Back to Journals » Journal of Pain Research » Volume 14
Evaluating Effectiveness of Fu’s Subcutaneous Needling for the Pain Nature and Quality of Life in Patients with Knee Osteoarthritis: A Study Protocol of Randomized Clinical Trial
Authors Chiu PE, Fu Z ![]() , Jian GW, Huang CH, Li TM, Chou LW
, Jian GW, Huang CH, Li TM, Chou LW ![]()
Received 9 August 2021
Accepted for publication 23 September 2021
Published 9 October 2021 Volume 2021:14 Pages 3163—3172
DOI https://doi.org/10.2147/JPR.S333299
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Po-En Chiu, 1, 2,* Zhonghua Fu, 3,* Guan-Wei Jian, 4, 5 Ching-Hsuan Huang, 2, 6 Te-Mao Li, 2 Li-Wei Chou 7– 9
1Department of Chinese Medicine, Chang Bing Show Chwan Memorial Hospital, Changhua, Taiwan; 2School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 3Institute of Fu’s Subcutaneous Needling, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 4Graduate Institute of Acupuncture Science, China Medical University, Taichung, Taiwan; 5Department of Chinese Medicine, Sinying Hospital, Ministry of Health and Welfare, Tainan, Taiwan; 6Department of Chinese Traumatology Medicine, China Medical University Hospital, Taichung, Taiwan; 7Department of Physical Medicine and Rehabilitation, China Medical University Hospital, Taichung, Taiwan; 8Department of Physical Therapy and Graduate Institute of Rehabilitation Science, China Medical University, Taichung, Taiwan; 9Department of Physical Medicine and Rehabilitation, Asia University Hospital, Asia University, Taichung, Taiwan
*These authors contributed equally to this work
Correspondence: Li-Wei Chou
Department of Physical Medicine and Rehabilitation, China Medical University Hospital, No. 2 Yuh-Der Road, Taichung, 40447, Taiwan
Tel +886-4-22052121-2381
Fax +886-4-22026041
Email [email protected]
Background: Knee osteoarthritis (OA) is a common clinical disease. Knee pain is the major symptom of knee OA and the primary reason why patients seek treatment. Fu’s subcutaneous needling (FSN) has been used to treat knee OA for more than 20 years. However, the establishment of treatment methods and rigorous evaluation of FSN’s efficacy are still lacking. A randomized single-blind clinical trial will be conducted to evaluate whether FSN treatment can immediately alleviate pain due to knee OA surrounding the patella and the curative effective of 1-week and 2-week treatments. In addition, the feasibility and initial effect of FSN treatment for patients with knee OA will be discussed.
Materials and Methods: Patients with confirmed knee OA, as diagnosed by doctors using X-ray films or from clinical symptoms, who are over 50 years old will be participants recruited. They will be randomly assigned either FSN treatment or transcutaneous electrical nerve stimulation treatment. In addition, their pressure pain threshold, muscle tone of lower leg muscle, and physical ability will be measured. Participants will be asked to complete the questionnaires of Western Ontario and McMaster Universities Osteoarthritis Index and Lequesne’ index as the measurements for quality of life.
Results: The findings of this study will reveal whether FSN or transcutaneous electrical nerve stimulation is clinically efficacious for treating pain due to knee OA, with respect to muscle stiffness, gait, dynamic balance, the pressure pain threshold, and quality of life before and after treatment.
Study Registration: This study is approved by the Research Ethics Committee of China Medical University & Hospital, Taichung, Taiwan (CMUH107-REC3-027) and registered at the ClinicalTrials.gov Protocol Registration and Results System (registration number NCT04356651).
Keywords: dry needling, Fu’s subcutaneous needling, knee osteoarthritis, myofascial trigger point, tightened muscle
A Letter to the Editor has been published for this article.
A Response to Letter has been published for this article.
Introduction
Knee osteoarthritis (OA) is a highly common chronic joint disease, and it is a major cause of chronic pain and disability. With an aging global population and increasing obesity ratio, knee OA has become increasingly prevalent in the last few decades. In the United States, approximately over 14 million people have knee OA with symptoms.1 In Taiwan, according to the statistics of the Ministry of Health and Welfare, the prevalence of knee OA is approximately 15%. Specifically, in Taiwan, approximately 3.5 million people have knee OA; among older adults over 58 years old, 1 in 5 people have joint degeneration problems; and for older adults over 70 years old, up to more than 70% of them have knee OA. In general, an extremely large portion of the population is affected by knee OA,2 and the disease can incur a large economic cost and social burden. In addition to bearing the health care cost from the disease, those with severe knee OA cannot work due to disability. Thus, treating this disease is important, especially considering that it is an important factor causing disability.
In research on the cause, knee OA has long been considered to be caused by cartilage loss resulting from the progressive wear of joint cartilage. In addition, knee OA is often accompanied by synovial joint inflammation.3 However, according to the recent literature, knee OA is caused by multiple factors. Characteristics of knee OA include functional changes in the surrounding structures of the entire joint, such as the meniscus, surrounding ligaments, and subchondral bone,4 particularly the abnormal arrangement of knee joints and weakness in the quadricep muscles. These result in the possibility of local joint damage.5 Some observational studies have reported that knee OA is primarily caused by the insufficient power of the knee extensor muscle group.6,7 Muscle dysfunction is also speculated to be the risk factor that aggravates knee OA. Consequently, improving muscle function eases pain symptoms and improves joint structures.8 Thus, the muscles are central to the pathogenesis of knee OA.
