Back to Journals » Journal of Pain Research » Volume 19
Establishing a Predictive Model for Acute Postoperative Pain at PACU Awakening Based on Preoperative Hypoalbuminemia and Anemia: Clinical Implications for Perioperative Nursing
Authors Tu Y ![]() , Du W
, Du W ![]() , Zhang X, Chen Y, Zhou B, Sun C, Xu M
, Zhang X, Chen Y, Zhou B, Sun C, Xu M
Received 6 December 2025
Accepted for publication 24 March 2026
Published 27 March 2026 Volume 2026:19 583667
DOI https://doi.org/10.2147/JPR.S583667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Karina Gritsenko
Yingying Tu,1 Wenwen Du,2 Xiaozhen Zhang,1 Yani Chen,1 Bingbing Zhou,1 Caixia Sun,1 Min Xu1
1Department of Nursing, The First Affiliated Hospital of Wenzhou Medical University, WenZhou, ZheJiang, 325000, People’s Republic of China; 2Department of Anesthesiology, The First Affiliated Hospital of Wenzhou Medical University, WenZhou, ZheJiang, 325000, People’s Republic of China
Correspondence: Min Xu, Email [email protected]
Background: The management of acute postoperative pain remains a major challenge in perioperative nursing, as it delays recovery and impacts patient satisfaction. Physiological markers such as preoperative serum albumin and hemoglobin are important indicators of pain risk but are often underutilized in conventional nursing assessments.
Methods: This single-center, retrospective cohort study, grounded in the Symptom Management Theory, analyzed data from 790 surgical patients who underwent procedures at the First Affiliated Hospital of Wenzhou Medical University between January and December 2023. Preoperative hypoalbuminemia and anemia were identified through routine laboratory tests. The primary outcome was acute postoperative pain, assessed upon awakening in the Post-Anesthesia Care Unit (PACU). Their associations with this outcome were examined using multivariable logistic regression, adjusting for key confounders including analgesic pump use. Finally, a predictive nomogram was developed to visualize the risk.
Results: The incidence of acute postoperative pain at PACU Awakening was 45.1%. Both preoperative hypoalbuminemia (OR 1.68, 95% CI 1.19– 2.39, p = 0.003) and anemia (OR 1.50, 95% CI 1.04– 2.16, p = 0.030) were independent predictors of acute postoperative pain at PACU Awakening. The nomogram demonstrated good calibration and acceptable discrimination (AUC = 0.690, 95% CI 0.653– 0.726). Decision curve analysis showed a positive net clinical benefit across a wide range of threshold probabilities.
Conclusion: Preoperative hypoalbuminemia and anemia are significant predictors of acute postoperative pain at PACU Awakening. Integrating these biomarkers into routine perioperative nursing assessments enables early identification of at-risk patients and facilitates evidence-based interventions such as nutritional optimization and anemia correction, fostering proactive and personalized pain management strategies. Decision curve analysis showed a positive net clinical benefit across a wide range of threshold probabilities.
Keywords: acute postoperative pain, PACU, hypoalbuminemia, anemia, pain management, perioperative nursing
Introduction
Behind the staggering global annual figure of over 310 million surgeries1 lies a pressing clinical reality: acute postoperative pain remains highly prevalent and distressing for patients.2,3 This pain, typically lasting 3–7 days, acts as a critical barrier to recovery when poorly managed, leading to delayed mobilization, impaired physical function, prolonged hospitalization, and increased healthcare costs.4 In particular, the immediate pain experienced by patients when waking up in the post-anesthesia care unit (PACU) is not only the beginning of postoperative stress responses but also a key predictor of later recovery quality. However, poorly managed acute pain can easily develop into chronic pain, further complicating the rehabilitation process.5
Serum albumin and hemoglobin are routinely monitored preoperative indicators that provide valuable insights into a patient’s nutritional and hematologic status. Hypoalbuminemia, defined as a serum albumin level < 35 g/L, reflects poor nutritional reserve and is associated with delayed wound healing, immune dysfunction, longer hospitalization, and increased mortality.6–11 Similarly, preoperative anemia, defined by WHO criteria (Hb < 130 g/L in men, < 120 g/L in women), affects approximately one-third of surgical patients and is a well-established risk factor for increased transfusion rates and postoperative complications.12–16 These biomarkers are routinely assessed by perioperative nurses, positioning them as useful tools for identifying patients at higher risk for adverse surgical outcomes.
Despite substantial research links these biomarkers to broader surgical outcomes, their specific association with acute pain at PACU awakening remains inadequately explored. We selected preoperative albumin (ALB) and hemoglobin (Hb) as core predictors based on the Symptom Management Theory (SMT).17,18 SMT posits that symptoms like pain are multidimensional experiences driven by modifiable biological antecedents, and that early identification of these factors is crucial for proactive symptom control. Biologically, ALB serves as a negative acute-phase protein reflecting systemic inflammation, which can modulate neural sensitivity and impair tissue repair. Meanwhile, Hb levels determine tissue oxygen-carrying capacity; preoperative anemia triggers localized hypoxia and the release of algogenic substances (eg, lactate and pro-inflammatory cytokines), thereby lowering the pain threshold. Crucially, unlike non-modifiable factors such as age or surgical type, ALB and Hb are clinically actionable. Identifying these risks enables perioperative nurses to implement proactive interventions-such as nutritional optimization and anemia correction—shifting care from reactive management to predictive prevention.
Grounded in the SMT, which conceptualizes biological status as a critical antecedent to symptom experience, this study aims to bridge this gap. The objectives are twofold: first, to investigate the independent associations between preoperative hypoalbuminemia, anemia, and acute pain at PACU awakening; and second, to develop and validate a practical predictive nomogram. This model is designed to empower perioperative nurses by enabling early risk stratification, facilitating timely nutritional support, and optimizing individualized pain management strategies.
