Back to Journals » Journal of Pain Research » Volume 19
Evaluation of Abuse Deterrent Formulations of Oxycodone Products: Real-World Data from an Enriched Population of Substance Users Assessed with the Addiction Severity Index-Multimedia Version (ASI-MV®)
Authors Green JL ![]() , Dailey-Govoni T
, Dailey-Govoni T ![]() , Vosburg SK
, Vosburg SK
Received 5 June 2025
Accepted for publication 9 December 2025
Published 8 January 2026 Volume 2026:19 541820
DOI https://doi.org/10.2147/JPR.S541820
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Timothy Atkinson
Jody L Green, Taryn Dailey-Govoni, Suzanne K Vosburg
Integrated Behavioral Health, Inflexxion, Irvine, CA, 82614, USA
Correspondence: Jody L Green, Integrated Behavioral Health, Inflexxion, 2 Park Plaza, Suite 1200, Irvine, CA, 82614, USA, Tel +1 303 618 9044, Email [email protected]
Purpose: The study purpose was to evaluate real-world data on routes of administration (ROAs) employed for nonmedical use (NMU) of XTAMPZA ER compared to other oxycodone extended-release (ER) and oxycodone immediate-release (IR) formulations in a population of adults assessed for substance use.
Patients and Methods: A cross-sectional observational study was conducted among adults assessed for substance use and treatment planning using the Addiction Severity Index-Multimedia Version (ASI-MV®) from July 2016 through December 2023. Demographic and substance use history data were summarized to characterize the sample. The primary outcome measure was the prevalence of past 30-day non-oral NMU, assessed first by using Pearson’s chi-square to test differences in prevalence, then by calculating the proportional reporting ratios (PRR) to determine if specific non-oral ROAs were more or less likely to be used for XTAMPZA ER NMU versus comparators.
Results: The prevalence of non-oral ROA cases was significantly higher among other oxycodone ER cases (2221/4935, 45.0%) and oxycodone IR cases (10,598/20,394, 52.0%) compared to XTAMPZA ER cases (31/141, 22.0%)(X2=29.43, p< 0.0001 and X2=50.41, p< 0.0001, respectively). Compared to other oxycodone ER, XTAMPZA ER had a 33% lower risk of snorting (PRR: 0.67, 95% CI: 0.47, 0.95) and a 63% lower risk of injecting (PRR: 0.37, 95% CI: 0.19, 0.71). Compared to oxycodone IR, XTAMPZA ER had a 46% lower risk of snorting (PRR: 0.54, 95% CI: 0.38, 0.77) and a 66% lower risk of injecting (PRR: 0.44, 95% CI: 0.23, 0.86).
Conclusion: Opioid medications can provide valuable patient benefits with risks best mitigated by using formulations associated with lower likelihood of NMU, particularly via higher-risk non-oral ROAs. These study findings suggest that XTAMPZA ER has a lower risk of NMU via non-oral ROA compared to other oxycodone ER and oxycodone IR products in an enriched population of substance users.
Keywords: pain management, opioid, nonmedical use, substance abuse treatment, real-world data, abuse deterrent formulations, routes of administration
Introduction
Promising trends in reductions of drug overdose fatalities have been reported in the United States (US). These include a 4% decrease in the overall age-adjusted rate between 2022 and 2023 with a 33.3% decline in deaths involving heroin, a 17.1% decline in deaths involving natural and semisynthetic opioids (prescription opioids), and a 2.2% decline in deaths involving synthetic opioids other than methadone (primarily fentanyl and fentanyl analogs).1 Another provisional report of drug overdose fatality data discovered a 24% overall decline from September 2023 to September 2024.2
While significant reductions in deaths involving prescription opioids have been reported, there has been a continued effort to reduce nonmedical use (NMU) of prescription opioids in the US. NMU is any deviation from legitimate medical use (defined as use of one’s own prescription medication from a healthcare provider only in the manner in which it was prescribed, including using via the intended route of administration (ROA)). This is challenging considering that in 2023, almost one in four (24.3%) American adults suffered from chronic pain and 8.5% suffered from high impact chronic pain (pain that often restricts life or work activities).3 Pain management is among the most common reasons adults seek medical care and has been associated with anxiety and depression4 and decreased quality of life.5 These patients and their providers often rely on prescription opioid therapies as part of their treatment plan. Restrictions on opioid prescribing have reduced the supply of these medications, however mixed results are reported in relation to the associated positive and negative effects on the intended patient population, the majority of which use their medications appropriately. The updated CDC guidelines for opioid prescribing noted unintended impacts of the original guidelines on patient health and encouraged patient-centric pain management going forward (with opioids and other therapies).6 This is important as healthcare providers balance treatment of chronic pain with mitigation of opioid-related risks.
Numerous interventions have been implemented to curb opioid NMU. However, only abuse deterrent formulations (ADFs) are product-specific and intended to deter use by non-oral ROAs (eg, snorting, smoking, injecting). Non-oral ROAs have been associated with a higher likelihood of life-threatening events and death.7 The Abuse-Deterrent Opioids – Evaluation and Labeling Guidance for Industry, published by the US Food and Drug Administration (FDA) in April 2015,8 defines abuse-deterrent properties as those shown to meaningfully deter abuse, even if they do not fully prevent abuse.
