Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Evaluation of Statin Indication and Dose Intensification Among Type 2 Diabetic Patients at a Tertiary Hospital
Authors Fisseha PY, Baye AM ![]() , Beyene MG
, Beyene MG ![]() , Makonnen E
, Makonnen E ![]()
Received 26 October 2023
Accepted for publication 27 February 2024
Published 7 March 2024 Volume 2024:17 Pages 1157—1169
DOI https://doi.org/10.2147/DMSO.S446711
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Pineal Yitbarek Fisseha,1 Assefa Mulu Baye,2 Melak Gedamu Beyene,2 Eyasu Makonnen2
1Tikur Anbessa Specialized Hospital, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Assefa Mulu Baye, Addis Ababa University, Addis Ababa, Ethiopia, Tel +251910980410, Email [email protected]
Background: Diabetes mellitus (DM) increases cardiovascular disease (CVD) incidence and mortality. While guidelines endorse statin use in type 2 DM (T2DM) to mitigate cardiovascular risks and mortality, challenges like statin initiation and prompt treatment adjustments affect patient outcomes. This study aimed to assess the appropriateness of indications for and dose intensification of statin therapy among T2DM patients at Tikur Anbessa Specialized Hospital (TASH).
Methodology: A hospital-based cross-sectional study was conducted from April 1 to June 30 2020. In total, 405 T2DM patients were selected using a systematic random sampling technique. The data were analyzed using SPSS version 26.0. An adjusted odds ratio (OR) was used and a 95% confidence interval (CI) and p-values of < 0.05 were utilized to determine statistical significance.
Results: Of the total 405 participants, 346 (85.4%) started taking statins for primary or secondary prevention purposes. Indication for statin use was appropriate in 96.2% patients, while for 216 (62.4%) patients their doses were appropriately intensified. Predictors of the inappropriateness of statin use were an atherosclerotic cardiovascular disease (ASCVD) score of ≥ 7.5% (AOR=0.28; 95% CI: 0.102– 0.738, p=0.01), the presence of dyslipidemia (AOR=4.48; 95% CI: 1.85– 10.84; p=0.001), initiation of aspirin therapy (AOR=3.7; 95% CI: 1.522– 9.144; p=0.004), and an LDL-cholesterol level of 70– 189 mg/dL (AOR=0.124; 95% CI: 0.042– 0.365; p=0.001). DM duration of ≥ 10 years (AOR=2.51; 95% CI: 1.35– 4.66, p=0.004), male gender (AOR=2.04; 95% CI: 1.16– 3.58, p=0.013), age ≥ 65 years (AOR=2.15; 95% CI: 1.23– 3.75, p=0.007) and uncontrolled blood pressure (AOR=2.09; 95% CI: 1.07– 4.08, p=0.031) were associated with inappropriate statin intensification.
Conclusion: The study found that indication of statins was optimal and about two-thirds of patients had their doses appropriately intensified. Monitoring is needed to avoid inappropriate intensification of statin therapy, particularly in patients with longer diabetes duration, those of male gender and advanced age, and those with uncontrolled blood pressure.
Keywords: atherosclerotic cardiovascular disease, diabetes mellitus, statin therapy
Introduction
Type 2 diabetes mellitus (T2DM) is a chronic disease characterized by hyperglycemia due to insulin resistance resulting in vascular complications. It accounts for approximately 75% of all atherosclerosis-related events.1 Moreover, 65% of patients with diabetes die from any type of cardiovascular disease or stroke. Currently, lipid-lowering statin therapy is recommended for the primary prevention of atherosclerotic cardiovascular diseases, as well as for secondary prevention in DM patients with established cardiovascular disease.2,3 The cardiovascular effects of statins extend beyond their effects on lipid fractions and include atherosclerotic plaque stabilization, anti-inflammatory effects, inhibition of vascular smooth muscle cell proliferation, inhibition of platelet function, and improved vascular endothelial function.4
Since the release of the 2013 American College of Cardiology/American Heart Association (ACC/AHA) blood cholesterol guidelines, there has been a shift from treating with a fixed LDL-C target to selecting appropriate intensity statin therapy based on individual atherosclerotic cardiovascular disease (ASCVD) risk.5 Despite current guidelines in routine clinical practice, statin intolerance and other factors may lead to treatment discontinuation, switching among statin agents, dose adjustments, or the need for augmentation of the statin regimen impacting therapeutic benefits and patient outcomes.6
The implementation of these guidelines is often poor and statin prescribing for patients with diabetes has been shown in some studies to be sub-optimal.7,8 A study in the Netherlands indicated that around 22% of T2DM patients were started on statin treatment at a dose lower than recommended and more than half of them remained on a low dose during a 2-year follow-up period; less than 15% received an increased dose.9 Another study, in the United Kingdom, showed that 43% of patients with atherosclerotic CVD discontinued their medication 1 year after initiation, and 31.5% had a mean LDL level above 2.5 mmol/L over 2 years of follow-up.10 Recent data in Ethiopia also showed utilization of statins among patients with T2D was substantially below the current clinical guideline recommendations.11 A study in Jimma also showed that about two-thirds of T2DM patients did not receive statins despite guideline recommendations.12
The increasing number of people in Ethiopia with cardiovascular disease (CVD) and the risk factors that lead to it, such as smoking, high blood pressure, and high cholesterol, requires immediate action and a modest increase in budget would be enough to make a significant difference.13 The literature shows that sub-optimal use of statins in diabetic patients, especially in individuals at high risk of cardiovascular disease, is usually the result of inappropriate dosage.2,14 However, there is limited information available about the appropriate utilization of statins in Ethiopia for primary and secondary prevention of CVD. Therefore, the purpose this study was to evaluate the appropriateness of indication for and dose intensification of statins for primary and secondary prevention of CVD in T2DM patients at TASH.
Materials and Methods
Study Setting
The study was conducted at TASH, the largest teaching hospital affiliated to Addis Ababa University College of Health Sciences. Five diabetic specialized doctors are involved in the service provided at the TASH diabetic center. The endocrinology unit in the hospital has a twice per week clinic visit schedule for patients with diabetes on regular follow-up and a weekly visit for patients with gestational DM.
Study Design and Period
The study design was a hospital-based cross-sectional study, and it was conducted from April 1 to June 30, 2020.
Eligibility Criteria
Adult T2DM patients (≥18 years) who provided consent and had follow-up in TASH during the study period were included. Pregnant diabetic patients and patients with incomplete medical charts (such as basic demographic data, diagnosis, medication history, and pertinent laboratory results) were excluded from the study.
Sample Size Determination and Sampling Technique
The sample size was determined using the single population proportion formula, whereby the population proportion (p) is typically assumed to be 50% to ensure the largest possible sample size, a Zα/2 of 1.96 is set for a 95% confidence level, and the margin of error is set at 0.05. The total calculated sample size was 422, including contingencies for potential non-response or incomplete data. A sample of T2DM cases was selected by systematic random sampling technique.