Fu’s subcutaneous needling (FSN) is a new acupuncture treatment developed by the Traditional Chinese physician, Zhonghua Fu, based on traditional acupuncture theory. FSN can provide some stimulation in the subcutaneous areas, and it has a rapid and lasting effect on soft tissue damage and some internal diseases.9 The treatment method involves inserting a disposable FSN needle (Figure 1) horizontally and swaying it in the subcutaneous tissue around the muscles with myofascial trigger points (MTrPs) along with using the reperfusion approach. In doing so, the symptoms of abnormal muscular tension, stiffness, pressure pain, spontaneous pain, and fatigue are alleviated. FSN is a type of dry needling therapy without any solution for injection, too.
 |
Figure 1 Schematic of structure of a typical disposable FSN needle. |
This study protocol aims to furnish preliminary results on the feasibility of using FSN treatment in patients with knee OA, thus evaluating the efficacy of FSN treatment on alleviating pain in the surrounding soft tissue from knee OA due to MTrPs. The findings provide a novel reference for the clinical treatment of knee OA.
Materials and Methods
Study Design
A randomized single-blind clinical trial design is adopted in the experiment, where every participant is randomly assigned to the experimental group or the control group. The participants will accept either FSN treatment or transcutaneous electrical nerve stimulation (TENS) treatment thrice (at Days 1, 2, and 4). The entire experiment will last for 2 weeks, with the aim of observing the immediate, post-1-week, and post-2-week curative effect. A single evaluation of the treatment will be conducted before and after the treatment on the 1st, 2nd, and 4th day; as well as on 8th day and 15th day after the first treatment.