Materials and Methods
Ethics Approval
This study was conducted in accordance with the ethical standards of the institutional and national research committees and with the 1964 Declaration of Helsinki and its later amendments. Ethical approval was obtained from the Research Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University (Approval No. KY2024-019). As a retrospective cohort study, this research did not involve clinical trials; therefore, a clinical trial registration number was not applicable. Due to the use of anonymized patient data and the retrospective nature of the study, a waiver of informed consent was granted by the ethics committee.
Participants and Randomization
This study was designed as a single-center, retrospective cohort study. From an initial population of 100,858 adult patients who underwent postoperative observation in the PACU between January 1, 2023, and December 31, 2023. Data were retrieved from the hospital’s electronic medical record system and anesthesia information management system, encompassing all adult patients who underwent postoperative observation during the study period.
Eligible participants met the following inclusion criteria: (1) postoperative observation after surgery, (2) age≥18 years, (3) ability to effectively communicate and provide reliable pain assessments, and (4) completion of preoperative clinical evaluations, including routine laboratory testing and medical history documentation. Patients were excluded if they had: (1) incomplete medical or anesthesia records, (2) diagnosed cognitive impairment or mental illness (eg, dementia, depression, schizophrenia), (3) a history of chronic pain lasting more than three months, or (4) ongoing psychiatric or pain management treatment.
To construct the analytical cohort, we employed a stratified random sampling strategy and completed the final cohort construction using R software (version 4.4.0). To ensure that the sample accurately reflected the diversity of surgical practice and the temporal distribution throughout the year, we defined strata based on the primary surgeon and surgery date. The specific reason for choosing this sampling method was its convenience for high-fidelity manual data verification-ensuring precise matching of preoperative biomarkers, surgical invasiveness, and individualized PCIA configurations, which would be difficult to achieve in a population sample of over 100,000 individuals. The final sample size of 790 patients provided sufficient statistical power for multivariable modeling, strictly meeting the standard requirement of at least 10 events per variable (EPV).
Data Collection
Data were retrospectively collected from three institutional information systems: the hospital’s electronic medical record system, the anesthesia information management system, and the laboratory information system. Relevant variables, including demographic information, preoperative, intraoperative, and postoperative data, were extracted. This included patient age, sex, BMI, educational level, comorbidities, surgical site, anesthesia type, surgery duration, anesthesia duration, intraoperative medication use, and postoperative pain assessment records.
Preoperative serum albumin and hemoglobin levels were obtained from routine laboratory tests performed 1–3 days before surgery. Hypoalbuminemia was defined as a serum albumin concentration < 35 g/L, and anemia was defined as a hemoglobin level < 120 g/L for men and < 110 g/L for women. Postoperative pain was assessed using the Visual Analog Scale (VAS) when the patient first achieved a Modified Aldrete Score of ≥ 9 (or when fully oriented to person, place, and time). The primary outcome was the VAS score at rest at this time point. To reflect the overall incidence of postoperative pain and support proactive nursing management, the outcome was dichotomized as “no pain” (VAS = 0) and “pain” (VAS > 0). This threshold ensures that patients experiencing even mild discomfort are identified for early nursing assessment and timely intervention, thereby preventing the escalation to severe pain. The VAS is a 10 - centimeter line anchored at 0 (“no pain”) and 10 (“worst imaginable pain”), where the patient indicated their pain intensity.
Postoperative analgesic management followed a standardized clinical protocol. For patients receiving Patient-Controlled Intravenous Analgesia (PCIA), the pump was configured with Sufentanil, and the dosage was strictly titrated according to the patient’s body weight to ensure pharmacological consistency. The presence or absence of a PCIA pump was then included in the multivariable model as a covariate to adjust for its potential influence on pain outcomes.
To ensure data integrity, two trained research nurses independently performed data extraction and cross-verification. Any discrepancies were resolved through discussion with a senior researcher. Data were entered into a secure Microsoft Access database with double-entry verification. The anonymized dataset was accessible exclusively to authorized research personnel, ensuring the accuracy, consistency, and completeness of all variables included in the analysis.
Statistical Analysis
Statistical analyses were performed using R software (version 4.4.0; R Foundation for Statistical Computing, Vienna, Austria). Continuous variables were summarized as mean ± standard deviation (SD) or median with interquartile range (IQR), based on the distribution assessed by the Kolmogorov–Smirnov test. Categorical variables were presented as counts and percentages. Group comparisons were conducted using the t test or Mann–Whitney U-test for continuous variables and the chi-square test for categorical variables.
Univariate logistic regression was used to identify potential factors associated with acute postoperative pain. Variables with a p-value < 0.05 were entered into a multivariable logistic regression model to identify independent predictors of acute postoperative pain. Model discrimination and calibration were evaluated using the receiver operating characteristic (ROC) curve, area under the curve (AUC), and calibration plots based on 1000 bootstrap resamples. Decision curve analysis (DCA) was applied to assess the model’s clinical benefit. Statistical significance was set at p < 0.05.
Results
Basic Characteristics of the Participants
A total of 790 postoperative patients were analyzed (Table 1). Of these, 356 patients (45.1%) experienced acute postoperative pain at PACU Awakening, while 434 patients (54.9%) did not report pain. The cohort had a mean age of 56.1 ± 16.4 years and a mean BMI of 23.4 ± 3.5 kg/m2, with a nearly equal gender distribution (47.9% male, 52.1% female). More than half of the participants (55.6%) had completed only primary school or less. Common comorbidities included hypertension (29.0%), diabetes mellitus (11.0%), stroke (2.5%), and coronary heart disease (2.0%). Preoperative hypoalbuminemia was present in 296 patients (37.5%), and 210 patients (26.6%) had preoperative anemia. Pain severity assessment revealed that 703 patients (89.0%) reported mild to moderate pain, while 87 patients (11.0%) experienced moderate to severe pain. The descriptive statistics for continuous variables, including age, BMI, and surgery duration, are provided in Table 2.
