")
Back to Journals » OncoTargets and Therapy » Volume 14
Evaluation of the UK Myeloma Research Alliance Risk Profile in Chinese Patients with Newly Diagnosed Multiple Myeloma without Autologous Stem Cell Transplantation
Authors Ma K, Ye J , Wang L, Sun C, Zhou X
Received 9 January 2021
Accepted for publication 25 February 2021
Published 6 April 2021 Volume 2021:14 Pages 2349—2361
DOI https://doi.org/10.2147/OTT.S300834
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Takuya Aoki
Kewa Ma,* Jiannan Ye,* Lingling Wang, Chao Sun, Xin Zhou
Department of Hematology, Affiliated Wuxi People’s Hospital, Nanjing Medical University, Wuxi, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chao Sun; Xin Zhou
Department of Hematology, Affiliated Wuxi People’s Hospital, Nanjing Medical University, Wuxi, Jiangsu, 214000, People’s Republic of China
Tel +86-15961806698; +86 51085350201
Fax +86 51085350201
Email [email protected]; [email protected]
Purpose: Recently, the British Myeloma Research Alliance put forward a Myeloma Risk Profile (MRP) for the first time to stratify the prognosis risk of non-transplanted patients with multiple myeloma. However, only limited studies have evaluated the applicability of this model in the Chinese population. This study aimed to estimate the prognostic value of MRP in newly diagnosed multiple myeloma patients without autologous stem cell transplantation in China.
Patients and Methods: Patients with multiple myeloma in Wuxi People’s Hospital from January 1, 2007, to June 30, 2018 were evaluated based on the MRP score, and the relationship between the clinical outcome of patients with MM and the score was analyzed retrospectively.
Results: First, significant differences were observed in the overall survival (OS) (P< 0.05) and progression-free survival (PFS) (P< 0.05) between the low-, middle-, and high-risk groups. Second, in the bortezomib treatment subgroup and complex chromosome karyotype subgroup, OS and PFS were significantly shorter in the high-risk group than in the low-risk group (P< 0.05). Third, the depth of remission still showed prognostic significance in the high-risk MRP group.
Conclusion: MRP is also applicable in Chinese patients with newly diagnosed MM who did not undergo transplantation, as it is simple and cost effective; hence, it is worth popularizing.
Keywords: multiple myeloma, myeloma risk profile, bortezomib, complex chromosome karyotype, prognosis
Introduction
GA scoring, R-ISS staging, and mSMART staging based on host and tumor factors, respectively, provide beneficial clinical value for estimating the prognosis of multiple myeloma.1–3 However, mSMART staging mainly focuses on cytogenetics, while GA scoring pays attention to the host factors and is rather complicated. In clinical practice, these staging systems have certain limitations. In 2019, the British Myeloma Research Alliance put forward a Myeloma Risk Profile (MRP) for the first time to stratify the prognosis risk of non-transplant patients with multiple myeloma.4 This prognosis model combines host factors and tumor load burden, which is simple and feasible. MRP shows a good prognosis in transplant-ineligible MM patients. However, only a few relevant studies have reported the applicability of this model in the real-world setting, especially in the Chinese population. In this study, the prognosis of 242 newly diagnosed non-transplanted MM patients was analyzed retrospectively to determine whether this scoring model is beneficial for predicting the clinical outcomes.
Patients and Methods
Patients
A total of 242 patients with newly diagnosed multiple myeloma in the Department of Hematology of Wuxi People’s Hospital from January 1, 2007 to June 30, 2018 were included in this study. Among them, 82 patients used traditional non-bortezomib-based (such as COMP, VAD, etc.) chemotherapy schemes due to personal and disease factors, while 160 used a protocol containing bortezomib (such as PAD, VTD, etc.). All patients were administered with thalidomide (75–150 mg) as maintenance treatment during the intermission period of chemotherapy. None of the MM patients included in the study underwent hematopoietic stem cell transplantation due to personal and disease factors. This research was carried out under agreements from the patients along with a written informed consent. It was approved by the ethics committee of the Affiliated Wuxi People’s Hospital, Nanjing Medical University, and conducted in accordance with the Declaration of Helsinki.
Follow-Up Parameters
The following parameters were evaluated: age, sex, WHO PS score, C-reactive protein (CRP), serum albumin (ALB), serum β2-microglobulin (β2-GM), ISS stage, lactate dehydrogenase (LDH), hemoglobin (Hb), serum creatinine (Cr), serum Ca2+, chromosomal karyotype, tumor cell ratio of bone marrow smear, treatment plan, remission depth after chemotherapy, comorbidities, total survival time (OS), and progression-free survival (PFS); the depth of remission after chemotherapy refers to the IMWG consensus criteria in 2016.5
MRP Score
The MRP score is calculated by combining the WHO PS score, ISS stage, age, and CRP, and is obtained using the following formula: (PS score − 2) × 0.199+ (age − 74.4) × 0.0165 + (ISS stage − 2) * 0.212+ [log (CRP+1) − 2.08] × 0.0315. Individuals with a score of < −0.256 were classified as the low-risk group, while those with a score of −0.256 ≤ score ≤ −0.0283 and > −0.0283 were classified as the medium-risk group and high-risk group respectively.6
Statistical Methods
For the continuous data, the Kruskal–Wallis nonparametric test was used to compare the differences among the groups. For the counting data, the chi-square test was used to compare the differences among groups, while the Fisher’s exact test was used for correction of multiple comparisons when needed. The Kaplan-Meier method was used for survival analysis, while the Log rank test was used for the analysis of survival difference. A P value of <0.05 was considered significant.
Results
Prognosis of the Overall Population
Based on the MRP score, 242 patients were divided into three groups: low-risk, medium-risk, and high-risk groups. As shown in Table 1, except for Cr level, other factors such as sex, Hb, LDH, serum Ca2+ level, tumor cell ratio, chemotherapy reaction, comorbidities, chromosome karyotype, and treatment plan were not significantly different.