Postmarket evaluation of ADF opioids has been generally positive. One study documented reduction in abuse, therapeutic errors, and accidental exposures involving ADF opioids reported to US poison centers.9 Another group of studies found reductions in prevalence of overall abuse and abuse via non-oral ROAs with ADF opioids in adults evaluated for substance use.10–12 One additional study reported a reduction in drug diversion of ADF medications13 and another reported a reduction in healthcare utilization and associated healthcare costs (eg, opioid-related emergency department visits and hospitalizations) of ADF opioids.14,15
Within the marketed opioid medications, oxycodone-containing products are available in ADF and non-ADF formulations, allowing for evaluation of the effectiveness of an ADF. As of 2013, all extended-release (ER) oxycodone products marketed in the US must have abuse-deterrent properties.16 On the contrary, immediate-release (IR) oxycodone products are not required to have abuse-deterrent properties and to date, the only ADF IR oxycodone product is RoxybondTM which was approved by the FDA in 2017. The first ADF to receive FDA labeling was OxyContin® (oxycodone HCl extended-release tablets, Purdue Pharma L.P., Stamford, CT) in 2010. This labeling included a statement that the formulation is expected to make abuse via injection difficult and expected to reduce abuse by the intranasal ROA.17 XTAMPZA ER (oxycodone extended-release, Collegium Pharmaceutical, Stoughton, MA) was approved in April 2016 and includes ADF labeling that states that the formulation is expected to make abuse by injection difficult and expected to reduce abuse via the oral and intranasal ROAs.18 The FDA labeling is different between these two ER ADFs because while both are intended to preserve the prolonged release mechanism and prevent immediate access to the full amount of active ingredient, they use different technology. OxyContin uses RESISTECTM, a polyethylene oxide matrix that hardens the tablet and becomes viscous in aqueous solutions which aids in resistance to syringe aspiration. XTAMPZA ER uses the DETERx® microsphere-in-capsule technology in which the oxycodone is homogenously dispersed within hydrophobic, waxy microspheres with each microsphere acting as an independent drug delivery system.
The published literature provides consistent evidence suggesting lower risk of misuse, abuse (particularly via non-oral ROAs), diversion, product tampering, severity of clinical outcomes, and opioid-related healthcare costs with XTAMPZA ER relative to other ADF opioids.11,12,15,19–22 The reported differences appeared to be sustained throughout the first five years that XTAMPZA ER was on the US market (2016–2021), however the opioid landscape is constantly evolving and ongoing surveillance is warranted. Hence, the objective of this study was to extend the surveillance period through 2023 and evaluate real-world data on NMU via non-oral ROAs of XTAMPZA ER compared to other oxycodone ER formulations and oxycodone IR formulations in a population of adults assessed for substance use.
Materials and Methods
A cross-sectional observational study was conducted to evaluate NMU by ROA among adults aged 18 years or older assessed for substance use and treatment planning using the Addiction Severity Index-Multimedia Version (ASI-MV®) assessment. The study groups included those who reported NMU of (1) XTAMPZA ER, (2) other oxycodone ER (excluding XTAMPZA ER), or (3) oxycodone IR. Individuals could report NMU of more than one product therefore these groups are not mutually exclusive. The primary outcome measure was past 30-day NMU stratified by ROA.
Data Source
The ASI-MV is a modified version of the original Addiction Severity Index (ASI), a clinical intake assessment designed for use upon admission to drug and alcohol treatment with demonstrated reliability and validity.23–26 The ASI-MV is used in a variety of clinical settings, including inpatient and outpatient treatment facilities.
The ASI-MV has good test-retest reliability, discriminant validity, and criterion validity.23 In addition to the original ASI domains (medical, employment/financial support status, alcohol use, drug use, legal, family/social status, and psychiatric status), the ASI-MV also collects patient characteristics, substance use and treatment history, and use of pharmaceutical substances via product-specific questions about use, past 30-day NMU, ROA, and sources of procurement. Specific medications are identified by presenting screens with images, text and audio including medication names and slang/street names, so that respondents are better able to differentiate between various products that they report having used. NMU was identified with the use of an algorithm of responses to several questions to identify any deviation from legitimate medical use (use of one’s own prescription medication from a healthcare provider only in the manner in which it was prescribed, including using the intended ROA). The definition of NMU as captured by ASI-MV and used in this study includes both abuse (intentional, non-therapeutic use of a drug even once to achieve a desirable psychological or physiological effect) and misuse (intentional therapeutic use of a drug in an inappropriate way).
A single ASI-MV assessment may report past 30-day NMU of multiple products within one study group or NMU of products from multiple study groups. For example, one assessment could report past 30-day NMU of XTAMPZA ER, other oxycodone ER, and oxycodone IR products. To address this aspect of real-world use, NMU was evaluated at the assessments level and at the mentions level. NMU mentions include the total number of past 30-day NMU reports of the opioid products within a study group (ie, the sum of reports). When evaluating NMU at the assessments level, a binary variable (Yes/No) is constructed in which each assessment is either assigned as reporting NMU of the study group (Yes) or not reporting NMU of the study group (No). Thus, the count of NMU mentions will be greater than the count of NMU assessments for the comparator oxycodone study groups. As the XTAMPZA ER study group includes only one product, the counts of NMU mentions and assessments will be the same. It is possible for a unique individual to complete more than one assessment over time. In this instance, the first assessment completed by the individual during the given quarter was retained and any subsequent assessments in that quarter were removed from the analysis dataset.
Data Analysis
The study period included ASI-MV assessments collected from 01 July 2016 through 31 December 2023. XTAMPZA ER was launched in June of 2016 and added to the ASI-MV in Q3 2017, allowing for a one-year market transition before data regarding this product were collected. One year of baseline data was included for comparator groups to account for this transition. Demographics and substance use history were summarized and compared between study groups using Pearson’s chi-square test (or Fisher’s exact test for comparisons with small cell size) for categorical data (demographics, ROA) and Wilcoxon rank sum tests for ordinal data (domain severity ratings). Statistical significance was determined for tests where p<0.05.
