Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Evolution of Peak Inspiratory Flow During Hospitalization of Patients with COPD – A Prospective Monocentric Observational Study
Authors Suter P ![]() , Grobéty T, Vaucher J, Grandmaison G
, Grobéty T, Vaucher J, Grandmaison G ![]()
Received 17 December 2024
Accepted for publication 25 March 2025
Published 4 April 2025 Volume 2025:20 Pages 957—969
DOI https://doi.org/10.2147/COPD.S512880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Philipp Suter,1,2 Thomas Grobéty,3 Julien Vaucher,1,4 Gaël Grandmaison1
1Division of Internal Medicine, Fribourg Hospital and University of Fribourg, Fribourg, Switzerland; 2Department for Pulmonology, Allergology and Clinical Immunology, Inselspital, University Hospital Bern, Bern, Switzerland; 3Division of Physiotherapy, Hospital of Fribourg, Fribourg, Switzerland; 4Division of Internal Medicine, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
Correspondence: Philipp Suter, Department of Pulmonary Medicine, Allergology and Clinical Immunology, University Hospital and University of Bern, Freiburgstrasse 20, Bern, 3010, Switzerland, Tel +41788921495, Email [email protected]
Purpose: Effective treatment of chronic obstructive pulmonary disease (COPD) primarily relies on treatment delivered through inhaler devices. The effectiveness of dry powder inhalers is compromised by insufficient peak inspiratory flow (PIF). Understanding the evolution of PIF during hospitalization is crucial for optimizing inhaler selection and improving patient outcomes.
Patients and Methods: A prospective monocentric observational study was conducted at Fribourg Hospital, Switzerland, from August 2022 to December 2022. PIF was assessed at hospital admission and discharge in all patients with COPD admitted to the internal medicine division. The primary outcome was the evolution of maximum PIF at a fixed medium-low resistance (R2) during hospitalization. Secondary outcomes included the variation of PIF in the intra-assessment evaluation and transitioning between sufficient and insufficient PIF.
Results: Forty-nine patients were enrolled, 61% were men and 65% experienced an acute COPD exacerbation (AECOPD). The maximum PIF for R2 increased from 64.8 ± 17.2 L/min at admission to 70.7 ± 17.9 L/min at discharge, showing a 5.9 L/min improvement (95% CI: 2.4– 9.5, p < 0.01). A hospitalization > 5 days in patients hospitalized for an AECOPD is associated with a higher increase in PIF (p < 0.05). In the intra-assessment measurement, we observed an increase in PIF in the successive measurements (p < 0.01).
Conclusion: Hospitalized patients with COPD experienced a significant increase in PIF during their stay. These results appear to be independent of the reason for hospitalization but need to be confirmed with a larger sample. Nevertheless, these findings underscore the importance of regular PIF assessment and influence inhaler selection.
Keywords: COPD, inhalers, peak inspiratory flow, peak inspiratory flow rate, chronic obstructive pulmonary disease
Introduction
Chronic obstructive pulmonary disease (COPD) poses a significant global health challenge, contributing substantially to mortality and imposing a considerable economic burden worldwide. Projections indicate a further escalation in prevalence and financial strain in the years ahead.1,2 COPD patients are susceptible to exacerbations, hospitalizations, and increased mortality rates. Inhaled self-administrated therapy is the cornerstone of pharmacological management, primarily delivered through inhaler devices.2 This way of administration offers the advantage of directly targeting receptors in the central and peripheric airways, minimizing systemic side effects.3 The primary goals of treatment include symptom control, enhancing the quality of life, preventing exacerbations, and reducing healthcare utilization, encompassing fewer hospitalizations, emergency ward visits, medical consultations and less reliever use.2 However, inhaler attributes are often overlooked, leading to handling errors, non-adapted inhalers to the patients characteristics, or inadequate peak inspiratory flow (PIF), which can compromise treatment effectiveness.4,5
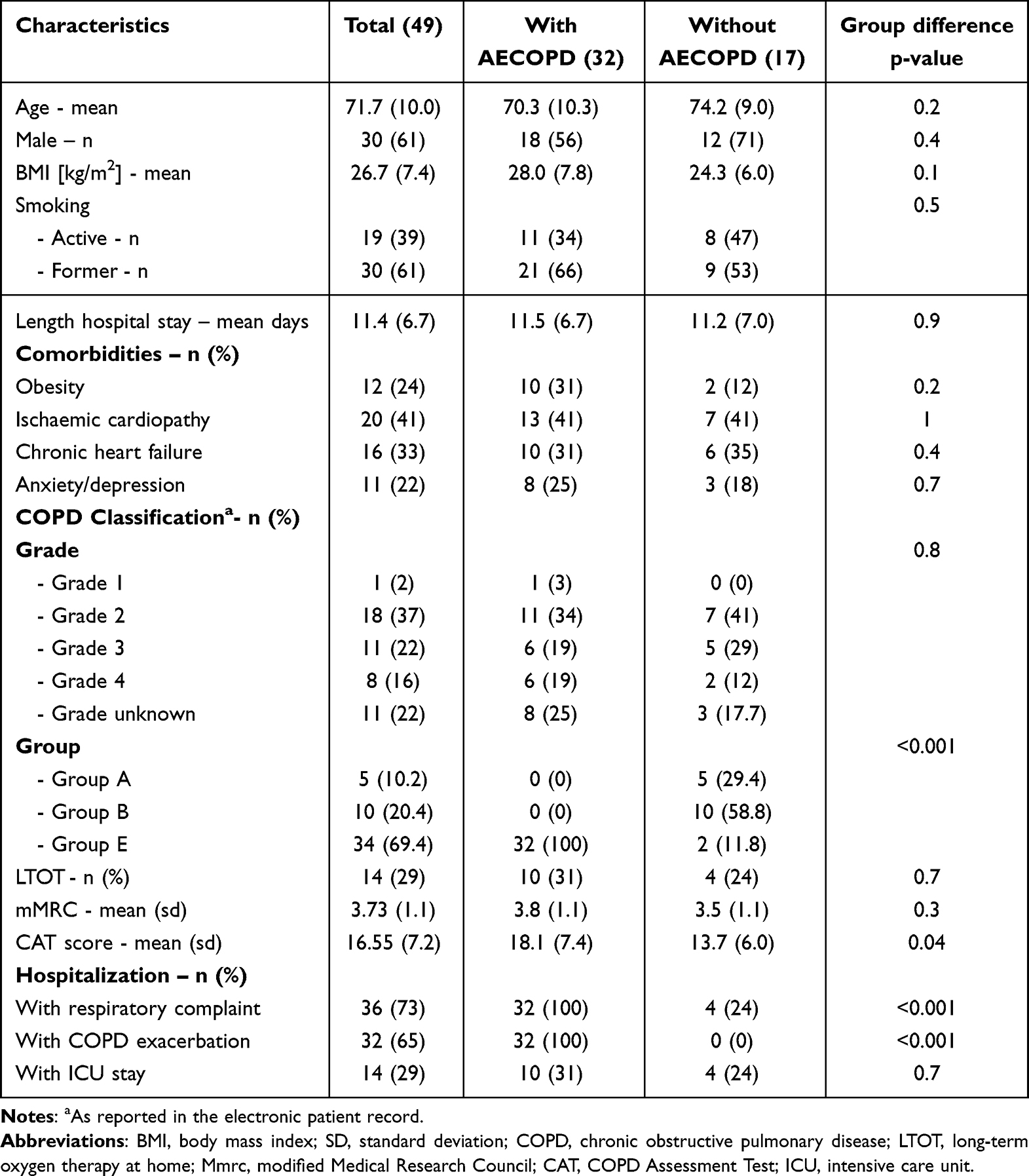 |
Table 1 Characteristics of Patients on Admission (Results are Presented with Standard Deviation or in Percentage Where Appropriate) |
Inhalers can be categorized into two types based on how they deliver medication: Pressurized metered-dose inhalers (pMDIs) and soft mist inhalers (SMIs) are activated by manual triggering by the patient. In contrast, dry powder inhalers (DPIs) require sufficient inspiratory effort to release the medication.6,7
In DPIs, a sufficient PIF is required to overcome the device’s internal resistance. This ensures proper disaggregation of the powdered drug into fine particles, leading to optimal lung deposition, consistent dose delivery, and a lower risk of side effects such as oral deposition or incomplete emptying.6–8 The internal resistance and the required PIF depend on the specific characteristics of each individual DPI.6
Many patients with COPD struggle to achieve a sufficient PIF, which can lead to suboptimal benefits from their inhaled treatment.9 This challenge is particularly prevalent during hospitalizations, with up to 56.9% of patients experiencing insufficient PIF.10–12 Insufficient PIF is associated with increased and earlier COPD exacerbations, all-cause and COPD hospitalizations, as well as poorer symptom control, a longer hospital stay, increased COPD inpatient and COPD intensive care unit (ICU) days.10,12–16 PIF-guided inhalation adaptation showed a lower probability for severe acute exacerbation of COPD (AECOPD).14
PIF tends to be lower in female gender, patients with short body stature, higher severity of COPD, lower forced vital capacity, lower inspiratory capacity, respiratory muscle weakness, hyperinflation and older patient’s age, and it is only marginally impacted by training efforts.17,18 However, there is a lack of available data regarding the evolution of PIF in hospitalized patients with COPD.19 Understanding how PIF changes over time is crucial for selecting the most suitable inhaler during hospitalization and upon discharge.
