Back to Journals » ClinicoEconomics and Outcomes Research » Volume 13
Evaluating the Cost-Effectiveness of Celecoxib versus Ibuprofen and Naproxen in Patients with Osteoarthritis in United Arab Emirates Based on the PRECISION Trial
Authors Chirikov VV, Walker C, Stephens JM, Schepman P ![]() , Chambers R, Bakir M, Poorman GW, Haider S, Farghaly M
, Chambers R, Bakir M, Poorman GW, Haider S, Farghaly M
Received 5 September 2020
Accepted for publication 23 April 2021
Published 19 May 2021 Volume 2021:13 Pages 409—420
DOI https://doi.org/10.2147/CEOR.S280556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio Colombo
Viktor V Chirikov,1 Chris Walker,2 Jennifer M Stephens,1 Patricia Schepman,3 Richard Chambers,4 Mahmoud Bakir,5 Gregory W Poorman,1 Seema Haider,6 Mohammed Farghaly7
1OPEN Health, Bethesda, MD, USA; 2Global Medical Affairs, Viatris, Tadworth, UK; 3Global Health Economics and Outcomes Research, Pfizer Inc, New York, NY, USA; 4Biostatistics, Pfizer Inc, Collegeville, PA, USA; 5Upjohn Export B.V., Jeddah, Saudi Arabia; 6Pfizer Inc., Groton, CT, USA; 7Dubai Medical College, Dubai, United Arab Emirates
Correspondence: Jennifer M Stephens
OPEN Health, Bethesda, MD, USA
Tel +1 703 625 5943
Email [email protected]
Objective: Data on osteoarthritis patients from the PRECISION trial were used to evaluate the cost-effectiveness of celecoxib (100 mg twice daily) versus ibuprofen (600– 800 mg three times daily) and naproxen (375– 500 mg twice daily). The perspective was that of the United Arab Emirates (UAE) healthcare system.
Methods: Discrete-state Markov model with monthly cycles, 30-month horizon, and 3% discount rate was constructed to assess incremental costs per quality adjusted life year (QALYs) gained from reduced incidence of three safety domains examined in PRECISION: renal, serious gastrointestinal (GI), and major adverse cardiovascular events (MACE). Costs for managing these toxicities were derived from Dubai Administrative Billing Claims (2018). Median monthly drug costs were derived from UAE Ministry of Health and Prevention’s published prices ($26.98 celecoxib; $20.25 ibuprofen; $20.50 naproxen). Health utility and excess mortality associated with toxicities were sourced from the literature. The willingness-to-pay thresholds used were 1 and 3 GDP per capita ($40,000–$120,000).
Results: The total average cost per patient was $812.88 for celecoxib, $775.26 for ibuprofen, and $731.17 for naproxen while cost components attributed to toxicities were lowest with celecoxib ($360.26, $438.31, and $388.60, respectively). Patients on celecoxib had more QALYs (1.339), compared with ibuprofen (1.335) and naproxen (1.337), resulting in an incremental cost-effectiveness ratio of $11,502/QALY gained for celecoxib versus ibuprofen and $39,779 for celecoxib versus naproxen. Probabilistic sensitivity analyses demonstrated celecoxib to be 81% cost-effective versus ibuprofen and 50% versus naproxen at $40,000/QALY. The most influential model parameters were MACE relative safety and drug costs.
Conclusion: From UAE third payer perspective, celecoxib is a long-term cost-effective treatment for osteoarthritis patients when compared with ibuprofen, and equally likely as naproxen to be cost-effective. With the expected increasing burden of chronic diseases in the Gulf region, study findings can inform decisions regarding the cost-effective pain management of osteoarthritis in UAE.
Clinicaltrials.gov Registration Number: NCT00346216.
Keywords: Markov, NSAIDs, comparative effectiveness, safety, Gulf region, AfME, MENA
Introduction
Pain management via traditional non-selective non-steroidal anti-inflammatory drugs (ns-NSAIDs) and selective cyclooxygenase-2 (COX-2) inhibitors is an effective treatment for patients in the Middle East and North Africa (MENA) and Gulf regions.1 Selective COX-2 inhibitors such as celecoxib reduce pain effectively while decreasing the incidence of gastrointestinal adverse effects compared with ns- NSAIDs such as ibuprofen and naproxen.2 While COX-2 inhibitors have been correlated with evidence of adverse cardiovascular outcomes at higher doses in placebo-controlled trials,3,4 data from meta-analyses of observational studies have suggested that the use of traditional NSAIDs is also not free of cardiovascular and renal risk and that this risk may not be entirely attributed to COX-2 selectivity.5
To highlight the importance of having head-to-head comparison with regard to safety outcomes of the COX-2 inhibitor celecoxib, the Food and Drug Administration (FDA) mandated the conduct of the cardiovascular safety trial Prospective Randomized Evaluation of Celecoxib Integrated Safety versus Ibuprofen or Naproxen (PRECISION) as Phase IV post-marketing surveillance. Patients were randomly assigned, in a 1:1:1 ratio, to receive celecoxib (100 mg twice a day), ibuprofen (600–800 mg three times a day), or naproxen (375–500 mg twice a day).6 The mean durations of treatment and follow-up, respectively, were 20.8±16.0 and 34.2±13.4 months in the celecoxib group, 20.5±15.9 and 34.2±13.3 months in the naproxen group, and 19.6±16.0 and 33.8±13.6 months in the ibuprofen group. The trial demonstrated that celecoxib was similar in terms of cardiovascular safety when compared with ibuprofen and naproxen in the pooled PRECISION population of 24,081 patients with osteoarthritis (~90%) or rheumatoid arthritis (~10%).6 In addition, the PRECISION trial found lower risk of serious gastrointestinal (GI) events for celecoxib versus naproxen and ibuprofen and lower risk of renal events for celecoxib versus ibuprofen in the intention-to-treat population of the trial.6 A post-hoc analysis of the osteoarthritis (OA) population in PRECISION7 found that celecoxib conferred similar or lower risk of cardiovascular, GI, and renal adverse events (AEs) compared with ibuprofen or naproxen in patients with rheumatoid arthritis.
