Back to Journals » Infection and Drug Resistance » Volume 17
Evaluation of Sulfasalazine as an Adjunctive Therapy in Treating Pulmonary Pre-XDR-TB: Efficacy, Safety, and Treatment Implication
Authors Fu L ![]() , Wang W, Xiong J
, Wang W, Xiong J ![]() , Zhang P
, Zhang P ![]() , Li H
, Li H ![]() , Zhang X, Liang H, Yang Q, Wang Z, Chen X, Deng G
, Zhang X, Liang H, Yang Q, Wang Z, Chen X, Deng G ![]() , Cai Y, Tang S
, Cai Y, Tang S ![]()
Received 10 October 2023
Accepted for publication 12 February 2024
Published 17 February 2024 Volume 2024:17 Pages 595—604
DOI https://doi.org/10.2147/IDR.S443897
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Liang Fu,1,2,* Wenfei Wang,2,3,* Juan Xiong,4,* Peize Zhang,2 Hui Li,2 Xilin Zhang,5 Hancheng Liang,6 Qianting Yang,2 Zhaoqin Wang,2 Xinchun Chen,3 Guofang Deng,2 Yi Cai,3 Shenjie Tang1
1Beijing Chest Hospital, Capital Medical University, Beijing Tuberculosis and Thoracic Tumour Research Institute, Beijing, People’s Republic of China; 2Shenzhen Third People’s Hospital, National Clinical Research Center for Infectious Disease (Shenzhen), Shenzhen Clinical Research Center for Tuberculosis, Southern University of Science and Technology, Shenzhen, Guangdong, People’s Republic of China; 3Department of Pathogen Biology, Guangdong Key Laboratory of Regional Immunity and Diseases, Shenzhen University School of Medicine, Shenzhen, Guangdong, People’s Republic of China; 4Health Science Center, Shenzhen University, Shenzhen, Guangdong, People’s Republic of China; 5Tuberculosis Prevention and Control Department, the Fourth People’s Hospital of Foshan, Foshan, Guangdong, People’s Republic of China; 6Division Two of Tuberculosis Diseases Department, the Sixth People’s Hospital of Dongguan, Dongguan, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shenjie Tang; Yi Cai, Email [email protected]; [email protected]
Background: The rising prevalence and limited efficacy of treatments for pre-extensively drug-resistant tuberculosis (pre-XDR-TB) underscore an immediate need for innovative therapeutic options. A combination of host-directed therapy (HDT) and anti-TB treatment presents a viable alternative for pre-XDR-TB management. Sulfasalazine (SASP), by targeting the amino acid transport system xc (xCT), potentially reduces the intracellular Mycobacterium tuberculosis load and mitigates lung pathology, positioning it as a promising TB HDT agent. This study aims to assess the efficacy of SASP as a supplementary therapy for pre-XDR-TB.
Methods: A pilot study examined the safety and effectiveness of two 9-month short-course, all-oral regimens for pre-XDR-TB treatment: Bdq-regimen (consisting of Bdq, linezolid, cycloserine, clofazimine, and pyrazinamide) and SASP-regimen (comprising SASP, linezolid, cycloserine, clofazimine, and pyrazinamide). The primary endpoint was the incidence of unfavorable outcomes 12 months post-treatment.
Results: Of the 44 participants enrolled, 43 were assessable 12 months post-treatment. Culture conversion rates stood at 73.2% by Month 2 and escalated to 95.1% by Month 6. Overall, 88.4% (38/43) of the participants exhibited favorable outcomes, 85.2% (19/23) for the Bdq-regimen and 93.8% (14/15) for the SASP-regimen. The SASP-regimen group recorded no deaths or treatment failures.
Conclusion: Both 9-month short-course, all-oral regimens manifested commendable primary efficacy in treating pre-XDR-TB patients. The SASP-regimen emerged as effective, safe, well-tolerated, and cost-effective.
Plain Language Summary: This study explored a new way to treat a hard-to-treat type of tuberculosis (TB) using a medicine called Sulfasalazine, alongside usual TB treatments. Over 9 months, two groups of patients were given different sets of medicines, one including Sulfasalazine. The results, checked 12 months after treatment, showed that most patients improved, especially those given Sulfasalazine. No one in the Sulfasalazine group died or had their treatment fail, suggesting that Sulfasalazine could be a promising addition to current treatments for this tough-to-treat TB.
Keywords: Sulfasalazine, host-directed therapy, pre-extensive drug-resistant tuberculosis, short-course, treatment
Introduction
Tuberculosis (TB) remains a formidable global health challenge with Mycobacterium tuberculosis (M. tb) accounting for numerous deaths worldwide.1 A significant hurdle in TB control is drug resistance, notably multi-drug resistant tuberculosis (MDR-TB) and the emergent pre-extensively drug-resistant tuberculosis (pre-XDR-TB).2 MDR-TB is caused by strains resistant to at least isoniazid and rifampicin; Rifampicin-resistant TB (RR-TB) is specifically resistant to rifampicin. Pre-XDR-TB involves MDR/RR-TB strains also resistant to any fluoroquinolone (FQ); Extensively drug-resistant TB (XDR-TB) extends to MDR/RR-TB strains resistant to any FQ and at least one of bedaquiline (Bdq) or linezolid (Lzd).1 Treatment for MDR-TB typically spans 6 to 18 months using a combination of antimicrobials, while pre-XDR-TB demands even more extended treatment with a lower success rate (57% vs 73% for MDR-TB).3 There’s an evident need for innovative therapeutic strategies.
Host-directed therapy (HDT) emerges as a potential solution, modulating the host immune system to limit inflammation and tissue damage. This approach, especially potent for drug-resistant TB, could mitigate lung inflammation, reduce treatment durations, and potentially curb drug resistance development.4–6 Our prior research indicated sulfasalazine (SASP) as a promising HDT candidate for TB, showing its efficacy in enhancing immune responses and curbing bacterial growth.7–9 Building on these findings, we hypothesized that a combination of chemotherapy and SASP as HDT could enhance the treatment efficacy for pre-XDR-TB, especially considering the low success rate and limited effective drug options for this form of TB.
