Back to Journals » Infection and Drug Resistance » Volume 17
Evaluation of MeltPro Assay in Identification of Second-Line Injectable Drug Resistance in Multidrug-Resistant Tuberculosis Isolates
Authors Hu Y, Yu M, You G, Fan J, Zheng H ![]()
Received 22 February 2024
Accepted for publication 15 May 2024
Published 24 May 2024 Volume 2024:17 Pages 2069—2076
DOI https://doi.org/10.2147/IDR.S459142
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yan Hu,1 Min Yu,1 Guoqing You,1 Jun Fan,1 Huiwen Zheng2
1Tuberculosis Reference Laboratory, Chongqing Tuberculosis Control Institute, Chongqing, People’s Republic of China; 2Laboratory of Respiratory Diseases, Beijing Key Laboratory of Pediatric Respiratory Infection Diseases, Beijing Pediatric Research Institute, Beijing Children’s Hospital, Capital Medical University, Key Laboratory of Major Diseases in Children, Ministry of Education, National Clinical Research Center for Respiratory Diseases, National Center for Children’s Health, Beijing, People’s Republic of China
Correspondence: Jun Fan; Huiwen Zheng, Email [email protected]; [email protected]
Objective: We compared the MeltPro assay to whole-genome sequencing (WGS) to investigate the molecular characterization of second-line injectable drug (SLID) resistance in multidrug-resistant tuberculosis (MDR-TB) isolates in Chongqing, China.
Methods: A total of 122 MDR-TB patient isolates were collected between March 2019 and June 2020 from Chongqing Municipality, China. Conventional drug-susceptibility testing was performed using the proportion method, followed to generate minimum inhibitory concentrations (MICs) of SLIDs determined by microplate alamarblue assay. All strains were subjected to both MeltPro and WGS assays.
Results: Among 122 MDR-TB isolates, 30 (24.6%), 22 (18.0%), and 14 (11.5%) were resistant to kanamycin (KM), amikacin (AM), and capreomycin (CM), respectively. Of the 31 SLID-resistant isolates, 24 (77.4%, 24/31) isolates harbored mutations in the rrs gene, with the most prevalent mutations in rrs A1401G (22/24, 91.7%). Mutation in rrs A1401G was associated with high levels of resistance to KM (MIC, ≥ 40 μg/mL) and AM (MIC, ≥ 64 μg/mL), but disparities in CM-resistance levels. Using phenotypic drug-susceptibility testing as gold standard, we found that the overall sensitivity of MeltPro and WGS was 87.1% and 90.32% and specificity 100% and 97.8%, respectively. Seven isolates had discordant results between phenotypic and genotypic resistance of SLIDs.
Conclusion: MeltPro is a promising diagnostic tool for accurate identification of SLID-resistant MTB isolates with mutations in the rrs and eis genes. There was a disparity between MeltPro with WGS results in the proportion of heterogeneous drug-resistant bacteria with rrs mutation and limited probes. Resistance mechanisms other than genetic mutations will affect the consistency of MeltPro and WGS with phenotypic drug-susceptibility results.
Keywords: MDR, MeltPro, resistance, genotype
Introduction
The prevalence of multidrug-resistant tuberculosis (MDR-TB), with an estimated of 0.41 million new cases in 2022, poses significant challenges to the prevention and control of TB disease globally.1 MDR-TB patients are difficult to treat, and the treatment success rate was only 60% in 2021.1 China has the second-greatest number of MDR-TB cases in the world, and the treatment success rate is only 54%.2
Effective anti-TB medications are essential for the treatment of MDR-TB. All-oral drugs are recommended in place of second-line injectable drugs (SLIDs), with the exception of amikacin due to several adverse events, for longer MDR-TB treatment in a 2018 guideline issued by the World Health Organization (WHO).3 Though the role of SLIDs has weakened, they should be considered as an alternative treatment when patients have limited access to all-oral drugs or have severe adverse reactions, such as with bedaquiline (BDQ). There is limited access to BDQ due to its high price in many countries, including China, and intolerance to BDQ in many patients.4 SLIDs are still emphasized as core drug treatment in standard short-course chemotherapy regimens, and they can prevent bacterial resistance to the core drug, thus providing the most effective protection.5,6 Second-line injections have been used in China for many years and play a certain role in the treatment of MDR-TB, so they are still in mainstream use.
