Back to Journals » International Journal of General Medicine » Volume 15
Establishment of Reference Intervals for Serum Protein Electrophoresis of Apparently Healthy Adults in Addis Ababa, Ethiopia
Authors Bikila D ![]() , Lejisa T, Tolcha Y
, Lejisa T, Tolcha Y ![]() , Bashea C
, Bashea C ![]() , Meles M, Getahun T
, Meles M, Getahun T ![]() , Ashebir G, Habtu W, Challa F
, Ashebir G, Habtu W, Challa F ![]() , Mohammed O
, Mohammed O ![]() , Kassaw M
, Kassaw M ![]() , Kebede A, G/Egzeabher L, Befekadu E, Wolde M, Tsegaye A
, Kebede A, G/Egzeabher L, Befekadu E, Wolde M, Tsegaye A ![]()
Received 7 June 2022
Accepted for publication 4 August 2022
Published 23 August 2022 Volume 2022:15 Pages 6701—6711
DOI https://doi.org/10.2147/IJGM.S376450
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Demiraw Bikila,1 Tadesse Lejisa,1 Yosef Tolcha,1 Chala Bashea,1 Mehari Meles,1 Tigist Getahun,1 Genet Ashebir,1 Wossene Habtu,1 Feyissa Challa,1 Ousman Mohammed,2 Melkitu Kassaw,3 Adisu Kebede,4 Letebrhan G/Egzeabher,5 Endalkachew Befekadu,6 Mistire Wolde,7 Aster Tsegaye7
1Department of National Clinical Chemistry Reference Laboratory, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 2Department of Medical Laboratory Sciences, Wollo University, Dessie, Ethiopia; 3Food Science and Nutrition Research Directorate, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 4National Capacity Building Directorate, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 5Department of Medical Laboratory, Yekatit 12 General Hospital, Addis Ababa, Ethiopia; 6Department of Medical Laboratory, Saint Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia; 7Department of Medical Laboratory Sciences, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Demiraw Bikila, Department of National Clinical Chemistry Reference Laboratory, Ethiopian Public Health Institute, Addis Ababa, Ethiopia, Email [email protected]
Background: Even though several factors affect reference intervals (RIs), company-derived values are currently in use in many laboratories worldwide. However, few or no data are available regarding serum proteins RIs, especially in resource-limited countries such as Ethiopia.
Objective: To establish RIs for serum protein electrophoresis of apparently healthy adults in Addis Ababa, Ethiopia.
Methods: A cross-sectional study was conducted on a total of 297 apparently healthy adults from April to October 2019 in four selected sub-cities (Akaki, Kirkos, Arada, and Yeka) of Addis Ababa, Ethiopia. Laboratory analysis of collected samples was performed using the Capillarys 2 Flex Piercing analyzer, while statistical analysis was conducted using SPSS version 23 and Med-Calc software. The Mann–Whitney test was used to check partitions. A non-parametric method of reference range establishment was performed as per CLSI guideline EP28A3C.
Results: The established RIs were: albumin 53.83– 64.59%, 52.24– 63.55%; alpha-1 globulin 3.04– 5.40%, 3.44– 5.60%; alpha-2 globulin 8.0– 12.67%, 8.44– 12.87%; and beta-1 globulin 5.01– 7.38%, 5.14– 7.86%. Moreover, the albumin to globulin ratios were 1.16– 1.8 and 1.09– 1.74 for males and females, respectively. The combined RIs for beta-2 globulin and gamma globulin were 2.54– 4.90% and 12.40– 21.66%, respectively.
Conclusion: The established reference interval for serum protein fractions revealed gender-specific differences, except for beta-2 globulin and gamma globulin.
Keywords: serum protein electrophoresis, reference interval, Addis Ababa, Ethiopia
Introduction
Serum protein electrophoresis is a laboratory technique routinely employed for the identification of patients with multiple myeloma and other disorders of serum protein fractions. Protein electrophoresis (separation of serum protein fractions) is a technique used in clinical laboratory for screening samples for protein abnormalities. The Capillarys 2 Flex Piercing (Sebia; Lisses, Evry Cedex, France) has been developed to provide complete automation of this testing procedure, with fast separation and good resolution,1–6 and is currently used at the National Clinical Chemistry Reference Laboratory of the Ethiopian Public Health Institute (EPHI).
In many African countries, the clinical laboratory reference intervals (RIs) have not been established, and western country-based RIs are usually used in many diagnostic laboratories and clinical trials to screen, diagnose, and monitor different disease states.7 In poor countries such as Ethiopia, almost all available clinical laboratories rely on RIs obtained either from textbooks or from the package kit inserts provided by the manufacturers.
The considerable differences in the established RIs in several countries and population groups may increase the chance of unnecessary additional investigations, failure to detect the specified abnormalities related to underlying disease states, or mismanagement of patients.8
Although laboratory tests represent 5% of a health system’s costs, they indirectly affect the remaining 95% of health expenditure. Laboratory findings have a crucial role in diagnosis, monitoring, and screening of different pathologies by influencing up to 70% (on average around 60–80%) of clinical decisions. Hence, the interpretation of laboratory results must rely on a background of well-established RIs that discriminate between “health” and “disease”.9
As per the recommendation of the guidelines developed by the Clinical and Laboratory Standards Institute (CLSI),10 every country must establish RIs for its own population to aid in the accurate diagnosis and interpretation of laboratory test results.
