")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Epidemiology of Diabetic Kidney Disease among US Veterans
Authors Kim K , Crook J , Lu CC, Nyman H, Abdelaziz A, LaFleur J
Received 6 December 2023
Accepted for publication 15 February 2024
Published 8 April 2024 Volume 2024:17 Pages 1585—1596
DOI https://doi.org/10.2147/DMSO.S450370
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Kibum Kim,1– 3 Jacob Crook,3,4 Chao-Chin Lu,3 Heather Nyman,2 Abdullah Abdelaziz,1 Joanne LaFleur2,3
1Department of Pharmacy Systems, Outcomes and Policy, University of Illinois Chicago, Chicago, IL, USA; 2Department of Pharmacotherapy, University of Utah, Salt Lake City, UT, USA; 3VA Salt Lake City Health Care System, Salt Lake City, UT, USA; 4Division of Epidemiology, University of Utah, Salt Lake City, UT, USA
Correspondence: Kibum Kim, Department of Pharmacy Systems, Outcomes and Policy, University of Illinois Chicago, 833 S. Wood Street | Rm 256 PHARM, MC 871, Chicago, IL, 60616, USA, Tel +1 (312) 413-0152, Email [email protected]
Rationale: With a large number of patients and high mortality, diabetic kidney disease (DKD) imposes a significant burden on US health care. Although diabetes is the leading cause of chronic kidney disease and complications, the epidemiology of DKD in the contemporary US veteran population is generally unknown.
Objective: We aimed to estimate the rate of DKD progression and to measure the general epidemiology of DKD in the United States veteran population.
Study Design: We performed a retrospective observational research using electronic health-care records and administrative databases.
Setting: The DKD patient cohort was abstracted from the Veterans Health Administration health-record data from January 2016 to March 2022.
Participants: We defined DKD patients using the laboratory test data based on Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guidelines.
Analytic Approach: Summary statistics include the five-year cumulative incidence of progression to an advanced stage from the DKD stage at the cohort entry date and prevalence at a series of single time points.
Results: A total of 685,288 patients (male [96%], mean age 62 years, Caucasian [64%], non-Hispanic [87%]) met our eligibility criteria. The 5-year cumulative incidence of progression to an advanced DKD stage or all-cause death from DKD stages G1 A2/A3, G2 A2/A3, G3a, and G3b were 52.0%, 47.4%, 50.5%, and 60.9%, respectively. In sum, 594,082 patients were classified as moderate or high risk as per KDIGO guidelines in 2021, and stages G3a and G3b accounted for 51.2% and 25.3%, respectively, of cases.
Conclusion: More than half of DKD patients underwent a stage progression or death within 5 years. A substantial number of DKD patients at an earlier stage might be left undetermined. The study findings warrant a revision of DKD patient identification and management in US veterans.
Keywords: diabetic kidney disease, prevalence, US veterans
Introduction
Chronic kidney disease (CKD) is a major public health problem. It affects approximately one in seven US adults, with an estimated count of 37 million.1 A recent simulation predicted that CKD prevalence in US adults will increase to 16.7% by 2030.2 CKD is characterized by reduced glomerular filtration rate (GFR), typically accompanied by elevated urine albumin and protein excretion. CKD typically presents with other chronic conditions, causing annual per-person medical care spending to exceed US$23,000 in 2020. The cost of CKD patient care is more than double the expenses of those without CKD, imposing a significant burden on the US health-care system.1,3 Besides the economic burden, the adverse symptoms associated with CKD progression, including weight gain, swelling, frequent urination, and anemia, impact patients’ daily lives and diminish their quality of life (QoL).4
Diabetes is the leading cause of CKD, with one in three adults with diabetes developing CKD, meaning that diabetic kidney disease (DKD) accounts for 44% of new CKD cases.1,5 Suboptimal glycemic control and other diabetes-related metabolic abnormalities can damage blood vessels in the nephrons, which irreversibly decreases overall kidney function.6 In addition, a significant proportion of patients with diabetes also develop hypertension and other metabolic disorders, which can accelerate kidney damage.6,7 The number of DKD patients in the US is projected to rise to 55 million by 2030.8
Studies show that US veterans suffer from an elevated risk of developing DKD. The proportion of veterans with kidney disease is around 34% higher than the general population.9 The main contributor to DKD among veterans is obviously the high prevalence of diabetes. A recent analysis demonstrated that veterans are more likely to have type 2 diabetes (T2D), with a prevalence of 25%, which is more than double the proportion of the general population.9,10 Of the various pertinent factors, including herbicide exposure, lack of awareness, or mental disorders, weight gain has been pointed to as the primary risk associated with both diabetes and kidney disorders.11–16 Overweight or obesity accounts for more than three quarters of veterans seeking health care from the Veterans Health Administration (VHA).15,16 The increase in the risk of DKD among veterans is also attributable to the higher prevalence of posttraumatic stress disorder and associated factors.17,18
With respect to concurrent conditions and prevalent risk factors, there has been a general consensus that the rate of progression is faster among US veterans with DKD than that of among DKD populations.10 Nevertheless, contemporary estimates of DKD prevalence and progression among US veterans are lacking, which creates challenges in understanding the real-world disease burden of DKD on US veterans. Assessments of the value of new health-care technologies for DKD patients in the VHA is challenging due to the lack of comprehensive summaries. The purpose of this study was to summarize the epidemiology of DKD among US veterans. We aimed to provide three key measures: 1) number of patients at various DKD stages by using current DKD definitions, 2) stage transitions from earlier DKD stages to advanced stages and chronic dialysis phase, and 3) longitudinal changes in the number of DKD patients in the VHA.