Nonparametric statistics were used to compare past 30-day NMU by ROA. The primary benefits of nonparametric testing are that they can accommodate smaller sample sizes, they do not require any assumptions about the underlying probability distribution of the data, and they appropriately use categorical data.27–29 This was assessed first by using Pearson’s chi-square to test differences in the volume of cases with non-oral ROA between XTAMPZA ER and comparator groups. Next, the proportional reporting ratios (PRR) were calculated to determine if specific ROAs were more or less likely to be used for XTAMPZA ER NMU versus comparator groups. PRR is a commonly used method to assess disproportionality in pharmacovigilance surveillance data and has been deemed a validated method in drug safety research and surveillance for signal detection.30,31
Using XTAMPZA ER as the reference group, the PRR was calculated for (a) any non-oral ROA (snorted, smoked, injected) versus any oral ROA (swallowed whole, chew then swallowed, dissolved like a cough drop, dissolved in liquid then drank), (b) any non-oral route versus swallowed whole, (c) snorted versus swallowed whole, and (d) injected versus swallowed whole. An individual assessment may include reported NMU of more than one oxycodone product by more than one ROA, hence ROAs are not mutually exclusive. Each mention of a product and ROA was used to calculate the ratios. Statistical significance was reached if the 95% confidence interval (CI) for the PRR did not include 1.0. Analyses were conducted using SAS statistical software version 8.3 (SAS Institute, Cary NC, USA).
Secondary analysis of existing de-identified clinical data was determined to be exempt from institutional review board review by the New England Institutional Review Board (now part of the WCG IRB). All data accessed complied with relevant data protection and privacy regulations.
Results
From 01 July 2016 through 31 December 2023, 879 sites located in 46 states contributed a total of 341,851 adult assessments to the ASI-MV network (Figure 1). A total of 67,855 (19.8%) of the 341,851 assessments included self-reported past 30-day NMU of a prescription opioid. Of these, 141 (0.2%) reported XTAMPZA ER NMU, 4935 (7.3%) reported other oxycodone ER NMU, and 20,394 (30.1%) reported oxycodone IR NMU (Table 1). The majority (97.9%) of assessments that reported XTAMPZA ER NMU also reported NMU of other prescription opioids, including 38.3% that also reported other oxycodone ER and 87.9% that also reported oxycodone IR.