Hospitalization is a critical period for studying PIF evaluation, as it often coincides with acute physiological stress and functional decline in patients with COPD.17,20 Factors such as respiratory muscle fatigue, increased airway resistance with hyperinflation, acute confusion state and overall deconditioning may impact a patient’s ability to generate sufficient PIF, especially during AECOPD.17,21,22
Therefore, PIF can vary significantly during hospitalization and lead to sub-optimal use of inhalers. In view of the prevalence of DPIs used with insufficient PIF, hospitalization also seems to be a valuable opportunity to ensure that patients are able to use their inhaler optimally.23
We aimed to track the evolution of maximum PIF during hospitalization among patients with COPD. Additionally, we sought to identify factors associated with either an increase in PIF or persistently insufficient PIF throughout the hospital stay.
Materials and Methods
Study Participants
This prospective monocentric observational study was conducted within the internal medicine division of Fribourg Hospital, Switzerland, from 1 August 2022 to 31 December 2022. The data were collected in the context of the MIPIF study.23
All enrolled patients underwent a tailored therapeutic intervention directed by the attending physician and based on the reason for admission. Patients experiencing an AECOPD were treated with oral or intravenous steroids, and the inhalation therapy was predominantly customized to include bronchodilators administered via nebulizer while maintaining the use of their pre-hospitalization inhalers.
AECOPD was defined conforming to the GOLD report as an event marked by a worsening of respiratory symptoms, including dyspnea, cough and sputum production, which occurs over a period of less than 14 days.
In the MIPIF study, patients benefited from an intervention designed to improve inhaler use. This intervention consisted of a systematic assessment of inhalation technique and PIF on admission, therapeutic education targeted at the errors identified, and, if necessary, selection of a more suitable inhaler based on a proposed algorithm (Supplement Figure 1). Inhaler technique and PIF were also assessed at discharge.23
Inclusion Criteria
Eligibility criteria encompassed patients older than 18 years diagnosed with COPD utilizing an inhaler at home and admitted to the University Teaching and Research Hospital Fribourg (HFR) general internal medicine division. Exclusion criteria involved challenges in assessment completion due to language, physical or cognitive impediments, hospitalization for less than 72 hours, and prior study inclusion.
Assessment
Within 72 hours of admission to the internal medicine division, a research nurse conducted interviews, collecting demographic data, and details about COPD and inhaler use. Furthermore, a physiotherapist assessed PIF through a brief inspiratory maneuver using the In-Check Dial G16® (Alliance Tech Medical, Inc, Hillsborough, NC, USA), a hand-held device replicating internal resistance profiles of the currently available different inhalers.6 Physiotherapists underwent specific training in In-Check Dial G16® device use.
At admission, PIF was measured against the resistance of the inhalers used by the patient at home, named personal inhaler, and against a predefined fixed medium-low resistance R2 (Ellipta®). PIF against resistance R2 was also assessed at discharge.
We specifically choose specifically the R2 resistance, as it was already widely applied in many other studies.13,17,18,24–26 Patients generally succeed to overcome the critical threshold for lower resistances R1 and R0.27 However, patients with a moderate to severe COPD often struggle to overcome higher resistances, even though a fact noted in only few studies. Furthermore, in our country, R2 inhalers, alongside R0 devices, the most commonly used.23 As recommended in the literature, we defined 60 L/min as the sufficient PIF threshold for low to medium-high DPI, respectively, 30 L/min for high-resistance DPIs.12,28 Even small reductions in PIF below the minimal effective threshold can lead to considerable decreases in drug delivery efficiency.12
Patients were instructed to inspire as powerful as possible through the In-Check Dial G16®. We documented the highest value among three consecutive inspiratory maneuvers as the maximum PIF and the mean of these three measurements as mean PIF. The fixed resistance PIF helped to track PIF during hospitalization. If maximum PIF of the personal inhaler was below the minimum threshold flow for optimal use, the inhaler was deemed to be used with an insufficient PIF.6,28,29
Outcome
The primary outcome was the evolution of maximum PIF at a fixed medium-low resistance R2 between admission and discharge. The primary outcome was assessed across specific subgroups, according to gender, age, presence of respiratory complaint on admission, presence of COPD exacerbation, length of stay and PIF value on admission. The diagnosis of exacerbation is established based on documentation provided by the attending physician, considering hospitalization with a respiratory complaint when an increase in respiratory symptoms compared to the usual pattern was evident. A sensitivity analysis was carried out using the evolution of the mean PIF.
The secondary outcomes included the prevalence of insufficient PIF at resistance R2 and at resistance of the personal inhaler. Additionally, the study assessed the variation of the PIF in the intra-assessment evaluation and the proportion of patients transitioning from insufficient to sufficient PIF or vice versa.
Statistical Analysis
Given the exploratory nature of this study, which aims to investigate potential trends and associations in PIF evolution without predefined hypotheses, it was not feasible to calculate sample size or statistical power a priori. Consequently, the sample size was determined based on the available data, acknowledging that the results may require further validation in larger, more powered studies. The analysis was conducted exclusively on complete cases.
To analyze the primary outcome of the evolution of PIF between admission and discharge, a paired t-test was employed, with differences in PIF expressed with a 95% confidence interval. Prior to performing the t-test, the normality of the PIF difference was assessed using histograms, Q–Q plots, and the Shapiro–Wilk test.