The study and experimental procedure have both been approved by an institutional review board. All participants will be recruited from the Rehabilitation Division and Acupuncture Division of China Medical University Hospital. The 90 patients who satisfy the inclusion criteria and who provide their written informed consent will be randomly divided into 2 equal-sized groups, each receiving either FSN or TENS treatment. The experimental procedure and study flow chart are shown in Figures 2 and 3.
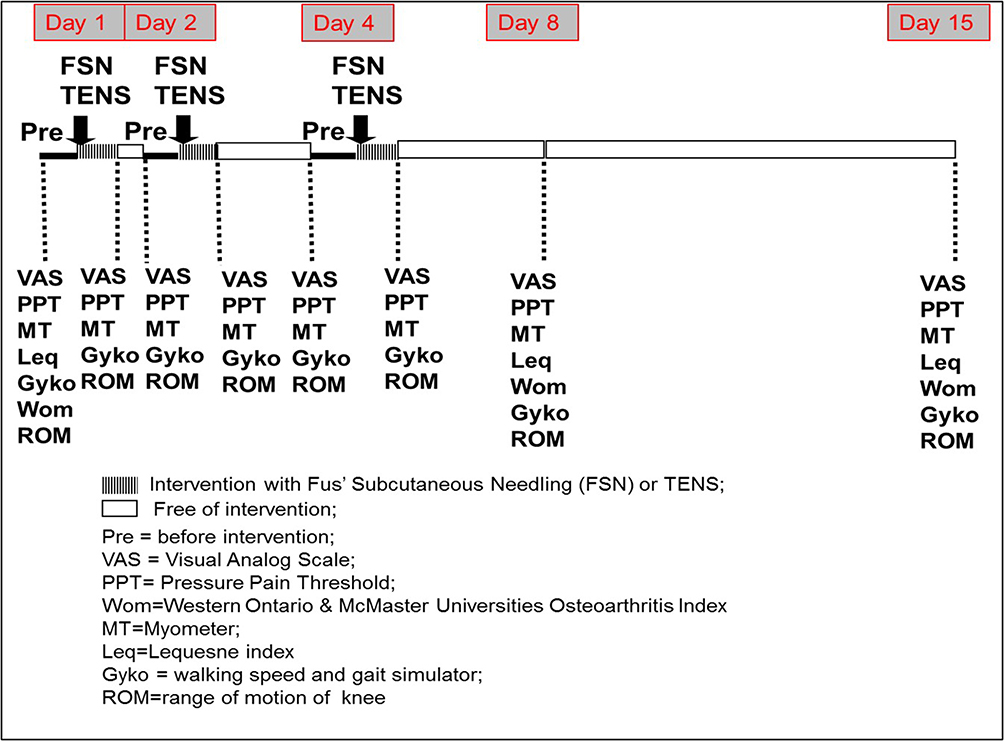 |
Figure 2 Schedule of enrollment, interventions, and assessments. |
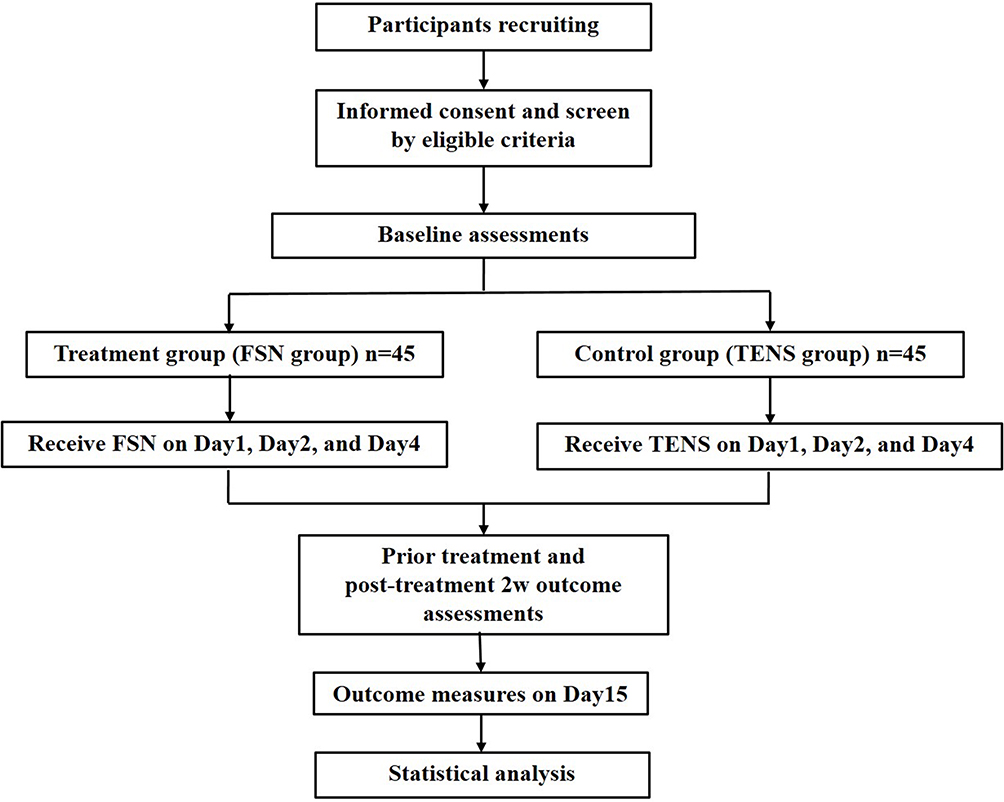 |
Figure 3 Flowchart of the study procedure. |
Participants
A total of 90 patients with knee OA are expected to participate in this study. Table 1 shows the inclusion and exclusion criteria of the patients. The participants will be recruited at the Rehabilitation Division and Acupuncture Division of China Medical University Hospital. Before participating in the experiment, the participants will provide their written informed consent after being thoroughly briefed. The study protocol was approved by the Research Ethics Committee and followed the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects.
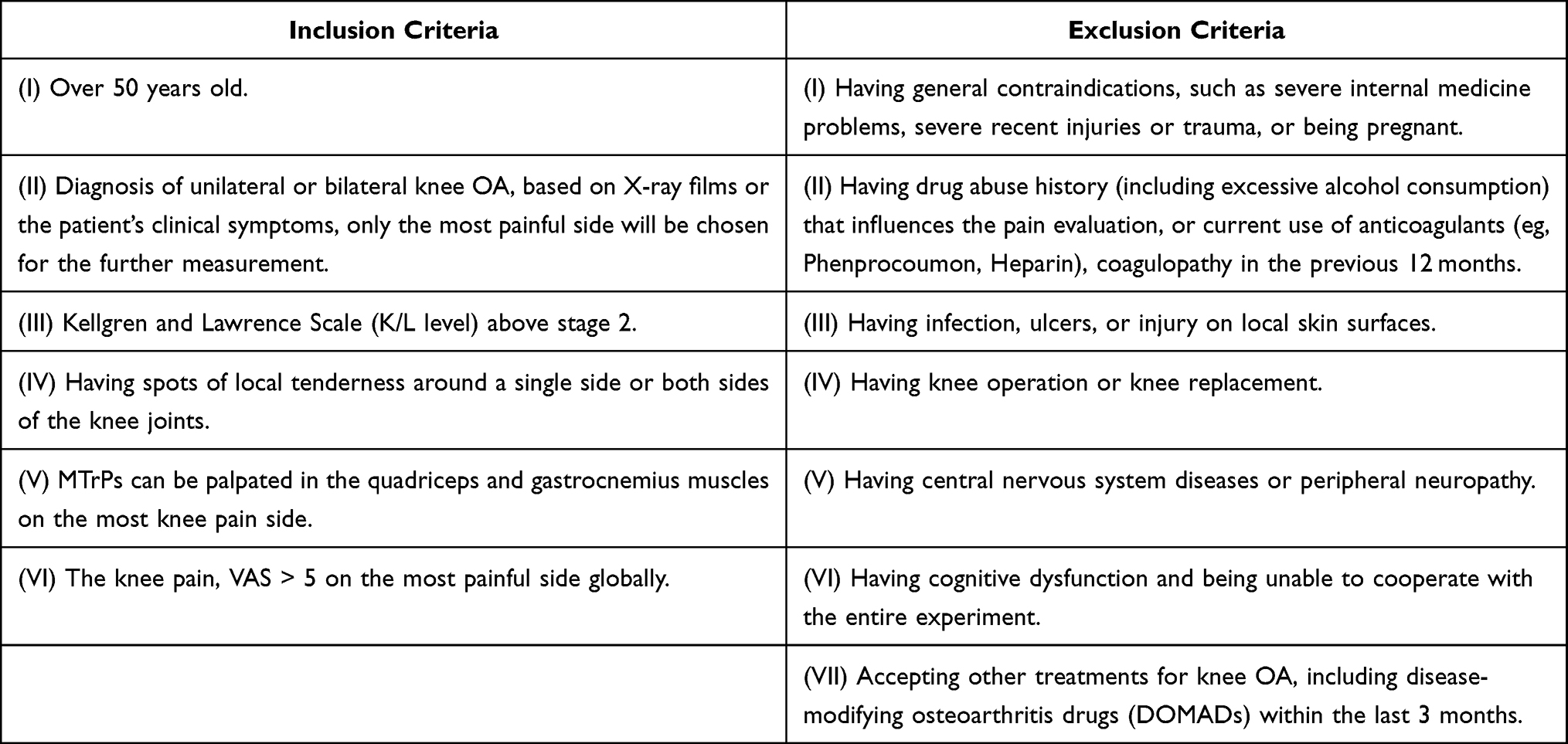 |
Table 1 Inclusion and Exclusion Criteria |
Study Interventions
Treatment Group (FSN Group)
Medium-size disposable FSN needles (Nanjing Paifu Medical Science and Technology) will be used for treatment. These products have received regulatory approval (approval license number: number 001018 of medical equipment imported from China, as given by China’s Ministry of Health and Welfare; License document number: DHA09200101807).