Data Collection Instruments and Techniques
A structured questionnaire was adopted from the 2018 guidelines for the management of blood cholesterol and American Diabetes Association standard of care 2018 guidelines.6,15 The questionnaire included variables such as sociodemographic characteristics, lifestyle, and disease condition. In addition, an ASCVD risk estimator and a calculator were used to calculate ASCVD score. All eligible study participants were interviewed face to face using structured questionnaire. Other necessary information such as comorbid conditions, medication history, and laboratory values were taken from medical charts. A pretested data abstraction format was used to extract all medical and treatment-related information from medical records of study participants.
Six nurses (2 MSc and 4 BSc) were recruited to collect data. Two-day training was given to the data collectors to familiarize them with the use of data collection tools, sampling techniques, methods of collecting the necessary data from patients’ charts, and ethical principles before their involvement in data collection. Then, 10% of the study population, 42 patients, was involved in pretesting the data collection tool. Participants involved in the pretest were not included in the sample used for final analysis. The principal investigator throughout the data collection period undertook continuous follow-up and the accuracy and completeness of the data were checked before entry of the data for analysis.
Data Analysis
Statin indication and dose intensification were evaluated based on the recommendations given in recent updated ADA standards of medical care in diabetes 2018.6 The ten-year ASCVD risk estimate was calculated using the ASCVD Risk Estimator Plus app. Then, the information was transferred to SPSS version 23 for Windows for analysis. Categorical variables were presented in numbers and percentages. Multicollinearity among independent variables was assessed using the variance inflation factor (VIF). A VIF exceeding 10 indicates serious multicollinearity, and a value greater than 4 may be a cause for concern. In this study, VIF result was close to one, and hence multicollinearity was not an issue. Multivariable logistic regression analysis was used to test for the presence of a significant association between the appropriateness of statin indication and intensity with independent variables. An adjusted odds ratio (AOR) was used to measure the association between dependent and independent variables at a 95% confidence interval (CI) and a p-value of <0.05 was utilized to determine the statistical significance of associations between the explanatory and dependent variables.
The inappropriate indication of statin use involves prescribing statin therapy to diabetic patients contrary to guideline recommendations, or failing to prescribe statins to patients who meet guideline criteria for treatment. Inappropriate statin dose intensification refers to failure to escalate statin therapy to that which is clinically warranted or recommended by guidelines.6
Results
Sociodemographic Characteristics
Of 422 type 2 diabetic patients interviewed, 405 were included in the final data analysis. Seventeen cases had incomplete documents, giving a response rate of 95.9%. Of 405 respondents, 222 (54.8%) were female. The mean (±SD) age of the study participants was 58 years (±10.3), ranging from 19 to 82 years. Of respondents, the majority (311, 76.8%) were married. Participants’ sociodemographic data is summarized in Table 1.
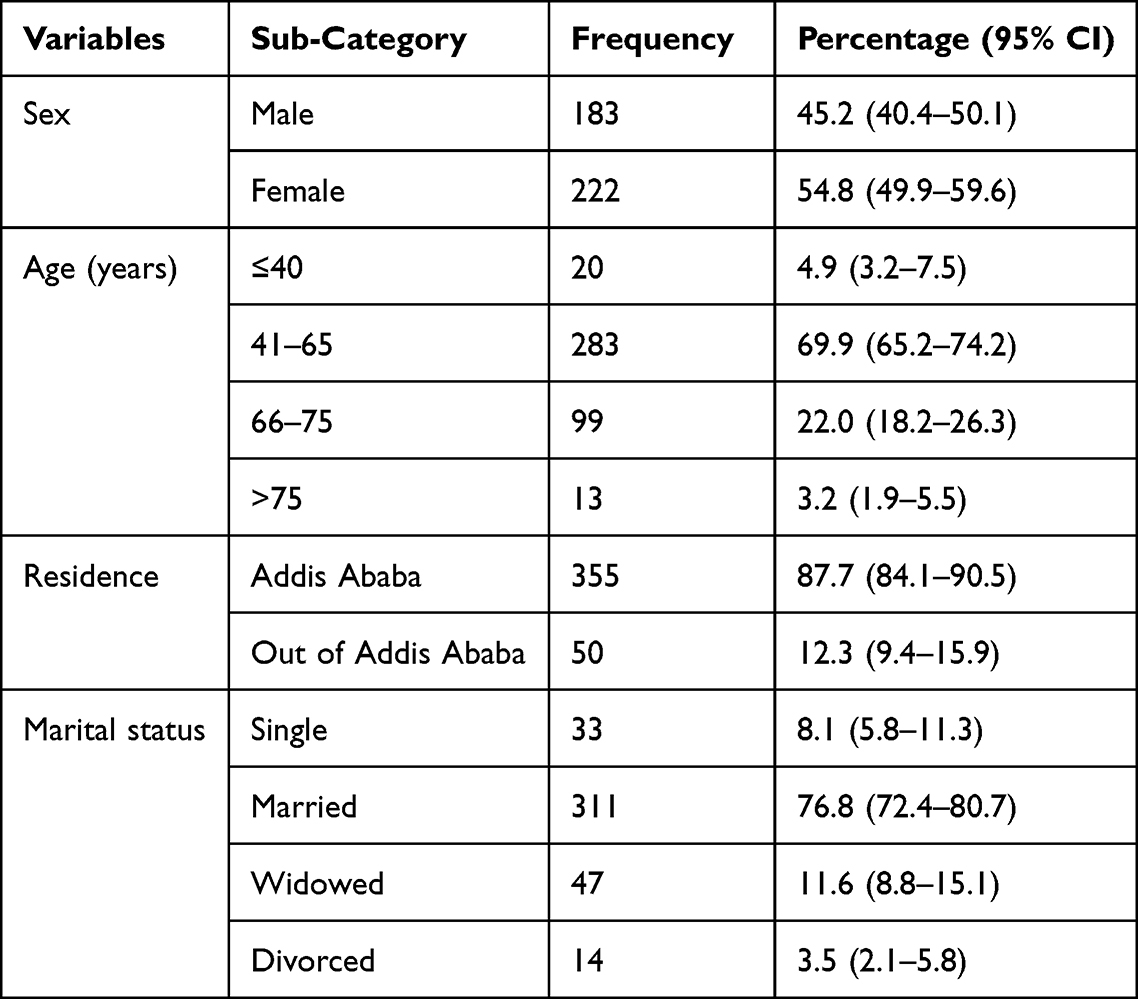 |
Table 1 Sociodemographic Characteristics Among Type 2 Diabetic Patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2019/20 (n=405) |
Lifestyle Modification
Among study subjects, 230 (56.8%) reported that they followed a diabetic diet in their daily routine. Their mean BMI was 26.4, and 249 (61.48%) patients were either overweight or obese. Nearly one-third of patients (148, 36.6%) drank alcohol now or had done so previously, and 53 (13.1%) patients smoked cigarettes (Table 2).
