risk of Inflammatory Bowel Disease in Patients With Atopic Dermatitis. JAMA Dermatol. 2023;159(10):1085. doi:10.1001/jamadermatol.2023.2875
9. Jimenez-Sanchez M, Celiberto LS, Yang H, Sham HP, Vallance BA. The gut-skin axis: a bi-directional, microbiota-driven relationship with therapeutic potential. Gut Microbes. 2025;17(1):2473524. doi:10.1080/19490976.2025.2473524
10. Wang L, Wang Y, Wang XE, Chen B, Zhang L, Lu X. Causal association between atopic eczema and inflammatory bowel disease: a two-sample bidirectional Mendelian randomization study of the East Asian population. J Dermatol. 2023;50(3):327–336. doi:10.1111/1346-8138.16642
11. Lopata O, Acencio ML, Wang X, et al. Identification of shared and unique mechanisms of atopic dermatitis and ulcerative colitis by construction and computational analysis of disease maps. Comput Struct Biotechnol J. 2025;27:4007–4018. doi:10.1016/j.csbj.2025.09.008
12. Taylor PC, Choy E, Baraliakos X, et al. Differential properties of Janus kinase inhibitors in the treatment of immune-mediated inflammatory diseases. Rheumatology. 2024;63(2):298–308. doi:10.1093/rheumatology/kead448
13. Donthu N, Kumar S, Mukherjee D, Pandey N, Lim WM. How to conduct a bibliometric analysis: an overview and guidelines. J Bus Res. 2021;133:285–296. doi:10.1016/j.jbusres.2021.04.070
14. Manoj Kumar L, George RJ, A PS. Bibliometric Analysis for Medical Research. Indian J Psychol Med. 2023;45(3):277–282. doi:10.1177/02537176221103617
15. Taylor AL, Dunstan JA, Prescott SL. Probiotic supplementation for the first 6 months of life fails to reduce the risk of atopic dermatitis and increases the risk of allergen sensitization in high-risk children: a randomized controlled trial. J Allergy Clin Immunol. 2007;119(1):184–191. doi:10.1016/j.jaci.2006.08.036
16. Kalliomäki M, Salminen S, Poussa T, Isolauri E. Probiotics during the first 7 years of life: a cumulative risk reduction of eczema in a randomized, placebo-controlled trial. J Allergy Clin Immunol. 2007;119(4):1019–1021. doi:10.1016/j.jaci.2006.12.608
17. Arslanoglu S, Moro GE, Schmitt J, Tandoi L, Rizzardi S, Boehm G. Early Dietary Intervention with a Mixture of Prebiotic Oligosaccharides Reduces the Incidence of Allergic Manifestations and Infections during the First Two Years of Life. J Nutr. 2008;138(6):1091–1095. doi:10.1093/jn/138.6.1091
18. Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016;387(10023):1109–1122. doi:10.1016/S0140-6736(15)00149-X
19. Schmitt J, Schwarz K, Baurecht H, et al. Atopic dermatitis is associated with an increased risk for rheumatoid arthritis and inflammatory bowel disease, and a decreased risk for type 1 diabetes. J Allergy Clin Immunol. 2016;137(1):130–136. doi:10.1016/j.jaci.2015.06.029
20. Fleischmann R, Pangan AL, Song I, et al. Upadacitinib Versus Placebo or Adalimumab in Patients With Rheumatoid Arthritis and an Inadequate Response to Methotrexate: results of a Phase III, Double-Blind, Randomized Controlled Trial. Arthritis Rheumatol. 2019;71(11):1788–1800. doi:10.1002/art.41032
21. Narla S, Silverberg JI. Association between atopic dermatitis and autoimmune disorders in US adults and children: a cross-sectional study. J Am Acad Dermatol. 2019;80(2):382–389. doi:10.1016/j.jaad.2018.09.025
