Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Evaluating Glycemic Control Efficacy and Safety of the Oral Small Molecule Glucagon-Like Peptide 1 Receptor Agonist Danuglipron in Type 2 Diabetes Patients: A Systemic Review and Meta-Analysis
Authors Fatima H ![]() , Rangwala HS
, Rangwala HS ![]() , Mustafa MS
, Mustafa MS ![]() , Shafique MA
, Shafique MA ![]() , Abbas SR, Rizwan A, Fadlalla Ahmed TK
, Abbas SR, Rizwan A, Fadlalla Ahmed TK ![]() , Arshad A
, Arshad A ![]()
Received 6 October 2023
Accepted for publication 3 November 2023
Published 7 November 2023 Volume 2023:16 Pages 3567—3578
DOI https://doi.org/10.2147/DMSO.S439587
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Hareer Fatima,1 Hussain Sohail Rangwala,1 Muhammad Saqlain Mustafa,1 Muhammad Ashir Shafique,1 Syed Raza Abbas,2 Azra Rizwan,3 Tagwa Kalool Fadlalla Ahmed,4 Ainan Arshad3
1Department of Medicine, Jinnah Sindh Medical University, Karachi, Pakistan; 2Department of Medicine, Dow University of Health Sciences, Karachi, Pakistan; 3Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan; 4Department of Medicine, Ahfad University for Women, Omdurman, Al-Khartum, Sudan
Correspondence: Tagwa Kalool Fadlalla Ahmed, Department of Medicine, Ahfad University for Women, PO Box 167, Omdurman, Al-Khartum, Sudan, Tel +923412127759, Email [email protected]
Introduction: Diabetes Mellitus (DM) is a significant global health concern, with Type 2 DM (T2DM) being highly prevalent. Glucagon-Like Peptide 1 receptor agonists (GLP-1RA), such as Danuglipron, offer potential benefits in T2DM management. This meta-analysis examines the safety and efficacy of Danuglipron, focusing on adverse outcomes and glycemic parameters.
Methods: A systematic search was conducted in PubMed, Scopus, and Cochrane Library for RCTs involving Danuglipron till August 2023, following PRISMA guidelines. The Cochrane risk-of-bias tool was used for quality assessment. Adverse outcomes (diarrhea, nausea, vomiting, headache, decreased appetite, dyspepsia, dizziness) and glycemic parameters like changes in HbA1C, fasting plasma glucose (FPG), and body weight were analyzed.
Results: Four RCTs published from 2021 to 2023 were included. Both doses of Danuglipron were associated with diarrhea (RR=2.66, 90% CI: 1.32 to 5.35, p=0.02), nausea (RR=5.5, 90% CI: 3.4 to 8.88, p< 0.00001), and vomiting (RR=5.98, 90% CI: 2.93 to 12.23, p=0.0001). The 120mg dose showed decreased appetite (RR=3.46, 90% CI: 1.57 to 7.62, p=0.01), dyspepsia (RR=4.04, 90% CI: 1.93 to 8.43, p=0.002), and dizziness (RR=5.08, 90% CI: 1.45 to 17.82, p=0.03). Reductions in HbA1C (SMD − 1.09, 90% CI − 1.39 to − 0.8, p < 0.00001), FPG (SMD − 1.10, 90% CI − 1.46 to − 0.75, p < 0.00001), and body weight (SMD − 1.08, 90% CI − 1.42 to − 0.74, p < 0.00001) were observed for both doses.
Conclusion: Danuglipron demonstrates potential for glycemic control and weight reduction in T2DM. Adverse outcomes include diarrhea, nausea, vomiting, and decreased appetite, with dose-related effects. Clinicians must weigh benefits against side effects when considering Danuglipron for T2DM management.
Keywords: diabetes mellitus, glucagon-like peptide 1 receptor agonists, Danuglipron, adverse outcomes, glycemic parameters
Introduction
Every year, an alarming toll of 1.5 million lives is attributed to Diabetes Mellitus (DM). The global prevalence of this condition is staggering, affecting approximately 422 million individuals, with a significant concentration in low and middle-income countries.1 Projections indicate a concerning trajectory in the diabetic patient population, with estimates anticipating a surge to 570 million individuals by 2030. Within this anticipated number, a staggering 90% are expected to be afflicted by Type 2 DM (T2DM).2 The Middle East, South Asia, and the Pacific Islands commonly exhibit elevated rates of DM. Among these regions, Pakistan stands out, finding itself among the nations with the most pronounced prevalence of DM, reaching approximately 30.8%.3
In the realm of clinical practice guidelines about managing T2DM without the use of insulin, the recommended approach involves initiating treatment escalation when dietary adjustments and physical activity prove insufficient in attaining the targeted glycemic levels. At this juncture, patients are typically commenced on an oral antihyperglycemic agent, such as Metformin, or a dipeptidyl peptidase‐4 inhibitor. Alternatively, an injectable glucagon-like peptide one receptor (GLP-1R) agonist could also be considered as part of the therapeutic strategy.4,5
In the context of T2DM, a noteworthy reduction in the incretin effect has been observed. This effect primarily involves the diminished activity of key incretin hormones, namely GLP-1 (glucagon-like peptide 1) and GIP (glucose-dependent insulinotropic peptide). The secretion of GLP-1 takes place within the body’s L cells located in the distal ileum and colon.6,7 Stimulation of the GLP-1R receptor triggers insulin release and a reduction in glucagon secretion in response to glucose levels. Additional functions encompass the slowing of gastric emptying, suppression of appetite, and facilitation of weight loss.8,9
The innovation of GLP-1R agonists has yielded encouraging outcomes, positively impacting metabolic parameters.6 Its administration has also demonstrated a substantial reduction in major cardiac events, independent of its impact on elevated blood glucose levels. This suggests the potential to enhance a patient’s cardiac profile concurrently with diabetes treatment.10
Presently accessible GLP-1R agonists, owing to their peptidic agonist structure, necessitate subcutaneous administration. Though compelling, this approach proves cumbersome for many patients, potentially leading to decreased adherence compared to those on oral medications. The limitation of this subcutaneous injection is that it can constrain patient usage and potentially hinder the feasibility of combining them in fixed-dose treatments with other small-molecule therapies for cardio-metabolic conditions.8,9 The only orally administered GLP-1 receptor agonist is semaglutide. However, it demands a fasting regimen both before and following intake.11,12
Danuglipron emerges as an orally administered GLP-1R agonist, serving dual purposes in managing T2DM and as a prospective weight loss therapy. Phase 1 trial findings highlight the potential of a Metformin and Danuglipron combination in diminishing glycemic levels and promoting considerable weight loss effects. In alignment with other GLP-1R agonists, it exhibits comparable adverse effects, predominantly manifesting in gastrointestinal discomfort, as reported in various clinical trials.13,14 While trials have not reported any instances of cardiotoxic events, it is worth noting that a small number of patients did experience arrhythmia and prolonged QT intervals.15
Following findings from other trials, Danuglipron is recommended to be administered twice daily, and its dosing can be independent of the timing of meals. Notably, in non-clinical studies comparing the efficacy of Danuglipron with other injectable GLP-1R agonists, similar patterns of glucose-dependent insulin release and increased satiety were observed.16 The degree of weight loss achieved through Danuglipron is similar to that of other subcutaneously injectable GLP-1R agonists when administered for the same duration of treatment. However, it’s important to note that GLP-1 is 30 times more potent than Danuglipron. As a result, higher doses are necessary to attain the desired beneficial effects.2,15 We aimed to systematically retrieve all currently available RCTs of Danuglipron in individuals with T2DM and pool the evidence by means of clinically relevant meta-analyses for outcomes of efficacy and safety.