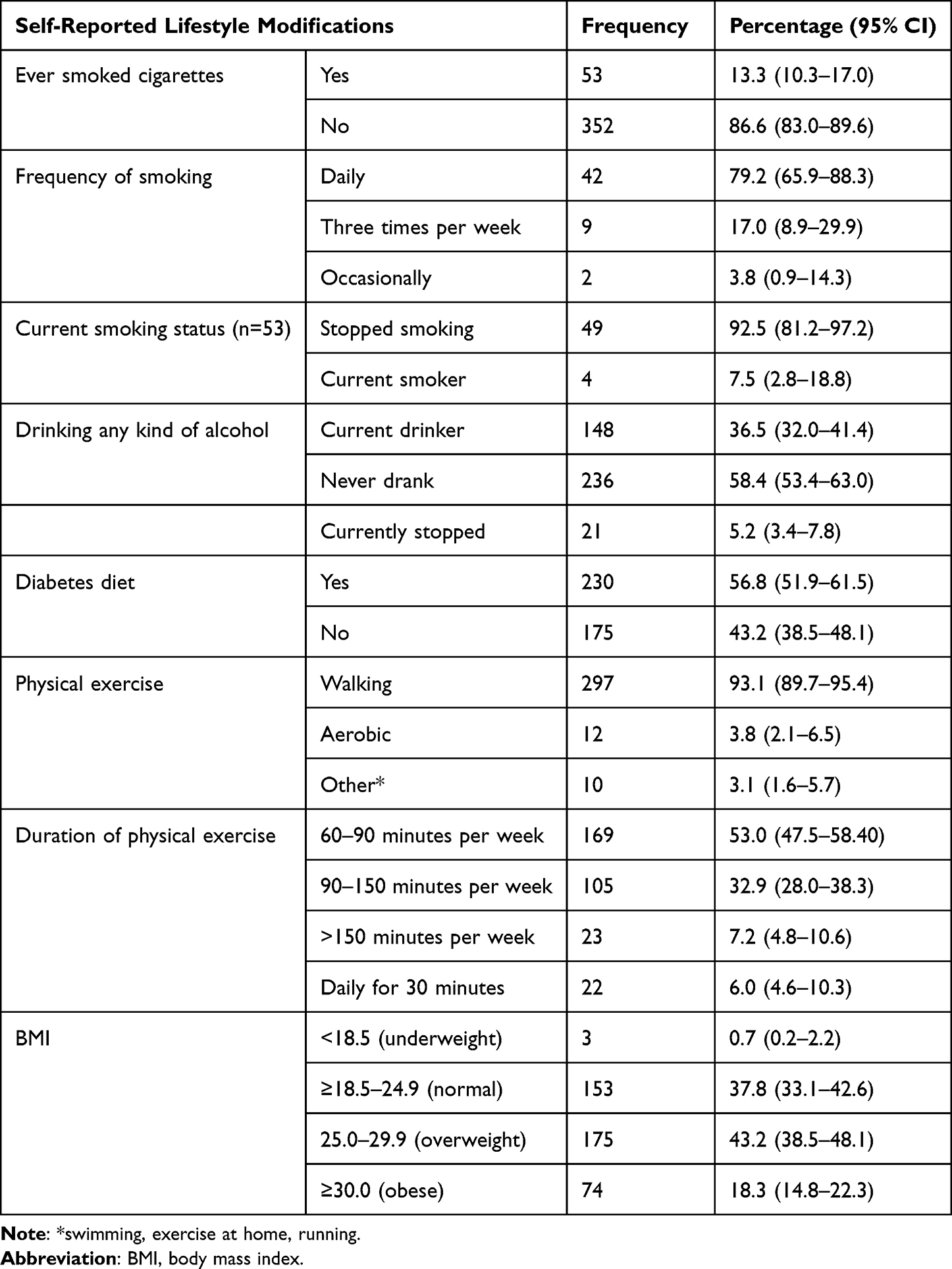 |
Table 2 Lifestyle Modification Among Type 2 Diabetic Patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2019/20 (n=405) |
Clinical Characteristics and Laboratory Values
The mean (±SD) diabetes duration since diagnosis of study participants was 12.2 (±8.0) years. More than half (59%) of participants had a diabetes duration of over ten years. The majority of participants (342, 84.4%) had comorbidities. Hypertension (69.6%) and dyslipidemia (44.2%) were the two most common comorbid conditions (Table 3).
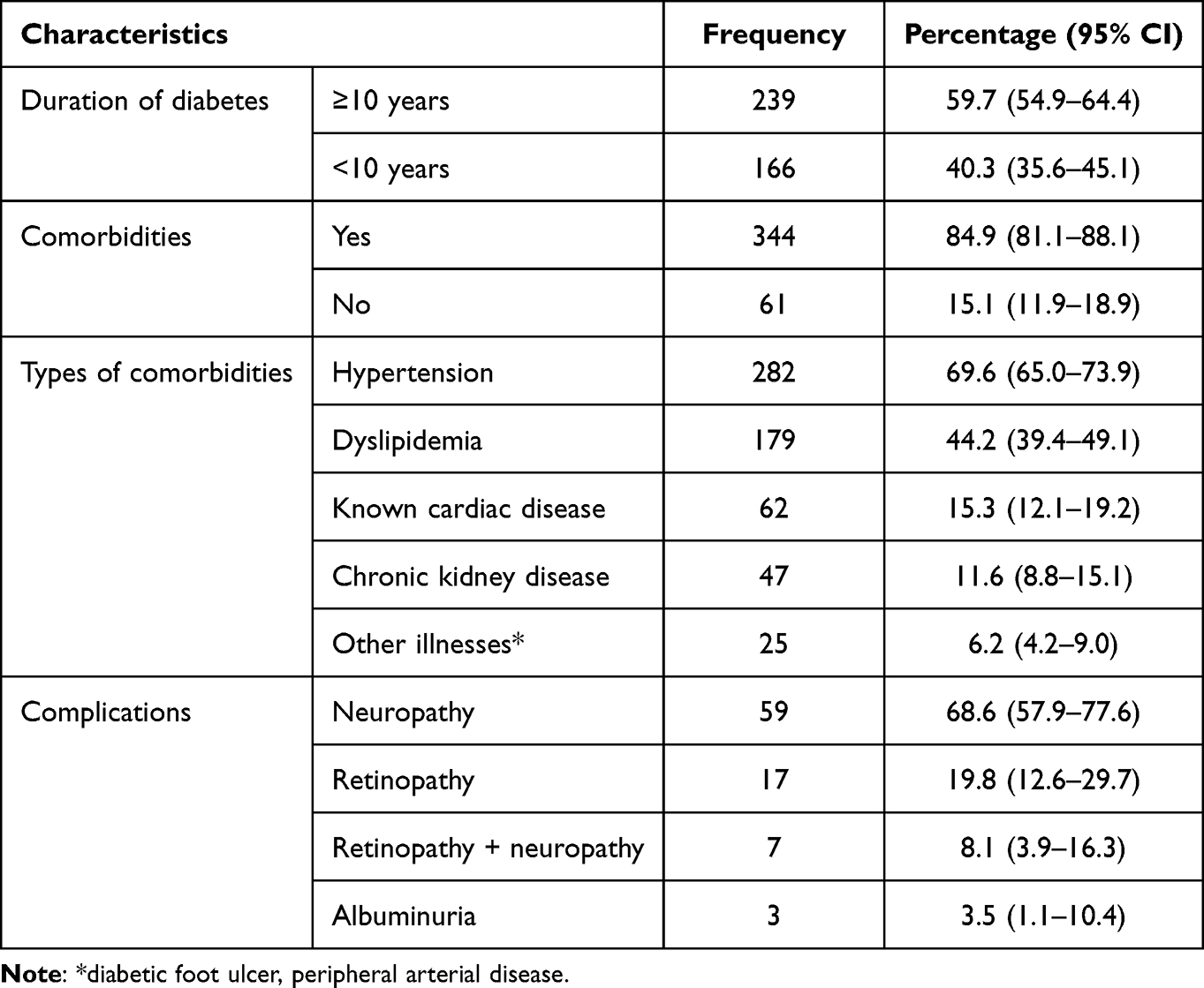 |
Table 3 Clinical Characteristics of Type 2 Diabetic Patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2019/20 (n=405) |
The total number of patients who had recent lipid profiles was 387. Among them, 52.2% did not meet the overall cholesterol target with respect to the individual patient profile. LDL-C measurement was ≥100mg/dL in 310 (50.9%) study participants.