The objective of the current study was to conduct a cost-effectiveness analysis of the use of celecoxib versus ibuprofen and naproxen in OA patients from the perspective of United Arab Emirates (UAE) health-care system. While previous research on the cost-effectiveness of celecoxib versus ns-NSAIDs has been conducted in other countries from the MENA and Gulf regions, such as Algeria8 and Saudi Arabia,9 this is one of the first cost-effectiveness studies on celecoxib in UAE using clinical data from the PRECISION trial. Previously published cost-effectiveness models on the use of celecoxib versus ns-NSAIDS8–12 have been limited in that they use pooled probabilities of adverse events data from multiple active comparator trials such as TARGET, CONDOR, CLASS, and MEDAL trials. This could be a source of significant variability in model results given varying inclusion/exclusion criteria across trials, inclusion of some patients with rheumatoid arthritis, varying therapeutic doses, and differential underlying patient risk across selected trials. Relying on a single source for safety parameters from a comprehensive safety evaluation such as the randomized, double-blind PRECISION trial with adjudicated endpoints allows for the opportunity to validate previous findings.
Methods
The study used a discrete-state Markov cohort model (Figure 1), adapted from a prior published economic model for OA used by the National Institute of Clinical Excellence (NICE).13 Incremental costs per quality adjusted life year (QALYs) gained from reduced incidence of three safety domains examined in PRECISION were modelled: major adverse cardiovascular events (MACE), serious GI, and renal events. Patients experience an elevated risk of AEs during the treatment period and can transition to any of the three AE states, which leads to reductions in quality of life, accumulation of AE management costs and increased risk of excess mortality. The three AE states serve as tunnel states before they transition to long-term post-AE recovery states, which are assumed to have persistent health effects and are also associated with excess mortality, albeit to a smaller extent.
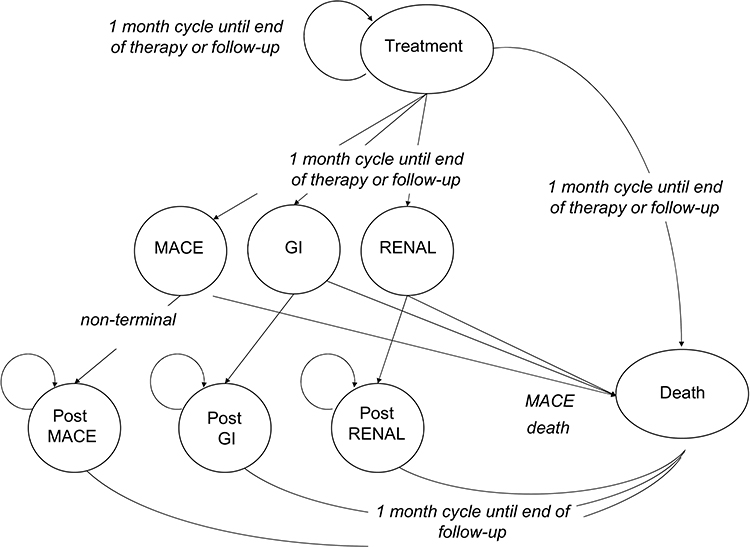 |
Figure 1 Schematic of Markov model used in the study. |
As our modelling effort used aggregate, published data from the PRECISION trial, it was waived from IRB review. Any data inputs from the PRECISION trial used in the model are free to access by referring to the relevant cited reference.
Patient Population
The model included parameters describing demographics, clinical characteristics, and relative safety estimates of the intention-to-treat OA patient cohort in PRECISION with a mean age of 64 years, 64% female, and 47% prior aspirin use.7 Ibuprofen had higher risk of MACE, serious GI and renal events than celecoxib; naproxen had similar MACE and renal risk but elevated serious GI risk compared with celecoxib (Table 1 – Panel A).
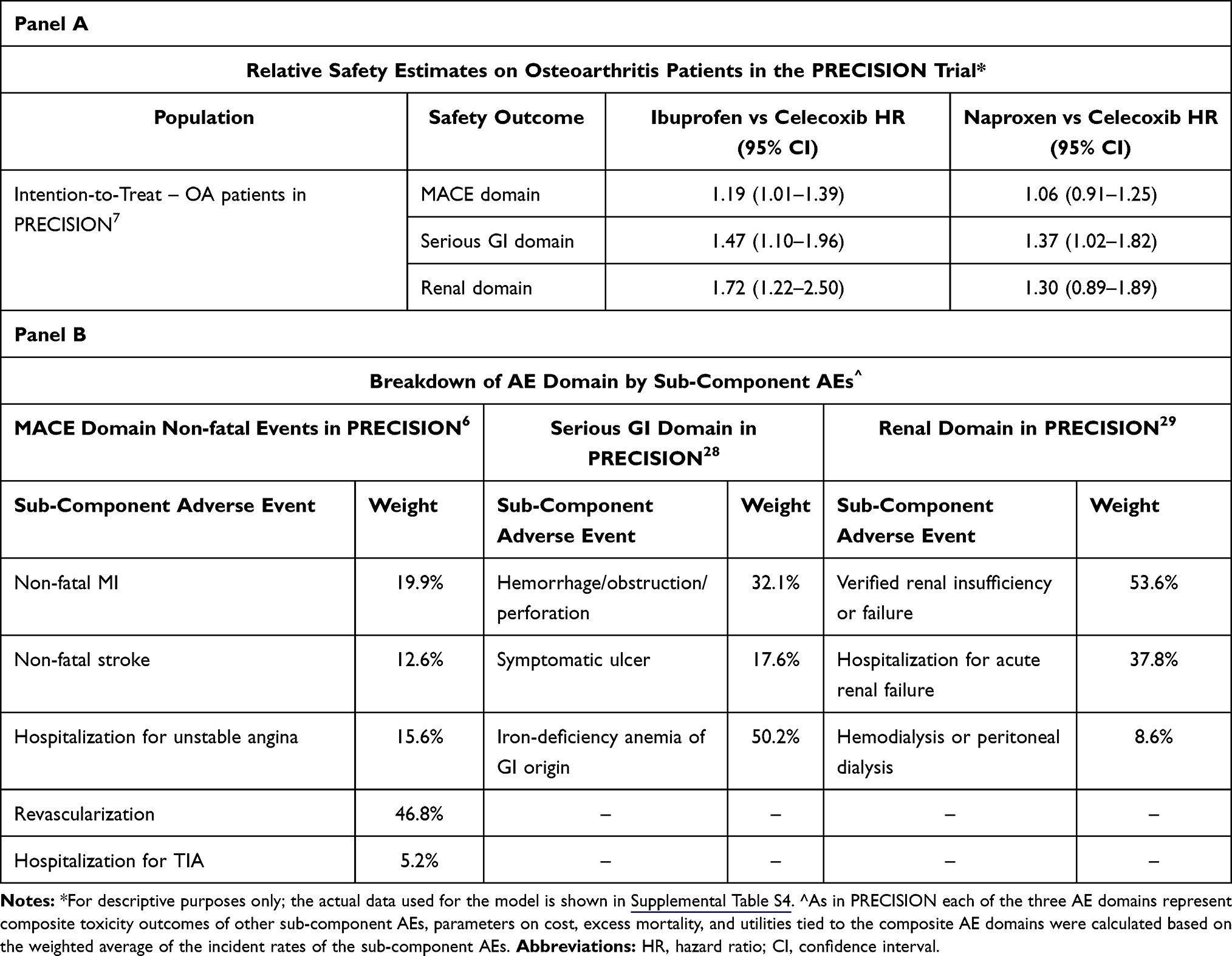 |
Table 1 Relative Safety Estimates on Osteoarthritis Patients in the PRECISION Trial (Panel A) and Calculated Sub- Component AE Weights (Panel B) |
While the country setting for this study reflects the healthcare utilization in UAE, clinical inputs were derived from publications on the OA population in PRECISION and assumed generalizable to UAE. Although PRECISION randomized 21,645 patients from 926 centers in 13 countries, this decision is substantiated by the fact that there is no clinical evidence to suggest that the clinical safety outcomes would differ by country setting. Any differences from the representative OA patients in PRECISION and OA patients in UAE were assumed to not influence model results as baseline GI risk is not affected by patient’s age14 and analyses of the primary composite outcome among prespecified subgroups showed no significant interactions for any pairwise comparison in PRECISION.6