22. Kim M, Choi KH, Hwang SW, Lee YB, Park HJ, Bae JM. Inflammatory bowel disease is associated with an increased risk of inflammatory skin diseases: a population-based cross-sectional study. J Am Acad Dermatol. 2017;76(1):40–48. doi:10.1016/j.jaad.2016.08.022
23. Smolen JS, Pangan AL, Emery P, et al. Upadacitinib as monotherapy in patients with active rheumatoid arthritis and inadequate response to methotrexate (SELECT-MONOTHERAPY): a randomised, placebo-controlled, double-blind Phase 3 study. Lancet. 2019;393(10188):2303–2311. doi:10.1016/S0140-6736(19)30419-2
24. Shi X, Chen Q, Wang F. The Bidirectional Association between Inflammatory Bowel Disease and Atopic Dermatitis: a Systematic Review and Meta-Analysis. Dermatology. 2020;236(6):546–553. doi:10.1159/000505290
25. Sandborn WJ, Ghosh S, Panes J, et al. Efficacy of Upadacitinib in a Randomized Trial of Patients With Active Ulcerative Colitis. Gastroenterology. 2020;158(8):2139–2149.e14. doi:10.1053/j.gastro.2020.02.030
26. Blauvelt A, Teixeira HD, Simpson EL, et al. Efficacy and Safety of Upadacitinib vs Dupilumab in Adults With Moderate-to-Severe Atopic Dermatitis. JAMA Dermatol. 2021;157(9):1047. doi:10.1001/jamadermatol.2021.3023
27. Cohen SB, van Vollenhoven RF, Winthrop KL, et al. Safety profile of upadacitinib in rheumatoid arthritis: integrated analysis from the SELECT phase III clinical programme. Ann Rheum Dis. 2021;80(3):304–311. doi:10.1136/annrheumdis-2020-218510
28. Danese S, Vermeire S, Zhou W, et al. Upadacitinib as induction and maintenance therapy for moderately to severely active ulcerative colitis: results from three phase 3, multicentre, double-blind, randomised trials. Lancet. 2022;399(10341):2113–2128. doi:10.1016/S0140-6736(22)00581-5
29. Ytterberg SR, Bhatt DL, Mikuls TR, et al. Cardiovascular and Cancer Risk with Tofacitinib in Rheumatoid Arthritis. N Engl J Med. 2022;386(4):316–326. doi:10.1056/NEJMoa2109927
30. Guttman-Yassky E, Teixeira HD, Simpson EL, et al. Once-daily upadacitinib versus placebo in adolescents and adults with moderate-to-severe atopic dermatitis (Measure Up 1 and Measure Up 2): results from two replicate double-blind, randomised controlled phase 3 trials. Lancet. 2021;397(10290):2151–2168. doi:10.1016/S0140-6736(21)00588-2
31. Soh H, Lee HJ, Han K, et al. Atopic Diseases Are Associated With Development of Inflammatory Bowel Diseases in Korea: a Nationwide Population-based Study. Clin Gastroenterol Hepatol. 2021;19(10):2072–2081.e6. doi:10.1016/j.cgh.2020.07.049
32. Lu Z, Zeng N, Cheng Y, et al. Atopic dermatitis and risk of autoimmune diseases: a systematic review and meta-analysis. J Can Soc Allergy Clin Immunol. 2021;17(1):96. doi:10.1186/s13223-021-00597-4
33. Reich K, Teixeira HD, de Bruin-Weller M, et al. Safety and efficacy of upadacitinib in combination with topical corticosteroids in adolescents and adults with moderate-to-severe atopic dermatitis (AD Up): results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2021;397(10290):2169–2181. doi:10.1016/S0140-6736(21)00589-4
34. Rios-Carlos M, Cervantes-García D, Córdova-Dávalos LE, Bermúdez-Humarán LG, Salinas E. Unraveling the gut-skin axis in atopic dermatitis: exploiting insights for therapeutic strategies. Gut Microbes. 2024;16(1):2430420. doi:10.1080/19490976.2024.2430420