Bdq, endorsed by the WHO for pre-XDR-TB treatment,10,11 presents challenges like limited accessibility and high costs in regions like China.12 In this study, we aimed to demonstrate that a treatment regimen incorporating Bdq could be shortened to nine months, in contrast to the longer, individualized regimens of up to 18 months or longer currently recommended by the WHO.11
Accordingly, our study compared the efficacy and safety of a Bdq-based regimen with a SASP-based regimen for the treatment of pre-XDR-TB. The SASP-based regimen may be a more accessible, cost-effective, and efficacious alternative to the current WHO-approved Bdq-based regimen.
Methods
Trial Design and Oversight
We conducted an prospective cohort study in Shenzhen, China, evaluating two pre-XDR-TB regimens: the Bdq regimen (Bdq, Lzd, cycloserine [Cs], clofazimine [Cfz], pyrazinamide [Pza]) and the SASP regimen (SASP, Lzd, Cs, Cfz, Pza). Patients chose between Regimen A and B based on preference. Each regimen lasts 9–12 months. After 6 months, patients from both regimens were categorized into 9-month or 12-month subgroups based on clinical assessment. The trial received approval from the ethics committee of Shenzhen Third People’s Hospital and registration with the Chinese Clinical Trials Registry (ChiCTR2000032298). All participants gave written consent, and the authors confirmed adherence to the protocol and data accuracy.
Participants
At the Shenzhen Third People’s Hospital, we enrolled pulmonary TB patients aged 15–75 years. Exclusion criteria encompassed: Fridericia-corrected QT interval (QTcF) over 450 ms; HIV positivity; known drug resistance; allergies/intolerance to study drugs; specific abnormal lab findings like hemoglobin under 90 g/L, platelet counts below 75,000/mm^3, alanine aminotransferase (ALT) or aspartate aminotransferase (AST) levels tripling the normal range, exceedingly high bilirubin or creatinine levels. Patients previously treated with study drugs for over a month within the past three months were excluded, unless drug susceptibility testing (DST) verified the drug’s effectiveness. Extrapulmonary TB patients were excluded. However, those with advanced pulmonary TB, marked by bilateral cavitary disease or major parenchymal damage on chest computed tomography (CT), were included. For comprehensive inclusion/exclusion criteria, refer to Table S1.
Confirmation of Pre-XDR-TB
Rifampicin resistance was detected using the Xpert MTB/RIF assay (Xpert, Cepheid). FQs resistance was ascertained through genotypic (gDST) or phenotypic drug susceptibility tests (pDST), which evaluated the minimum inhibitory concentration (MIC) (Thermo Scientific, USA). gDST encompassed PCR melting curve analysis (Zeesan Biotech, China), whole genome sequencing (Novogene, China), and mass spectrometry (Conlight Medical, China). Since DST results for Bdq, Lzd, Cfz, and Pza were not available, these drugs did not influence treatment modifications. Cs pDST was affirmed by measuring the MIC. Despite spotting Cs resistance, treatment protocols persisted unchanged due to the unreliable nature of Cs resistance test results.
Study Procedures and Treatment Protocols
Eligible participants were informed about potential risks and benefits by study staff. After giving consent, participants chose between Bdq-regimen and SASP-regimen based on financial, adherence, and insurance considerations.
Upon enrollment, participants underwent initial screenings. Follow-up assessments occurred bi-weekly for two months, monthly during treatment, and quarterly post-treatment for a year (detailed in Tables S2 and S3). The initial screening covered medical history, physical exams, and vision tests. Further clinical evaluations included a quick peripheral neuropathy check, anxiety and depression gradings.13 Other evaluations included respiratory sample collection, AFB smear microscopy, Xpert MTB/RIF assays, M. tb cultures, and both gDST and pDST tests. Blood tests were conducted regularly. The chest CT scans were conducted bi-monthly during the initial six months and then once every three months until a year post-treatment, which is the empirical preference over X-rays for assessing lung lesions and evaluating anti-TB efficacy.
An independent committee evaluated whether participants with confirmed active pre-XDR TB were eligible for treatment. Post-enrollment exclusions included those with negative M. tb cultures or evidence of rifampicin susceptibility. Participants were regularly assessed for treatment efficacy and potential AEs. Chest CT images were blindly reviewed by two experts from the Shenzhen Third People’s Hospital (Table S4). The mid-point review committee meticulously evaluated clinical outcomes to determine the favorable treatment response at Month 6 (FR-6, detailed in Table S4). FR-6 criteria include: Sputum culture conversion (CC) by month 4; positive treatment response at month 6, excluding those taking less than approximately 90% of the prescribed dose; consistent findings on chest CT scans at month 6. Patients meeting FR-6 criteria completed treatment in 9 months; otherwise, treatment was extended to 12 months. In the 12-month group, lack of culture conversion at month 8 extended treatment to 18–20 months, indicating treatment failure. An end-point committee identified undesirable outcomes, like treatment failures or recurrences.
SASP (250 mg) was administered in divided doses to 3000 mg per day. All drugs were used throughout the course without being cut back halfway through. Detailed regimen drugs and dosages are given in Tables S5 and S6.
Adherence was measured by questionnaires at each visit. Study participants and their families received educational counseling and psychological support throughout the study, primarily through the WeChat app (Tencent Tech, Shenzhen, China).
Treatment Outcomes and Operational Definitions
By study end, participants were categorized as having an unfavorable, favorable, or unassessable outcome. Those marked “unassessable” were omitted from primary analysis.