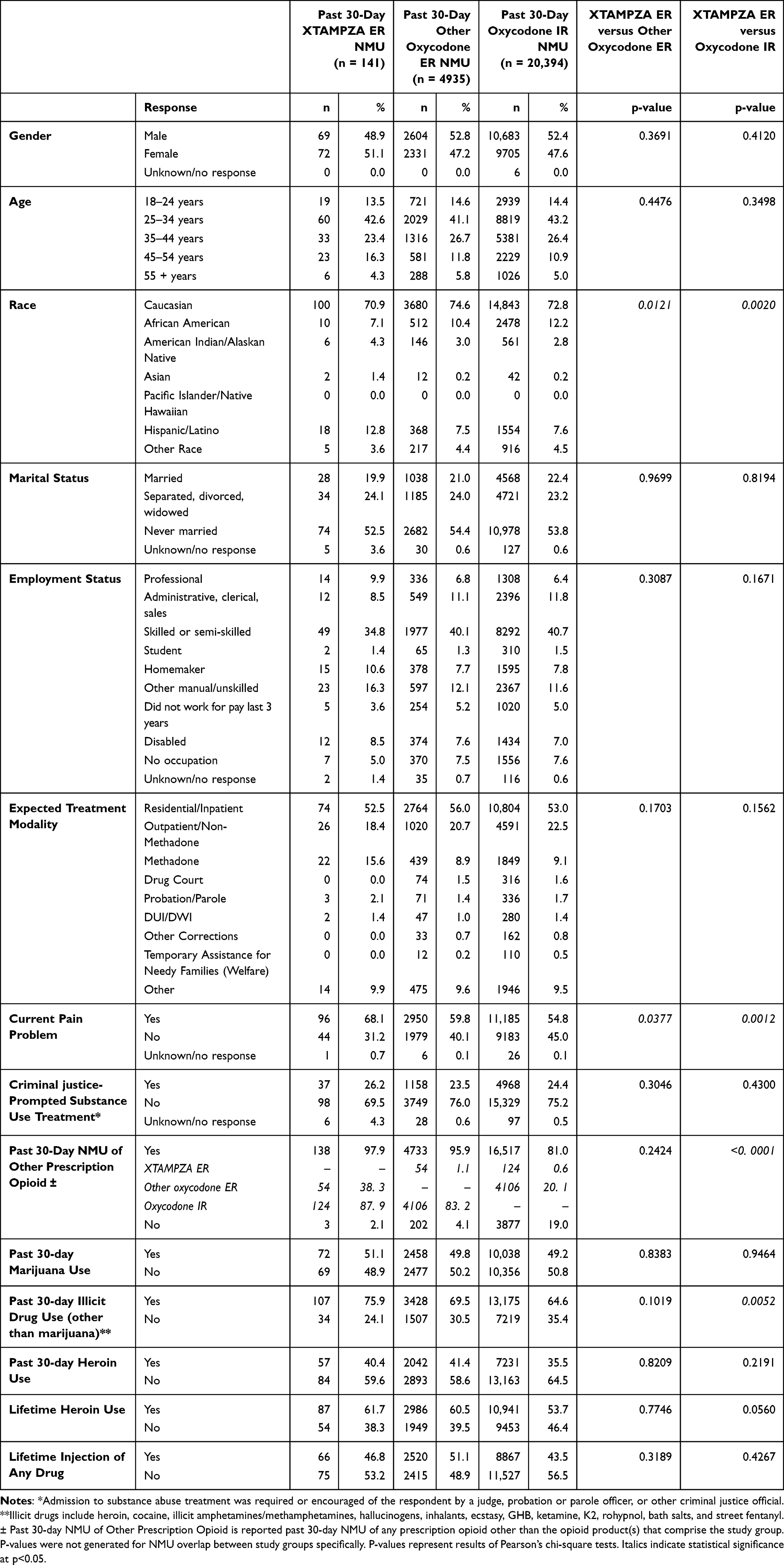 |
Table 1 Demographics and Substance Use History of Individuals Reporting Past 30-Day Nonmedical Use (NMU) from 01 July 2016 Through 31 December 2023 |
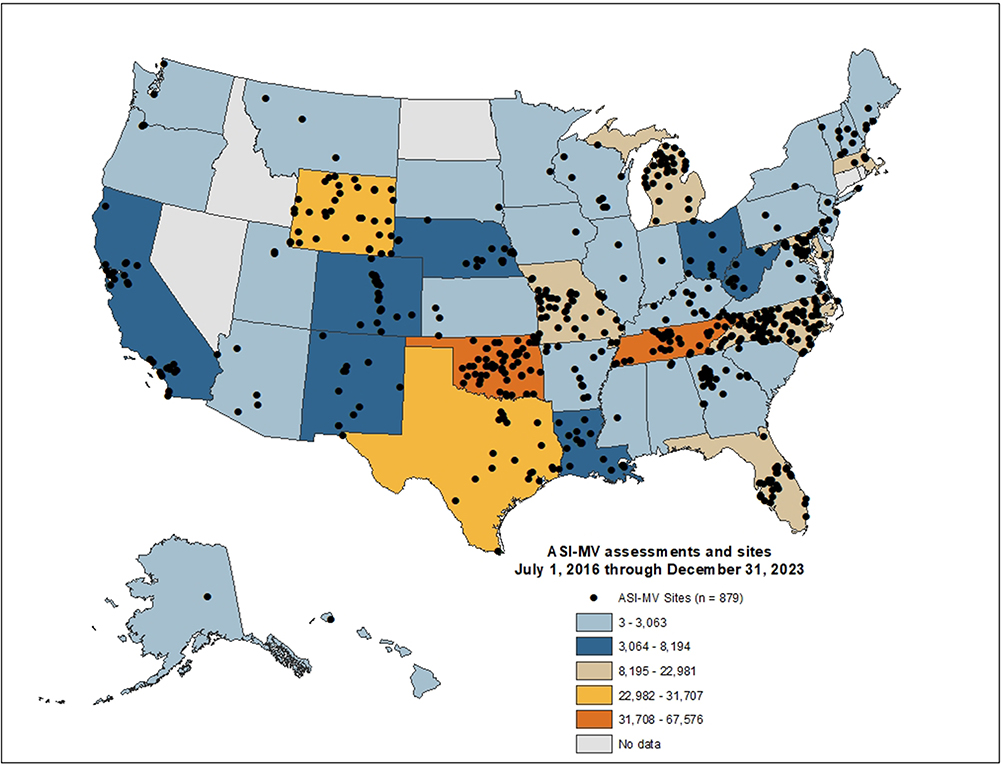 |
Figure 1 Geographic Distribution of ASI-MV Assessments and Sites, by State (01 July 2016 through 31 December 2023). Abbreviation: ASI-MV, Addiction Severity Index-Multimedia Version. Notes: Figure 1 displays the number of ASI-MV assessments submitted by state location of site; with black dots representing the zip code location of site. It is possible to have more than one site in the same zip code or city in which case the dots will be superimposed on the map. |
The distribution of demographics was similar between the XTAMPZA ER and comparator groups except for race; Hispanic/Latino race was reported by a greater proportion of the XTAMPZA ER group (12.8%) compared to the other oxycodone ER and oxycodone IR groups (7.5% and 7.6%, respectively) (Table 1). Those reporting XTAMPZA ER NMU were more likely to have a current pain problem than both comparator groups and more likely to report past 30-day illicit drug use than the oxycodone IR group. Otherwise, historical drug use was similar among the study groups. Other notable differences were that, relative to the oxycodone IR group, a greater proportion of the XTAMPZA ER group had severity ratings in the alcohol, employment, family and medical domains that reflected moderate, considerable, or extreme problems (Table 2). Further, the XTAMPZA ER group had a higher proportion of moderate/considerable/extreme legal severity ratings than the other oxycodone ER group and the oxycodone IR group.
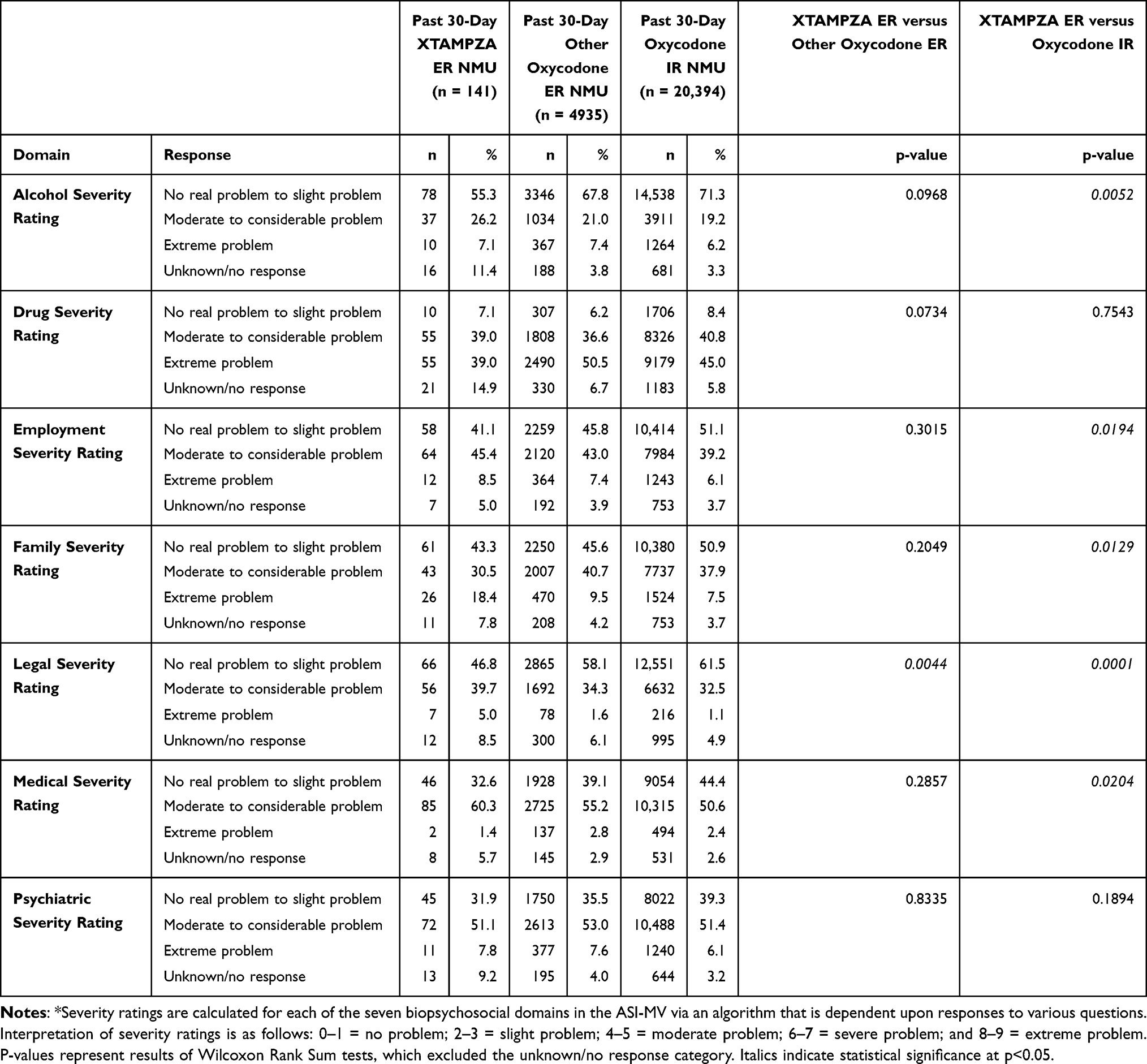 |
Table 2 Addiction Severity Index (ASI) Domain Severity Ratings* by Study Group |
