Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Evaluating Arrhythmia Risk in Patients with Chronic Obstructive Pulmonary Disease Treated with Aclidinium/Formoterol Fumarate and Other Inhaled Bronchodilators: A Post-Authorization Safety Study
Authors Rebordosa C, Aguado J ![]() , Bartsch J
, Bartsch J ![]() , Saigi-Morgui N
, Saigi-Morgui N ![]() , Carsin AE, Garcia-Esteban R, Ignatova E
, Carsin AE, Garcia-Esteban R, Ignatova E ![]() , Freedman D, Perez-Gutthann S
, Freedman D, Perez-Gutthann S ![]() , Rivero-Ferrer E
, Rivero-Ferrer E ![]()
Received 19 July 2025
Accepted for publication 11 December 2025
Published 16 January 2026 Volume 2026:21 554888
DOI https://doi.org/10.2147/COPD.S554888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vanesa Bellou
Cristina Rebordosa,1 Jaume Aguado,1 Jennifer Bartsch,2 Nuria Saigi-Morgui,1 Anne-Elie Carsin,1 Raquel Garcia-Esteban,1 Elena Ignatova,3 Daniel Freedman,3 Susana Perez-Gutthann,1 Elena Rivero-Ferrer1
1RTI Health Solutions, Barcelona, Spain; 2RTI Health Solutions, Research Triangle Park, NC, USA; 3Covis Pharma Gmbh, a Wholly-Owned Subsidiary of Azurity Pharmaceuticals, Inc., Woburn, MA, USA
Correspondence: Cristina Rebordosa, RTI Health Solutions, Av. Diagonal, 605, 9-1, Barcelona, 08028, Spain, Tel +34 932 41 77 66, Email [email protected]
Purpose: A post-authorization safety study program examined the cardiovascular safety of the long-acting muscarinic antagonist (LAMA) aclidinium bromide monotherapy and the LAMA/long-acting β2-agonist (LABA) aclidinium bromide/formoterol fumarate. We assessed frequency and risk of any cardiac arrhythmias (CA), atrial fibrillation (AF), and serious ventricular arrhythmias (SVA) in aclidinium and aclidinium/formoterol users.
Patients and Methods: This population-based cohort study included adults with chronic obstructive pulmonary disease (COPD) initiating COPD medications in the UK Clinical Practice Research Datalink Aurum database (Jan 2015-Mar 2021). CA, AF, and SVA incidence rate ratios (IRR) were estimated using Poisson regression models for continuous current users initiating aclidinium and aclidinium/formoterol versus LABA, and during the first episode of current single use for aclidinium versus LAMA and aclidinium/formoterol versus LAMA/LABA, adjusting for clinically relevant covariables.
Results: The study included a total of 248,148 initiators. For CA and AF, respectively, adjusted IRRs (95% confidence intervals [CIs]) ranged from 0.98 (0.69– 1.41) for LAMA/LABA to 2.08 (1.36– 3.18) for aclidinium/formoterol and from 0.83 (0.55– 1.24) for LAMA/LABA to 1.85 (1.15– 3.00) for aclidinium/formoterol versus current LABA use. For current single use (first episode), adjusted IRRs (95% CIs) for CA and AF were 1.46 (0.93– 2.29) and 1.57 (0.94– 2.62) for aclidinium versus other LAMAs, and 2.15 (1.33– 3.49) and 1.79 (0.96– 3.33) for aclidinium/formoterol versus LAMA/LABA, respectively. There were few SVA events.
Conclusion: CA and AF risks were increased for most study medications compared with LABA. Increased risks of CA and AF for several medications relative to LABA, LAMA, or LAMA/LABA may be driven by differences in baseline characteristics (eg, COPD severity).
Keywords: aclidinium, arrhythmia, LAMA, LABA, United Kingdom
Introduction
Inhaled bronchodilators, including long-acting muscarinic antagonists (LAMAs) and long-acting β2-agonists (LABA), are recommended in international treatment guidelines for the management of chronic obstructive pulmonary disease (COPD).1 The LAMA, aclidinium bromide 322 µg twice daily, was approved by the European Medicines Agency in July 2012, and aclidinium bromide combined with the LABA, formoterol fumarate 322/12 µg twice daily, was approved in November 2014 for the treatment of COPD.2,3 Both aclidinium bromide and aclidinium bromide/formoterol fumarate have been demonstrated to improve lung function and health status and have similar safety and tolerability profiles compared with placebo and bronchodilator monotherapy in patients with COPD, with no observed differences in arrhythmia risk.4–7
Treatments for COPD have been independently associated with mechanisms that can initiate cardiac arrhythmias and atrial fibrillation, such as chronotropic effects due to β2-adrenergic agonists8 and suppression of the parasympathetic system due to anticholinergic effects.9 In addition, COPD itself, frequent COPD exacerbations, low forced expiratory volume in 1 second (FEV1), and forced vital capacity (FVC) increase the risk of atrial fibrillation.10–13 Evidence from previous studies suggests that the LAMAs, tiotropium and ipratropium bromide, may be associated with an increased risk of adverse cardiovascular outcomes.14–20 However, data from previous population-based studies have reported inconsistent results.14–20 In addition, few studies on the cardiovascular safety of LAMAs have evaluated cardiac arrhythmias, although those that performed this evaluation did not find an increased risk of these events compared with beta-agonists.21–23 Consequently, a post-authorization safety study (PASS) program was initiated to examine the cardiovascular safety of aclidinium bromide monotherapy and aclidinium bromide/formoterol fumarate (EUPAS13616; HMA-EMA ID 42316). Previously reported data from the PASS evaluated the risks of all-cause mortality, heart failure, myocardial infarction, and stroke associated with these therapies.24–26 These studies found that risks of all-cause mortality;24 hospitalization for congestive heart failure;25 or acute myocardial infarction, stroke, and major adverse cardiac events26 were not increased in new users of aclidinium, aclidinium/formoterol, tiotropium, other LAMA, other LAMA/LABA combinations, or LABA/inhaled corticosteroid (ICS) compared with LABA monotherapy.
The objective of this substudy of the PASS was to assess the incidences of any cardiac arrhythmias, atrial fibrillation, and serious ventricular arrhythmias in new users of aclidinium compared with new users of LABA and other LAMA, and in new users of aclidinium/formoterol compared with new users of LABA and LAMA/LABA.
Methods
Study Design and Setting
This was a population-based cohort study of patients with a recorded diagnosis of COPD initiating selected COPD medications from January 2015 through March 2021 (Figure S1). The study was conducted using the UK Clinical Practice Research Datalink (CPRD) Aurum primary care database and included all practices where linkage was available to obtain information on date and cause of death from the Office for National Statistics (ONS) and information on hospitalizations from the Hospital Episode Statistics (HES) database. CPRD Aurum contains anonymized routine clinical practice data from approximately 15 million registered patients (23.4% of the UK population) as of November 2022. The index date was defined as the date of the first prescription of a selected COPD medication. Follow-up started on the date of COPD medication initiation and ended at the earliest of an occurrence of selected endpoint, death, disenrollment, or end of the study period (latest date of the period covered by both HES and ONS data).