To the best of the investigators’ knowledge, no research has been conducted on the establishment of RIs for serum protein electrophoresis of apparently healthy adults in Addis Ababa, Ethiopia. Therefore, the findings of the present study are of great importance, since they can assist in the correct interpretation of serum protein fractions for the diagnosis, treatment, and management of associated abnormalities. This study will also be useful for patients, clinicians, communities, other researchers, and policymakers at large, for prevention, diagnosis, interpretation of results, early control, and management of abnormalities associated with serum protein fractions, such as multiple myeloma, in Ethiopia in general and in the study area in particular. Since no other study has been conducted in the study area, the findings of the present study will serve as baseline information and reference for future studies.
Materials and Methods
Study Area
The study was conducted in four selected sub-cities (Akaki, Kirkos, Arada, and Yeka) of Addis Ababa, Ethiopia. Addis Ababa is the capital city of Ethiopia, established in 1887, and serves as the headquarters for several international organizations, such as the African Union (AU) and the United Nations Economic Commissions for Africa (UNECA). The city is located between 8°55’ and 9°05’ N latitude and between 38°40’ and 38°50’ E longitude. The capital city’s average elevation is 2500 m above sea level, and hence it has a fairly favorable climate and moderate weather conditions. It is the largest city in the country by population, with a total population of more than 3 million. The area of the capital city is about 527 km2. There is an estimated population density of about 5000 per available km2. According to the 2007 census, the city of Addis Ababa has a higher population of female residents than male residents. Almost one-quarter of all people in Ethiopia who live in urban areas live in the capital city.11,12
Study Design and Period
A cross-sectional study design was conducted to establish reference intervals for serum protein electrophoresis of apparently healthy adults from April to October 2019 in Addis Ababa, Ethiopia.
Population
Source Population
All adult individuals who lived in Addis Ababa, Ethiopia, were the source population.
Study Population
Adult individuals who lived in four selected sub-cities (Akaki, Kirkos, Arada, and Yeka) of Addis Ababa, Ethiopia, and were willing to give blood samples as per the eligibility criteria, were the study population.
Inclusion and Exclusion Criteria
This study is part of the national reference interval study; thus, both the inclusion and exclusion criteria followed the national reference study protocol. Accordingly, the following eligibility criteria were applied in participant selection.
Inclusion Criteria
Apparently healthy individuals aged 18 years and above, who were willing to participate in the study and had lived in the study area for at least 5 years.
Exclusion Criteria
Samples showing hemolysis, icterus, or lipemia, or which displayed an abnormality, were excluded. Outlier exclusion was as described in CLSI Guideline EP28A3C.10
Study Variables
Dependent Variables
The dependent variables were RIs for serum protein fractions (albumin, alpha globulin, beta globulin, gamma globulin, and albumin to globulin ratio).
Independent Variables
Independent variables were age and sex.
Participant Selection, Sample Size Calculation and Sampling Method
Participant Selection and Sample Size Calculation
As per CLSI Guideline EP28A3C recommendation, the best way to establish an RI is to collect samples from a sufficient number of reference individuals to yield a minimum of 120 samples for analysis, by non-parametric means for each partition (eg, sex, age range) with a power of 90%. One of the IFCC’s primary recommendations, the posteriori sampling approach, was employed as a direct means to determine RI. Thus, to obtain a minimum recommended sample size (120 men and 120 women) for two partitions, a total of 297 samples were obtained by considering a 20% rejection rate13 from already collected samples.
Sampling Method
As this study is part of the national RI study, two types of sampling technique were employed to obtain the required sample size. First, for the establishment of RIs of clinical chemistry parameters and other hematological parameters, a total of 1030 participants were recruited using the probability proportional to size (PPS) sampling method, where the size depends on the number of households of woredas (former kebeles) in a city/town. Accordingly, all the woredas in the town were considered/selected to be the participants of the study. Since Addis Ababa is very large city, four sub-cities were selected based on PPS, namely Arada, Kirkos, Akaki, and Yeka sub-cities; thus, all woredas under the selected sub-cities was included. To recruit 1030 participants, the number of households was determined by dividing the total household in the selected towns (sub-cities for Addis Ababa) by the estimated number of individuals per household, which is four for urban households. Individuals in every Kth household were approached at their house by well-trained sample collectors. Given the average number of individuals in each household of four, the next households were used to recruit the remaining age groups that were not found in the selected household. Once volunteering participants fulfilling the eligibility criteria had been identified by the sample collectors, they were invited to go to nearby health facilities to facilitate biological sample collection. Finally, for the current study, a convenience sampling technique was employed to obtain the required sample size of 288.
Measurement and Data Collection
Data Collection Procedure
The required data for the current study were collected using a data collection format, which contains code, age, sex, residence, and laboratory results of the six serum protein fractions plus the albumin to globulin ratio (see Annex I in supplementary material). The original data were collected by health extension workers mobilizing eligible individuals from the community to a nearby health facility. Serum samples were stored at the EPHI until analysis.