The evolution of PIF was studied in different subgroups, namely according to sex (male vs female), age category (<70 years vs ≥70 years), presence of an AECOPD or respiratory complaint, PIF at admission (≤ mean value of PIF at admission vs > mean value of PIF at admission) and length of stay (≤5 days vs >5 days). Differences in PIF within these subgroups were compared using independent t-tests, with differences expressed with a 95% confidence interval. The normality of the difference of PIF in each group was checked using graphical methods and the Shapiro–Wilk test.
To better characterize the factors influencing the evolution of PIF between admission and discharge, a multiple linear regression model was constructed by integrating variables with a potential impact on the evolution of PIF according to the literature. The variables included in the model were age (categorized as ≥ 70 years or <70 years), sex, group classification of COPD (Group A or B vs Group E), presence of COPD exacerbation, length of hospital stay (categorized as >5 days or ≤5 days), and the initial PIF at admission.19,21 Given the existing scientific literature suggesting that the evolution of PIF during a COPD exacerbation depends on the duration of hospitalization, an interaction term between the presence of an AECOPD and the length of hospital stay was introduced into the model.19 To better describe the interaction between the presence of an AECOPD and length of stay, the difference in PIF over the course of the stay as a function of the presence or absence of a COPD exacerbation and length of stay is presented graphically.
To assess the differences between the successive PIF measurements at admission, the normality of the differences between each pair of measurements was evaluated using graphical methods and the Shapiro–Wilk test. If the normality assumption was violated, the Wilcoxon signed-rank test was employed. The results of the Wilcoxon signed-rank test are reported, highlighting the median differences along with their interquartile ranges (IQRs) and their statistical significance.
We described the transitions of patients between categories of PIF from admission to discharge. Specifically, we examined how many patients who were classified as having sufficient or insufficient PIF at admission moved to a different category at discharge.
Data are presented as mean ± standard deviation for normally distributed values, as median and interquartile range for non-normally distributed values, and as number and percentage for categorical values. All statistical tests conducted are two-sided, with a significance threshold set at 0.05. Given the exploratory nature of this study, no adjustments were made for multiple comparisons. Statistical tests were performed using STATA version 17.0 (StataCorp LLC, College Station, Texas).
Ethical Considerations
The study was approved by the Ethics Commission of the Canton of Vaud (project No: BASEC 2021–01122) and all participants provided written consent. Data anonymization and confidentiality were ensured. The results are reported in accordance with the “Strengthening the Reporting of Observational Studies in Epidemiology” statement and the study followed the principles of Declaration of Helsinki.30,31
Results
Patient Characteristics
We included 49 patients into the study. All patients underwent assessment at the fixed resistance R2 at admission and discharge and were included in the analysis.
Table 1 presents the patients’ characteristics on admission. The mean age was 72 ± 10 years, with 30 (61%) being male, 36 (73%) were hospitalized for a respiratory complaint, 32 (65%) for an AECOPD and 14 (29%) were initially admitted to the intensive care unit. The mean hospital stay was 11.4 ± 6.7 days. Except for the CAT score (p = 0.04) and patients with respiratory complaints (p < 0.001), no statistically significant differences were observed between the AECOPD group and the non-AECOPD group.
Primary Outcome
Upon admission, the mean maximum PIF measured at R2 was 64.8 ± 17.2 L/min, increasing to 70.7 ± 17.9 L/min at discharge. This resulted in a significant increase in PIF by 5.92 L/min (CI95% 2.4–9.5, p < 0.01) (Figure 1). Figure 2 illustrates the distribution of difference between admission and discharge, 30 patients (61.2%) presented an increase in PIF during hospitalization and 19 (38.8%) a decrease (Figure 2).
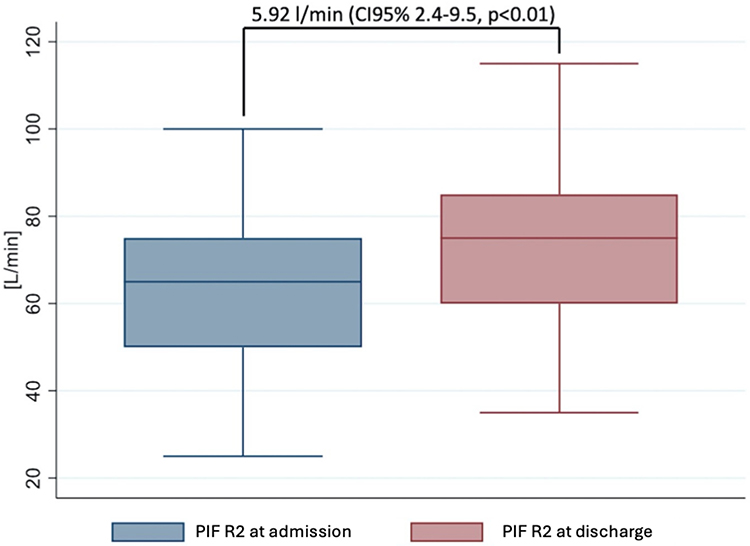 |
Figure 1 PIF at admission and discharge. Abbreviations: CI, Confidence Interval; PIF, Peak inspiratory Flow; R2, resistance level 2 measured with the In-Check Dial G16®. |
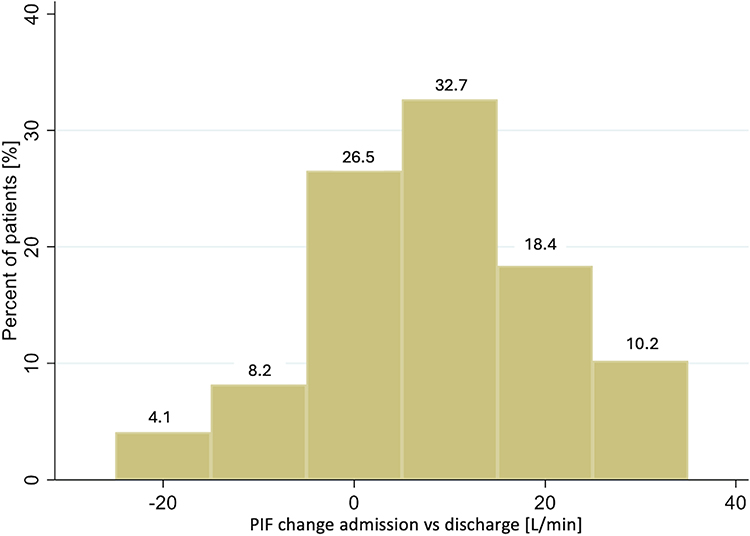 |
Figure 2 Distribution of difference of PIF at admission and discharge. Abbreviation: PIF, Peak inspiratory flow. |
This rise of PIF was also consistent in the sensitivity analysis with the mean PIF measurements, showing a difference of 6.08 L/min (CI95% 1.8–10.3, p < 0.01), transitioning from 63 ± 16.7 L/min to 69.1 ± 18.1 L/min.
In subgroup analysis, the evolution of PIF was more favorable in patients with a low initial PIF, with an age under 70, being female and hospitalized with a respiratory complaint or AECOPD. However, the evolution of PIF during the hospitalization was not statistically significant in the different subgroups (Table 2). In the AECOPD group, PIF increased by 7.34 L/min (95% CI: 3.0–11.2, p < 0.01), whereas the increase was 3.2 L/min (95% CI: −3.1–9.6, p = 0.3) in the non-AECOPD group. Although the difference between the two groups was not statistically significant, the AECOPD group showed a more substantial improvement in PIF (Table 2).
