Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Evaluation of the Long-Term Cost-Effectiveness of the Dexcom G6 Continuous Glucose Monitor versus Self-Monitoring of Blood Glucose in People with Type 1 Diabetes in Canada
Authors Roze S, Isitt JJ, Smith-Palmer J ![]() , Lynch P
, Lynch P
Received 27 May 2021
Accepted for publication 28 July 2021
Published 11 August 2021 Volume 2021:13 Pages 717—725
DOI https://doi.org/10.2147/CEOR.S304395
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dean Smith
Stephane Roze,1 John J Isitt,1 Jayne Smith-Palmer,2 Peter Lynch3
1Vyoo Agency, Paris, France; 2Ossian Health Economics and Communications, Basel, Switzerland; 3Dexcom, San Diego, CA, USA
Correspondence: Jayne Smith-Palmer
Ossian Health Economics and Communications GmbH, Bäumleingasse 20, Basel, 4051, Switzerland
Tel +41 61 271 6214
Email [email protected]
Background: The Dexcom G6 real-time continuous glucose monitoring (RT-CGM) system is one of the most sophisticated RT-CGM systems developed to date and became available in Canada in 2019. A health economic analysis was performed to determine the long-term cost-effectiveness of the Dexcom G6 RT-CGM system versus SMBG in adults with type 1 diabetes (T1D) in Canada.
Methods: The analysis was performed using the IQVIA Core Diabetes Model. Based on clinical trial data, patients with mean baseline HbA1c of 8.6% were assumed to have a HbA1c reduction of 1.0% with RT-CGM versus 0.4% reduction with SMBG. RT-CGM was also associated with a quality of life (QoL) benefit owing to reduced incidence of hypoglycemia, reduced fear of hypoglycemia (FoH) and elimination of fingerstick testing. Direct medical costs were sourced from published literature, and inflated to 2019 Canadian dollars (CAD).
Results: Dexcom G6 RT-CGM was projected to improve mean quality-adjusted life expectancy by 2.09 quality-adjusted life years (QALYs) relative to SMBG (15.52 versus 13.43 QALYs) but mean total lifetime cots were CAD 35,353 higher with RT-CGM (CAD 227,357 versus CAD 192,004) resulting in an incremental cost-effectiveness ratio (ICER) of CAD 16,931 per QALY gained. Sensitivity analyses revealed that assumptions relating to the QoL benefit associated with reduced FoH and the elimination of fingerstick testing with RT-CGM as well as SMBG usage and change in HbA1c were the key drivers of cost-effectiveness.
Conclusion: For adults with T1D in Canada, RT-CGM is associated with improved glycemic control and QoL benefits owing to a reduced FoH and elimination of the requirement for fingerstick testing and over a lifetime time horizon is cost-effective relative to SMBG.
Keywords: type 1 diabetes, Canada, real-time continuous glucose monitoring, cost-effectiveness
Introduction
Real-time continuous glucose monitoring (RT-CGM) devices typically take a reading of glucose levels within the interstitial fluid once every 5 minutes providing the user with a level of detail relating to glucose levels and changes in glucose levels over time that cannot be achieved using self-monitoring of blood glucose. Moreover, RT-CGM devices are able to alert users if their blood glucose levels fall, or are predicted to fall to dangerous levels, allowing the user to take action to prevent hypoglycemia. There is also a strong evidence base from clinical trials showing that for people with type 1 diabetes (T1D) RT-CGM can improve glycemic control, reduce the incidence of hypoglycemic events, improve quality of life (QoL) and reduce the frequency of hospital admissions compared with SMBG.1,2
In Canada, 2018 guidelines issued by Diabetes Canada endorsed the use of RT-CGM in particular groups of people with T1D including those with recurrent or severe hypoglycemia or unawareness of hypoglycemia and those not achieving target HbA1c levels, contingent on a willingness to wear the sensor on an almost daily basis. RT-CGM may also be used in adults achieving HbA1c targets to maintain HbA1c levels without increasing hypoglycemia and Diabetes Canada guidelines also endorse the use of RT-CGM in combination with continuous subcutaneous insulin infusion (CSII) to improve quality of life (QoL) or treatment satisfaction.3–5 Despite this guidance covering a wide range of indications for RT-CGM, the reimbursement of this technology by public payers in Canada is very limited across all provinces.6 Focus groups and interviews conducted in adults with T1D as well as the parents of children with T1D in Ontario revealed that many considered RT-CGM to be an invaluable asset for disease management with parents in particular frequently expressing the view that RT-CGM restored a degree of normalcy and freedom for their children.7 However, cost was often cited as a barrier to widespread uptake, with RT-CGM being funded as an out-of-pocket expense for many of those interviewed. Indeed, on a national level, annual out-of-pocket costs for all people with T1D, which may include costs such as SMBG strips beyond the limit of what is reimbursed, as well as devices such as RT-CGM or continuous subcutaneous insulin infusion (CSII) exceed CAD 280 million.8 As the acquisition cost of RT-CGM presents a barrier to access in many instances, there is a need for robust long-term cost-effectiveness analyses to determine whether, over the lifetime of the patients, the initial acquisition costs of RT-CGM are offset by the long-term clinical benefits conferred by RT-CGM including improved glycemic control and reduced incidence of hypoglycemic events.