The diagnosis of drug-resistant TB by phenotypic drug-susceptibility testing (DST) is lengthy, laborious, and expensive.7 As such, reliable and automated molecular assays are recommended by the WHO for detecting resistance to first-line and second-line drugs.8 The MeltPro TB assay developed by Zeesan Biotech (Xiamen, China) is an innovative molecular test for detection of resistance to SLIDs. It is based on melting curve analysis with dual-labeled, self-quenched probes to detect multiple mutations in a single reaction, making it flexible and sensitive for use for clinical practice.9 MeltPro TB assays for detecting rifampin (RIF), isoniazid (INH), and fluoroquinolone resistance have been officially approved by the China Food and Drug Administration for diagnostic purposes in clinical settings. In addition, whole-genome sequencing (WGS) approaches have the potential to identify various genetic polymorphisms and predict drug-resistance profiles, and are used to evaluate sequencing technologies for routine genotypic DST.10,11 In this study, we compared the MeltPro assay with WGS to investigate the molecular characterization of SLID resistance in MDR-TB isolates in Chongqing, the largest municipality in southwest China and which has a high incidence of TB.
Methods
Bacterial Strains
Simple randomized sampling was used to obtain a representative sample of patients with TB. A total of 122 MDR-TB patient isolates were collected between March 2019 and June 2020 from Chongqing Municipality, China. All isolates were subcultured on Löwenstein–Jensen medium for 4 weeks at 37°C. Demographic and clinical characteristics were obtained from the electronic recording and reporting system for TB in China.
Conventional Drug-Susceptibility Testing
Conventional DST using the 1% proportion method as per WHO guidelines12 was performed with the following drug concentrations: RIF (40 μg/mL), INH (0.2 μg/mL), streptomycin (10 μg/mL), ethambutol (2 μg/mL), capreomycin (CM, 40 μg/mL), kanamycin (KM, 30 μg/mL), amikacin (AM, 30 μg/mL), levofloxacin (2 μg/mL), protionamide (40 μg/mL) and p-aminosalicylic acid (1 μg/mL). The MDR-TB was defined as resistance to at least INH and RIF. SLID resistance was defined as resistance to any of AM, CM, and KM.
Minimum Inhibitory Concentrations
The minimum inhibitory concentrations (MICs) of SLIDs were determined using broth microdilution in accordance with the guidelines of the Clinical and Laboratory Standards Institute.13 The breakpoint concentrations were defined as 1 μg/mL for AM and 2.5 μg/mL for KM and CM.14 Mycobacterium tuberculosis H37Rv (ATCC 27249) was used as the control strain. The MIC was defined as the lowest concentration of antibiotic that inhibited visible growth of mycobacteria.
MeltPro Assay
Genomic DNA was extracted from culture-positive M. tuberculosis isolates using the cetyltrimethylammonium bromide method, as previously reported.15 A MeltPro M. tuberculosis SLID-resistance mutation test kit (Zeesan, Xiamen, China) was used within the SLAN-96S system (Hongshi, Shanghai, China). The results were automatically exported by SLAN software (Zeesan). Mutation types, drug-resistance patterns, and the interpretation of results are shown in Supplementary Table 1.
Whole-Genome Sequencing
Extracted genomic DNA was quantified using a Qubit 2.0 Fluorometer (Thermo Fisher Scientific). Genomic DNA libraries were constructed using an Illumina Nextera kit according to the manufacturer’s protocol. All whole-genome sequencing procedures were performed by Annoroad Gene Technology (Beijing, China) on an Illumina HiSeq 2500 (Illumina, San Diego, CA) sequencing platform with a mean depth of coverage >100×. The sequencing reads were aligned with the H37Rv reference genome (GenBank ID NC_000962.3) to analyze the variant calls for drug resistance.