A total cholesterol level of ≥200 mg/dL was reported in 74.4%, triglycerides of ≥150 mg/dL in 55%, HDL of ≤40 for males in 23.2%, and HDL≤50 for females in 38.5%. The proportion of type 2 diabetic patients with poor fasting glycemic control (FBS >130 mg/dL) was documented in 60.7% out of the total 405 patients. Recent HgA1c was documented for 250 patients; among these, HgA1c level was >7% in 81.6% of patients (Table 4).
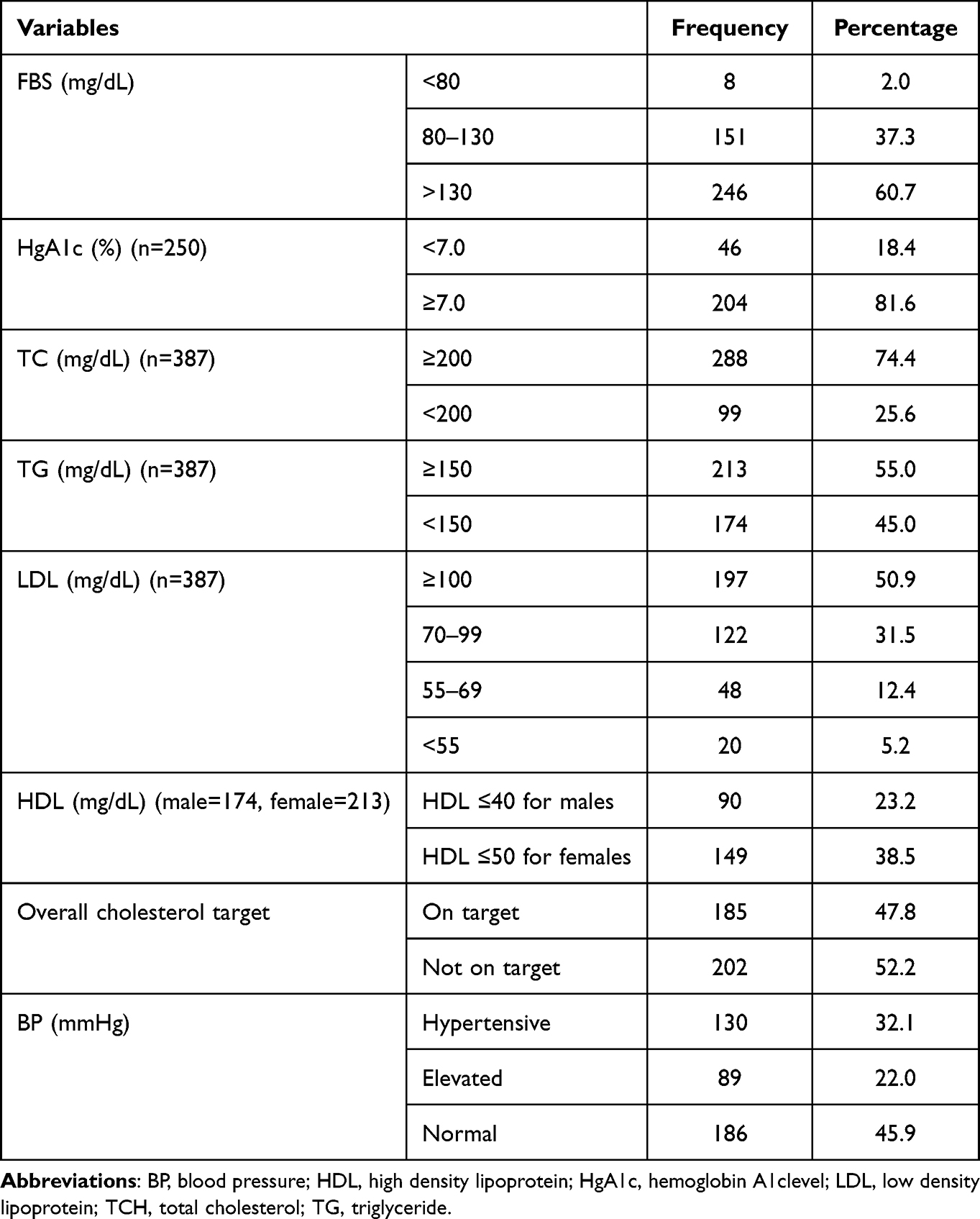 |
Table 4 Latest Laboratory Test Results of Type 2 Diabetic Patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2019/20 (n=405) |
Medication
Of all patients with T2DM, 43% took either a combination or single type of oral anti-diabetic medication, while 19.2% took insulin alone. Among statin-initiated patients, 284 (82%) received statins for primary prevention of CVD, whereas 62 (17.9%) received them for secondary prevention; that is, they had established cardiovascular diseases. The most frequently prescribed statin was atorvastatin (85.5%). Of the 346 patients who started taking statins, 52.6% were prescribed moderate-intensity statins (Table 5).
 |
Table 5 Medications Taken by Type 2 Diabetic Patients at Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2019/20 (n=405) |
ASCVD Risk Estimation for Primary Prevention
The 10-year ASCVD risk assessment was calculated using the ASCVD Risk Estimator Plus app. The calculator showed 10-year risk estimates and optimal ASCVD risk estimates for individuals 40–79 years of age; lifetime risk was calculated only for younger individuals.16
The ASCVD risk score was calculated for a total of 343 patients without a CVD. The calculator displays the 10-year ASCVD risk level, optimal risk level, and lifetime risk for each patient based on their age. Of total study participants, 86.2% had their 10-year risk of cardiovascular disease estimated. Of those, 28.7% were at low risk, 11.1% were at borderline risk, 30.4% were at intermediate risk, and 29.7% were at high risk.