Oral ROAs were most commonly reported across all study groups (Table 3). The proportion of non-oral ROA cases was significantly higher with other oxycodone ER cases (45.0%) and oxycodone IR cases (52.0%) compared to XTAMPZA ER cases (22.0%)(X2=29.43, p<0.0001 and X2=50.41, p<0.0001, respectively). Snorting was the most reported non-oral ROA in all study groups, followed by injecting. Compared to other oxycodone ER, XTAMPZA ER had a 40% lower risk of NMU via non-oral ROAs (PRR: 0.60, 95% CI: 0.45, 0.80), a 33% lower risk of snorting (PRR: 0.67, 95% CI: 0.47, 0.95), and a 63% lower risk of injecting (PRR: 0.37, 95% CI: 0.19, 0.71) (Figure 2). Compared to oxycodone IR, XTAMPZA ER had a 46% lower risk of NMU via non-oral ROAs (PRR: 0.54, 95% CI: 0.41, 0.72), a 46% lower risk of snorting (PRR: 0.54, 95% CI: 0.38, 0.77), and a 66% lower risk of injecting (PRR: 0.44, 95% CI: 0.23, 0.86). All differences were statistically significant (CI did not include 1.0).
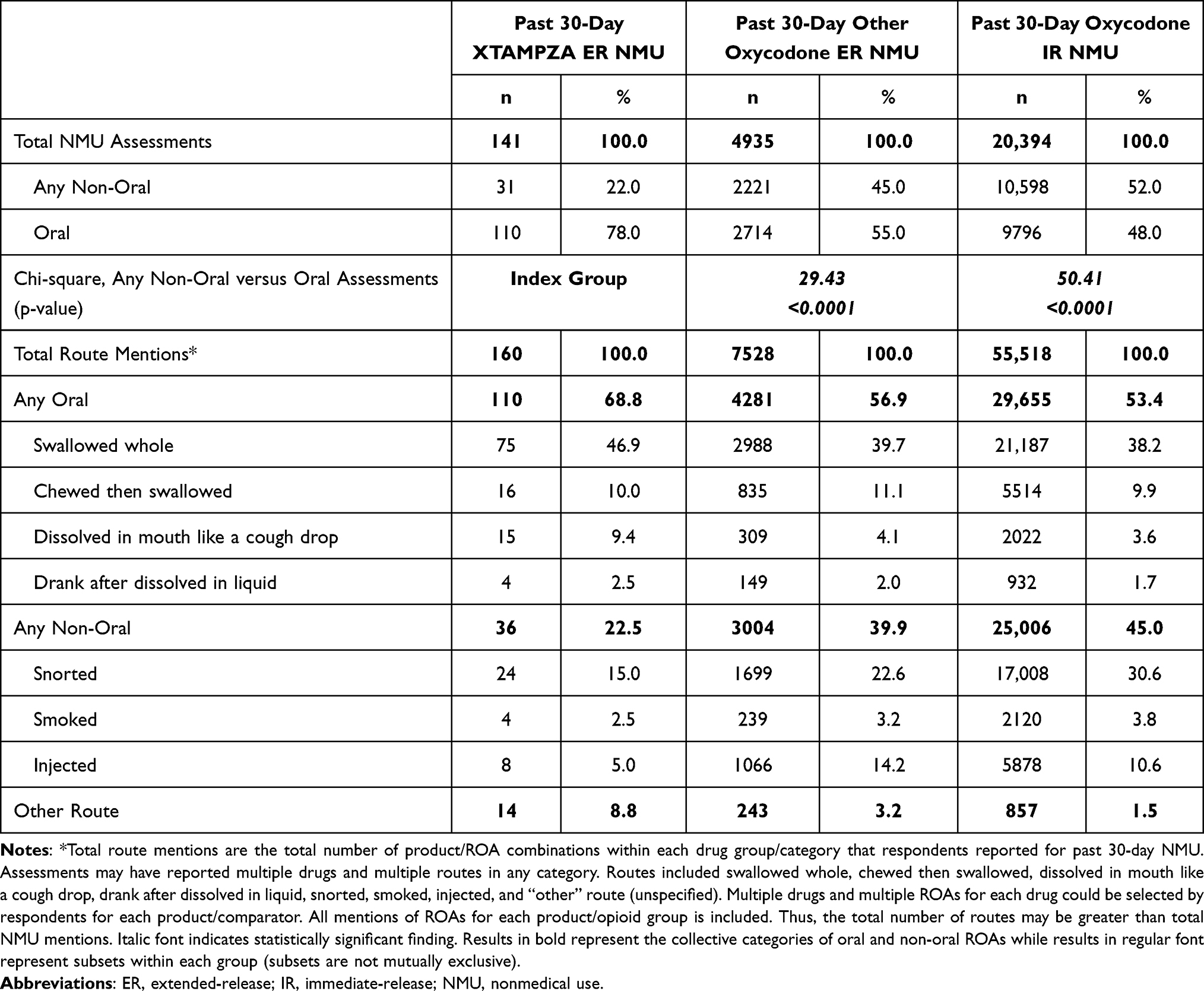 |
Table 3 Prevalence of Nonmedical Use (NMU) by Route of Administration |
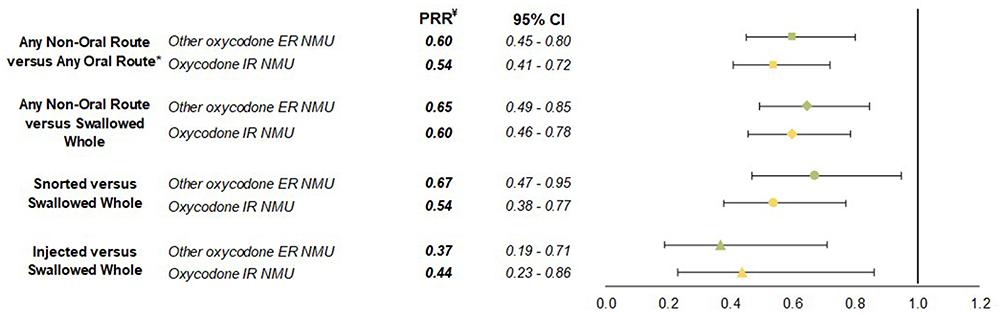 |
Figure 2 Proportional Reporting Ratios (PRR) of Routes of Administration: XTAMPZA ER NMU versus Comparator Groups. *Any Non-oral ROA includes snorted, smoked, and injected. Any Oral ROA includes swallowed whole, chewed then swallowed, dissolved in mouth like a cough drop, and drank after dissolved in liquid. ¥Italicized PRR values indicate statistical significance (confidence intervals did not include 1.0). PRR values <1.0 indicate a reduced risk for XTAMPZA ER versus comparator group. Abbreviations: CI, confidence interval; ER, extended-release; IR, immediate-release; NMU, nonmedical use. |
Discussion
Ongoing efforts to prevent prescription opioid NMU are important considering the need for effective and safe pain therapies. ADF formulations are a product-specific innovation, and some may be more effective than others at deterring use via non-oral ROAs. This is impactful since opioid abuse via non-oral ROAs has been associated with a higher likelihood of life-threatening events or death.7 Considering the primary goal of an ADF is to deter manipulation of the drug to be used via non-oral ROAs, ROAs should be considered as a primary outcome in assessing their effectiveness. In this study, XTAMPZA ER had a reduced risk of NMU via non-oral ROAs, snorting, and injecting compared to other oxycodone ER and oxycodone IR. These findings were statistically significant even with the relatively small number of XTAMPZA ER NMU mentions. A previous study analyzed ASI-MV data through 2019 and reported a statistically significant difference