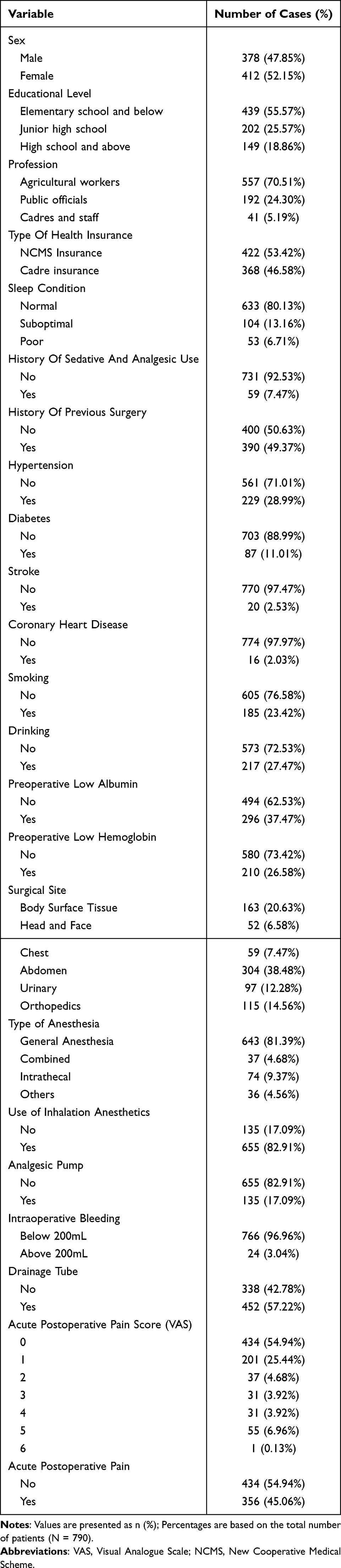 |
Table 1 Overall Patients Baseline (N = 790) |
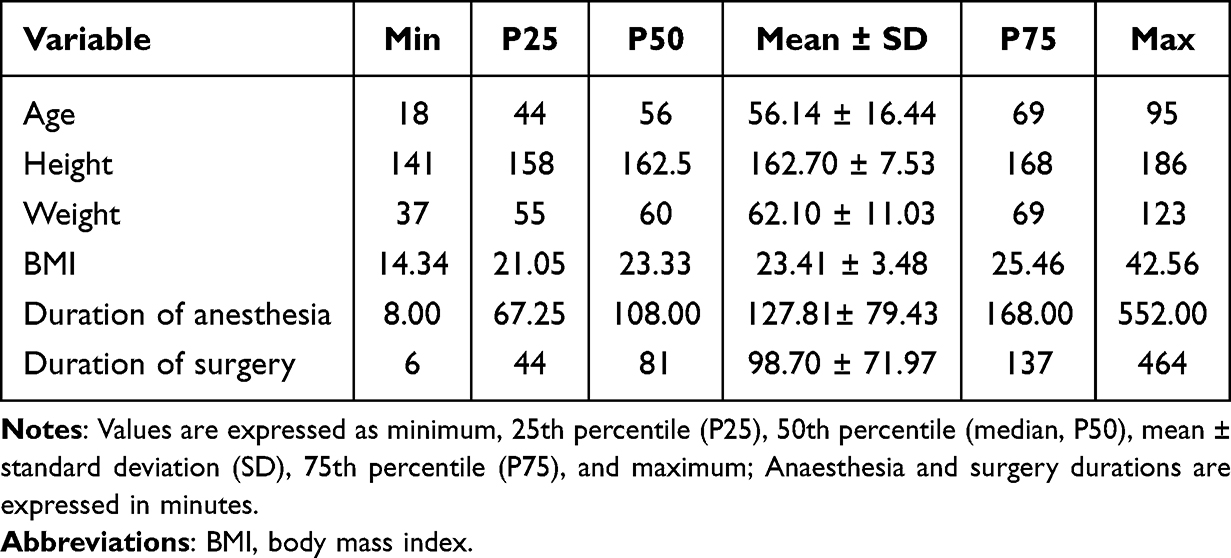 |
Table 2 Descriptive Statistics General Population Characteristics (N = 790) |
In univariate comparisons between patients with and without postoperative pain (Table 3), several factors demonstrated statistically significant differences, including sex (p = 0.001), age (p < 0.001), preoperative hypoalbuminemia (p < 0.001), preoperative anemia (p < 0.001), type of anesthesia (p = 0.016), surgery duration (p < 0.001), anesthesia duration (p < 0.001), intraoperative analgesic pump use (p < 0.001), and drainage tube placement (p < 0.001).
