Back to Journals » Journal of Pain Research » Volume 18
Episodic Migraine Pain Curves: Real-Time Smartphone-Based Analysis and Clinical Implications
Authors Gago-Veiga AB ![]() , Gonzalez-Martinez A, Quintas S, Vieira A
, Gonzalez-Martinez A, Quintas S, Vieira A ![]() , Gálvez-Goicuría J, Sanz-García A, Ayala JL
, Gálvez-Goicuría J, Sanz-García A, Ayala JL ![]() , Sobrado M, Vivancos J, Pagan J
, Sobrado M, Vivancos J, Pagan J ![]()
Received 27 July 2025
Accepted for publication 22 October 2025
Published 11 December 2025 Volume 2025:18 Pages 6711—6722
DOI https://doi.org/10.2147/JPR.S550684
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rune Häckert Christensen
Ana Beatriz Gago-Veiga,1 Alicia Gonzalez-Martinez,1 Sonia Quintas,1 Alba Vieira,1 Javier Gálvez-Goicuría,2,3 Ancor Sanz-García,4 Jose L Ayala,5,6 Monica Sobrado,1 Jose Vivancos,1 Josué Pagan3,6
1Neurology Department, Hospital Universitario de La Princesa & Instituto de Investigación Sanitaria Princesa (IIS-Princesa), Madrid, Spain; 2Brainguard SL, Pozuelo de Alarcón, Spain; 3Electronic Engineering Department, Universidad Politécnica de Madrid, Madrid, Spain; 4Unidad de Análisis de datos, Instituto de Investigación Sanitaria (IIS-Princesa), Hospital Universitario de la Princesa, Madrid, Spain; 5Computer Architecture and Automation Department, Universidad Complutense de Madrid, Madrid, Spain; 6CCS: Center for Computational Simulation, Universidad Politécnica de Madrid, Madrid, Spain
Correspondence: Ana Beatriz Gago-Veiga, Hospital Universitario de la Princesa, Headache Unit, Neurology Department, Hospital Universitario La Princesa, Calle Diego de León, 62, Madrid, 28006, Spain, Email [email protected]
Purpose: Migraine involves a wide range of symptoms, with pain being one of the most prominent and disabling. While the ICHD-3 provides a well-established classification framework, exploring pain dynamics such as onset, duration, and intensity may offer additional insights to support the development of more personalized treatment strategies.
Patients and Methods: A previous study categorized episodic migraine patients based on pain curve dynamics (onset, duration, and intensity). This study analyzes socio-demographic and clinical characteristics across the previously identified subgroups. Patients met ICHD-3 criteria and used a smartphone app for real-time data collection on migraine parameters, including onset, pain duration and intensity, symptoms, triggers, and treatment responses. The aim was to identify differences across subgroups in these variables.
Results: The study included 51 participants, mostly women, with a mean age of 39.1 years. Four distinct migraine patterns emerged based on pain dynamics: Type 1 (High intensity), Type 2 (Acute onset and intense), Type 3 (Prolonged and intense), and Type 4 (Low intensity). Significant associations were found between curve types and demographic factors such as sex, aura presence, and cardiovascular risk. Although food-related triggers were common across groups, their distribution did not significantly differ. However, prolonged migraines posed unique challenges regarding treatment timing and effectiveness.
Conclusion: Pain curve-based classification reveals clinically relevant migraine subtypes. Significant differences were observed across curve types in sex distribution, aura prevalence, associated symptoms such as nausea and phonophobia, and treatment response profiles. This approach, supported by real-time data, may advance personalized migraine management.
Plain Language Summary: Migraine is a disabling condition that affects millions of people worldwide, causing intense headaches and other symptoms such as nausea or sensitivity to light. Each person experiences migraines differently, and not all migraine attacks are the same. Understanding these differences is key to providing better, more personalized care.
In this study, patients used a smartphone application to record their migraine attacks in real time. The app captured how quickly pain started, how long it lasted, how intense it was, and what treatments were used.
From these recordings, we identified four main patterns of migraine pain:
Type 1 (High intensity), Type 2 (Acute onset and intense), Type 3 (Prolonged and intense), and Type 4 (Low intensity). Each type showed different clinical features. For example, prolonged migraines were more often linked to additional symptoms like nausea and tended to respond more slowly to treatment.
These findings suggest that classifying migraine attacks by the way pain develops could help doctors adapt treatment strategies to each patient’s typical migraine pattern. This research shows how digital tools can bring us closer to truly personalized migraine care.
Keywords: migraine disorders, pain measurement, cluster analysis, mobile applications, treatment outcome
A Letter to the Editor has been published for this article.
A Response to Letter by Drs Zhang has been published for this article.