Statistical Analysis
Pearson’s χ2 or Fisher’s exact test was used to compare proportions or resistant rates. P<0.05 was considered statistically significant. Sensitivity, specificity, positive predictive value, and negative predictive value were calculated at the 95% CI, while concordance between two methods was assessed with κ tests. All statistical analyses were performed in SPSS 20.0 (IBM, Armonk, NY).
Results
Demographic Characteristics of SLID-Resistant MDR Isolates
Of the 122 MDR patients, 68.9% (84/122) were male, 64.8% (79/122) were retreated cases, 38.5% (47/122) had lung cavitation, and 4.1% (5/122) had diabetes. The predominant genotype was lineage 2 (86.1%, 105/122). Of the 31 (25.4%) SLID-resistant isolates, cases with treatment history (77.4%) were more common than new cases (2.6%). The resistance rate of levofloxacin and p-aminosalicylic acid in patients resistant to SLIDs was higher than in patients susceptible to SLIDs (77.4% vs 35.2%, 25.8% vs 5.5%, respectively; P <0.05; Table 1).
 |
Table 1 Characteristics of SLIDsR and SLIDsS MDR isolates (n=122) |
Second-Line Injectable Drug–Resistance Profile
Phenotypic DST showed that among 122 MDR isolates, 30 (24.6%), 22 (18.0%), and 14 (11.5%) were resistant to KM, AM, and CM, respectively. Of the 31 (25.5%) SLID-resistant isolates, 13 (41.9%) isolates showed cross-resistance to KM, AM, and CM, with 12 (92.3%) isolates harboring the rrs A1401G mutation and one (7.7%) rrs G1484T + rrs A1401G on WGS. Nine (29.0%) isolates were cross-resistant to AM and KM and carried the rrs A1401G mutation. Only one (3.2%) isolate showed resistance to CM (Figure 1).
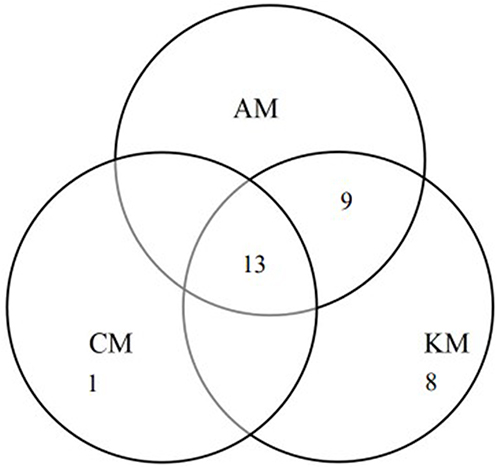 |
Figure 1 Cross-resistance of MDR against SLIDs. |
Of the 31 SLID-resistant isolates, 24 (77.4%, 24/31) isolates harbored mutations in the rrs gene, with the most prevalent mutations being rrs A1401G (22/24, 91.7%), followed by rrs G1484T (1/24, 4.2%) and rrs A1401G + rrs G1484T (1/24, 4.2%), while 95.5% (21/22) and 78.6% (11/14) of isolates with the rrs A1401G mutation were observed in AM- and CM-resistant isolates, respectively. The one isolate (3.2%) of rrs A1401G + rrs G1484T was associated with KM, AM, and CM resistance, and one isolate (3.2%) with rrs G1484T showed resistance only to KM (Figure 2).