The primary efficacy measure was the unfavorable status at 24 months post-enrollment. Unfavorable status covered treatment failure, treatment discontinuation, or any-cause death. Treatment failure required regimen changes or stops due to factors like poor clinical/bacteriological response, drug reactions, or drug resistance evidence. Bacteriologic measures, such as failure, relapse, or re-infection, were pivotal for this classification. Bacteriological failure meant no conversion without reversion by Month 8, necessitating two positive M. tb cultures on separate days without any negative in-between. Relapse involved a prior negative-testing individual becoming positive for the original MDR-TB strain within a year post-successful treatment. Reinfection pertained to a TB return due to a genetically distinct M. tb strain. Without strain analysis, any TB recurrence was termed “bacteriological recurrence”. A favorable outcome is defined as a participant’s last culture result during the month 9 analysis visit window being M. tb-negative, with no subsequent positive cultures until the end of the follow-up period, and the absence of active TB symptoms/signs, provided no unfavorable outcome has occurred. An unassessable outcome is defined as a participant who, without having an unfavorable outcome, either misses a visit with a negative M. tb culture result, becomes pregnant, dies from non-TB-related causes, experiences an accidental or violent death, or receives modified or prolonged treatment due to reinfection with a different M. tb strain.
Secondary efficacy outcomes concentrated on Month 2 sputum CC and FR-6 achievement. Primary safety outcomes revolved around AEs of grade 3 or more and any-grade SAEs within the first year. AEs were scaled from 1 to 4. At every visit, the severity of AEs was jointly evaluated by researchers and participants. More outcome details are in Tables S4 and S7.
Sample Size
As a prospective cohort study, we continuously enrolled available participants during the study period.
Statistical Analysis
Statistical analyses were performed using R software (version 4.1.3; R Project for Statistical Computing, Vienna, Austria). Continuous variables were expressed as the median (interquartile range, IQR), and categorical variables were reported as a percentage (frequency). The Shapiro–Wilk test was conducted to assess the normality of variables. The Wilcoxon rank sum test, Fisher’s exact test, and Pearson’s chi-squared test were performed to evaluate differences between groups. The time to an unfavorable outcome and time to culture-conversion (overall and stratified according to the treatment group) were compared by using Kaplan–Meier estimates. A two-sided P < 0.05 was considered to indicate statistical significance.
Results
Participants