Methodology
Data Sources and Search Strategy
This meta-analysis was performed according to the “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) guidelines.17 To ensure a comprehensive search for the systematic review and meta-analysis, databases of PubMed, Scopus and Cochrane Library were searched for published studies up to 31st August 2023. By using all of these databases, we aimed to minimize the potential for publication bias. In our search strategy, we utilized a carefully constructed search string to identify the studies relevant to our research. The search string included various combinations of key terms such as “Danuglipron”, “Diabetes”, “GLP-1 receptor agonist”, articles were retrieved and identified manually for further evaluation.
Inclusion Criteria
The inclusion criteria were established based on the following requirements: (1) RCTs published up to 31st August 2023. (2) Studies that reported 80mg and 120mg doses of Danuglipron (3) Comparison between Danuglipron vs Placebo. (4) Studies that reported Glycemic parameters. (5) Studies that reported adverse outcomes. (6) Studies that included patients regardless of any background glucose lowering therapy.
Data Extraction and Quality Assessment
Initially, titles and abstracts were screened to exclude studies that did not meet our eligibility criteria. To avoid duplication of articles, we utilized the EndNote Reference Library program. Full-text articles were retrieved and thoroughly examined to determine their suitability for inclusion in our meta-analysis. To ensure consistency and accuracy in data extraction, three authors (HF, HSR and SRA) were involved in the process of extracting relevant data from each included RCT. The data extracted from each study included baseline characteristics, intervention details, and outcomes. The primary outcome of interest in our meta-analysis was changes in HbA1C, FPG, bodyweight, HOMA-IR, FPI and fasting glucagon from baseline and secondary outcomes of interest were nausea, vomiting, diarrhea, headache, dyspepsia, abdominal distention, decreased appetite, hypoglycemia and dizziness.
To assess the quality of the included studies, two authors (HF and HSR) utilized the Cochrane risk-of-bias tool for randomized trials (RoB 2), aiming to assess the risk of bias within each included study.18 Any disagreement was resolved by consensus or consultation with a third investigator (SRA).
Statistical Analysis
For the statistical analysis of our meta-analysis, we employed the Review Manager Software Package (Review Manager, Version 5.4.1, The Cochrane Collaboration, 2020). To determine the significance between Danuglipron and placebo groups, we estimated the risk ratio (RR) with 90% confidence intervals (CIs). The results were reported as risk ratio (RR) for dichotomous outcomes and standard mean difference (SMD) for continuous outcomes with 90% confidence intervals (Cls). The results were pooled using a random-effects model, and forest plots were developed to examine the effects visually. I2 was used to assess the heterogeneity between the studies, and a value of I2 = 25–50% was considered mild, 50–75% as moderate, and > 75% as severe. A p-value of < 0.05 was considered significant in all cases. In case heterogeneity > 50%, sensitivity analysis was performed by the leave-one-out analysis method to find the study causing heterogeneity. Furthermore, subgroup analysis was performed based on the types of dose of Danuglipron.
Results
Studies Selection
Our initial search retrieved 26 studies. Duplication of 8 records were found which were then removed. 9 titles and abstract were excluded for irrelevance. Remaining of 9 studies were selected for further assessment because of relevance to subject. After that, exclusion of 5 studies was done out of which 2 studies were non RCTs. As a result, final selection included 4 RCTs2,11,13,16 for meta-analysis. (Supplemental Figure S1) illustrates the study selection process.
Study Characteristics
The main characteristics of the included studies are presented in Supplemental Table S1.
Two studies were published in 202311,13, one in 202216 and another one in 2021.2 Three studies assessed both 80mg and 120 mg doses of Danuglipron,11,13,16 while only one study did not asses 80mg dose.2 In our analyses, we merged data of 80mg LS and 80mg HS and similarly 120mg LF and 120mg HF in Saxena et al.13 In another study Saxena et al2 we merged 120mg BID and 120mg BID ST. The comparator arm was a placebo. All studies were double blinded and had a parallel-group design, and two were open-label. Duration of intervention was 4,8,12, and 16 weeks respectively.2,11,13,16 Overall risk of bias for the primary outcome was low in all studies.
Participant Characteristics
Across all trials, participants that met the inclusion criteria were 376 and mean age was 58.02 years (9.22), with mean duration of diabetes 9.02 years (6.87). There mean HbA1c at baseline was 8.16 mmol/mol (0.94), mean body weight was 92.3 kg (18.13), mean FPG mg. dl−1172.58(43.02), mean BMI was 32.9 Kg.m−2 (5.5). (Supplemental Table S1). In three studies, background glucose-lowering treatment comprised metformin either as monotherapy or in combination with another oral medication.2,11,13 In one study, there was no previous use of oral glucose lowering medication.16
Quality Assessment
The Cochrane risk of bias 2 tool was used to assess the studies, and the findings are presented in Supplemental Table 2. All our studies were considered to have minimal risk of bias, indicating a high level of reliability.