Statin Indication and Dose Intensification
Of the total 405 patients, statins were initiated for 346 (85.4%). Among those on statin therapy, 333 (96.2%) had an appropriate indication for statin use, whereas 13 (3.7%) patients did not have an appropriate indication. Among the 59 T2DM patients who did not receive statin therapy, 41 (69.5%) were not prescribed statins even though they met the criteria for statin therapy. Hence, 54 (13.3%) T2DM patients, including those with no indication of statins and those requiring statins, had inappropriate indications for statin therapy.
Evaluation of guideline-directed dose intensity of statins was performed for 346 statin-initiated patients for primary or secondary prevention purposes. As a result, 216 (62.4%) patients on statins had their dose appropriately intensified. However, 130 (37.6%) patients required dose adjustment as a result of considering their cardiovascular risk profile and clinical practice guideline recommendations. Among those who required statin dose adjustment, 84 (64.6%) were taking lower than the dose recommended in the guidelines. The other 33 (25.4%) patients took a higher than recommended statin dose. The remaining 13 (10%) discontinued statin therapy after initiation.
Predictors of Appropriateness of Statin Indication
Binary logistic regression revealed that explanatory variables such as presence of comorbidity, dyslipidemia, antihypertensive drugs, ASCVD score, and ASA initiation had a significant association with indications for statin use. After adjusting confounding factors using multivariate logistic regression analysis, ASCVD score, dyslipidemia, aspirin therapy and LDL-cholesterol level were significantly associated with indications for use of statins. Patients without dyslipidemia had more than a four times (AOR=4.48; 95% CI: 1.85–10.84; p=0.001) greater chance of being on inappropriate statins icompared to their counterparts. In addition, patients who did not receive aspirin had nearly a four times (AOR=3.7; 95% CI: 1.522–9.144; p=0.004) greater chance of being on inappropriate statins than patients who received aspirin. Patients with an intermediate risk of ASCVD had a 72.5% (AOR=0.275; 95% CI: 0.102–0.738, p=0.01) lower odds of being on inappropriate statin therapy than low-risk patients. Patients with an LDL-C between 70 to 189 mg/dL had an 87.6% (AOR=0.124; 95% CI: 0.042–0.365; p=0.001) lower odds of being on inappropriate statin therapy than patients with an LDL-C of <70 mg/dL. Predictors of appropriateness of statin therapy are illustrated in Table 6.
 |
Table 6 Predictor Factors for Inappropriateness of Statin Indication in Type 2 Diabetic Patients in Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia, 2019/20 (n=405) |
Predictors of Inappropriate Statin Dose Intensification
Using multivariate logistic regression, we found that sex, age, duration of DM for at least 10 years, and current BP level were significantly associated with statin dose intensification. Male patients were twice (AOR=2.04; 95% CI: 1.16–3.58, p=0.013) as likely to have their statin dose inappropriately intensified than female DM patients. Likewise, elderly DM individuals were twice (AOR=2.15; 95% CI: 1.23–3.75, p=0.007) as likely to have their statin therapy inappropriately intensified than patients under 65 years of age. The odds of inappropriate intensification of statins in patients who had had diabetes for more than 10 years was 2.5 times (AOR=2.51; 95% CI: 1.35–4.66, p=0.004) higher than for those who were diabetic for less than ten years. In addition, patients with uncontrolled BP were about twice (AOR=2,09; 95% CI: 1.07–4.08, p=0.031) as likely to be inappropriately offered intensified statin therapy than patients with controlled BP (Table 7).
 |
Table 7 Predictor Factors for Inappropriateness of Intensification of Statins in Type 2 Diabetic Patients, Addis Ababa, Ethiopia, 2019/20 (n=346) |
Discussion
This study was the first study conducted in TASH to evaluate the appropriateness of indications for and intensification of statin therapy among patients with T2DM. The study evaluated the appropriateness and intensification of statin therapy in accordance with the American Diabetes Association (ADA) Standard Medical Care in Diabetes 2018 guideline.6 The ASCVD Risk Estimator Plus app was used to estimate cardiovascular risk.16 This guideline was selected based on physicians’ choice to practice in our setting. In addition, the guideline recommendations are updated every year to reflect the latest evidence. Cholesterol management guidelines developed by ADA and other societies also recommends statin treatment in four statin-eligible groups: those with atherosclerotic cardiovascular disease (ASCVD), diabetes, low-density lipoprotein cholesterol (LDL-C) of ≥190 mg/dL, and higher risk primary prevention. The guideline divides patients with primary prevention into low, borderline, intermediate, and high-risk categories based on the ASCVD Risk Estimator Plus. It also considers a wider range of factors, called “risk enhancers”, to inform treatment decisions.15
Initiation of statin therapy in patients with diabetes has enormous benefits, including lower risk of kidney disease and prevention of atherosclerotic cardiovascular disease (ASCVD).17 In this study, statins were initiated in 346 (85.4%) patients. Of these patients, 284 (82.8%) were receiving statins for primary prevention, while 59 (17.2%) were receiving statins for secondary prevention. Among patients who did not take statins, 41 (69.5%) were eligible for statin therapy. These results are comparable to those of a study done in Botswana, which revealed that 54.5% of type 2 diabetic patients were not on statin therapy despite being eligible for it.18 The percentage of statin-eligible diabetic patients who did not take statins in our study was higher than those in Malaysia (35.1%),19 Hong Kong (33.3%),20,21 and Saudi Arabia (27.2%).8 The difference might be due to inadequate adherence to guidelines, medication unavailability, or the high cost of medications in developing countries.18,21
ASCVD risk assessment for diabetic patients is crucial when considering treatment modification or making a decision on whether to provide statin therapy for primary prevention. The 2018 Cholesterol Clinical Practice Guidelines15,22 recommend the use of quantitative 10-year risk assessment based on measurement of ASCVD risk factors and with the use of a validated risk prediction tool. The pooled cohort equation is also widely used in countries with diverse ethnicities. This equation is more accurate than the Framingham Risk Score (FRS) at estimating cardiovascular disease (CVD) risk in black people, and this accuracy also extends to measures of subclinical vascular disease.23 The current study estimated the 10-year ASCVD risk for patients who should take statins for primary prevention (n=296) to assess whether statin intensification therapy was needed or not.22 Among those, 29.7% were at high ASCVD risk (≥20%). This result is comparable to a recent study conducted among Ghanaian and European diabetic patients, which reported that 23.7% of type 2 diabetic patients were at high risk.24 A similar result was also reported in Pakistan, whereby 20.7% (80/386) of T2DM patients were at high risk of a 10-year ASCVD event.25 Another study, in Iranian diabetic patients, comparing the 10-year ASCVD risk score according to the FRS and pooled cohort equation methods found that the mean ASCVD score was 12.39%. Though all these studies used a similar ASCVD risk calculator for estimation of 10-year ASCVD risk, they reflect the diversity of high-risk diabetic patients in terms of ethnicity, cardiovascular risk factors, sample sizes, and study designs.