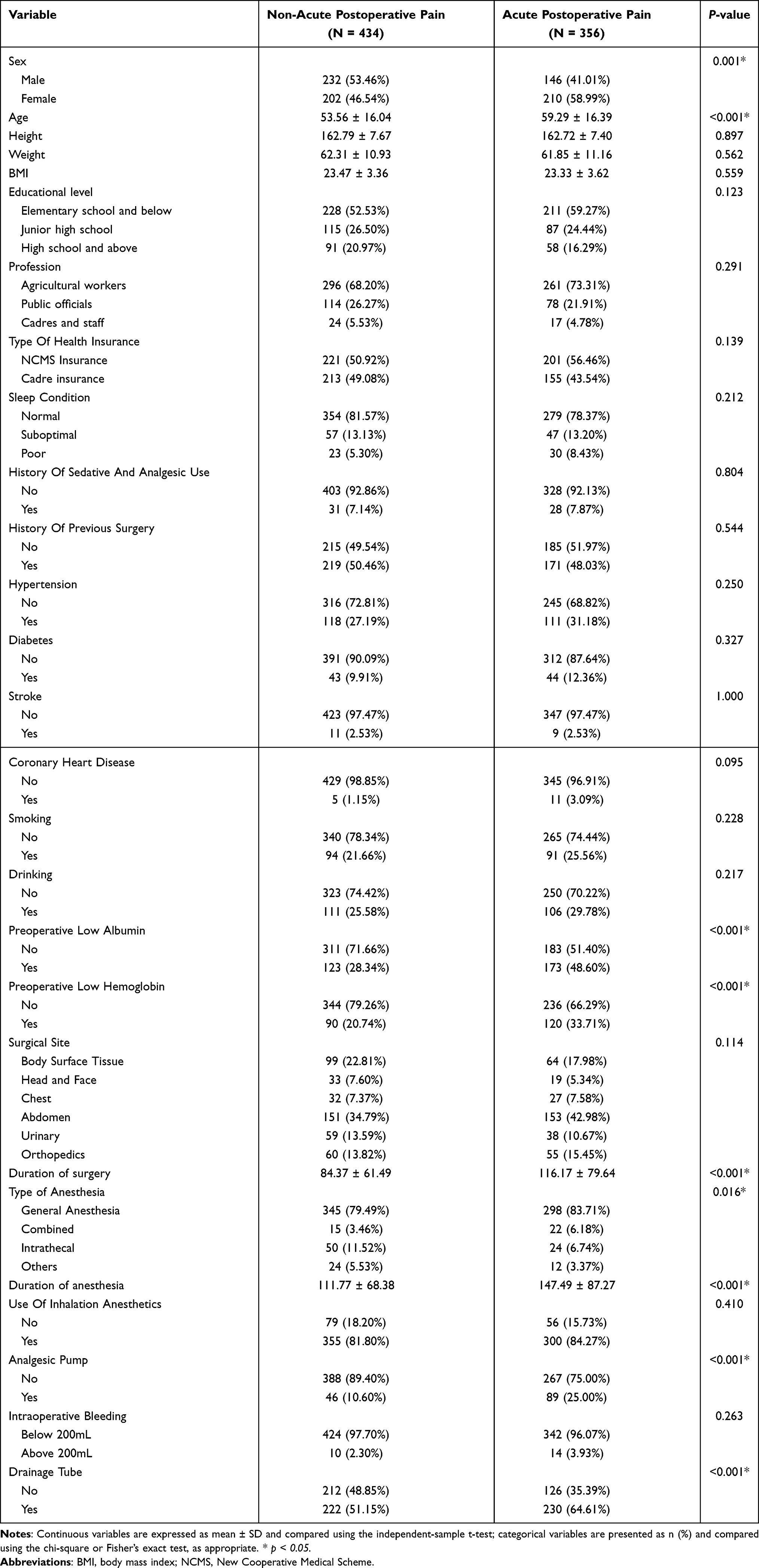 |
Table 3 Analysis of People with Acute Postoperative Pain in Different States (N = 790) |
Risk Factors and Multivariable Logistic Regression Analysis
After adjusting for potential confounders in the multivariable logistic regression, preoperative hypoalbuminemia and anemia remained independently associated with PACU Awakening pain (Table 4). As shown in the predictive model (Figure 1), after comprehensively controlling for surgical site, duration, and standardized PCIA use, both biomarkers were identified as significant independent predictors. Specifically, the odds of experiencing early PACU resting pain were 1.50 times higher in patients with preoperative anemia (adjusted OR 1.50, 95% CI 1.04–2.16, p = 0.030) and 1.68 times higher in those with hypoalbuminemia (adjusted OR 1.68, 95% CI 1.19–2.39, p = 0.003). Other independent risk factors identified in the adjusted model included female sex and longer surgical duration.
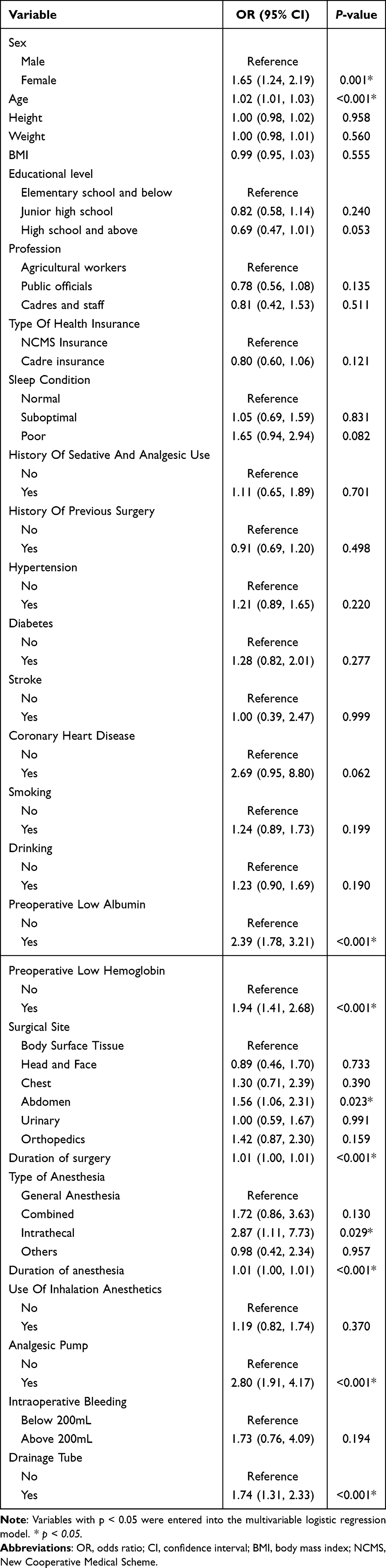 |
Table 4 Analysis of Univariate Logistic Regression (N = 790) |
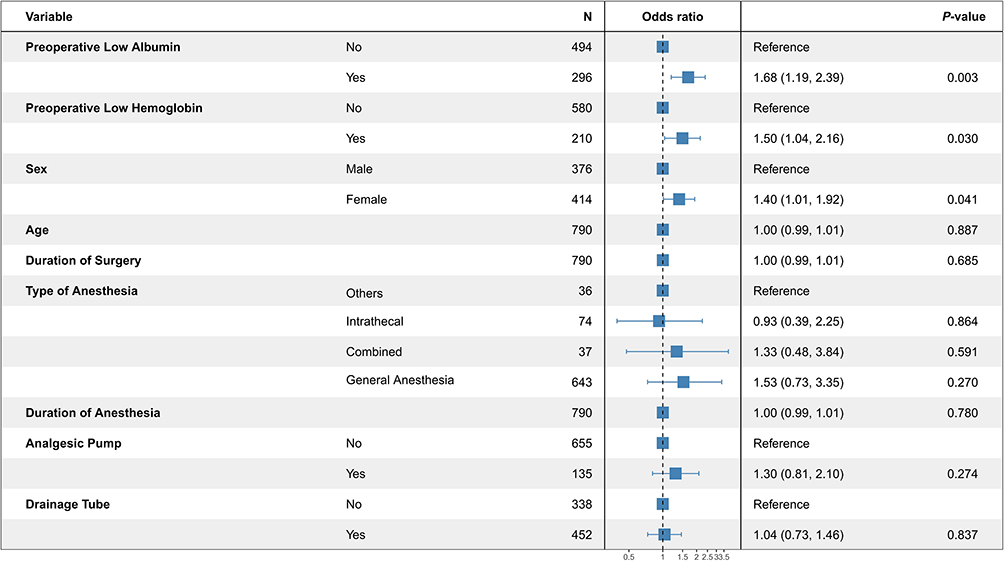 |
Figure 1 Multifactor logistic regression model of acute postoperative pain at PACU Awakening. |
These findings suggest that preoperative nutritional and hematologic deficiencies, which are routinely assessed in clinical practice, may serve as valuable indicators for early identification of patients at risk for postoperative pain, even after accounting for the underlying surgical insult. This highlights the importance of integrating these readily available biomarkers into perioperative risk assessment protocols.