Adverse Outcome
Diarrhea was observed in patients receiving two doses of Danuglipron, 80mg and 120mg. In the subgroup analysis of the 80mg dose, data from three studies indicated that Danuglipron did not show a significant association with an increased risk of diarrhea compared to the placebo. However, this analysis had a considerable heterogeneity estimate of 57%. To address this, sensitivity analysis was performed, which revealed that the 80mg dose was indeed associated with a significant increase in diarrhea events (472%) (RR=5.72, 90% CI: 1.91 to 17.06, p=0.009, I2=0%) (Figure 1) (Supplemental Figures S2 and S3).
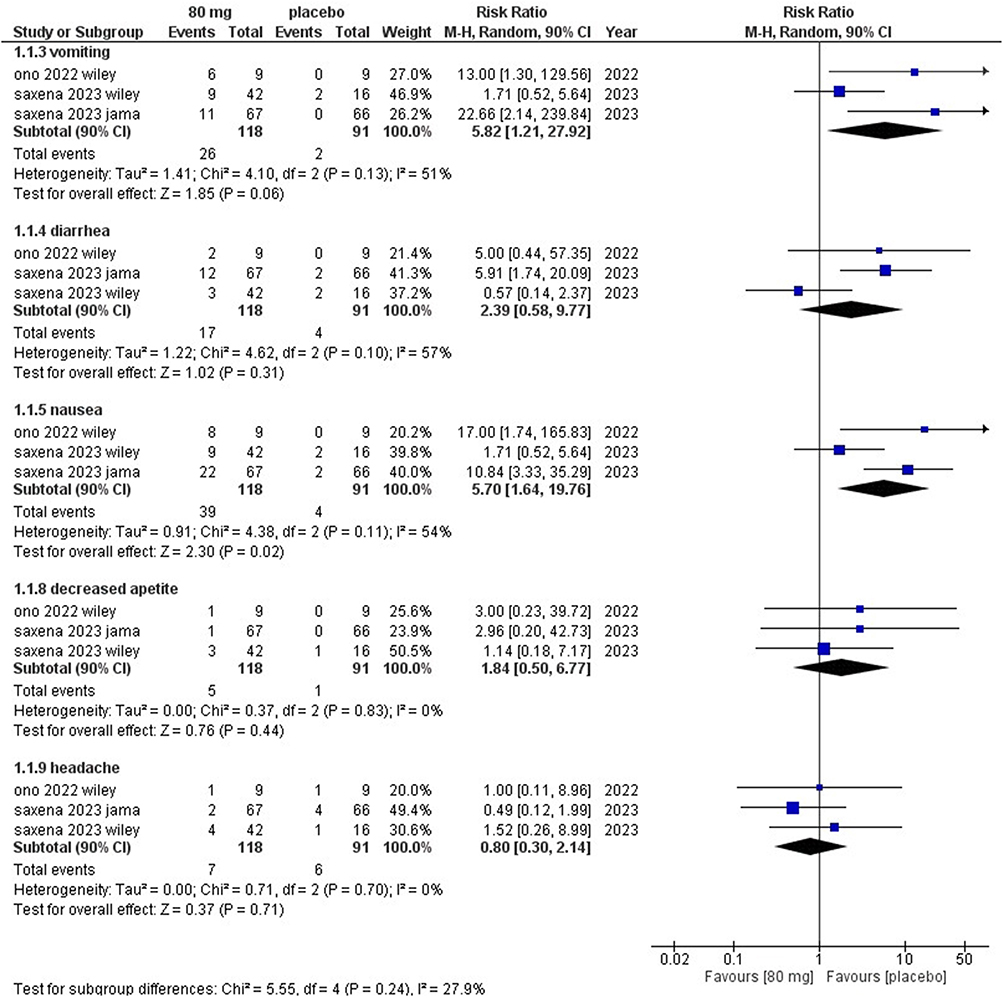 |
Figure 1 Summary plot for adverse outcomes 80mg. |
For the 120mg dose, the subgroup analysis involved four studies, showing an association with an increase in diarrhea events (186%), but the results were not statistically significant (RR=2.86, 90% CI: 1.13 to 7.2, p=0.06, I2=52%). However, upon conducting sensitivity analysis, the results became statistically significant (317%) (RR=4.17, 90% CI: 1.40 to 12.42, p=0.03, I2=39%). Surprisingly, our findings suggested that higher doses were associated with fewer diarrhea events (Figure 2) (Supplemental Figures S2 and S3).