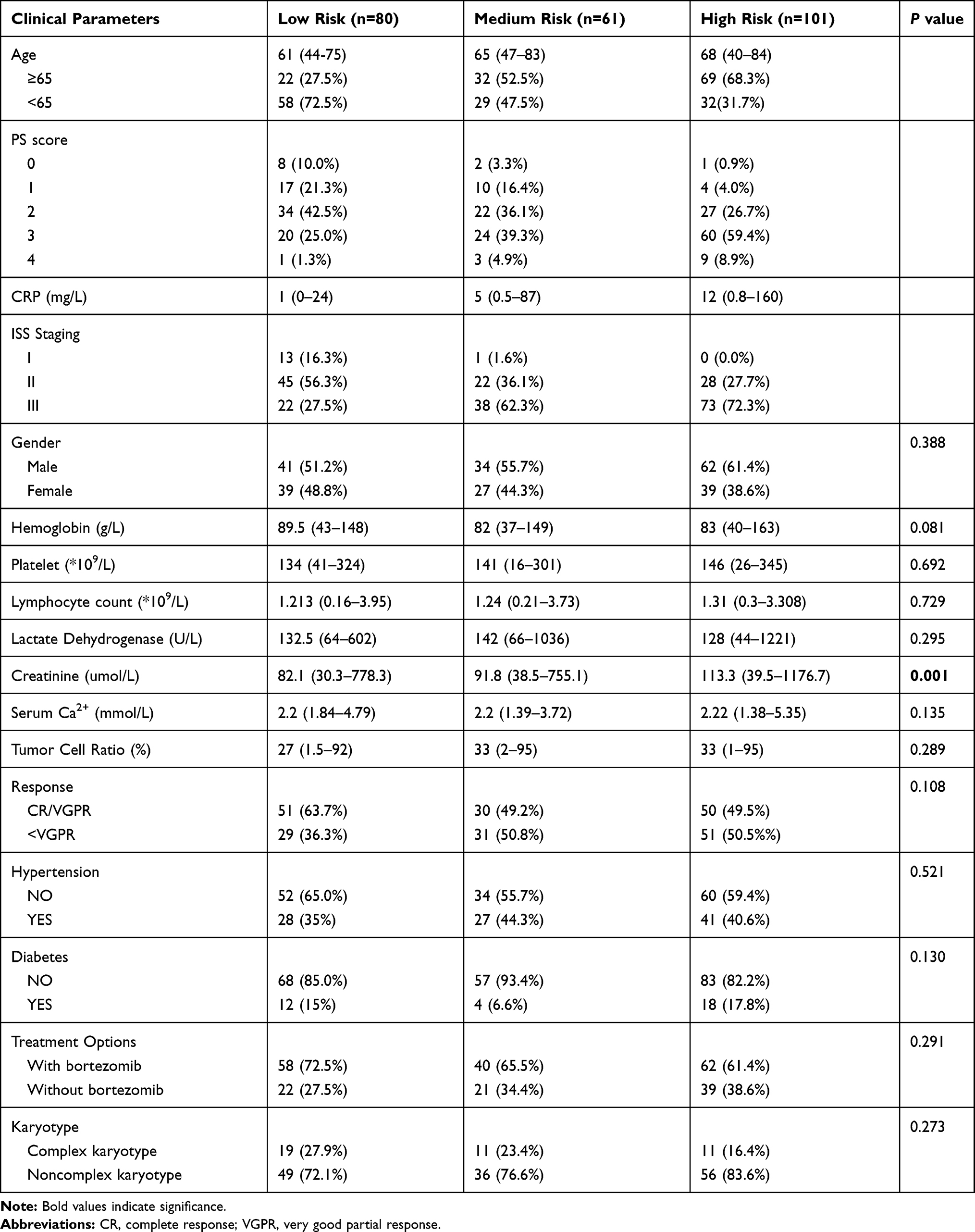 |
Table 1 Clinical Characteristics of Overall Patients of Different MRP Stratification |
As shown in Figure 1, the median OS of the low-risk, medium-risk, and high-risk groups were 48, 37, and 29 months, respectively; meanwhile, the median PFS of the low-risk, medium-risk, and high-risk groups were 31, 25, and 20 months, respectively. There were significant differences in OS (P=0.003) and PFS (P=0.007) among the three groups, and the OS and PFS in the medium-risk and high-risk groups were shorter.
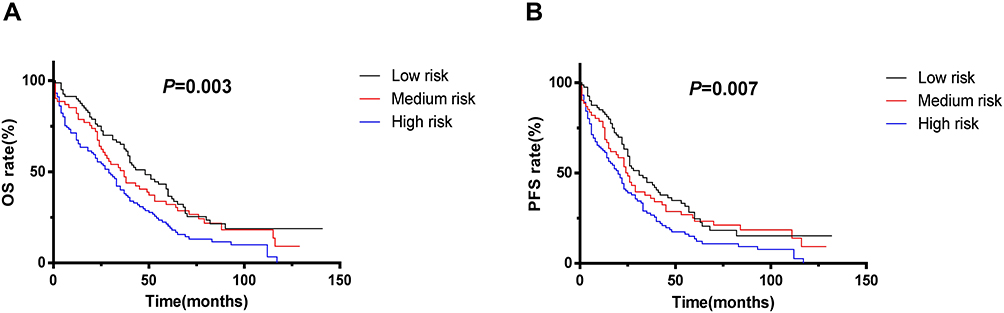 |
Figure 1 (A) The medium OS of overall 242 patients in MRP low-risk, medium-risk and high-risk groups were 48 months, 37 months and 29 months respectively. (B) The medium PFS of overall 242 patients in MRP low-risk, medium-risk and high-risk groups were 31 months, 25 months and 20 months respectively. Abbreviations: OS, the overall survival time; PFS, the progression-free survival time. |
Prognosis of Different MRP Stratifications in the Treatment Subgroup Receiving Bortezomib
The 160 patients who received bortezomib regimen were divided into low-risk, medium-risk, and high-risk groups. As shown in Table 2, the serum Cr level in the high-risk group increased significantly, while the other baseline characteristics such as sex, Hb, and so on were not significantly different.