Model Validation and Clinical Application
To make the predictive model more accessible and practical at the bedside, we developed a nomogram (Figure 2) that visually estimates the probability of acute postoperative pain at PACU Awakening. The nomogram incorporates preoperative albumin and hemoglobin levels, sex, surgery duration, and anesthesia duration — parameters easily measured through routine nursing assessments. By summing the individual scores for each variable, nurses can quickly obtain a total score that corresponds to the patient’s predicted risk, facilitating rapid risk stratification at the bedside.
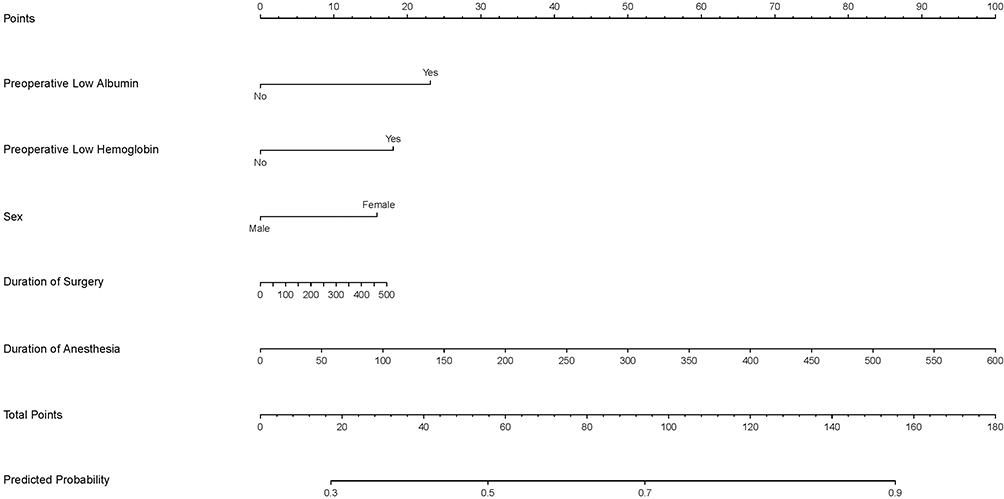 |
Figure 2 The nomogram model to predict acute postoperative pain at PACU Awakening. |
The model’s performance was evaluated in terms of three key dimensions: discrimination, calibration, and clinical utility. The area under the receiver operating characteristic (ROC) curve was 0.690 (95% CI: 0.653–0.726, Figure 3), indicating moderate discriminative ability. A calibration plot, generated from 1000 bootstrap resamples, demonstrated good agreement between predicted and observed outcomes (Figure 4), The mean absolute error (MAE) was 0.029 (n=790), indicating minimal overfitting and high reliability. Additionally, decision curve analysis (Figure 5) confirmed that the model provides a positive net clinical benefit across a wide range of clinically relevant threshold probabilities (0.10 to 0.85). Within this window, the model outperformed both the “treat-all” and “treat-none” strategies, highlighting its practical value in clinical decision-making.