Model Description
The model time horizon is 30 months (consistent with average follow-up in PRECISION) where each cycle has a length of 1 month. Treatment continues until the end of the treatment period, until occurrence of one of the three toxicities domains, or early treatment discontinuation, as observed in the clinical data from the trial. As the PRECISION trial demonstrated negligible differences across treatment agents with respect to time to drug discontinuation and time to non-retention,6 the model does not include differential treatment discontinuation by comparator or switching between comparators. Over 30 months of follow-up, 61.6% of patients discontinued study treatment in the OA arm in PRECISION.7 The monthly probability of discontinuation (Table S1) was equally applied across the three study drugs as it impacts treatment acquisition costs over time. A discounting rate of 3% over the time horizon was used for both cost and health outcomes.
Outcomes
Previous models8–12 discretely model toxicity by each individual state of myocardial infarction, stroke, heart failure, symptomatic ulcer, GI bleeding, for example, and source clinical probabilities of occurrence as well as cost and utility inputs from multiple trials and sources.
In PRECISION each of the three AE domains represent composite toxicity outcomes of other sub-component AEs. The MACE domain includes the composite of death from cardiovascular causes, non-fatal myocardial infarction; non-fatal stroke, coronary revascularization or hospitalization for unstable angina or transient ischemic attack. The serious GI events domain includes the composite of hemorrhage, gastric outlet obstruction, perforation, symptomatic gastric of duodenal ulcer. The renal events domain includes the composite of serum creatinine level of ≥2.0 mg/dL, hospitalization for acute renal failure, initiation of hemodialysis or peritoneal dialysis (Table 1 – Panel B).
Parameters on cost, excess mortality, and utilities tied to these three composite AE domains were calculated based on the weighted average of the incident rates of the sub-component AEs (e.g. symptomatic ulcer) mentioned above times each individual sub-component AE’s cost, excess mortality, and utility. The contributing weight of each sub-component AE was derived by taking the proportion of the incident rate for that particular sub-component AE as part of the overall domain.
Cost Inputs
AE management cost inputs for the model were derived from de-identified billing data from Dubai Administrative Billing Claims (year 2018). Mean cost per patient on outpatient, inpatient, and physician encounters were obtained by a query of pre-specified diagnosis codes in any claim field (Table S2) and a weighted average for the AE management cost of each composite domain was calculated (Table 2).
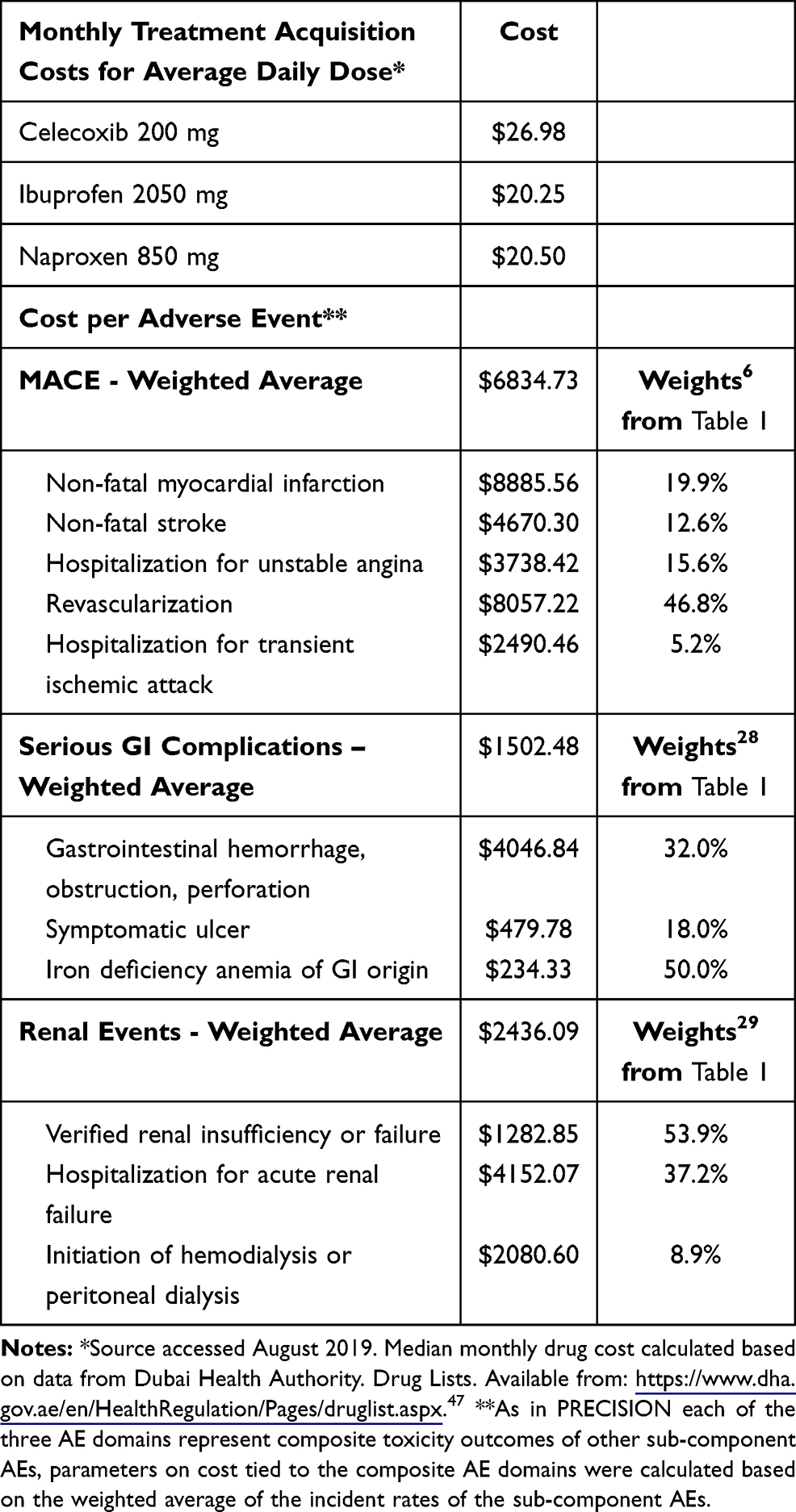 |
Table 2 Cost Model Parameters |
As data are limited for UAE on annual post-AE recovery costs, they were assumed to constitute 10% of the costs for the management of the index event. In the original model by NICE10 as well as in other cost-effectiveness models in the UK11 and Sweden,12 post-AE recovery costs constitute from <5% (for serious GI event) to up to 20% (for stroke) of the cost of the originating AE and contribute only negligible costs given the short time horizon of the study and when combined with the context of small absolute event rates of the three AE domains.