35. Iliev ID, Ananthakrishnan AN, Guo CJ. Microbiota in inflammatory bowel disease: mechanisms of disease and therapeutic opportunities. Nat Rev Microbiol. 2025;23(8):509–524. doi:10.1038/s41579-025-01163-0
36. Song H, Yoo Y, Hwang J, Na YC, Kim HS. Faecalibacterium prausnitzii subspecies–level dysbiosis in the human gut microbiome underlying atopic dermatitis. J Allergy Clin Immunol. 2016;137(3):852–860. doi:10.1016/j.jaci.2015.08.021
37. Dokoshi T, Chen Y, Cavagnero KJ, et al. Dermal injury drives a skin to gut axis that disrupts the intestinal microbiome and intestinal immune homeostasis in mice. Nat Commun. 2024;15(1):3009. doi:10.1038/s41467-024-47072-3
38. Smits HH, Engering A, van der Kleij D, et al. Selective probiotic bacteria induce IL-10–producing regulatory T cells in vitro by modulating dendritic cell function through dendritic cell–specific intercellular adhesion molecule 3–grabbing nonintegrin. J Allergy Clin Immunol. 2005;115(6):1260–1267. doi:10.1016/j.jaci.2005.03.036
39. Kwon HK, Lee CG, So JS, et al. Generation of regulatory dendritic cells and CD4+Foxp3+ T cells by probiotics administration suppresses immune disorders. Proc Natl Acad Sci. 2010;107(5):2159–2164. doi:10.1073/pnas.0904055107
40. Xie L, Alam MJ, Marques FZ, Mackay CR. A major mechanism for immunomodulation: dietary fibres and acid metabolites. Semin Immunol. 2023;66:101737. doi:10.1016/j.smim.2023.101737
41. Qi C, Li A, Su F, et al. An atlas of the shared genetic architecture between atopic and gastrointestinal diseases. Commun Biol. 2024;7(1):1696. doi:10.1038/s42003-024-07416-7
42. Jia H, Wan H, Zhang D. Innate lymphoid cells: a new key player in atopic dermatitis. Front Immunol. 2023;14:1277120. doi:10.3389/fimmu.2023.1277120
43. Meng J, Xiao H, Xu F, She X, Liu C, Canonica GW. Systemic barrier dysfunction in type 2 inflammation diseases: perspective in the skin, airways, and gastrointestinal tract. Immunol Res. 2025;73(1):60. doi:10.1007/s12026-025-09606-9
44. Hisamoto T, Suga H, Yoshizaki-Ogawa A, Sato S, Yoshizaki A. Increased Serum Levels of Tumor Necrosis Factor-like Ligand 1A in Atopic Dermatitis. Int J Mol Sci. 2023;24(3):1813. doi:10.3390/ijms24031813
45. Royeck S. Biologics in the treatment of atopic dermatitis: approved active substances and monoclonal antibodies in advanced clinical trials. Allergo J Int. 2025;34(6):159–166. doi:10.1007/s40629-025-00340-0
46. Chen Z, Jiang P, Su D, Zhao Y, Zhang M. Therapeutic inhibition of the JAK-STAT pathway in the treatment of inflammatory bowel disease. Cytokine Growth Factor Rev. 2024;79:1–15. doi:10.1016/j.cytogfr.2024.07.008
47. Loftus EV, Panés J, Lacerda AP, et al. Upadacitinib Induction and Maintenance Therapy for Crohn’s Disease. N Engl J Med. 2023;388(21):1966–1980. doi:10.1056/NEJMoa2212728
48. Burmester GR, Deodhar A, Irvine AD, et al. Safety Profile of Upadacitinib: descriptive Analysis in Over 27,000 Patient-Years Across Rheumatoid Arthritis, Psoriatic Arthritis, Axial Spondyloarthritis, Atopic Dermatitis, and Inflammatory Bowel Disease. Adv Ther. 2025;42(10):5215–5237. doi:10.1007/s12325-025-03328-y
