")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Impact of COPD Exacerbations and Burden of Disease in Spain: AVOIDEX Study
Authors Soler-Cataluña JJ , Izquierdo JL , Juárez Campo M, Sicras-Mainar A, Nuevo J
Received 26 January 2023
Accepted for publication 30 May 2023
Published 8 June 2023 Volume 2023:18 Pages 1103—1114
DOI https://doi.org/10.2147/COPD.S406007
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Juan José Soler-Cataluña,1– 3 José Luis Izquierdo,4,5 Mónica Juárez Campo,6 Antoni Sicras-Mainar,7 Javier Nuevo6
1Pneumology Department, Hospital Arnau de Vilanova-Lliria, Valencia, Spain; 2Medicine Department, Universitat de València, Valencia, Spain; 3CIBER de Enfermedades Respiratorias (CIBERES), Madrid, Spain; 4Medicine and Medical Specialties Department, Universidad de Alcalá, Alcalá de Henares, Madrid, Spain; 5Respiratory Medicine Department, Hospital Universitario de Guadalajara, Guadalajara, Spain; 6Medical Department, AstraZeneca MC, Madrid, Spain; 7Health Economics and Outcomes Research Department, Atrys Health SA, Barcelona, Spain
Correspondence: Juan José Soler-Cataluña, Pneumology Department, Hospital Arnau de Vilanova-Lliria, Carrer de Sant Clement, 12, València, 46015, Spain, Tel +34 961 97 60 00, Fax +34 963868580, Email [email protected]
Purpose: Chronic obstructive pulmonary disease (COPD) is characterized by high morbidity and mortality, with a considerable consumption of healthcare resources (HRU). This study aims to obtain real world evidence regarding the consequences of COPD exacerbations and to provide updated data on the burden of this disease and its treatment.
Patients and Methods: A retrospective study in seven Spanish regions was conducted among COPD patients diagnosed between 1/01/2010 and 31/12/2017. The index date was the diagnosis of COPD and patients were followed until lost to follow-up, death or end of the study, whichever occurred first. Patients were classified by patient pattern (incident or prevalent), type and severity of exacerbations, and treatments prescribed. Demographic and clinical characteristics were evaluated, together with the incidence of exacerbations, comorbidities, and the use of HRU, during the baseline (12 months before the index date) and the follow-up periods by incident/prevalent and treatment prescribed. Mortality rate was also measured.
Results: The study included 34,557 patients with a mean age of 70 years (standard deviation: 12). The most frequent comorbidities were diabetes, osteoporosis, and anxiety. Most patients received inhaled corticosteroids (ICS) with long-acting beta agonists (LABA), or long-acting muscarinic agonists (LAMA), followed by LABA with LAMA. Incident patients (N=8229; 23.8%) had fewer exacerbations than prevalent patients (N=26328; 76.2%), 0.3 vs 1.2 exacerbations per 100 patient-years. All treatment patterns present a substantial disease burden, which seems to increase with the evolution of the disease (ie moving from initial treatments to combination therapies). The overall mortality rate was 40.2 deaths/1000 patient-years. General practitioner visits and tests were the HRU most frequently required. The frequency and severity of exacerbations positively correlated with the use of HRU.
Conclusion: Despite receiving treatment, patients with COPD suffer a considerable burden mainly due to exacerbations and comorbidities, which require a substantial use of HRU.
Keywords: COPD, real-world evidence, clinical practice, triple therapy, ICS, LABA, LAMA
Introduction
Chronic obstructive pulmonary disease (COPD) causes airflow obstruction, which is not fully reversible.1 According to the World Health Organization (WHO), it is estimated that 3.3 million people died of COPD in 2008, which corresponds to 5.8% of deaths globally.2 The WHO predicts that COPD will become the third leading cause of death worldwide by 2030.2 In addition, COPD was reported to be the fourth leading cause of death in Spain in 2016.3
COPD symptoms include cough, sputum, and dyspnoea, and can vary in terms of frequency and severity.4 Patients with COPD also experience periods of acute worsening of respiratory symptoms, called exacerbations. These events are triggered by factors such as smoking, pollution, and respiratory viruses and bacteria, which can infect the lower airways and increase inflammation.5,6 Most patients with exacerbations can be managed in outpatient centres and receive pharmacological therapies, but others might require hospitalization, due to severe exacerbations.7
The pharmaceutical treatment of COPD is mainly based on long-term bronchodilator therapy.4,8 The cornerstone of COPD treatment is a combination of long-acting muscarinic antagonists (LAMA) and long-acting beta agonists (LABA), with or without inhaled corticosteroids (ICS), to decrease inflammation and exacerbation rates.9,10 Patients who have experienced moderate or severe exacerbations are more susceptible to recurrent exacerbations.11 If COPD patients experience moderate (2 or more) or severe exacerbations, triple therapy with LABA, LAMA and ICS is indicated.12
Although the progression of COPD is heterogeneous, exacerbations cause a significant decrease in lung function.13,14 In particular, severe exacerbations are associated with cardiovascular complications and high mortality rates, and they have a negative impact on patients’ quality of life.14–16 Therefore, the management of COPD exacerbations is linked to high healthcare resource utilization, which is a considerable burden on healthcare systems.17–20
In Spain, observational studies on the management of COPD exacerbations in clinical practice are scarce. Thus, the aim of this study was to address the evidence gap regarding to the impact of exacerbations, and to provide updated clinical data on the treatment patterns and the burden of this disease in Spain. In particular, the primary objective was to assess the pattern distribution and consequences (mortality and health use resources) of moderate to severe COPD exacerbations in two separate cohorts of patients with COPD (prevalent and incident patients). The secondary objectives were to describe the treatment patterns and to estimate the burden of COPD by treatment pattern, in both populations.