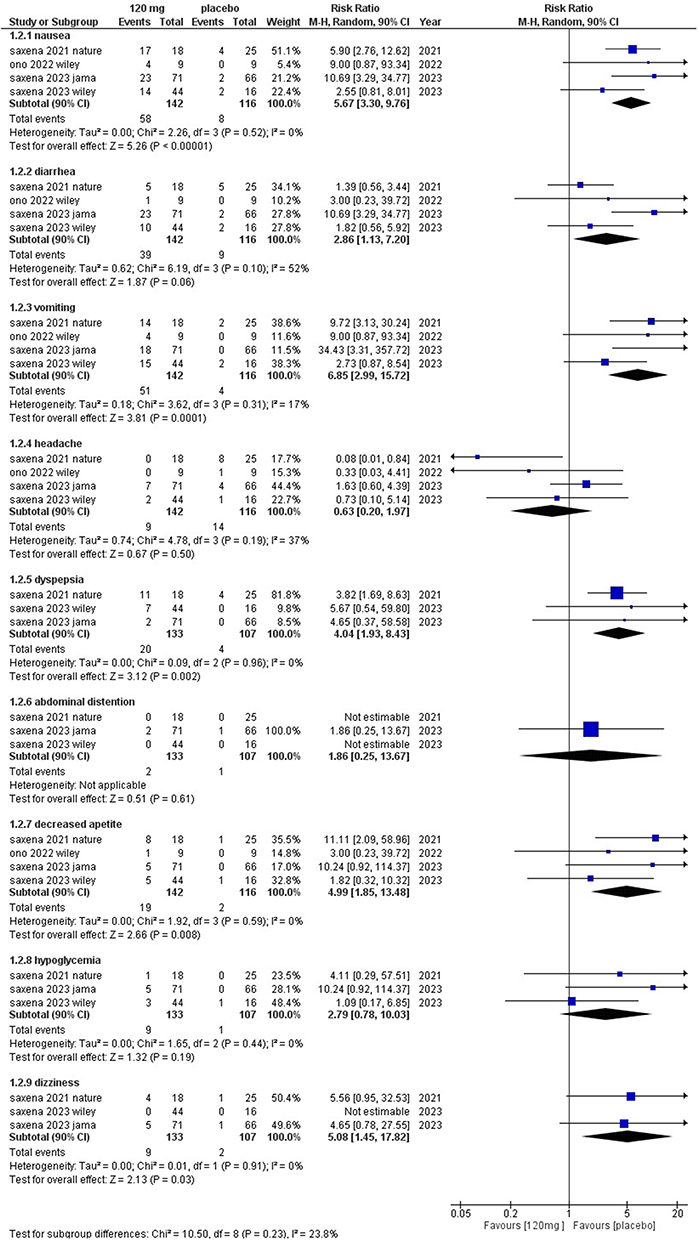 |
Figure 2 Summary plot for adverse outcomes 120mg. |
The pooled analysis of both doses revealed a significant association with an increased risk of diarrhea (166%) for patients taking Danuglipron (RR=2.66, 90% CI: 1.32 to 5.35, p= 0.02, I2=44%). After conducting sensitivity analysis (RR=4.71, 90% CI: 2.48 to 8.95, p<0.0001, I2=0%), the results remained significant, further supporting the link between Danuglipron and diarrhea risk (Supplemental Figures S2 and S3).
Upon conducting subgroup analysis, it was found that both the 80mg (20%) (RR=0.8, 90% CI: 0.3 to 2.14, p=0.71, I2=0%) and 120mg (37%) (RR=0.63, 90% CI: 0.2 to 1.97, p=0.5, I2=37%) doses of Danuglipron did not exhibit any significant difference in the occurrence of headaches when compared to the placebo. The combined pooled analysis also supported these findings, showing no statistically significant results for headaches between the Danuglipron doses and the placebo group (Figures 1 and 2) (Supplemental Figures S4).
The analysis of the drug’s 80mg (470%) and 120mg (467%) doses revealed a significant association with increased nausea. Interestingly, both doses demonstrated nearly identical percentages of nausea, suggesting that increasing the dose does not substantially increase nausea. Specifically, for the 80mg dose, the risk ratio (RR) was 5.70 (90% CI: 1.64 to 19.7, p=0.02, I2=54%), while for the 120mg dose, it was 5.67 (90% CI: 3.3 to 9.76, p<0.00001, I2=0%). The pooled analysis also corroborated these findings, indicating a risk ratio 5.5 (90% CI: 3.4 to 8.88, p<0.00001, I2=9%) (Figures 1 and 2) (Supplemental Figures S5 and S6).
On subgroup analysis of the 80mg Danuglipron dose (482%), the results indicated a non-significant association with an increase in vomiting when compared to the placebo (RR=5.82, 90% CI: 1.21 to 27.92, p=0.06, I2=51%). However, the sensitivity analysis revealed significant results (1640%) (RR=17.40, 90% CI: 3.28 to 88.43, p=0.005, I2=0%), suggesting a substantial effect of the drug on vomiting at this dosage (Figure 1) (Supplemental Figures S7 and S8).
In contrast, the 120mg Danuglipron dose (585%) showed a significant increase in vomiting events compared to the placebo (RR=6.85, 90% CI: 2.99 to 15.72, p=0.0001, I2=17%). The pooled analysis also demonstrated a significant increase in vomiting events associated with the drug (RR=5.98, 90% CI: 2.93 to 12.23, p=0.0001, I2=0%). These findings collectively suggest that an increase in dose may be related to a higher incidence of vomiting (Figure 2) (Supplemental Figures S7 and S8).
The 80mg Danuglipron dose (84%) showed no significant association with decreased appetite compared to the placebo. However, the 120mg dose (399%) was associated with a higher incidence of decreased appetite than the placebo (RR=4.99, 90% CI: 1.85 to 13.48, p=0.008, I2=0%). The combined pooled analysis also confirmed a significant increase in decreased appetite with Danuglipron compared to the placebo (RR=3.46, 90% CI: 1.57 to 7.62, p=0.01, I2=0%) (Figures 1 and 2) (Supplemental Figures S9).
Regarding other adverse outcomes of Danuglipron, such as dyspepsia, abdominal distention, and hypoglycemia, only dizziness was reported with the 120mg dose. The 80mg drug dose was excluded from the analysis due to insufficient available data.
The incidence of hypoglycemia and abdominal distention with Danuglipron did not differ significantly compared to the placebo. However, dyspepsia (304%) showed a significant increase in events with the drug (RR=4.04, 90% CI: 1.93 to 8.43, p=0.002, I2=0%), as well as dizziness (408%) (RR=5.08, 90% CI: 1.45 to 17.82, p=0.03, I2=0%), when compared to the placebo (Figure 2) (Supplemental Figures S10).
Glycemic Parameters
Only three trials reported the relationship between the 80mg dose of Danuglipron and changes in HbA1C from baseline. These trials collectively demonstrated a significant reduction in HbA1C in the overall analysis, with no observable heterogeneity effect (SMD −0.84, 90% CI −1.25 to −0.42, P = 0.0009, I2=48%) (Figure 3) (Supplemental Figures S11 and S12).