The Dexcom G6 RT-CGM system was launched in Canada in 2019.9 This system has multiple improvements and additional features relative to earlier generations, all of which may contribute to improved efficacy, usability and cost-effectiveness relative to previous generations. These include improved sensor lifetime (sensor lifetime of 10 days versus 7 days with previous generation devices) factory calibration, which eliminates the need for twice-daily calibration with fingerstick testing and an Urgent Low Soon Alert, which alerts the user if their blood glucose levels are predicted to drop below 55 mg/dL (3.056 mmol/L) within the next 20 minutes, allowing them to take action to avoid a hypoglycemic event. The G6 RT-CGM system also allows for remote monitoring, which may be particularly useful for the parents of children or adolescents with T1D as well as adults with T1D who live alone. Further, real-world data have shown that the use of the Dexcom G6 RT-CGM system is associated with incremental improvements in terms of reducing the proportion of time spent in hypoglycemia and increasing the proportion of time spent in the euglycemic range.10
Previously, the DIAMOND trial in adults with T1D compared RT-CGM (using the older Dexcom G4 platinum system) with SMBG and demonstrated that RT-CGM was associated with statistically significant improvements in glycemic control, diabetes distress, fear of hypoglycemia and hypoglycemic confidence relative to SMBG.11,12 In light of the these clinical and QoL benefits and the recent introduction of the Dexcom G6 RT-CGM system to Canada, a long-term cost-effectiveness analysis was performed to investigate the cost-effectiveness of this system compared with SMBG in adults with T1D in Canada.
Methods
Model Structure
The analysis was performed using the IQVIA CORE Diabetes Model (CDM, version 9.0 E360). The CDM is a published and validated computer simulation model that can be used to project long-term clinical and economic outcomes for either type 1 or type 2 diabetes and the architecture and validation of the model has been previously described in detail in publications by Palmer et al 13,14 and McEwan et al.15 Outputs provided by the CDM include life expectancy, quality-adjusted life expectancy, cumulative incidence of long-term complications including cardiovascular, cerebrovascular, renal, ophthalmic and diabetic foot complications, mean time to onset of complications, direct and indirect costs and the incremental cost-effectiveness ratio (ICER).
Simulation Cohort Characteristics and Treatment Effects
Clinical input data including baseline cohort characteristics and treatment effects were sourced from the DIAMOND trial in adults with T1D11 (supplemented where necessary with data from other trials in people with T1D (Table 1)). The DIAMOND trial was a randomized controlled trial conducted across multiple sites in North America, in which a total of 158 adults aged ≥25 years with T1D and treated with multiple daily injections of insulin for at least 1 year previously were randomly allocated (in a 2:1 ratio) to either RT-CGM (using the Dexcom G4 platinum system) or usual care with SMBG. The mean baseline HbA1c in both treatment arms of the simulated cohort was assumed to be 8.6% (70 mmol/mol). A treatment effect in terms of reduction in HbA1c of 1.0% (10 mmol/mol) was applied to the arm using the Dexcom G6 RT-CGM system and a reduction of 0.4% (4 mmol/mol) was applied to the SMBG arm, based on findings of the DIAMOND trial. Hypoglycemic event rates were also sourced from the DIAMOND trial; the rate of severe hypoglycemic events (SHEs; defined as an event requiring medical assistance) was 4.2 per 100 person-years in the RT-CGM arm and 12.2 per 100 person-years in the SMBG arm.11 Similarly, the rate of non-severe hypoglycemic events was 5840 per 100 person-years for RT-CGM and 10,950 per 100 person-years for the SMBG arm.16
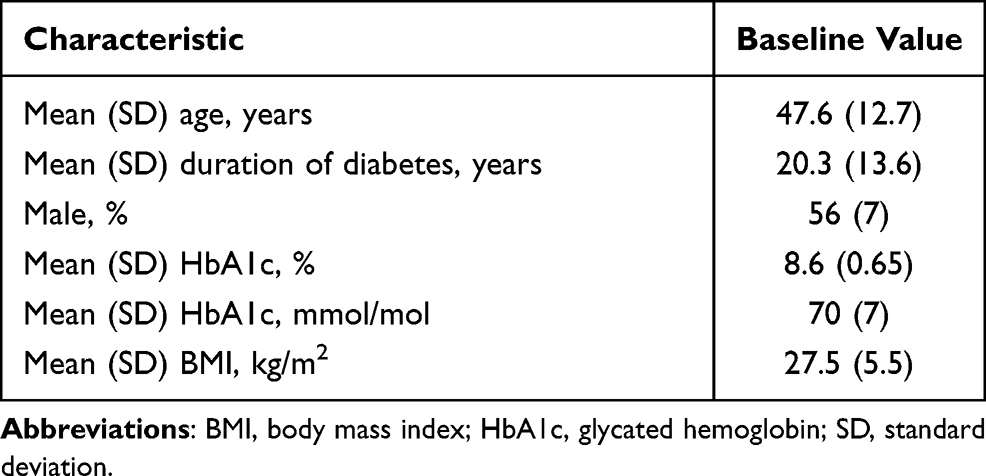 |
Table 1 Baseline Cohort Characteristics |
All clinical input data utilized has been previously published and is freely available. As no new patient data were collected, institutional review board approval was not required for the present analysis.
Costs and Health State Utilities
A utility benefit was applied to the RT-CGM arm owing to the combined benefits to QoL associated with a reduced fear of hypoglycemia (FoH) and avoidance of fingerstick testing with the Dexcom G6 RT-CGM system. In the DIAMOND trial FoH was measured using the worry subscale of the Hypoglycemia Fear Survey. The mean difference in FoH score between the treatment arms was 3.17 units, with patients in the RT-CGM having less FoH. This benefit was converted to a utility benefit of 0.02536 based on a previously published mapping to the EQ-5D by Currie et al.17 Similarly, a 0.03 utility benefit was also applied owing to the avoidance of fingerstick testing, based on the findings of a study comparing flash glucose monitoring with SMBG as this method of glucose monitoring also reduces or negates the requirement for fingerstick testing.18 This resulted in a total utility benefit of 0.05536 applied to the arm using the Dexcom G6 RT-CGM system (0.03 + 0.02536).