Methods
Study Design and Data Source
This was a historical cohort study that utilized VHA electronic health-record data for the period between January 2015 and March 2022. The VHA is the largest health-care system in the United States, providing care at 1298 health-care facilities, including 171 VHA medical centers and 1113 outpatient-care sites. The database includes inpatient, outpatient, pharmacy service records, and laboratory test results of 9 million veterans enrolled in the VHA program. This study did not involve patient identifiers and was exempt by the University of Utah and VHA institutional review boards.
Eligibility Criteria
Prior to inclusion the DKD cohort, patients needed meet either of the two T2D criteria: two or more outpatient diagnoses of T2D on two different dates within 365 days, or one outpatient T2D diagnosis with at least one record of non-insulin antidiabetic medication dispensing no more than 365 days apart. To be eligible for the analysis, the first diagnosis of T2D had to be before the date presenting with abnormal kidney function with moderate or high risk of progression, as defined by Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guidelines.19
KDIGO classifies DKD based on two criteria: GFR (G1, G2, G3a, G3b, G4, and G5) and albuminuria (A1, A2, and A3). Each DKD patient falls into one category at the intersection of the two criteria. The categories of both criteria are ordered, with lower numbers indicating less severe stages of DKD and higher numbers indicating more severe stages. Patients are considered at moderate or high risk of progression if they either fall into the G3–G5 GFR categories, regardless of albuminuria or stage G1 or G2 accompanied by A2 or A3 albuminuria.19
For our study, we included DKD patients at moderate or high risk of progression. We identified these patients if their estimated GFR (eGFR) values measured on two days 90–365 days apart corresponded to the G3–G5 categories.19 The index date throughout this study was the cohort entry date, defined as the first of the two dates meeting the eGFR criteria. Also, G1 and G2 DKD patients were included if they were persistent albuminuria cases (A2 or A3). This was defined by urinary albumin:creatinine ratio (uACR) ≥3 mg/mmol or urinary albumin ≥30 mg/day on two days within 365 days besides the eGFR criteria. For patients with missing albuminuria records, we used urinary protein:creatinine ratio (uPCR) ≥15 mg/mmol or urinary protein ≥150 mg/day as an alternative indicator of the kidney damage.
Dialysis and kidney-transplant stage were ascertained using procedure records defined by Logical Observation Identifiers Names and Codes or procedure description. Receiving two or more dialyses within 90 days was considered chronic dialysis. Date of kidney transplant was defined as the first date of procedure indicating transplant-recipient status. Whenever two time points were used to define eligibility, the first of the two was considered the index date for the entire analysis. We excluded patients who had any of the moderately increased or high-risk abnormal kidney-function criteria during the 365 days before the index date. Also, patients who were younger than 18 years at the index date were excluded.
Baseline Characteristics
Baseline characteristics were extracted from the treatment, diagnosis, and laboratory test records spanning 1 year before the index date. We ascertained demographic information, including age, body mass index (BMI), sex, race, ethnicity, and smoking status. Also, we captured clinical characteristics and laboratory test results, including systolic blood pressure (SBP), diastolic blood pressure (DBP), glycated hemoglobin (HbA1c), low-density lipoprotein, high-density lipoprotein, total cholesterol, and triglyceride levels. We additionally reviewed the diagnosis codes and VHA problem lists to identify comorbid conditions associated with rapid DKD progression. Such conditions included hypertension, dyslipidemia, malignancy, liver disorder, anemia, gout, connective tissue disorder, and substance abuse.20–22
Outcomes
We measured two epidemiological outcomes. First, DKD progression was defined as the composite of DKD stage transition from the index stage to any of the advanced stages or all-cause death recorded in the VHA data. The second outcome was the number of DKD patients in the VHA overall and across years. All cases at the end of each year between 2018 and 2021 conditional on the absence of reported death during or prior to the calendar year were captured for the case count.