Laboratory Analysis
The collected serum samples were analyzed using the Capillarys 2 Flex Piercing analyzer (Sebia, France) at the EPHI clinical chemistry reference laboratory. The analyzer has been approved by the Food and Drug Administration (FDA) for clinical use.14 The separation of proteins occurs in free solution in a narrow fused silica capillary that is exposed to a high voltage at a pH of 10 buffers, at which serum protein fractions exhibit negative charge. After application of the voltage, the two forces acting in opposite directions on the serum proteins are the force of the electric field and electro-osmotic force (EOF). At pH 10, the internal surface of the fused silica capillaries is negatively charged owing to ionization of the silanol groups.
Cations in the electrolyte near the capillary wall migrate toward the negative electrode (cathode), pulling electrolyte solution with them, which constitutes the EOF, which surpasses the force of the electric field and carries all the serum proteins toward the cathode. Albumin is more acidic than gamma globulins, which makes albumin resist the EOF, resulting in a delay of albumin reaching the cathode. There is direct qualitative and quantitative determination of serum protein fractions at 200 nm. For details of the principle and procedure of the test, refer to Annex II (Supplementary material).15
Data Quality Assurance
Data Collection Tool
Data regarding the demographic characteristics of the study participants were collected using a data collection format (see Annex I) from previously gathered data of the national reference interval study.
Pre-Analytical Quality Assurance
The quality of blood samples was ensured during collection and processing by following standard operating procedures (SOPs). In this study, serum samples stored at the EPHI were used. Samples with incomplete information, and turbid or hemolyzed samples, were rejected.
Analytical Quality Assurance
Analytical quality assurance was conducted in the EPHI National Clinical Chemistry Reference Laboratory, which is accredited by the Ethiopian National Accreditation Office (ENAO) to perform tests in accordance with the requirement of ISO 15189:2012, Medical laboratory requirements for quality and competence [Accreditation No. M0025]. Well-trained and experienced laboratory professionals performed the analysis, and SOPs were strictly followed for each of the measured parameters.
The performance of the fully automated clinical chemistry analyzers (Capillarys 2 Flex Piercing) was checked by running quality control samples, and the results were evaluated using control data provided by the manufacturer.
Post-Analytical Quality Assurance
The results were printed out after checking the appropriateness of all the test results, and the data were carefully entered into a Microsoft Excel worksheet and saved for statistical analysis.
Data Analysis and Interpretation
The data were entered into Microsoft Excel, then exported to SPSS version 23 and Med-Calc software for analysis. Before data analysis was performed, all continuous variables were visually assessed, using histograms, to determine whether they were normally distributed or not. Data were also explored and tested by the Kolmogorov–Smirnov and Shapiro–Wilk tests of normality and the Mann–Whitney test to check partitions. When p≥0.05, the data were considered to be normally distributed. A non-parametric method of reference range establishment was performed as per CLSI guideline EP28A3C.10 Using the non-parametric method, the lower and upper limits, including 95% distribution with 90% confidence intervals, were calculated. The results were expressed as percentages and absolute concentration, and presented in tables.
Operational Definitions
The definitions were as per the CLSI Guideline EP28A3C.10
- Reference interval: the interval between, and including, two reference limits; it is designated as the interval of values from the lower reference limit to the upper reference limit (EP28A3C).10
- Establishing (or determining) a reference interval: the process used in creating an RI de novo, encompassing all of the steps from the selection of reference individuals, through exact details of the analytical methods, and concluding with data collection and analysis (EP28A3C).10
- Reference individual: a person selected for testing on the basis of well-defined criteria (EP28A3C).10
- Reference limit: a value derived from the reference distribution and used for descriptive purposes; the descriptive of the reference values, which may be distinguished from various other types of decision limits (EP28A3C).10
- Reference distribution: the distribution of reference values (EP28A3C).10
- Serum protein fractions: albumin, alpha globulin, beta globulin, and gamma globulin.
- Electrophoresis: separation technique (migration of charged particles in an electrical field).16
- Adult: in this study, refers to individuals aged 18–65 years.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki. Ethical clearance and permission were obtained from the Department of Medical Laboratory Science Research and Ethical Review Committee (DRERC), College of Health Science, Addis Ababa University (protocol ID DRERC/477/19/MLS). Permission was also obtained from Addis Ababa Health Bureau and was sought from the respective health institutions before the start of the data collection process.
The study participants were informed about the purpose of the study and the importance of their participation in the study by providing blood samples that may help in the establishment of reference intervals for serum protein electrophoresis of apparently healthy adults in Addis Ababa, Ethiopia.
The study participants were also informed that they could stop participating at any time if they wanted to do so. Then, after assuring the confidentiality of the information obtained and completion of the informed consent from the study participants, sample collection was started with strict privacy. Confidentiality of the participants’ data was maintained throughout the study by locking and limiting accessibility to the study information.