For patients with no complications, a utility value of 0.90 was assumed, based on findings of the DIAMOND trial.12 Disutilities associated with long-term diabetes-related complications and hypoglycemic events were sourced from the literature (Table 2).19,20
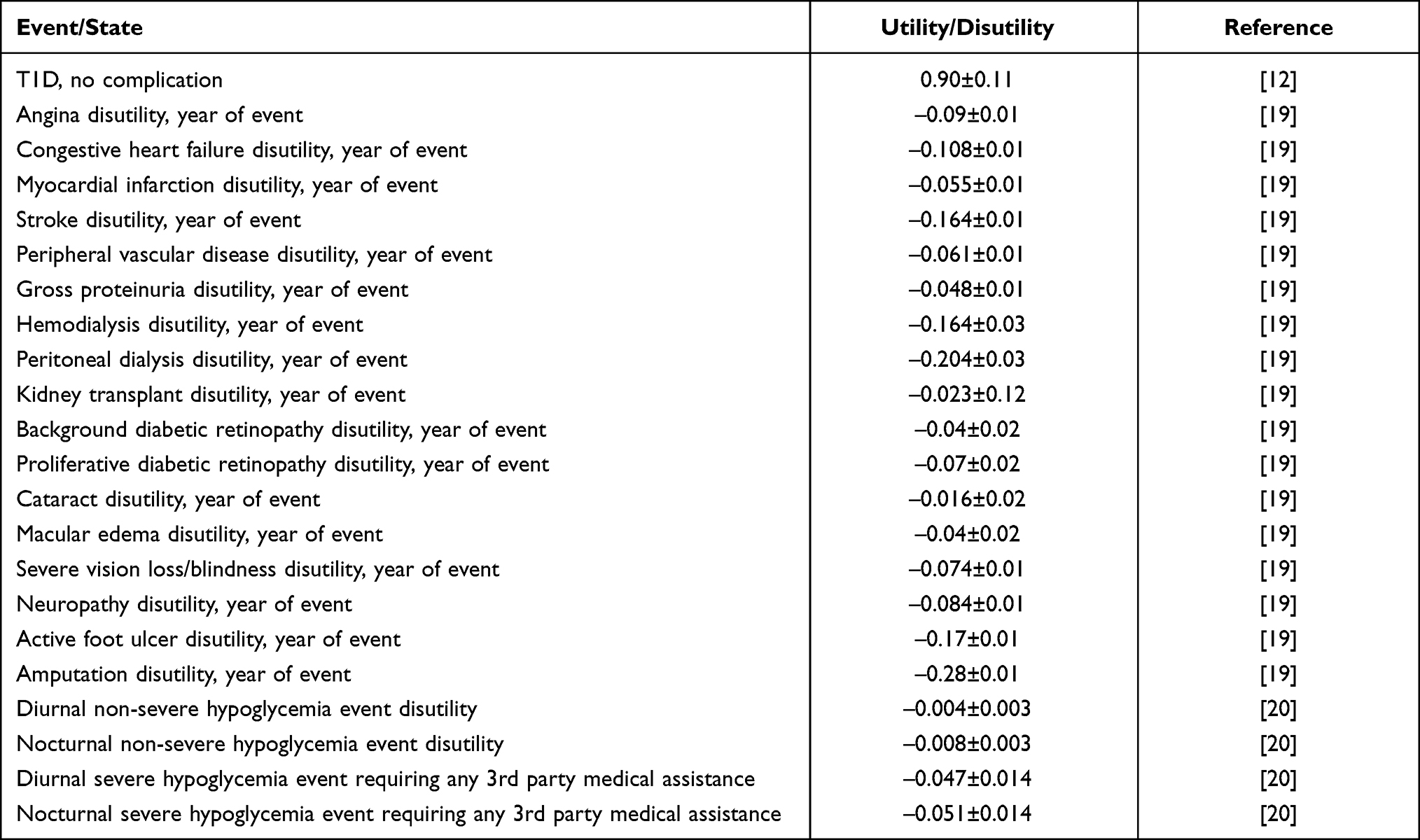 |
Table 2 Utilities and Diabetes Complication Disutility Values |
The annual cost associated with the sensors and transmitters associated with the Dexcom G6 RT-CGM system was CAD 3588, which included a total of 36 sensors per year (based on a sensor lifetime of 10 days each) and four transmitters per year. Annual costs in the SMBG arm were CAD 1226, which assumed a mean of 4.6 SMBG tests per day, based on findings from the DIAMOND trial.11 Direct costs associated with the treatment and management of diabetes-related complications were sourced from the literature, and where necessary inflated to 2019 CAD (Supplementary Table 1).21–23
Sensitivity Analyses
A series of one-way sensitivity analyses were performed to determine key parameters that influenced cost-effectiveness. Firstly, the influence of treatment effect was examined in analyses in which HbA1c change in the RT-CGM was increased and decreased by 30%. Similarly, the influence of the reduction in both severe and non-severe hypoglycemic events was assessed in analyses in which the rate of severe or non-severe hypoglycemic events in the RT-CGM arm was increased or decreased by 50%. The influence of the utility benefit associated with the combined effect of reduced FoH and lack of fingerstick testing was explored by either increasing or decreasing this utility benefit in the RT-CGM by 50%, and by reducing the utility benefit to 0. A series of sensitivity analyses were also performed around daily SMBG use in the SMBG arm; in the base case, it was assumed that patients performed a mean of 4.6 tests per day, sensitivity analyses were performed in which this was decreased to 4.0 tests per day or increased to 5.2 or 10 tests per day. Finally, sensitivity analyses were performed around the utility value for the T1D with no complications state (utilizing a value of 0.672, sourced from the Sheffield Type 1 Diabetes Policy Model24) and also around the time horizon of the analysis.