The procedure of FSN is illustrated as the following:
- Needle insertion: The participant is asked to lie on their back, keep their knee straight, and maintain their pelvis at the central position. Subsequently, the needle is inserted at the 1/3 spot at the near end of the connecting line between the anterior superior iliac spine and the superior border of patella (Figure 4). The needle is inserted toward the patella until it is fully submerged in the subcutaneous tissue. To confirm that the needle does not extend into the dermis or muscles, the participant must confirm that there they experience completely no pain throughout the entire insertion process.
- Swaying: The needle is backed into the soft tube. The needle handle is held by the hand, and the needle is swayed left and right in a sector shape. The angle of the sector is approximately 60°, and the needle is swayed for 45 times in 30 s. In the entire swaying process, the participant must confirm that they experience completely no pain.
- Reperfusion approach: The participant is requested to undertake the dorsiflexion movement with their sole of foot. Every cycle includes 10 s of continual movement and a 10-s break. The participant is asked to do 3 cycles for a total of 1 min. Subsequently, the participant is asked to sit and then to bend and extend their knee. The cycle includes 10 s of continual movement and a 10-s break. The participant is asked to do 3 cycles for a total of 1 min.
- Needle withdrawal: After the 2 actions are completed, the FSN needle is withdrawn directly.
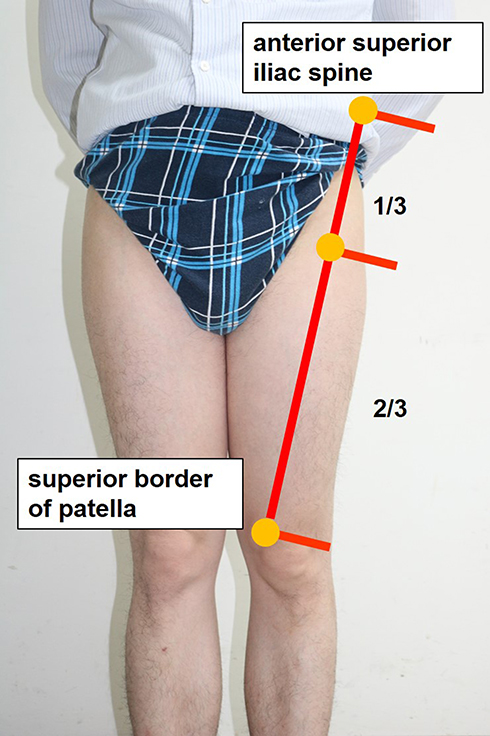 |
Figure 4 The yellow spot is the insertion point, which is at the 1/3 spot at the near end of the connecting line between the anterior iliac spine and the superior border of patella. |
Control Group (TENS Group)
A 2205A TENS machine (Well-Life Healthcare) will be adopted. TENS is an extensively used and accepted method of pain relief. The effect of pain relief is achieved by delivering electric stimulation at different frequencies and intensities through patches on the skin. TENS is extensively used by clinicians for pain relief in the musculoskeletal system and for different types of neuralgia. Its effect has been approved by regulatory authorities, and it has the advantages of being simple to operate and having few side effects.10
One electrode pad is attached to the Liangqiu point (ST34) and Yanglingquan point (GB34) on the lateral side of the knee, and another electrode pad is attached to the Xuehai point (SP10) and Yinlingquan point (SP9) on the medial side of the knee. Current is then passed through each patch knee joint in an alternating fashion. The parameters of the electric stimulation differ depending on the depth of the muscular tissue.
Nonetheless, some general guidelines apply. According to other studies, the common treatment frequency for patients with knee OA is 110 Hz in the continual mode.11–13 After continual stimulation of 20 min, the machine is turned off, and the electrode pads are peeled off (Figure 5).