Introduction
Migraine is a prevalent neurological condition affecting approximately 15% of the population worldwide, manifesting with recurrent episodes of throbbing headaches often accompanied by nausea, vomiting, and increased sensitivity to light and sound, significantly affecting quality of life.1,2 Recent comprehensive reviews have further highlighted current advances in migraine pathophysiology, diagnosis, and management.3
The International Classification of Headache Disorders, 3rd edition [ICHD-3], comprehensively categorizes migraine into episodic and chronic forms, with further subtypes based on the presence of aura and other specific features.1,4 Episodic migraine with up to 15 headache days per month and chronic migraine, which is defined by 15 or more headache days per month of which at least 8 have migraine features.1,5 Additionally, complications of migraine include vascular risk complications such as infarction, which have been described and might be associated with demographic characteristics such as sex and obesity.6–8 This detailed classification system not only aids in precise diagnosis but also informs targeted treatment approaches tailored to each migraine type’s unique set of symptoms and characteristics. However, steps forward are being made towards a better understanding of the pain phase of migraine, which may also have therapeutic implications.9,10 Despite these classifications, there remains an unmet need to understand dynamic pain patterns in patient stratification to enhance personalized treatment approaches.11 From a pathophysiological perspective, migraine has been associated with central and peripheral sensitization, cortical hyperexcitability, and thalamo-cortical dysrhythmia, mechanisms that contribute to pain amplification and the complexity of clinical manifestations. These processes also explain the widespread burden of disease and disability associated with migraine, as demonstrated by studies on pressure pain sensitivity in both episodic and chronic patients.12,13 Incorporating these mechanisms into clinical research provides a stronger framework to interpret patient subgroups and to advance toward precision management strategies.While significant progress has been made in identifying the clinical characteristics of migraine attacks, the classification of patients based on both clinical features and pain curve dynamics has not been thoroughly explored.14 Such studies could potentially lead to a biometric classification of migraines. However, the classification of patients into distinct groups based on these features remains an open question. The variability in clinical presentation suggests the existence of patient subtypes that might correlate with pain curve characteristics.15
Recent technological advancements have provided tools to capture the dynamic nature of migraine pain through smartphone applications. These applications allow for real-time tracking of pain intensity and associated symptoms, representing a significant advancement toward personalized migraine management.16–18 They meticulously record the intensity and duration of pain, as well as accompanying symptoms such as nausea, vomiting, and sensitivity to light and sound. These developments pave the way for a better understanding of migraine subtypes based on pain curve characteristics.This study aims to build on these technological advancements to address the gap in migraine classification by considering pain curve dynamics alongside clinical features. Our objective is to categorize episodic migraine patients into distinct subtypes, reflecting the observed heterogeneity in clinical presentations. The real-time data from these analyses may reveal patient subgroups with unique pain trajectories and treatment responses, facilitating a more nuanced understanding of migraine and paving the way for tailored therapeutic strategies.
Materials and Methods
In this prospective study, we aim to analyze the relationship between the socio-demographic and clinical characteristics of the episodic migraine patients and the pain curve classification developed in a previous study.10
Patient Enrollment and Data Collection
Patients were selected by a neurologist specialized in Headache based on a confirmed diagnosis of episodic migraine as per the International Classification of Headache Disorders, 3rd edition [ICHD-3] criteria1 and no changes were made to their symptomatic or preventive medication regimen during their participation in the study. A complete clinical evaluation was conducted for each patient to ensure compliance with the ICHD-3 criteria. Also, trigger factors were recorded prospectively in real time through the smartphone application, directly marked by the patients in each attack. All triggers, including “food”, were reported globally based on patients’ subjective perception in real time, without further subcategorization. Patients were consecutively recruited at the Headache Unit of Hospital Universitario de La Princesa over a two-year period. Each participant was followed prospectively for approximately 4–6 weeks, during which all migraine attacks were recorded in real time through the smartphone application.
For the present analysis, pain intensity was the primary feature considered. Data on onset, duration, and pain intensity were collected prospectively and in real time through a dedicated smartphone application, with patients entering the information at the moment of each migraine attack.
Upon recruitment, participants were involved in a prospective study that utilized a specially designed smartphone application. This application was instrumental in gathering real-time data, allowing patients to log various aspects of their migraine episodes, such as onset time, duration, intensity, and treatment as they occurred.19 A prior study captured a wide array of data points that are crucial for analyzing the pain curves, including the onset, peak, and cessation of pain.19 The recorded data was analyzed using K-means clustering to identify four distinct groups of migraine pain curves. To account for the sensitivity of the K-means algorithm to centroid initialization, we employed a robust procedure to ensure the stability of our results. The clustering was performed using the K-means++ algorithm for centroid initialization, which strategically selects initial cluster centers to improve the quality and consistency of the clustering. Furthermore, the algorithm was run 10 times with different random centroid seeds. The final cluster solution reported is the one with the lowest within-cluster sum of squares (WCSS), ensuring that our results represent a stable and optimal partitioning of the data.
A logistic model tree classification was trained afterwards to develop a classification model.10
Statistical Analysis
Statistical analyses were performed to compare baseline characteristics, migraine features, triggers, and treatment responses across the four identified pain curve groups. For continuous variables, which are presented as mean (standard deviation), group comparisons were conducted using a one-way Analysis of Variance (ANOVA). For categorical variables, presented as counts (percentages), comparisons were made using the Chi-square (χ2) test. A p-value of < 0.05 was considered statistically significant.
Assumptions of normality and homogeneity of variances for ANOVA were assessed using the Shapiro–Wilk and Levene’s tests, respectively. For Chi-squared tests, expected cell counts were verified to ensure validity. Given that multiple attacks could derive from the same participant, we also performed sensitivity analyses with mixed-effects ANOVAs, which confirmed the robustness of the main findings. All statistical analyses were performed using Python (SciPy library, version 1.10.0).
Data were analyzed on a complete-case basis for each variable. Due to the low percentage of missing data, no imputation methods were used. This approach ensures that the analyses are based only on observed data, avoiding the introduction of artificial data and the assumptions that imputation methods require.
Ethics Approval and Consent to Participate
The study was approved by Hospital de la Princesa’s Ethics Committee (register number: PI-879). All patients signed informed consent forms prior to inclusion in the study. Patient data were anonymized for data analysis. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Results
The study included 51 patients, predominantly women (90.2%). The demographic characteristics are included in Table 1.
 |
Table 1 Characteristics of the Sample |
The average age of participants was 39.1 years, with a diverse age range from 21 to 64 years. A considerable proportion of the sample had an early onset of migraines, averaging at 14.6 years old, indicating the chronic nature of the condition. A significant history of headaches was present in 72% of the sample. Notably, 21.6% of the participants experienced migraines with aura. Regarding cardiovascular risk factors, 40% of the participants had at least one, with hypertension being the most common (6%). Diabetes Mellitus and Dyslipidemia were less prevalent, found in 2% and 12% of the sample, respectively. Lifestyle factors such as smoking were reported in 16% of the sample. The study also considered the participants’ body mass index (BMI), with an average BMI of 24.7, which is within the normal weight range, and cognitive reserve evaluation scores, which averaged at 16.2. Educational levels varied, with 74% having undergone secondary studies. Finally, a significant portion of the sample (72%) was on preventive migraine treatment.