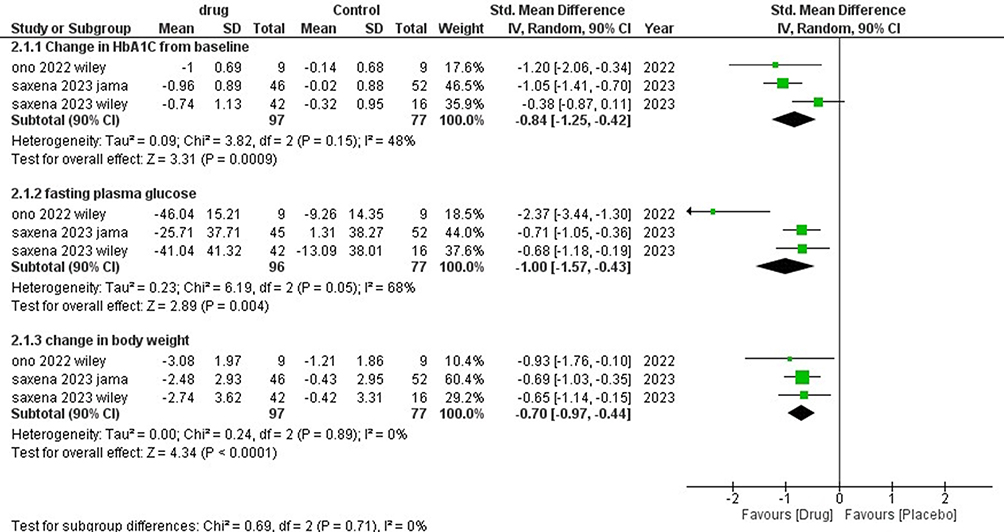 |
Figure 3 Summary plot for glycemic parameters 80mg. |
Regarding the 120mg dose, four trials reported this outcome, and they also showed a significant reduction in HbA1C from baseline, but heterogeneity was present (SMD −0.91, 90% CI −1.59 to −0.22, P = 0.03, I2=84%). However, the heterogeneity was reduced to 36% after a sensitivity analysis, and the results remained significant. The pooled analysis further confirmed a significant association (SMD −1.09, 90% CI −1.39 to −0.8, P <0.00001, I2=53%) (Figure 4) (Supplemental Figures S11 and S12).
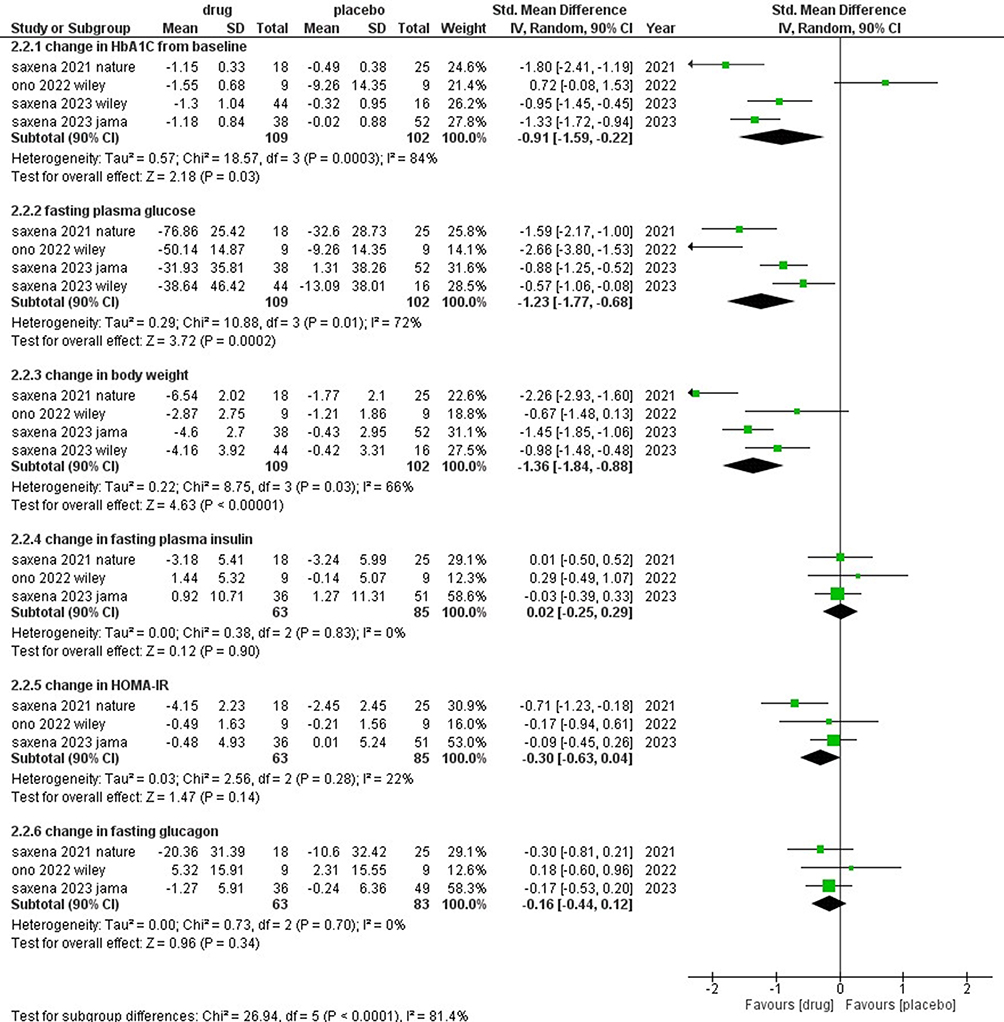 |
Figure 4 Summary plot for glycemic parameters 120mg. |
All doses of Danuglipron, including 80mg and 120mg, were found to be superior to the placebo in reducing HbA1C levels.
Our analysis revealed that FPG (fasting plasma glucose) was significantly reduced from baseline in both doses of Danuglipron. For the 80mg dose, the standardized mean difference (SMD) was −1.00 (90% CI −1.57 to −0.43, P = 0.004, I2=68%). Similarly, for the 120mg dose, the SMD was −1.23 (90% CI −1.77 to −0.68, P = 0.0002, I2=72%). The overall pooled analysis showed a consistent reduction in FPG for both doses (SMD −1.10, 90% CI −1.46 to −0.75, P <0.00001, I2=67%). Upon performing sensitivity analysis, the results remained significant and consistent for both the 80mg (SMD −0.7, 90% CI −0.97 to −0.44, P = 0.0001, I2=0%) and 120mg (SMD −0.77, 90% CI −1.06 to −0.48, P = 0.0001, I2=0%) doses. Notably, increasing the dose did not significantly reduce FPG, suggesting that both doses effectively reduced fasting plasma glucose levels (Figures 3 and 4) (Supplemental Figures S13 and S14).