Materials and Methods
Data Source
AvoidEx was a retrospective, observational, multicenter, and longitudinal study carried out on secondary data unified in the dissociated and anonymized BIG-PAC® database, according to clinical practice in Spain. BIG-PAC® contains the integrated records of general practitioner (GP) visits (primary care), emergency care, pharmacy dispensation/prescription data (verified daily dose records, time intervals, and duration of each treatments administered), hospital admissions, working days lost and disability data, and deaths. BIG-PAC® is registered with the European Network of Centers for Pharmacoepidemiology and Pharmacovigilance which operates under the directive of the European Medicines Agency (EMA). Data were obtained from electronic medical records and other supplementary databases of financing/provision of public services to seven Spanish Autonomous Communities (1.9 million patients). BIG-PAC® has proven to be representative of the Spanish population.21,22
The study protocol was approved by the Institutional Research Board of the Hospital de Terrassa in Barcelona (Ethic committee code: 02-20-399-092) on 21 September 2020. Patient consent was not obtained as Spanish legislation excludes existing data that are aggregated for analysis. All personal data were removed as specified in Spanish Law 15/1999, of 13 December 1999, on Personal Data Protection.
Patient Population
Data for patients aged ≥40 years with a codified diagnosis of COPD between 1 January 2010 and 31 December 2017 were evaluated (Figure S1). The date of COPD diagnosis was considered the index date of the study population. A diagnosis of COPD was defined by using the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM),23 code J44 in primary or secondary care.
A minimum of 12-months of history prior to index date (baseline period) was required as well as a minimum 12-months of subsequent follow-up period. Patients were followed until lost to follow-up, death or the end of the study, whichever occurred first.
Patient Subgroups
Patients were classified as either incident (newly diagnosed) or prevalent (previously diagnosed) patients. Incident patients were those diagnosed with COPD for the first time between 1 January 2010 and 31 December 2017; prevalent patients were those who had been diagnosed before 1 January 2010.
To assess the consequences of exacerbations, subgroups of patients were defined by patient pattern, type and severity of exacerbations. According to the number and severity of patient exacerbations, the study population was grouped into 4 categories: A (0 exacerbations), B (1 moderate exacerbation), C (1 severe exacerbation), and D (≥2 moderate and/or ≥2 severe exacerbations). These classifications were based on exacerbations registered in prevalent patients during the baseline period (last 12 months before inclusion) and those reported in incident and prevalent patients during the follow-up period.
Patients were also divided into subgroups according to the treatment they had been prescribed for COPD during the baseline period. The study considered five treatments: 1) monotherapy with LAMA or LABA, 2) monotherapy with ICS, 3) combinations of LABA with LAMA, 4) combinations of ICS with LABA or ICS with LAMA and 5) combinations of ICS with LABA and LAMA (open triple therapy).
Variables Analyzed
Demographic and Clinical Characteristics
Demographic and clinical characteristics of patients were analyzed at the baseline. Demographic variables included age (continuous and by range), sex and body mass index (BMI). Clinical characteristics included forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) values and eosinophil levels, and comorbidities (pneumonia, asthma, osteoporosis, diabetes, ischemic heart disease, peripheral arterial disease, stroke, atrial fibrillation, dementia, heart failure, malignant neoplasms, depression and anxiety). The average number of comorbidities per patient was also estimated.
For exacerbations, this study considered moderate exacerbations as those that required the prescription of antibiotics and/or oral corticosteroids (OCS); severe exacerbations were defined as those that required hospital admission (ICD-10-CM code J44 as the primary diagnosis or J44.0/J44.1 as the secondary diagnosis) or an emergency room (ER) visit (ICD-10-CM code J44.0/J44.1 in outpatient hospital care). If more than one of these events occurred within a 2-week window, they were considered as one exacerbation. The number of patients and the incidence rate of exacerbations were both estimated during the follow-up period of the study.
Treatments
The consumption of medicines and other healthcare resources was estimated during the follow-up period. Medicines were identified according to the drug dispensation records and according to the Anatomical Therapeutic Chemical (ATC) Classification System (Table S1).24 The drugs considered in the study were those for obstructive airway diseases (code R03), glucocorticoids (code H02AB) and antibiotics (codes J01AA and J01CA).
Death
All-cause mortality was estimated during in the follow-up period in terms of the number of deaths and mortality rates per 1000 patient-years (p-y). These results were estimated in the overall prevalent and incident population and by exacerbation categories to assess the impact of exacerbations categories on mortality.
Healthcare Resources
Healthcare resource use associated with the management of COPD and those not related to COPD were identified during the first year after the index date. They included primary care visits (GP), ER visits, hospitalizations, specialized care visits, and complementary tests (laboratory tests, radiology tests, computerized tomography scans, magnetic resonance imaging, lung pulmonary function test, among others). Hospitalizations were reported as the percentage of total number of patients hospitalized, the length of hospitalization, and the number of inpatients per 100 p-y.
Data Management and Statistical Analysis
All patient records available during the study period were obtained, and their characteristics were described in relation to the index date (baseline and follow-up outcomes). The data were carefully reviewed through exploratory analysis and by observing the frequency distributions to identify possible coding or recording errors. All categorical variables were summarized with absolute and relative frequencies. Statistical analyses were descriptive and were conducted among the overall study population and subgroups (eg, according to patient pattern, type and severity of exacerbations and treatment prescribed).
Absolute and relative frequencies were obtained for qualitative data; the mean, standard deviation (SD), median, 25th and 75th percentiles of the distribution (interquartile range) are reported for quantitative variables. The 95% confidence intervals (CI) were based on the total number of subjects with non-missing values. The normality of the data distribution was verified with the Kolmogorov–Smirnov test.
Results
Baseline Characteristics of the Study Population
The study included 34,557 patients with a mean age of 70 years (SD: 12). Prevalent patients (n=26,328; 76.2%) were older than incident patients (n=8229; 23.8%) (73 [SD: 10] vs 57 years [SD: 9], respectively). The proportion of males was similar in both groups (incident patients: 70.5%; prevalent patients: 71.6%) (Table 1).