Between May 23 and December 31, 2020, 59 pre-XDR-TB patients were screened for the study. Of these, 44 were enrolled, with 15 being excluded due to reasons such as an inability to attend follow-ups, presence of extrapulmonary TB, and use of injectable agents. Upon completion, 27 participants from the Bdq-regimen and 17 from the SASP-regimen finished both the treatment and the subsequent 12-month follow-up (Figure 1). The data analysis, which includes details presented in Table 1, revealed that 25 participants had lung cavities—15 with unilateral and 10 with bilateral cavities. There were no significant differences between groups in terms of age, sex, BMI, TB recurrence, and treatment history.
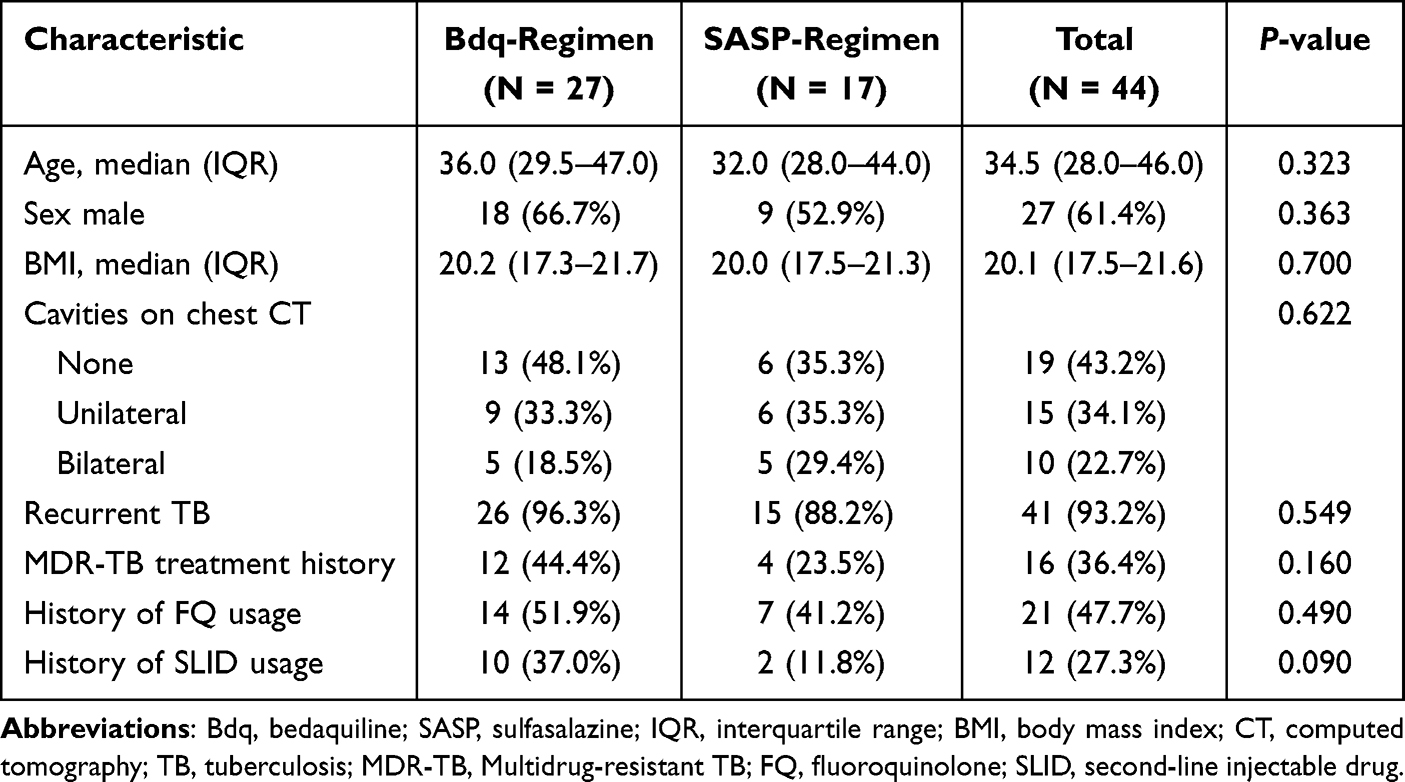 |
Table 1 Baseline Characteristics of the Participants |
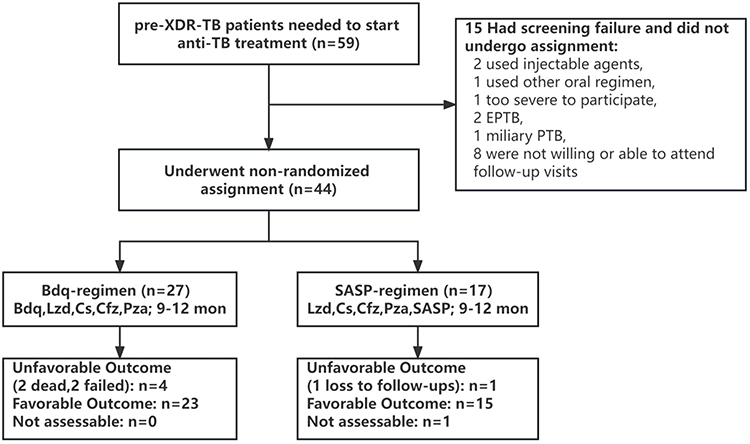 |
Figure 1 Enrollment and profile of trial participants. Abbreviations: pre-XDR-TB, pre-extensively drug-resistant tuberculosis; TB, tuberculosis; Bdq, bedaquiline; Lzd, linezolid; Cs, cycloserine; Cfz, clofazimine; Pza, pyrazinamide; SASP, sulfasalazine; EPTB, extrapulmonary tuberculosis; PTB, pulmonary tuberculosis. |
Efficacy Outcome
Till 24 months after treatment completion, one participant on the SASP-regimen who missed the final visit was deemed “not assessable.” Overall, 88.4% (38/43) of patients had favorable outcomes: 85.2% (23/27) in the Bdq-regimen and 93.8% (15/16) in the SASP-regimen. Unfavorable outcomes were observed in 11.6% (5/43): two deaths, two treatment failures in the Bdq-regimen, and one loss to follow-up in the SASP-regimen. Despite the SASP-regimen indicating a marginally better outcome rate, no significant difference in time to unfavorable outcome was seen between the two regimens (P=0.41) (Table 2). There was no significant difference in the time to an unfavorable outcome between the Bdq-regimen and SASP-regimen groups (P = 0.43) (Figure 2).
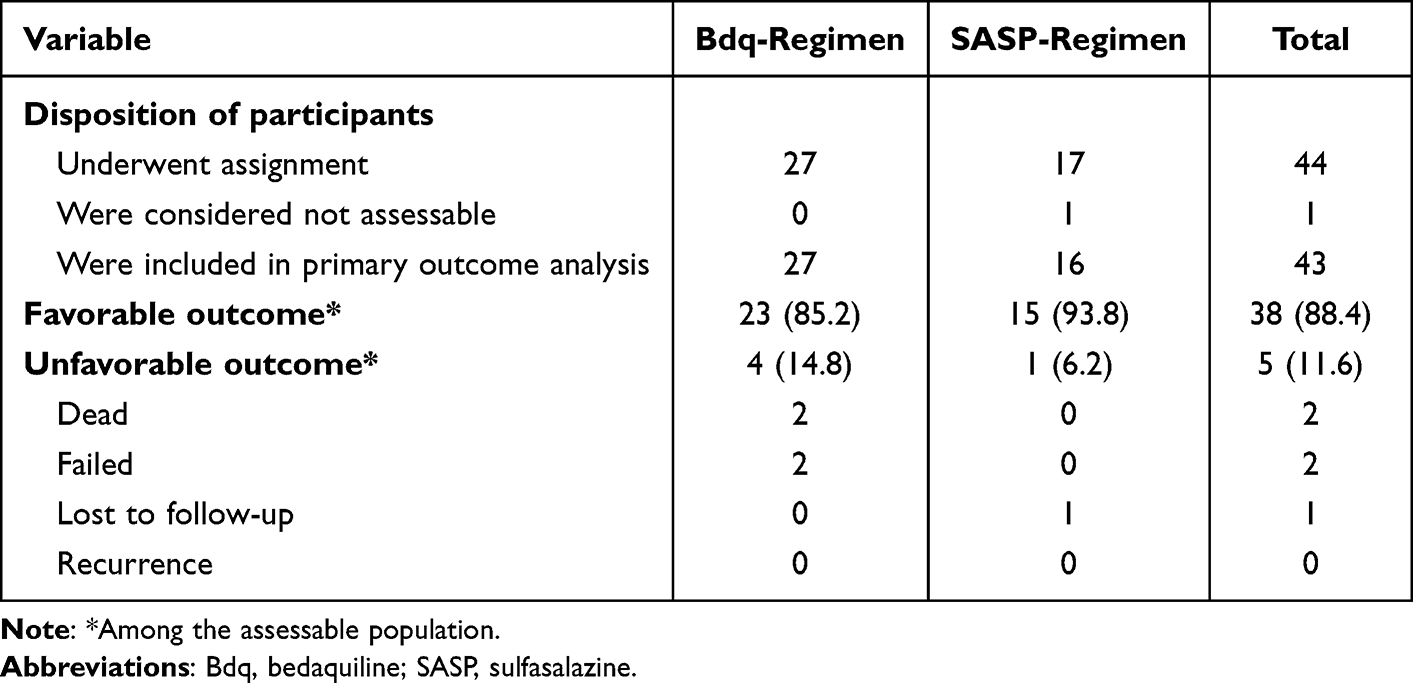 |
Table 2 Primary Efficacy Analysis |
 |
Figure 2 Time to unfavorable outcomes. The time to an unfavorable outcome stratified according to treatment group. Log rank tests showed that there was no significant difference in the time to an unfavorable outcome between the Bdq-regimen and SASP-regimen groups (P = 0.43). Abbreviations: TRT, treatment; Bdq, bedaquiline; SASP, sulfasalazine. Notes: due to limited number of unfavorable outcomes, the median to an unfavorable outcome is unavailable for the Bdq- and SASP-regimens. |
Culture-conversion at Month 2 was observed in 76% (19/25) of the Bdq-regimen group and 68.8% (11/16) of the SASP-regimen. By Month 6, these figures rose to 96.2% and 93.3% for the Bdq and SASP regimens, respectively. The median time to culture-conversion was 56 days, with no significant disparity between the two treatments: 50.5 (29.8–75.5) days for Bdq and 60.5 (46.5–96.8) days for SASP (P=0.30) (Table 3). There was no significant difference in the time to culture-conversion between Bdq- and SASP-regimens (P = 0.41) (Figure 3). No instances of relapse or re-infection occurred (Table 2).