The results demonstrated dose-dependent reductions in body weight when comparing Danuglipron to placebo. Specifically, for the 80mg dose, the standardized mean difference (SMD) was −0.7 (90% CI −0.97 to −0.44, P = 0.0001, I2=0%), indicating a significant reduction in body weight. Similarly, for the 120mg dose, the SMD was −1.36 (90% CI −1.84 to −0.88, P = 0.00001, I2=66%), further supporting a significant decrease in body weight (Figures 3 and 4) (Supplemental Figures S15 and S16).
The pooled analysis combined data from both doses and demonstrated a significant reduction in body weight (SMD −1.08, 90% CI −1.42 to −0.74, P = 0.00001, I2=66%). Furthermore, the sensitivity analysis, which excluded one trial in the 120mg group, yielded similar results and reduced statistical heterogeneity (Supplemental Figures S15 and S16).
As for the other parameters, like change in fasting plasma insulin, plasma glucagon, and HOMA-IR, showed no significant association compared to placebo (Figure 4) (Supplemental Figures S17).
Discussion
To our knowledge, this study presents the inaugural meta-analysis examining the comprehensive profile of Danuglipron, an oral GLP-1 receptor agonist primarily employed in the management of T2DM. The study focuses on analyzing the adverse outcomes and glycemic parameters associated with two different doses (80mg and 120mg) of Danuglipron compared to placebo. The adverse outcomes studied include diarrhea, headache, nausea, vomiting, and decreased appetite. Additionally, the study evaluates glycemic parameters such as reduction in HbA1C from baseline, change in fasting plasma glucose (FPG), and change in body weight. These findings provide valuable insights into the safety and efficacy of Danuglipron in the management of diabetes.
In terms of adverse outcomes, the study indicates that both doses of Danuglipron are associated with certain side effects. Diarrhea was observed in patients receiving both the 80mg and 120mg doses, with sensitivity analysis suggesting a significant increase in diarrhea events for both doses. Interestingly, there appears to be an unexpected relationship between dose and diarrhea incidence, where higher doses might be associated with fewer events. For headache, neither the 80mg nor the 120mg dose of Danuglipron showed a significant difference in occurrence compared to the placebo. This is important in assessing the potential impact of Danuglipron on patient comfort. Both doses of Danuglipron were linked to an increased risk of nausea, with the percentages of nausea events being similar for both doses. These finding prompts consideration of the balance between glycemic control and side effects when choosing the appropriate dose. Vomiting showed a dose-dependent relationship, with higher doses of Danuglipron associated with a higher incidence of vomiting. This information is crucial for managing patients who might be sensitive to gastrointestinal disturbances. The more substantial reduction in mean daily glucose (MDG), as opposed to fasting plasma glucose (FPG), among participants treated with Danuglipron is in line with the known effect of GLP-1 receptor agonism. This effect is consistent with the fact that GLP-1 receptor agonists mitigate postprandial glucose spikes, partly through the delay of gastric emptying.9,19
Ono et al16 and Saxena et al11 observed an elevated heart rate in patients administered higher doses of the specified regimen. However, their analysis of additional vital signs, laboratory tests, and ECG examinations did not reveal any statistically significant findings. This adverse event was noted to be prevalent among GLP-1 agonists.2,20 The degree of heart rate elevation observed in the present study aligns with the short-term clinical data reported for established GLP-1 receptor agonists, such as dulaglutide and liraglutide.21,22 The 120mg dose of Danuglipron showed a significant increase in decreased appetite compared to the placebo. This finding might influence treatment decisions, particularly for patients struggling with appetite-related issues due to diabetes. Other adverse outcomes, such as dyspepsia and dizziness, were associated with Danuglipron. Dyspepsia showed a significant increase in events, while no significant differences were observed in hypoglycemia and abdominal distention compared to the placebo. The overall safety profile, as well as the gastrointestinal safety profile, of Danuglipron, aligns closely with what has been documented for peptidic GLP-1 receptor agonists. This includes comparability with the recently developed oral formulation of semaglutide, as reported in previous studies.23–26
The study findings suggest that both doses of Danuglipron (80mg and 120mg) result in significant reductions in HbA1C from baseline. This indicates a favorable effect on glycemic control. Both doses also led to significant reductions in FPG levels, demonstrating the drug’s effectiveness in managing blood glucose. Furthermore, both doses of Danuglipron were associated with significant reductions in body weight. This is promising, as weight management is a crucial aspect of diabetes care.
In a different combination treatment approach, the novel dual GIP and GLP-1 receptor agonist tirzepatide showcased remarkable advancements in glucose management and weight reduction compared to the selective GLP-1 receptor agonist dulaglutide. Notably, it was revealed that tirzepatide outperformed dulaglutide in enhancing markers of insulin sensitivity (IS) and beta-cell function. Importantly, the observed effects of tirzepatide on insulin sensitivity were only partially attributable to weight loss, implying that the dual receptor agonism of tirzepatide encompasses distinct mechanisms for achieving glycemic control.21,27–29
Recent clinical trials have presented contradictory findings regarding the link between GLP-1 receptor agonists and diabetic retinopathy. However, the potential impact of GLP-1 receptor agonists on angiogenesis, both in clinical and preclinical settings, has been a topic of prolonged discussion. The AngioSafe T2DM studies contribute experimental and clinical evidence, affirming that GLP-1 receptor agonists do not influence angiogenesis and demonstrate no discernible connection between GLP-1 exposure and severe diabetic retinopathy.30–32
Limitations
The meta-analysis conducted in this study encountered several notable limitations that should be acknowledged. Firstly, a noteworthy constraint pertains to the limited number of trials available for inclusion. This scarcity in trial availability inherently led to a diminutive overall sample size, thereby potentially limiting the statistical power and robustness of the findings. Another significant limitation is the restricted evaluation of all Danuglipron doses, primarily focused on 80 mg and 120 mg. The lack of data for other doses hampers a comprehensive understanding of the dose-response relationship and its implications for effectiveness. This highlights the importance of exercising caution when extrapolating findings to doses not directly studied. The variability in study durations across the included trials constitutes yet another limitation of this meta-analysis. The disparate timeframes over which the studies were conducted introduce an element of heterogeneity that could influence the consistency and generalizability of the results. Such diversity in study durations may introduce confounding factors and hinder the establishment of clear causal relationships between Danuglipron and its outcomes. Lastly, the diversity in study populations is crucial. While three studies included participants on background glucose-lowering therapy, one study did not have such treatment. This inconsistency introduces treatment variation that could affect evaluating Danuglipron’s effectiveness across different glucose-lowering therapies. A more balanced distribution of study populations with and without background glucose therapy is needed for a thorough assessment of Danuglipron’s utility. A more substantial number of trials, a broader range of doses, standardized study durations, and carefully balanced study populations would collectively contribute to a more robust understanding of the glycemic efficacy and adverse outcomes associated with Danuglipron.