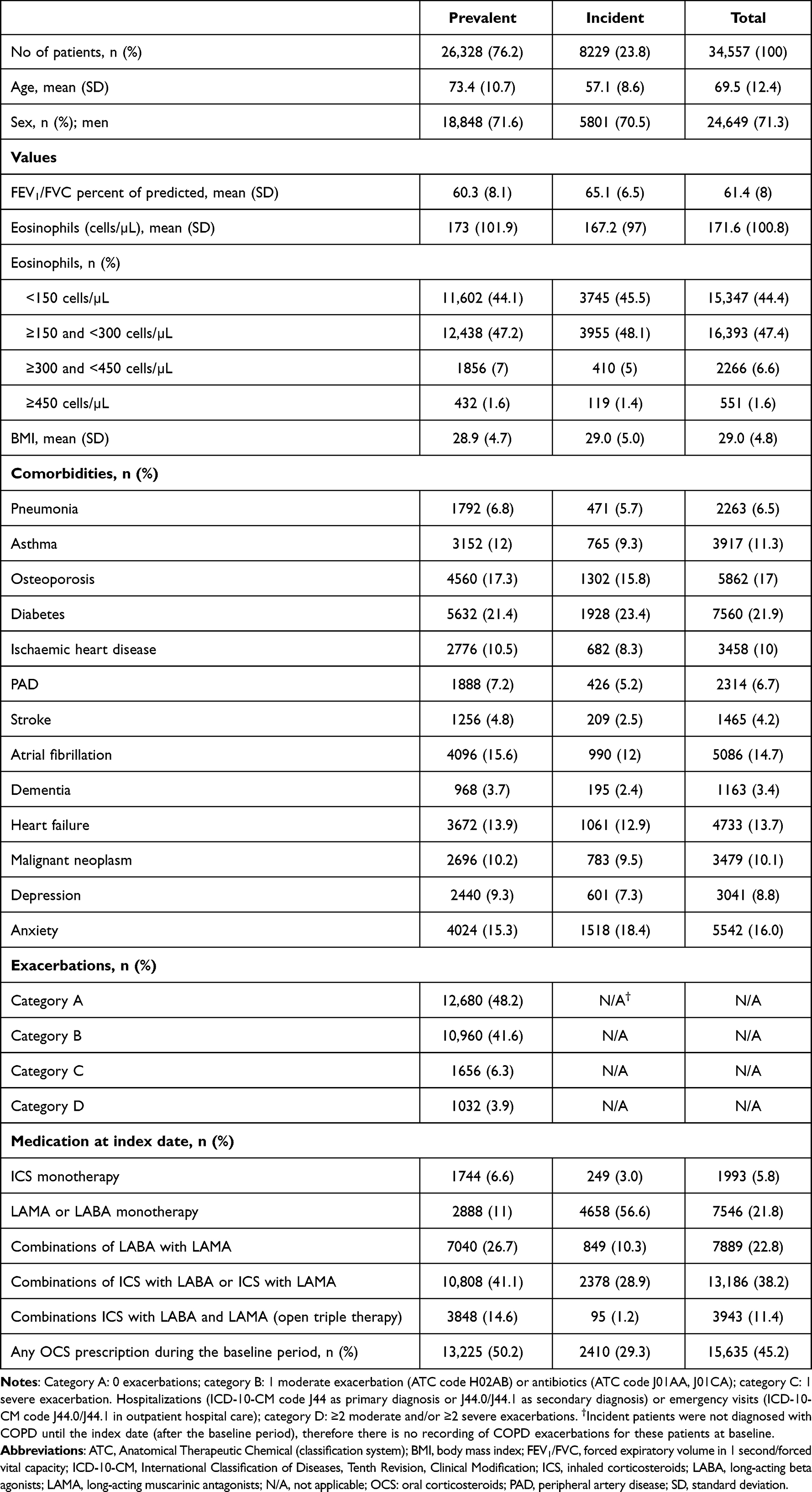 |
Table 1 Baseline Characteristics, Overall and by Prevalent and Incident Patients |
Mean FEV1/FVC ratio was 61.4 (SD: 8) overall and was higher in incident patients than prevalent patients (65.1 [SD: 6.5] vs 60.3 [SD: 8.1], respectively). Mean eosinophil concentration (cells/µL) was higher in prevalent patients compared with incident patients (173.0 [SD: 101.9] vs 167.2 [SD: 97.0], respectively). Most patients had eosinophil levels between ≥150 cells/µL and <300 cells/µL (47.4%), followed by those with levels <150 cells/µL (44.4%) (Table 1).
The comorbidities observed most frequently were diabetes (21.9%), osteoporosis (17.0%), anxiety (16%) and atrial fibrillation (14.7%). These percentages were similar in incident and prevalent patients. In the prevalent population, most patients with exacerbations belonged to categories A (48.2%) and B (41.6%) (Table 1). Different patterns of comorbidities were not observed across the exacerbation categories A to D (Table S2).
The most common COPD treatments in the study population were combinations of ICS with LABA or LAMA (38.2%), followed by combinations of LABA with LAMA (22.8%), and LABA or LAMA monotherapy (21.8%) (Table 2). Most of incident patients were treated with LABA or LAMA monotherapy (56.6%) and combinations of ICS with LABA or LAMA (28.9%), whereas prevalent patients mainly received combinations of ICS with LABA or LAMA (41.1%) or combinations of LABA with LAMA (26.7%) (Table 1 and Table S3). In addition, 45.2% of patients were prescribed at least one OCS during the baseline period (29.3% in the incident population; 50.2% in the prevalent population) (Table 1).