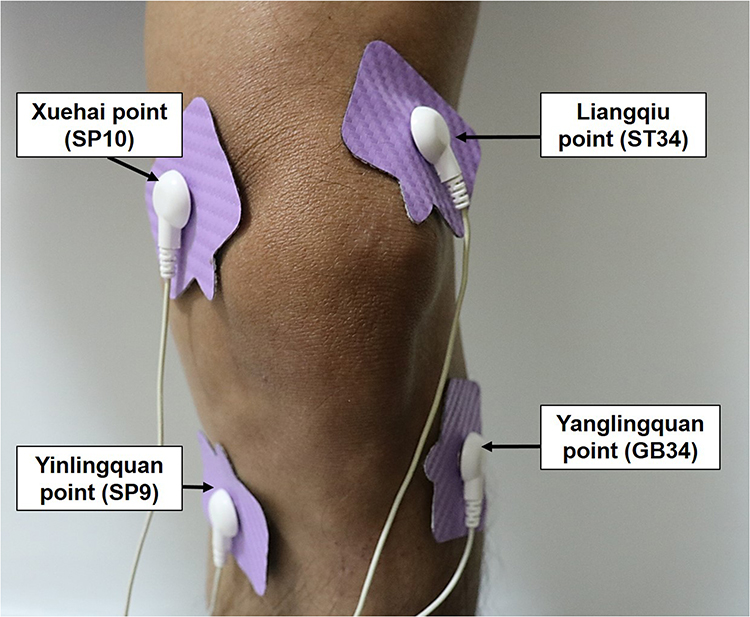 |
Figure 5 Electrotherapy method for the TENS group. |
Sample Size Calculation
To calculate the requisite sample size, as FSN treatment is a new therapy, lack of previous treatment experience is unavoidable, we referred to the variance of the results of similar previous study for treatment of knee osteoarthritis,14 comparing VAS scores among patients receiving sham acupuncture treatment to standard acupuncture, we assumed anticipated means and standard deviations in the treatment groups is 3.75±1.5, the anticipated percent difference (decrease) in control group compared to treatment group is 25%. According to our calculations, the sample size required for an unpaired t test was 80 individuals, with 40 individuals each in the FSN and TENS groups. The calculation was performed using a significance level of P < 0.05 (ie, 5% of type I errors, resulting in a 95% confidence interval) and an absolute error of 5%. Considering a dropout rate of 10%, 90 patients are required to generate 80% of the power, at a significance level of P < 0.05.
Randomization and Allocation Concealment
In this study, 90 patients will be divided into equally-sized FSN and TENS groups. With regard to the assignment, each patient will be given a sealed, opaque envelope that contain information on which group they belong to. Eligible and consenting patients (ie, participants) will pass the envelope to the researchers, who will then pass them on to the doctor conducting the operation. The doctor will then open the envelope and assign the participant to the FSN group or TENS group. Through such a method, the researchers are blinded to the group assignment. Specifically, blinding is assured through the following methods.
The random numbers will be generated in SPSS software (version 22.0, IBM SPSS Statistics, IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp). In addition, another person who is not affiliated with this study will be responsible for the operation, and the treatment and evaluation of the experiment will be conducted by a different set of personnel. These ensure that the evaluators are blinded to the group assignment.
Single-Blinding
A single-blind method will be used. Because the participants and treatment operators cannot be blinded, we blinded the personnel in charge of assessing the outcome, managing the data, and conducting the statistical analysis. The evaluators will be instructed to not communicate with the participants about anything that may be remotely related to their treatment.
Discontinuation Criteria
Participants Who Request to Withdraw for Any Reason
If participants decide to withdraw from all components of this study, investigator must discontinue all of the following research activities involving that subject’s participation in this study, but still retain collected data of those participants who withdraw from the research.
Abnormal Adverse Event Measurements at Any Point of the Testing Including Syncope, Massive Hemorrhage, Local Infection and Systemic Infection
If any of these complications occur during the course of the study, all adverse events will be recorded and will be reported immediately by the principal investigator. The study will be suspended if more than 1 out of the first 10 patients enrolled in the study group experiences any of above situation attributable to the investigational treatment.
Outcomes Measurements
Subjective Pain Intensity, Visual Analog Scales (VAS)15
Participants will be asked to describe how intense the pain around their knee is. Pain intensity will be measured using the visual analog pain scale. In this experiment, participants are asked to rate the pain intensity around their knee before and after every treatment.
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)
The WOMAC16–18 will be used to evaluate how severe knee OA is and how effective the treatment is, according to the patient’s symptoms and signs. The structures and functions of the hip and knee joints are evaluated with respect to the 3 major aspects of pain, stiffness, and joint function. Descriptions of such functions apply mainly to the lower limbs. Parts or entirety of the scale can be used. Participants will be asked to complete questions based on the scale before, 7 days after, and 2 weeks after the first treatment. In addition, patients will be asked to rate their pain on a 5-point scale (from 0 to 4).
Lequesne’ Index for Pain in Patients with Knee OA
Questions based on the Lequesne’ index19 for pain in patients with knee OA are divided into 3 parts. In the first part, the patient rates their pain and discomfort from 0 to 8 points from least to most painful (in their clinical symptoms). In the second part, the patient’s walking distance is rated from 1 to 8 points from least to greatest difficulty in walking. In the third part, the patient rates their ability to use their joints in everyday activity from 0 to 8 points. The total score ranges from 1 to 24 points from the slightest to most severe clinical symptoms. In the experiment, the patients complete these questions before, 7 days after, and 2 weeks after the first treatment. In addition, the patients will be asked to rate their pain on a 5-point scale from 0 to 4.