The cluster analysis was performed on a total of 344 migraine attacks recorded by these 51 patients. The analysis identified four distinct and clinically relevant clusters based on their pain curve dynamics. The distribution of the attacks was as follows: i) High Intensity (Type 1): 118 attacks (34.3%); ii) Acute Onset and intense (Type 2): 107 attacks (31.1%); iii) Prolonged and intense (Type 3): 33 attacks (9.6%); iv) Low Intensity (Type 4): 86 attacks (25.0%) (Figure 1). The distribution of episodes across these types was fairly balanced, with most episodes falling into the high intensity and acute onset and intense categories. The characteristics of migraine attacks, including symptoms and triggers, varied depending on the pain curve classification.
 |
Figure 1 Classification of four distinct migraine groups based on the dynamics of their pain curves. Type 1 = High intensity; Type 2 = Acute onset and intense; Type 3 = Prolonged and intense; Type 4 = Low intensity. Modified from Galvez-Goicuria et al 2022.10 |
Regarding demographic characteristics, sex distribution across the different pain curve types showed significant differences (p=0.010), with a higher percentage of women in the high intensity and prolonged categories, and a higher percentage of men in the low intensity category. There were no significant differences in age and age of onset across the pain curve types, indicating that these demographic factors may not be predictive of the pain curve category. The presence of migraine with aura varied significantly among the pain curve types, with a notably lower percentage in the low intensity category compared to the high intensity one, suggesting a potential link between pain intensity and aura (p=0.004).
In terms of cardiovascular risk factors, hypertension was more common in the high intensity and prolonged categories compared to low intensity (p=0.010). Regarding lifestyle factors, BMI showed significant variation across groups, with the prolonged and intense pain curve category having a higher average BMI (p=0.030).
The migraine pain curve types were also significantly associated with differences in cognitive reserve (p=0.010), and educational levels, where a higher percentage of individuals with university studies were found in the acute onset and prolonged categories (p=0.004). Lastly, preventive treatment was most used among those in the prolonged pain curve category (p=0.001) (Table 2).
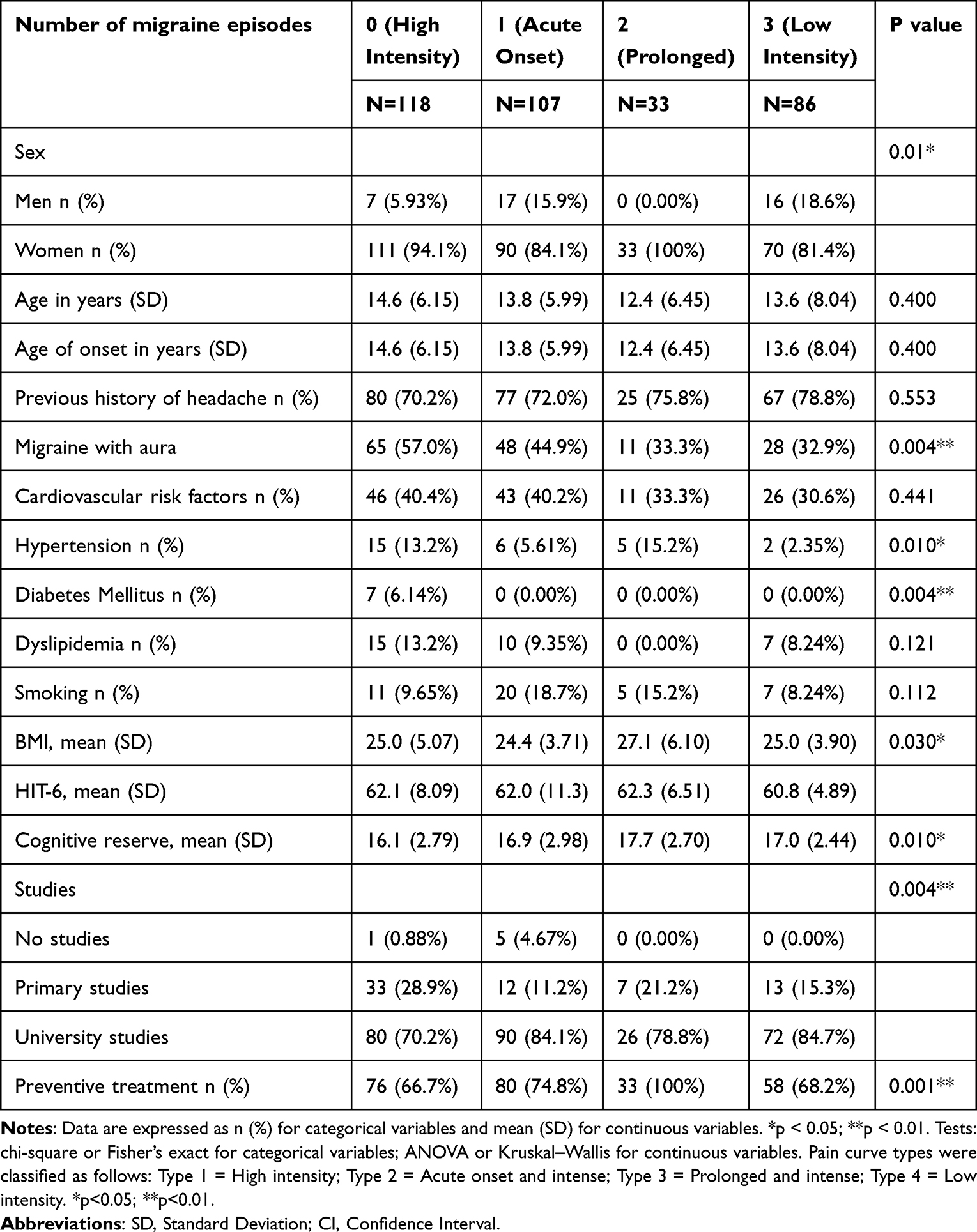 |
Table 2 Baseline Characteristics Regarding the Migraine Curve |
The analysis of migraine characteristics across four types of pain curves (high intensity, onset and intense, prolonged and intense, and low intensity) showed significant variation in symptom presentation (Table 3). Pain intensity, measured by the Visual Analog Scale (VAS), varied significantly across the types, with the high intensity and prolonged and intense groups reporting severe pain, while the low intensity group had notably milder pain (p<0.001). Nausea was more prevalent in the prolonged and intense type group (81.8%), suggesting a correlation between longer-lasting migraines and gastrointestinal symptoms (p<0.001). The occurrence of vomiting, photophobia, and phonophobia did not show significant differences across the pain types, indicating that these symptoms are common migraine accompaniments regardless of the pain curve type. Regarding osmophobia (sensitivity to odors) and the number of simultaneous symptoms experienced during a migraine episode were significantly different among the groups. The prolonged and intense pain type group reported the highest number of simultaneous symptoms, suggesting a more complex clinical picture (p<0.030 and p<0.001, respectively).