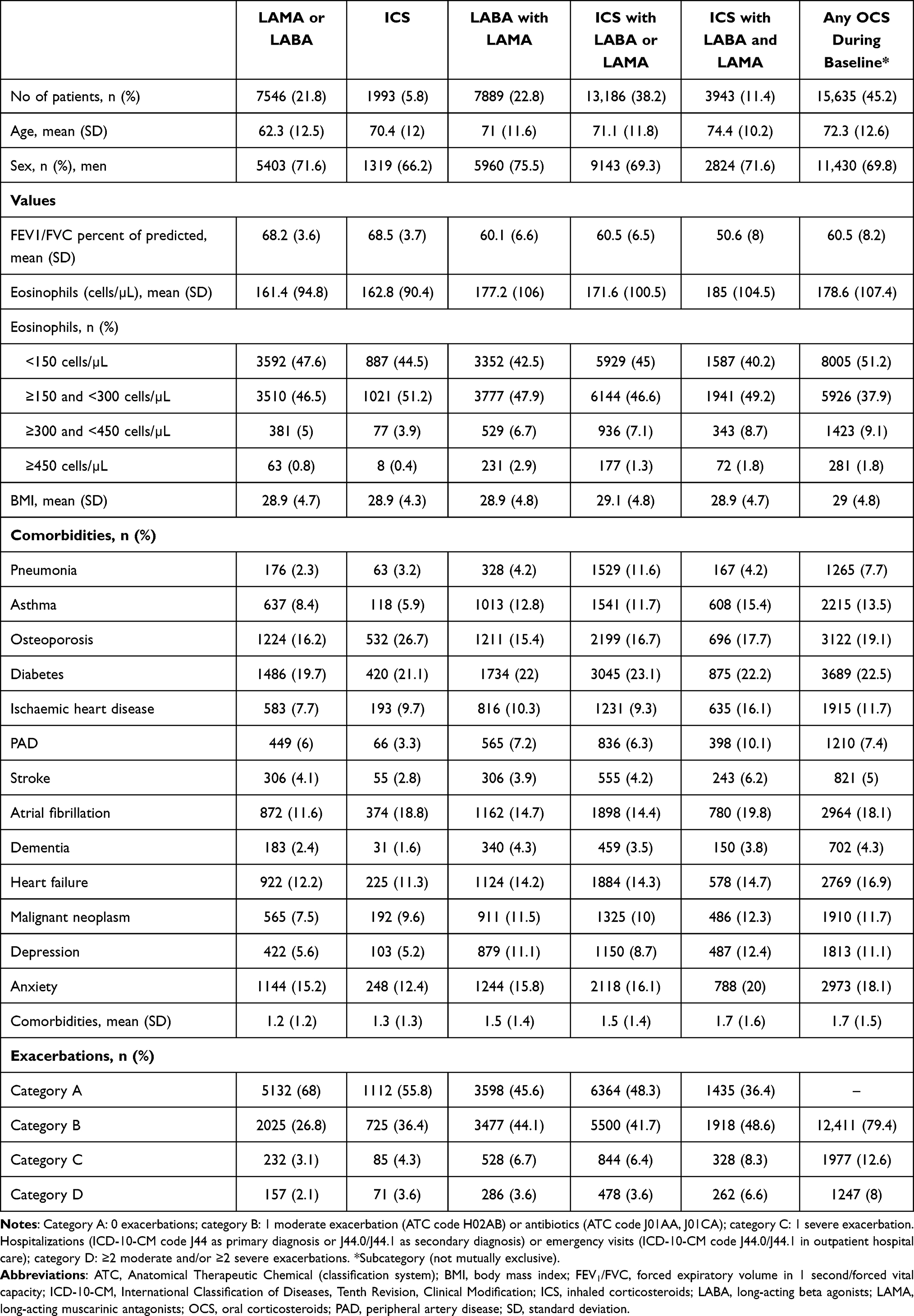 |
Table 2 Baseline Characteristics by Medication at Index Date |
Baseline characteristics of the study population by medication subgroup are reported in Table 2. Patients who received LABA or LAMA were younger than the other subgroups (particularly compared with those who had received ICS with LABA and LAMA, 62.3 years (SD: 12.5) vs 74.4 years (SD: 10.2), respectively). The FEV1/FVC ratio was higher in patients treated with LAMA or LABA and ICS (68.2 [SD: 3.6] vs 68.5 [SD: 3.7], respectively). Most patients who received any OCS during the baseline period had eosinophil levels <150 cells/µL (51.2%) and between ≥150 to 300 cells/µL levels (37.9%). Mean eosinophils concentration was lower for LABA or LAMA and ICS subgroups (161.4 cells/µL [SD: 94.8] vs 162.8 cells/µL [SD: 90.4], respectively). Exacerbations by treatment subgroup in the prevalent population are shown in Table S4.
Follow-Up Period
Exacerbations
As shown in Table 3, 13,648 prevalent patients (51.8%) suffered at least one exacerbation during the baseline period. The overall average was 1.3 exacerbations (SD: 0.3). Most of them belonged to category B (80.3%) and had one exacerbation (79.8%). Prevalent patients who suffered at least one exacerbation during the baseline period showed similar results during the follow-up period, as most of them were classified in category B (76.9%) and had one exacerbation (89.5%). The overall average number of exacerbations during the follow-up period in these patients was 1.2 (SD: 0.3) (Table 3).