Information on monthly drug treatment cost for naproxen, ibuprofen and celecoxib was derived from UAE Ministry of Health and Prevention’s published prices (August 2019) on most prevalent package size and dosages. The dosage of drug package labels was standardized to the average daily dosage in the PRECISION trial (2050 mg for ibuprofen, 850 mg for naproxen, and 210 mg for celecoxib) and the median pill cost across various package labels was used to calculate monthly treatment acquisition costs (Table 2). Costs were converted to USD using an exchange rate of 3.67 AED per 1 USD.
While UAE has experienced deflation at a rate of −2% per annum over the past two years since 2018, the medical sector has remained at 0% change since 2018.15 As such, cost inputs coming from sources used in 2018 and 2019 are reasonable approximations for the costs of 2020 as well.
Clinical Inputs
The main data source for the probabilities of incident toxicities was the PRECISION trial7 (Table S3). An additional targeted literature review was conducted to obtain representative utility information and excess mortality on AE and post-AE health states in the model.
For ease of comparison across studies, model inputs were borrowed from the original NICE model when AE outcome definitions were overlapping (e.g. non-fatal myocardial infarction); values for inputs specific only to the PRECISION study (e.g. revascularization) were extracted from the published literature so they are clinically coherent with the values of outcomes in the original model.13
Quality of Life
The model assumed equal clinical efficacy among comparators with respect to alleviating OA pain as the PRECISION trial showed that clinical efficacy differences across comparators were smaller than the clinically meaningful threshold.6 Quality of life impact was modeled based on the differential incidence of toxicities across comparators. Utility weight of 0.723 was used for OA patients on NSAIDs treatment16 as well as age- and sex-specific background utilities (0.79 for men and 0.76 for women) as previously done elsewhere.16,17 Cycle-specific utilities were calculated by multiplying the OA and background utility weights by AE-specific utility weights while in an AE state or post-AE state (Table 3). Utility weights were sourced by searching the Tufts Cost-Effectiveness Analysis Registry.
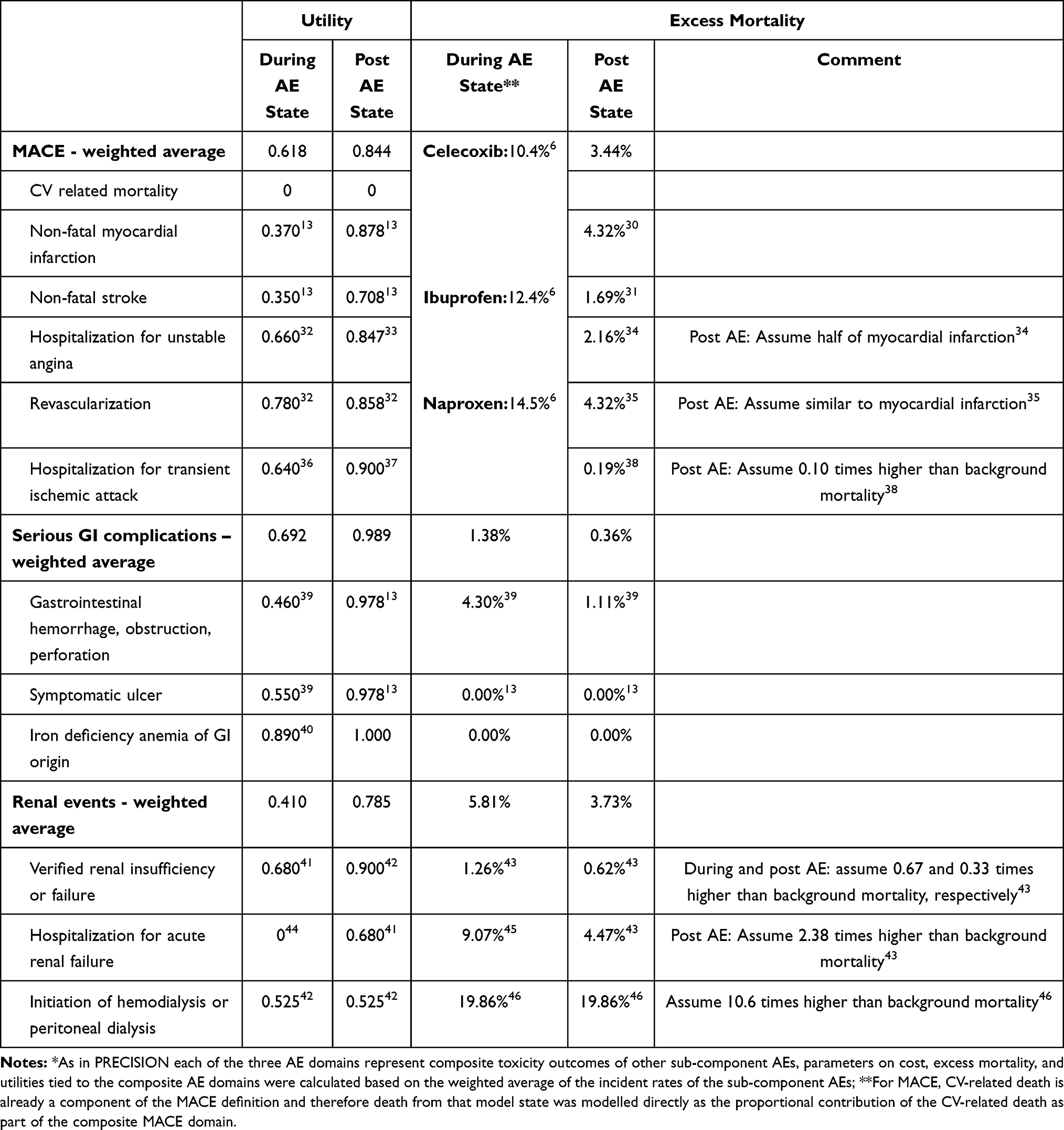 |
Table 3 Utility and Excess Mortality Model Parameters* |
Mortality
Death was only a tertiary endpoint in the PRECISION trial with overall 1.73% of patients dying over the course of 34.1 months of average follow-up. As PRECISION was a trial conducted in 13 countries over 10 years, the background mortality is a mix of various countries and time periods. About 80% of PRECISION participants came from the USA and therefore mortality was modeled indirectly using background mortality for UAE. The age of the cohort during each cycle in the treatment and post-treatment periods determined the appropriate background mortality (Table S4).