Perspective, Time Horizon and Discount Rate
The analysis was performed from the public payer perspective. The time horizon used was that of patient lifetimes (50 years) and both future costs and clinical outcomes were discounted at a rate of 1.5% per annum in line with guidance from the Canadian Agency for Drugs and Technologies in Health.25
Results
In the base case analysis, the use of the Dexcom G6 RT-CGM system was associated with a mean gain in quality-adjusted life expectancy of 2.09 quality-adjusted life years (QALYs) compared with SMBG (15.52 QALYs for RT-CGM versus 13.429 QALYs for SMBG) (Table 3). Mean direct lifetime costs were CAD 35,353 higher with RT-CGM than SMBG, resulting in an ICER of CAD 16,931 per QALY gained and at a willingness-to-pay (WTP) threshold of CAD 50,000 per QALY gained the likelihood of the Dexcom G6 RT-CGM system being considered cost-effective relative to SMBG was 99.7% (Figure 1). The higher overall lifetime costs in the RT-CGM arm were driven by the higher treatment costs associated with the device (CAD 87,153 versus CAD 29,416; difference CAD 57,737). However, the higher cost associated with the use of the Dexcom G6 RT-CGM system was partially offset by reduced costs associated with a reduced incidence of long-term complications owing to improved HbA1c with RT-CGM as well as a lower incidence of severe hypoglycemic events (Table 3). The mean time to onset of complications was also delayed owing to the improved glycemic control in the RT-CGM arm. The use of RT-CGM delayed the mean time to onset of any long-term complication by 0.34 years relative to SMBG and the mean time to onset of several complications including proliferative retinopathy, microalbuminuria, neuropathy and macula edema were delayed by more than 2 years.
 |
Table 3 Summary Results of Base Case Analysis |
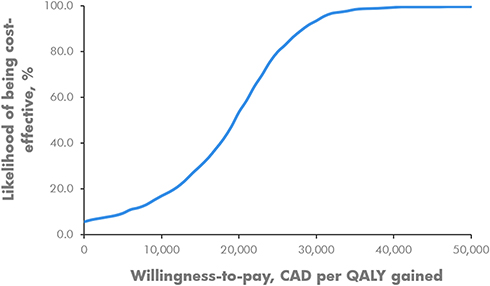 |
Figure 1 Cost-effectiveness acceptability curve in the overall T1D population (based on DIAMOND trial patient population) acceptability curve based on second-order Monte Carlo simulation based on 1000 iterations each based on a cohort of 1000 simulated patients. Abbreviations: CAD, Canadian dollars; QALY, quality-adjusted life year. |
The results of one-way sensitivity analyses revealed that the cost-effectiveness of RT-CGM was most sensitive to changes in assumptions around the QoL benefit associated with reduced FoH and avoidance of fingerstick testing (Table 4). In a sensitivity analysis in which the combined utility benefit associated with reduced FoH and avoidance was halved to +0.02768 the ICER increased to CAD 24,974 per QALY gained. Similarly, if this utility benefit was increased by 50% relative to the base case to +0.08304 the ICER decreased to CAD 12,808 per QALY gained.
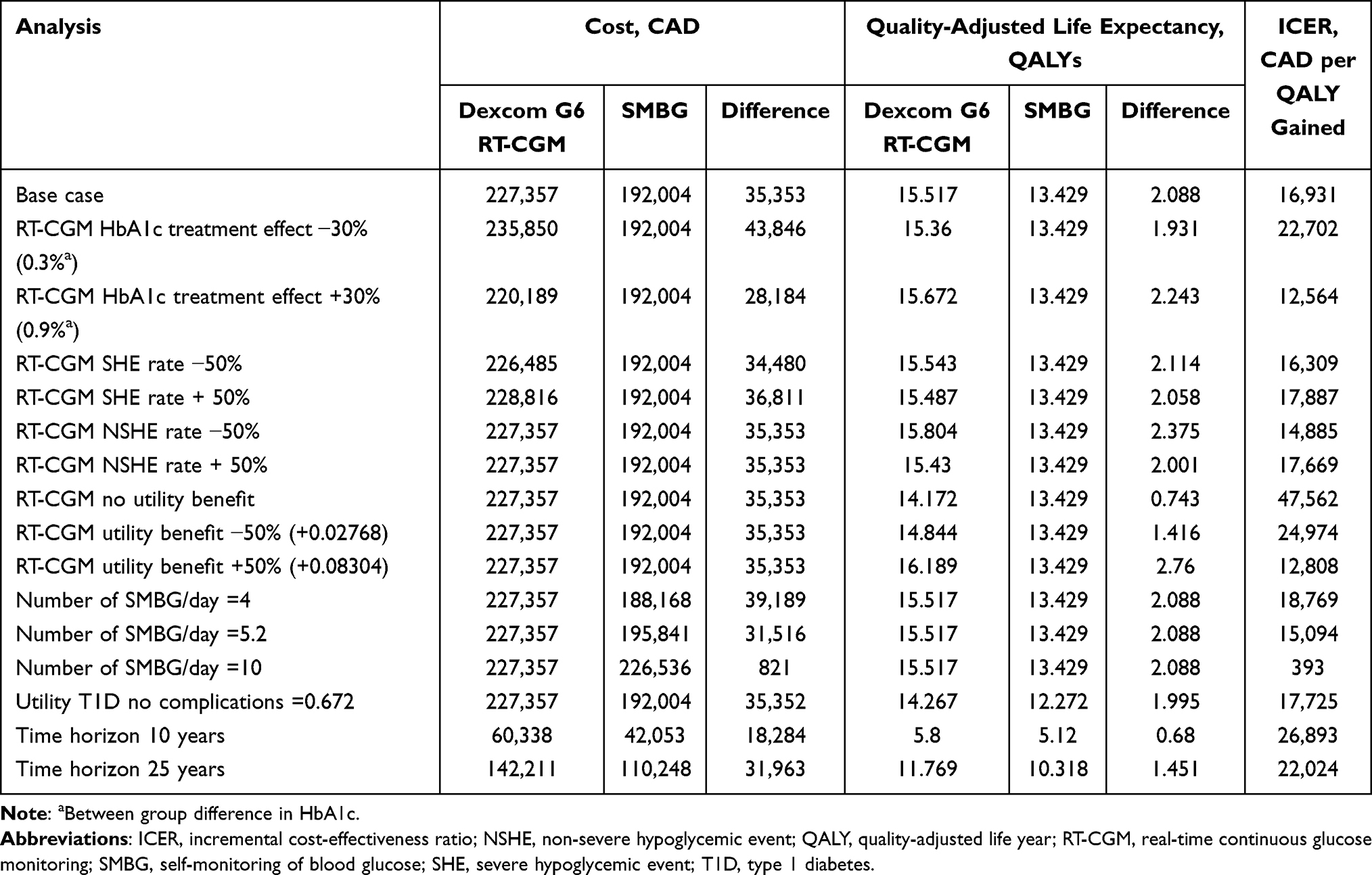 |
Table 4 Summary Findings of Sensitivity Analyses |
The ICER was also relatively sensitive to assumptions around the frequency of SMBG testing in the SMBG arm. In the base case analysis, based on DIAMOND trial data, a mean of 4.6 tests per day in the SMBG arm was assumed. This is in line with Canadian guidelines, which recommend a minimum of three tests per day for people with T1D5 as well as in particular situations such as prior to driving.26 It also closely concurs with the findings from the T1D exchange registry where the mean number of SMBG tests per day performed among people aged 25–<50 years was 5.2, but that 8% of patients in this age group were performing more than 10 tests per day27 Accordingly, in a sensitivity analysis in which the frequency of testing in the SMBG arm was increased to ten per day, the ICER decreased to CAD 393 per QALY gained. However, it should be noted that this sensitivity analysis did not capture any potential effect of the higher SMBG frequency leading to improved HbA1c.