Study data were stored on a secure, access-controlled server. Due to CPRD small cell count policy, patient counts with fewer than 5 observations have been reported as “1 ≤ n < 5” with no person-years reported. In the event that the sum of components were additive and back calculation could be performed using the total number of events, cells with numbers above 5 have been masked.
The study protocol was approved by the Independent Scientific Advisory Committee of the Medicines and Healthcare products Regulatory Agency (protocol 21_000506) on 8 October 2021. The RTI Institutional Review Board reviewed the study protocol (STUDY00021693) and determined on 9 September 2021 that, because this study did not involve private, identifiable, human-patient data nor interaction with any human patients, institutional review board approval and informed consent were not required. The research team did not have access to identifying patient information.
Cohort Selection
Patients in the study were new users of the following medicines: aclidinium bromide; aclidinium/formoterol; or other COPD medications, including tiotropium, other LAMA, LABA, other LAMA/LABA, LABA/ICS, or LAMA/LABA/ICS combinations. Other LAMAs included glycopyrronium bromide and umeclidinium. LABAs included formoterol, salmeterol, indacaterol, and olodaterol. LAMA/LABA combinations included glycopyrronium/indacaterol, umeclidinium/vilanterol, and tiotropium/olodaterol. LABA/ICS combinations included formoterol/budesonide, formoterol/beclometasone, formoterol/fluticasone, salmeterol/fluticasone propionate, and vilanterol/fluticasone. LAMA/LABA/ICS combinations included glycopyrronium/formoterol/beclometasone, glycopyrronium/indacaterol/mometasone, and umeclidinium/vilanterol/fluticasone.
Eligible patients were aged ≥40 years at the index date, had a recorded COPD diagnosis (International Classification of Disease, 10th edition [ICD-10] codes J40–J44) with or without asthma any time or within 30 days after the index date, and had no prescription for the same COPD medication or medication group during the 6 months before the index date. Patients were also required to have ≥1 year of CPRD enrollment before the index date and to be enrolled in a practice eligible for HES and ONS linkage. Patients were excluded if they had a prior diagnosis of a cardiac arrhythmia at any time before the index date, a prescription for digoxin or anticoagulant, a history of cancer, were receiving palliative care, had serious non-cardiovascular life-threatening conditions or severe comorbidities, or had missing data on smoking or body mass index (BMI).
Patients might have received prescriptions for the same COPD medication or medication group ≥6 months before the index date or for other COPD medications at any time before the index date.
Variables and Outcomes
Study medication exposure was determined based on prescription records and days’ supply calculated from prescription instructions. Missing information was imputed using the mode of days’ supply for each medication, strength, and quantity prescribed, when available. Time at risk for the effects of study medication was based on days’ supply plus a 7-day extension period. Current medication use was defined as the sum of all episodes of continuous use. Current single medication use was defined as the sum of all episodes of continuous use of a single study medication group, not concurrently with any other study medication group. Analysis using LAMA or LAMA/LABA as a reference was restricted to the first episode of continuous current single use. Periods of continuous medication use were defined as consecutive prescriptions where there was a gap less than 7 days between the end of one prescription and the start of the next. Medication use was further stratified based on duration of continuous use: short if the sum of episodes was <6 months and long if the sum was ≥6 months.
Study outcomes included any cardiac arrhythmias, atrial fibrillation, and serious ventricular arrhythmias that resulted in hospitalization (identified by a primary discharge diagnosis on HES data) or events resulting in death where the event was the main cause of death, identified from ICD-10 codes in ONS data. Serious ventricular arrhythmias included torsade de pointes, ventricular tachycardia, and ventricular fibrillation or flutter.
Potential confounding factors included age, assessed at the index date; as well as sex, race/ethnicity, BMI, smoking history, alcohol use history, socioeconomic status, healthcare resource utilization, comorbidities, comedications, and severity of Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2016 stage, all assessed before the index date.
Statistical Analyses
Cohort characteristics were summarized descriptively. Crude and adjusted incidence rates, as well as incidence rate ratios (IRRs), with 95% confidence intervals (CIs), for any cardiac arrhythmia, atrial fibrillation, and serious ventricular arrhythmia events were estimated using Poisson regression models; these models were adjusted for clinically relevant risk factors, including age, sex, and COPD severity, which were forced to be included in the model. If the number of events allowed it, then other potential confounding variables also were included. A forward approach was used to determine the inclusion of additional potential confounding variables (eg, variables associated with both the endpoint and being a new user of aclidinium/formoterol versus LABA) in the final Poisson regression models. Each of the remaining confounding factors with a prevalence ≥5% was included in the Poisson regression models if it changed the magnitude of the model coefficient estimates by ≥10%.
For history of medical conditions and drug exposure, the absence of a code was interpreted as an absence of the condition or exposure.
Statistical significance or its proxies was not used to interpret study results. All analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, North Carolina).
Results
Cohort Characteristics
Of the 1,345,954 patients identified as having used the selected COPD medications, 248,148 met the study eligibility criteria and were included in study cohorts (Figure 1). In total, 11,766 patients were included in the LABA cohort, 11,126 in the aclidinium cohort, 7682 in the aclidinium/formoterol cohort, 54,694 in the tiotropium cohort, 29,564 in the other LAMA cohort, 30,974 in the LAMA/LABA cohort, 71,104 in the LABA/ICS cohort, and 31,238 in the LAMA/LABA/ICS cohort.