For MACE, CV-related death is already a component of the MACE definition and therefore death from that model state was modeled directly as the proportional contribution of the CV-related death as part of the composite MACE domain; specifically, 10.4% of MACE events were terminal for celecoxib while for ibuprofen and naproxen they were 12.4% and 14.5%, respectively (Table 3).6
For the GI and renal domains as well as the post-MACE, post-GI, and post-renal, the elevated risk of death was modeled indirectly using AE excess mortality parameters (Table 3). For those five states, cycle-specific mortality was calculated from the interaction between the age- and sex-specific background mortalities and excess mortality due to AEs while in a particular AE or post-AE recovery state.
Sensitivity Analyses
Deterministic sensitivity analysis (DSA) was conducted by varying select model parameters by 10–20% from their base case value or by setting the relative safety estimates at the low and high 95% confidence interval bounds. Additionally, as medication cost was obtained using the median package price for each drug agent, we examined the variability of results by setting the monthly medication cost at the 25th and 75th percentile of the distribution of prices. Probabilistic sensitivity analyses (PSA) were conducted by varying model parameters at the same time in 5000 model runs. The distributions used for the PSA and associated probabilistic parameters are shown in Table S5.
Results
Over a time horizon of 30 months, the total average cost per patient was $812.88 for celecoxib, $775.26 for ibuprofen, and $731.17 for naproxen while costs attributed to toxicities were the lowest with celecoxib overall ($360.26, $438.31, and $388.60, respectively) as well as per each individual toxicity domain (Table 4). Drug acquisition costs ($452.63, $336.96, and $342.57, respectively) and costs for the management of MACE ($293.77, $346.38, and $310.03, respectively) constituted the majority of total patient costs over the time horizon. Incremental total costs per patient were $37.62 higher for celecoxib versus ibuprofen (due to $115.67 higher drug acquisition costs but −$78.05 offset in toxicities cost) and $81.71 higher versus naproxen (due to $110.05 higher drug acquisition costs but −$28.35 offset in toxicities cost). The cost of post-toxicities management was negligible.
 |
Table 4 Model Results – Cumulative Outcomes and Cost per Patient |
Patients treated with celecoxib had more incremental LYs and QALYs compared with ibuprofen (ΔLYs: 0.0030; ΔQALYs: 0.0033) and naproxen (ΔLYs: 0.0028; ΔQALYs: 0.0021). The incremental cost-effectiveness ratio (ICER) was $12,676 per LY and $11,502 per QALY gained for celecoxib versus ibuprofen and $29,092 per LY and $39,779 per QALY for celecoxib versus naproxen (Table 4).
In deterministic sensitivity analyses, the most influential model parameters were those for HR for MACE relative safety, monthly drug costs, and HR for renal events relative safety (Figure 2). Setting the relative safety estimates for MACE and renal events at the upper 95% HR confidence intervals (i.e. much higher relative safety for celecoxib vs NSAIDs) resulted in cost-effectiveness estimates that were more favorable for celecoxib than base case results. Conversely, setting those parameters at the lower 95% bound resulted in much higher cost-effectiveness ratios (sometimes as high as $188,600 for celecoxib vs naproxen). Such big variation is likely due to the fact that toxicities rates are generally small leading to small but very sensitive changes in incremental QALYs and therefore the ICER. Setting monthly drug acquisition costs at the 25th and 75th percentile of the price of the average prescription for celecoxib or NSAIDs resulted in sensitive ICER estimates varying between <$0 and ~$45,000 for celecoxib versus ibuprofen and <$0 and ~$93,000 versus naproxen. Inputs on costs or utilities related to managing toxicities had little impact on model results.
 |
Figure 2 Tornado diagrams on deterministic sensitivity analyses: celecoxib vs ibuprofen (top) and vs naproxen (bottom). |
Country-specific willingness-to-pay thresholds are difficult to determine from available evidence as various methodologies exist.18 The World Health Organization CHOICE (CHOosing Interventions that are Cost-Effective) project has recommended thresholds of 1–3 times the gross domestic product (GDP) per capita, with those interventions meeting the <1 GDP threshold considered highly cost-effective.19 Therefore, we examined the cost-effectiveness at WTP thresholds of near 1 GDP (~$40,000 in UAE) and 3 GDP per capita (~$120,000 in UAE). Probabilistic sensitivity analyses of 5000 model runs demonstrated celecoxib to be 81% cost-effective versus ibuprofen and 50% versus naproxen at 1 GDP threshold (Figures S1 and S2). At threshold near 3 times GDP per capita, celecoxib was 95% cost-effective versus ibuprofen and 85% versus naproxen.