The cost-effectiveness of the Dexcom G6 RT-CGM system was also relatively sensitive to changes in assumptions around the treatment effect in terms of HbA1c reduction (Table 4).
Discussion
Overall, findings from long-term health economic analyses suggest that for adults with long-standing T1D based in Canada, the use of the Dexcom G6 RT-CGM system represents a cost-effective management option compared with SMBG. In the base case analysis, the ICER was CAD 16,931 per QALY gained, suggesting that at a WTP threshold of CAD 50,000 per QALY gained the Dexcom G6 RT-CGM system is likely to represent good value for money relative to SMBG. Moreover, it should be noted that the analysis was performed from the public payer perspective and therefore does not capture any potential reduction in lost productivity owing to the lower incidence of complications such as hypoglycemic events with RT-CGM. In the Canadian Hypoglycemia Assessment Tool Program, for people with T1D, mean annual indirect costs associated with hypoglycemic events requiring hospitalization or additional outpatient visits were estimated at CAD 771 per patient.28 Further, even though many non-severe hypoglycemic events can be quickly resolved some may be associated with productivity losses and in Canada, even non-severe events have been reported with mean of 3.5 hours of lost work time.29 This suggests that if indirect costs are also considered the cost-effectiveness of the Dexcom G6 RT-CGM system versus SMBG is likely to be increased further.
The results of one-way sensitivity analyses indicated that the cost-effectiveness of the Dexcom G6 RT-CGM system is sensitive to changes in assumptions around the QoL benefits conferred by reduced FoH as well as the treatment effect in terms of change in HbA1c, assumptions around SMBG usage and time horizon. In particular, increasing the magnitude of treatment effect was associated with improved cost-effectiveness and subgroup analyses from the DIAMOND trial have shown that the effect in terms of HbA1c reduction is greatest with those with higher HbA1c values at baseline.30 FoH, to varying degrees, is common in people with T1D, particularly those with a history of frequent and/or severe hypoglycemic events or those with impaired awareness of hypoglycemia.31 Moreover, FoH can influence many aspects of daily life as it has been reported to represent a barrier to physical activity, particularly in young adults31 as well as influencing aspects of disease management, with some patients adjusting insulin doses and maintaining blood glucose levels above targets to avoid hypoglycemia.32 FoH specifically in people with T1D based in Canada was recently investigated in the Canadian Hypoglycemia Assessment Tool program.33 The degree of FoH was determined on a scale of 0–10 where 0 represented “not afraid” and 10 represented “absolutely terrified”. The mean FoH among adults was 5.1, and although 18% of respondents had a score ranging from 0 to 2, 22% of respondents had a FoH score of ≥8, indicating that FoH is a major concern for over one-fifth of adults with T1D based in Canada.33 Taken together, these findings suggest that people with high baseline levels of FoH may therefore derive substantial clinical and QoL benefits from the security and alert features provided by the Dexcom G6 RT-CGM system.