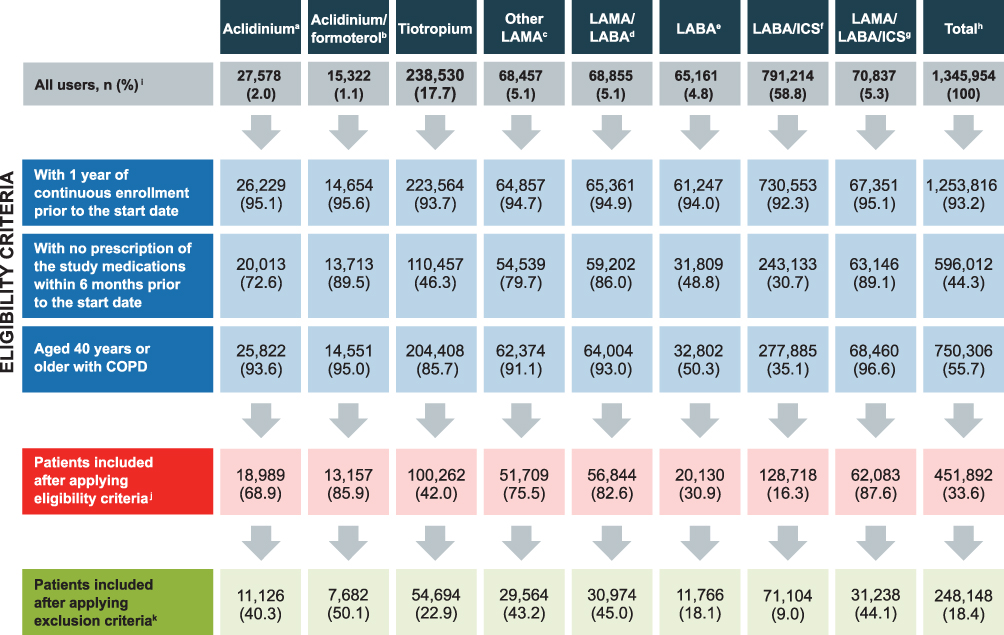 |
Figure 1 Cohort Attrition. aAclidinium bromide group includes aclidinium bromide with or without concomitant use of formoterol fumarate in a free-dose combination. It does not include aclidinium/formoterol in a fixed-dose combination. bFixed-dose combination of aclidinium bromide and formoterol fumarate. cOther LAMA includes glycopyrronium and umeclidinium. dLAMA/LABA includes umeclidinium/vilanterol, glycopyrronium/indacaterol, tiotropium/olodaterol, and glycopyrrolate/formoterol. eLABA includes formoterol, salmeterol, olodaterol, and indacaterol. fLABA/ICS includes formoterol/budesonide, formoterol/beclomethasone, indacaterol/mometasone, formoterol/fluticasone, salmeterol/fluticasone propionate, and vilanterol/fluticasone. gLAMA/LABA/ICS includes umeclidinium/vilanterol/fluticasone, glycopyrronium/indacaterol/mometasone, glycopyrrolate/formoterol/budesonide, and glycopyrronium/formoterol/beclomethasone. hThe numbers represent cohort users and, because a patient may enter more than one cohort, totals might include the same patient more than once. iPercentages in the row are row percentages over the “Total.” The rest of the percentages in the table are column percentages over the total number of “all users” in each column. jEligibility criteria were assessed at each prescription recorded within the study period for each user of the study medication. For those patients not included in the cohort, the eligibility criteria were assessed through their last prescription within the study period. kExclusion criteria: cancer or other serious, non-cardiovascular life-threatening conditions or indicators of severe comorbidity recorded in the database at any time before the index date; missing data on smoking or body mass index; patients with a prior diagnosis of any cardiac arrhythmia, including atrial fibrillation ever before the index date; and patients with a prescription of digoxin or anticoagulation treatment in the 12 months before the index date. Abbreviations: COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting anticholinergic. |
Patients who were included had a mean age of 67.3–69.5 years; 46.5–51.5% were male, 63.4–67.6% were overweight or obese, 10.7–12.3% were classified as heavy drinkers, and 44.2–49.6% were current smokers (Table 1). Some heterogeneity was observed in the study cohorts’ clinical characteristics. The LAMA/LABA/ICS cohort had the largest proportion of patients with GOLD C or D COPD (67.6%), followed by the aclidinium group (52.8%), and the LABA group had the largest proportion with GOLD A COPD (43.5%), followed by LABA/ICS (40.2%). A similar proportion of patients across cohorts had a history of ischemic heart (19.0–21.3%) and cerebrovascular diseases (10.2–12.1%); the mean Charlson Comorbidity Index (CCI) score was 0.9–1.0. LABA/ICS and tiotropium were the study medications most frequently prescribed within 12 months before the index date. Use of cardiovascular medications ranged from 66.6% in the LABA/ICS cohort to 72.0% in the LAMA/LABA/ICS cohort (Table 1).
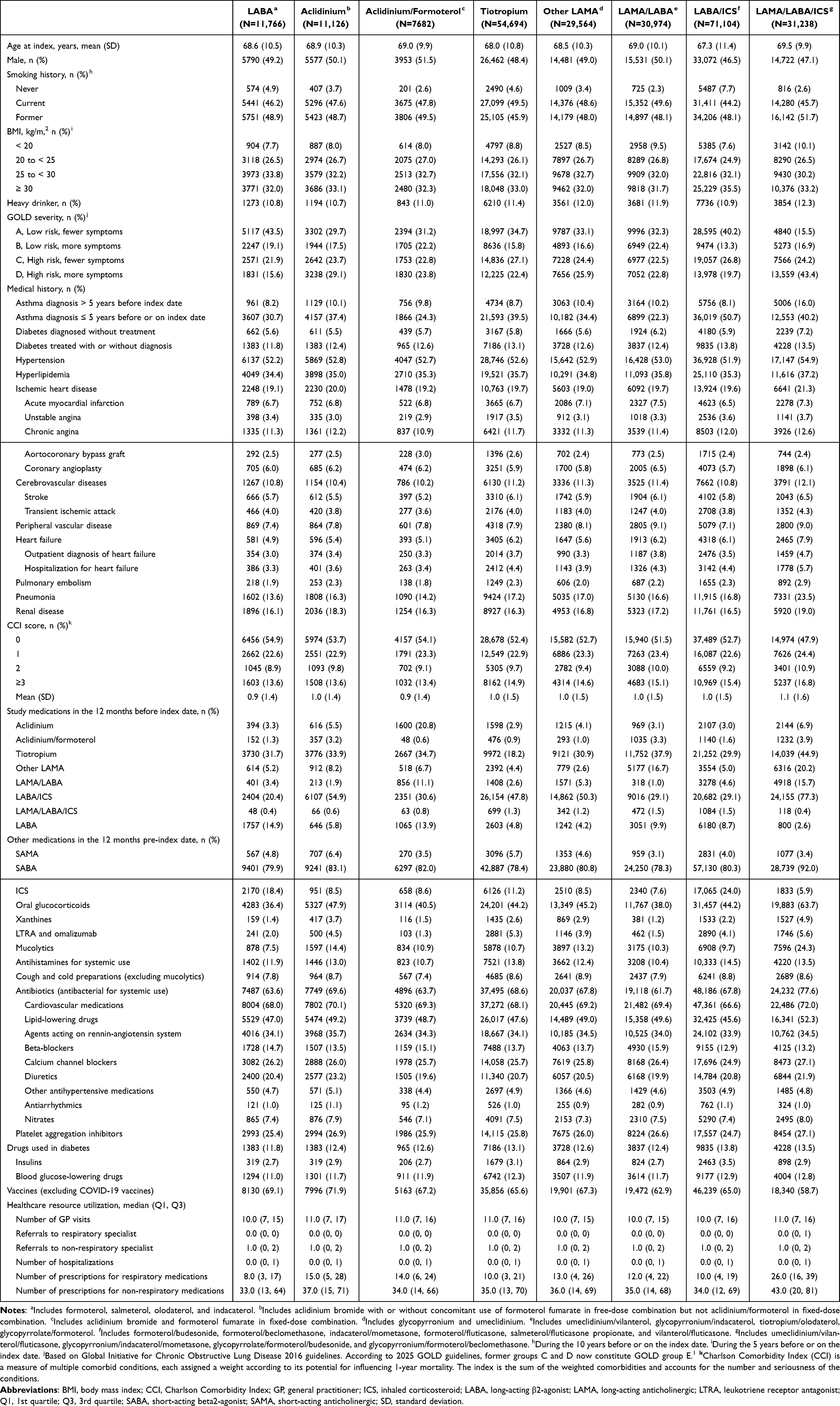 |
Table 1 Patient Demographics and Baseline Characteristics |
Aclidinium, Aclidinium/Formoterol, and Other COPD Medications versus LABA
The first set of analyses compared aclidinium, aclidinium/formoterol, tiotropium, other LAMA, other LAMA/LABA, LABA/ICS, or LAMA/LABA/ICS combinations relative to LABA medications, encompassing formoterol, salmeterol, olodaterol, and indacaterol. The crude incidence rates of any cardiac arrhythmias per 1000 person-years ranged from 4.11 for LAMA/LABA to 7.49 for aclidinium/formoterol during current use and from 3.53 for LABA to 7.01 for aclidinium/formoterol during current single use. The crude incidence rates of atrial fibrillations per 1000 person-years ranged from 2.85 for LAMA/LABA to 5.38 for aclidinium/formoterol during current use and from 2.76 for LAMA/LABA to 5.02 for aclidinium/formoterol during current single use. For serious ventricular arrhythmias, the number of events was very low, resulting in crude incidence rates below 1 per 1000 person-years (Table S1).