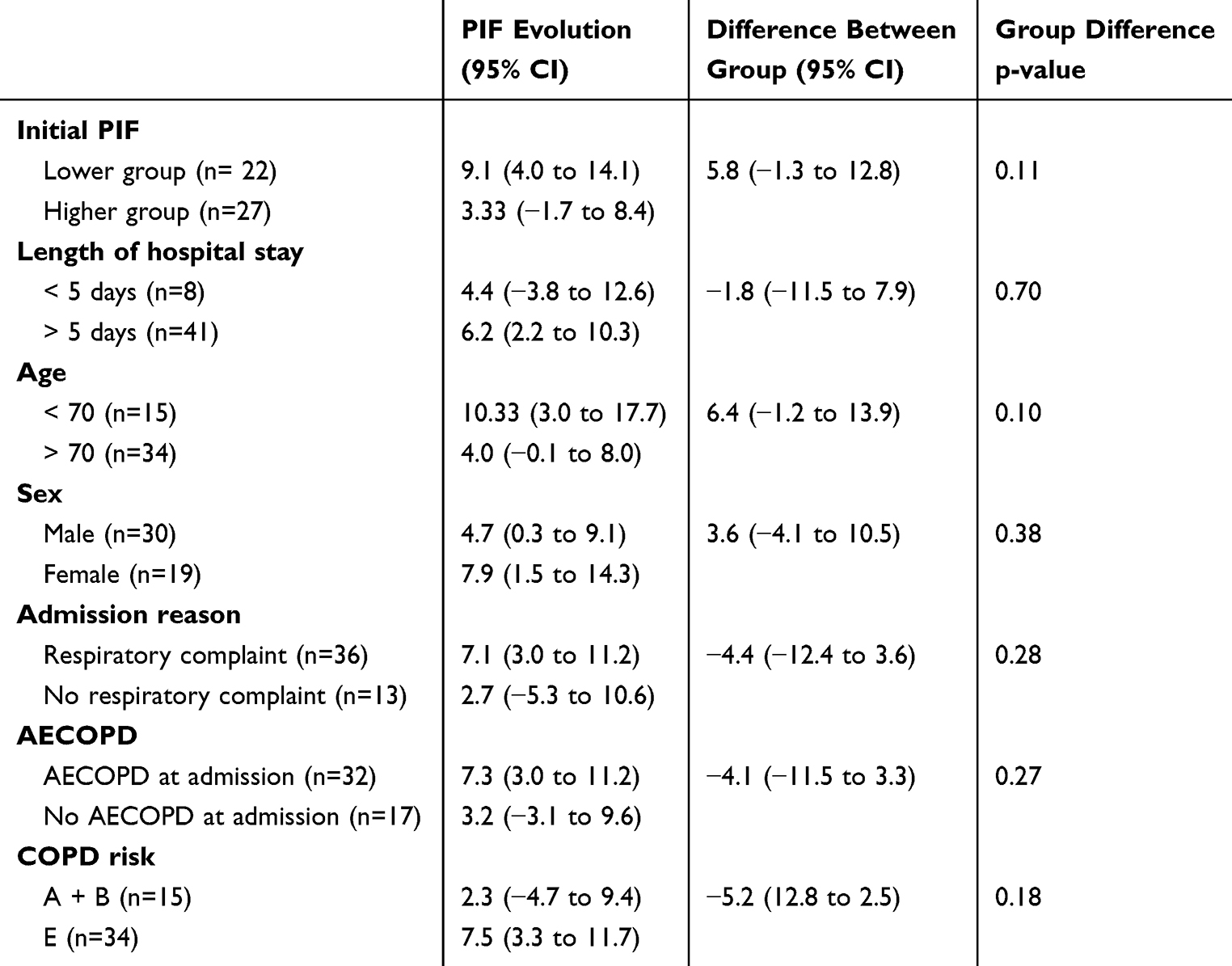 |
Table 2 Subgroup Analysis |
In the multiple linear regression model including the interaction between the presence of an AECOPD and the length of hospital stay, age under 70 (coefficient 9.3; 95% CI: 1.5–17.1, p = 0.02) and a low initial PIF (coefficient 8.6; 95% CI: 1.3–15.9, p = 0.02) were associated with a significant improvement of PIF during hospitalization (Table 3).
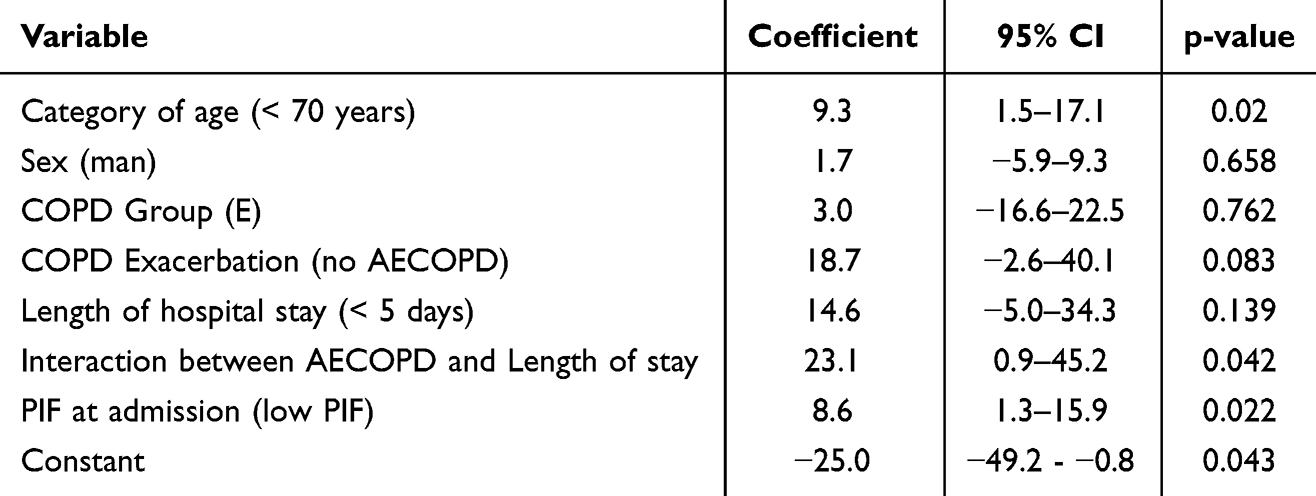 |
Table 3 Multiple Linear Regression Model with Interaction Between Length of Stay and the Presence of a COPD Exacerbation |
The analysis of the different quartiles of the length of hospital stay shows that in the first quartile (≤5 days), the PIF changes the least. In the subsequent quartiles (6–10, 11–15, and ≥16 days), there could be observed a stable and similar increase in PIF (Figure 3).