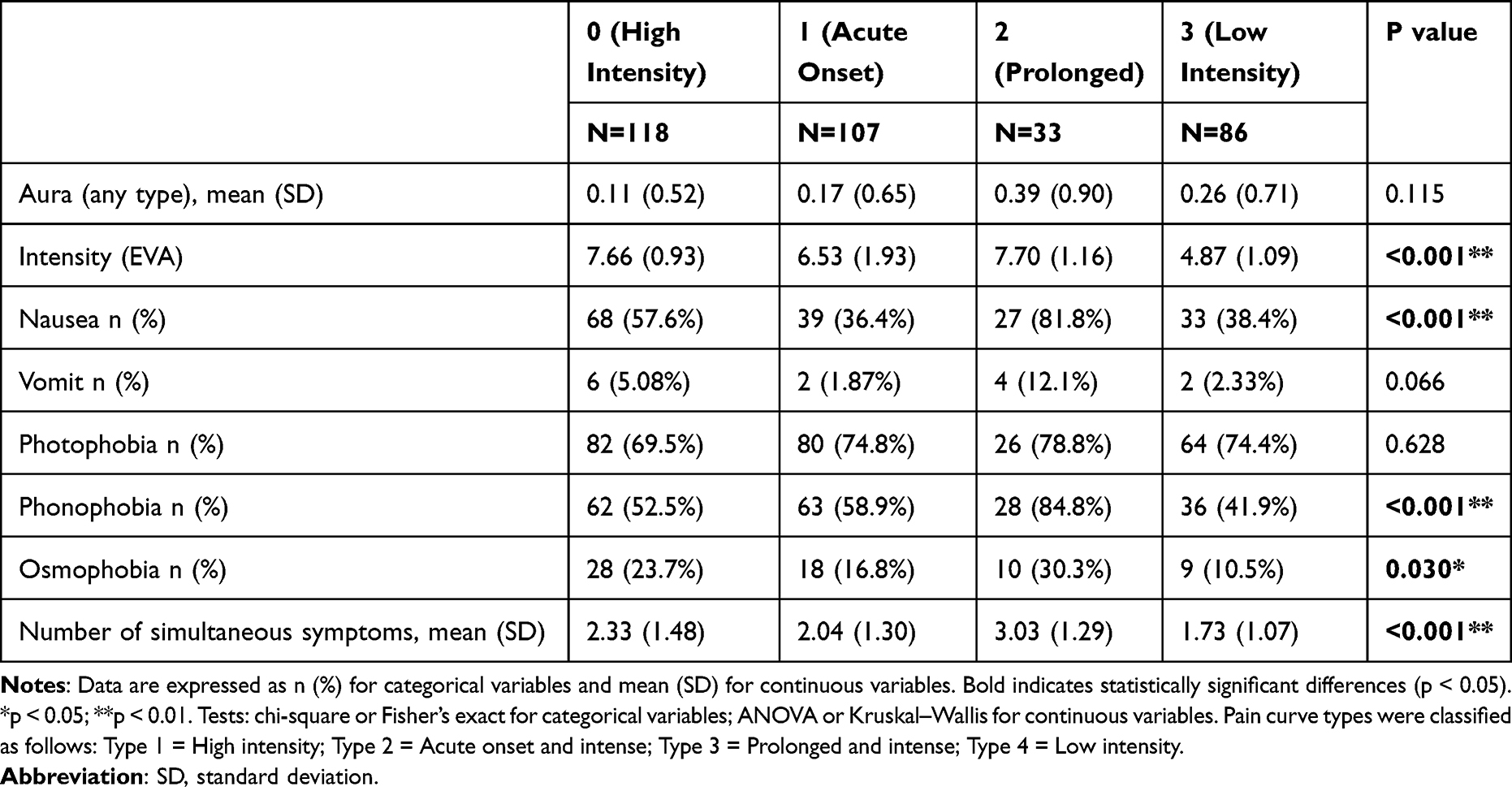 |
Table 3 Migraine Characteristics Regarding the Migraine Curve |
Regarding the relationship between migraine triggers and the four classified migraine pain curve types: 1 (High intensity), 2 (Acute onset and intense), 3 (Prolonged and intense), 4 (Low intensity): we found that food was reported as a trigger in a high proportion of migraine episodes across all pain curve types, with the highest frequency in the high intensity group (92.4%). However, differences in food as a trigger were not statistically significant among the different pain curve types. Triggers related to drinks, stress, sleep, and weather were also reported among the different pain curve types but did not show a significant variation, indicating these triggers are common across various migraine experiences (Table 4). Exercise or sports as triggers had a low occurrence rate and did not vary significantly between the pain curve types.