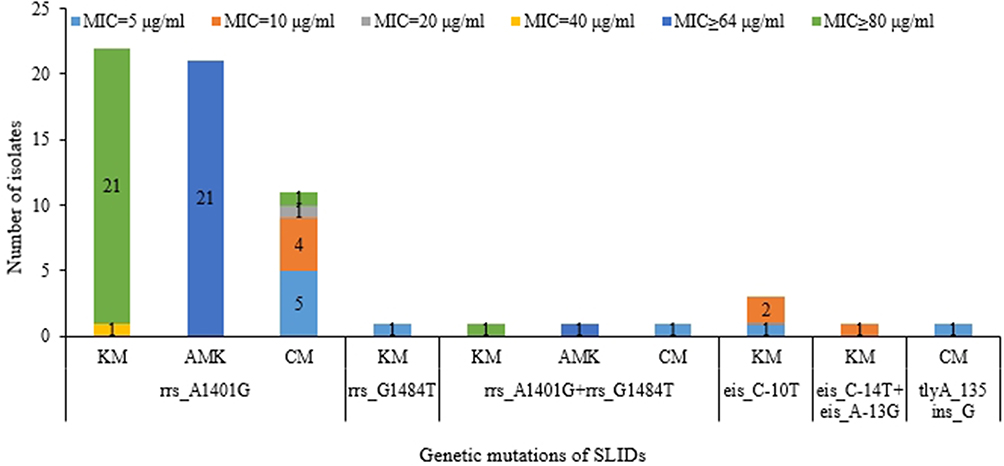 |
Figure 2 Association of MICs and genetic mutations of SLIDs (KM, kanamycin; AM, amikacin; CM, capreomycin) resistance in MDR isolates. |
Association of MICs and Genetic Mutations
Three isolates (10%) with eis C–10T were associated with a low level of resistance (MIC <10 μg/mL) to KM, and 22 (73.3%) isolates harboring the rrs A1401G mutation showed high levels of resistance (MIC ≥40 μg/mL). The rrs A1401G mutation was associated with high levels of resistance to AM (MIC ≥64 μg/mL), but there were disparities in CM resistance. The one isolate with rrs A1401G + rrs G1484T showed a high level of resistance to KM and AM, but a low level of resistance to CM. The one isolate with tlyA 135 ins_G (MIC=5 μg/mL) was resistant only to CM, but at a low level (MIC ≤10 μg/mL; Figure 2).
Comparing MeltPro and WGS in Phenotypic DST
Using phenotypic DST as gold standard, of the 31 SLIDs-resistant isolates, 27 were correctly identified by MeltPro with sensitivity of 87.1%, and 28 isolates were correctly identified by WGS with sensitivity of 90.32%. The overall specificity of MeltPro and WGS was 100% and 97.8%, respectively. There was excellent agreement between these two methods and phenotypic DST (κ≥0.85; Table 2). In terms of SLID resistance detected by MeltPro and WGS, two isolates with phenotypic susceptibility to SLIDs were identified on MeltPro, and two mutations within the tlyA gene were detected on WGS: one 590 del_T (35.37%) and the other 394 ins_A (95.38%). Five isolates showing phenotypic resistance were identified as SLID-sensitive by MeltPro or WGS. Two isolates identified as SLID-susceptible by MeltPro showed phenotypic resistance, and WGS analysis indicated that one isolate harbored the rrs A1401G mutation (24.65%) and the other tlyA 135 ins_G (94.76%). One phenotypically SLID-resistant isolate was predicted to be resistant by MeltPro with eis C-14T/eis A-13G/eis G-10A mutations, but was identified as sensitive by WGS. Two phenotypically SLID-resistant isolates were identified as sensitive by MeltPro and WGS (Table 3).