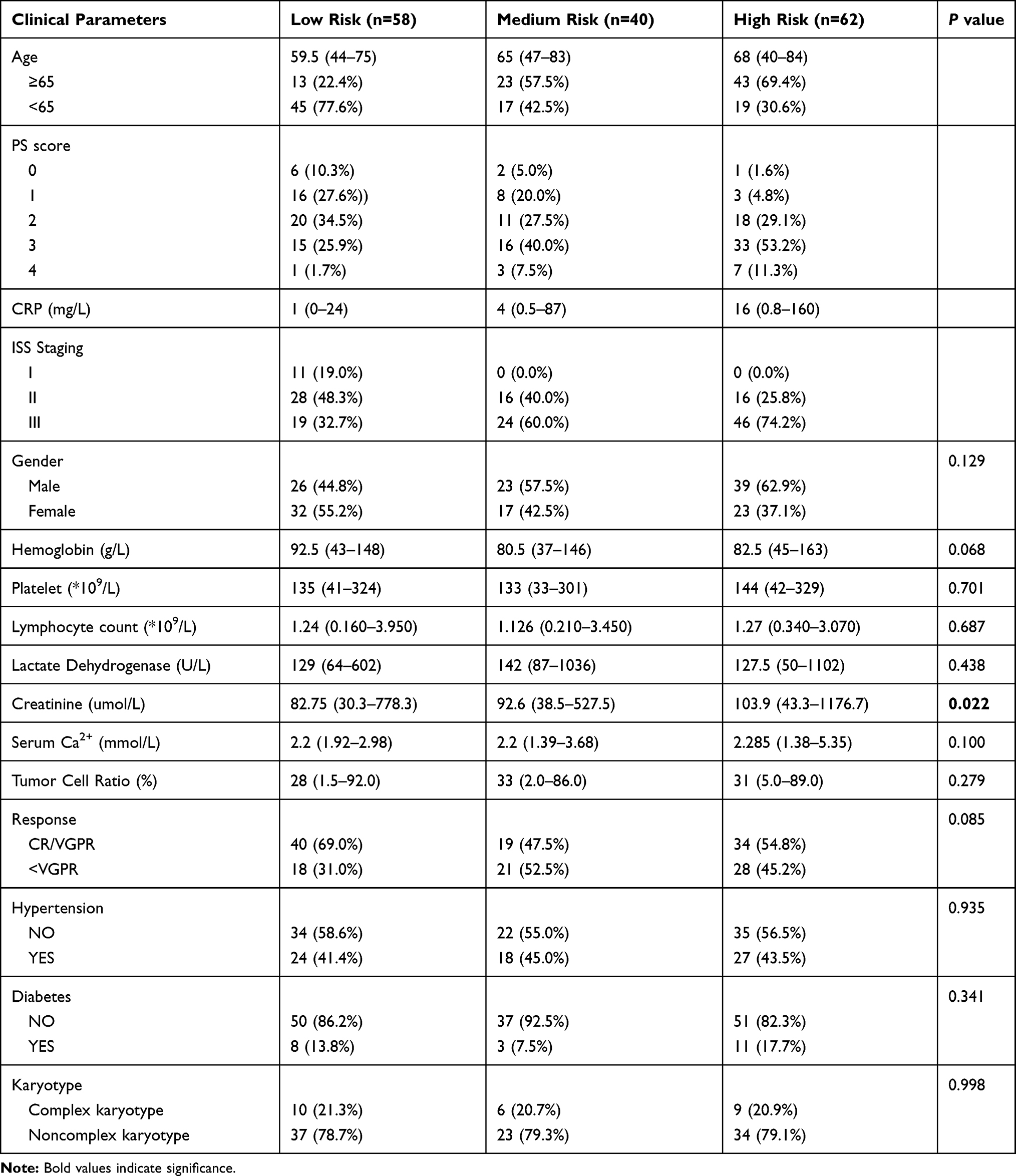 |
Table 2 Clinical Characteristics of Patients Treated with Bortezomib of Different MRP Stratification |
As shown in Figure 2A and B, the median OS of the low-risk, medium-risk, and high-risk groups were 48, 30, and 32 months, respectively, while their median PFS were 31, 24, and 22 months, respectively. The median OS (P=0.019) and median PFS (P=0.013) were significantly different among the three groups.
 |
Figure 2 (A) The medium OS of patients treated with bortezomib in MRP low-risk, medium-risk and high-risk groups were 48 months, 30 months and 32 months respectively; (B) the median PFS of patients treated with bortezomib in MRP low-risk, medium-risk and high-risk groups were 31 months, 24 months and 22 months respectively; (C) the medium OS of patients treated with bortezomib in ISS I, ISS II and ISS III groups were 65 months, 43 months and 33 months respectively; (D) the median PFS of patients treated with bortezomib in ISS I, ISS II and ISS III groups were 57 months, 26 months and 25 months respectively. |
Meanwhile, patients treated with bortezomib were divided into three groups by ISS stage as we found that there was a certain correlation between the MRP scoring system and ISS staging (Spearman correlation coefficient, r=0.408, P<0.05). The median OS of patients in the ISS I, ISS II, and ISS III groups were 65, 43, and 33 months, respectively; their median PFS were 57 months, 26 months, and 25 months, respectively. However, no significant difference was observed in the OS and PFS (P>0.05) in the ISS I, ISS II, and ISS III groups (Figure 2C and D).
MRP-Stratified Prognosis of Patients with Complex Chromosome Karyotype Abnormality
Of the 242 newly diagnosed non-transplanted MM patients, 182 underwent chromosome tests (including G+R banding, FISH) due to personal preference and presence of economic conditions. Among the 182 patients, 41 had complex chromosomal karyotype abnormalities (According to G+R banding and FISH detection, three or more kinds of chromosomal abnormalities were defined as complex karyotype, and those if they did not reach the standard of complex karyotype or no abnormalities were defined as others.) as shown on the results of G+R banding and FISH. In this subgroup, no significant differences were observed in other baseline characteristics except serum Cr level and serum Ca2+ level in the MRP low-risk group and middle-high-risk group (Table 3). The median OS and PFS of the MRP-stratified low-risk group were 31 months and 25 months, respectively, while those of the MRP-stratified medium-to-high-risk groups were 12 months and 8 months, respectively. The OS (P=0.004) and PFS (P=0.007) were significantly shorter in the middle-to-high-risk group than in the low-risk group (Figure 3).