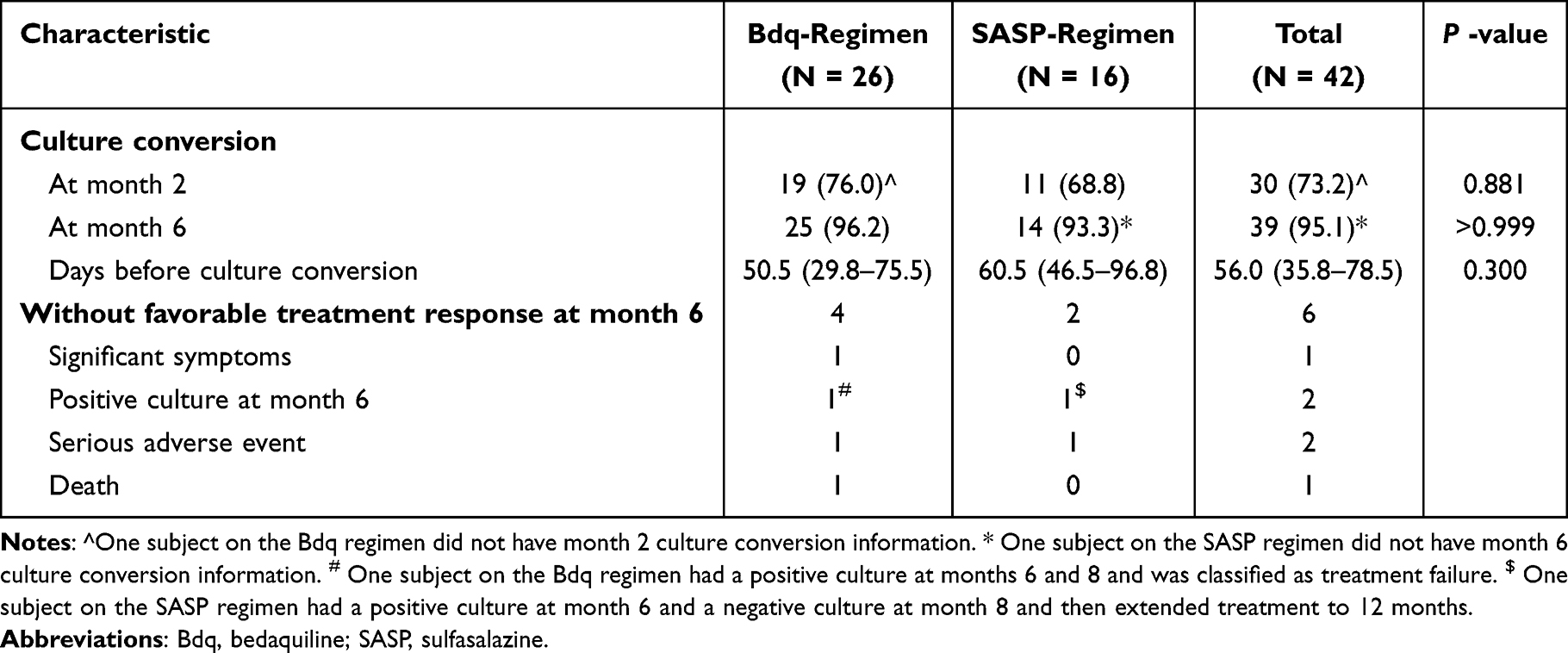 |
Table 3 Time to Culture-Conversion Comparisons Between Bdq-Regimen and SASP-Regimen |
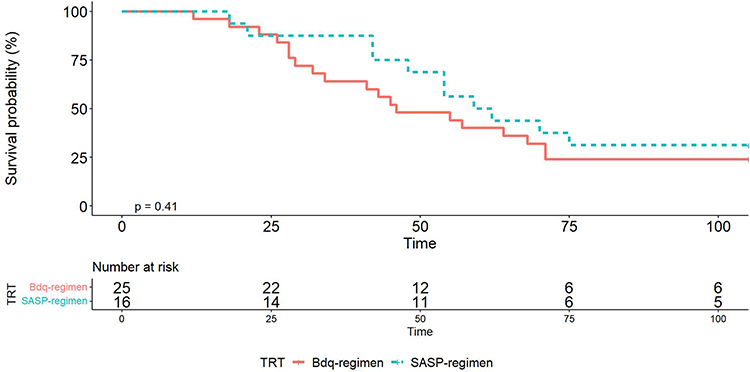 |
Figure 3 Time to culture-conversion among patients who were positive at baseline. Kaplan-Meier estimates of the time to culture-negative status stratified according to treatment group. The median to the CC for Bdg-regimen group is 50.5 days, while the median time to CC for SASP-regimen group is 60.5 days. There was no significant difference in the time to culture-conversion between Bdq- and SASP-regimens (P = 0.41). Abbreviations: cc, culture conversion; TRT, treatment; Bdq, bedaquiline; SASP, sulfasalazine. |
Regarding FR-6, 85.7% (36/42) of participants achieved it. However, it was unattained by a few due to reasons like serious adverse events, positive cultures, or death. Specifically, one SASP-regimen participant, after a positive culture at Month 6 but negative at Month 8, extended their treatment duration to 12 months (Table 3).