Statistical Analysis
We use descriptive statistics to present the number of patients at each DKD stage at the index date and DKD stage transition. Continuous variables, such as age, BMI, and laboratory values, are summarized using means and standard deviations. Continuous values are categorized into three or four classes based on the distribution of the features and clinical risk thresholds. All the categorical variables are summarized using frequencies and percentages of the total number of eligible subjects, where missing records are grouped into an “unknown” category.
Time to DKD progression from the index stage was analyzed using a Kaplan–Meier product-limit estimator, where patients were followed up from the index date to the earliest occurrence of DKD progression (the outcome of interest), 5 years post–index date, or the end of the study period (March 2022). Conditional on DKD progression, the proportion of each of the next DKD stages of all the progressions was calculated. For the case count, we estimated the DKD cases each year and longitudinal changes in the number of patients across the years. We counted the number of DKD patients at the end of each calendar year between 2019 and 2021, the most recent 3-year data. The proportion of each stage of the year-end DKD patient count is presented.
Results
The total number of patients meeting the DKD cohort entry criteria was 685,288 (Table 1). Most DKD patients (78.97%) entered the cohort once they had reached stages G3a and G3b. The cohort was predominantly male (96.38%), Caucasian (75.45%), and non-Hispanic (93.68%), and 78.52% of patients were 65 years old or older (Table 1). Clinical characteristics from the point of care showed elevated cardiovascular risk and metabolic markers, with mean BMI of 32 kg/m2, HbA1c of 7.44%, and SBP of 136 mmHg. Hypertension and dyslipidemia were the most prevalent comorbidities across the DKD stages, with respective overall prevalence estimates of 71.71% and 59.58%, respectively (Table 2). The prevalence of anemia increased with later stages of DKD, with the prevalence among G5 patients of 28.2% compared to 2.9% among G1 patients (A2 or A3; Table 2).
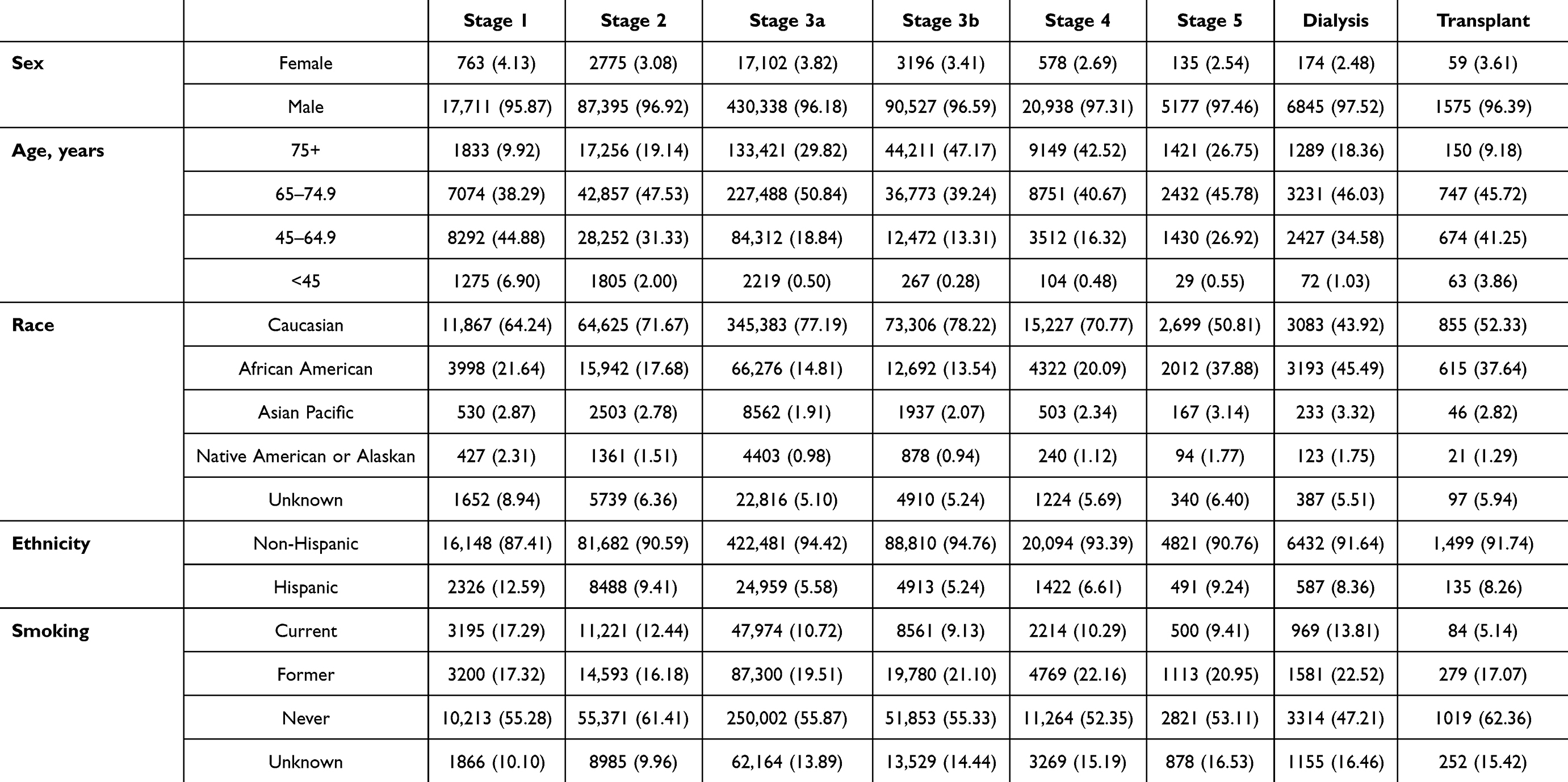 |
Table 1 Demographics at baseline, n (%) |
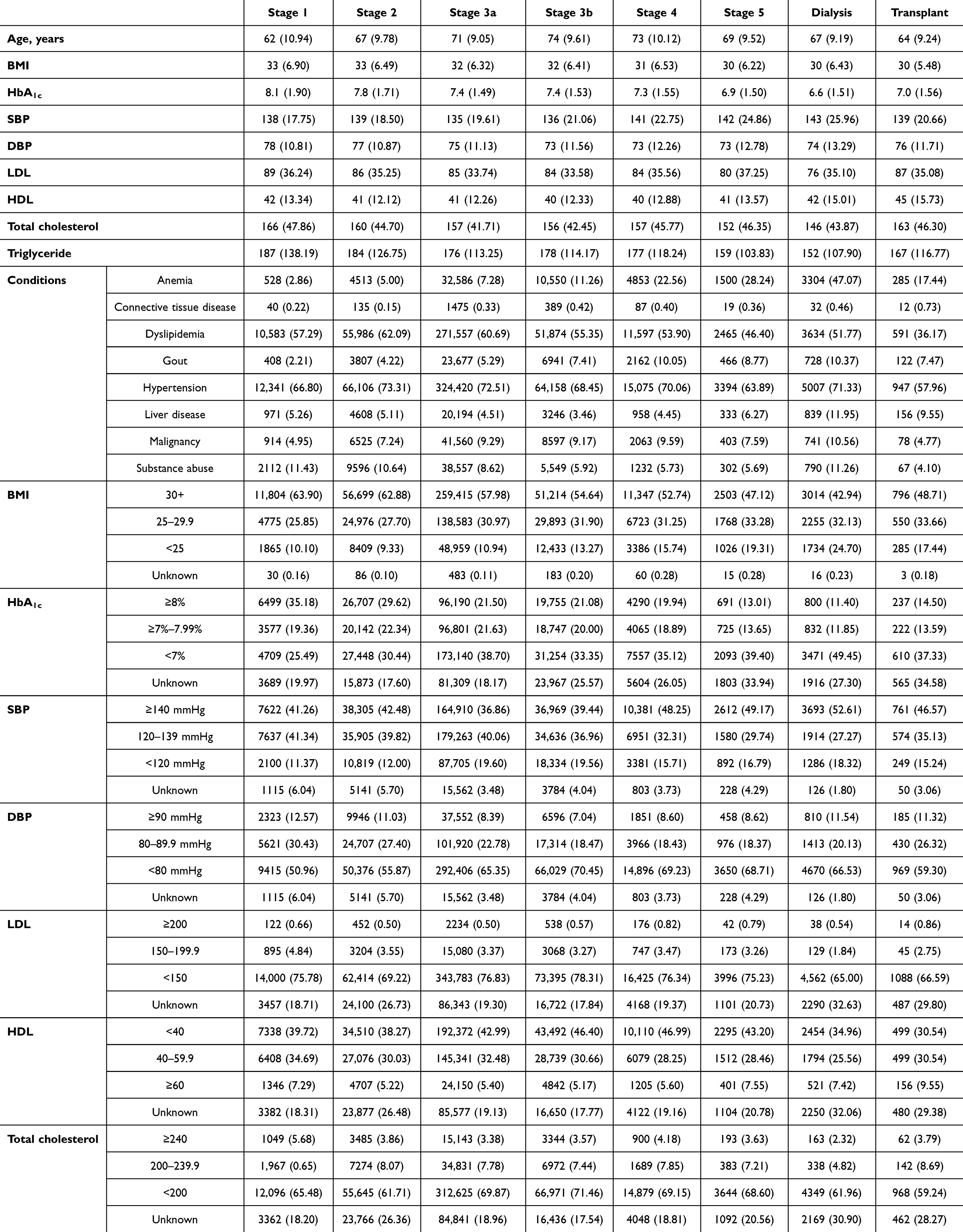 |
Table 2 Clinical characteristics, mean (SD) |
The cumulative incidence of DKD-stage transition or death is summarized in Figure 1. The respective 5-year cumulative incidence of progression to an advanced DKD stage or all-cause death from DKD stages G1, G2, G3a, and G3b was 52.0%, 47.4%, 50.5%, and 60.9%. Overall, 11.9%–16.7% of G1–G3b patients experienced DKD progression within a year from the index date. Among G5 patients, the cumulative incidence of transition to chronic dialysis, kidney transplant, or death was 43.6% at year 1 and 88.3% at year 5 (Figure 1).