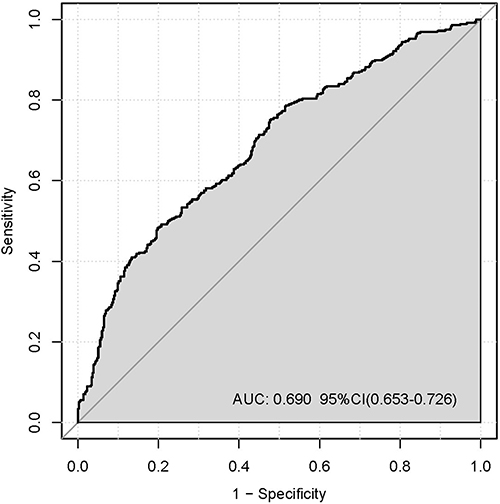 |
Figure 3 The AUC of the nomogram model. |
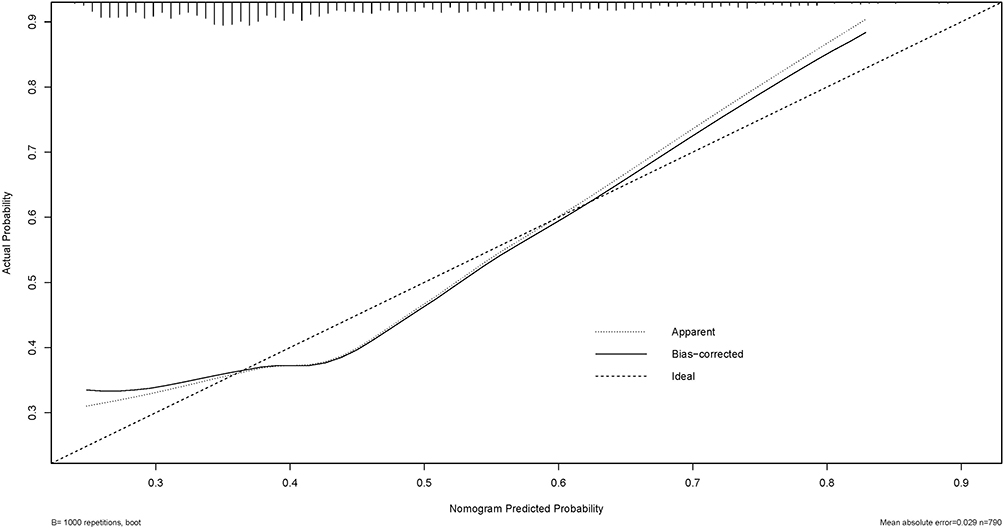 |
Figure 4 The calibration curve of the nomogram model. |
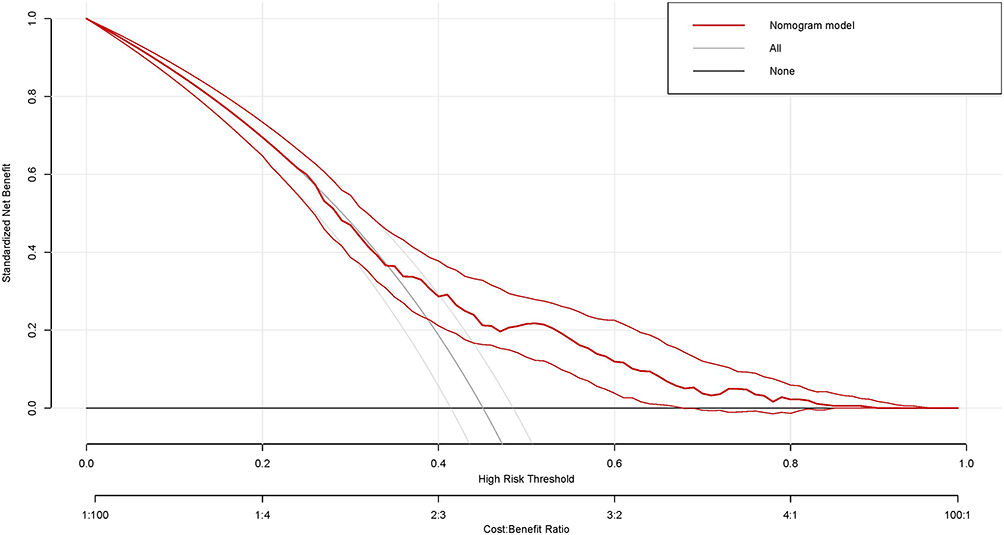 |
Figure 5 The decision curve of the nomogram model. |
Discussion
This study identified preoperative hypoalbuminemia and anemia as independent predictors of acute postoperative pain at PACU Awakening in surgical patients. After adjusting for confounding factors, hypoalbuminemia increased the likelihood of postoperative pain by 68%, while anemia raised the risk by 50%. Female sex, longer anesthesia duration, and longer surgery duration were also associated with a higher incidence of pain. The predictive model showed good calibration and moderate discrimination (AUC = 0.690), suggesting its utility in early risk stratification for perioperative care.
Interpreted through the Symptom Management Theory (SMT), these findings provide a valuable connection between empirical evidence and a theoretical nursing framework. SMT views symptoms, such as postoperative pain, as dynamic experiences that can be managed through an iterative process of assessment, intervention, and evaluation.17,18 Within this framework, serum albumin and hemoglobin levels serve as objective biomarkers that reflect physiological reserves and a patient’s vulnerability to symptoms like pain. Preoperative assessment of these biomarkers allows nurses to identify high-risk patients early, enabling proactive interventions such as nutritional optimization and anemia correction before surgery. Postoperative pain monitoring, as part of the SMT cycle, serves as the evaluation component, ensuring that pain management strategies are tailored and adjusted to the individual patient’s needs.