Compared with current use of LABA, adjusted IRRs (95% CI) for any cardiac arrhythmias and atrial fibrillation ranged, respectively, from 0.98 (0.69–1.41) for LAMA/LABA to 2.08 (1.36–3.18) for aclidinium/formoterol and from 0.83 (0.55–1.24) for LAMA/LABA to 1.85 (1.15–3.00) for aclidinium/formoterol (Figure 2A and B). Due to the very low number of serious ventricular arrhythmia events, the precision of effect estimates was low (Figure 2C and Table S1). For any cardiac arrhythmia, a slight increase in risk was noted with short-duration use across all medications except aclidinium/formoterol, whereas for atrial fibrillation, IRRs were generally close to or below 1 for most comparisons. When analyses were restricted to current single use, the risk of both any cardiac arrhythmias and atrial fibrillation was higher for all study medications compared with current single use of LABA, except for the LAMA/LABA/ICS combination (Figure 3A and B).
Figure 2 Continued. Figure 2 Adjusted Incidence Rate Ratio for Any Cardiac Arrhythmias, Atrial Fibrillation, and Serious Ventricular Arrhythmias During Current Use, Current Use of Long Duration, and Current Use of Short Duration of Each Study Medication Versus Current Use of LABA. (A) Any Cardiac Arrhythmias: Current Use, Current Use of Short Duration, and Current Use of Long Durationa, b (B) Atrial Fibrillation: Current Use, Current Use of Short Duration, and Current Use of Long Durationa, b (C) Serious Ventricular Arrhythmias: Current Use of Short Duration, and Current Use of Long Durationa, c aThe numbers in parentheses are the number of outcome events in each cohort. Vertical bars represent 95% confidence intervals of the incidence rate ratio estimates. bIncidence rate ratios were estimated using a Poisson regression model adjusted for age, sex, COPD severity, calendar period, number of prescriptions for respiratory medications, use of aclidinium in 12 months before the index date, number of referrals to non-respiratory specialist, prior use of diuretics, use of LABA/ICS in 12 months before the index date, ischemic heart disease, smoking history, body mass index, hypertension, heart failure, heavy drinking status, and diabetes. cIncidence rate ratios were estimated using a Poisson regression model adjusted by age, sex, and COPD severity. Abbreviations: COPD, chronic obstructive pulmonary disease; CPRD, ClinicalPractice Research Datalink; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting anticholinergic. Note: Per CPRD small cell count policy, cell counts with an n between 1 and 4 have been reported as “1 ≤ n < 5” with no person-years reported. The sum of components is not additive; therefore, no back calculation can be performed using the total number of events. LABA includes formoterol, salmeterol, olodaterol, and indacaterol. Aclidinium includes aclidinium bromide with or without concomitant use of formoterol fumarate in a free-dose combination. It does not include aclidinium/formoterol in a fixed-dose combination. Aclidinium/formoterol includes a fixed-dose combination of aclidinium bromide and formoterol fumarate. Other LAMA includes glycopyrronium