 |
Figure 1 Cumulative incidence of progression, including transition to advanced DKD stage or death. |
Stage transitions were gradual and to the next stage in general. For example, 69.93% of progression from G1 A2/A3 was transition to G2 A2/A3, and 63% of progression from G3a was transition to G3b. The data showed a gradual increase in the proportion of deathsout of all transitions with higher DKD stage. From G1 A2/A3, 19.6% of any progression within 5 years was death, while all-cause death accounted for 53.4% of any transitions from G4 (Table 3).
 |
Table 3 Proportion of observed next stage conditional on DKD progression or death |
Across a series of single time points, the number of patients with DKD was approximately 600,000 over the calendar years, with respective numbers of patients alive at the end of 2020 and 2021 of 603,397 and 594,082. Stages G1 A2/A3, G2 A2/A3, G3a, and G3b accounted for 1.8%, 10.8%, 51.2%, and 25.3% of cases, respectively, at the end of 2021. Although the number of cases varied yearly, the proportion of DKD patients at each stage of the total year-end DKD count was generally consistent (Figure 2).
 |
Figure 2 DKD prevalence at single time points. |
Discussion
This is the first comprehensive description of DKD among US veterans using statistics of the incidence of stage progression and DKD case count. Using recorded measures of decline in kidney function and kidney damage, we included approximately 700,000 patients into an analytic cohort over the 6 years of the observational period. Most of the DKD cases were not classified with DKD until they reached stage G3a after a 1-year baseline period free from indicators of kidney damage or decline in kidney function. Of those classified as having moderate-risk or high-risk DKD in the US veterans,19 47%–61% progressed to an advanced stage or died within 5 years. This comes to 13%–19% of the annual figure for DKD stage progression or death, exceeding the anticipated rate of stage progression on a controlled decline in kidney function.23–25
Veterans with DKD had a moderate increase in the risk of cardiovascular complications. The moderate escalation in blood pressure translated into more than two thirds of patients having a diagnosis of hypertension at baseline, with 38.7% of the overall cohort being classified as having stage 2 hypertension.26 Approximately three of five veterans with DKD had a BMI >30 kg/m2 which is greater than the prevalence of this condition in the overall veteran population.16 The proportion of patients with a diagnosis of dyslipidemia is similar to the prevalence in veterans without DKD.27,28 Despite veterans generally being considered to carry more concurrent chronic conditions than the general US population, such a moderate increase in risk among veterans with DKD does not exceed that in commercially insured DKD patients.29,30 Whether the risk profiles from our analysis indicate that the VHA DKD population is generally healthier than the commercially insured population when developing DKD or VHA patients suffering from concurrent conditions were left-censored withincreased mortality should be further analyzed in future research.
Early detection of DKD is important, since intervention in the conservative phase is likely to be more effective in preventing further complications.31 For example, renin–angiotensin system blockers are most effective in slowing kidney damage in patients with diabetes when prescribed in the early stages.32 Clinical practice has also acknowledged the benefits of recently advanced nephroprotective antidiabetic agents, as the acceptance of SGLT2-inhibitor use is rapidly increasing for patients with stage G1 or G2 DKD.33 To allocate patients to a proper treatment plan as early as possible, major clinical communities and associations, including the American Diabetes Association, KDIGO, and the National Kidney Foundation, have recommended annual measurement of kidney function to identify and monitor diabetic nephropathy for T2D patients.19,34,35
Despite the importance of managing early-stage DKD, a sizable number of DKD cases might be determined only once it has become symptomatic. Using the 1-year baseline period, which corresponds to the recommended annual interval, we found that around four of five DKD cases at greater-than-minimal risk were determined once their kidney function criteria had met the stage G3a criteria. This is probably due to a lack of regular follow-up with albuminuria or proteinuria testing, while eGFR testing is obtained from almost all diabetes patients.36–38 For example, our post hoc analysis of patient characteristics found that 72.7% of the patients with eGFR <90 (G2 criteria) did not have follow-up uACR or uPCR testing within 365 days of the eGFR record, which ruled a significant proportion of stage G2 patients out from our study. The low rate of uACR/uPCR utilization aligns with the rate of albuminuria testing, consistently lower than 50% in various US health-care settings,39,40 and specifically matched with a recent real-world data analysis, where only 23.2% of albuminuria cases were determined among hypertensive or diabetic persons at risk of CKD.41 Our research cohort, dominated by patients who had already advanced to or beyond stage G3a, also matches a recent analysis of administrative claims from the commercially insured population, where stages G3a and G3b accounted for 77% of all newly recognized DKD cases.30 Diagnosis of DKD after a considerable decline in kidney function must be addressed in order to maximize the benefits of advanced treatment options in the overall DKD cohort.