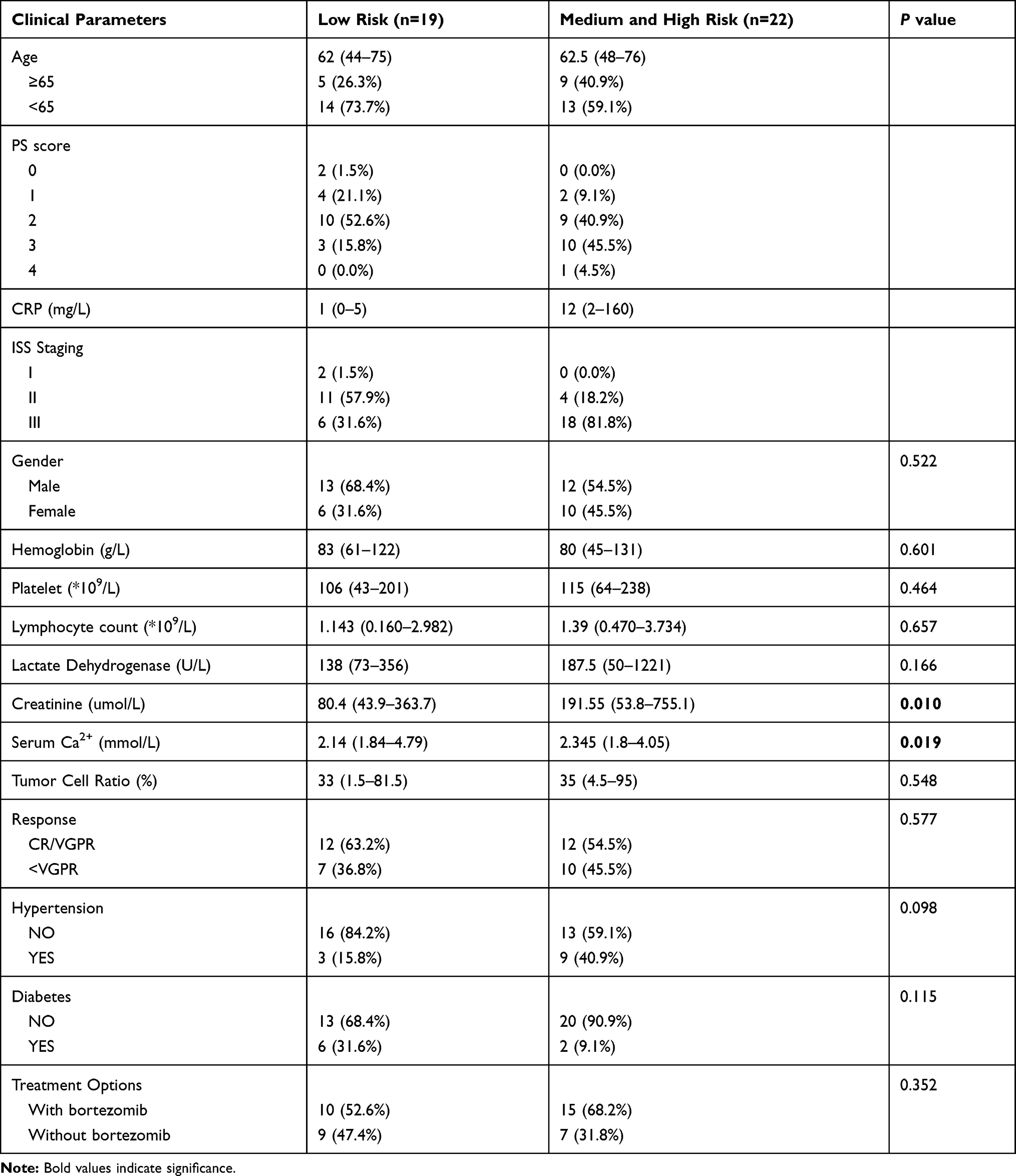 |
Table 3 Clinical Characteristics of Patients with Complex Chromosomal Karyotype of Different MRP Stratification |
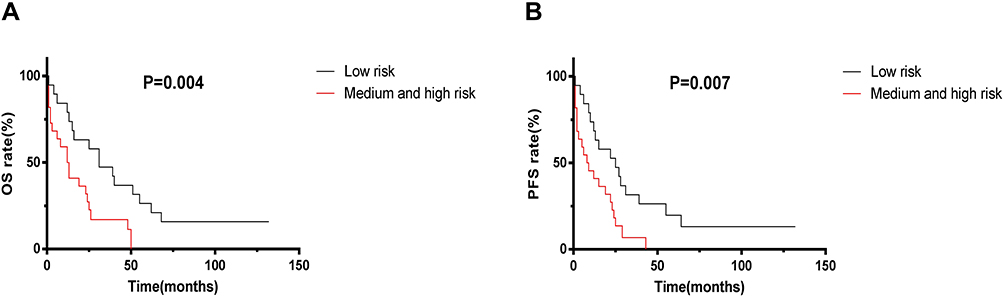 |
Figure 3 (A) The medium OS of patients with complex chromosome karyotype abnormality in MRP low risk group and medium-and-high risk group were 31 months and 12 months respectively. (B) The median PFS of patients with complex chromosome karyotype abnormality in MRP low risk group and medium-and-high risk group were 25 months and 8 months respectively. |
Prognostic Significance of Remission Depth in Different MRP Groups
The baseline characteristics of MRP patients in the low-risk group and medium-risk group, patients with VGPR and above after treatment, and patients without VGPR are shown in Tables 4 and 5, and no significant difference was found except Ca2+ in Table 4. After treatment, no significant difference was observed in the OS and PFS (P>0.05) in different remission degrees (VGPR and above or below VGPR) between the two groups (Figure 4A–D). In the MRP high-risk group, after treatment, the median OS and PFS of patients with VGPR and above were 44 months and 32 months, respectively, while those of patients with remission degree below VGPR were 12 months and 8 months, respectively. There were significant differences in the OS (P<0.0001) and PFS (P<0.0001) between the two groups with different remission degrees (Figure 4E and F), although the tumor cell ratio was higher in those with remission degree below VGPR (Table 6).