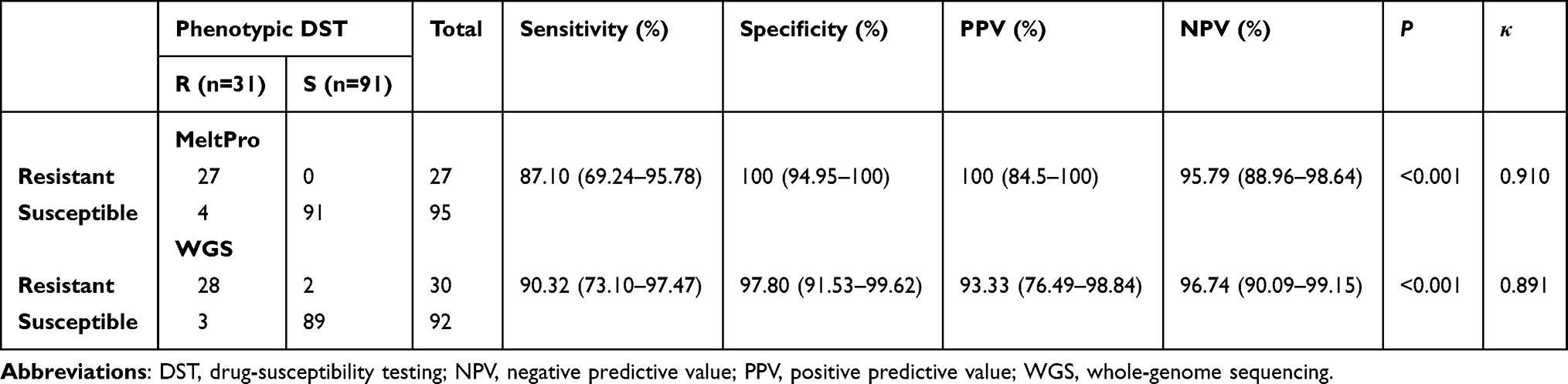 |
Table 2 Comparision of MeltPro and WGS for Detecting SLIDs Resistance |
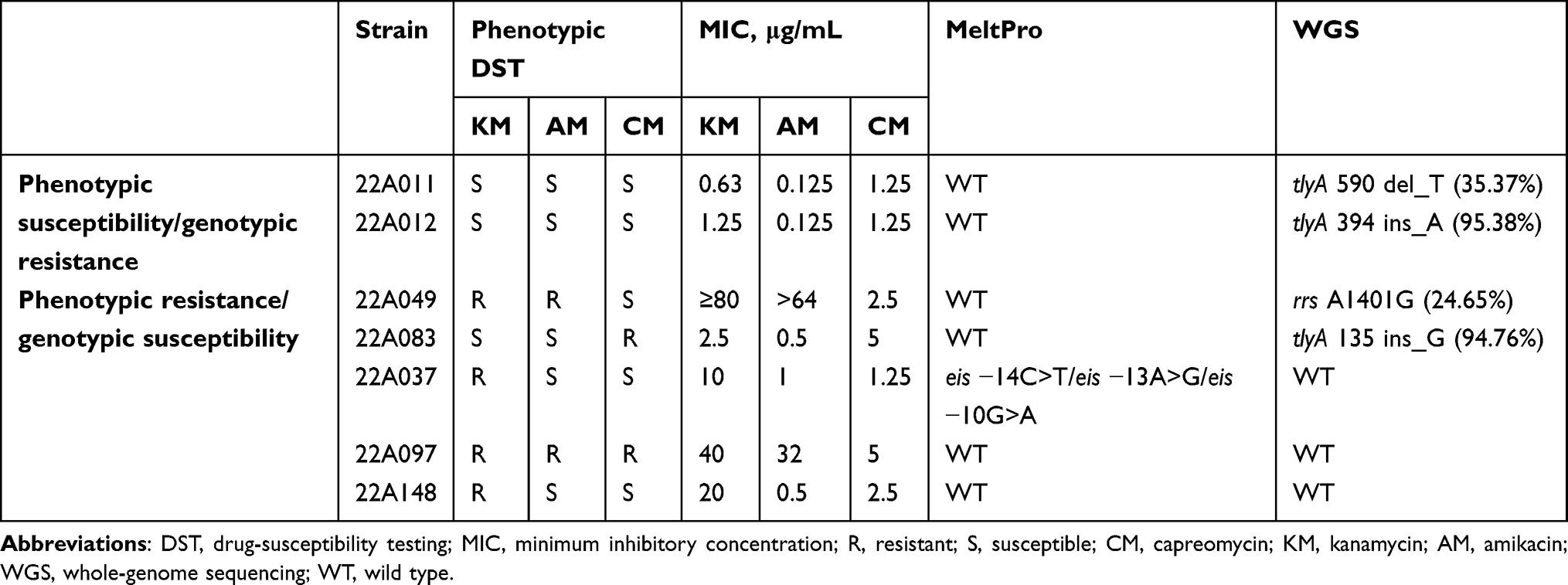 |
Table 3 Analysis on Discordant results between phenotypic and genotypic methods for SLID resistance |
Discussion
As it will take time to transition to all-oral regimens, SLIDs remain in use,16 so there will be a period with the injection and oral regimen coexistence. Molecular tests for rapid TB drug-resistance detection have become increasingly popular. In the present study, we assessed the diagnostic accuracy of MeltPro with WGS assays for SLID resistance among MDR-TB patients.