Besides the underutilized albuminuria testing, our data suggest practice gaps in identifying rapid DKD progressions in terms of patient follow-up intervals. For example, of the patients entering the cohort with observed DKD G1 A2 or A3, more than 10% progressed to stage G3a or above before their eGFR decline was captured at stage G2. Similarly, more than 5% of the observed DKD progressions from stage G2 A2 or A3 were not a transition through stage G3a. The lifetime benefits of early detection and proper nephroprotective agent use would be greater in patients with such accelerated DKD progression whose eGFR decline exceeds 5 mL/min/1.73 m2 within a year or 10 mL/min/1.73 m2 within 5 years.42 To close the gap, health-care systems need to evaluate strategies to assess the risk of progressive renal decline.43,44
We employed the entire VHA database to calculate DKD epidemiology, which represents the most significant strength of our study. Previous studies performed in the VHA setting analyzed a regional cohort or a panel of DKD patients to estimate prevalence, with inherent limitations in understanding the full scope of DKD in the entire health-care system due to variations across facilities.10,39 Given that figures for the prevalence of comorbidities among CKD patients is available from multiple retrospective analyses, we may also approximate the overall epidemiology of DKD among veterans.45,46 Nevertheless, such calculations could be debatable in terms of accuracy in reflecting the temporal sequence of diabetes and nephropathy, with limited ability to reflect the longitudinal changes in population size. Based on the number of beneficiaries and the cases that we determined, DKD currently influences approximately 65–70 per 1000 veterans, which is more than a quarter of veterans with T2D. When the calculation is limited to a narrower CKD definition upon eGFR criteria before progression to end-stage renal disease (15–60 mL/min/1.73 m2),47,48 DKD affects 56 out of each 1000 US veterans. This estimate is about double the DKD prevalence in the general US population.49
Besides inclusion of the entire DKD population from the VHA, our study provides contemporary estimates of the prevalence of DKD and DKD progression rates in the VHA system. This quantitative summary can be valuable for understanding the disease burden on the VHA system and support health- technology value assessment, DKD-related health programs, and economic evaluations. Nonetheless, our study has several limitations. First, our definition of DKD required multiple time points for ascertainment and the follow-up started from the earliest of the two points. This might have introduced selection bias to the analysis by excluding those who had their eGFR calculated on only one occasion and died later. Similarly, due to the study design, no patients died between the two time points, which could make our mortality estimates biased downwards. Second, although we used a 1-year retrospective period to ascertain the DKD incidence, it is possible that patients received care outside the VHA before the index date, which could entail that DKD cases were misclassified as new cases. Third, almost half of our cohort were above 65 years old and could be entitled to receive Medicare benefits, which increased the chance of missing laboratory results and health-service records. Finally, general limitations of the retrospective design, including but not being limited to miscoding, missing observations, and limited generalizability, should be considered when interpreting the study findings.
Conclusion
Using recent data from the VHA, we quantitatively summarized longitudinal changes in the prevalence and rapid progression of DKD among US veterans. With the anticipated rise in the number of patients with diabetes and other comorbidities, DKD will pose significant clinical and economic challenges for the VHA to address. More exploratory research into treatment, diagnosis, and screening strategies is warranted to mitigate the prevalence of various DKD risk factors among US veterans. Furthermore, our findings underscore the need for innovations in health-care delivery so as to intervene at early DKD stages to delay progression into advanced stages, which can subsequently reduce the clinical and economic burden of DKD among US veterans.
Funding
This study was funded by Renalytix. Renalytix had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
Dr Kibum Kim reports grants from Institute for Clinical and Economic Review, Grail, AstraZeneca, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Johansen KL, Chertow GM, Foley RN, et al. US renal data system 2020 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis Apr. 2021;77(4 Suppl 1):A7–a8. doi:10.1053/j.ajkd.2021.01.002
2. Hoerger TJ, Simpson SA, Yarnoff BO, et al. The future burden of CKD in the United States: a simulation model for the CDC CKD Initiative. Am J Kidney Dis. 2015;65(3):403–411. doi:10.1053/j.ajkd.2014.09.023
3. National Institute of Diabetes and Digestive and Kidney Diseases. Kidney disease statistics for the United States; 2023. Available from: https://www.niddk.nih.gov/health-information/health-statistics/kidney-disease.