These findings extend existing literature by demonstrating that preoperative nutritional and hematologic deficits are not only predictive of complications and mortality but also of subjective symptoms, specifically acute postoperative pain. Previous studies have linked hypoalbuminemia to systemic inflammation and oxidative stress, both of which sensitize nociceptors and amplify pain responses. Specifically, hypoalbuminemia can lead to an imbalance in cytokine production, resulting in an exaggerated inflammatory response that increases pain sensitivity.10,19,20 Liu et al21 reported that hypoalbuminemia predicted early postoperative complications in revision shoulder arthroplasty, reinforcing its prognostic relevance beyond merely indicating malnutrition. Similarly, anemia has been consistently associated with delayed wound healing and increased morbidity.12,22,23 The underlying mechanisms include impaired oxygen delivery and tissue hypoxia, which activate inflammatory mediators such as prostaglandins and bradykinin, sensitizing peripheral pain receptors and lowering pain thresholds.15,24,25 Together, these biological pathways help explain how hypoalbuminemia and anemia may potentiate acute postoperative pain responses.
Additional findings, including the influence of female sex, surgery duration, and anesthesia time, align with prior research. Women are generally reported to experience greater pain sensitivity due to hormonal fluctuations, variations in endogenous opioid systems, and gender differences in immune responses.26,27 Furthermore, prolonged surgical and anesthesia durations are linked to increased tissue trauma, a higher inflammatory burden, and longer exposure to anesthetic agents, all of which contribute to greater postoperative pain.28,29 These findings highlight that postoperative pain is multifactorial, arising from the interaction of biological, procedural, and demographic factors, emphasizing the need for comprehensive, individualized pain management strategies.
From a nursing perspective, this study offers both theoretical and practical insights into perioperative pain management. Grounded in SMT, the proposed model integrates the full cycle of assessment, intervention, and evaluation into perioperative nursing practice. Preoperative evaluation of albumin and hemoglobin allows for objective pain risk assessment. High-risk patients can receive preoperative interventions such as nutritional counseling, anemia correction, and perioperative education. Postoperatively, standardized pain assessments using validated tools allow for timely adjustment of analgesic strategies. When incorporated into electronic nursing documentation systems, this model could serve as a clinical decision-support tool, generating automated alerts for high-risk patients and enhancing interdisciplinary collaboration between nurses, anesthesiologists, and dietitians. This approach exemplifies precision nursing, utilizing individualized, data-driven interventions to improve outcomes and enhance patient satisfaction.
Several limitations must be acknowledged. First, this study’s retrospective, single-center design limits the generalizability of its findings. Although stratified sampling was used to minimize selection bias, variations in surgical practice across institutions may affect the external validity of the model. Future prospective, multicenter studies should validate the predictive performance of this model and assess the impact of implementing model-guided interventions in diverse settings. Second, psychosocial variables such as anxiety, coping styles, and pain catastrophizing were not included in this analysis, even though they are known to influence pain perception. Incorporating these variables into future studies could enhance the model’s accuracy and predictive power. Lastly, this study focused solely on acute postoperative pain at PACU Awakening; Future research should employ prospective, multicenter designs to validate these findings and utilize longitudinal trajectory analysis to determine whether preoperative nutritional markers can predict the evolution of pain from the acute phase to chronic postsurgical recovery.
Conclusions
In conclusion, preoperative hypoalbuminemia and anemia are significant, modifiable predictors of acute postoperative pain at PACU Awakening. Incorporating these biomarkers into routine preoperative nursing assessments facilitates early risk identification and supports evidence-based interventions, including nutritional optimization and anemia correction. Grounded in the Symptom Management Theory, this predictive model shifts perioperative care from reactive pain management to predictive and preventive nursing. While the model offers moderate predictive value, it provides a pragmatic, evidence-based tool for clinical decision-making. Future research involving longitudinal trajectory analysis and external validation is warranted to further confirm the clinical utility of these predictors in enhancing long-term postoperative recovery.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Research Ethics Committee of the First Affiliated Hospital of Wenzhou Medical University (Approval No. KY2024-019). All procedures were performed in accordance with the ethical standards of the institutional research committee and the 1964 Declaration of Helsinki and its later amendments. Because this was a retrospective analysis of anonymized clinical data, the requirement for informed consent was waived by the ethics committee.
Acknowledgments
We sincerely thank all the participants, nursing staff, and research team members for their invaluable contributions to this study. Special appreciation is extended to the perioperative nursing team and the institutional departments involved in data collection and patient care documentation.