Pressure Pain Threshold of MTrPs
The pressure pain threshold of MTrPs20–22 is a semi-objective evaluation tool. Pressure algometry is used to measure the pressure pain threshold values on the quadriceps, pes anserinus, and gastrocnemius muscles. The measured points are the MTrPs of the quadriceps and gastrocnemius muscles in the muscle belly, and the attachment of tendons of the sartorius, gracilis and semitendinosus muscles on the pes anserinus. The machine we use is a Tissue Hardness Meter/Algometer Combo (OE-220). We will adopt the method recommended by Fischer to measure pressure pain thresholds and expressed the unit as N/cm2.
Myotone of MTrPs
The myotone of MTrPs23–25 is a semi-objective evaluation tool. A muscle tone measurement device (myometer) is used to measure the muscle tone around the MTrPs in the quadriceps, and gastrocnemius muscles. The unit for myotone of MTrPs in this study is expressed as Hz. In the experiment, the participants will be asked to lie on their back for a researcher to measure their muscle tone, stiffness, and elasticity.
Gyko
A physical ability detection system (GYKO; Microgate)26,27 will be used. This system contains a high-speed 3D accelerometer and gyroscope to capture data on 4 aspects: (1) walking and running, where the rocking levels of the torso during walking and running are compared; (2) posture, where the ability of the torso to maintain stability and balance when standing still is monitored; (3) power, specially used to monitor performance in sports; and (4) rehabilitation and biological feedback. This system mainly uses 1RM for evaluation, monitors the balance of the left and right sides simultaneously, and is used to evaluate the extent of damage and progress in rehabilitation. Before and after every treatment, the participants are asked to wear the GYKO during the experiment. Their gait and movement trajectories, center of gravity distribution when trying to balance while standing, and balance when transitioning from sitting to standing are monitored by the computer.
Complications and Adverse Events During and After the Treatment
The study process results in no harm to the participant’s health. However, there exists a slight risk of local bleeding or bruises after the FSN needle is withdrawn, which is the case in general acupuncture treatment. Should locally bleeding or bruises occur, the patient can apply direct pressure to the affected spot to stop the bleeding and apply a warm compress after 24 h. In the entire study process, the researchers will document all adverse events. All severe adverse events will be reported to the project emergency contact and the principal investigator of the project to further investigate the cause.
Data Management
After the all data are collected, trained research assistants will independently code the data using case report forms. Due to the known extremely low risk in FSN and TENS treatment, no official Data Safety Monitoring Board is required. The researchers will regularly monitor and review the experimental data themselves.
Statistical Analysis
The continuous variables are scores for the visual analog scale, WOMAC scale, Lequesne’ index, pressure pain threshold, muscle tone, stiffness, elasticity, and GYKO. The data will be analyzed using a t test, and statistical significance is indicated if P < 0.05.
Immediate effects are defined as immediate changes before and after every treatment. One-week effects are defined as the effects between the first treatment and 7 days after the treatment. Two-week effects are defined as the effects between the first treatment and 2 weeks after the treatment. A paired t test will be used for intra-group comparisons for the experimental and control groups. An independent t test will be used for inter-group comparisons.
We will use intention to treat analysis, all recruited patients will analyze as randomized regardless of the actual treatment received or whether they withdrew before the end of follow-up.
Ethics and Dissemination
This study strictly adheres to the medical ethics governing all medical personnel. The original medical records of the participants will be directly viewed by the host doctor, the institutional review board, and the competent authority. In addition, the process and data of the clinical experiment are checked for legality. In addition, the aforementioned personnel promise to never violate participant confidentiality, and the experimental data of all participants will be brought to the Rehabilitation Science Institute of China Medical University for analysis. The identities of the participants will be kept strictly confidential, as stipulated by law. Even if the experimental results are made public, the participants will be strictly anonymized.
The results of the experiment have been published on the ClinicalTrials.gov website and will be published in peer-reviewed journals as well as presented in academic conferences after the experiment ends.
Study Progression
The clinical trial had been sent to the Institutional Review Board in China Medical University & Hospital, Taichung, Taiwan and the approval letter was obtained on February 17, 2020 with the number of CMUH107-REC3-027. The protocol had also been submitted to the ClinicalTrials.gov website on April 20, 2020 and got the Identifier number of NCT04356651 (https://clinicaltrials.gov/ct2/show/record/NCT04356651). The clinical trial had been started on July 7, 2020, and completed on December 31, 2020. Now, all information and data are compiled and processed to statistical analysis.
Discussion
Knee OA is a common geriatric degenerative disease. It causes chronic pain and influences patients’ mobility. It is a cause of disability, which substantially reduces the patient’s everyday quality of life.28 As the population ages, the incidence rate of knee OA increases, which poses a serious public health challenge. Thus, treating and preventing knee OA are highly important.