4. Finkelstein FO, Wuerth D, Finkelstein SH. Health related quality of life and the CKD patient: challenges for the nephrology community. Kidney Int. 2009;76(9):946–952. doi:10.1038/ki.2009.307
5. National Kidney Foundation. Diabetes and chronic kidney disease; 2023. Available from: https://www.kidney.org/news/newsroom/factsheets/Diabetes-And-CKD.
6. Barrera-Chimal J, Jaisser F. Pathophysiologic mechanisms in diabetic kidney disease: a focus on current and future therapeutic targets. Diabetes Obesity Metab. 2020;22(S1):16–31. doi:10.1111/dom.13969
7. Van Buren PN, Toto R. Hypertension in diabetic nephropathy: epidemiology, mechanisms, and management. Adv Chronic Kidney Dis. 2011;18(1):28–41. doi:10.1053/j.ackd.2010.10.003
8. Rowley WR, Bezold C, Arikan Y, Byrne E, Krohe S. Diabetes 2030: insights from yesterday, today, and future trends. Popul Health Manag. 2017;20(1):6–12. doi:10.1089/pop.2015.0181
9. Chen C Support for Veterans with kidney disease; 2023. Available from: https://news.va.gov/119226/support-for-veterans-with-kidney-disease/.
10. Young BA, Pugh JA, Maynard C, Reiber G. Diabetes and renal disease in veterans. Diabetes Care. 2004;27(suppl_2):b45–b49. doi:10.2337/diacare.27.suppl_2.B45
11. Huang CJ, Chiu HC, Lee MH, Wang SY. Prevalence and incidence of anxiety disorders in diabetic patients: a national population-based cohort study. Gen Hosp Psychiatry. 2011;33(1):8–15. doi:10.1016/j.genhosppsych.2010.10.008
12. Liu Y, Sayam S, Shao X, et al. Prevalence of and trends in diabetes among veterans, United States, 2005-2014. Prev Chronic Dis. 2017;14:E135. doi:10.5888/pcd14.170230
13. Reiber GE, Koepsell TD, Maynard C, Haas LB, Boyko EJ. Diabetes in nonveterans, veterans, and veterans receiving department of veterans affairs health care. Diabetes Care. 2004;27(suppl_2):b3–b9. doi:10.2337/diacare.27.suppl_2.B3
14. Institute of Medicine (US). Committee to Review the Evidence Regarding the Link Between Exposure to Agent Orange and Diabetes. Veterans and Agent Orange: Herbicide/Dioxin Exposure and Type 2 Diabetes. National Academies Press (US); 2000.
15. Rush T, LeardMann CA, Crum-Cianflone NF Obesity and associated adverse health outcomes among US military members and veterans: findings from the millennium cohort study; 1930.
16. Breland JY, Phibbs CS, Hoggatt KJ, et al. The obesity epidemic in the veterans health administration: prevalence among key populations of women and men veterans. J Gen Intern Med. 2017;32(Suppl 1):11–17. doi:10.1007/s11606-016-3962-1
17. Boyko EJ, Jacobson IG, Smith B, et al. Risk of diabetes in U.S. military service members in relation to combat deployment and mental health. Diabetes Care. 2010;33(8):1771–1777. doi:10.2337/dc10-0296
18. Kanchi R, Lopez P, Rummo PE, et al. Longitudinal analysis of neighborhood food environment and diabetes risk in the veterans administration diabetes risk cohort. JAMA Network Open. 2021;4(10):e2130789–e2130789. doi:10.1001/jamanetworkopen.2021.30789
19. KDIGO 2022. Clinical practice guideline for diabetes management in chronic kidney disease. Kidney Int. 2022;102(5s):S1–s127. 10.1016/j.kint.2022.06.008.