Conclusion
In conclusion, this pioneering meta-analysis offers a comprehensive overview of the effects of Danuglipron, an oral GLP-1 receptor agonist used in the management of T2DM. The study’s focus on adverse outcomes and glycemic parameters associated with different doses of Danuglipron compared to a placebo yields valuable insights into its safety and efficacy. The analysis reveals that both 80mg and 120mg doses of Danuglipron are linked to specific adverse effects, notably diarrhea, nausea, vomiting, and decreased appetite. Interestingly, higher doses might show a paradoxical reduction in diarrhea incidents. The findings underscore the need for a careful balance between glycemic control and potential side effects in dose selection. The study demonstrates Danuglipron’s effectiveness in reducing HbA1C, fasting plasma glucose, and body weight, aligning with its GLP-1 receptor agonism effect. The drug’s impact on mean daily glucose highlights its ability to manage postprandial glucose spikes, contributing to improved glycemic control. Comparisons to other GLP-1 receptor agonists, like tirzepatide, emphasize the potential for innovative treatments in diabetes management. This study provides critical data for clinicians considering Danuglipron in T2DM treatment. It underscores the drug’s positive effects on glycemic control and weight reduction while delineating its associated adverse effects. These findings contribute to the evolving landscape of diabetes therapeutics, offering insights that can aid clinicians in making informed decisions regarding treatment strategies. Further research and real-world evidence will continue to refine our understanding of Danuglipron’s role in the comprehensive care of individuals with Type 2 Diabetes.
Data Sharing Statement
Data available within the article. The authors confirm that the data supporting the findings of this study are available within the article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no potential conflicts of interest in this work.
References
1. Diabetes; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/diabetes.
2. Saxena AR, Gorman DN, Esquejo RM, et al. Danuglipron (PF-06882961) in type 2 diabetes: a randomized, placebo-controlled, multiple ascending-dose phase 1 trial. Nat Med. 2023;27(6):1079–1087. doi:10.1038/s41591-021-01391-w
3. Countries with highest number of diabetes cases unveiled; 2023. Available from: https://www.diabetes.co.uk/news/2023/jun/countries-with-highest-number-of-diabetes-cases-unveiled.html.
4. Araki E, Goto A, Kondo T, et al. Japanese clinical practice guideline for diabetes 2019. Diabetol Int. 2020;11(3):165–223. doi:10.1007/s13340-020-00439-5
5. Morita Y, Murayama H, Odawara M, Bauer M. Treatment patterns of drug-naive patients with type 2 diabetes mellitus: a retrospective cohort study using a Japanese hospital database. Diabetol Metab Syndr. 2023;11:1.
6. Karagiannis T, Avgerinos I, Liakos A, et al. Management of type 2 diabetes with the dual GIP/GLP-1 receptor agonist tirzepatide: a systematic review and meta-analysis. Diabetologia. 2023;65(8):1251–1261. doi:10.1007/s00125-022-05715-4
7. Tsapas A, Avgerinos I, Karagiannis T, et al. Comparative effectiveness of glucose-lowering drugs for type 2 diabetes. Ann Int Med. 2020;173(4):278–287. doi:10.7326/M20-0864
8. Griffith DA, Edmonds DJ, Fortin JP, et al. A small-molecule oral agonist of the human glucagon-like peptide-1 receptor. J Med Chem. 2022;65(12):8208–8226. doi:10.1021/acs.jmedchem.1c01856
9. Aspnes GE, Bagley SW, Coffey SB, et al. 6-Azaspiro[2.5]octanes as small molecule agonists of the human glucagon-like peptide-1 receptor. Bioorg Med Chem Lett. 2023;94. doi:10.1016/j.bmcl.2023.129454
10. Rahman A, Alqaisi S, Saith SE, Alzakhari R, Levy R. The impact of glucagon-like peptide-1 receptor agonist on the cardiovascular outcomes in patients with type 2 diabetes mellitus: a meta-analysis and systematic review. Cardiol Res. 2023;14(4):250–260. doi:10.14740/cr1523
11. Saxena AR, Frias JP, Brown LS, et al. Efficacy and safety of oral small molecule glucagon-like peptide 1 receptor agonist danuglipron for glycemic control among patients with type 2 diabetes: a randomized clinical trial. JAMA Netw Open. 2023;6(5):e2314493–e2314493. doi:10.1001/jamanetworkopen.2023.14493
12. Sikirica MV, Martin AA, Wood R, Leith A, Piercy J, Higgins V. Reasons for discontinuation of GLP1 receptor agonists: data from a real-world cross-sectional survey of physicians and their patients with type 2 diabetes. Diabetes Metab Syndr Obes. 2017;10:403–412. doi:10.2147/DMSO.S141235
13. Saxena AR, Frias JP, Gorman DN, et al. Tolerability, safety and pharmacodynamics of oral, small-molecule glucagon-like peptide-1 receptor agonist danuglipron for type 2 diabetes: a 12-week, randomized, placebo-controlled, Phase 2 study comparing different dose-escalation schemes. Diabetes Obes Metab. 2023;25(10):2805–2814. doi:10.1111/dom.15168
14. Davies M, Pieber TR, Hartoft-Nielsen ML, Hansen OKH, Jabbour S, Rosenstock J. Effect of oral semaglutide compared with placebo and subcutaneous semaglutide on glycemic control in patients with type 2 diabetes: a randomized clinical trial. JAMA. 2017;318(15):1460–1470. doi:10.1001/jama.2017.14752
15. Chen L, Yun Y, Guo S, et al. Discovery of novel 5,6-dihydro-1,2,4-triazine derivatives as efficacious glucagon-like peptide-1 receptor agonists. J Med Chem. 2023;66(12):7988–8010. doi:10.1021/acs.jmedchem.3c00320
16. Ono R, Furihata K, Ichikawa Y, et al. A phase 1 study to evaluate the safety, tolerability, pharmacokinetics and pharmacodynamics of danuglipron PF −06882961), an oral small-molecule glucagon-like peptide-1 receptor agonist, in Japanese adults with type 2 diabetes mellitus. Diabetes Obes Metab. 2023;25(3):805. doi:10.1111/dom.14928
17. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;88:372.
18. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;2019:366.
19. Nauck MA, Quast DR, Wefers J, Meier JJ. GLP-1 receptor agonists in the treatment of type 2 diabetes - state-of-The-art. Mol Metab. 2021;46:101102.
20. Drucker DJ. The cardiovascular biology of glucagon-like peptide-1. Cell Metab. 2016;24(1):15–30. doi:10.1016/j.cmet.2016.06.009
21. Coskun T, Sloop KW, Loghin C, et al. LY3298176, a novel dual GIP and GLP-1 receptor agonist for the treatment of type 2 diabetes mellitus: from discovery to clinical proof of concept. Mol Metab. 2018;18:3–14. doi:10.1016/j.molmet.2018.09.009
22. Shankar SS, Vella A, Raymond RH, et al. Standardized mixed-meal tolerance and arginine stimulation tests provide reproducible and complementary measures of β-cell function: results from the foundation for the national institutes of health biomarkers consortium investigative series. Diabetes Care. 2016;39(9):1602–1613. doi:10.2337/dc15-0931
23. Niswender K, Pi-Sunyer X, Buse J, et al. Weight change with liraglutide and comparator therapies: an analysis of seven Phase 3 trials from the liraglutide diabetes development programme. Diabetes Obes Metab. 2013;15(1):42–54. doi:10.1111/j.1463-1326.2012.01673.x
24. Ahrén B, Atkin SL, Charpentier G, et al. Semaglutide induces weight loss in subjects with type 2 diabetes regardless of baseline BMI or gastrointestinal adverse events in the SUSTAIN 1 to 5 trials. Diabetes Obes Metab. 2018;20(9):2210–2219. doi:10.1111/dom.13353
25. Yabe D, Nakamura J, Kaneto H, et al. Safety and efficacy of oral semaglutide versus dulaglutide in Japanese patients with type 2 diabetes (PIONEER 10): an open-label, randomised, active-controlled, phase 3a trial. Lancet Diabetes Endocrinol. 2020;8(5):392–406. doi:10.1016/S2213-8587(20)30074-7
26. Niman S, Hardy J, Goldfaden RF, et al. A review on the efficacy and safety of oral semaglutide. Drugs R D. 2021;21(2):133–148. doi:10.1007/s40268-021-00341-8
27. Thomas MK, Nikooienejad A, Bray R, et al. Dual GIP and GLP-1 receptor agonist tirzepatide improves beta-cell function and insulin sensitivity in type 2 diabetes. J Clin Endocrinol Metab. 2021;106(2):388. doi:10.1210/clinem/dgaa863
28. Hartman ML, Sanyal AJ, Loomba R, et al. Effects of novel dual GIP and GLP-1 receptor agonist tirzepatide on biomarkers of nonalcoholic steatohepatitis in patients with type 2 diabetes. Diabetes Care. 2020;43(6):1352–1355. doi:10.2337/dc19-1892
29. Frias JP, Nauck MA, Van J, et al. Efficacy and safety of LY3298176, a novel dual GIP and GLP-1 receptor agonist, in patients with type 2 diabetes: a randomised, placebo-controlled and active comparator-controlled phase 2 trial. Lancet. 2018;392(10160):2180–2193. doi:10.1016/S0140-6736(18)32260-8
30. Gaborit B, Julla JB, Besbes S, et al. Glucagon-like peptide 1 receptor agonists, diabetic retinopathy and angiogenesis: the angiosafe type 2 diabetes study. J Clin Endocrinol Metab. 2020;105(4):E1549–60. doi:10.1210/clinem/dgz069
31. Pang B, Zhou H, Kuang H. The potential benefits of glucagon-like peptide-1 receptor agonists for diabetic retinopathy. Peptides. 2018;100:123–126. doi:10.1016/j.peptides.2017.08.003
32. Cai X, Li J, Wang M, et al. GLP-1 treatment improves diabetic retinopathy by alleviating autophagy through GLP-1R-ERK1/2-HDAC6 signaling pathway. Int J Med Sci. 2017;14(12):1203–1212. doi:10.7150/ijms.20962
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Understanding the Role of Metabolic Syndrome as a Risk Factor for Hepatocellular Carcinoma
Chavez-Tapia NC, Murúa-Beltrán Gall S, Ordoñez-Vázquez AL, Nuño-Lambarri N, Vidal-Cevallos P, Uribe M
Journal of Hepatocellular Carcinoma 2022, 9:583-593
Published Date: 5 July 2022
New Discovered Adipokines Associated with the Pathogenesis of Obesity and Type 2 Diabetes
Cheng JX, Yu K
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2381-2389
Published Date: 7 August 2022
Clinical Insight on Semaglutide for Chronic Weight Management in Adults: Patient Selection and Special Considerations
Chao AM, Tronieri JS, Amaro A, Wadden TA
Drug Design, Development and Therapy 2022, 16:4449-4461
Published Date: 29 December 2022
Design and Protocol of the Biobank for Metabolic Syndrome Consequences (BMSC): A Prospective Cohort Study in Northwest China
Yang X, Li Q, He Y, Yin G, Li M, Zhu W, Fan X, Gong Y, Wang Y, Qiang W, Wang Y, Willems van Dijk K, Rensen PCN, Guo H, Shi B, Wang Y
Clinical Epidemiology 2025, 17:823-835
Published Date: 14 October 2025
Modulating Metabolic Health and Physiological Functions: Advances in Dietary Interventions Targeting Gut Microbiota
Rabbani SA, El-Tanani M, Janić M, Janež A, Tanani YE, Hajeer E, Matalka MI, Rizzo M, Kumar R
Therapeutics and Clinical Risk Management 2025, 21:1701-1733
Published Date: 13 December 2025