in the proportion of non-oral versus oral ROAs between XTAMPZA ER and other oxycodone ER (X2=18.57, p<0.001) and oxycodone IR (X2=52.47, p<0.001) with mixed results for the PRR analysis.11 All PRRs favored XTAMPZA ER but not all were statistically significant, likely due to the small sample size for the XTAMPZA ER group (n=73). The current study included data through 2023 and a sample size of 141 for the XTAMPZA ER group, with all PRR analyses resulting in statistically significant differences. These findings suggest reduced risk with XTAMPZA ER even with increasing utilization.
Abuse profiles with specific evaluation by ROAs have also been evaluated using data from US poison centers and other substance use treatment center-based data sources with similar findings12,22 Severtson et al 2020 reported that (1) non-oral abuse cases involving XTAMPZA ER were infrequent and occurred at lower rates than with oxycodone IR, other ADF ER opioids, and non-ADF ER opioids, and (2) while drug utilization increased during the study period, there was not an increase in abuse/misuse. Building upon this study, Severtson et al 2023 noted that as of 2021, which was almost 5 years since market introduction, no reports of use of XTAMPZA ER via injecting or snorting had yet been reported to participating poison centers.
It is possible that prescribing of these different oxycodone medications is differential, meaning prescribers may choose a particular medication for a patient with certain characteristics or risks, thus introducing a selection bias. The XTAMPZA ER group had higher alcohol, medical, family and employment severity ratings than oxycodone IR, a higher legal severity rating than other oxycodone ER and oxycodone IR groups, and higher likelihood of history of illicit drug use, yet XTAMPZA ER was still less likely to be used via non-oral ROAs. These real-world data findings are supported by the technology of the formulations as evaluated with premarket studies.32–37 One such study, a comparative cross-over pharmacokinetic study,32 found that crushed and intact XTAMPZA ER were bioequivalent and had lower peak plasma concentrations than crushed IR oxycodone, while crushed OxyContin exhibited a rapid increase in plasma oxycodone and was bioequivalent to IR oxycodone. This may help explain the differences in ROA profiles.