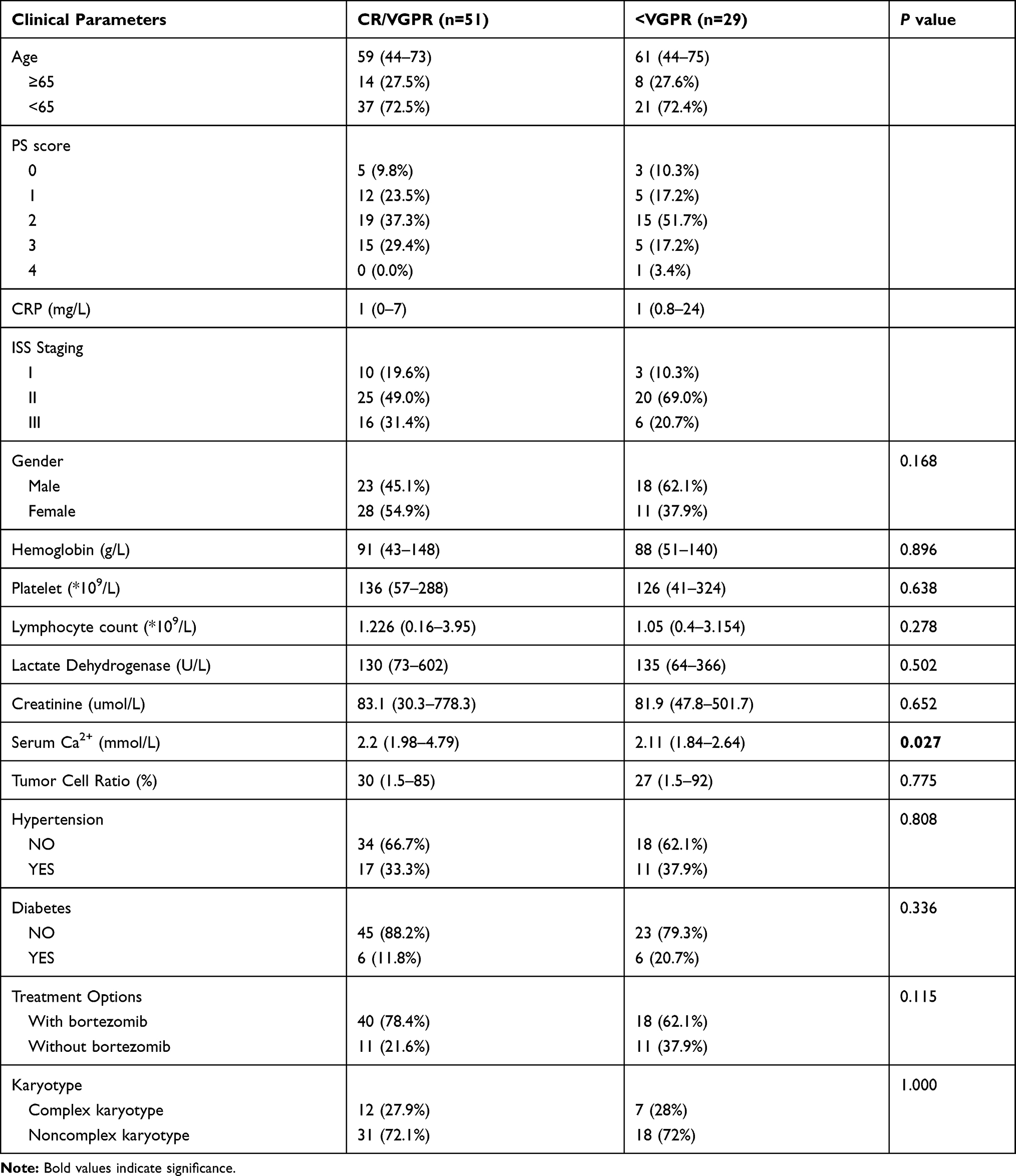 |
Table 4 Clinical Characteristics of Low-Risk Patients with Different Remission Depth |
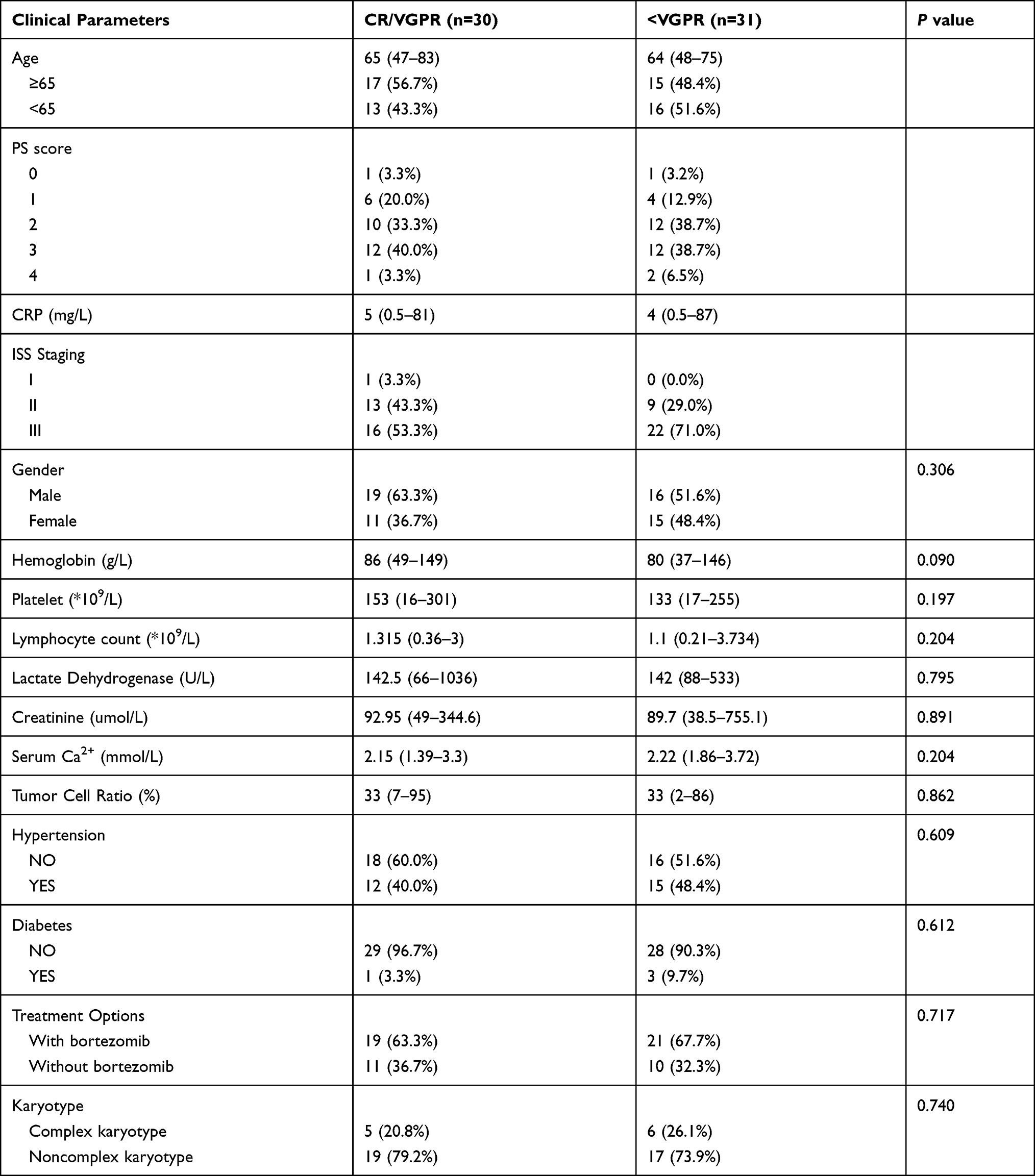 |
Table 5 Clinical Characteristics of Medium-Risk Patients with Different Remission Depth |
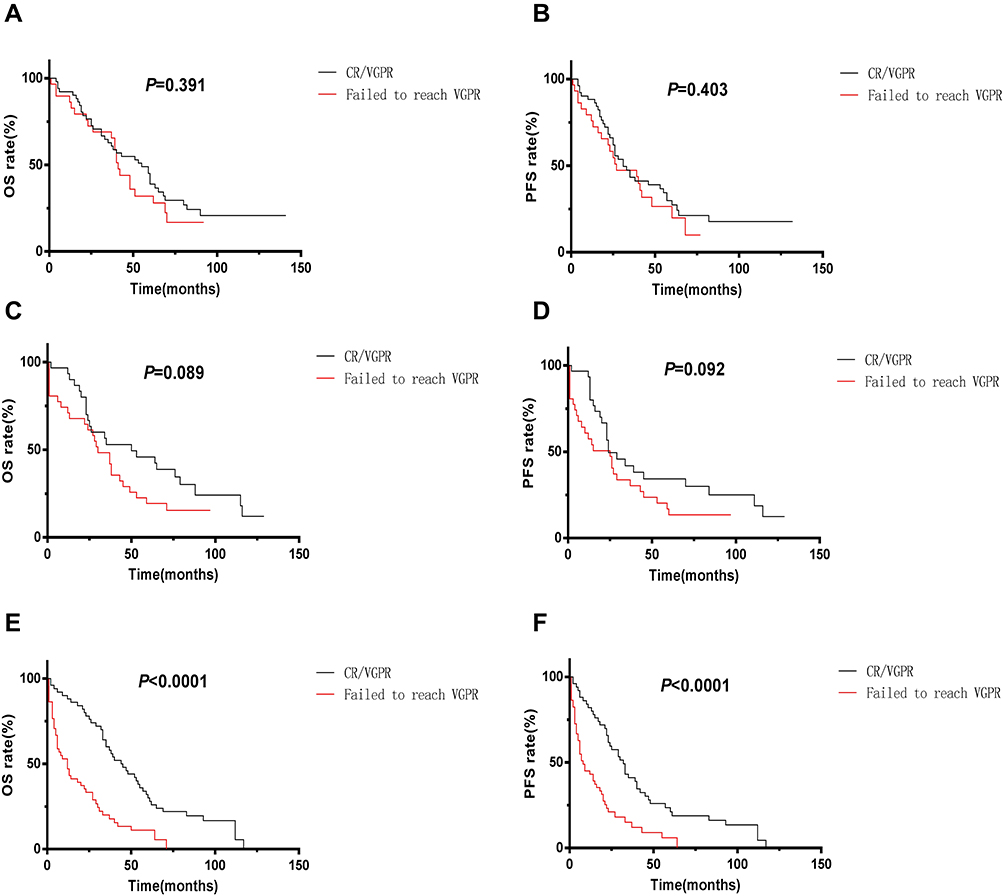 |
Figure 4 (A) The medium OS of MRP low-risk patients who reached CR/VGPR and failed to reach VGPR after treatment were 55 months and 41 months respectively. (B) The medium PFS of MRP low-risk patients who reached CR/VGPR and failed to reach VGPR after treatment were 31 months and 27 months respectively. (C) The medium OS of MRP medium-risk patients who reached CR/VGPR and failed to reach VGPR after treatment were 50 months and 30 months respectively. (D) The medium PFS of MRP medium-risk patients who reached CR/VGPR and failed to reach VGPR after treatment were 24 months and 25 months respectively.(E) The medium OS of MRP high-risk patients who reached CR/VGPR and failed to reach VGPR after treatment were 44 months and 12 months respectively. (F) The medium PFS of MRP high-risk patients who reached CR/VGPR and failed to reach VGPR after treatment were 32 months and 8 months respectively. |
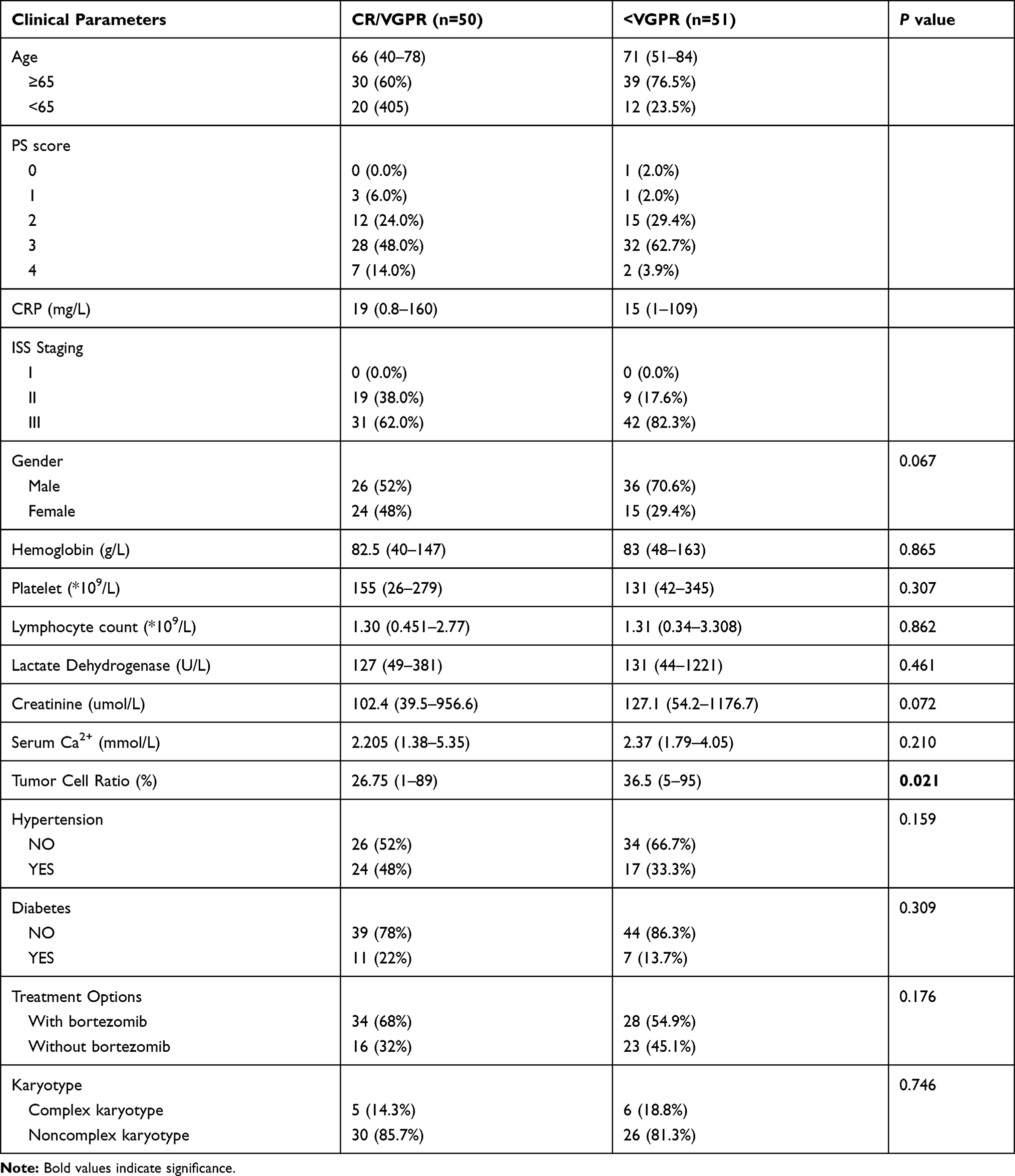 |
Table 6 Clinical Characteristics of High-Risk Patients with Different Remission Depth |
Discussion
MM remains an incurable disease. In recent years, many studies have focused on the risk assessment of MM. Based on host factors, the GA score proposed by IMWG in 2015 was an additive scoring system (range: 0–5) based on age, comorbidities, and cognitive and physical conditions and was developed to identify three groups: fit, intermediate fitness, and frail. It was used to predict mortality and the risk of toxicity in older myeloma patients.1 Compared with the IMWG scoring strategy, Murillo et al developed the Fried weakness scoring model, which excluded age and found that the Fried model was significantly associated with risk of death and a better predictor of survival.7 Facon et al have also put forward a different prognosis assessment model for MM; they used an ECOG PS-containing frailty scale as a predictive measure of clinical outcomes in patients with transplant-ineligible NDMM and documented that frail patients have worse PFS and OS compared with nonfrail patients.8 On the contrary, based on tumor factors, Kim et al and Liu et al successively put forward the MPI and IPSI risk assessment models, and confirmed their survival relevance with MM.9,10 The MPI comprised NLR, PLT, and CRP, while the IPSI consisted of RDW, NLR, and PLT. Both models played an important role in the prognosis of NDMM in the bortezomib-based chemotherapy era and identified that inflammatory factors affect the prognosis of MM.9,10 Of course, ISS and RISS are still more commonly used in the clinical setting. In 2019, the British Myeloma Research Alliance first proposed the prognosis evaluation model of MRP composed of physical fitness score, age, ISS stage, and CRP using the data from the NCRI Myeloma XI study [NCRI-XI, n=1852] and