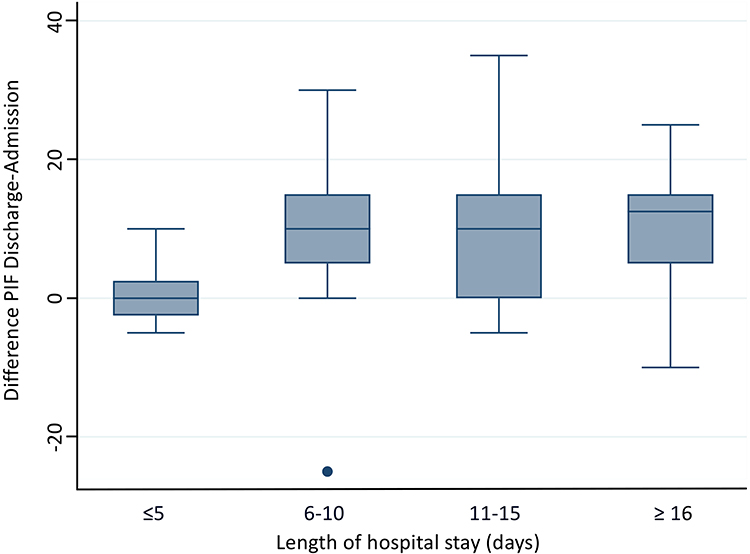 |
Figure 3 Evolution of PIF by length of hospital stay in patients with AECOPD, analyzed by quantiles. Abbreviations: PIF, Peak inspiratory flow, AECOPD, acute exacerbation of chronic obstructive pulmonary disease. |
In the absence of an AECOP, PIF improves more when the hospital spray is less than 5 days. In contrast, for patients with an AECOPD, PIF improves when the stay exceeds 5 days. In the AECOPD subgroup, the length of stay with a 5-day cut-off was associated with a significant difference in PIF (p = 0.03), whereas no significant difference was observed in patients not hospitalized for an AECOPD (p = 0.16) (Supplement Figure S2).
Secondary Outcome
Intra-Assessment Evaluation
In the intra-assessment measurement of the PIF, we observed a significant increase between the first, the second and the third measurement (each p < 0.01), independent if the measurement was performed at admission or discharge (Figure 4). The evolution of the PIF across successive measurements is consistent across the analyzed subgroups, including reasons for hospitalization (AECOPD vs non-AECOPD), and patient age (younger vs older than the median), with the only exception of the length of hospital stay (shorter vs longer than the median) (Supplement Figure S3A–E).
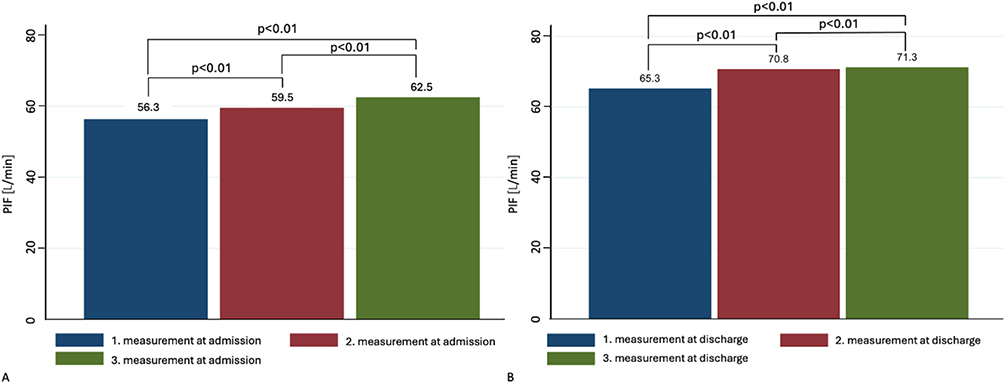 |
Figure 4 (A) Evolution of intra-assessment PIF at admission using the Wilcoxon signed-rank test. (B) Evolution of PIF intra-assessment at discharge using the Wilcoxon signed-rank test. Abbreviation: PIF, Peak inspiratory flow. |
Insufficient PIF at Admission at R2
At admission, 22 patients (44.9%) presented an insufficient maximum PIF (<60 L/min) under the R2 resistance condition, with 5 patients (6.1%) generating <30 L/min. By discharge, 19 patients still presented an insufficient PIF (38.8%). Seven patients (14.3%) transitioned from insufficient to sufficient PIF, while 4 patients (8.2%) deteriorated from sufficient to insufficient PIF. These 4 patients were all male, notably older (77.5 vs 72.0 years old) and most were hospitalized for AECOPD with an ICU stay and longer than the medium length of hospital stay. Most patients remained in their initial PIF category, 23 patients (46.9%) maintained a sufficient PIF, and 15 patients (30.6%) continued to have insufficient PIF.
PIF Personal Inhaler
Among the 49 patients analyzed upon admission, 80 personal inhaler devices were used, averaging 1.6 inhalers per patient. Of these, 40 were DPIs. Notably, no insufficient PIF was detected for pMDI, with the cut-off set at <10 L/min. However, among the DPIs assessed, 12 (30%) inhalers were used with an insufficient maximum PIF (Table 4). For high resistance inhalers, no instances of insufficient PIF were observed.
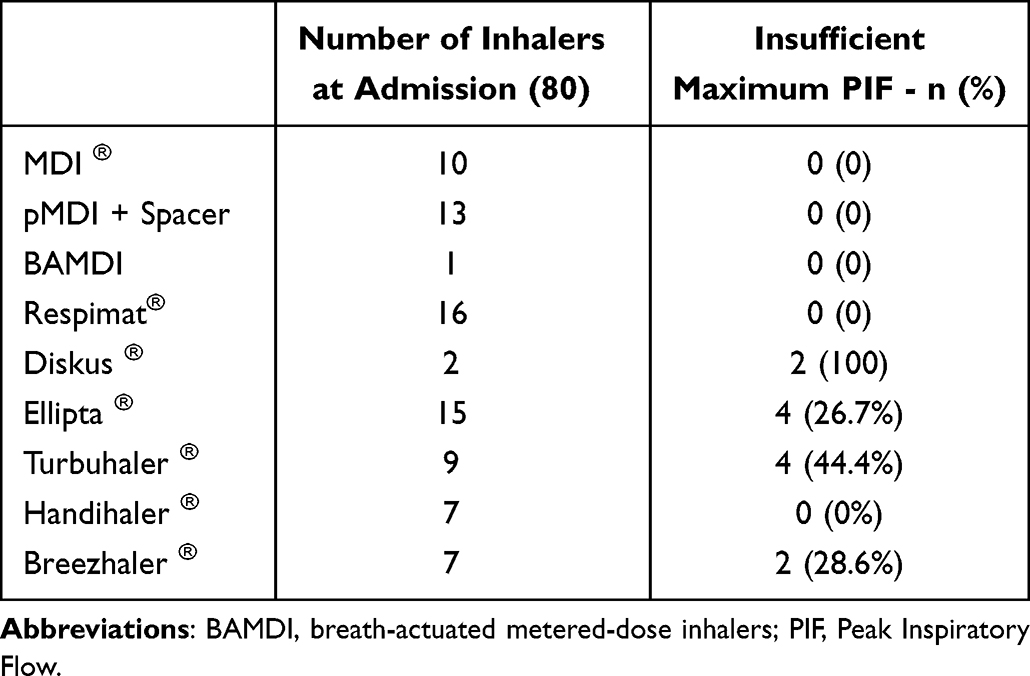 |
Table 4 Insufficient Peak Inspiratory Flow for Personal Inhaler at Admission Pressurized Metered-Dose Inhalers |
Discussion
Our study revealed an increase of maximal PIF during hospitalization by 9.1% on average, which is important clinically. The improvement in PIF was present in patients with an AECODP as a main diagnosis and also with patient without an AECOPD. Increase in PIF was mainly associated with a young age of patients and a lower PIF on admission.