Limitations
As with any evaluations of real-world data, there are limitations to this study. While the ASI-MV uses photos and names of products, all assessments rely on self-report, including product selection and recall of ROA. The ASI-MV is not a nationally representative sample, hence it is unknown if these results are generalizable to all adults in the United States assessed for substance use and treatment planning. NMU of multiple opioid products, including products comprising one or more study groups, may be reported in a single assessment. The study included one year of baseline data for other oxycodone ER and oxycodone IR NMU prior to the addition of XTAMPZA ER. The PRR is typically used for signal detection and these analyses are associative, thus a direct causal relationship cannot be established. Finally, the number of assessments reporting past 30-day NMU of XTAMPZA ER during the study period was relatively low with just three instances of XTAMPZA ER NMU alone (no other prescription opioid NMU reported in past 30-days), limiting evaluation of XTAMPZA ER NMU outside of polysubstance NMU. However, even with the overlap of opioids reported, differences were still discovered between study groups.
Conclusion
XTAMPZA ER was associated with significantly lower rates of NMU via non-oral routes compared with other oxycodone formulations in a large, treatment-seeking population. Although limited by reliance on self-report and the inability to assign a causal relationship, these findings are consistent with the abuse deterrent properties of XTAMPZA ER. This real-world evidence supports the potential role of ADFs in reducing high-risk patterns of opioid misuse.
Acknowledgments
This study was funded by Collegium Pharmaceutical, Inc.
Disclosure
JLG reports personal fees from Opioid PMR Consortium, outside the submitted work. JLG, TDG, and SKV are employees of Uprise Health. Uprise Health contracts with government agencies and private companies with interests in some of the products included in the compounds evaluated for this article. Although the sponsor was involved in reviewing the content of this article, all data collection, analysis, and ultimate data interpretation were made by the authors without sponsor influence. An abstract of this paper was presented at PAINWeek Conference 2024 as a poster presentation with preliminary findings.
References
1. Garnett MF, Minino AM. Drug overdose deaths in the United States, 2003–2023. NCHS Data Brief. National Center for Health Statistics; 2024:522. doi:10.15620/cdc/170565
2. Ahmad FB, Cisewski JA, Rossen LM, Sutton P. Provisional drug overdose death counts. 2025. Available from: https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm.
3. Lucas JW, Sohi I. Chronic Pain and High-impact Chronic Pain in U.S. Adults, 2023. NCHS Data Brief. 2024;(518):169630. doi:10.15620/cdc/169630
4. De La Rosa JS, Brady BR, Ibrahim MM, et al. Co-occurrence of chronic pain and anxiety/depression symptoms in U.S. adults: prevalence, functional impacts, and opportunities. Pain. 2024;165(3):666–11. doi:10.1097/j.pain.0000000000003056
5. Pitcher MH, Von Korff M, Bushnell MC, Porter L. Prevalence and profile of high-impact chronic pain in the United States. J Pain. 2019;20(2):146–160. doi:10.1016/j.jpain.2018.07.006
6. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain - United States, 2022. MMWR Recomm Rep. 2022;71(3):1–95. doi:10.15585/mmwr.rr7103a1
7. Green JL, Bucher Bartelson B, Le Lait MC, et al. Medical outcomes associated with prescription opioid abuse via oral and non-oral routes of administration. Drug Alcohol Depend. 2017;175:140–145. doi:10.1016/j.drugalcdep.2017.01.039
8. CDER. Abuse deterrent opioids—evaluation and labeling, guidance for industry. Division of Drug Information; 2015. Available from: https://www.fda.gov/downloads/Drugs/Guidances/UCM334743.pdf.
9. Coplan PM, Kale H, Sandstrom L, Landau C, Chilcoat HD. Changes in oxycodone and heroin exposures in the National Poison Data System after introduction of extended-release oxycodone with abuse-deterrent characteristics. Pharmacoepidemiol Drug Saf. 2013;22(12):1274–1282. doi:10.1002/pds.3522
10. Butler SF, Cassidy TA, Chilcoat H, et al. Abuse rates and routes of administration of reformulated extended-release oxycodone: initial findings from a sentinel surveillance sample of individuals assessed for substance abuse treatment. J Pain. 2013;14(4):351–358. doi:10.1016/j.jpain.2012.08.008
11. Green JL, Robbins RS, Dailey-Govoni T, Butler SF. Nonmedical use of Xtampza((R)) ER and other oxycodone medications in adults evaluated for substance abuse treatment: real-world data from the Addiction Severity Index-Multimedia Version (ASI-MV((R))). J Pain Res. 2021;14:1773–1783. doi:10.2147/JPR.S304805
12. Severtson SG, Kreider SED, Amioka EC, Margolin ZR, Iwanicki JL, Dart RC. Postmarketing analysis of misuse, abuse, and diversion of XTAMPZA ER. Pain Med. 2020;21(12):3660–3668. doi:10.1093/pm/pnaa272
13. Severtson SG, Bartelson BB, Davis JM, et al. Reduced abuse, therapeutic errors, and diversion following reformulation of extended-release oxycodone in 2010. J Pain. 2013;14(10):1122–1130. doi:10.1016/j.jpain.2013.04.011
14. Petrilla A, Marrett E, Shen X, Kwong WJ, Pezalla E. Association between formulary coverage and use of abuse-deterrent prescription opioids, risk for abuse or overdose, and associated healthcare resource utilization. Am Health Drug Benefits. 2020;13(1):21–31.
15. Green JL, Dailey-Govoni T, Vosburg SK. Opioid-related clinical outcomes and associated healthcare costs following abuse/misuse of oxycodone formulations: a HEOR analysis from real-world data. J Opioid Manag. 2024;20(4):281–288. doi:10.5055/jom.0878
16. Notice FR. Determination that the OXYCONTIN (Oxycodone Hydrochloride) drug products covered by new drug application 20–553 were withdrawn from sale for reasons of safety or effectiveness. Silver Spring, MD: HHS; 2013:23273–23275.