49. Ertus C, Scailteux LM, Lescoat A, et al. Major adverse cardiovascular events in patients with atopic dermatitis treated with oral Janus kinase inhibitors: a systematic review and meta-analysis. Br J Dermatol. 2023;189(4):368–380. doi:10.1093/bjd/ljad229
50. Lin YH, Wang YC, Wu CY, Chang YT, Chen CC. Risk of Herpes Zoster With Janus Kinase Inhibitors Across Disease Indications: a Systematic Review and Network Meta-Analysis. Dermatol Ther. 2025;2025(1):2928433. doi:10.1155/dth/2928433
51. Ried JS, Li J, Zuo XB, et al. Multi-ancestry genome-wide association study of 21,000 cases and 95,000 controls identifies new risk loci for atopic dermatitis. Nat Genet. 2015;47(12):1449–1456. doi:10.1038/ng.3424
52. de Lange KM, Moutsianas L, Lee JC, et al. Genome-wide association study implicates immune activation of multiple integrin genes in inflammatory bowel disease. Nat Genet. 2017;49(2):256–261. doi:10.1038/ng.3760
53. Lazanas P, Antonatos C, Tsoumani KT, Sgourou A, Vasilopoulos Y. Shared Genetic Architecture Between Atopic Dermatitis and Autoimmune Diseases. Int J Mol Sci. 2025;26(18):9124. doi:10.3390/ijms26189124
54. Gong T, Brew BK, Lundholm C, et al. Comorbidity Between Inflammatory Bowel Disease and Asthma and Allergic Diseases: a Genetically Informed Study. Inflamm Bowel Dis. 2024;30(9):1556–1565. doi:10.1093/ibd/izae027
55. Lerchova T, Størdal K, Andersson B, Ludvigsson J, Mårild K. Atopic Dermatitis in Early Childhood and Risk of Inflammatory Bowel Disease: a Scandinavian Birth Cohort Study. J Pediatr. 2024;270:114027. doi:10.1016/j.jpeds.2024.114027
56. Akdis CA. Does the epithelial barrier hypothesis explain the increase in allergy, autoimmunity and other chronic conditions? Nat Rev Immunol. 2021;21(11):739–751. doi:10.1038/s41577-021-00538-7
57. Grieco T, Paolino G, Moliterni E, et al. Non-Skeletal Roles of Vitamin D in Skin, Gut, and Cardiovascular Disease: focus on Epithelial Barrier Function and Immune Regulation in Chronic Disease. Int J Mol Sci. 2025;26(17):8520. doi:10.3390/ijms26178520
58. Manousaki D, Paternoster L, Standl M, et al. Vitamin D levels and susceptibility to asthma, elevated immunoglobulin E levels, and atopic dermatitis: a Mendelian randomization study. PLoS Med. 2017;14(5):e1002294. doi:10.1371/journal.pmed.1002294
59. Meisinger C, Freuer D. Causal Association Between Atopic Dermatitis and Inflammatory Bowel Disease: a 2-Sample Bidirectional Mendelian Randomization Study. Inflamm Bowel Dis. 2022;28(10):1543–1548. doi:10.1093/ibd/izab329
60. Li J, Wang L, Ma Y, Liu Y. Inflammatory bowel disease and allergic diseases: a Mendelian randomization study. Pediatr Allergy Immunol. 2024;35(5):e14147. doi:10.1111/pai.14147
61. Wan M, Yang X. Does Atopic Dermatitis Increase the Risk of Inflammatory Bowel Disease? A Meta-Analysis of Data from 61 Million Participants. Int Arch Allergy Immunol. 2025;186(7):607–618. doi:10.1159/000542777
62. Rom H, Snir Y, Schwartz N, Hodak E, Leshem YA. The association between atopic dermatitis and inflammatory bowel disease in adults: a cross-sectional study in a specialized atopic dermatitis clinic. J Eur Acad Dermatol Venereol. 2024;38(7):1357–1363. doi:10.1111/jdv.19769