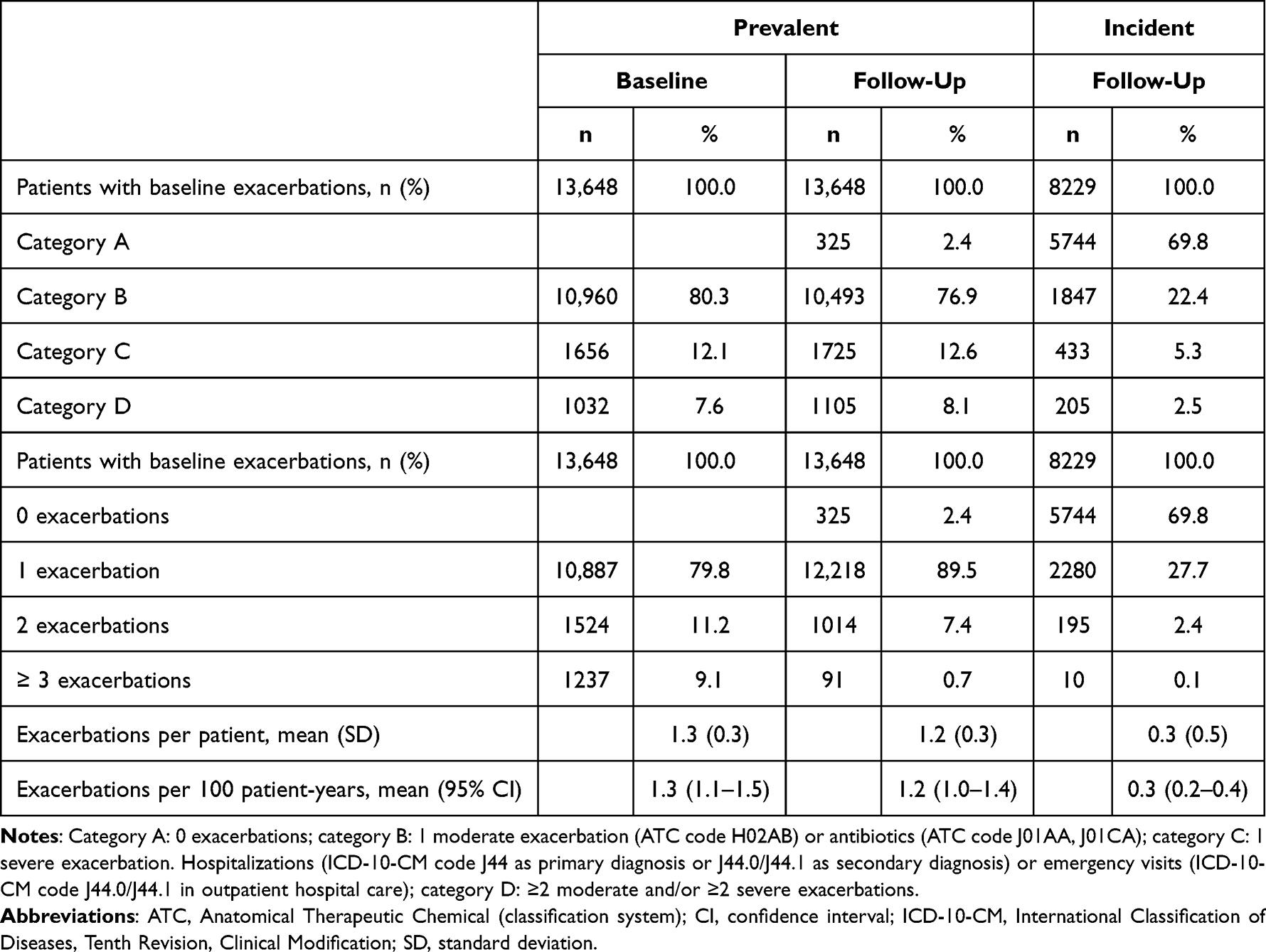 |
Table 3 Exacerbations in the Follow-Up Period, Prevalent and Incident Patients (Only in Patients with ≥1 Moderate to Severe Exacerbation During the Baseline Period) |
The incidence of exacerbations by treatment subgroup is reported in Table S5. The prevalence of exacerbations in patients on treatment with ICS with LABA and LAMA was 63.6% and in those on treatment with LABA with LAMA was 54.5%. Most of patients in all treatment subgroups had at least one exacerbation (from 80.2% to 90.8%).
Most incident patients did not have any exacerbations during the follow-up period (69.8% were in category A), but 27.7% experienced at least one exacerbation. An average of 0.3 exacerbations (SD: 0.5) was reported in this subgroup of patients (Table 3). When treatment groups were taken into account, it was estimated that patients on treatment with ICS with LABA and LAMA (open triple therapy) experienced the highest rate of exacerbations (0.5 exacerbations [SD: 0.6]), likely reflecting current disease status. Patients were included in categories C and D most frequently in the ICS with LABA and LAMA subgroup (11.6% and 5.3%, respectively) (Table S5).
Mortality
Mortality rates were estimated in incident and prevalent patients, according to their exacerbation category at the baseline. The overall mortality rate in incident patients was lower than in prevalent patients (27.1 deaths per 1000 p-y [95% CI: 18.4–39.8] vs 42.7 deaths per 1000 p-y [95% CI: 38.4–47.5] (Table S6).
Among the incident patients, those included in category D had the highest mortality rate (96.7 deaths per 1000 p-y [95% CI: 50.4–177.4]), followed by those in category C (82.3 deaths per 1000 p-y [95% CI: 44.8–146.4]) and category B (36.8 deaths per 1000 p-y [95% CI: 22.2–60.4]). Prevalent patients in category D presented the highest mortality rate (155,4 deaths per 1000 p-y [95% CI: 132.2–181.8]), followed by those in category C (144,7 deaths per 1000 p-y [95% CI: 126.2–165.5]), category B (43.3 deaths per 1000 p-y [95% CI: 36.8–51]), and category A (26.0 deaths per 1000 p-y [95% CI: 20.2–33.2]) (Table S6).
Healthcare Resources
Healthcare resource use was estimated in incident and prevalent patients, during the baseline and follow-up period, and considered the resources associated and not associated with management of COPD. In general, the healthcare resources most frequently required were GP visits and complementary tests. Prevalent patients were admitted to hospitals more frequently (baseline period: 14.5 [95% CI: 14.1–14.9] and follow-up period: 15.3 [95% CI: 14.9–15.7]) compared with incident patients (baseline period: 7.7 [95% CI: 7.1–8.3] and follow-up period: 7.9 [95% CI: 7.3–8.5]) (Table 4). Healthcare resource use was also estimated in incident and prevalent patients by treatment type. Patients on treatment with ICS with LABA and LAMA reported higher healthcare resources use (Tables S7–S9), again likely reflecting current disease status. In addition, prevalent patients in category D required more healthcare resources compared to the other groups (Table S10).