Discussion
Our study is also one of the first ones to evaluate the cost-effectiveness of celecoxib from UAE third payer perspective. Having the perspective of our model being that of UAE, the study findings could have value in contextualizing OA management decisions in other countries from the MENA and Gulf regions. With the trend of people older than 65 becoming one of the fastest growing demographics groups,20 those countries are facing an increasing burden of chronic diseases, including OA, and higher demand for health-care services.21 This is happening at a time when healthcare expenditure as a proportion of GDP in those countries is already increasing and higher costs are partially attributed to inefficiencies of the largely public, government-run financing of health-care delivery.20 To address the issue of increasing costs, investments in privatization of the health-care system have been suggested with Saudi Arabia, for example, most recently outlining a plan to privatize the healthcare system under the reforms of the National Transformation Program and Saudi Vision 2030.22,23 The effect and cost of these reforms, however, would not be known for some time. UAE, with its mostly private financing of health care, has informally been serving as a model example to other countries that have recently started transitioning from largely public to private health-care financing.24,25 Other countries from the region could refer to our study results in an attempt to compare how any previous cost-effectiveness estimates on the management of OA patients may change under ongoing health-care system reforms.
A previous model from an Algerian perspective8 found celecoxib to be cost-effective versus ibuprofen (ICER $508.94 per QALY) and naproxen (ICER $322.25 per QALY) over a time horizon of 6 months, while a similarly structured model from a Saudi Arabian perspective found celecoxib to be cost-effective versus ibuprofen with ICER $1805.00 per QALY; naproxen was not modelled.9 Over a long-term horizon of 30 months (of which ~20 months on treatment), in our model we found celecoxib 100 mg twice daily to be a cost-effective treatment compared with ibuprofen but equally likely cost-effective as naproxen at a threshold of 1 times GDP. At thresholds near 3 times GDP per capita, celecoxib was at least 85% cost-effective against both comparators. The difference in ICER scale between our study and previous studies could be due to differences in toxicities risk estimates in source trials of prior models (e.g. based on pooled estimates from CONDOR, MEDAL, CLASS, EDGE and TARGET trials) compared with what was observed in the head-to-head PRECISION trial, as well as differences in input cost parameters.
In secondary published analyses of the PRECISION trial, where all major NSAID toxicity endpoints, including all-cause mortality, were modelled as a composite outcome, 4.1% of subjects sustained any major toxicity in the celecoxib arm, 4.8% in the naproxen arm (overall 17% higher than celecoxib), and 5.3% in the ibuprofen arm (overall 29% higher than celecoxib).26 Our study findings indicate similar directionality as the costs attributed to managing toxicities in our model were 7.9% higher for naproxen versus ibuprofen and 21.7% higher for ibuprofen versus celecoxib. In our model, any cost savings in managing toxicities when on treatment with celecoxib were offset by the generally higher drug acquisition cost of celecoxib, especially in the comparison versus naproxen. As in PRECISION celecoxib had similar rates to naproxen with respect to MACE (HR = 1.06 (0.91–1.25)) and renal domains (1.30 (0.89–1.89)) (Table 1 – Panel A), cost savings generated from lower rates of serious GI events did not fully make up for $110.05 higher monthly drug acquisition cost for celecoxib. This could explain why celecoxib is equally likely to be cost-effective compared with naproxen at the more conservative threshold of 1 times GDP per capita.
Generally, model results were sensitive to the input for drug acquisition costs, which we sourced as the median package price for each of the comparators as published by UAE Ministry of Health and Prevention price list. A limitation of this approach is that we did not know the actual market share for each type of manufacturer’s brand or formulation (e.g. extended/sustained release) used in UAE. Future research efforts should incorporate market share in the analysis in order to calculate monthly drug acquisition costs accurately. Additionally, although we sourced toxicities cost inputs from Dubai claims data, we assume that they are applicable to UAE overall as Dubai together with Abu Dhabi – also with mostly private health-care services – are the two largest emirates in UAE.24 While previous models focused on sensitivity analysis to examine the impact of age and baseline GI and cardiovascular risks, data from PRECISION highlighted that relative safety estimates are not modified by prior aspirin use or use of NSAID for primary or secondary cardiovascular risk category prevention.6
It should be mentioned that our analysis did not consider the indirect costs of OA (productivity loss and absenteeism), which are substantial and of similar magnitude as direct costs.27 Transient AEs (e.g. dyspepsia, nausea, diarrhea, constipation, insomnia, pruritus, vomiting, dizziness, somnolence) were not modeled as their costs and effects are also negligible compared with those of persistent AEs and are expected to only marginally impact results. The three domains of persistent AE events were considered mutually exclusive and patients could only have one AE in each treatment cycle. Additionally, once the first serious AE had occurred, another one could not explicitly occur in the model. Although this may not be entirely realistic, it is necessary to make the model workable and is unlikely to change the results significantly given the small incidence of those events. This assumption was made by the original OA economic model on which our model is based.13 A limitation to the approach is that we modeled mortality indirectly using assumptions for excess mortality associated with each toxicity.
Additionally, despite the higher than anticipated non-retention rate on treatment in PRECISION, it could reflect real-world use of pharmacologic pain management consistent with clinical practice. Dose up-titration in OA patients in PRECISION was allowed for naproxen and ibuprofen but not celecoxib 100 mg twice daily (due to regulatory restrictions in the USA), which may have affected the results observed in the PRECISION trial. However, we should expect this to not hinder the ability to generalize and use the results from PRECISION for the current study as OA management practices in the Middle East do follow those of Western countries.9
Conclusion
Our study is one of the first to examine the cost-effectiveness of celecoxib in UAE using clinical data from the randomized, double-blind PRECISION trial with adjudicated safety endpoints for adverse cardiovascular, gastrointestinal, and renal events. From a UAE perspective, our study found celecoxib to be a long-term cost-effective treatment for osteoarthritis patients when compared with ibuprofen at a decision threshold of 1 times GDP per capita, and equally likely as naproxen to be cost-effective.
Funding
The PRECISION trial was sponsored by Pfizer.
Disclosure
Earlier versions of this analysis were presented at International Society for Pharmacoeconomics and Outcomes Research (ISPOR) 2020, USA as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” (Ahmed OH, Chirikov V, Walker C, Stephens JM, Schepman P, Chambers R, Bakir M, Poorman G, Haider S. Cost-Effectiveness of Celecoxib Versus Ibuprofen and Naproxen In Patients With Osteoarthritis In United Arab Emirates And Saudi Arabia Based On Results From The Precision Trial. Value in Health. 2020 May 1;23:S130. https://www.valueinhealthjournal.com/article/S1098-3015(20)30488-5/abstract).