This study showed that 25.4% MDR-TB patients had resistance to at least one SLID, slightly higher than another report (17.3%) in Chongqing,17 which may be attributed to medication history and the diversity in TB epidemiology. In the present study, the most frequent mutation was rrs A1401G (77.4%) in SLID-resistant isolates, which was higher than Chinese Center for Disease Control and Prevention (40.7%)18 and Hebei (33.3%) figures.19 This phenomenon was principally due to the differences in sequencing methods, as WGS showed an obvious advantage of improved sensitivity over Sanger sequencing. We found that the A1401G mutation was present in 73.3% of KM-resistant, 78.6% of CM resistant and 95.5% of AM-resistant isolates, and the mutation-prevalence trend was consistent with a previous report.18,20 In accordance with previous research,21,22 the rrs A1401G mutation was associated with a high level of resistance to KM and AM, while CM showed different levels of resistance. In our study, 92.3% of isolates carried the A1401G mutation, contributing to cross-resistance and indicating that rrs might serve as a marker to predict cross-resistance, which was consistent with a previous study.23 Mutations in the eis promoter were found only in KM-resistant isolates with low-level resistance, implying that it does not always confer cross-resistance among SLIDs, which was concordant with previous studies.17,24,25
The excellent sensitivity of both MeltPro and WGS was associated with a high frequency of A1401G (91.7%) in rrs mutations circulating in Chongqing. Excellent agreement with phenotypic DST indicated that MeltPro and WGS assays provided an accurate option for the diagnosis of SLID resistance. Discordance occurred in four SLID isolates identified as sensitive by MeltPro but resistant by WGS, including three isolates with mutations in the tlyA gene, which was not covered by MeltPro, leading to inconsistent results. The other isolate, with 24.65% rrs A1401G heteroresistance, was identified by WGS assay but missed by MeltPro, which was principally attributed to the different limits of detection of various molecular diagnostics. The one phenotypically SLID-resistant isolate was predicted to be resistant by MeltPro with mutations in eis C-14T/eis A-13G/eis G-10A, but sensitive by WGS, which may be attributed to the incomplete WGS database of mutation sites. In addition, the design principle of the MeltPro kit, with these three mutation sites in the ROX fluorescence channel, resulted in differences in ΔTm values and uninterpretable specific mutation type.
Though it has been shown to be accurate and reliable compared to conventional phenotypic diagnostics,7 there is a potential barrier to WGS popularization in resource-limited settings, due to its cumbersome nature, cost, and technical accessibility. Recent work demonstrated that a high-resolution melting curve outperformed conventional PCR-based assays on identifying heteroresistant samples,26,27 indicating that MeltPro was a better solution for accurate heteroresistance. Two isolates showing phenotypic resistance were identified as SLID-sensitive by MeltPro and WGS, which may be attributed to other resistance mechanisms, such as drug efflux and decreased permeability of the cell wall.
In conclusion, MeltPro is a promising diagnostic tool for accurate identification of SLID-resistant MTB isolates with mutations in the rrs and eis genes. The proportion of heterogeneous drug-resistant bacteria with rrs mutations and limited probes in MeltPro resulted in disparity with WGS results. Resistance mechanisms other than genetic mutations will affect the consistency of MeltPro and WGS in phenotypic drug-susceptibility results. Though SLIDs have been removed as a mainstream treatment of drug-resistant TB, developing molecular assays with other drugs presently used for treatment is important.