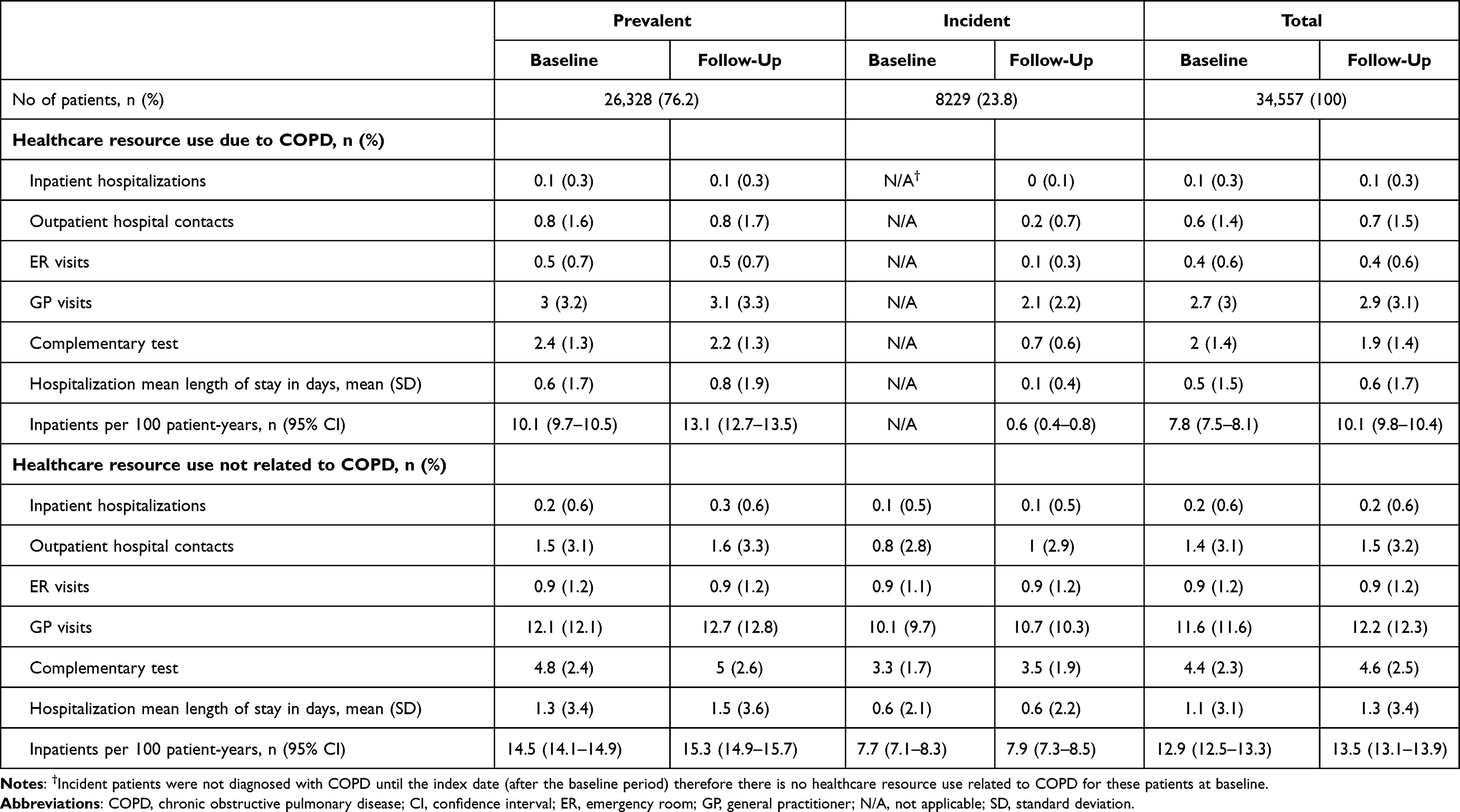 |
Table 4 Healthcare Resource Use |
Discussion
This large and representative cohort of patients with COPD in Spain shows that the burden of COPD exacerbation is different between newly diagnosed patients (incident population) and prevalent (previously diagnosed) patients. It is possible that this difference directly relates to the progressive nature of the disease and the impact of having clinical deterioration (ie, an exacerbation). Half of the prevalent population showed one or more exacerbations during the baseline period, but incident patients barely presented with exacerbations and 70% did not have an exacerbation in the follow-up period. In terms of the consequences of exacerbations, it should be noted that the overall annual mortality rate was 40.2 deaths per 1000 p-y (Table S6), with the highest mortality rate in category D (≥2 moderate and/or ≥2 severe exacerbations). The rate of hospitalization was double for prevalent versus incident patients. The main treatments prescribed for COPD in the study population were ICS with LABA or LAMA followed by LABA with LAMA. All treatment patterns had substantial disease burden, which appeared to increase with the evolution of the disease (ie, transitioning from initial treatments to combination therapies). Different patterns of comorbidities were not observed across the exacerbation categories considered.
Incident patients had fewer exacerbations compared with prevalent patients (1.3 vs 0.3). This is probably associated with the fact that incident patients were younger and had a less advanced disease, with less lung function impairment and lower eosinophil counts than prevalent patients, although incident patients had a similar number of comorbidities. These results are in agreement with previous research, which concluded that exacerbations became more frequent and more severe as COPD progressed.11 In addition, average eosinophil counts in prevalent patients (173 cells/µL) was similar to that reported in the EPISCAN-II study. This multicenter and population-based epidemiological study, carried out in Spain, estimated that prevalent patients with COPD had an average of 192 cells/µL.25 Thus, our results may be representative of the Spanish population.