Although the current analysis was limited to adults with T1D, FoH has been shown to be particularly pronounced at night and for parents/caregivers of children with T1D.7,31 In qualitative interviews conducted in patients and parents/caregivers in Ontario, parents often reported that nocturnal hypoglycemia was one of the gravest concerns with regard to their child’s diabetes management and many highlighted the alarm features of RT-CGM devices as a key factor in reducing anxiety.7 Additionally, several parents/caregivers with previous experience of RT-CGM, as well as adult patients who lived alone, cited an unlicensed open-source app (Nightscout34) as also being a major contributor to reduced fear and anxiety. This app allowed remote monitoring of glucose levels by parents who also noted that this feature allowed a greater degree of normalcy and independence for their child, whilst simultaneously allowing strict control of glucose levels.7 The functionality for remote monitoring is a feature that is inbuilt within the Dexcom G6 RT-CGM system, as such it is feasible that the additional features of this system (ie remote monitoring and Urgent Low Soon alert) may alleviate FoH to a greater extent than that observed in the DIAMOND trial, which utilized an earlier generation device.
Two previous analyses have examined the long-term cost-effectiveness of different RT-CGM devices in Canada. In the first of these Health Quality Ontario examined the overall cost-effectiveness of RT-CGM devices as a class and reported an ICER of over CAD 950,000 per QALY gained versus SMBG.7 However, it should be noted that there are several methodologic differences between the analysis performed by Health Quality Ontario and the analysis presented here; these include differences in model structure, patient cohort characteristics, differences in treatment effects in terms of the incidence rate and disutility associated with SHEs. In particular, the model utilized in the analysis by Health Quality Ontario did not capture key cardiovascular or cerebrovascular complications such as myocardial infarction and stroke, and the severity of several complications was also not considered. Additionally, the analysis by Health Quality Ontario did not capture any QoL benefit associated with reduced FoH.7 This patient-related benefit was however acknowledged, with the authors acknowledging that RT-CGM conferred clinical, safety, social and emotional benefits and recommending RT-CGM be reimbursed for people with T1D with severe hypoglycemia despite optimized treatment and those unable to recognize the symptoms of hypoglycemia.7 In the second analysis, Chaugule and Graham examined the cost-effectiveness of the Dexcom G5 RT-CGM system versus SMBG, also utilizing clinical input data from the DIAMOND trial and reporting an ICER of CAD 33,789 per QALY gained.35 The analysis presented here builds on that presented by Chaugule and Graham as it captures the incremental benefits associated with Dexcom G6 RT-CGM system, specifically, the longer sensor lifetime (10 days versus 7 days for previous generation systems) and the QoL benefit associated with reduced FoH or the elimination of the requirement for fingerstick calibration. There is also evidence to show that the Dexcom G6 RT-CGM system is associated with a significant increase in time in range relative to previous generation systems.36 Although there is emerging evidence linking time in range to both glycemic control and complications in type 2 diabetes;37–39 however, at this time, the long-term implications of improved time in range in people with T1D remain largely unknown.
The analysis is associated with several limitations that should be considered alongside the interpretation of findings. Firstly, in the absence of long-term (>5 years) longitudinal data, clinical input data from a trial of 24 weeks duration were used to project long-term clinical outcomes. However, although long-term data are lacking, data from the COMISAIR study suggest that the treatment effects of RT-CGM are maintained over a period of at least 3 years.40 The possibility of a waning in treatment effect over time was not examined; however, a sensitivity analysis was performed in which the magnitude of the HbA1c treatment effect with RT-CGM was reduced by 30% and even with this reduction, the ICER remained considerably below CAD 50,000 per QALY gained. Secondly, the DIAMOND T1D study was performed in adults with a mean age of 48 years and a median duration of diabetes of 19 years, which limits the generalizability of the findings. For example, these findings may not be strictly generalizable to patients with newly diagnosed T1D or children and adolescents, where input from parents/caregivers represents an important aspect of diabetes management. In particular, attitudes to fingerstick testing may be different among those with newly diagnosed versus long-standing disease, and features of the Dexcom G6 RT-CGM system such as remote monitoring may be particularly valuable in terms of alleviating anxiety among parents/caregivers of children/adolescents with T1D.
Overall, findings of long-term cost-effectiveness analysis suggest that for adult patients with T1D in Canada, the Dexcom G6 RT-CGM system is cost-effective relative to SMBG, particularly for patients with a pronounced FoH such as those with a history of frequent and/or severe hypoglycemic events. The Dexcom G6 RT-CGM system improves glycemic control and reduces the risk of costly long-term diabetes-related complications, providing a cost-effective disease management option (relative to SMBG) based on a willingness-to-pay threshold of CAD 50,000 per QALY gained.
Acknowledgments
The abstract of this paper was presented at the Canadian Association for Population Therapeutics annual meeting 2020 (October 26th–27th, 2020) as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in The Journal of Population Therapeutics and Clinical Pharmacology: https://www.jptcp.com/index.php/jptcp/article/view/805.
Author Contributions
JJI and PL were responsible for the inception and design of the analysis. JJI, PL and SR were involved in the preparation of analysis settings and running of the analysis. JSP prepared the first draft of the manuscript. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
Funding for this analysis was provided by Dexcom.
Disclosure
PL is a current employee of Dexcom, which manufactures the G6 RT-CGM system. SR and JJI are current employees of HEVA HEOR, which has received consulting fees from Dexcom. JSP is a current employee of Ossian Health Economics and Communications, which has received consulting fees from Dexcom. The authors report no other conflicts of interest in this work.