Adverse Events
During the treatment, 97.7% of participants experienced at least one AE, with every participant in the Bdq-regimen experiencing an AE, compared to 94.1% in the SASP-regimen (Table 4). The most frequent AEs included visual problems, numbness, joint issues, low energy, dizziness, palpitations, insomnia, and memory decline. Fortunately, most of these were mild (grade 1 or 2) and were manageable.
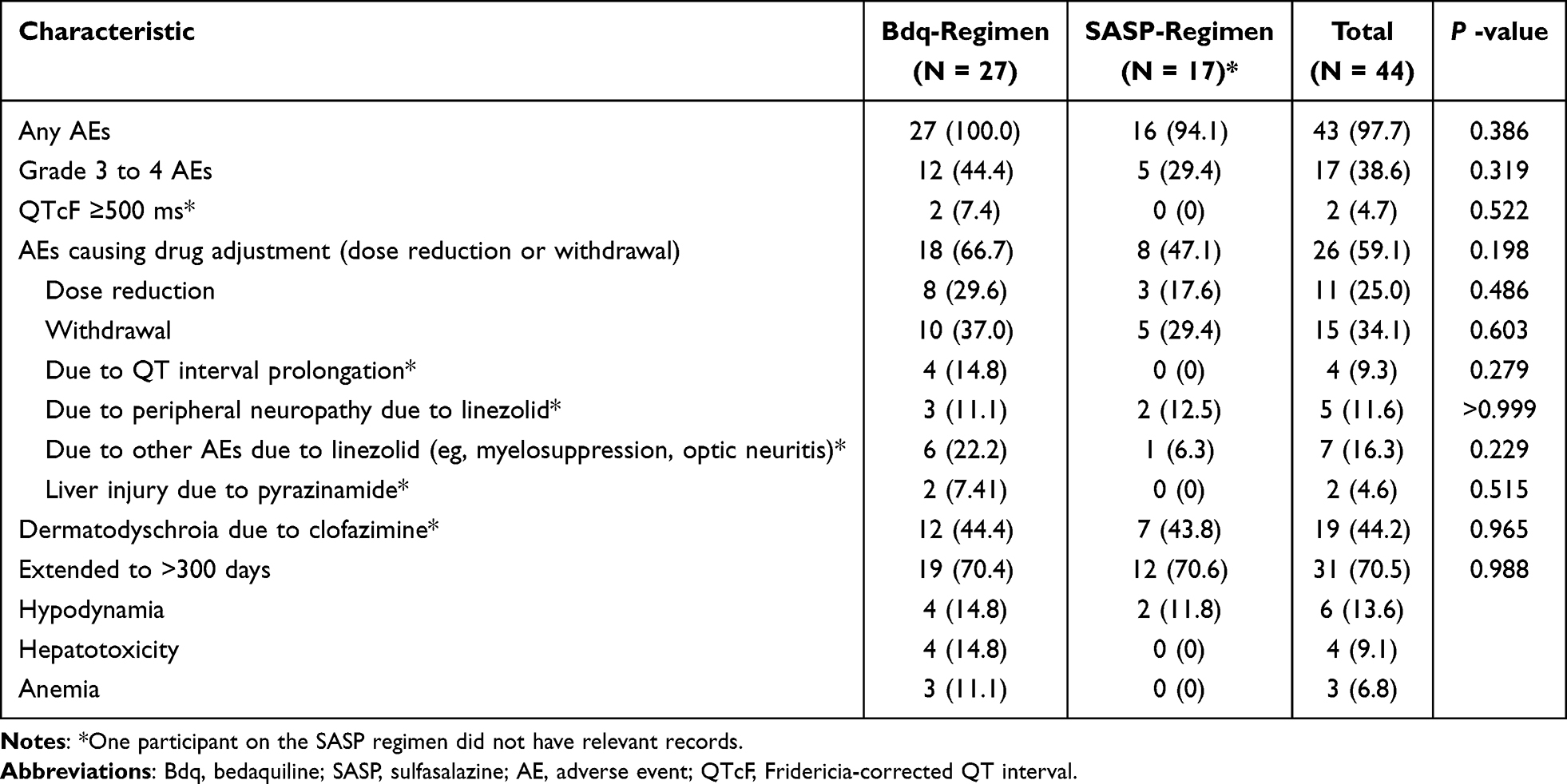 |
Table 4 Adverse Events That Occurred or Worsened During Treatment |
When it came to more SAEs, 38.6% (17/44) of patients reported them. The Bdq-regimen had a slightly higher proportion at 44.4% (11/27), compared to 29.4% (5/17) in the SASP-regimen. The most frequent severe AEs were low energy, experienced by six patients; hepatotoxicity, observed in four patients; and anemia, reported by three patients. All of these were more common in the Bdq-regimen. Notably, prolonged QTcF, a potential heart rhythm complication, was rare, with only one severe case in the Bdq-regimen.
More than half (59.1%, 26/44) of the participants had to adjust their medication either by reducing the dose or withdrawing due to AEs. Every participant who had to adjust their medication because of QT interval prolongation >500 ms was on the Bdq-regimen. The drug Lzd was discontinued the most, affecting 27.3% (12/44) in the Bdq-regimen and 18.8% (3/17) in the SASP-regimen. Another drug, Pza, which led to liver toxicity, was halted for 4.6% (2/44) of participants, all of whom were on the Bdq-regimen.