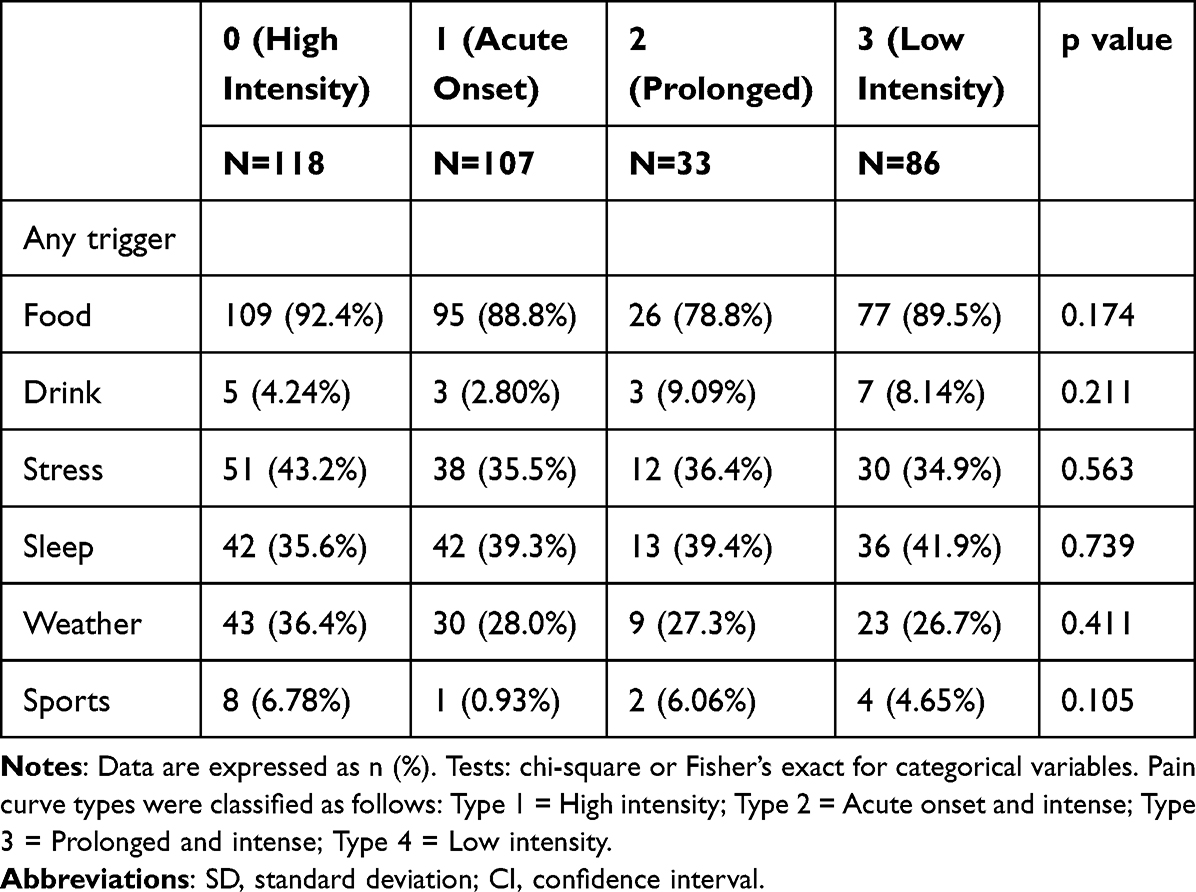 |
Table 4 Migraine Triggers Regarding the Migraine Curve |
Regarding treatment responses across different migraine pain curve types, a notable portion of participants in each pain curve category had received some form of treatment, with the highest treatment application observed in the high intensity group (88.1%). There was a significant difference in treatment application across the pain curve types (p=0.006), suggesting varying treatment needs or effectiveness. The use of nonsteroidal anti-inflammatory drugs (NSAIDs) was common across all groups but did not differ significantly between them. Triptans were more frequently used in the high intensity group (61.9%), significantly more than in the low intensity group (p<0.001). There was a significant difference in the reported duration of migraines, with the prolonged and intense pain type having a markedly longer duration (p<0.001). The time from treatment to the peak of pain intensity varied significantly among the groups (p<0.001), with the prolonged and intense type experiencing a longer delay to maximum pain intensity. Similarly, the time from treatment to resolution of pain also showed significant variation, with prolonged and intense migraines having the longest duration (p<0.001).
Discussion
Following this research, migraine attacks can be classified into four distinct types based on pain dynamics: type 1 [high intensity], type 2 [acute onset and intense], type 3 [prolonged and intense], and type 4 [low intensity],10 with these classifications being closely related to patient characteristics. The current analysis demonstrates that variables such as sex, aura presence, and specific cardiovascular and lifestyle factors are significantly associated with particular pain curve types,15,20 underscoring the phenotypic heterogeneity of migraine. Moreover, the significant difference in aura prevalence across pain curve types suggests a possible pathophysiological link between aura mechanisms and pain intensity. Cortical spreading depression, which underlies migraine aura, has been associated with enhanced trigeminovascular activation and altered pain modulation, potentially explaining the higher frequency of aura in more intense pain curves. Clinically, this association highlights that patients experiencing aura may be more prone to severe attacks, which could influence both acute treatment selection and preventive strategies. In addition, the significant differences in nausea and phonophobia across pain curve types, particularly their higher prevalence in prolonged attacks, suggest that longer migraine episodes may represent a more complex clinical phenotype. This phenotype may be characterized not only by extended pain duration but also by a greater burden of associated symptoms, reflecting enhanced central sensitization. Clinically, these findings highlight the importance of early and aggressive management in prolonged attacks, as patients experiencing this phenotype may require combined or targeted therapeutic strategies. Furthermore, patients with prolonged pain episodes were more likely to receive preventive treatment, reflecting the increased clinical burden and complexity associated with these migraine profiles.