References
1. Rodbard D. Continuous glucose monitoring: a review of recent studies demonstrating improved glycemic outcomes. Diabetes Technol Ther. 2017;19(S3):S25–S37. doi:10.1089/dia.2017.0035
2. Parkin CG, Graham C, Smolskis J. Continuous glucose monitoring use in type 1 diabetes: longitudinal analysis demonstrates meaningful improvements in HbA1c and reductions in health care utilization. J Diabetes Sci Technol. 2017;11(3):522–528. doi:10.1177/1932296817693253
3. McGibbon A, Adams L, Ingersoll K, Kader T, Tugwell B; Diabetes Canada Clinical Practice Guidelines Expert Committee. Glycemic management in adults with type 1 diabetes. Can J Diabetes. 2018;42(Suppl 1):S80–S87. doi:10.1016/j.jcjd.2017.10.012
4. Yale JF, Paty B, Senior PA; Diabetes Canada Clinical Practice Guidelines Expert Committee. Hypoglycemia. Can J Diabetes. 2018;42(Suppl 1):S104–S108. doi:10.1016/j.jcjd.2017.10.010
5. Berard LD, Siemens R, Woo V; Diabetes Canada Clinical Practice Guidelines Expert Committee. Monitoring glycemic control. Can J Diabetes. 2018;42(Suppl 1):S47–S53. doi:10.1016/j.jcjd.2017.10.007
6. Diabetes Canada. Paying for your glucose monitoring device; November 28, 2019. Available from: https://www.diabetes.ca/managing-my-diabetes/stories/paying-for-glucose-monitoring-devices.
7. Health Quality Ontario. Continuous monitoring of glucose for type 1 diabetes: a health technology assessment. Ont Health Technol Assess Ser. 2018;18(2):1–160.
8. Diabetes Canada. Diabetes in Canada Backgrounder. Ottawa: Diabetes Canada; 2020. Available from: https://www.diabetes.ca/DiabetesCanadaWebsite/media/Advocacy-and-Policy/Backgrounder/2020_Backgrounder_Canada_English_FINAL.pdf.
9. Newswire.ca. Dexcom CGM system now available in Canada; September 09 2019. Available from: https://www.newswire.ca/news-releases/dexcom-g6-r-cgm-system-now-available-in-canada-887735218.html.
10. Puhr S, Derdzinski M, Welsh JB, Parker AS, Walker T, Price DA. Real-world hypoglycemia avoidance with a continuous glucose monitoring system’s predictive low glucose alert. Diabetes Technol Ther. 2019;21(4):155–158. doi:10.1089/dia.2018.0359
11. Beck RW, Riddlesworth T, Ruedy K; DIAMOND Study Group. et al. Effect of continuous glucose monitoring on glycemic control in adults with type 1 diabetes using insulin injections: the DIAMOND randomized clinical trial. JAMA. 2017;317(4):371. doi:10.1001/jama.2016.19975.
12. Polonsky WH, Hessler D, Ruedy KJ, Beck RW; DIAMOND Study Group. The impact of continuous glucose monitoring on markers of quality of life in adults with type 1 diabetes: further findings from the DIAMOND randomized clinical trial. Diabetes Care. 2017;40(6):736–774. doi:10.2337/dc17-0133
13. Palmer AJ, Roze S, Valentine WJ, et al. The CORE diabetes model: projecting long-term clinical outcomes, costs and cost-effectiveness of interventions in diabetes mellitus (types 1 and 2) to support clinical and reimbursement decision-making. Curr Med Res Opin. 2004;20(Suppl 1):S5–26. doi:10.1185/030079904X1980
14. Palmer AJ, Roze S, Valentine WJ, et al. Validation of the CORE diabetes model against epidemiological and clinical studies. Curr Med Res Opin. 2004;20(Suppl 1):S27–S40. doi:10.1185/030079904X2006
15. McEwan P, Foos V, Palmer JL, Lamotte M, Lloyd A, Grant D. Validation of the IMS CORE diabetes model. Value Health. 2014;17(6):714–724. doi:10.1016/j.jval.2014.07.007
16. Riddlesworth T, Price D, Cohen N, Beck RW. Hypoglycemic event frequency and the effect of continuous glucose monitoring in adults with type 1 diabetes using multiple daily insulin injections. Diabetes Ther. 2017;8(4):947–951. doi:10.1007/s13300-017-0281-4
17. Currie CJ, Morgan CL, Poole CD, Sharplin P, Lammert M, McEwan P. Multivariate models of health-related utility and the fear of hypoglycaemia in people with diabetes. Curr Med Res Opin. 2006;22(8):1523–1534. doi:10.1185/030079906X115757
18. Matza LS, Stewart KD, Davies EW, Hellmund R, Polonsky WH, Kerr D. Health state utilities associated with glucose monitoring devices. Value Health. 2017;20(3):507–551. doi:10.1016/j.jval.2016.10.007
19. Beaudet A, Clegg J, Thuresson PO, Lloyd A, McEwan P. Review of utility values for economic modeling in type 2 diabetes. Value Health. 2014;17(4):462–470. doi:10.1016/j.jval.2014.03.003
20. Evans M, Khunti K, Mamdani M, et al. Health-related quality of life associated with daytime and nocturnal hypoglycaemic events: a time trade-off survey in five countries. Health Qual Life Outcomes. 2013;11(1):90. doi:10.1186/1477-7525-11-90
21. Canadian Agency for Drugs and Technologies in Health. Optimal use recommendations forsecond and third-line therapy for patients with type 2 diabetes. Ottawa: The Agency; 2013. (CADTHoptimal use report; vol.3, no. 1d). Available from: https://www.cadth.ca/media/pdf/OP0512_Diabetes_RecsReport_2nd_3rd-line_e.pdf.