17. Pharma P. OxyContin medication prescribing information and label. 2023. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/022272s048lbl.pdf.
18. Pharmaceutical C. XTAMPZA ER medication prescribing information and label. 2023. Available from: https://www.xtampzaer.com/assets/pdf/xtampza-pi.pdf.
19. Jewell J, Black J, Ellis M, Olsen H, Iwanicki J, Dart R. Correction to: a cross-sectional study of tampering in XTAMPZA ER, an abuse-deterrent formulation of an extended-release opioid, in a treatment center population. Clin Drug Investig. 2023;43(5):379. doi:10.1007/s40261-023-01259-6
20. Jewell J, Black J, Ellis M, Olsen H, Iwanicki J, Dart R. A cross-sectional study of tampering in XTAMPZA ER, an abuse-deterrent formulation of an extended-release opioid, in a treatment center population. Clin Drug Investig. 2023;43(3):197–203. doi:10.1007/s40261-023-01248-9
21. Olatoke O, Zah V, Stanicic F, et al. A US retrospective claims analysis comparing healthcare costs of patients transitioning from immediate-release oxycodone to two different formulations of extended-release oxycodone: XTAMPZA ER or OxyContin. Clinicoecon Outcomes Res. 2022;14:119–128. doi:10.2147/CEOR.S340290
22. Severtson SG, Haanschoten EE, Iwanicki J, Dart RC. Differences in severity of poison centers exposures involving XTAMPZA((R)) ER versus other opioid analgesics. Pain Manag. 2023;13(9):519–527. doi:10.2217/pmt-2022-0068
23. Butler SF, Budman SH, Goldman RJ, et al. Initial validation of a computer-administered addiction severity index: the ASI-MV. Psychol Addict Behav. 2001;15(1):4–12. doi:10.1037/0893-164x.15.1.4
24. Hendriks VM, Kaplan CD, van Limbeek J, Geerlings P. The addiction severity index: reliability and validity in a Dutch addict population. J Subst Abuse Treat. 1989;6(2):133–141. doi:10.1016/0740-5472(89)90041-x
25. Kosten TR, Rounsaville BJ, Kleber HD. Concurrent validity of the addiction severity index. J Nerv Ment Dis. 1983;171(10):606–610. doi:10.1097/00005053-198310000-00003
26. McLellan AT, Kushner H, Metzger D, et al. The fifth edition of the addiction severity index. J Subst Abuse Treat. 1992;9(3):199–213. doi:10.1016/0740-5472(92)90062-s
27. Nahm FS. Nonparametric statistical tests for the continuous data: the basic concept and the practical use. Korean J Anesthesiol. 2016;69(1):8–14. doi:10.4097/kjae.2016.69.1.8
28. Schober P, Vetter TR. Nonparametric statistical methods in medical research. Anesth Analg. 2020;131(6):1862–1863. doi:10.1213/ANE.0000000000005101
29. Siegel S, Castellan NJ. Nonparametric Statistics for the Behavioral Sciences.
30. Boehm R. Primer on disproportionality analysis. Open Vigil Source Forge; 2018.
31. Duggirala HJ, Tonning JM, Smith E, et al. Use of data mining at the food and drug administration. J Am Med Inform Assoc. 2016;23(2):428–434. doi:10.1093/jamia/ocv063
32. Brennan MJ, Kopecky EA, Marseilles A, O’Connor M, Fleming AB. The comparative pharmacokinetics of physical manipulation by crushing of Xtampza((R)) ER compared with OxyContin((R)). Pain Manag. 2017;7(6):461–472. doi:10.2217/pmt-2017-0030
33. Fleming AB, Scungio TA, Grima MP, Mayock SP. In vitro assessment of the potential for abuse via the intravenous route of oxycodone DETERx(R) microspheres. J Opioid Manag. 2016;12(1):57–65. doi:10.5055/jom.2016.0312
34. Gudin J. Oxycodone DETERx((R)): a novel abuse-deterrent, extended-release analgesic option for the treatment of patients with chronic pain. Pain Ther. 2016;5(2):171–186. doi:10.1007/s40122-016-0062-1
35. Gudin J. Effect of physical manipulation on the oral pharmacokinetic profile of Xtampza((R)) ER (oxycodone DETERx((R)) formulation): a review of published studies. J Opioid Manag. 2020;16(2):127–139. doi:10.5055/jom.2020.0559
36. Mayock SP, Saim S, Fleming AB. Author Correction to: in Vitro Drug Release After Crushing: evaluation of Xtampza((R)) ER and Other ER Opioid Formulations. Clin Drug Investig. 2017;37(12):1203. doi:10.1007/s40261-017-0599-8
37. Mayock SP, Saim S, Fleming AB. In vitro drug release after crushing: evaluation of Xtampza((R)) ER and other ER opioid formulations. Clin Drug Investig. 2017;37(12):1117–1124. doi:10.1007/s40261-017-0561-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Opioid Utilization and Management in the Setting of Stewardship During Inpatient Rehab Care
Murphy L, Leblanc K, Badr S, Ching E, Mao L, Steenhof N, Hamandi B, Rubin B, Seto A, Furlan AD
Drug, Healthcare and Patient Safety 2022, 14:161-170
Published Date: 11 September 2022
Interventional Pain Procedures: A Narrative Review Focusing on Safety and Complications. Part 1 Injections for Spinal Pain
Lo Bianco G, Tinnirello A, Papa A, Torrano V, Russo G, Stogicza A, Mercadante S, Cortegiani A, Mazzoleni S, Schatman ME
Journal of Pain Research 2023, 16:1637-1646
Published Date: 18 May 2023