Taken together, the study population consisted exclusively of individuals with episodic migraine, ensuring adequate characterization and differentiation of discrete migraine events. Despite the episodic nature, the high rates of both acute and preventive treatment use emphasize the substantial impact of migraine on functional status and quality of life.21–23 In addition, the mean HIT-6 score of approximately 61 indicates a severe impact of migraine on daily functioning in this cohort. Clinically, this reflects the considerable burden of disease even among patients with episodic migraine, underscoring the importance of effective and individualized management strategies. These findings therefore contribute to the growing body of evidence supporting the relevance of pain trajectory as a clinically meaningful dimension in migraine, with implications for stratified management approaches.
Regarding migraine characteristics, while some symptoms are common across all types of migraine pain curves, the intensity of pain, presence of nausea, and number of simultaneous symptoms experienced can be significantly associated with specific pain curve categories. Consequently, these findings could profoundly impact tailoring treatment strategies to patient experiences, potentially revolutionizing migraine management.9 Similarly, triggers such as food were consistently reported across pain types, suggesting that their impact is uniform. This suggests that the impact of these triggers does not vary with the pain curve classification, a fact that may streamline the identification of migraine precipitants across subtypes. However, healthy lifestyle choices such as exercise, good sleep, adequate stress management, and eating often may prevent triggers and therefore transformation to chronic migraine over time.24–26 Importantly, all triggers were recorded based on patients’ subjective perception in real time through the smartphone application. While this method minimizes recall bias and reflects ecological validity, it also entails limitations, as the absence of predefined subcategories (eg, for food) may reduce the precision and clinical applicability of the trigger data.
In terms of treatment, triptan use was predominantly noted in the high-intensity group, linking this treatment to the management of severe pain. This observation aligns with the therapeutic use of triptans, which are often reserved for acute and severe migraine episodes, and its early intake is recommended in these situations.27,28 Moreover, the variability in treatment response across pain curve types, especially the management challenges presented by prolonged and intense migraines, highlights the potential for optimizing therapeutic approaches.27–29 The pronounced delay in symptom resolution in prolonged and intense migraines represents a striking clinical observation, underscoring the complexity of this phenotype and the need for more personalized and aggressive treatment strategies.
Therefore, the classification of migraine patients based on pain curve dynamics introduces a personalized approach to understanding and managing migraines.10 Distinct patient groups may benefit from targeted therapies, suggesting the need for a more nuanced approach to treatment protocols.30 The study’s findings also align with recent advancements in migraine research and highlight the potential application to better select treatment regarding the pain curve characteristics.
Moreover, clinical implications may vary depending on the type of pain curve. For instance, targeted anti-emetic use could be prioritized in prolonged and intense attacks, while early administration of fast-acting nasal or injectable formulations may be particularly beneficial in acute onset and intense episodes. Similarly, mini-prophylaxis or long-acting strategies might be more suitable for patients with recurrent prolonged attacks. Future pilot clinical trials should be designed to test these tailored approaches, integrating pain curve classification as a stratification tool. In addition, novel acute treatments such as gepants (CGRP receptor antagonists) may play a key role in pain curve–based stratification. Their efficacy in both acute and preventive settings, along with good tolerability and lack of vasoconstrictive effects,31 suggests that patients with prolonged or high-intensity attacks—who showed delayed response and greater symptom burden in our cohort—might particularly benefit from these agents.
Strengths and Limitations
Despite the informative findings of this study, several limitations must be considered. First, the study sample size was relatively modest, which may affect the statistical power of the analyses and limit the generalizability of the results to all episodic migraine sufferers. A larger sample size would be beneficial for future studies to validate our classification system and to explore the nuances between different subtypes further. However, it is one of the biggest sample sizes in the literature with a proper methodological design. Although clinical data research poses significant challenges, especially in the context of real-time data collection, the present study provides a suitable and reliable dataset of migraine triggers and pain curve characteristics that would contribute to the current knowledge of pain curves in migraine.32,33 Second, the reliance on self-reported data through a smartphone application may introduce a degree of reporting bias. Participants’ subjective interpretations of pain and symptoms could influence the recorded data, potentially affecting the accuracy of the pain curve categorizations. However, this was prevented by a careful design of the pain curve evaluation.10 A limitation of our study is the absence of an a priori power calculation, which is often challenging in exploratory studies where effect sizes are not known in advance. The data-driven nature of our clustering approach resulted in subgroups of varying sizes, with the “prolonged” cluster being the smallest (n=33 episodes). While our study successfully identified several highly significant differences between the groups (p < 0.001), we must interpret non-significant findings with caution. It is possible that our analysis was underpowered to detect more subtle differences for some variables. For instance, in Table 5, the difference in paracetamol use approached statistical significance (p=0.086) and might have become significant with a larger sample in the “prolonged” group. Future, larger-scale studies would be beneficial to confirm our findings and to provide greater statistical power to explore more nuanced distinctions between these pain curve phenotypes. Finally, patients with chronic migraine were not included to adequately evaluate the start and end of a migraine crisis. Future studies will address these limitations. Continued exploration in larger, more diverse populations, with a multifaceted approach to data collection and analysis, will be critical in advancing our understanding of migraine pain curves and in developing personalized migraine management protocols.