Our results also showed that the mortality rate increased in patients with more and severe exacerbations. Most patients in category C and D were hospitalized during the follow-up period due to their exacerbations, and their mortality rates were in line with the mortality rates reported by Soler-Cataluña et. al26 (11.6% after 12 months in patients admitted to hospital, equivalent to 116 deaths per 1000 patients per year). In addition, a more recent study carried out by Izquierdo et al27 estimated the in-hospital mortality in patients with COPD of 5.6% between 2011 and 2018. Differences in the estimations of the mortality rates should be noted, as they analyzed the in-hospital mortality, whereas we estimated the mortality rate in a wide cohort of patients after a 12-month follow-up. Moreover, we estimated as deaths in 1000 patients-year, thus considering the contribution in years of each patient to the study period until the event of death. It should also be noted that AUDIPOC reported a mortality rate of 11.3% after 90 days of hospital discharge in patients with COPD in Spain.28 Our results also showed that the mortality rate was lower in incident patients than in prevalent ones, a finding that may be due to the differences in age and the health status.
A recent study carried out by Izquierdo et al,27 evaluated the treatment of patients with COPD in Spain using the electronic medical records from 59,369 patients attended in Castilla-La Mancha in a real-world setting, between 2011 and 2018. The study reported a reduction in the use of monotherapy with LABA and LAMA, and an increase in the use of two bronchodilators, occasionally combined with an ICS.27 Our results provide more information about the clinical characteristics of COPD patients, according to their treatment, and the incidence and severity of their exacerbations.
Although our results showed the predominant use of ICS with LABA or LAMA, followed by LABA with LAMA, compared with open triple therapy (ICS with LABA and LAMA), the latter has demonstrated significant clinical benefits in terms of exacerbations, lung function, survival, and health status compared with monotherapy of LABA or LAMA or dual therapy (LABA with LAMA).29,30 These clinical improvements are associated with reductions in healthcare resource use and costs.31–33
Limitations of the study included the categorization of the disease, the possible bias in patient classification and the selection of the therapeutic groups, which were attributable to the information system used. The study had the inherent limitations of retrospective studies, such as underreporting of the disease and possible differences in the health professionals and patients due to its observational design. In this regard, the potential for inaccuracies in diagnostic coding and registration of deaths and other comorbidities, or the lack of any variables that could influence the results (ie, socioeconomic level, exposure to work, smoking status, etc.) may be considered limitations. It should be noted that the only clinical criteria for study inclusion was having a medical record with the ICD-10-CM code J44. Therefore, this methodology may underestimate or overestimate the number of patients considered in the study. In addition, spirometry measures other than FEV1/FVC values were not taken into consideration. However, it is considered that any possible confounding variables would affect the study variables equally. Additional limitations of this study are that we used COPD patients’ hospital admissions and ER visits as a proxy for exacerbation severity. Moreover, the risk of a potential survival bias between prevalent and incident COPD patients cannot be ruled out. Finally, a potential switch of patients from one treatment group to another between the baseline period and the follow-up period was not considered and therefore the pharmacological treatment recorded at the index date might not be an accurate definition of the treatment during the follow-up period. By contrast, the study has the strength of using the BIG-PAC® database, which gathers data on clinical practice from 7 autonomous communities and has been shown to be representative of the Spanish population.21,22
Conclusions
Patients with COPD have a substantial burden of disease, particularly the subpopulation of prevalent patients, which resulted in a substantial use of healthcare resources. Despite receiving treatment, more than half of patients had at least one moderate or severe exacerbation per year during the follow-up period. Throughout the data-collection period (2010–2017), the use of triple therapy (ICS with LABA and LAMA) remained very low. This suggests that it is necessary to consider and increase the use of new available therapeutic approaches that could help reduce the burden of disease and the associated use of health resources observed in this study. A key aspect of our study is that the data were collected in a real-life setting and is based on the electronic medical records of patients with COPD from a Spanish database, allowing us to follow-up patients in routine clinical practice. Therefore, the results presented here might be a valuable source of information for pulmonologists and GPs and healthcare authorities involved in the management of patients with COPD exacerbations.
Acknowledgments
The authors thank Inés Pérez Román for her collaboration in writing the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by AstraZeneca MC, Spain.
Disclosure
JN and MJC are fulltime employees of AstraZeneca. ASM is a fulltime employee of Atrys Health. JJSC declares personal fees from AstraZeneca during the conduct of the study; personal fees and grants from GlaxoSmithKline and personal fees and non-financial support from AstraZeneca, Boehringer-Ingelheim, Bial, Chiesi, Menarini, and Novartis. JLI reports personal fees from AstraZeneca, Bayer, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Grifols, Menarini, Novartis, Orion, Pfizer, Sandoz, Teva, and Zambon during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. World Health Organization (WHO). Chronic respiratory diseases; 2021. Available from: https://www.who.int/westernpacific/health-topics/chronic-respiratory-diseases.
2. European Respiratory Society. The burden of lung disease; 2013. Available from: https://www.erswhitebook.org/chapters/the-burden-of-lung-disease/.
3. Soriano JB, Kendrick PJ, Paulson KR, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596.
4. Global Initiative for Chronic Obstuctuve Lung DIsease (GOLD). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease; 2022. Available from: https://goldcopd.org/wp-content/uploads/2021/12/GOLD-REPORT-2022-v1.1-22Nov2021_WMV.pdf.
5. Ritchie AI, Wedzicha JA. Definition, causes, pathogenesis, and consequences of chronic obstructive pulmonary disease exacerbations. Clin Chest Med. 2020;41(3):421–438. doi:10.1016/j.ccm.2020.06.007
6. Viniol C, Vogelmeier CF. Exacerbations of COPD. Eur Respir Rev. 2018;27:147. doi:10.1183/16000617.0103-2017
7. Vogelmeier CF, Román-Rodríguez M, Singh D, Han MK, Rodríguez-Roisin R, Ferguson GT. Goals of COPD treatment: focus on symptoms and exacerbations. Respir Med. 2020;166:105938. doi:10.1016/j.rmed.2020.105938
8. Bollmeier SG, Hartmann AP. Management of chronic obstructive pulmonary disease: a review focusing on exacerbations. Am J Health Syst Pharm. 2020;77(4):259–268. doi:10.1093/ajhp/zxz306
9. Burge PS, Calverley PM, Jones PW, Spencer S, Anderson JA, Maslen TK. Randomised, double blind, placebo controlled study of fluticasone propionate in patients with moderate to severe chronic obstructive pulmonary disease: the ISOLDE trial. BMJ. 2000;320(7245):1297–1303. doi:10.1136/bmj.320.7245.1297
10. Calverley PMA, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356(8):775–789. doi:10.1056/NEJMoa063070
11. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
12. National Institute for Health and Care Excellence (NICE). Chronic obstructive pulmonary disease in over 16s: diagnosis and management; 2019. Available from: https://www.nice.org.uk/guidance/ng115.