the MRC Myeloma IX study [MRC-IX, n=520]. They found that the median OS values of the low-risk, medium-risk, and high-risk MRP groups in the NCRI-XI and MRC IX studies were 60, 44, and 25 months and 49, 34, and 20 months respectively; meanwhile, their median PFS values were 20, 17, 12, months and 15, 13, and 9 months, respectively. These results indicated that MRP could predict early mortality and had a good prognostic value in older MM patients who are not suitable for transplantation.4 They found that MRP has a prognostic value in patients with different treatment schemes and in those with high-risk genetic abnormalities defined base on the MRP criteria,4 which may indirectly reflect that MRP had better prognostic value than RISS.
However, few studies have verified whether MRP can be implemented in the real-world setting. Redder et al made a retrospective analysis and found that the median OS of the low-risk MRP group was 55 months, while those of the high-risk and median-risk groups were 13.9 months and 35.9 months, respectively. The PFS in the high-risk group showed a hazard ratio of 2.06, while that in the medium-risk group showed a hazard ratio of 1.39. Therefore, they showed consistent results in terms of the prognostic value of MRP score; that is, the high-risk group had a higher risk of early death and a shorter PFS.6 They also found that the high-risk group had much higher Cr, lower Hb, and higher LDH levels, which differed from the results of our study.6 In addition, patients in the high-risk group had shorter treatment durations and worse treatment responses.6
In China, in addition to patients who were not suitable for transplantation after undergoing a medical evaluation, some patients were unable to undergo transplantation due to personal factors (fear of transplantation, inability to understand and recognize this method because of low literacy levels, etc.) and objective conditions (such as economic constraints, and lack of care and support from their families) in the real world. Whether MRP is applicable to the above non-transplant patients remains unclear. This study retrospectively analyzed 242 newly diagnosed non-transplanted MM patients in China and found that MRP, as a simple prognostic evaluation model, was also suitable for this patient group. Similar to the studies mentioned above, significant differences were found in the OS and PFS among the different MRP risk groups. MM patients who used the treatment regimen containing bortezomib can still carry out prognosis stratification using the MRP.
Significant differences were observed between this study and other foreign studies. First, the patients enrolled in this study were slightly different from those included in the study conducted in Britain and Denmark, but both were objectively evaluated as unsuitable for transplantation. However, this study included some non-transplant patients who preferred not to undergo this procedure or due to objective conditions. There are many such patients in China and other developing countries, and including them in this