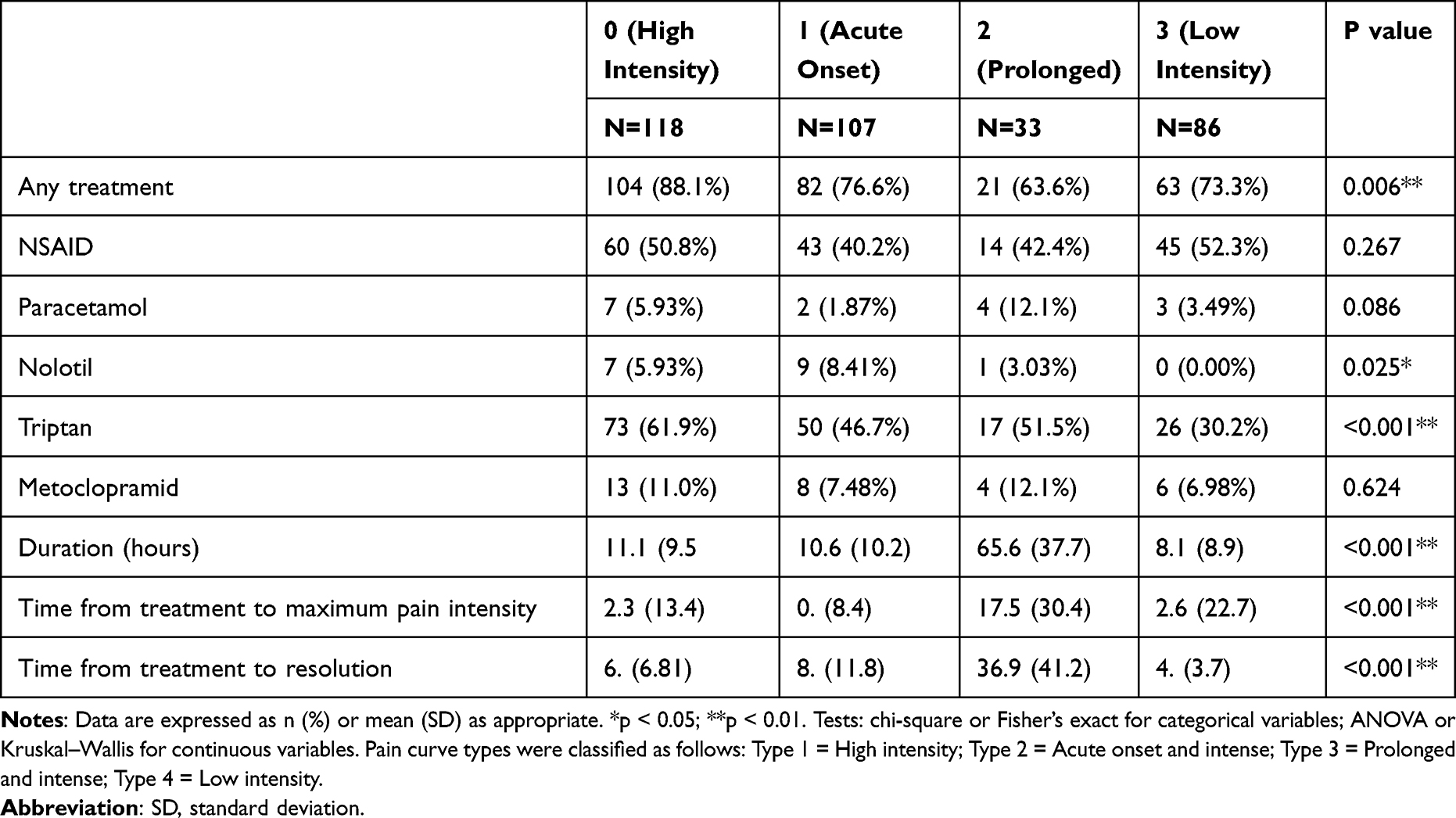 |
Table 5 Treatment Response Regarding the Type of Curve |
Conclusion
In conclusion, the novel classification of migraine patients based on pain curve dynamics outlined in this study exemplifies the shift toward personalized management strategies in migraine care. Through the application of real-time data capture and sophisticated analytical techniques, we have unveiled a spectrum of migraine experiences. This approach not only aligns with the contemporary direction of migraine research but also sets the stage for the development of more nuanced and effective treatment regimens tailored to the individual pain profiles of migraine sufferers.
Abbreviation
APP, Application; BMI, Body Mass Index; CCS, Center for Computational Simulation; ICHD-3, International Classification of Headache Disorders, 3rd edition; NSAIDs, Nonsteroidal Anti-Inflammatory Drugs; VAS, Visual Analog Scale.
Acknowledgments
We thank the patients and researchers for their dedication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Instituto de Salud Carlos III (ISCIII), through IMPaCT project PMP22/00158, and co-funded by the European Union through the Recovery, Transformation and Resilience Plan – Next Generation EU to A.B.G.V, A.G.M, S.Q and J.V. Research by J.G.G. was founded by the Consejería de Educación e Investigación under grant IND2019/BMD-17276.
Disclosure
This work was partially presented as a poster at the 16th European Headache Congress (Vienna, December 7–10, 2022), where it received an award as one of the best poster. ABG-V has received speaker honoraria and/or served as a clinical advisor for Novartis, Lilly, TEVA, Exeltis, Chiesi, Abbvie, Pfizer, Dr. Reddy’s, and Lundbeck. She is the coordinator and principal investigator of a research IMPaCT project, grant number PMP22/00158. A.G.M. has received speaker honoraria from TEVA, Lilly, and Altermedica. S.Q. has received honoraria from Lilly, Novartis, Exeltis, UCB Pharma, Bial, and Altermedica. The remaining authors declare no conflicts of interest.
References
1. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202.