Data Sharing
Data can be made available through contact with the corresponding author.
Ethical Approval
This study was approved by the Ethics Committee of Chongqing Tuberculosis Control Institute (KY201801), and written informed consent was obtained from all participants. This study was conducted in accordance with the Declaration of Helsinki.
Funding
This work was supported by the Beijing Natural Science Foundation (7224328), Chongqing Middle-and-Young Medical High-end Talent Project ([2023] 10), and the first batch of Key Disciplines on Public Health in Chongqing ([2022]72).
Disclosure
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
1. World Health Organization. Global Tuberculosis Report 2022. Geneva: World Health Organization; 2022.
2. World Health Organization. Global Tuberculosis Report 2020. Geneva: World Health Organization; 2020.
3. World Health Organization. Rapid Communication: Key Changes to Treatment of Multidrug- and Rifampicin-Resistant Tuberculosis (MDR/RR-TB); 2018.
4. Ramakrishna V, Singh PK, Prakash S, Jain A. Second Line Injectable Drug Resistance and Associated Genetic Mutations in Newly Diagnosed Cases of Multidrug-Resistant Tuberculosis. Microb Drug Resist. 2020;26(8):971–975. doi:10.1089/mdr.2019.0215
5. Deun AV, Decroo T. How Second-Line Injectable Drugs Work. Clin Infect Dis. 2021;72(12):e1167–e1168. doi:10.1093/cid/ciaa1874
6. Decroo T, Maug AKJ, Hossain MA, et al. Injectables’ key role in rifampicin-resistant tuberculosis shorter treatment regimen outcomes. PLoS One. 2020;15(8):e0238016. doi:10.1371/journal.pone.0238016
7. van Beek J, Haanpera M, Smit PW, Mentula S, Soini H. Evaluation of whole genome sequencing and software tools for drug susceptibility testing of Mycobacterium tuberculosis. Clin Microbiol Infect. 2019;25(1):82–86. doi:10.1016/j.cmi.2018.03.041
8. World Health Organization. Tuberculosis; 2017.
9. Hu S, Li G, Li H, et al. Rapid detection of isoniazid resistance in Mycobacterium tuberculosis isolates by use of real-time-PCR-based melting curve analysis. J Clin Microbiol. 2014;52(5):1644–1652. doi:10.1128/JCM.03395-13
10. Papaventsis D, Casali N, Kontsevaya I, Drobniewski F, Cirillo DM, Nikolayevskyy V. Whole genome sequencing of Mycobacterium tuberculosis for detection of drug resistance: a systematic review. Clin Microbiol Infect. 2017;23(2):61–68. doi:10.1016/j.cmi.2016.09.008
11. Meehan CJ, Goig GA, Kohl TA, et al. Whole genome sequencing of Mycobacterium tuberculosis: current standards and open issues. Nat Rev Microbiol. 2019;17(9):533–545. doi:10.1038/s41579-019-0214-5
12. Falzon D, Jaramillo E, Schunemann HJ, et al. WHO guidelines for the programmatic management of drug-resistant tuberculosis: 2011 update. Eur Respir J. 2011;38(3):516–528. doi:10.1183/09031936.00073611
13. CLSI. Susceptibility Testing of Mycobacteria, Nocardia Spp. and Other Aerobic Actinomycetes. Wayne, PA: Clinical and Laboratory Standards Institute; 2018.
14. CLSI. Performance Standards for Susceptibility Testing of Mycobacteria, Nocardia Spp. and Other Aerobic Actinomycetes. Wayne, PA: Clinical and Laboratory Standards Institute; 2018.