V Chirikov and J Stephens are employees of Pharmerit International - an OPEN Health Company. P Schepman and R Chambers are employees of Pfizer and may own stock options. M Bakir is an employee of Upjohn Export B.V. and may own sotck options. At the time of the study conduct, C Walker, G Poorman and S Haider were employees of Pfizer. Pharmerit International - an OPEN Health Company received funding from Pfizer to conduct the study. C Walker is now an employee of Viatris and may own stock options. The authors report no other conflicts of interest in this work.
References
1. Zeidan AZ, Al Sayed B, Bargaoui N, et al. A review of the efficacy, safety, and cost‐effectiveness of COX‐2 inhibitors for Africa and the Middle East region. Pain Pract. 2013;13(4):316–331. doi:10.1111/j.1533-2500.2012.00591.x
2. Whittle B. COX-1 and COX-2 products in the gut: therapeutic impact of COX-2 inhibitors. Gut. 2000;47(3):320–325. doi:10.1136/gut.47.3.320
3. Solomon SD, McMurray JJ, Pfeffer MA, et al. Cardiovascular risk associated with celecoxib in a clinical trial for colorectal adenoma prevention. N Engl J Med. 2005;352(11):1071–1080. doi:10.1056/NEJMoa050405
4. Bhala N, Emberson J, Merhi A, et al.; Coxib and traditional NSAID Trialists’(CNT) Collaboration. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet. 2013;382(9894):769–779.
5. Walker C, Biasucci LM. Cardiovascular safety of non-steroidal anti-inflammatory drugs revisited. Postgrad Med. 2018;130(1):55–71. doi:10.1080/00325481.2018.1412799
6. Nissen SE, Yeomans ND, Solomon DH, et al. Cardiovascular safety of celecoxib, naproxen, or ibuprofen for arthritis. N Engl J Med. 2016;375(26):2519–2529. doi:10.1056/NEJMoa1611593
7. Solomon DH, Husni ME, Wolski KE, et al. Differences in safety of nonsteroidal antiinflammatory drugs in patients with osteoarthritis and patients with rheumatoid arthritis: a Randomized Clinical Trial. Arthritis Rheumatol. 2018;70(4):537–546. doi:10.1002/art.40400
8. Hammoumraoui N, Kherraf SA, Mould-Quevedo J, Ismail TA. The cost-effectiveness of celecoxib versus non-steroidal anti-inflammatory drugs plus proton-pump inhibitors for treating osteoarthritis in Algeria. J Health Econ Outcomes Res. 2013;1(2):184–199. doi:10.36469/9865
9. Nasef SA, Shaaban AA, Mould-Quevedo J, Ismail TA. The cost-effectiveness of celecoxib versus non-steroidal anti-inflammatory drugs plus proton-pump inhibitors in the treatment of osteoarthritis in Saudi Arabia. Health Econ Rev. 2015;5(1):13. doi:10.1186/s13561-015-0053-7
10. Chen Y, Jobanputra P, Barton P, et al. Cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs (etodolac, meloxicam, celecoxib, rofecoxib, etoricoxib, valdecoxib and lumiracoxib) for osteoarthritis and rheumatoid arthritis: a systematic review and economic evaluation. Health Technol Assess (Rockv). 2008;12(11):1–278. doi:10.3310/hta12110
11. Brereton N, Winn B, Akehurst R. The cost-effectiveness of celecoxib vs diclofenac in the treatment of osteoarthritis in the UK; an update to the NICE model using data from the CONDOR trial. J Med Econ. 2012;15(3):465–472. doi:10.3111/13696998.2012.659778
12. Brereton N, Pennington B, Ekelund M, Akehurst R. A cost-effectiveness analysis of celecoxib compared with diclofenac in the treatment of pain in osteoarthritis (OA) within the Swedish health system using an adaptation of the NICE OA model. J Med Econ. 2014;17(9):677–684. doi:10.3111/13696998.2014.933111
13. National Collaborating Centre for Chronic Conditions. Appendix D, Osteoarthritis: National Clinical Guidelines for Care and Management in Adults. London: Royal College of Physicians; 2008:2014.
14. Gore M, Tai KS, Sadosky A, Leslie D, Stacey BR. Use and costs of prescription medications and alternative treatments in patients with osteoarthritis and chronic low back pain in community‐based settings. Pain Pract. 2012;12(7):550–560. doi:10.1111/j.1533-2500.2012.00532.x
15. Federal Competitiveness and Statistics Authority. Consumer Price Index (CPI) Report, UAE; April, 2020. Available from: www.fcsa.gov.ae.
16. Latimer N, Lord J, Grant RL, O’Mahony R, Dickson J, Conaghan PG. Cost effectiveness of COX 2 selective inhibitors and traditional NSAIDs alone or in combination with a proton pump inhibitor for people with osteoarthritis. BMJ. 2009;339:b2538. doi:10.1136/bmj.b2538
17. Wielage RC, Bansal M, Andrews JS, Klein RW, Happich M. Cost-utility analysis of duloxetine in osteoarthritis: a US private payer perspective. Appl Health Econ Health Policy. 2013;11(3):219–236. doi:10.1007/s40258-013-0031-3
18. McDougall JA, Furnback WE, Wang BC, Mahlich J. Understanding the global measurement of willingness to pay in health. J Mark Access Health Policy. 2020;8(1):1717030. doi:10.1080/20016689.2020.1717030
19. Adam T. Making Choices in Health: WHO Guide to Cost-Effectiveness Analysis. Vol. 1. World Health Organization; 2003.
20. Ram P. Management of Healthcare in the Gulf Cooperation Council (GCC) countries with special reference to Saudi Arabia. Int J Acad Res Bus Soc Sci. 2014;4(12):24. doi:10.6007/IJARBSS/v4-i12/1326
21. Khoja T, Rawaf S, Qidwai W, Rawaf D, Nanji K, Hamad A. Health care in Gulf Cooperation Council countries: a review of challenges and opportunities. Cureus. 2017;9(8). doi:10.7759/cureus.1586
22. Alharbi MF. An analysis of the Saudi health-care system’s readiness to change in the context of the Saudi National Health-care Plan in Vision 2030. Int J Health Sci. 2018;12(3):83.