and umeclidinium. LAMA/LABA includes umeclidinium/vilanterol, glycopyrronium/indacaterol, tiotropium/olodaterol, and glycopyrrolate/formoterol. LABA/ICS includes formoterol/budesonide, formoterol/beclomethasone, indacaterol/mometasone, formoterol/fluticasone, salmeterol/fluticasone propionate, and vilanterol/fluticasone. LAMA/LABA/ICS includes umeclidinium/vilanterol/fluticasone, glycopyrronium/indacaterol/mometasone, glycopyrrolate/formoterol/budesonide, and glycopyrronium/formoterol/beclomethasone.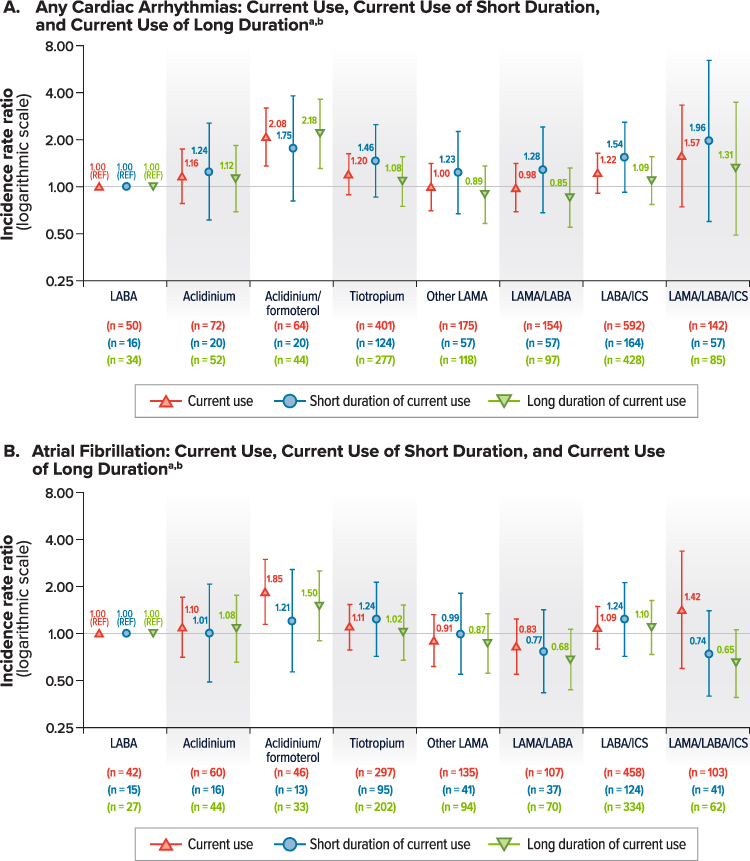
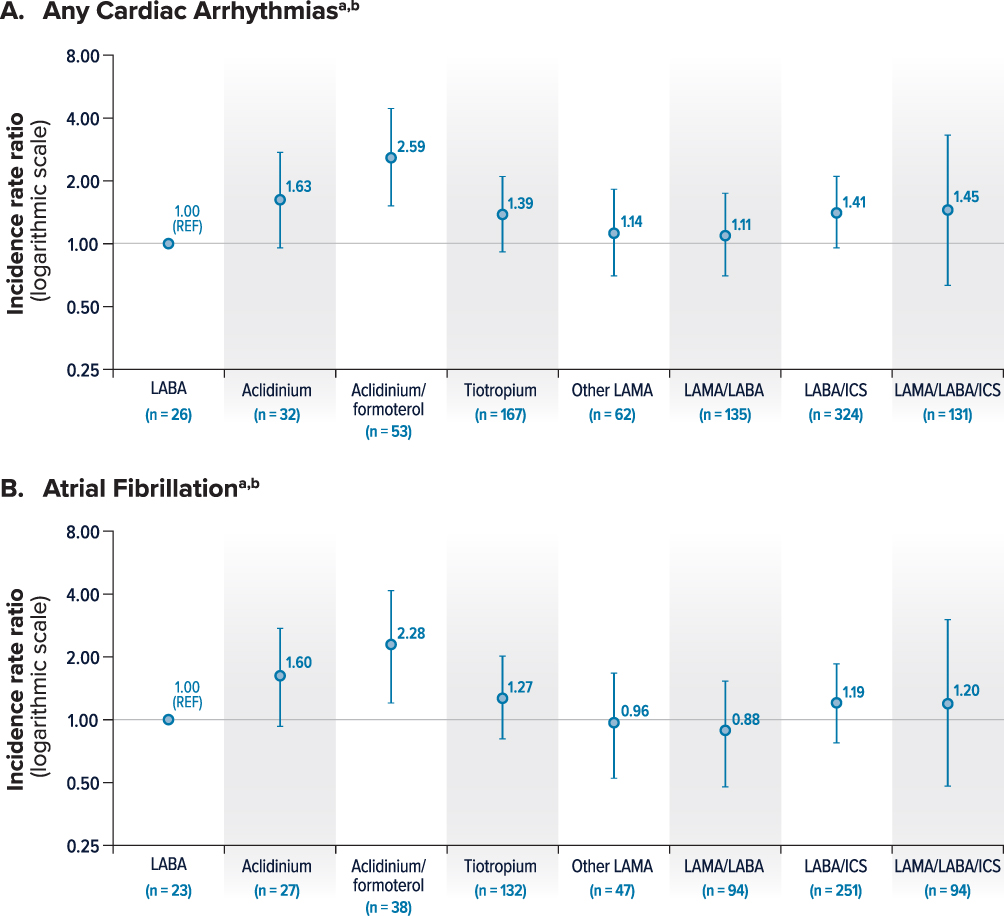 |
Figure 3 Adjusted Incidence Rate Ratio for Any Cardiac Arrhythmias and Atrial Fibrillation for Current Single Use of Each Study Medication Versus Single Use of LABA. (A) Any Cardiac Arrhythmias.a,b (B) Atrial Fibrillation.a,b aThe numbers in parentheses are the number of any cardiac arrhythmia events or atrial fibrillation during current single use in each cohort. Vertical bars represent 95% confidence intervals of the incidence rate ratio estimates. bIncidence rate ratios were estimated using a Poisson regression model adjusted by age, sex, COPD severity, and calendar year. Abbreviations: COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; LABA, long-acting beta2-agonist; LAMA, long-acting anticholinergic. Note: LABA includes formoterol, salmeterol, olodaterol, and indacaterol. Aclidinium includes aclidinium bromide with or without concomitant use of formoterol fumarate in a free-dose combination. It does not include aclidinium/formoterol in a fixed-dose combination. Aclidinium/formoterol includes a fixed-dose combination of aclidinium bromide and formoterol fumarate. Other LAMA includes glycopyrronium and umeclidinium. LAMA/LABA includes umeclidinium/vilanterol, glycopyrronium/indacaterol, tiotropium/olodaterol, and glycopyrrolate/formoterol. LABA/ICS includes formoterol/budesonide, formoterol/beclomethasone, indacaterol/mometasone, formoterol/fluticasone, salmeterol/fluticasone propionate, and vilanterol/fluticasone. LAMA/LABA/ICS includes umeclidinium/vilanterol/fluticasone, glycopyrronium/indacaterol/mometasone, glycopyrrolate/formoterol/budesonide, and glycopyrronium/formoterol/beclomethasone. |
Aclidinium versus LAMA
The second set of analyses compared aclidinium relative to LAMA medications, encompassing glycopyrronium and umeclidinium. For overall current single use of aclidinium and other LAMAs, the crude incidence rates per 1000 person-years for any cardiac arrhythmias were 6.17 and 4.15, respectively, and 4.80 and 3.03 for atrial fibrillation, respectively. The adjusted IRR (95% CI) for current single use of aclidinium versus other LAMAs was 1.46 (0.93–2.29) for any cardiac arrhythmias and 1.57 (0.94–2.62) for atrial fibrillation (Figure 4A and B, Table S2). When stratifying by use of ICS, the adjusted IRRs (95% CI) among the 2% of concomitant ICS users were 2.53 (0.42–15.28) for any cardiac arrhythmias and 3.83 (0.53–27.66) for atrial fibrillation, respectively (Table S2). There were small numbers of events or no events for serious ventricular arrhythmias, precluding the estimation of IRRs.