15. Somerville W, Thibert L, Schwartzman K, Behr MA. Extraction of Mycobacterium tuberculosis DNA: a question of containment. J Clin Microbiol. 2005;43(6):2996–2997. doi:10.1128/JCM.43.6.2996-2997.2005
16. Syed RR, Catanzaro DG, Colman RE, et al. Clinical Evaluation of the XDR-LFC Assay for the Molecular Detection of Isoniazid, Rifampin, Fluoroquinolone, Kanamycin, Capreomycin, and Amikacin Drug Resistance in a Prospective Cohort. J Clin Microbiol. 2023;61(3):e0147822. doi:10.1128/jcm.01478-22
17. Hu Y, Xu L, He YL, et al. Prevalence and Molecular Characterization of Second-Line Drugs Resistance among Multidrug-Resistant Mycobacterium tuberculosis Isolates in Southwest of China. Biomed Res Int. 2017;2017:4563826. doi:10.1155/2017/4563826
18. Li G, Guo Q, Liu H, et al. Detection of Resistance to Fluoroquinolones and Second-Line Injectable Drugs Among Mycobacterium tuberculosis by a Reverse Dot Blot Hybridization Assay. Infect Drug Resist. 2020;13:4091–4104. doi:10.2147/IDR.S270209
19. Li Q, Gao H, Zhang Z, et al. Mutation and Transmission Profiles of Second-Line Drug Resistance in Clinical Isolates of Drug-Resistant Mycobacterium tuberculosis From Hebei Province, China. Front Microbiol. 2019;10:1838. doi:10.3389/fmicb.2019.01838
20. Georghiou SB, Magana M, Garfein RS, Catanzaro DG, Catanzaro A, Rodwell TC. Evaluation of genetic mutations associated with Mycobacterium tuberculosis resistance to amikacin, kanamycin and capreomycin: a systematic review. PLoS One. 2012;7(3):e33275. doi:10.1371/journal.pone.0033275
21. Jugheli L, Bzekalava N, de Rijk P, Fissette K, Portaels F, Rigouts L. High level of cross-resistance between kanamycin, amikacin, and capreomycin among Mycobacterium tuberculosis isolates from Georgia and a close relation with mutations in the rrs gene. Antimicrob Agents Chemother. 2009;53(12):5064–5068. doi:10.1128/AAC.00851-09
22. Reeves AZ, Campbell PJ, Willby MJ, Posey JE. Disparities in capreomycin resistance levels associated with the rrs A1401G mutation in clinical isolates of Mycobacterium tuberculosis. Antimicrob Agents Chemother. 2015;59(1):444–449. doi:10.1128/AAC.04438-14
23. WHO. World Health Organization the Use of Next-Generation Sequencing Technologies for the Detection of Mutations Associated with Drug Resistance in Mycobacterium Tuberculosis Complex: Technical Guide. Geneva: Switzerland; 2018.
24. Miotto P, Tessema B, Tagliani E, et al. A standardised method for interpreting the association between mutations and phenotypic drug resistance in Mycobacterium tuberculosis. Eur Respir J. 2017;50(6):1701354. doi:10.1183/13993003.01354-2017
25. Zaunbrecher MA, Sikes RD Jr, Metchock B, Shinnick TM, Posey JE. Overexpression of the chromosomally encoded aminoglycoside acetyltransferase eis confers kanamycin resistance in Mycobacterium tuberculosis. Proc Natl Acad Sci. 2009;106(47):20004–20009. doi:10.1073/pnas.0907925106
26. Huo F, Ma Y, Li S, et al. Specific gyrA Gene Mutations Correlate with High Prevalence of Discordant Levofloxacin Resistance in Mycobacterium tuberculosis Isolates from Beijing, China. J Mol Diagn. 2020;22(9):1199–1204. doi:10.1016/j.jmoldx.2020.06.010
27. Hu Y, Chi Y, Feng X, et al. Comparison of the Diagnostic Performance of MeltPro and Next-Generation Sequencing in Determining Fluoroquinolone Resistance in Multidrug-Resistant Tuberculosis Isolates. J Mol Diagn. 2023;25(6):342–351. doi:10.1016/j.jmoldx.2023.02.003
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.