23. Rahman R, Alsharqi OZ. What drove the health system reforms in the Kingdom of Saudi Arabia? An analysis. Int J Health Plann Manage. 2019;34(1):100–110. doi:10.1002/hpm.2584
24. Koornneef E, Robben P, Blair I. Progress and outcomes of health systems reform in the United Arab Emirates: a systematic review. BMC Health Serv Res. 2017;17(1):672. doi:10.1186/s12913-017-2597-1
25. El-Hassan O, Sharif A, Al MR, Blair I. Tracking the implementation of electronic medical records in Dubai, United Arab Emirates, using an adoption benchmarking tool. Stud Health Technol Inform. 2017;245:64–68.
26. Solomon DH, Husni ME, Libby PA, et al. The risk of major NSAID toxicity with celecoxib, ibuprofen, or naproxen: a secondary analysis of the PRECISION Trial. Am J Med. 2017;130(12):1415–1422.e4. doi:10.1016/j.amjmed.2017.06.028
27. Hunsche E, Chancellor JV, Bruce N. The burden of arthritis and nonsteroidal anti-inflammatory treatment. Pharmacoeconomics. 2001;19(1):1–15. doi:10.2165/00019053-200119001-00001
28. Yeomans ND, Graham DY, Husni ME, et al. Randomised clinical trial: gastrointestinal events in arthritis patients treated with celecoxib, ibuprofen or naproxen in the PRECISION trial. Aliment Pharmacol Ther. 2018;47(11):1453–1463. doi:10.1111/apt.14610
29. Obeid S, Libby P, Husni ME, et al. Cardiorenal risks of celecoxib, naproxen or ibuprofen in arthritis patients: a sub-anaylsis from the PRECISION Trial. Circulation. 2017;136(suppl_1):A20401–A20401.
30. Fihn SD, Vaughan-Sarrazin M, Lowy E, et al. Declining mortality following acute myocardial infarction in the Department of Veterans Affairs Health Care System. BMC Cardiovasc Disord. 2009;9(1):44. doi:10.1186/1471-2261-9-44
31. Lakshminarayan K, Anderson DC, Jacobs DR, Barber CA, Luepker RV. Stroke rates: 1980–2000 the Minnesota Stroke Survey. Am J Epidemiol. 2009;169(9):kwp029. doi:10.1093/aje/kwp029
32. Parthan A, Leahy KJ, O’Sullivan AK, et al. Cost effectiveness of targeted high-dose atorvastatin therapy following genotype testing in patients with acute coronary syndrome. Pharmacoeconomics. 2013;31(6):519–531. doi:10.1007/s40273-013-0054-5
33. Ara R, Pandor A, Stevens J, et al. Prescribing high-dose lipid-lowering therapy early to avoid subsequent cardiovascular events: is this a cost-effective strategy? Eur J Prev Cardiol. 2012;19(3):474–483. doi:10.1177/1741826711406616
34. Fox K, Collier T, Wood D, et al. Contemporary mortality due to acute myocardial infarction, unstable angina and exertional angina in a population in South East London. J Assoc Physicians. 2006;99(7):437–443. doi:10.1093/qjmed/hcl064
35. Weintraub WS, Boden WE. Reexamining the efficacy and value of percutaneous coronary intervention for patients with stable ischemic heart disease. JAMA Intern Med. 2016;176(8):1190–1194. doi:10.1001/jamainternmed.2016.3071
36. Wang Y, Xie F, Kong MC, Lee LH, Ng HJ, Ko Y. Cost-effectiveness of dabigatran and rivaroxaban compared with warfarin for stroke prevention in patients with atrial fibrillation. Cardiovasc Drugs Ther. 2014;28(6):575–585. doi:10.1007/s10557-014-6558-1
37. Kreisz FP, Merlin T, Moss J, Atherton J, Hiller JE, Gericke CA. The pre-test risk stratified cost-effectiveness of 64-slice computed tomography coronary angiography in the detection of significant obstructive coronary artery disease in patients otherwise referred to invasive coronary angiography. Heart Lung Circ. 2009;18(3):200–207. doi:10.1016/j.hlc.2008.10.013
38. Gattellari M, Goumas C, Biost FGM, Worthington JM. Relative survival after transient ischaemic attack: results from the Program of Research Informing Stroke Management (PRISM) study. Stroke. 2012;43(1):79–85. doi:10.1161/STROKEAHA.111.636233
39. Maetzel A, Krahn M, Naglie G The cost-effectiveness of celecoxib and rofecoxib in patients with osteoarthritis or rheumatoid arthritis. 605 Third Ave, New York, NY 10158-0012 USA: Wiley-Liss Div John Wiley & Sons Inc; 2001:S310–S310.
40. Retèl VP, Steuten LM, Foppen MHG, et al. Early cost-effectiveness of tumor infiltrating lymphocytes (TIL) for second line treatment in advanced melanoma: a model-based economic evaluation. BMC Cancer. 2018;18(1):895. doi:10.1186/s12885-018-4788-5
41. Luebke T, Brunkwall J. Cost-effectiveness of endovascular versus open repair of acute complicated type B aortic dissections. J Vasc Surg. 2014;59(5):1247–1255. doi:10.1016/j.jvs.2013.11.086
42. Hogan TJ, Elliott WJ, Seto AH, Bakris GL. Antihypertensive treatment with and without Benazepril in patients with chronic renal insufficiency. Pharmacoeconomics. 2002;20(1):37–47. doi:10.2165/00019053-200220010-00004
43. van Domburg RT, Hoeks SE, Welten GM, Chonchol M, Elhendy A, Poldermans D. Renal insufficiency and mortality in patients with known or suspected coronary artery disease. J Am Soc Nephrol. 2008;19(1):158–163. doi:10.1681/ASN.2006101112
44. Bae SC, Corzillius M, Kuntz KM, Liang MH. Cost-effectiveness of low dose corticosteroids versus non-steroidal anti-inflammatory drugs and COX-2 specific inhibitors in the long-term treatment of rheumatoid arthritis. Rheumatology (Oxford). 2003;42(1):46–53. doi:10.1093/rheumatology/keg029
45. Brown JR, Rezaee ME, Marshall EJ, Matheny ME. Hospital mortality in the United States following acute kidney injury. Biomed Res Int. 2016;2016:1–6. doi:10.1155/2016/4278579
46. Neovius M, Jacobson SH, Eriksson JK, Elinder C-G, Hylander B. Mortality in chronic kidney disease and renal replacement therapy: a population-based cohort study. BMJ Open. 2014;4(2):e004251. doi:10.1136/bmjopen-2013-004251
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.