Most of the available literature explored the prescribing pattern of statins and their determinants. However, there is a limited number of studies evaluating the appropriateness of statin indications and dose intensification. Among patients on statin therapy, 216 (62.42%) had appropriately intensified statin therapy, which is comparable with the results of a study done in Malaysia (71.5%).26 In contrast, a recent study in Denver reported that all patients (n=115, 100%) were prescribed an appropriate intensity of statins.27 The difference might be that the Denver study evaluated the appropriateness of statin intensification after pharmacist intervention or when pharmacists provided collaborative drug therapy management (CDTM) to improve treatment outcome and adherence to statin treatment.28 The present study did not involve clinical pharmacist interventions.
In this study, it was found that diabetic patients with normal lipid profiles were more than four times as likely to receive inappropriate statin treatment compared to patients with dyslipidemia. T2DM patients with normal lipid profiles may have been missed in terms of offering statin therapy even though they were eligible. Statins are indicated for diabetic patients without dyslipidemia, who are above the age of 40 years, have an LDL-C value of >70 mg/dL, and an ASCVD risk of >7.5%.15
In our study, the odds of inappropriate statin indication among patients with intermediate ASCVD risk (≥7.5%) was significantly reduced (by 72%) as compared to low ASCVD risk (by <5%). This is in line with guideline recommendations for indication of statins for patients with an ASCVD risk of >7.5% (6). Hence, diabetic patients at low ASCVD risk may not be started on statin therapy early, and doctors may only consider starting them after ASCVD complications have occurred. Physicians could also have played their part in this therapeutic inertia, as they were found to underestimate cardiovascular risk or fail to identify the appropriate LDL-C targets, and therefore under-treat and under-control their patients.29 Furthermore, other studies identified predictors of statin indications, such as being a former smoker, hypertension, race, and cardiovascular risk estimates were significantly associated with statin prescription.30,31
The other predictor of statin indication was LDL-C level. The odds of inappropriate indication of statin therapy among patients with an LDL-C level of 70–189 mg/dL was significantly reduced (by 88%) as compared to patients with an LDL-C level of <70 mg/dL. Similarly, evidence showed that LDL value is an important predictor for appropriate indication of statins in the United States32 and Malaysia.26
In routine clinical practice, aspirin and statins were concurrently initiated for primary prevention of CVD. The likelihood of inappropriate indication of statin therapy among patients not on aspirin was nearly four times higher than among patients on aspirin. Aspirin is known to reduce risk of atherosclerosis by inhibiting lipid biosynthesis and inflammation33 and improving vascular outcomes.34
Reports showed that after initiation of a low-dose statin upward titration or treatment intensification was uncommon in clinical practice.8,35 Similarly, in our findings patients with a 10-year or longer duration of diabetes had inappropriate statin dose intensification. It may imply that once statins are initiated in these patients, dose modification is unusual. In addition, physicians may not order routine cholesterol monitoring tests or the patient cannot afford to pay for laboratory tests. If appropriate prevention measures are not taken, longer duration of diabetes is a major risk factor for developing ASCVD.27
Furthermore, patients with uncontrolled blood pressure (≥140/90 mmHg) did not have their statin therapy appropriately intensified. Hypertension and dyslipidemia are major risk factors for CVD [3]. Hence, patients with inappropriate intensification of statin therapy and uncontrolled BP are at high risk of CVD.36 This indicates that patients should receive appropriate statin intensity to benefit from the cardio protective effects of statins. These findings strongly support guideline recommendation of individualized statin intensity according to ASCVD risk estimation or by considering other risk factors (LDL-cholesterol, hypertension, smoking). A double-blind multicenter trial also supports these findings, that is, a dose-dependent reduction of plague inflammation occurs on high intensity atorvastatin 80 mg compared to low intensity atorvastatin 10 mg.37 Another research report showed that statin therapy can reduce CVD-associated morbidity among diabetic patients by 41% and CVD incidence by 39%.14 Similarly, a prospective cohort study on Chinese patients with T2DM revealed that the use of statins was associated with a 68% reduction of risk for renal dysfunction.38
The odds of inappropriate statin dose intensification among male patients was twice as likely as compared to female patients. This might be attributed to difference in patient preferences and fear of anticipated medication side effects. In a study by Ahmed et al, it was found that, although males had a higher mean 10-year atherosclerotic cardiovascular disease risk score, they were less likely than females to receive the appropriate intensity statin because of gender disparities in statin prescribing patterns.39
The likelihood of inappropriate statin intensification among elderly patients (age ≥65 years) was twice as high than for their counterparts. This may be explained by older patients being predisposed to comorbid conditions, leading to polypharmacy and exposure to medication side effects, thus resulting in inadequate statin intensification.40
In addition to the gaps related to indications for and dose intensification of statins, the shortage of other lipid-lowering agents in low-income countries has significant consequences. Important lipid lowering agents such as ezetimibe and proprotein convertase subtilisin/kexin type 9 (PCSK9) were not available in the study setting. Limited availability and affordability of these medications contribute to low utilization rates and poor management of dyslipidemia patients.41 This leads to a high percentage of undiagnosed patients and low adherence to treatment.
The strength of this study is the novel work done with respect to ASCVD risk score in our setup. It provides an update on statin therapy indication and dose intensification practices and offers insights for understanding current challenges in CVD preventive therapy among patients with T2DM. However, it might not be possible to draw conclusions about causal relationships as the design is cross-sectional. In addition, all important laboratory results were not recorded in the electronic record system of the hospital, including HgA1c and organ function test results, at the time of data collection.
Conclusion
Overall, this study showed that the majority of T2DM patients were initiated with statins either for primary or secondary prevention of CVD. The indication of statin therapy among T2DM patients was optimal based on guideline recommendations. However, among statin-initiated patients about two-thirds had their dosage appropriately intensified. The study also found that ASCVD score, dyslipidemia, aspirin therapy, and LDL-cholesterol level were the predictors for indication of statin therapy, whereas patients with longer diabetic duration (≥10 years), male patients, elderly patients and patients with uncontrolled BP were found to be predictors of inappropriate intensification of statins. Optimal initiation of statin therapy in type 2 diabetes mellitus patients aligns with guideline recommendations. However, vigilance is needed to avoid inappropriate intensification of statin therapy, particularly in patients with longer diabetes duration, male gender, advanced age, and uncontrolled blood pressure.