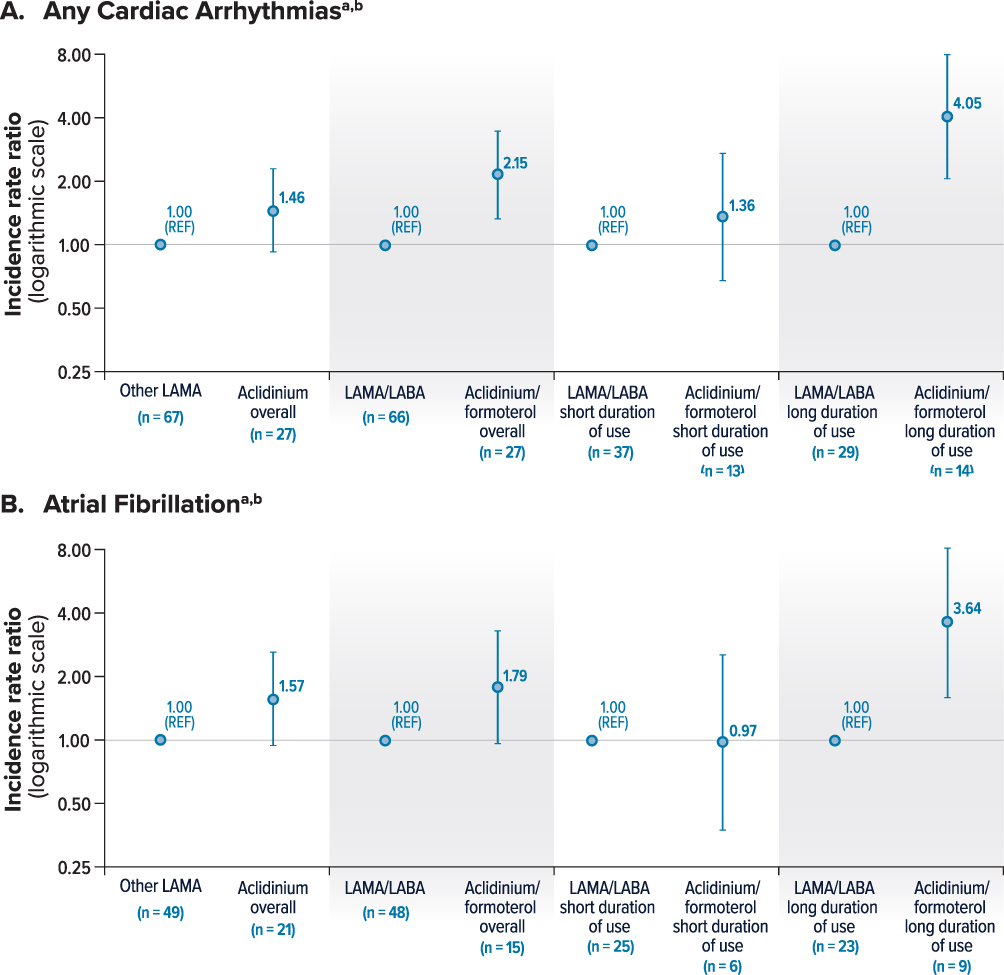 |
Figure 4 Adjusted Incidence Rate Ratios for Any Cardiac Arrhythmias and Atrial Fibrillation by Current Single Use of Aclidinium Versus Current Single Use of Other LAMA, and Current Single Use of Aclidinium/Formoterol Versus Current Single Use of Other LAMA/LABA During the First Episode of Continuous Use, Overall and by Duration of Use. (A) Any Cardiac Arrhythmiasa,b (B) Atrial Fibrillationa,b aThe numbers in parentheses are the number of any cardiac arrhythmia events or atrial fibrillation events during the first episode of current single use in each cohort. Vertical bars represent 95% confidence intervals of the incidence rate ratio estimates. bIncidence rate ratios were estimated using a Poisson regression model adjusted by age, sex, and COPD severity. Abbreviations: COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist; LAMA, long-acting anticholinergic; n, number of events; REF, reference. Note: Other LAMA includes glycopyrronium and umeclidinium. Aclidinium includes aclidinium bromide with or without concomitant use of formoterol fumarate in a free-dose combination. It does not include aclidinium/formoterol in a fixed-dose combination. LAMA/LABA includes umeclidinium/vilanterol, glycopyrronium/indacaterol, tiotropium/olodaterol, and glycopyrrolate/formoterol. Aclidinium/formoterol includes a fixed-dose combination of aclidinium bromide and formoterol fumarate. |
Aclidinium/Formoterol versus LAMA/LABA
The third set of analyses compared aclidinium/formoterol relative to LAMA/LABA regimens, encompassing umeclidinium/vilanterol, glycopyrronium/indacaterol, tiotropium/olodaterol, and glycopyrrolate/formoterol. For overall current single use of aclidinium/formoterol and LAMA/LABA, the crude incidence rates per 1000 person-years for any cardiac arrhythmias were 9.14 and 4.15, respectively, and 5.07 and 3.02 for atrial fibrillation, respectively; similar trends were seen for patients without concomitant ICS (Table S3).
The adjusted IRR (95% CI) for current single use of aclidinium/formoterol versus LAMA/LABA was 2.15 (1.33–3.49) for any cardiac arrhythmias and 1.79 (0.96–3.33) for atrial fibrillation (Figure 4A and B, Table S3). IRRs for serious ventricular arrhythmias were not estimated as there were <5 and no events for aclidinium/formoterol and LAMA/LABA users, respectively. When stratified by ICS use, the adjusted IRR for any cardiac arrhythmias and atrial fibrillation could not be estimated among the 4.3% of aclidinium/formoterol users and the 2.9% of LAMA/LABA users who were concomitant ICS users due to the absence of events in the aclidinium/formoterol cohort. When comparing short durations of current single use, the adjusted IRR (95% CI) was 1.36 (0.68–2.73) for any cardiac arrhythmias and 0.97 (0.37–2.54) for atrial fibrillation among aclidinium/formoterol users versus LAMA/LABA users. For long durations of current single use, the adjusted IRR was 4.05 (2.05–7.98) for any cardiac arrhythmias and 3.64 (1.60–8.26) for atrial fibrillation (Figure 4A and B).
Discussion
In this population-based cohort study, compared with LABA use, current use of aclidinium/formoterol and LAMA/LABA/ICS was associated with an increased risk of any cardiac arrhythmias and atrial fibrillation, whereas a slightly elevated risk was also observed among users of aclidinium, tiotropium, and LABA/ICS. The magnitude of the increased risk was higher when the analysis was restricted to the first episode of continuous current single use. During the first 6 months of use (short duration of use), the magnitude of the risk of any cardiac arrhythmias also tended to be higher, whereas the magnitude of the risk of atrial fibrillation was lower or null. The analysis results of the current use of study medications beyond 6 months (long duration of use) showed that the risk of any cardiac arrhythmias was lower in magnitude compared with the risk observed with overall current use. Indirect comparison of these initial results suggested that aclidinium and aclidinium/formoterol may have a higher risk of arrhythmias than other LAMA or LAMA/LABA combinations. For this reason, additional analyses were performed directly comparing with LAMA and with LAMA/LABA medications as a reference. Compared with LAMA use, current single use of aclidinium was associated with a 50% increased risk of any cardiac arrhythmias and atrial fibrillation. Additionally, during the first episode of continuous use, aclidinium/formoterol was associated with approximately a two-fold increased risk of any cardiac arrhythmias and atrial fibrillation compared with LAMA/LABA. As observed in comparisons with LABA, no increased risk of atrial fibrillation was observed during the first 6 months of use (short duration of use).
Risk differences that were observed across varying durations of use of the study medications may be driven by a number of factors. Risk assessment during episodes of current use allowed the inclusion of more periods of medication exposure because it included person-time of exposure to a study medication that was restarted after a period of non-exposure. However, this may have led to time-varying confounding and residual confounding that may explain the lower magnitude of risk observed over a long duration of use relative to overall use. Such confounding cannot be ruled out in patients who remained on study medication for longer durations, as their characteristics may have changed after 6 months of initiation and may differ from those of patients with a shorter duration of use. In addition, the definition of current use may have introduced the potential for selection bias by including people who restarted the medication because they survived, tolerated the medications, or restarted after an acute decompensation or exacerbation. Additional analyses restricted the duration of exposure to the first episode of use, irrespective of concomitant medications (ie, among current single users). In analyses evaluating the first episode of continuous current use over a short duration, the observed greater risk of any cardiac arrhythmias alongside a lower risk of atrial fibrillation suggests that arrhythmias other than atrial fibrillation (ie, paroxysmal tachycardia and unspecified cardiac arrhythmias) are driving the overall arrhythmia risk during the first 6 months of use. This is in line with several studies suggesting an increased risk of adverse cardiovascular outcomes with the initiation of LAMA/LABA therapy.27,28 On the other hand, results for the first episode of continuous current use over a long duration showed an increased risk, both of any cardiac arrhythmias and of atrial fibrillation, suggesting that the increased risk of any cardiac arrhythmias during long-term use is driven by atrial fibrillation.