Results
Socio-Demographic Characteristics of Study Participants
A total of 356 study participants were recruited for the serum protein electrophoresis RI establishment study. Among these, because of elevated highly sensitive C-reactive protein (hsCRP), both elevated hsCRP and lipemia, lipemia, and hemolysis, 34 samples (9.55%), 13 samples (3.65%), 11 samples (3.09%), and one sample (0.28%), respectively, were rejected. Finally, 297 apparently healthy adults (124 males and 173 females) were involved in the final analysis. The median age of the study participants was 30 years, with an interquartile range of 27–39 years. The distribution of study participants in terms of age and sex is shown in Table 1.
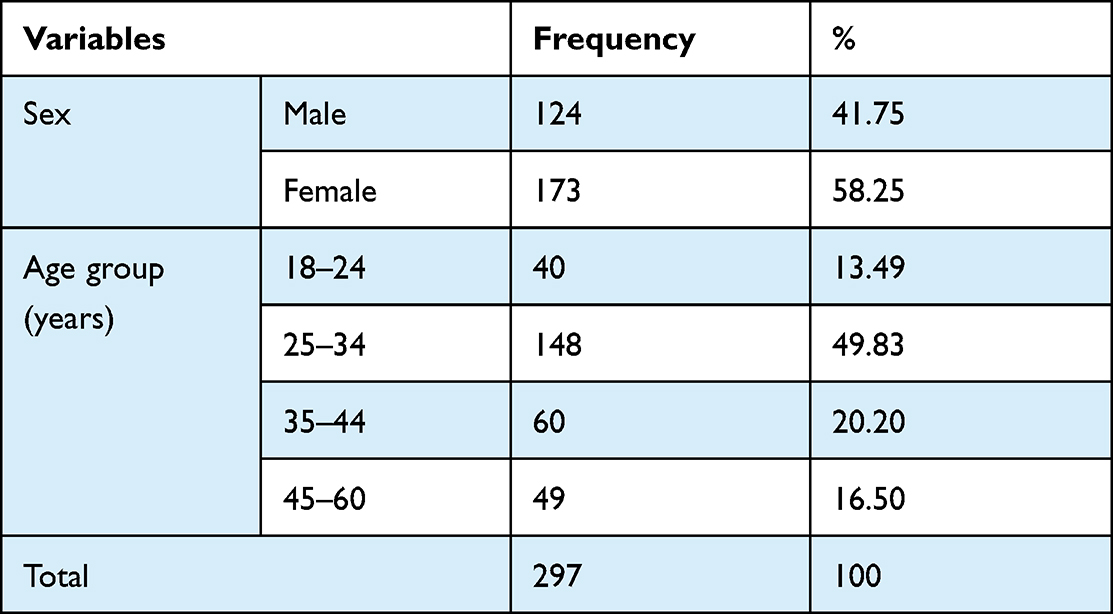 |
Table 1 Socio-Demographic Characteristics of Study Participants in Addis Ababa, Ethiopia, 2020 (N=297; Male=124 and Female=173) |
Normality Test for Laboratory Data Distribution
Primarily, continuous variables were tested for normality with the Kolmogorov–Smirnov and Shapiro–Wilk tests. The tests showed a normal distribution for albumin (%), alpha-1 (%), beta-1 (%), gamma (%), and the albumin to globulin ratio. However, albumin (g/dL), alpha-1 (g/dL), alpha-2 (%), alpha-2 (g/dL), beta-1 (g/dL), beta-2 (%), beta-2 (g/dL), and gamma (g/dL) failed to be normally distributed even after they had been logarithmically transformed.
Reference Intervals of Serum Protein Electrophoresis
As shown in Table 2, except for the gamma and beta globulin fractions, all of the serum protein fractions showed significant difference between males and females. The established RIs with 90% CI for the six serum protein fractions, including the albumin to globulin ratio, are summarized in Table 3. They were: albumin 53.83–64.59%, 52.24–63.55%; alpha-1 globulin 3.04–5.40%, 3.44–5.60%; alpha-2 globulin 8.0–12.67%, 8.44–12.87%; beta-1 globulin 5.01–7.38%, 5.14–7.86%; and albumin to globulin ratio 1.16–1.81 and 1.09–1.74 for males and females, respectively. The combined RIs for beta-2 globulin and gamma globulin were 2.54–4.90% and 12.40–21.66%, respectively.