63. Vernero M, Saibeni S, Scalvini D, et al. Prevalence and Clinical Impact of Immune-Mediated Inflammatory Diseases in Patients with Inflammatory Bowel Disease: results from a Large Retrospective Observational Study. J Clin Med. 2024;13(4):1019. doi:10.3390/jcm13041019
64. Hua C, Liang Q, Chen S, et al. Human umbilical cord mesenchymal stem cell treatment alleviates symptoms in an atopic dermatitis-like mouse model. Stem Cell Res Ther. 2023;14(1):147. doi:10.1186/s13287-023-03365-w
65. Tak LJ, Kim HY, Ham WK, et al. Superoxide Dismutase 3-Transduced Mesenchymal Stem Cells Preserve Epithelial Tight Junction Barrier in Murine Colitis and Attenuate Inflammatory Damage in Epithelial Organoids. Int J Mol Sci. 2021;22(12):6431. doi:10.3390/ijms22126431
66. Jafar H, Alqudah D, Rahmeh R, et al. Safety and Potential Efficacy of Expanded Umbilical Cord-Derived Mesenchymal Stromal Cells in Luminal Ulcerative Colitis Patients. Stem Cells Dev. 2024;33(23–24):645–651. doi:10.1089/scd.2024.0102
67. Simpson EL, Papp KA, Blauvelt A, et al. Efficacy and Safety of Upadacitinib in Patients With Moderate to Severe Atopic Dermatitis: analysis of Follow-up Data From the Measure Up 1 and Measure Up 2 Randomized Clinical Trials. JAMA Dermatol. 2022;158(4):404. doi:10.1001/jamadermatol.2022.0029
68. Irvine AD, Prajapati VH, Guttman-Yassky E, et al. Efficacy and Safety of Upadacitinib in Patients With Moderate-to-Severe Atopic Dermatitis: phase 3 Randomized Clinical Trial Results Through 140 Weeks. Am J Clin Dermatol. 2025;26(6):1003–1016. doi:10.1007/s40257-025-00975-3
69. Winthrop KL, Vermeire S, Long MD, et al. Long-term Risk of Herpes Zoster Infection in Patients With Ulcerative Colitis Receiving Tofacitinib. Inflamm Bowel Dis. 2023;29(1):85–96. doi:10.1093/ibd/izac063
70. Russell MD, Stovin C, Alveyn E, et al. JAK inhibitors and the risk of malignancy: a meta-analysis across disease indications. Ann Rheum Dis. 2023;82(8):1059–1067. doi:10.1136/ard-2023-224049
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Successful Treatment of Atopic Dermatitis with a Predominant Nipple Involvement by Abrocitinib During COVID-19 Pandemic: A Case Report
Teng Y, Tang H, Yu Y, Fan Y, Tao X, Xu D
Journal of Asthma and Allergy 2023, 16:789-792
Published Date: 1 August 2023
Trends and Hotspots in the Health Economics Evaluation of Chronic Fatigue Syndrome
Wan H, Wei B, Qian W, Zhang J
Journal of Multidisciplinary Healthcare 2024, 17:4877-4892
Published Date: 24 October 2024
Research Trend and Future Perspectives of Traditional Chinese Medicine for Atopic Dermatitis from 2004 to 2023: A Bibliometric Analysis
Feng H, Qin Y, Li Y, Li S, Zheng Y, Yan J, Xu R, Yu S, Liang R, Wang J, Zou H
Clinical, Cosmetic and Investigational Dermatology 2024, 17:2595-2613
Published Date: 21 November 2024
Concurrent Refractory Atopic Dermatitis and Generalized Vitiligo Successfully Treated with Abrocitinib: A Case Report
Shao X, Pan X, Chen Y, Zhu Y, Chen S, Chen J
Journal of Asthma and Allergy 2024, 17:1259-1263
Published Date: 3 December 2024
Trends and Emerging Research Areas in Postoperative Sleep Disturbances: A Bibliometric Analysis
Du W, Qiao X, Liu W, Li C, Jia H
Nature and Science of Sleep 2025, 17:1021-1035
Published Date: 23 May 2025