Discussion
With the growing global challenge of antimicrobial resistance, there is an urgent need for innovative therapeutic interventions. In this context, our pilot study aimed to understand the therapeutic potential of adding SASP to short-course regimens for pulmonary pre-XDR-TB patients. Notably, our results underscored a comparable efficacy between the SASP regimen and the Bdq regimen. Equally important, SASP demonstrated commendable safety and was well tolerated by patients.
The first 12 months after completion of treatment have been identified as critical for detecting TB relapse,14 a fact that influenced our decision to establish it as the primary endpoint of our study. In the grand scheme of treating pre-XDR-TB, the overarching goals remain twofold: to achieve robust efficacy while minimizing treatment duration and number of drugs.15 In our study, two experimental arms, each based on a quintet of oral drugs, demonstrated favorable results (85.2% for the Bdq regimen and 93.8% for the SASP regimen). The SASP regimen appears to have better treatment outcomes, but due to the small sample size, no definitive conclusions can be drawn. At the very least, the SASP regimen is a promising direction for treatment. These results are congruent with those of the Nix-TB and ZeNix trials, with the former reporting a 90% favorable outcome rate16 and the latter showing success rates between 84% and 93%.17
The robust culture-conversion rates at the 2 and 6-month markers stand as a testament to the positive therapeutic response. Bdq is a bacteriostatic drug with good early bactericidal activity;3 SASP is an adjuvant therapy that does not directly kill M. tuberculosis but reduces the inflammatory response.4–9 This explains the higher rate of sputum culture conversion at month 2 with the Bdq-based regimen. A minor portion of the participants (6 out of 44) failed to meet the FR-6 criteria, with five requiring a treatment extension up to 12 months. Nevertheless, a significant majority (88.6%, or 37/44) reached the treatment endpoint within 9 months. Interestingly, while Bdq regimen recorded Grade 3 to 4 AE in 44.4% of participants, the SASP regimen showed a markedly reduced incidence at 29.4%.
SASP’s clinical application, especially at elevated doses for conditions like rheumatoid arthritis and inflammatory bowel disease, is well-documented.18,19 Its dual role in reducing pro-inflammatory cytokines and inhibiting prostaglandin synthesis during M. tb infection signifies its therapeutic versatility.7 Preclinical studies on mouse models have already vouched for SASP’s potency in reducing lung lesion size, ameliorating lung pathology, and curtailing the M. tb burden.7 Our study, in which SASP was administered at the CFDA-approved dose for irritable bowel disease,20,21 reiterated its safety in treating pre-XDR-TB patients. Furthermore, the SASP-regimen, besides displaying higher efficacy, also had the distinction of zero incidents of QTcF ≥500 ms and no recorded fatalities. While the limited sample size tempers the statistical implications of these findings, the clinical significance is undebatable
The financial burden associated with Bdq, despite its 2020 introduction in China, cannot be overlooked.22,23 The towering cost—20-fold that of SASP—positions SASP as a plausible, cost-effective alternative, especially in regions with constrained Bdq access or for economically disadvantaged patients. The cardiotoxicity associated with Bdq, manifested in our study as a pronounced QT prolongation, further underscores the merits of SASP.
However, this study is not without its limitations. The modest sample size potentially curbed the statistical heft of our findings, underscoring the need for larger trials in the future. Unavoidable unblinding of patients and clinicians might have induced biases, a challenge future studies should strive to mitigate. Additionally, the genetic predisposition indicated by SNP, rs13120371, in the xCT gene needs further elucidation in future studies.9
Conclusion
In essence, our study heralds the 9-month SASP regimen as a promising therapeutic strategy for pre-XDR-TB, characterized by high culture conversion rates, favorable treatment outcomes, and minimal recurrence. Coupled with an admirable safety profile and affordability, SASP emerges as a potent and accessible HDT for TB. However, this study is only a preliminary investigation, and larger, more comprehensive studies are needed to validate and strengthen these findings.
Abbreviations
AEs, adverse events; ALT, alanine aminotransferase; AST, aspartate aminotransferase; Bdq, bedaquiline; BMI, body mass index; CFDA, China Food and Drug Administration; CC, culture conversion; Cfz, clofazimine; ChiCTR, Chinese Clinical Trials Registry; CT, computed tomography; Cs, cycloserine; DST, drug susceptibility testing; FQs, fluoroquinolones; FR-6, favorable treatment response at Month 6; gDST, genotypic drug susceptibility tests; HDT, host-directed therapy; IQR, interquartile range; Lzd, linezolid; M. tb, Mycobacterium tuberculosis; MIC, minimum inhibitory concentration; MDR-TB, multi-drug resistant tuberculosis; pDST, phenotypic drug susceptibility tests; pre-XDR-TB, pre-extensively drug-resistant tuberculosis; Pza, pyrazinamide; QTcF, Fridericia-corrected QT interval; SAEs, serious adverse events; SASP, sulfasalazine; SNP, single nucleotide polymorphism; Tb, tuberculosis; WHO, World Health Organization; XDR-TB, extensively drug-resistant tuberculosis; Xpert, Xpert MTB/RIF assay.
Data Sharing Statement
The raw/processed forms of the data presented in this manuscript cannot be shared at this time as they constitute part of an ongoing study.
Ethical Approval and Consent
The Ethical Committee of the Shenzhen Third People’s Hospital approved this study (number: 2020-019-03, date: 2020-05-23). After providing a clear explanation of their rights and duties, written informed consent was obtained from all study participants or a guardian in the case of minors before screening and assignment. The study was conducted according to the principles of the World Medical Association Declaration of Helsinki, Good Clinical Practice Guidelines, and local laws and regulations.