Differences in pharmacokinetic and pharmacodynamic parameters or clinical effectiveness among LAMAs do not appear to account for the observed variation in arrhythmia risk, including the short-term occurrence of tachycardias and the long-term development of atrial fibrillation. Independent of medication use, COPD itself, and COPD exacerbations have been associated with an increased risk for atrial fibrillation but not for other arrhythmias.29,30 Differences in effectiveness preventing COPD exacerbations have not been described and were not evaluated in this study. An alternative explanation is that the different baseline characteristics of aclidinium users may have inherently increased their risk of COPD exacerbations or arrhythmias. Consequently, the observed associations could be influenced by unmeasured confounding at baseline and by time-varying confounding related to exacerbations occurring during follow-up.
The risk of any cardiac arrhythmias and atrial fibrillation among non-users of ICS did not differ from the main analysis, likely because the majority of subjects were not using ICS. Among ICS users, the risk estimates had low precision or could not be estimated due to the limited number of events. Use of ICS has not been associated with an increase in the risk of arrhythmias; thus, it is possible that the increased risks observed when comparing aclidinium with other LAMAs are, at least in part, due to baseline patient characteristics associated with an increased risk of the endpoints of interest (eg, higher COPD severity and more COPD exacerbations).
In addition to residual and time-varying confounding, this study has other potential limitations that should be considered when interpreting results. The study was conducted using health information recorded in automated population-based databases, which can be subject to misclassification of exposure, particularly if prescription adherence is poor. Potential outcome misclassification was minimized by using validated definitions with a positive predictive value of approximately 80%.31 The precision of the IRRs for serious ventricular arrhythmias was low due to the small number of these events in patients included in this study. Finally, because each LAMA or LABA/LAMA combination regimen evaluated in this study may have distinct risk profiles, comparisons at the class level may obscure some specific drug-substance differences in relative risk.
Conclusions
The risk of any cardiac arrhythmias and atrial fibrillation was increased for most study medications when compared with LABA. However, these analyses included patients who were also using other concomitant medications, were at different stages of COPD treatment, and may have discontinued and restarted therapy. Analysis compared with LABA indirectly suggested that the risk of arrhythmias might be higher among users of aclidinium and aclidinium/formoterol than among users of other LAMA and LAMA/LABA therapies. A direct evaluation of the risk of arrhythmias during the first episode of current single use for users of aclidinium compared with LAMA users, and users of aclidinium/formoterol compared with LAMA/LABA users, suggested an increased short-term risk of tachycardia after exposure and an increased long-term risk of atrial fibrillation. These results are not supported by literature reporting any pharmacokinetic, pharmacodynamic, or effectiveness differences between LAMAs. They do suggest that the observed associations may be driven by differences in baseline patient characteristics—such as COPD severity—that inherently increase the risk of exacerbations or arrhythmias. Because individual LAMA or LABA/LAMA combination regimens may have distinct risk profiles, the class-level comparisons conducted in this study potentially obscure differences in relative risk associated with specific drugs.
Data Sharing Statement
This study is based in part on data from the Clinical Practice Research Datalink obtained under license from the UK Medicines and Healthcare products Regulatory Agency. The data are provided by patients and collected by the National Health Service as part of their care and support. The interpretation and conclusions contained in this study are those of the authors alone. The same applies to the use of the Office of National Statistics and Health Episodes Statistics data, copyright © 2025, re-used with the permission of the Health & Social Care Information Centre. All rights are reserved.
Acknowledgments
Medical writing services were provided by Alex Lowe and Kate Lothman; editorial services were provided by John Forbes; and graphic design services were provided by Jason Crouch, all with funding from Covis Pharma GmbH, a wholly-owned subsidiary of Azurity Pharmaceuticals, Inc. Covis Pharma GmbH, a wholly-owned subsidiary of Azurity Pharmaceuticals, Inc., Woburn, MA, United States, was Dr Elena Ignatova’s affiliation at the time of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Cristina Rebordosa, Jaume Aguado, Jennifer Bartsch, Nuria Saigi-Morgui, Anne-Elie Carsin, Raquel Garcia-Esteban, Susana Perez-Gutthann, and Elena Rivero-Ferrer are full-time employee of RTI Health Solutions, a unit of RTI International, a nonprofit organization that conducts work for government, public, and private organizations, including pharmaceutical companies, such as AstraZeneca and Covis Pharma GmbH. Susana Perez-Gutthann reports grants from Astra Zeneca and grants from Covis Pharma GmbH during the conduct of the study. Daniel Freedman is an employee and at the time of this study Elena Ignatova was an employee of Covis Pharma GmbH, a wholly-owned subsidiary of Azurity Pharmaceuticals, Inc., which funded the development of this publication. The authors report no other conflicts of interest in this work.
References
1. GOLD. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2025 report). 2025. Available from: https://goldcopd.org/wp-content/uploads/2024/11/GOLD-2025-Report-v1.0-15Nov2024_WMV.pdf.
2. EMA. Eklira Genuair (Aclidinium bromide) Summary of Product Characteristics. 24, May 2017. Available from: https://www.ema.europa.eu/en/documents/product-information/eklira-genuair-epar-product-information_en.pdf.
3. EMA. Duaklir Genuair (aclidinium bromide/formoterol) Summary of Product Characteristics. 23, August 2019. Available from: https://www.ema.europa.eu/en/documents/product-information/duaklir-genuair-epar-product-information_en.pdf.