In recent years, FSN has been extensively applied to diseases caused by MTrPs, including pain in the soft tissue of the joints and other diseases related to internal medicine.29–31 According to clinical observations, FSN treatment for MTrP-induced soft tissue pain has an instant curative effect. In addition, FSN treatment can effectively and immediately relieve pain symptoms, with no apparent side effects, in the surrounding soft tissue of the knee in patients with knee OA.32 However, most of these findings have been based on the patient’s subjective description of their symptoms. A rigorous evaluation of the curative effect of FSN treatment, a non-surgical method, is still lacking - despite a belief by patients and practitioners that FSN treatment mitigates the patient’s diminished ability to work.
From the perspective of FSN, knee joint pain in osteoarthritis is caused by pathological stress in muscles. Such muscles are referred to as pathological tightened muscles (TMs). The concept of TM was proposed by Prof. Zhonghua Fu in 2014, who asserted that a TM occurs when the central nervous system is relaxed but the target muscle is fully or partially stiff. TMs are closely related to MTrPs, and in general, TMs are formed on MTrPs. A single or multiple MTrPs might exist within a TM. The causes of TM are mainly ascribed to tightness and cramps induced by ischemia or hypoxia in local muscle tissues, which reduce muscle contraction and cause muscle stiffness and tightness. Patients with TMs might also experience soreness, swelling, or other types of discomfort in local muscles. In patients with knee OA, TMs mostly occur in the thigh or calf, in which local muscles experience tightness or cramps for an extensive period. Under this condition, the knee joint must adapt to the continuous stress load, which eventually causes hyperostosis and bone damage. FSN treatment aims to restore and enhance knee joint function by eliminating TMs, alleviating muscle tightness and cramps, and reducing pain.33,34
The FSN treatment has clinical value and a scientific basis. However, a deeper and more systematic study of its mechanisms is still lacking. We expect our experiment to verify whether FSN effectively treats pain in the surrounding soft tissue of the knee in patients with knee OA. This study will also discuss the mechanisms underlying FSN treatment regarding how the treatment at the remote end influences the MTrPs in the near end. Our study places FSN treatment on a more robust, scientific basis for use by clinicians.
Conclusion
The findings of this study will reveal whether Fu’s subcutaneous needling or transcutaneous electrical nerve stimulation which is superior to clinical application for treating pain due to knee OA. In addition, focus on mechanism expounding to improve research methods and selecting more objective evaluation system, in order to play a reference role in the future research on Fu’s subcutaneous needling treatment of knee OA.
Acknowledgments
This study was supported by a grant from of the China Medical University Hospital (DMR-109-095) and Asia University Hospital (10951025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Deshpande BR, Katz JN, Solomon DH, et al. Number of Persons With Symptomatic Knee Osteoarthritis in the US: impact of Race and Ethnicity, Age, Sex, and Obesity. Arthritis Care Res. 2016;68:1743–1750. doi:10.1002/acr.22897
2. Zhu ZL, Hou SM, Chen ZG, et al. Evolution of osteoarthritis treatment: mesenchymal stem cells of autologous fat. J Taipei Med Assoc. 2019;63:59–64.
3. Berenbaum F. Osteoarthritis as an inflammatory disease (osteoarthritis is not osteoarthrosis!). Osteoarthritis Cartilage. 2013;21:16–21. doi:10.1016/j.joca.2012.11.012
4. Mobasheri A, Bat M. An update on the pathophysiology of osteoarthritis. Ann Phys Rehabil Med. 2016;59:333–339. doi:10.1016/j.rehab.2016.07.004
5. Øiestad BE, Juhl CB, Eitzen I, Thorlund JB. Knee extensor muscle weakness is a risk factor for development of knee osteoarthritis. A systematic review and meta-analysis. Osteoarthritis Cartilage. 2015;23:171–177. doi:10.1016/j.joca.2014.10.008
6. Kavainio T, Lyytinen T, Tyrväinen E, Sipilä S, Arokoski JP. Physical function and properties of quadriceps femoris muscle in men with knee osteoarthritis. Arch Phys Med Rehabil. 2008;89:2185–2194. doi:10.1016/j.apmr.2008.04.012
7. Slemenda C, Brandt KD, Heilman DK, et al. Quadriceps weakness and osteoarthritis of the knee. Ann Intern Med. 1997;127:97–104. doi:10.7326/0003-4819-127-2-199707150-00001
8. Bennell KL, Wrigley TV, Hunt MA, Lim BW, Hinman RS. Update on the role of muscle in the genesis and management of knee osteoarthritis. Rheum Dis Clin North Am. 2013;39:145–176. doi:10.1016/j.rdc.2012.11.003
9. Li GF, Fu ZH. The enlightenment of Fu’s subcutaneous needling on pain medicine. Zhongguo Zhen Jiu. 2014;34:591–593.
10. Vance CG, Dailey DL, Rakel BA, Sluka KA. Using TENS for pain control: the state of the evidence. Pain Manag. 2014;4:197–209. doi:10.2217/pmt.14.13
11. Osiri M, Welch V, Brosseau L, et al. Transcutaneous electrical nerve stimulation for knee osteoarthritis. Cochrane Database Syst Rev. 2000;2:CD002823.