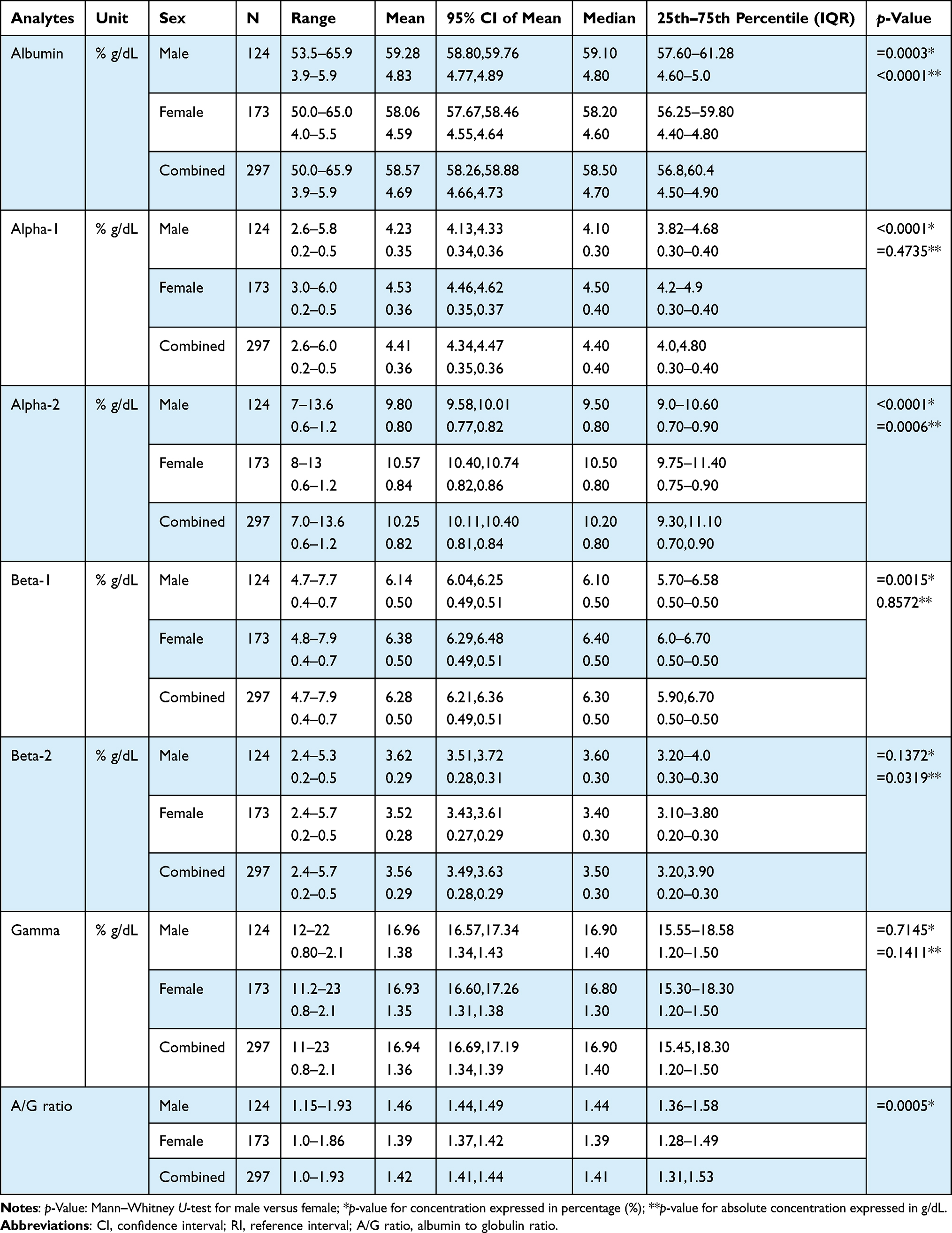 |
Table 2 Mean, Median with IQR of Serum Protein Electrophoresis of Apparently Healthy Adults in Addis Ababa, Ethiopia, 2020 (N=297; Male=124 and Female=173) |
 |
Table 3 Reference Interval with 90% CI of Reference Limits of Serum Protein Electrophoresis of Apparently Healthy Adults in Addis Ababa, Ethiopia, 2020 (N=297; Male=124 and Female=173) |
The RIs of apparently healthy adults in Addis Ababa, Ethiopia, established in the current study were compared with manufacturer-provided RIs and with already published RIs (Table 4). The lower limit of combined RIs established in the current study is higher than that of the manufacturer-provided RIs, except for albumin and beta-2 globulin. The current upper reference limit of alpha-1 globulin is lower than in a study conducted in Belgium,13 but this value is higher for alpha-2 globulin. A comparison of the published RIs obtained with Paragon and with Capillarys is summarized in Table 4.