2. Burch RC, Buse DC, Lipton RB. Migraine: epidemiology, burden, and comorbidity. Neurol Clin. 2019;37(4):631–649. doi:10.1016/j.ncl.2019.06.001
3. Raggi A, Leonardi M, Arruda M, et al. Hallmarks of primary headache: part 1 – migraine. J Headache Pain. 2024;25(1):189. doi:10.1186/s10194-024-01889-x
4. Ruscheweyh R, Müller M, Blum B, Straube A. Correlation of headache frequency and psychosocial impairment in migraine: a cross-sectional study. Headache. 2014;54(5):861–871. doi:10.1111/head.12362
5. Kung D, Rodriguez G, Evans R. Chronic migraine: diagnosis and management. Neurol Clin. 2023;41(1):141–159. doi:10.1016/j.ncl.2022.05.005
6. Chiang CC, Chen SP. Migrainous infarction. Handb Clin Neurol. 2024;199:465–474. doi:10.1016/B978-0-12-823357-3.00021-5
7. Bigal ME, Kurth T, Hu H, Santanello N, Lipton RB. Migraine and cardiovascular disease: possible mechanisms of interaction. Neurology. 2009;72(21):1864–1871. doi:10.1212/WNL.0b013e3181a71220
8. Dodick DW. Review of comorbidities and risk factors for the development of migraine complications (infarct and chronic migraine). Cephalalgia. 2009;29 Suppl 3:7–14. doi:10.1111/j.1468-2982.2009.01847.x
9. Juhasz G, Gecse K, Baksa D. Towards precision medicine in migraine: recent therapeutic advances and potential biomarkers to understand heterogeneity and treatment response. Pharmacol Ther. 2023;250:108523. doi:10.1016/j.pharmthera.2023.108523
10. Galvez-Goicuria J, Pagan J, Gago-Veiga AB, Moya JM, Ayala JL. Cluster-then-classify methodology for the identification of pain episodes in chronic diseases. IEEE J Biomed Health Inform. 2021. doi:10.1109/JBHI.2021.3056360
11. Karsan N, Goadsby PJ. Migraine: beyond pain. Pract Neurol. 2021;21(6):475–480. doi:10.1136/practneurol-2021-003018
12. Palacios-Ceña D, Neira-Martín B, Silva-Hernández L, et al. Women with chronic and episodic migraine exhibit similar widespread pressure pain sensitivity. Pain Med. 2016;17(11):2127–2133. doi:10.1093/pm/pnw056
13. Deodato M, Rinaldi F, Cocco L, et al. Pressure pain threshold and widespread pressure pain hypersensitivity in episodic and chronic migraine. Neurol Sci. 2024;45(5):1509–1518. doi:10.1007/s10072-024-07372-4
14. Viana M, Sances G, Linde M, et al. Clinical features of migraine aura: results from a prospective diary-aided study. Cephalalgia. 2017;37(10):979–989. doi:10.1177/0333102417706350
15. Stewart WF, Shechter A, Lipton RB. Migraine heterogeneity: disability, pain intensity, and attack frequency and duration. Neurology. 1994;44(6 Suppl 4):S24–39. doi:10.1212/WNL.44.6_Suppl_4.S24
16. Stubberud A, Ingvaldsen SH, Brenner E, et al. Forecasting migraine with machine learning based on mobile phone diary and wearable data. Cephalalgia. 2023;43(5):3331024231169244. doi:10.1177/0333102423116924
17. Casanova A, Vives-Mestres M, Donoghue S, Mian A, Martin PR. An observational study of self-reported migraine triggers and prospective evaluation of the relationships with occurrence of attacks enabled by a smartphone application (App). Headache. 2022;62(10):1406–1415. doi:10.1111/head.14397
18. Chiang CC, Fang X, Horvath Z, et al. Simultaneous comparisons of 25 acute migraine medications based on 10 million users’ self-reported records from a smartphone application. Neurology. 2023;101(24):e2560–70. doi:10.1212/WNL.0000000000209683
19. Pagán J, De Orbe MI, Gago A, et al. Robust and accurate modeling approaches for migraine per-patient prediction from ambulatory data. Sensors. 2015;15(7):15419–15442. doi:10.3390/s150715419
20. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: epidemiology, mechanisms, and implications. Headache. 2010;50(4):631–648. doi:10.1111/j.1526-4610.2009.01555.x
21. Lipton RB, Bigal ME, Diamond M, et al. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007;68(5):343–349. doi:10.1212/01.wnl.0000252808.97649.21
22. GBD 2016 Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2018;17(11):954–976. doi:10.1016/S1474-4422(18)30322-3.
23. Lipton RB, Silberstein SD. Episodic and chronic migraine headache: breaking down barriers to optimal treatment and prevention. Headache. 2015;55 Suppl 2:103–122. doi:10.1111/head.12525
24. Bigal ME, Lipton RB. Migraine chronification. Curr Neurol Neurosci Rep. 2011;11(2):139–148. doi:10.1007/s11910-010-0157-z
25. Torres-Ferrús M, Ursitti F, Alpuente A, et al. From transformation to chronification of migraine: pathophysiological and clinical aspects. J Headache Pain. 2020;21(1):42. doi:10.1186/s10194-020-01189-0
26. Agbetou M, Adoukonou T. Lifestyle modifications for migraine management. Front Neurol. 2022;13:719467. doi:10.3389/fneur.2022.719467
27. Cameron C, Kelly S, Hsieh SC, et al. Triptans in the acute treatment of migraine: a systematic review and network meta-analysis. Headache. 2015;55 Suppl 4:221–235. doi:10.1111/head.12657
28. Sacco S, Lampl C, Amin FM, et al. European Headache Federation (EHF) consensus on the definition of effective treatment of a migraine attack and of triptan failure. J Headache Pain. 2022;23(1):133. doi:10.1186/s10194-022-01495-7
29. Saracco MG, Allais G, Tullo V, et al. Efficacy of frovatriptan and other triptans in the treatment of acute migraine of normal weight and obese subjects: a review of randomized studies. Neurol Sci. 2014;35 Suppl 1:115–119. doi:10.1007/s10072-014-1771-5
30. Pagán J, Risco-Martín JL, Moya JM, Ayala JL. Modeling methodology for the accurate and prompt prediction of symptomatic events in chronic diseases. J Biomed Inform. 2016;62:136–147. doi:10.1016/j.jbi.2016.07.004
31. Pellesi L, Jedie B, Barhum F, Al-Abdullah S, Martelletti P, Xiao Z. Head-to-head relief: ubrogepant, rimegepant, and zavegepant in migraine treatment. Pain Manag. 2025;15(5):279–284. doi:10.1080/17581869.2025.2494494
32. Ashina M, Terwindt GM, Al-Karagholi MAM, et al. Migraine: disease characterisation, biomarkers, and precision medicine. Lancet. 2021;397(10283):1496–1504. doi:10.1016/S0140-6736(20)32162-0
33. Hoffmann J, Recober A. Migraine and triggers: post hoc ergo propter hoc? Curr Pain Headache Rep. 2013;17(10):370. doi:10.1007/s11916-013-0370-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.