To our knowledge, this is the largest prospective study assuring a consequent follow-up of PIF during hospitalization. The evolution of the PIF during hospitalization is important to consider when choosing the best time for assessment throughout the hospitalization period to ensure that the patient benefits from a suitable inhaler. Our findings align with those of Broeders et al, who observed a rise in PIF in a cohort of 15 individuals. In contrast to our observation, improvements in PIF were evident for the Turbuhaler and Diskus inhalers within the first five days of an AECOPD, after which PIF remained stable until day 50.19 A retrospective real-world clinical study by Clark et al compared PIF measured near discharge and 30 days post-hospitalization and an increase during this period was observed, meaning patients were no longer in respiratory distress at the initial measurement.12 Another study evaluated PIF once the patients was clinically stable, a moment that is difficult to define.10 We opted to exclusively monitor PIF during hospitalization rather than through remote follow-up consultations like we expected an variation of PIF throughout the hospitalization period. Our results build on these findings by demonstrating that PIF varies during hospitalization, not only in patients experiencing a COPD exacerbation but also in those hospitalized for other reasons.
Possible explanations for the increase in PIF during hospitalization include a decrease in hyperinflation during the hospital stay, especially for AECOPD. Hyperinflation has been found to negatively impact PIF.17,21,22 Improved health status during hospitalization may enhance inspiratory force by increasing strength or decreasing thoracic hyperinflation. Reduced confusion and resolution of acute confusion state by the end of hospitalization also likely contribute to better PIF.21
Bronchodilator treatment, which reduced hyperinflation and consequently improves inspiratory pressure, is an important factor influencing PIF.32 During hospital stays, treatment adherence is ensured by supervision, and with the transition to prepared nebulizer administration, optimal lung deposition is guaranteed as spontaneous non-forceful tidal breathing is sufficient for nebulizer treatment.21,33 Our patients benefited in the context of the MIPIF study of an inhaler adaptation of their standard inhaler if deemed necessary. These better adapted inhalers may influence positively our results.23 These factors may explain why PIF improvement seems to occur only after 5 days of hospitalization in patients with AECOPD, whereas those without AECOPD show an increase within the first few days.
All our patients received specific respiratory physiotherapy, including inhaler education, exercise, and muscle training. Factors such as specific inspiratory muscle training, inhaler education and exercise training positively influence PIF.34–36 Weiner et al demonstrated not only an increase in maximal PIF after inspiratory muscle training but also that all trained patients with moderate-to-severe COPD achieved the optimal PIF for adequate lung deposition following eight weeks of training.34 After inhaler technique training using in-Check-DIAL® an increase of 5.3 L/min was achieved in newly diagnosed patients with COPD, with a significant improvement in the proportion of patients achieving optimal PIF post-training. Though no increase was observed in patients with an AECOPD.37 Close training on admission and discharge could explain the improvement in PIF observed during the first few days of hospitalization in the absence of AECOPD.
Interestingly, a significant improvement in PIF was observed during intra-assessment measurements, likely due to a training effect associated with using the In-Check Dial G16®. Notably, almost no patients showed fatigue or a decrease in PIF across the three measurements, similar to the patients in the article of Broeders et al.19 This observation suggests that repeated inhalations with a DPI do not cause fatigue in patients even more a learning effect and a better coordination between expiration and deep inspiration. This point is highlighted by the study of Mahler et al, which analyzed PIF variability over a 4-week period. The study found that within-patient PIF variability decreased during this period, suggesting a potential training effect.38
In our study, even patients without an AECOPD demonstrated an increase of PIF and consequently may require inhaler adaptation. This group has been previously overlooked, as most studies have focused on patients experiencing AECOPD. The only other existing study evaluating PIF in patients with COPD, regardless of the cause of hospital admission, found that these patients tend to have a lower PIF compared to those hospitalized for an AECOPD.10 Meanwhile, patients admitted for cardiac decompensation or acute neurological conditions may also present with muscle weakness, malnutrition or deconditioning, which could be improved through treatment, leading to an increase in PIF.
Compared to other studies, we observed a low prevalence of insufficient PIF at 44.9%. In our study, a high percentage of patients used pMDI with a low resistance profile (28.8%), which could explain a lower prevalence of insufficient PIF compared to other studies. Variations in studies settings, the resistances tested, and the severity of COPD in the included patients make direct comparisons challenging.13,17,20,26 It is to mention that even lower PIF are expected in at-home measurements.38
The suboptimal use of inhalers is common, particularly among hospitalized patients, regardless of the reason for hospitalization.39 Every opportunity to improve their use should be taken, as hospitalization can affect the ability to use inhalers properly, making this evaluation even more important and interventions during hospitalization can help improve inhaler use and even led to fewer post-hospitalization health-related events.23,40 Improved inhalation techniques lead to better treatment adherence and more effective bronchodilator therapy, resulting in higher PIF values.21,24,41,42 In our study, optimal adherence was ensured through direct supervision of treatment intake.
Decrease During Hospitalization
Interestingly, some patients demonstrated sufficient PIF at admission but insufficient PIF at discharge (n = 4), while others had insufficient PIF both at admission and at discharge (n = 15). Possible explanations are longer hospitalizations or more severely ill patients with coexisting metabolic derangements, muscle wasting, loss of respiratory and peripheral muscle strength or poor nutrition.17,20 Larger samples are needed to better characterize these categories of patients.
Based on these results, we recommend an initial assessment of PIF upon hospital admission and a follow-up PIF assessment should be conducted at least at hospital discharge, ideally after the achievement of clinical stability. Although clinical stability is difficult to define. This approach ensures that the patient is receiving optimal treatment during hospital stay and upon discharge, allowing for the potential resumption of their regular therapy.
Limitations
Our study is subject to several limitations. First, it is a monocentric study within an internal medicine division. Other divisions may have patients with other characteristics that could influence the PIF outcomes.4 The small sample size limits the ability to accurately assess the impact of various parameters on the progression of PIF and in the absence of sample size calculation, our main observation should be confirmed in larger trials. Patients were tested as soon as possible after hospital admission; nevertheless, we opted for a maximum delay of 72h, permitting also to include patients during holiday and weekends where the evaluation did only take place afterwards. During the longer delay of evaluation, a hyperinflation may already be partially treated, in consequence the longer delay probably even underestimates the evolution of PIF during hospitalization.