Acknowledgments
We thank all the physicians and assistants who participated in this study and enrolled patients. We thank the Haibo Wang for assistance in data management and analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82070016), the National Key Research and Development Program of China (2023YFC2306700, 2023YFC2306703), the Guangdong Provincial Clinical Research Center for Tuberculosis Project (2020B1111170014), the Shenzhen High-level Hospital Construction Fund (XKJS-CRGRK-008), the Shenzhen Clinical Research Center for Tuberculosis (20210617141509001), the Shenzhen Scientific and Technological Foundation (KCXFZ20211020163545004), Shenzhen Third People’s Hospital Research Fund (G2021010, G2021015, G2021023, G2022155).
Disclosure
All authors declare that they have no competing interests in this work.
References
1. WHO. Global Tuberculosis Report 2022. Geneva: World Health Organization; 2022.
2. Diriba G, Alemu A, Yenew B, et al. Epidemiology of extensively drug-resistant tuberculosis among patients with multidrug-resistant tuberculosis: a systematic review and meta-analysis. Int J Infect Dis. 2023;132:50–63. doi:10.1016/j.ijid.2023.04.392
3. Ahmad N, Ahuja SD, Akkerman OW, et al. Treatment correlates of successful outcomes in pulmonary multidrug-resistant tuberculosis: an individual patient data meta-analysis. Lancet. 2018;392(10150):821–834. doi:10.1016/S0140-6736(18)31644-1
4. Tiberi S, du Plessis N, Walzl G, et al. Tuberculosis: progress and advances in development of new drugs, treatment regimens, and host-directed therapies. Lancet Infect Dis. 2018;18(7):e183–98. doi:10.1016/S1473-3099(18)30110-5
5. Kilinç G, Saris A, Ottenhoff T, Haks MC. Host-directed therapy to combat mycobacterial infections. Immunol Rev. 2021;301(1):62–83. doi:10.1111/imr.12951
6. Zumla A, Maeurer M, Chakaya J, et al. Towards host-directed therapies for tuberculosis. Nat Rev Drug Discov. 2015;14(8):511–512. doi:10.1038/nrd4696
7. Cai Y, Yang Q, Liao M, et al. xCT increases tuberculosis susceptibility by regulating antimicrobial function and inflammation. Oncotarget. 2016;7(21):31001–31013. doi:10.18632/oncotarget.9052
8. Wang W, Ning Y, Wang Y, et al. Mycobacterium tuberculosis-Induced Upregulation of the COX-2/mPGES-1 Pathway in Human Macrophages Is Abrogated by Sulfasalazine. Front Immunol. 2022;13.
9. Wang W, Cai Y, Deng G, et al. Allelic-Specific Regulation of xCT Expression Increases Susceptibility to Tuberculosis by Modulating microRNA-mRNA Interactions. Msphere. 2020;5(2). doi:10.1128/mSphere.00263-20
10. WHO. WHO Model List of Essential Medicines - 22nd List. Geneva: World Health Organization; 2021.
11. WHO. WHO Consolidated Guidelines on Tuberculosis. Module 4: Treatment - Drug-Resistant Tuberculosis Treatment, 2022 Update. Geneva: World Health Organization; 2022.
12. Fu L, Weng T, Sun F, et al. Insignificant difference in culture conversion between bedaquiline-containing and bedaquiline-free all-oral short regimens for multidrug-resistant tuberculosis. Int J Infect Dis. 2021;111:138–147. doi:10.1016/j.ijid.2021.08.055
13. DAIDS. Division of AIDS (DAIDS) Table for Grading the Severity of Adult and Pediatric Adverse Events (Corrected Version 2.1); 2017.
14. Saderi L, Puci M, Di Lorenzo B, et al. Rapid Diagnosis of XDR and Pre-XDR TB: a Systematic Review of Available Tools. Arch Bronconeumol. 2022;58(12):809–820. doi:10.1016/j.arbres.2022.07.012
15. Tiberi S, Utjesanovic N, Galvin J, et al. Drug resistant TB - latest developments in epidemiology, diagnostics andmanagement. Int J Infect Dis. 2022;124 Suppl 1:S20–5. doi:10.1016/j.ijid.2022.03.026
16. Conradie F, Diacon AH, Ngubane N, et al. Treatment of Highly Drug-Resistant Pulmonary Tuberculosis. New Engl J Med. 2020;382(10):893–902. doi:10.1056/NEJMoa1901814
17. Conradie F, Bagdasaryan TR, Borisov S, et al. Bedaquiline–Pretomanid–Linezolid Regimens for Drug-Resistant Tuberculosis. New Engl J Med. 2022;387(9):810–823. doi:10.1056/NEJMoa2119430
18. Amos RS. The history of the use of sulphasalazine in rheumatology. Br J Rheumatol. 1995;34(Suppl 2):2–6. doi:10.1093/rheumatology/XXXIV.suppl_2.2
19. Conley B, Bunzli S, Bullen J, et al. What are the core recommendations for rheumatoid arthritis care? Systematic review of clinical practice guidelines. Clin Rheumatol. 2023;42(9):2267–2278. doi:10.1007/s10067-023-06654-0
20. González-Rayas JM. Drugs for inflammatory bowel disease. Med Lett Drugs Ther. 2023;65(1680):105–112. doi:10.58347/tml.2023.1680a
21. Asgharzadeh F, Yaghoubi A, Nazari SE, et al. The beneficial effect of combination therapy with sulfasalazine and valsartan in the treatment of ulcerative colitis. Excli J. 2021;20:236–247. doi:10.17179/excli2021-3370
22. Worley MV, Estrada SJ. Bedaquiline: a novel antitubercular agent for the treatment of multidrug-resistant tuberculosis. Pharmacotherapy. 2014;34(11):1187–1197. doi:10.1002/phar.1482
23. Zou J, Chen S, Rao W, et al. Population Pharmacokinetic Modeling of Bedaquiline among Multidrug-Resistant Pulmonary Tuberculosis Patients from China. Antimicrob Agents Ch. 2022;66(10). doi:10.1128/aac.00811-22
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.