12. Zeng C, Li H, Yang T, et al. Electrical stimulation for pain relief in knee osteoarthritis: systematic review and network meta-analysis. Osteoarthritis Cartilage. 2015;23:189–202. doi:10.1016/j.joca.2014.11.014
13. Kim ED, Won YH, Park SH, et al. Efficacy and Safety of a Stimulator Using Low-Intensity Pulsed Ultrasound Combined with Transcutaneous Electrical Nerve Stimulation in Patients with Painful Knee Osteoarthritis. Pain Res Manag. 2019;2019:7964897. doi:10.1155/2019/7964897
14. Itoh K, Hirota S, Katsumi Y, Ochi H, Kitakoji H. Trigger point acupuncture for treatment of knee osteoarthritis–a preliminary RCT for a pragmatic trial. Acupunct Med. 2008;26:17–26. doi:10.1136/aim.26.1.17
15. Reed MD, Van Nostran W. Assessing pain intensity with the visual analog scale: a plea for uniformity. J Clin Pharmacol. 2014;54:241–244. doi:10.1002/jcph.250
16. Symonds T, Hughes B, Liao S, Ang Q, Bellamy N. Validation of the Chinese Western Ontario and McMaster Universities Osteoarthritis Index in Patients From Mainland China With Osteoarthritis of the Knee. Arthritis Care Res. 2015;67:1553–1560. doi:10.1002/acr.22631
17. Li SF, Wang XH. Determinants of Health-Related Quality of Life in Patients with Knee Osteoarthritis. Sports Exe Res. 2012;14:387–398.
18. Zhou YL, Liu SY. The Related Factors of Exercise Behaviors and Quality of Life in Knee Osteoarthritis: an Application of Transtheoretical Model. Phys Educ J. 2007;40:51–62.
19. Stucki G, Sangha O, Stucki S, et al. Comparison of the WOMAC (Western Ontario and McMaster Universities) osteoarthritis index and a self-report format of the self-administered Lequesne-Algofunctional index in patients with knee and hip osteoarthritis. Osteoarthritis Cartilage. 1998;6:79–86. doi:10.1053/joca.1997.0097
20. Fischer AA. Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold. Pain. 1987;30:115–126. doi:10.1016/0304-3959(87)90089-3
21. Fischer AA. Pressure threshold meter: its use for quantification of tender spots. Arch Phys Med Rehabil. 1986;67:836–838.
22. Han TI, Hong CZ, Kuo FC, Hsieh YL, Chou LW, Kao MJ. Mechanical pain sensitivity of deep tissues in children–possible development of myofascial trigger points in children. BMC Musculoskelet Disord. 2012;13:13. doi:10.1186/1471-2474-13-13
23. Aird L, Samuel D, Stokes M. Quadriceps muscle tone, elasticity and stiffness in older males: reliability and symmetry using the MyotonPRO. Arch Gerontol Geriatr. 2012;55:e31–39. doi:10.1016/j.archger.2012.03.005
24. Pruyn EC, Watsford ML, Murphy AJ. Validity and reliability of three methods of stiffness assessment. J Sport Health Sci. 2016;5:476–483. doi:10.1016/j.jshs.2015.12.001
25. Wang JS, Um GM, Choi JH. Immediate effects of kinematic taping on lower extremity muscle tone and stiffness in flexible flat feet. J Phys Ther Sci. 2016;28:1339–1342. doi:10.1589/jpts.28.1339
26. Jaworski J, Ambroży T, Lech G, et al. Absolute and relative reliability of several measures of static postural stability calculated using a GYKO inertial sensor system. Acta Bioeng Biomech. 2020;22:94–99. doi:10.37190/ABB-01502-2019-02
27. Hamersma DT, Hofste A, Rijken NHM. Reliability and validity of the Microgate Gyko for measuring range of motion of the low back. Musculoskelet Sci Pract. 2020;45:102091. doi:10.1016/j.msksp.2019.102091
28. World Health Organization. Global Burden of Disease: 2004 Update. Geneva: World Health Organization; 2008.
29. Fu ZH, Chen XY, Lu LJ, Lin J, Xu JG. Immediate effect of Fu’s subcutaneous needling for low back pain. Chin Med J. 2006;119:953–956. doi:10.1097/00029330-200606010-00014
30. Fu ZH, Wang JH, Sun JH, Chen XY, Xu JG. Fu’s subcutaneous needling: possible clinical evidence of the subcutaneous connective tissue in acupuncture. J Altern Complement Med. 2007;13:47–51. doi:10.1089/acm.2006.6125
31. Fu ZH, Hsieh YL, Hong CZ, Kao MJ, Lin JG, Chou LW. Remote subcutaneous needling to suppress the irritability of myofascial trigger spots: an experimental study in rabbits. Evid Based Complement Alternat Med. 2012;2012:353916. doi:10.1155/2012/353916
32. Xiao AJ, Xia YB, Fu ZH, Guo J, Liang S. Review on the role of Fu’s subcutaneous needling (FSN) in pain relieving. Zhongguo Zhen Jiu. 2013;33:1143–1146.
33. Chou LW, Hsieh YL, Kuan TS, Hong CZ. Needling therapy for myofascial pain: recommended technique with multiple rapid needle insertion. Biomedicine. 2014;4:13. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4264979/. Accessed October 6, 2021.
34. Fu ZH. The Foundation of Fu’s Subcutaneous Needling. Beijing: People’sMedical Publishing House; 2016:116–117.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.