study may better reflect the actual real-world setting. Second, Redder et al found significant differences in the degree of remission among different MRP groups,6 but no differences were found in this study either in general or in different subgroups. In our opinion, this may be related to the differences in treatment schemes. According to Redder et al, there were significant differences in the treatment schemes among different MRP groups,6 which may lead to bias in the degree of remission. By contrast, no MRP difference was noted between the different MRP groups in this study, and they showed relatively consistent results, which may reflect the prognosis of MRP patients more accurately. Of course, this difference may also exist due to racial differences, which requires further verification using a large sample size. Third, some studies found that patients with MM had a better prognosis if they achieved better remission after treatment.11,12 In this study, among 242 MM patients, the OS and PFS of those with VGPR and above were longer (VGPR and above vs. less than VGPR patients’ OS: 50 months vs. 27 months; PFS: 31 months vs. 16 months, P<0.05). Similarly, the patients in the high-risk group who had a treatment response above VGPR based on the MRP score showed similar prognosis; moreover, the depth of remission still showed prognostic significance in the high-risk MRP group. However, the remission depth of patients in the MRP low-risk group and middle-risk group did not show a correlation with survival time, which indicated that the remission depth has no prognostic significance in the low-risk and middle-risk groups based on the MRP score. Fourth, the high-risk genetic abnormalities defined by IMWG et al will seriously affect the prognosis of MM.13,14 The prognosis of MM patients with complex karyotypes was also extremely poor.15 Studies in the UK and Denmark have analyzed the prognosis of MM patients with high-risk genetic abnormalities, but no studies have reported the prognosis of MRP in patients with complex karyotypes. Our study found that in the complex karyotype subgroup with poor prognosis, the MRP model can be used to further stratify the prognosis of MM patients in this subgroup, which proves that the MRP model has the ability to evaluate the prognosis of MM patients based on the biological factors and has nothing to do with tumor invasiveness. Fifth, even though both MRP and ISS can be used to stratify patients into three groups, the MRP comprises host factors such as age, WHO PS score, and tumor factors such as ISS and CRP, that can be utilized as a more comprehensive prognostic assessment tool. In addition, ISS was first proposed in 2003 and had a limited prognostic value in MM patients in the era of new drugs based on recent researches.2 Similar with our previous published data, 16 ISS did not show significant prognostic value in these patients treated with bortezomib, while MRP still had a prognostic significance, which makes it necessary to study a new and simple scoring system such as MRP in the era of new drugs.