Funding
This work was supported by a hospital-level scientific research project (Grant No. HLKY202506). The funding body had no role in the study design, data collection, analysis, interpretation, or manuscript preparation.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Dobson GP. Trauma of major surgery: a global problem that is not going away. Int J Surg. 2020;81:47–15. doi:10.1016/j.ijsu.2020.07.017
2. Chou R, Gordon DB, de Leon-Casasola OA. Management of postoperative pain: a clinical practice guideline from the American pain society, the American society of regional anesthesia and pain medicine, and the American society of anesthesiologists’ committee on regional anesthesia, executive committee, and administrative council. J Pain. 2016;17:131–157. doi:10.1016/j.jpain.2015.12.008
3. Meissner W, Zaslansky R. A survey of postoperative pain treatments and unmet needs. Best Pract Res Clin Anaesth. 2019;33:269–286. doi:10.1016/j.bpa.2019.10.003
4. Kehlet H, Dahl JB. Postoperative pain. World J Surg. 1993;17:215–219. doi:10.1007/BF01658929
5. Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;10:2287–2298. doi:10.2147/JPR.S144066
6. Roche M, Law TY, Kurowicki J, et al. Albumin, prealbumin, and transferrin may be predictive of wound complications following total knee arthroplasty. J Knee Surg. 2018;31:946–951. doi:10.1055/s-0038-1672122
7. Sayeed Z, Anoushiravani AA, Simha S, et al. Markers for malnutrition and BMI status in total joint arthroplasty and pharmaconutrient therapy. JBJS Rev. 2019;7:e3. doi:10.2106/JBJS.RVW.18.00056
8. Erstad BL. Serum albumin levels: who needs them? Ann Pharmacother. 2021;55:798–804. doi:10.1177/1060028020959348
9. Manolis AA, Manolis TA, Melita H, Mikhailidis DP, Manolis AS. Low serum albumin: a neglected predictor in patients with cardiovascular disease. Eur J Internal Med. 2022;102:24–39. doi:10.1016/j.ejim.2022.05.004
10. Tischler EH, Vummidi S, McDermott JR, Tiburzi HA, Gross JM, Suneja N. The implications of preoperative hypoalbuminemia on postoperative readmission, reoperation, and mortality among orthopaedic trauma patients: a systematic review and meta-analysis. J Clinl Orthopaedics Trauma. 2025;67:103108. doi:10.1016/j.jcot.2025.103108
11. Rahman TM, Fleifel D, Padela MT, et al. Interventions for obesity and nutritional status in arthroplasty patients. JBJS Rev. 2020;8:e0161. doi:10.2106/JBJS.RVW.19.00161
12. Fowler AJ, Ahmad T, Phull MK, Allard S, Gillies MA, Pearse RM. Meta-analysis of the association between preoperative anaemia and mortality after surgery. Br J Surg. 2015;102:1314–1324. doi:10.1002/bjs.9861
13. Rubinger DA, Cahill C, Ngo A, Gloff M, Refaai MA. Preoperative anemia management: what’s new in 2020? Curr Anesthesiol Rep. 2020;10:166–175. doi:10.1007/s40140-020-00385-7
14. Garcia-Casal MN, Dary O, Jefferds ME, Pasricha S-R. Diagnosing anemia: challenges selecting methods, addressing underlying causes, and implementing actions at the public health level. Ann NY Acad Sci. 2023;1524:37–50. doi:10.1111/nyas.14996
15. Shander A, Corwin HL, Meier J, et al. Recommendations from the international consensus conference on anemia management in surgical patients (ICCAMS). Ann Surg. 2023;277:581. doi:10.1097/SLA.0000000000005721
16. Howell K, Garvan C, Amini S, et al. Association between preoperative anemia and cognitive function in a large cohort study of older patients undergoing elective surgery. Anesthesia Analg. 2025;140:14. doi:10.1213/ANE.0000000000006998
17. Smith MJ, Liehr PR. Middle Range Theory for Nursing.
18. da SLAGP, Lopes VJ, Das MNNA. Symptom management theory applied to nursing care: scoping review. Rev Bras Enferm. 2021;74:e20201004. doi:10.1590/0034-7167-2020-1004
19. McMillan DC, Watson WS, O’Gorman P, Preston T, Scott HR, McArdle CS. Albumin concentrations are primarily determined by the body cell mass and the systemic inflammatory response in cancer patients with weight loss. Nutr Cancer. 2001;39:210–213. doi:10.1207/S15327914nc392_8
20. Kalantar-Zadeh K, Kilpatrick RD, Kuwae N, et al. Revisiting mortality predictability of serum albumin in the dialysis population: time dependency, longitudinal changes and population-attributable fraction. Nephrol Dial Transplant. 2005;20:1880–1888. doi:10.1093/ndt/gfh941
21. Liu SH, Cerri-Droz P, Loyst RA, Komatsu DE, Wang ED. Hypoalbuminemia predicts early postoperative complications following noninfectious revision total shoulder arthroplasty. Eur J Orthop Surg Traumatol. 2024;34:3129–3134. doi:10.1007/s00590-024-04041-2
22. Zhang F-Q, Yang Y-Z, Li P-F, et al. Impact of preoperative anemia on patients undergoing total joint replacement of lower extremity: a systematic review and meta-analysis. J Orthop Surg Res. 2024;19:249. doi:10.1186/s13018-024-04706-y
23. Kumar M, Hepner DL, Grawe ES, et al. Diagnosis and treatment of perioperative anemia: a society for perioperative assessment and quality improvement collaborative review. Anesthesiology. 2024;141:984–996. doi:10.1097/ALN.0000000000005111
24. Gómez-Ramirez S, Jericó C, Muñoz M. Perioperative anemia: prevalence, consequences and pathophysiology. Transfus Apheresis Sci. 2019;58:369–374. doi:10.1016/j.transci.2019.06.011
25. Lin J, Wang C, Liu J, et al. Prevalence and intervention of preoperative anemia in Chinese adults: a retrospective cross-sectional study based on national preoperative anemia database. eClinicalMedicine. 2021;36. doi:10.1016/j.eclinm.2021.100894
26. Athnaiel O, Cantillo S, Paredes S, Knezevic NN. The role of sex hormones in pain-related conditions. Int J Mol Sci. 2023;24:1866. doi:10.3390/ijms24031866
27. Keogh E. Sex and gender differences in pain: past, present, and future. PAIN. 2022;163:S108. doi:10.1097/j.pain.0000000000002738
28. Kim S-D. Twelve weeks of yoga for chronic nonspecific lower back pain: a meta-analysis. Pain Manag Nurs. 2020;21:536–542. doi:10.1016/j.pmn.2020.07.002
29. Ivascu R, Torsin LI, Hostiuc L, Nitipir C, Corneci D, Dutu M. The surgical stress response and anesthesia: a narrative review. J Clin Med. 2024;13:3017. doi:10.3390/jcm13103017
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Decrease in Hb and Hypoproteinemia: Possible Predictors of Complications in Neonates with Late-Onset Sepsis in a Developing Country
Cai N, Liao W, Chen Z, Tao M, Chen S
International Journal of General Medicine 2022, 15:6583-6589
Published Date: 13 August 2022
Application of Perioperative Nursing Based on Enhanced Recovery After Surgery (ERAS) Principles in Patients Undergoing Total Knee Arthroplasty
Huang J, Wu G, Li X
Therapeutics and Clinical Risk Management 2025, 21:829-839
Published Date: 31 May 2025