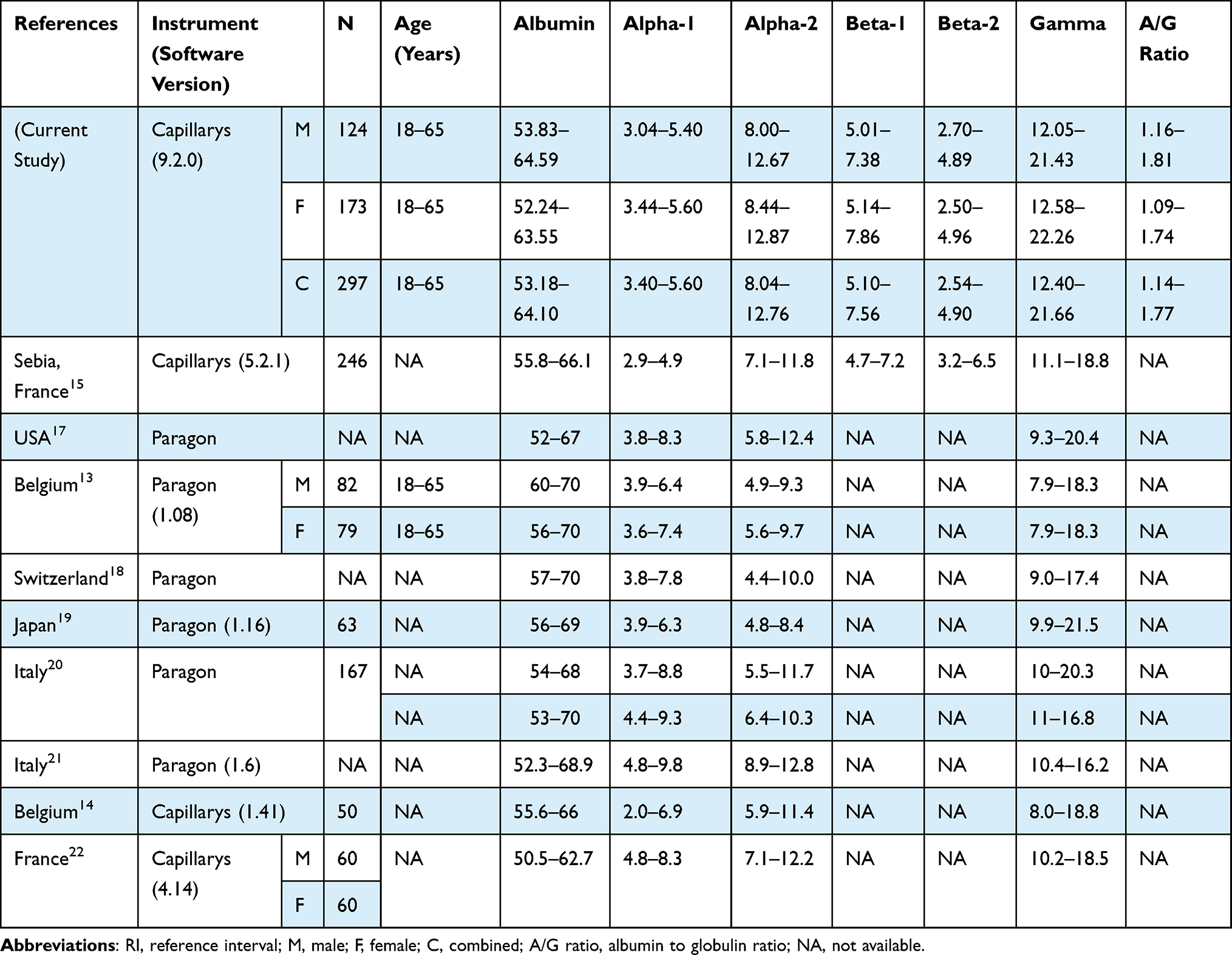 |
Table 4 Comparison of Serum Protein Electrophoresis RIs of Apparently Healthy Adults in Addis Ababa, Ethiopia, with Manufacturer Ranges and Published RIs |
Discussion
Reference intervals are useful in interpreting laboratory results to screen, diagnose, and monitor different disease states in patient management as well as research undertakings, including in clinical trials. However, because of a lack of locally established RIs, the clinical laboratory RIs currently in use in many African countries, including Ethiopia, are provided by companies and are based on mainly western populations.7 There is also a paucity of data on RIs for serum protein fractions in the literature.
The marked differences in the existing established RIs among population groups may lead to unnecessary additional investigations, failure to detect underlying disease, or mismanagement of patients.8
Since few or no RI data are available in poor countries such as Ethiopia, the current study established RIs for serum protein fractions, which could serve as baseline data for the diagnosis, interpretation, and monitoring of problems associated with serum proteins fractions in clinical laboratories.
The RIs provided by the reagent manufacturer in France,15 and other published RIs in Belgium,14 the USA,17 Switzerland,18 Japan,19 Italy,20 and France22 revealed a combined RI for both males and females for all serum protein fractions. But a study conducted by Lim et al24 recommended the establishment of gender-specific RIs, which would play a crucial role in the interpretation of laboratory results of serum protein fractions. As a result, the RIs established in the current study provide gender-specific values for serum protein fractions.
In the current study, the non-parametric test (Mann–Whitney U-test) reveals statistically significant gender-specific differences for albumin and alpha-2 globulin (expressed both as a percentage and as absolute concentration), alpha-1, beta-1, and the albumin to globulin ratio. However, the differences for beta-2 and gamma globulin were not statistically significant. This study is in agreement with a study conducted by Bossuyt et al in Belgium,13 which showed non-significant gender-specific differences in gamma globulin RIs.
The upper percentile of RIs established for albumin in current study is lower than either the RIs provided by the reagent manufacturer in France15 or previously published RIs in Belgium,13,14 the USA,17 Switzerland,18 Italy,20,21 and Japan,19 but higher than RIs established by Lissoir et al in France.22 The lower percentile for albumin is lower than already published RIs in Belgium,13,14 Switzerland,18 France,15 and Japan,19 but higher than those in the USA,17 Italy,21 and France.22 The discrepancies may be attributed to the genetic makeup and eating habits of study participants involved in RI establishment. The lower percentile is concordant with RIs established by Petrini et al in Italy.20
In the established RIs, females have a higher upper limit (97.5th percentile) for all globulin fractions (alpha-1 globulin, alpha-2 globulin, beta-1 globulin, beta-2 globulin, and gamma globulin) than males. This study is in agreement with findings of Bossuyt et al in Belgium13 for alpha and alpha-2, but differs in gamma globulin, which is the same for male and females. The variation may result from differences in antibody production during exposure to different disease states.