13. Casanova C, de Torres JP, Aguirre-Jaíme A, et al. The progression of chronic obstructive pulmonary disease is heterogeneous: the experience of the BODE cohort. Am J Respir Crit Care Med. 2011;184(9):1015–1021. doi:10.1164/rccm.201105-0831OC
14. Halpin DM, Miravitlles M, Metzdorf N, Celli B. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis. 2017;12:2891–2908. doi:10.2147/COPD.S139470
15. Hurst JR, Skolnik N, Hansen GJ, et al. Understanding the impact of chronic obstructive pulmonary disease exacerbations on patient health and quality of life. Eur J Intern Med. 2020;73:1–6. doi:10.1016/j.ejim.2019.12.014
16. Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(5 Pt 1):1418–1422. doi:10.1164/ajrccm.157.5.9709032
17. Rehman AU, Ahmad Hassali MA, Muhammad SA, et al. The economic burden of chronic obstructive pulmonary disease (COPD) in the USA, Europe, and Asia: results from a systematic review of the literature. Expert Rev Pharmacoecon Outcomes Res. 2020;20(6):661–672. doi:10.1080/14737167.2020.1678385
18. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic burden of chronic obstructive pulmonary disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–460. doi:10.2147/COPD.S234942
19. Pasquale MK, Sun SX, Song F, Hartnett HJ, Stemkowski SA. Impact of exacerbations on health care cost and resource utilization in chronic obstructive pulmonary disease patients with chronic bronchitis from a predominantly Medicare population. Int J Chron Obstruct Pulmon Dis. 2012;7:757–764. doi:10.2147/COPD.S36997
20. Price LC, Lowe D, Hosker HSR, et al. UK National COPD Audit 2003: impact of hospital resources and organisation of care on patient outcome following admission for acute COPD exacerbation. Thorax. 2006;61(10):837–842. doi:10.1136/thx.2005.049940
21. Sicras-Mainar A, Enriquez JL, Hernández I, Sicras-Navarro A, Aymerich T, Leon M. PMU146 Validation and representativeness of the Spanish BIG-PAC database: integrated computerized medical records for research into epidemiology, medicines and health resource use (real world evidence). Value Health. 2019;22:S734. doi:10.1016/j.jval.2019.09.1764
22. Sicras-Mainar A, Sicras-Navarro A, Palacios B, Varela L, Delgado JF. Epidemiología y tratamiento de la insuficiencia cardiaca en España: estudio PATHWAYS-HF. Rev Esp Cardiol. 2020;149(6):240–247. doi:10.1016/j.recesp.2020.09.014
23. Ministerio de S, Consumo y bienestar social. international classification of diseases (9th edition) clinical modification (ICD-09-CM); 2021. Available from: https://eciemaps.mscbs.gob.es/ecieMaps/browser/index_9_mc.html.
24. World Health Organization (WHO). The anatomical therapeutic chemical classification system with defined daily doses (ATC/DDD). Available from: https://www.who.int/standards/classifications/other-classifications/the-anatomical-therapeutic-chemical-classification-system-with-defined-daily-doses.
25. Miravitlles M, Soler-Cataluña JJ, Soriano JB, et al. Determinants of blood eosinophil levels in the general population and patients with COPD: a population-based, epidemiological study. Respir Res. 2022;23(1):49. doi:10.1186/s12931-022-01965-3
26. Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
27. Izquierdo JL, Morena D, González Y, et al. Clinical management of COPD in a real-world setting. a big data analysis. Arch Bronconeumol. 2021;57(2):94–100. doi:10.1016/j.arbr.2019.12.023
28. Pozo-Rodríguez F, López-Campos JL, Alvarez-Martínez CJ, et al. Clinical Audit of COPD Patients Requiring Hospital Admissions in Spain: AUDIPOC Study. PLos One. 2012;7(7):e42156. doi:10.1371/journal.pone.0042156
29. Cazzola M, Rogliani P, Calzetta L, Matera MG. Triple therapy versus single and dual long-acting bronchodilator therapy in COPD: a systematic review and meta-analysis. Eur Respir J. 2018;52(6):1801586. doi:10.1183/13993003.01586-2018
30. Vanfleteren L, Fabbri LM, Papi A, Petruzzelli S, Celli B. Triple therapy (ICS/LABA/LAMA) in COPD: time for a reappraisal. Int J Chron Obstruct Pulmon Dis. 2018;13:3971–3981. doi:10.2147/COPD.S185975
31. Fenwick E, Martin A, Schroeder M, et al. Cost-effectiveness analysis of a single-inhaler triple therapy for COPD in the UK. ERJ Open Res. 2021;7:1. doi:10.1183/23120541.00480-2020
32. Buendía JA, Patiño DG. Cost-utility of triple versus dual inhaler therapy in moderate to severe asthma. BMC Pulm Med. 2021;21(1):398. doi:10.1186/s12890-021-01777-z
33. Paly V, Vallejo-Aparicio LA, Gabrio A, Baio G, Martin A, Ismaila A. IMPACT: healthcare resource use data and associated costs for single-inhaler triple therapy versus dual therapies in Spain. Eur Respir J. 2021;58(suppl):65. doi:10.1183/13993003.congress-2021.OA4283
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.