However, this study has some limitations. The number of clinical cases used in this study was relatively small, and this study was retrospective in nature, which could lead to bias. By contrast, due to economic constraints, some patients did not previously undergo complete cytogenetic examination; hence, only those patients with complete information underwent MRP analysis to determine the complex karyotype subsets. Third, due to the limited conditions, only the IMWG efficacy standard in 2016 can be used to judge the remission degree in the study population, but a more comprehensive MRD analysis to evaluate the MRP score cannot be carried out.
Conclusion
In summary, the prognostic value of MRP score in 242 newly diagnosed non-transplanted MM patients in China has been preliminarily verified, which can provide prognostic information for newly diagnosed MM patients treated with proteasome inhibitors. In addition, tumor biological factors, including genetic abnormalities or complex chromosome karyotypes, did not affect the prognostic stratification significance of the MRP model based on host biological factors. After treatment, the depth of remission still showed prognostic value in the high-risk MRP group. Importantly, CRP, physical fitness score, age, and ISS staging (including β 2-microglobulin and albumin) are routine hematological and biochemical indexes, which are easy to obtain and have low economic burden. Moreover, the prognostic assessment model is simple and easy to operate; therefore, the model can be applied in the different levels of the health care system.
Acknowledgments
The authors would like to thank Mrs Yudi Qiu for assistance with language help.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Palumbo A, Bringhen S, Mateos MV, et al. Geriatric assessment predicts survival and toxicities in elderly myeloma patients: an International Myeloma Working Group report. Blood. 2015;125(13):2068–2074. doi:10.1182/blood-2014-12-615187
2. Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised international staging system for multiple myeloma: a report from International Myeloma Working Group. J Clin Oncol. 2015;33(26):2863–2869. doi:10.1200/JCO.2015.61.2267
3. Mikhael JR, Dingli D, Roy V, et al. Management of newly diagnosed symptomatic multiple myeloma: updated Mayo Stratification of Myeloma and Risk-Adapted Therapy (mSMART) consensus guidelines 2013. Mayo Clin Proc. 2013;88(4):360–376. doi:10.1016/j.mayocp.2013.01.019
4. Cook G, Royle K-L, Pawlyn C, et al. A clinical prediction model for outcome and therapy delivery in transplant-ineligible patients with myeloma (UK myeloma research alliance risk profile): a development and validation study. Lancet Haematol. 2019;6(3):e154–e166. doi:10.1016/S2352-3026(18)30220-5
5. Kumar S, Paiva B, Anderson KC, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016;17(8):e328–e346. doi:10.1016/S1470-2045(16)30206-6
6. Redder L, Klausen TW, Vangsted AJ, et al. Validation of the UK myeloma research alliance risk profile, a new clinical prediction model for outcome in patients with newly diagnosed multiple myeloma not eligible for autologous stem cell transplantation; a population-based study from the Danish national multiple myeloma registry. Br J Haematol. 2020. doi:10.1111/bjh.16806
7. Murillo A, Cronin AM, Laubach JP, et al. Performance of the International Myeloma Working Group myeloma frailty score among patients 75 and older. J Geriatr Oncol. 2019;10(3):486–489. doi:10.1016/j.jgo.2018.10.010
8. Facon T, Dimopoulos MA, Meuleman N, et al. A simplified frailty scale predicts outcomes in transplant-ineligible patients with newly diagnosed multiple myeloma treated in the FIRST (MM-020) trial. Leukemia. 2020;34(1):224–233. doi:10.1038/s41375-019-0539-0
9. Kim DS, Yu ES, Kang K-W, et al. Myeloma prognostic index at diagnosis might be a prognostic marker in patients newly diagnosed with multiple myeloma. Korean J Intern Med. 2017;32(4):711–721. doi:10.3904/kjim.2016.054
10. Liu S, Shi J, Guo H, et al. Prognostic significance of the inflammatory index-based scoring system in patients preliminarily diagnosed with multiple myeloma in the bortezomib-based chemotherapy era. Cancer Manag Res. 2019;11:9409–9420. doi:10.2147/CMAR.S227671
11. Lahuerta JJ, Paiva B, Vidriales MB, et al. Depth of response in multiple myeloma: a pooled analysis of three PETHEMA/GEM clinical trials. J Clin Oncol. 2017;35(25):2900–2910. doi:10.1200/JCO.2016.69.2517
12. Yan Y, Mao X, Liu J, et al. The impact of response kinetics for multiple myeloma in the era of novel agents. Blood Adv. 2019;3(19):2895–2904. doi:10.1182/bloodadvances.2019000432
13. Boyd KD, Ross FM, Chiecchio L, et al. A novel prognostic model in myeloma based on co-segregating adverse FISH lesions and the ISS: analysis of patients treated in the MRC myeloma IX trial. Leukemia. 2012;26(2):349–355. doi:10.1038/leu.2011.204
14. Chng WJ, Dispenzieri A, Chim CS, et al. IMWG consensus on risk stratification in multiple myeloma. Leukemia. 2014;28(2):269–277. doi:10.1038/leu.2013.247
15. Aoki G, Sawazaki A, Notsumata K, et al. Ultra high-risk refractory multiple myeloma with a complex karyotype including t(14;19). Rinsho Ketsueki. 2020;61(3):240–244. doi:10.11406/rinketsu.61.240
16. Wang H, Zhou X, Zhu J-W, et al. Association of CD117 and HLA-DR expression with shorter overall survival and/or progression-free survival in patients with multiple myeloma treated with bortezomib and thalidomide combination treatment without transplantation. Oncol Lett. 2018;16(5):5655–5666. doi:10.3892/ol.2018.9365
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.