Abbreviations
ADA, American Diabetes Association; ASCVD, atherosclerotic cardiovascular disease; FRS, Framingham Risk Score; LDL-C, low density cholesterol; TASH, Tikur Anbessa Specialized Hospital; T2DM, type 2 diabetes mellitus.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Considerations
Ethical approval was obtained from Addis Ababa University, School of Pharmacy Ethical Review Committee (Ref No.: ERB/SOP/200/01/2020), and permission to conduct the study was also obtained from the hospital medical director. Only numerical identifiers were used as a reference. Not recording identifying details, such as name or any other personal identifiers, maintained the confidentiality and anonymity of study participants. No patient names, healthcare providers, or drug products were disclosed. Consent was obtained from the study participants. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We are grateful to the Tikur Anbessa Specialized Hospital for allowing access to its medical records. We acknowledge study participants and data collectors for their time.
Author Contributions
All authors made considerable contributions to conception and design, acquisition of data, or analysis and interpretation of data; were involved in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There was no funding source for this study; data collection fees were covered by the authors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Farmer JA. Diabetic dyslipidemia and atherosclerosis: evidence from clinical trials. Curr Diabetes Rep. 2008;8(1):71–77. doi:10.1007/s11892-008-0013-2
2. De Vries FM, Denig P, Pouwels KB, Postma MJ, Hak E. Primary prevention of major cardiovascular and cerebrovascular events with statins in diabetic patients: a meta-analysis. Drugs. 2012;72(18):2365–2373. doi:10.2165/11638240-000000000-00000
3. Kurihara O, Thondapu V, Kim HO, et al. Comparison of vascular response to statin therapy in patients with versus without diabetes mellitus. Am j Cardiol. 2019;123(10):1559–1564. doi:10.1016/j.amjcard.2019.02.020
4. Almeida SO, Budoff M. Effect of statins on atherosclerotic plaque. Trend Cardiovasc Med. 2019;29(8):451–455. doi:10.1016/j.tcm.2019.01.001
5. Bavishi A, Howard T, Kim JP, et al. Treatment gap in primary prevention patients presenting with acute coronary syndrome. Am J Cardiol. 2019;123(3):368–374. doi:10.1016/j.amjcard.2018.10.034
6. Care I Standards of medical care in diabetes—2018 Abridged for primary care providers; 2018.
7. Ofori SN, Odia OJ. Risk assessment in the prevention of cardiovascular disease in low-resource settings. Indian Heart J. 2016;68(3):391–398. doi:10.1016/j.ihj.2015.07.004
8. Alkhail BA, Iftikhar R, Al Shaikh A. Use of aspirin and statin as primary prevention for cardiovascular diseases. Pak J Med Sci. 2016;32(6):1336. doi:10.12669/pjms.326.10615
9. de Vries FM, Voorham J, Hak E, Denig P. Prescribing patterns, adherence and LDL‐cholesterol response of type 2 diabetes patients initiating statin on low‐dose versus standard‐dose treatment: a descriptive study. Int J Clin Pract. 2016;70(6):482–492. doi:10.1111/ijcp.12806
10. Danese MD, Gleeson M, Kutikova L, et al. Management of lipid-lowering therapy in patients with cardiovascular events in the UK: a retrospective cohort study. BMJ open. 2017;7(5):e013851. doi:10.1136/bmjopen-2016-013851
11. Demoz GT, Wahdey S, Kasahun GG, et al. Prescribing pattern of statins for primary prevention of cardiovascular diseases in patients with type 2 diabetes: insights from Ethiopia. BMC Res Notes. 2019;12(1):1–7. doi:10.1186/s13104-019-4423-9
12. Melaku T, Solomon Y, Chelkeba L. Statin utilization patterns among Type 2 diabetes mellitus patients with high cardiovascular disease risks in Ethiopia. J Pharm Care. 2018;3:44–51.
13. Tolla MT, Norheim OF, Memirie ST, et al. Prevention and treatment of cardiovascular disease in Ethiopia: a cost-effectiveness analysis. Cost Eff Resour Allocation. 2016;14(1):1–14. doi:10.1186/s12962-016-0059-y
14. Katsiki N, Athyros VG, Karagiannis A, Mikhailidis DP. The role of statins in the treatment of type 2 diabetes mellitus: an update. Curr Pharm Des. 2014;20(22):3665–3674. doi:10.2174/13816128113196660673
15. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2019;73(24):3168–3209. doi:10.1016/j.jacc.2018.11.002
16. Lloyd-Jones DM, Braun LT, Ndumele CE, et al. Use of risk assessment tools to guide decision-making in the primary prevention of atherosclerotic cardiovascular disease: a special report from the American Heart Association and American College of Cardiology. Circulation. 2019;139(25):e1162–e1177. doi:10.1161/CIR.0000000000000638
17. Zhou S, Nie S, Xin X. # 4326 Statin initiation and risk of incident kidney disease in patients with diabetes. Nephrol Dial Transplant. 2023;38(Supplement_1):
18. Mwita JC, Godman B, Esterhuizen TM. Statin prescription among patients with type 2 diabetes in Botswana: findings and implications. BMC Endocr Disord. 2020;20(1):1–9. doi:10.1186/s12902-020-0516-7
19. Elnaem MH, Mohamed MHN, Huri HZ, Azarisman SM, Elkalmi RM. Statin therapy prescribing for patients with type 2 diabetes mellitus: a review of current evidence and challenges. J Pharm Bioallied Sci. 2017;9(2):80. doi:10.4103/jpbs.JPBS_30_17
20. Lee VW, Ho IC, Chan WS, Tam KY, Lee KK. Statin utilization patterns for the primary prevention of cardiovascular events: a retrospective study in patients with diabetes mellitus in Hong Kong. Am J Cardiovasc Drugs. 2008;8(3):199–205. doi:10.2165/00129784-200808030-00006
21. Sobngwi E, Ndour-Mbaye M, Boateng KA, et al. Type 2 diabetes control and complications in specialised diabetes care centres of six sub-Saharan African countries: the Diabcare Africa study. Diabetes Res Clin Pract. 2012;95(1):30–36. doi:10.1016/j.diabres.2011.10.018
22. Preiss D, Kristensen SL. The new pooled cohort equations risk calculator. Cana J Cardiol. 2015;31(5):613–619. doi:10.1016/j.cjca.2015.02.001