Patients were instructed to inhale as powerful and rapidly as possible, which may not accurately reflect their actual inhalation technique during regular inhaler use and leading to an underestimation of insufficient PIF.21 The instructions given by a team of physiotherapists specialized in the respiratory field have potentially improved the results of the PIF.43
Furthermore, the COPD diagnosis was based on information available in the patients’ electronic files, and lung function results were not available for all patients. However, a previous report indicates that 87% of patients hospitalized in our division with a COPD diagnosis had confirmed obstructive pulmonary disease.44
PIF can be significantly impacted by acute bronchodilation or the patient’s physical position. Our PIF assessments were not standardized regarding the time of the day, last clinical effort, or interval after bronchodilator treatment.32 This lack of standardization may have falsely elevated PIF values if measured too close to bronchodilator administration. Additionally, we did not define the exact physical position during PIF measurement, though it is recommended to perform inhalation in an upright position to achieve the highest PIF and avoid semi-upright positions.45
Conclusion
Our findings reveal a significant increase in PIF over the hospital stay, highlighting the dynamic nature of PIF and the necessity for regular assessments to ensure patients receive optimal inhaler therapy during hospitalization and at discharge. Factors such as younger age and low PIF at admission were linked to greater PIF improvements, particularly in patients hospitalized with AECOPD or those with longer hospital stays. This suggests the need for tailored interventions based on individual patient characteristics. Our findings also underscore the importance of assessing PIF to guide inhaler adaptation, as a substantial proportion of patients used inhalers with insufficient PIF at admission. Future research should focus on identifying the optimal timing for PIF assessments, particularly in relation to clinical stability, treatment effects, and hospital discharge, to maximize the benefits of inhaler therapy.
Abbreviations
COPD, Chronic obstructive pulmonary disease; PIF, Peak inspiratory flow; pMDIs, Pressurized metered-dose inhalers; SMI, Soft mist inhaler; DPI, Dry Powder Inhalers; AECOPD, acute exacerbation of COPD; ICU, Intensive care unit; CI, Confidence interval.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The informed consent forms and study protocol was approved by the Ethics Commission of the Canton Vaud of (project number: BASEC 2021-01122). All patients provided written informed consent prior to inclusion in the study.
Acknowledgments
The authors would like to thank all the patients and their families, as well as the team of investigators involved in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by a HFR grant (Grant-2201), HFR Fribourg, Fribourg, Switzerland. The funder of the study was not involved in the study design, data collection, data analysis, data interpretation, and writing of the report.
Disclosure
Prof. Dr Julien Vaucher reports grants from SNSF, Leenaards Foundation, and AGLA, outside the submitted work. The authors declare that they have no other known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
2. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: gold executive summary. Eur Respir J. 2023;61(4):2300239. doi:10.1183/13993003.00239-2023
3. Borghardt JM, Kloft C, Sharma A. Inhaled therapy in respiratory disease: the complex interplay of pulmonary kinetic processes. Can Respir J. 2018;2018:2732017. doi:10.1155/2018/2732017
4. Renaud Y, Suter P, Grandmaison G. Patient characteristics to consider when selecting an inhaler for the treatment of chronic obstructive pulmonary disease and available assessment methods: a narrative review. Respiration. 2023;102(6):416–425. doi:10.1159/000530277
5. Bonini M, Usmani OS. The importance of inhaler devices in the treatment of COPD. COPD Res Pract. 2015;1(1):9. doi:10.1186/s40749-015-0011-0
6. Sanders MJ. Guiding inspiratory flow: development of the in-check DIAL G16, a tool for improving inhaler technique. Pulm Med. 2017;2017:e1495867. doi:10.1155/2017/1495867
7. Chrystyn H, van der Palen J, Sharma R, et al. Device errors in asthma and COPD: systematic literature review and meta-analysis. NPJ Prim Care Respir Med. 2017;27(1):22. doi:10.1038/s41533-017-0016-z
8. Mahler DA. The role of inspiratory flow in selection and use of inhaled therapy for patients with chronic obstructive pulmonary disease. Respir Med. 2020;161:105857. doi:10.1016/j.rmed.2019.105857
9. Mahler DA, Halpin DMG. Peak inspiratory flow as a predictive therapeutic biomarker in COPD. Chest. 2021;160(2):491–498. doi:10.1016/j.chest.2021.03.049
10. Mahler DA, Demirel S, Hollander R, et al. High prevalence of suboptimal peak inspiratory flow in hospitalized patients with COPD: a real-world study. Chronic Obstr Pulm Dis. 2022;9(3):427–438. doi:10.15326/jcopdf.2022.0291
11. Molimard M, Raherison C, Lignot S, et al. Chronic obstructive pulmonary disease exacerbation and inhaler device handling: real-life assessment of 2935 patients. Eur Respir J. 2017;49(2). doi:10.1183/13993003.01794-2016
12. Clark B, Wells BJ, Saha AK, et al. low peak inspiratory flow rates are common among COPD inpatients and are associated with increased healthcare resource utilization: a retrospective cohort study. Int J Chron Obstruct Pulmon Dis. 2022;17:1483–1494. doi:10.2147/COPD.S355772
13. Loh CH, Peters SP, Lovings TM, Ohar JA. Suboptimal inspiratory flow rates are associated with chronic obstructive pulmonary disease and all-cause readmissions. Ann Am Thorac Soc. 2017;14(8):1305–1311. doi:10.1513/AnnalsATS.201611-903OC
14. Chen SY, Huang CK, Peng HC, et al. Peak-inspiratory-flow-rate guided inhalation therapy reduce severe exacerbation of COPD. Front Pharmacol. 2021;12:704316. doi:10.3389/fphar.2021.704316
15. Mahler DA, Niu X, Deering KL, Dembek C. Prospective evaluation of exacerbations associated with suboptimal peak inspiratory flow among stable outpatients with COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:559–568. doi:10.2147/COPD.S353441
16. Mahler DA, Waterman LA, Ward J, Gifford AH. Comparison of dry powder versus nebulized beta-agonist in patients with COPD who have suboptimal peak inspiratory flow rate. J Aerosol Med Pulm Drug Deliv. 2014;27(2):103–109. doi:10.1089/jamp.2013.1038
17. Ohar JA, Mahler DA, Davis GN, Lombardi DA, Moran EJ, Crater GD. Clinical burden of chronic obstructive pulmonary disease in patients with suboptimal peak inspiratory flow. Can Respir J. 2024;2024:8034923. doi:10.1155/2024/8034923
18. Prime D, de Backer W, Hamilton M, et al. Effect of disease severity in asthma and chronic obstructive pulmonary disease on inhaler-specific inhalation profiles through the ELLIPTA® dry powder inhaler. J Aerosol Med Pulm Drug Deliv. 2015;28(6):486–497. doi:10.1089/jamp.2015.1224
19. Broeders MEAC, Molema J, Hop WCJ, Vermue NA, Folgering HTM. The course of inhalation profiles during an exacerbation of obstructive lung disease. Respir Med. 2004;98(12):1173–1179. doi:10.1016/j.rmed.2004.04.010
20. Samarghandi A, Ioachimescu OC, Qayyum R. Association between peak inspiratory flow rate and hand grip muscle strength in hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease. PLoS One. 2020;15(1):e0227737. doi:10.1371/journal.pone.0227737
21. Leving MT, van Boven JFM, Bosnic-Anticevich SZ, et al. Suboptimal peak inspiratory flow and critical inhalation errors are associated with higher COPD-related healthcare costs. Int J Chron Obstruct Pulmon Dis. 2022;17:2401–2415. doi:10.2147/COPD.S380736
22. Duarte AG, Tung L, Zhang W, Hsu ES, Kuo YF, Sharma G. Spirometry measurement of peak inspiratory flow identifies suboptimal use of dry powder inhalers in ambulatory patients with COPD. Chronic Obstr Pulm Dis. 2019;6(3):246–255. doi:10.15326/jcopdf.6.3.2018.0163
23. Grandmaison G, Grobéty T, Dumont P, Vaucher J, Hayoz D, Suter P. An in-hospital intervention to reduce the proportion of misused inhalers at hospital discharge among patients with COPD: a non-randomised intervention study. Swiss Med Wkly. 2024;154:3394. doi:10.57187/s.3394
24. Sharma G, Mahler DA, Mayorga VM, Deering KL, Harshaw O, Ganapathy V. Prevalence of low peak inspiratory flow rate at discharge in patients hospitalized for COPD exacerbation. Chronic Obstr Pulm Dis. 2017;4(3):217–224. doi:10.15326/jcopdf.4.3.2017.0183
25. Janssens W, VandenBrande P, Hardeman E, et al. Inspiratory flow rates at different levels of resistance in elderly COPD patients. Eur Respir J. 2008;31(1):78–83. doi:10.1183/09031936.00024807
26. Mahler DA, Waterman LA, Gifford AH. Prevalence and COPD phenotype for a suboptimal peak inspiratory flow rate against the simulated resistance of the Diskus® dry powder inhaler. J Aerosol Med Pulm Drug Deliv. 2013;26(3):174–179. doi:10.1089/jamp.2012.0987
27. Chen SY, Huang CK, Peng HC, Yu CJ, Chien JY. Inappropriate peak inspiratory flow rate with dry powder inhaler in chronic obstructive pulmonary disease. Sci Rep. 2020;10(1):7271. doi:10.1038/s41598-020-64235-6
28. Barnes CN, Mahler DA, Ohar JA, Lombardi DA, Crater GD. Peak inspiratory flows: defining repeatability limits and a predictive equation for different inhalers. Chest. 2020;158(4):1413–1419. doi:10.1016/j.chest.2020.03.072
29. Ghosh S, Ohar JA, Drummond MB. Peak inspiratory flow rate in chronic obstructive pulmonary disease: implications for dry powder inhalers. J Aerosol Med Pulm Drug Deliv. 2017;30(6):381–387. doi:10.1089/jamp.2017.1416
30. von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg Lond Engl. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
31. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053.