22. Brown ST, Grima DG, Sauriol L. Cost-effectiveness of insulin glargine versus sitagliptin in insulin-naïve patients with type 2 diabetes mellitus. Clin Ther. 2014;36(11):1576–1578. doi:10.1016/j.clinthera.2014.07.019
23. Canadian Institute for Health Information. Patient cost estimator. Ottawa, ON: CIHI; 2020. Available from: https://www.cihi.ca/en/patient-cost-estimator.
24. Thokala P, Kruger J, Brennan A, Basarir H, Duenas A, Pandor A, Gillett M, Elliot J, Heller S. The Sheffield Type 1 Diabetes Policy Model. HEDS Discussion Paper 13/05. 2013. Available from: https://www.sheffield.ac.uk/scharr/sections/heds/discussion-papers/1305-1.258469.
25. Canadian Agency for Drugs and Technologies in Health. Guidelines for the economic evaluation of health technologies 4th edition; March 2017. Available from: https://www.cadth.ca/sites/default/files/pdf/guidelines_for_the_economic_evaluation_of_health_technologies_canada_4th_ed.pdf.
26. Houlden RL, Berard L, Lakoff JM, Woo V, Yale JF; Diabetes Canada Clinical Practice Guidelines Expert Committee. Diabetes and driving. Can J Diabetes. 2018;42(Suppl 1):S150–S153. doi:10.1016/j.jcjd.2017.10.018
27. Miller KM, Beck RW, Bergenstal RM, et al.; T1D Exchange Clinic Network. Evidence of a strong association between frequency of self-monitoring of blood glucose and hemoglobin A1c levels in T1D exchange clinic registry participants. Diabetes Care. 2013;36(7):2009–2014. doi:10.2337/dc12-1770
28. O’Reilly DJ, Burke N, Tarride JE, Hahn J, Nurkanovic L. Direct health-care costs and productivity costs associated with hypoglycemia in adults with type 1 and type 2 diabetes mellitus that participated in the Canadian hypoglycemia assessment tool program. Can J Diabetes. 2018;42(6):659–663. doi:10.1016/j.jcjd.2018.01.010
29. Brod M, Wolden M, Christensen T, Bushnell DM. Understanding the economic burden of nonsevere nocturnal hypoglycemic events: impact on work productivity, disease management, and resource utilization. Value Health. 2013;16(8):1140–1149. doi:10.1016/j.jval.2013.09.002
30. Billings LK, Parkin CG, Price D. Baseline Glycated hemoglobin values predict the magnitude of glycemic improvement in patients with type 1 and type 2 diabetes: subgroup analyses from the DIAMOND study program. Diabetes Technol Ther. 2018;20(8):
31. Martyn-Nemeth P, Schwarz Farabi S, Mihailescu D, Nemeth J, Quinn L. Fear of hypoglycemia in adults with type 1 diabetes: impact of therapeutic advances and strategies for prevention - a review. J Diabetes Complications. 2016;30(1):167–177. doi:10.1016/j.jdiacomp.2015.09.003
32. Fidler C, Elmelund Christensen T, Gillard S. Hypoglycemia: an overview of fear of hypoglycemia, quality-of-life, and impact on costs. J Med Econ. 2011;14(5):646. doi:10.3111/13696998.2011.610852
33. Aronson R, Goldenberg R, Boras D, Skovgaard R, Bajaj H. The Canadian hypoglycemia assessment tool program: insights into rates and implications of hypoglycemia from an observational study. Can J Diabetes. 2018;42(1):11–17. doi:10.1016/j.jcjd.2017.01.007
34. The Nightscout Project. Nightscout #WeAreNotWaiting. 2020. Available from: http://www.nightscout.info/.
35. Chaugule S, Graham C. Cost-effectiveness of G5 Mobile continuous glucose monitoring device compared to self-monitoring of blood glucose alone for people with type 1 diabetes from the Canadian societal perspective. J Med Econ. 2017;20(11):1128–1135. doi:10.1080/13696998.2017.1360312
36. Welsh JB, Gao P, Derdzinski M, et al. Accuracy, utilization, and effectiveness comparisons of different continuous glucose monitoring systems. Diabetes Technol Ther. 2019;21(3):128–132. doi:10.1089/dia.2018.0374
37. Vigersky RA, McMahon C. The relationship of hemoglobin A1C to time-in-range in patients with diabetes. Diabetes Technol Ther. 2019;21(2):81–85. doi:10.1089/dia.2018.0310
38. Yoo JH, Choi MS, Ahn J, et al. Association between continuous glucose monitoring-derived time in range, other core metrics, and albuminuria in type 2 diabetes. Diabetes Technol Ther. 2020;22(10):768–776. doi:10.1089/dia.2019.0499.
39. Guo Q, Zang P, Xu S, et al. Time in range, as a novel metric of glycemic control, is reversely associated with presence of diabetic cardiovascular autonomic neuropathy independent of HbA1c in Chinese type 2 diabetes. J Diabetes Res. 2020;2020:5817074. doi:10.1155/2020/5817074
40. Šoupal J, Petruželková L, Grunberger G, et al. Glycemic outcomes in adults with T1D are impacted more by continuous glucose monitoring than by insulin delivery method: 3 years of follow-up from the COMISAIR study. Diabetes Care. 2020;43(1):37–43. doi:10.2337/dc19-0888
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.