In the current study, the RIs established for serum protein electrophoresis fractions (albumin, alpha globulin, beta globulin, and gamma globulin) are different from the RIs in a previously published RI study, conducted in Belgium by Bossuyt et al, on 161 apparently healthy adults aged 18–65 years.13
Formerly, the albumin to globulin ratio was mainly used for the diagnosis of liver function and immunological diseases. In recent times, it has been reported as a novel inflammatory indicator for prognosis in various cancers, such as colorectal cancer, lung cancer, esophageal cancer, and breast cancer.23 This study established RIs for the albumin to globulin ratio, which had not been provided by the manufacturer of reagents in France15 or in the study conducted by Bossuyt et al in Belgium,13 or with other published RIs in Belgium,13,14 the USA,17 Switzerland,18 Italy,20,21 Japan,19 and France.22
Except for beta-2 globulin, the RIs established in the current study had a higher upper percentile in all globulin fractions (alpha-1 globulin, alpha-2 globulin, beta-1 globulin, beta-2 globulin, and gamma globulin) compared to the values provided by the reagent manufacturer in France.15 These variations may be attributed to racial differences (genetic predispositions).24
Conclusion
The present study established RIs for albumin, alpha-1 globulin, alpha-2 globulin, beta-1 globulin, beta-2 globulin, gamma globulin, and the albumin to globulin ratio for the first time in Ethiopia, and provides baseline data for future studies. The analysis was carried out in the National Reference Laboratory, which participates in external quality assurance and is accredited by the ENAO. The established RIs revealed gender-specific differences in all RIs except for beta-2 globulin and gamma globulin. Limitations of the study are that there have been no similar published studies in Ethiopia to compare with the present study, the present study did not cover participants above 65 years of age, and multiple myeloma patients were not enrolled in our study. Thus, further study is needed to cover this area.
Abbreviations
CLSI, Clinical and Laboratory Standards Institute; DRERC, Department of Medical Laboratory Science Research and Ethical Review Committee; ENAO, Ethiopian National Accreditation Office; EOF, electro-osmotic force; EPHI, Ethiopian Public Health Institute; FDA, Food and Drug Administration; hsCRP, highly sensitive C-reactive protein; ISO, International Organization for Standardization; RI, reference interval; SOP, standard operating procedure.
Data Sharing Statement
All necessary data generated or analyzed during this study are included in this article.
Acknowledgments
We would like to acknowledge the Ethiopian Public Health Institute National Clinical Chemistry Reference Laboratory for allowing us to use their laboratory for sample analysis. Addis Ababa University and the Ministry of Innovation and Technology are gratefully acknowledged for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas, contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article was submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Ethiopian Public Health Institute, Addis Ababa University, and Ministry of Innovation and Technology. However, they had no role in manuscript writing, editing, approval, or decision to publish.
Disclosure
A thesis of this paper by Bikila et al has previously been published.25
The abstract of this paper was presented at the International Conference on Clinical Pathology, Diagnostic Techniques and Testing as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in International Journal of Medical and Health Sciences.26 All authors declare that they have no conflicts of interest in relation to this work.
References
1. Clark R, Katzmann JA, Wiegert E, et al. Rapid capillary electrophoretic analysis of human serum proteins: qualitative comparison with high-throughput agarose gel electrophoresis. J Chromatogr A. 1996;744:205–213. doi:10.1016/0021-9673(96)00190-2
2. Henskens Y, De Winter J, Pekelharing M, Ponjee G. Detection and identification of monoclonal gammopathies by capillary electrophoresis. Clin Chem. 1998;1190:1184–1190. doi:10.1093/clinchem/44.6.1184
3. Jellum E, Dollekamp H, Brunsvig A, Gislefoss R. Diagnostic applications of chromatography and capillary electrophoresis. J Chromatogr B Biomed Sci Appl. 1997;689:155–164. doi:10.1016/s0378-4347(96)00333-7
4. Oda RP, Clark R, Katzmann JA, Landers JP. Capillary electrophoresis as a clinical tool for the analysis of protein in serum and other body fluids. Electrophor. 1997;18:1715–1723. doi:10.1002/elps.1150181004
5. Katzmann JA, Clark R, Wiegert E, et al. Identification of monoclonal proteins in serum: a quantitative comparison of acetate, agarose gel, and capillary electrophoresis. Electrophor. 1997;18:1775–1780. doi:10.1002/elps.1150181011
6. Wijnen PA, Van Dieijen-Visser MP. Capillary electrophoresis of serum proteins, reproducibility, comparison with agarose gel electrophoresis and a review of the literature. Clin Chem Lab Med. 1996;34:535–546. doi:10.1515/cclm.1996.34.7.535
7. Karita E, Ketter N, Price MA, et al. CLSI-derived hematology and biochemistry reference intervals for healthy adults in eastern and Southern Africa. PLoS One. 2009;4:e4401. doi:10.1371/journal.pone.0004401
8. Wayne PA. CLSI, how to define and determine reference intervals in the clinical laboratory: approved guideline– 2nd ed. C28-A2. 2000;20:13.