32. Pleasants RA, Shaikh A, Henderson AG, Bayer V, Drummond MB. Changes in peak inspiratory flow after acute bronchodilation: an observational study of patients with stable chronic obstructive pulmonary disease. J Aerosol Med Pulm Drug Deliv. 2024;37(4):171–179. doi:10.1089/jamp.2023.0045
33. Mahler DA, Ohar JA, Barnes CN, Moran EJ, Pendyala S, Crater GD. Nebulized versus dry powder long-acting muscarinic antagonist bronchodilators in patients with COPD and suboptimal peak inspiratory flow rate. Chronic Obstr Pulm Dis. 2019;6(4):321–331. doi:10.15326/jcopdf.6.4.2019.0137
34. Weiner P, Weiner M. Inspiratory muscle training may increase peak inspiratory flow in chronic obstructive pulmonary disease. Respiration. 2006;73(2):151–156. doi:10.1159/000088095
35. Al-Showair RAM, Tarsin WY, Assi KH, Pearson SB, Chrystyn H. Can all patients with COPD use the correct inhalation flow with all inhalers and does training help? Respir Med. 2007;101(11):2395–2401. doi:10.1016/j.rmed.2007.06.008
36. Chen R, Chen R, Chen X, Chen L. Effect of endurance training on expiratory flow limitation and dynamic hyperinflation in patients with stable chronic obstructive pulmonary disease. Intern Med J. 2014;44(8):791–800. doi:10.1111/imj.12483
37. Hua JL, Ye XF, Du CL, et al. Optimizing inhalation therapy in the aspect of peak inhalation flow rate in patients with chronic obstructive pulmonary disease or asthma. BMC Pulm Med. 2021;21(1):302. doi:10.1186/s12890-021-01674-5
38. Mahler DA, Watz H, Emerson-Stadler R, et al. Clinical implications of peak inspiratory flow in COPD: post Hoc analyses of the TRONARTO study. Int J Chron Obstruct Pulmon Dis. 2023;18:1729–1740. doi:10.2147/COPD.S404243
39. Grandmaison G, Grobéty T, Vaucher J, Hayoz D, Suter P. Prevalence of critical errors and insufficient peak inspiratory flow in patients hospitalized with COPD in a department of general internal medicine: a cross-sectional study. Chronic Obstr Pulm Dis. 2024. doi:10.15326/jcopdf.2024.0505
40. Press VG, Arora VM, Shah LM, et al. Teaching the use of respiratory inhalers to hospitalized patients with asthma or COPD: a randomized trial. J Gen Intern Med. 2012;27(10):1317–1325. doi:10.1007/s11606-012-2090-9
41. Ding N, Zhang W, Wang Z, et al. prevalence and associated factors of suboptimal daily peak inspiratory flow and technique misuse of dry powder inhalers in outpatients with stable chronic airway diseases. Int J Chron Obstruct Pulmon Dis. 2021;16:1913–1924. doi:10.2147/COPD.S311178
42. Kawamatawong T, Khiawwan S, Pornsuriyasak P. Peak inspiratory flow rate measurement by using in-check DIAL for the different inhaler devices in elderly with obstructive airway diseases. J Asthma Allergy. 2017;10:17–21. doi:10.2147/JAA.S127580
43. Melani AS, Bracci LS, Rossi M. Reduced peak inspiratory effort through the diskus((R)) and the turbuhaler((R)) due to mishandling is common in clinical practice. Clin Drug Investig. 2005;25(8):543–549. doi:10.2165/00044011-200525080-00007
44. Tschopp J, Dumont P, Hayoz D. True prevalence of COPD and its association with peripheral arterial disease in the internal medicine ward of a tertiary care hospital. Swiss Med Wkly. 2017;147:w14460. doi:10.4414/smw.2017.14460
45. Pleasants RA, Henderson AG, Bayer V, Shaikh A, Drummond MB. Effect on physical position of peak inspiratory flow in stable COPD: an observational study. Chronic Obstr Pulm Dis. 2024;11(2):174–186. doi:10.15326/jcopdf.2023.0460
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Phenotyping COPD Patients with Emphysema Distribution Using Quantitative CT Measurement; More Severe Airway Involvement in Lower Dominant Emphysema
Park J, Kim EK, Lee SH, Kim MA, Kim JH, Lee SM, Lee JS, Oh YM, Lee SD, Lee JH
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2013-2025
Published Date: 31 August 2022
Chronic Obstructive Pulmonary Disease Prevalence and Associated Risk Factors in Adults Aged 40 Years and Older in Southeast China: A Cross-Sectional Study During 2019–2020
Chen J, Yin Y, Zhang Y, Lin X, Chen T, Yang Z, Wang D, Zhong W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2317-2328
Published Date: 17 September 2022
Effects of High-Frequency Chest Wall Oscillation on Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Huang HP, Chen KH, Tsai CL, Chang WP, Chiu SYH, Lin SR, Lin YH
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2857-2869
Published Date: 10 November 2022
Prevalence of Chronic Obstructive Pulmonary Disease in England from 2000 to 2019
Stone PW, Osen M, Ellis A, Coaker R, Quint JK
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1565-1574
Published Date: 21 July 2023
A Long-Term Study of Adverse Outcomes Associated With Oral Corticosteroid Use in COPD

Tse G, Emmanuel B, Ariti C, Bafadhel M, Papi A, Carter V, Zhou J, Skinner D, Xu X, Müllerová H, Price D
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2565-2580
Published Date: 15 November 2023