23. Topel ML, Shen J, Morris AA, et al. Comparisons of the Framingham and pooled cohort equation risk scores for detecting subclinical vascular disease in blacks versus whites. Am j Cardiol. 2018;121(5):564–569. doi:10.1016/j.amjcard.2017.11.031
24. Boateng D, Agyemang C, Beune E, et al. Cardiovascular disease risk prediction in sub-Saharan African populations—Comparative analysis of risk algorithms in the RODAM study. Int J Cardiol. 2018;254:310–315. doi:10.1016/j.ijcard.2017.11.082
25. Ashraf T, Mengal MN, Muhammad AS, et al. Ten years risk assessment of atherosclerotic cardiovascular disease using Astro-CHARM and pooled cohort equation in a south Asian sub-population. BMC Public Health. 2020;20(1):1–6. doi:10.1186/s12889-020-08472-4
26. Elnaem MH, Mohamed MHN, Huri HZ, Shah ASM. Effectiveness and prescription pattern of lipid-lowering therapy and its associated factors among patients with type 2 diabetes mellitus in Malaysian primary care settings. Ther Clin Risk Manage. 2019;15:137–145. doi:10.2147/TCRM.S182716
27. Shah AS, Dolan LM, Kimball TR, et al. Influence of duration of diabetes, glycemic control, and traditional cardiovascular risk factors on early atherosclerotic vascular changes in adolescents and young adults with type 2 diabetes mellitus. J Clin Endocrinol Metab. 2009;94(10):3740–3745. doi:10.1210/jc.2008-2039
28. Elkomos M, Jahromi R, Kelly MS. Pharmacist-led programs to increase statin prescribing: a narrative review of the literature. Pharmacy. 2022;10(1):13. doi:10.3390/pharmacy10010013
29. Morieri ML, Lamacchia O, Manzato E, Giaccari A, Avogaro A. Physicians’ misperceived cardiovascular risk and therapeutic inertia as determinants of low LDL-cholesterol targets achievement in diabetes. Cardiovasc Diabetol. 2022;21(1):57. doi:10.1186/s12933-022-01495-8
30. Berthold HK, Gouni-Berthold I, Böhm M, Krone W, Bestehorn KP. Patterns and predictors of statin prescription in patients with type 2 diabetes. Cardiovasc Diabetol. 2009;8(1):1–12. doi:10.1186/1475-2840-8-25
31. Pauff BR, Jiroutek MR, Holland MA, Sutton BS. Statin prescribing patterns: an analysis of data from patients with diabetes in the national hospital ambulatory medical care survey outpatient department and national ambulatory medical care survey databases, 2005–2010. Clin. Ther. 2015;37(6):1329–1339. doi:10.1016/j.clinthera.2015.03.020
32. Karmali KN, Lee J-Y, Brown T, Persell SD. Predictors of cholesterol treatment discussions and statin prescribing for primary cardiovascular disease prevention in community health centers. Preventive Med. 2016;88:176–181. doi:10.1016/j.ypmed.2016.04.011
33. Han Y-M, Lee Y-J, Jang Y-N, et al. Aspirin Improves Nonalcoholic Fatty Liver Disease and Atherosclerosis through Regulation of the PPARδ-AMPK-PGC-1α Pathway in Dyslipidemic Conditions. Biomed Res. Int. 2020;2020:1–17. doi:10.1155/2020/7806860
34. Frisbee JC, Goodwill AG, Stapleton PA, Frisbee SJ, d’Audiffret AC. Aspirin resistance with genetic dyslipidemia: contribution of vascular thromboxane generation. Physiol Genom. 2010;42(3):331–341. doi:10.1152/physiolgenomics.00090.2010
35. Simpson RJ, Tunceli K, Ramey DR, et al. Treatment pattern changes in high-risk patients newly initiated on statin monotherapy in a managed care setting. J Clin Lipidol. 2013;7(5):399–407. doi:10.1016/j.jacl.2013.06.002
36. Iskandar MF, Nurmainah N, Susanti R. The risk of atherosclerotic cardiovascular disease among hyperlipidaemia patients and appropriateness of statin therapy. Pharmacol Clin Pharm Res. 2018;3(1). doi:10.15416/pcpr.v3i1.16452
37. Tawakol A, Fayad ZA, Mogg R, et al. Intensification of statin therapy results in a rapid reduction in atherosclerotic inflammation: results of a multicenter fluorodeoxyglucose-positron emission tomography/computed tomography feasibility study. J Am Coll Cardiol. 2013;62(10):909–917. doi:10.1016/j.jacc.2013.04.066
38. Ting RZ, Yang X, Yu LW, et al. Lipid control and use of lipid-regulating drugs for prevention of cardiovascular events in Chinese type 2 diabetic patients: a prospective cohort study. Cardiovasc Diabetol. 2010;9(1):1–9. doi:10.1186/1475-2840-9-77
39. Ahmed F, Lin J, Ahmed T, Siddiqui D, Nguyen J, Sarpong D. Health disparities: statin prescribing patterns among patients with diabetes in a family medicine clinic. Health Equity. 2022;6(1):291–297. doi:10.1089/heq.2021.0144
40. Alwhaibi M, Alkofide H. Potentially inappropriate medications use among older adults with dyslipidaemia. J Clin Med. 2023;12(12):4063. doi:10.3390/jcm12124063
41. Kalinić D, Škrbić R, Vulić D, et al. Eleven-year trends in lipid-modifying medicines utilisation and expenditure in a low-income country: a study from the republic of Srpska, Bosnia and Herzegovina. Clinicoecon Outcomes Res. 2023;15:513–523. doi:10.2147/CEOR.S410711
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Urinary Albumin Creatinine Ratio on Cardiovascular Morbidity and Mortality in Diabetes Patients with Atherosclerotic Disease
Gao F, Zhou Y, Yan X, Huang H, Liang G, Xie Y, Zhu Q, Chen Z, Wang B, Li H, Mai Z, Ying M, Liu J, Chen S, Chen J
Diabetes, Metabolic Syndrome and Obesity 2023, 16:819-828
Published Date: 17 March 2023
Impact of Acute Kidney Injury, Co-Existing with and without Chronic Kidney Disease on the Short‐Term Adverse Outcomes Following Atherosclerotic Cardiovascular Disease Events in Patients with Diabetes
Chou CL, Zheng CM, Chiu HW, Tsou LLC, Kao PF, Hsu YH, Lin CL, Sung LC
Journal of Multidisciplinary Healthcare 2025, 18:2019-2037
Published Date: 12 April 2025
Hs-CRP, Diabetic Status, and Adverse Events Among Patients Receiving Statin Therapy Following PCI—A Prospective Registry-Based Study
Chen X, Wang HY, Sun W, Lin Z, Qiao Z, Bian X, Yin D, Feng L, Zhu C, Song W, Wang H, Jia L, Dong Q, Dou K
Journal of Inflammation Research 2025, 18:9261-9274
Published Date: 15 July 2025