4. D’Urzo A, Rennard S, Kerwin E, et al. A randomised double-blind, placebo-controlled, long-term extension study of the efficacy, safety and tolerability of fixed-dose combinations of Aclidinium/formoterol or monotherapy in the treatment of chronic obstructive pulmonary disease. Respir Med. 2017;125:39–15. doi:10.1016/j.rmed.2017.02.008
5. D’Urzo AD, Rennard SI, Kerwin EM, Mergel V, Leselbaum AR, Caracta CF. Efficacy and safety of fixed-dose combinations of Aclidinium bromide/formoterol fumarate: the 24-week, randomized, placebo-controlled AUGMENT COPD study. Respir Res. 2014;15(1):123. doi:10.1186/s12931-014-0123-0
6. Gelb AF, Tashkin DP, Make BJ, Zhong X, Garcia Gil E, Caracta C. Long-term safety and efficacy of twice-daily Aclidinium bromide in patients with COPD. Respir Med. 2013;107(12):1957–1965. doi:10.1016/j.rmed.2013.07.001
7. Singh D, Jones PW, Bateman ED, et al. Efficacy and safety of Aclidinium bromide/formoterol fumarate fixed-dose combinations compared with individual components and placebo in patients with COPD (ACLIFORM-COPD): a multicentre, randomised study. BMC Pulm Med. 2014;14:178. doi:10.1186/1471-2466-14-178
8. Insulander P, Juhlin-Dannfelt A, Freyschuss U, Vallin H. Electrophysiologic effects of salbutamol, a beta2-selective agonist. J Cardiovasc Electrophysiol. 2004;15(3):316–322. doi:10.1046/j.1540-8167.2004.03105.x
9. Singh S, Loke YK, Enright P, Furberg CD. Pro-arrhythmic and pro-ischaemic effects of inhaled anticholinergic medications. Thorax. 2013;68(1):114–116. doi:10.1136/thoraxjnl-2011-201275
10. Matarese A, Sardu C, Shu J, Santulli G. Why is chronic obstructive pulmonary disease linked to atrial fibrillation? A systematic overview of the underlying mechanisms. Int J Cardiol. 2019;276:149–151. doi:10.1016/j.ijcard.2018.10.075
11. Buch P, Friberg J, Scharling H, Lange P, Prescott E. Reduced lung function and risk of atrial fibrillation in the Copenhagen City Heart Study. Eur Respir J. 2003;21(6):1012–1016. doi:10.1183/09031936.03.00051502
12. Chahal H, Heckbert SR, Barr RG, et al. Ability of reduced lung function to predict development of atrial fibrillation in persons aged 45 to 84 years (from the Multi-Ethnic Study of Atherosclerosis-Lung Study). Am J Cardiol. 2015;115(12):1700–1704. doi:10.1016/j.amjcard.2015.03.018
13. Grymonprez M, Vakaet V, Kavousi M, et al. Chronic obstructive pulmonary disease and the development of atrial fibrillation. Int J Cardiol. 2019;276:118–124. doi:10.1016/j.ijcard.2018.09.056
14. de Luise C, Lanes SF, Jacobsen J, Pedersen L, Sørensen HT. Cardiovascular and respiratory hospitalizations and mortality among users of tiotropium in Denmark. Eur J Epidemiol. 2007;22(4):267–272. doi:10.1007/s10654-007-9106-5
15. Jara M, Lanes SF, Wentworth CI, May C, Kesten S. Comparative safety of long-acting inhaled bronchodilators: a cohort study using the UK THIN primary care database. Drug Saf. 2007;30(12):1151–1160. doi:10.2165/00002018-200730120-00007
16. Jara M, Wentworth CI, Lanes S. A new user cohort study comparing the safety of long-acting inhaled bronchodilators in COPD. BMJ Open. 2012;2(3):e000841. doi:10.1136/bmjopen-2012-000841
17. Macie C, Wooldrage K, Manfreda J, Anthonisen N. Cardiovascular morbidity and the use of inhaled bronchodilators. Int J Chron Obstruct Pulmon Dis. 2008;3(1):163–169. doi:10.2147/copd.s1516
18. Ogale SS, Lee TA, Au DH, Boudreau DM, Sullivan SD. Cardiovascular events associated with ipratropium bromide in COPD. Chest. 2010;137(1):13–19. doi:10.1378/chest.08-2367
19. Verhamme KM, Afonso AS, van Noord C, et al. Tiotropium Handihaler and the risk of cardio- or cerebrovascular events and mortality in patients with COPD. Pulm Pharmacol Ther. 2012;25(1):19–26. doi:10.1016/j.pupt.2011.10.004
20. Singh S, Loke YK, Furberg CD. Inhaled anticholinergics and risk of major adverse cardiovascular events in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA. 2008;300(12):1439–1450. doi:10.1001/jama.300.12.1439
21. Gershon A, Croxford R, Calzavara A, et al. Cardiovascular safety of inhaled long-acting bronchodilators in individuals with chronic obstructive pulmonary disease. JAMA Intern Med. 2013;173(13):1175–1185. doi:10.1001/jamainternmed.2013.1016
22. Lee CH, Choi S, Jang EJ, et al. Inhaled bronchodilators and the risk of tachyarrhythmias. Int J Cardiol. 2015;190:133–139. doi:10.1016/j.ijcard.2015.04.129
23. Suissa S, Dell’Aniello S, Ernst P. Concurrent use of long-acting bronchodilators in COPD and the risk of adverse cardiovascular events. Eur Respir J. 2017;49(5):1602245. doi:10.1183/13993003.02245-2016
24. Rebordosa C, Aguado J, Plana E, et al. Use of Aclidinium did not increase the risk of death in a noninterventional cohort study in the Clinical Practice Research Datalink (CPRD. United Kingdom Respir Med. 2019;152:37–43. doi:10.1016/j.rmed.2019.04.018
25. Rebordosa C, Plana E, Rubino A, et al. A cohort study to evaluate the risk of hospitalisation for congestive heart failure associated with the use of Aclidinium and other chronic obstructive pulmonary disease medications in the UK Clinical Practice Research Datalink. Int J Chron Obstruct Pulmon Dis. 2021;16:1461–1475. doi:10.2147/COPD.S301624
26. Rebordosa C, Plana E, Rubino A, et al. Risk assessment of acute myocardial infarction and stroke associated with long-acting muscarinic antagonists, alone or in combination, versus long-acting beta2-agonists. Int J Chron Obstruct Pulmon Dis. 2022;17:1715–1733. doi:10.2147/COPD.S363997
27. Liou JT, Lin CW, Tsai CL, et al. Risk of severe cardiovascular events from add-on tiotropium in chronic obstructive pulmonary disease. Mayo Clin Proc. 2018;93(10):1462–1473. doi:10.1016/j.mayocp.2018.05.030
28. Wang MT, Liou JT, Lin CW, et al. Association of cardiovascular risk with inhaled long-acting bronchodilators in patients with chronic obstructive pulmonary disease: a nested case-control study. JAMA Int Med. 2018;178(2):229–238. doi:10.1001/jamainternmed.2017.7720
29. Goudis CA. Chronic obstructive pulmonary disease and atrial fibrillation: an unknown relationship. J Cardiol. 2017;69(5):699–705. doi:10.1016/j.jjcc.2016.12.013
30. Simons SO, Elliott A, Sastry M, et al. Chronic obstructive pulmonary disease and atrial fibrillation: an interdisciplinary perspective. Eur Heart J. 2021;42(5):532–540. doi:10.1093/eurheartj/ehaa822
31. Bourgon Labelle J, Farand P, Vincelette C, Dumont M, Le Blanc M, Rochefort CM. Validation of an algorithm based on administrative data to detect new onset of atrial fibrillation after cardiac surgery. BMC Med Res Methodol. 2020;20(1):75. doi:10.1186/s12874-020-00953-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Assessment of Acute Myocardial Infarction and Stroke Associated with Long-Acting Muscarinic Antagonists, Alone or in Combination, versus Long-Acting beta2-Agonists
Rebordosa C, Plana E, Rubino A, Aguado J, Martinez D, Lei A, Daoud S, Saigi-Morgui N, Perez-Gutthann S, Rivero-Ferrer E
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1715-1733
Published Date: 2 August 2022
Impact of COPD Exacerbations and Burden of Disease in Spain: AVOIDEX Study
Soler-Cataluña JJ, Izquierdo JL, Juárez Campo M, Sicras-Mainar A, Nuevo J
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1103-1114
Published Date: 8 June 2023