9. Hallworth MJ. The ‘70% claim’: what is the evidence base? Ann Clin Biochem. 2011;48:487–488. doi:10.1258/acb.2011.011177
10. Horowitz GL, Altaie S, Boyd JC, et al. EP28-A3C Defining, Establishing, and Verifying Reference Intervals in the Clinical Laboratory; Approved Guideline. San Diego: CLSI; 2010.
11. Addis Ababa city administration website; 2019. Available from: http://www.addisababa.gov.et/fr/web/guest/city-map.
12. CSA. Third national population and housing census in May and November 2007. Addis Ababa; 2010. Available from: https://www.ethiopianreview.com/pdf/001/Cen2007_firstdraft(1).pdf.
13. Bossuyt X, Schiettekatte G, Bogaerts A, Blanckaert N. Serum protein electrophoresis by CZE 2000 clinical capillary electrophoresis system. Clin Chem. 1998;44:749–759. PMID: 9554485. doi:10.1093/clinchem/44.4.749
14. Bossuyt X, Lissoir B, Marien G, et al. Automated serum protein electrophoresis by Capillarys. Clin Chem Lab Med. 2003;41:704–710. doi:10.1515/CCLM.2003.107
15. Capillarys protein (E) 6; 2010. Available from: https://www.ilexmedical.com/files/Sebia%20inserts/CAPILLAR S_PROTEIN (E) _6.pdf.
16. Keren D. Protein Electrophoresis in Clinical Diagnosis. CRC Press; 2003.
17. Jolliff CR, Blessum CR. Comparison of serum protein electrophoresis by agarose gel and capillary zone electrophoresis in a clinical setting. Electrophor. 1997;18:1781–1784. doi:10.1002/elps.1150181012
18. Thormann W, Wey AB, Lurie IS, et al. Capillary electrophoresis in clinical and forensic analysis: recent advances and breakthrough to routine applications. Electrophor. 1999;20:3203–3236. doi:10.1002/(SICI)1522-2683(19991001)20:15/16<3203::AID-ELPS3203>3.0.CO;2-E
19. Ihara H, Toya N, Kakinoki T, et al. Clinical analysis of human serum proteins using the Beckman automated Paragon 2000 CZE system. Seibutsu Butsuri Kagaku. 1999;43:165–169. doi:10.2198/sbk.43.165
20. Petrini C, Alessio MG, Scapellato L, Brambilla S, Franzini C. Serum protein by capillary zone electrophoresis: approaches to the definition of reference values. Clin Chem Lab Med. 1999;37:975–980. doi:10.1515/CCLM.1999.144
21. Luraschi P, Dalla Dea E, Franzini C. Capillary zone electrophoresis of serum proteins: effects of changed analytical conditions. Clin Chem Lab Med. 2003;41:782–786. doi:10.1515/CCLM.2003.118
22. Lissoir B, Wallemacq P, Maisin D. Serum protein electrophoresis: comparison of capillary zone electrophoresis Capillarys (Sebia) and agarose gel electrophoresis Hydrasys (Sebia). Ann Biol Clin. 2003;61:557–562. PMID: 14671753.
23. Mao M, Wei X, Sheng H, et al. Clinical significance of preoperative albumin and globulin ratio in patients with gastric cancer undergoing treatment. Bio Med Res Int. 2017. doi:10.1155/2017/3083267
24. Lim E, Miyamura J, Chen J. Racial/ethnic-specific reference intervals for common laboratory tests: a comparison among Asians, blacks, Hispanics, and white. Hawaii J Public Health. 2015;74:302. PMID: 26468426 PMCID: PMC4578165.
25. Bikila D. Establishment of reference interval for serum protein electrophoresis of apparently healthy adults in Addis Ababa, Ethiopia [master's thesis]. Addis Ababa: Addis Ababa University. Available from: http://213.55.95.56/bitstream/handle/123456789/23375/Demiraw%20Bikila.pdf?sequence=1&isAllowed=y.
26. Bikila D, Lejisa T, Tolcha Y, et al. Establishment of Reference Interval for Serum Protein Electrophoresis of Apparently Healthy Adults in Addis Ababa, Ethiopia. Int. J Med and Health Sci. 2022; 16(4). Available from: https://publications.waset.org/abstracts/145858/establishment-of-reference-interval-for-serum-protein-electrophoresis-of-apparently-healthy-adults-in-addis-ababa-ethiopia.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Reference Intervals for Absolute and Percentage CD4+ T Lymphocytes among an Apparently Healthy Population in Addis Ababa, Ethiopia
Chalchisa D, Belay Y, Befekadu E, Kassaw M, G/Egzeabher L, Gebremicael G, Lengiso B, Chala D, Sahlemariam Z, Kebede E, Abate E, Tsegaye A
International Journal of General Medicine 2022, 15:5361-5367
Published Date: 1 June 2022
Incidence, Bacterial Profile and Predictors of Surgical Site Infection After Cesarean Section in Ethiopia, A Prospective Cohort Study
Mezemir R, Olayemi O, Dessie Y
International Journal of Women's Health 2023, 15:1547-1560
Published Date: 13 October 2023