20. Choi HG, Kwon BC, Kwon MJ, et al. Association between gout and dyslipidemia: a nested case-control study using a national health screening cohort. J Pers Med. 2022;12(4):605. doi:10.3390/jpm12040605
21. Lee WC, Lee YT, Li LC, et al. The number of comorbidities predicts renal outcomes in patients with stage 3⁻5 chronic kidney disease. J Clin Med. 2018;7(12):493. doi:10.3390/jcm7120493
22. Pan CS, Ju TR, Lee CC, et al. Alcohol use disorder tied to development of chronic kidney disease: a nationwide database analysis. PLoS One. 2018;13(9):e0203410. doi:10.1371/journal.pone.0203410
23. Persson F, Rossing P. Diagnosis of diabetic kidney disease: state of the art and future perspective. Kidney Int. 2018;8(1):2–7. doi:10.1016/j.kisu.2017.10.003
24. Weldegiorgis M, de Zeeuw D, Li L, et al. Longitudinal estimated GFR trajectories in patients with and without type 2 diabetes and nephropathy. Am J Kidney Dis. 2018;71(1):91–101. doi:10.1053/j.ajkd.2017.08.010
25. García-Carro C, Vergara A, Bermejo S, et al. How to assess diabetic kidney disease progression? From albuminuria to GFR. J Clin Med. 2021;10(11):2505. doi:10.3390/jcm10112505
26. Whelton PK, Carey RM, Mancia G, Kreutz R, Bundy JD, Williams B. Harmonization of the American College of Cardiology/American heart association and European society of cardiology/European society of hypertension blood pressure/hypertension guidelines: comparisons, reflections, and recommendations. Circulation. 2022;146(11):868–877. doi:10.1161/CIRCULATIONAHA.121.054602
27. Steinman MA, Lee SJ, John Boscardin W, et al. Patterns of multimorbidity in elderly veterans. J Am Geriatr Soc. 2012;60(10):1872–1880. doi:10.1111/j.1532-5415.2012.04158.x
28. Fryar CD, Herrick K, Afful J, Ogden CL. Cardiovascular disease risk factors among male veterans, U.S., 2009-2012. Am J Prev Med. 2016;50(1):101–105. doi:10.1016/j.amepre.2015.06.011
29. Roy S, Schweiker-Kahn O, Jafry B, et al. Risk factors and comorbidities associated with diabetic kidney disease. J Prim Care Community Health. 2021;12:21501327211048556. doi:10.1177/21501327211048556
30. Folkerts K, Petruski-Ivleva N, Kelly A, et al. Annual health care resource utilization and cost among type 2 diabetes patients with newly recognized chronic kidney disease within a large U.S. administrative claims database. J Manag Care Spec Pharm. 2020;26(12):1506–1516. doi:10.18553/jmcp.2020.26.12.1506
31. Locatelli F, Vecchio LD, Pozzoni P. The importance of early detection of chronic kidney disease. Nephrol Dial Transplant. 2002;17(Suppl 11):2–7. doi:10.1093/ndt/17.suppl_11.2
32. Momoniat T, Ilyas D, Bhandari S. ACE inhibitors and ARBs: managing potassium and renal function. Cleve Clin J Med. 2019;86(9):601–607. doi:10.3949/ccjm.86a.18024
33. Center for Disease Control and Prevention Kidne Disease Surveillance System. Percentage of patients with CKD and diabetes using SGLT2i; 2021. Available from: https://nccd.cdc.gov/ckd/detail.aspx?Qnum=Q719.
34. ElSayed NA, Aleppo G, Aroda VR, et al. 11. chronic kidney disease and risk management: standards of care in diabetes—2023. Diabetes Care. 2022;46(Supplement_1):S191–S202. doi:10.2337/dc23-S011
35. National Kidney Foundation. KDOQI clinical practice guideline for diabetes and CKD: 2012 Update. Am J Kidney Dis. 2012;60(5):850–886. doi:10.1053/j.ajkd.2012.07.005
36. Chu CD, Powe NR, Shlipak MG, et al. Albuminuria testing and nephrology care among insured US adults with chronic kidney disease: a missed opportunity. BMC Prim Care. 2022;23(1):299. doi:10.1186/s12875-022-01910-9
37. Alfego D, Ennis J, Gillespie B, et al. Chronic kidney disease testing among at-risk adults in the U.S. remains low: real-world evidence from a national laboratory database. Diabetes Care. 2021;44(9):2025–2032. doi:10.2337/dc21-0723
38. Shin JI, Chang AR, Grams ME, et al. Albuminuria testing in hypertension and diabetes: an individual-participant data meta-analysis in a global consortium. Hypertension. 2021;78(4):1042–1052. doi:10.1161/hypertensionaha.121.17323
39. Navaneethan SD, Akeroyd JM, Ramsey D, et al. Facility-level variations in kidney disease care among veterans with diabetes and CKD. Clin J Am Soc Nephrol. 2018;13(12):1842–1850. doi:10.2215/cjn.03830318
40. Lee J, Chu C, Guzman D, et al. Albuminuria testing by race and ethnicity among patients with hypertension with and without diabetes. Am J Nephrol. 2019;50(1):48–54. doi:10.1159/000500706
41. Chu CD, Xia F, Du Y, et al. Estimated prevalence and testing for albuminuria in us adults at risk for chronic kidney disease. JAMA Network Open. 2023;6(7):e2326230–e2326230. doi:10.1001/jamanetworkopen.2023.26230
42. Thornton Snider J, Sullivan J, van Eijndhoven E, et al. Lifetime benefits of early detection and treatment of diabetic kidney disease. PLoS One. 2019;14(5):e0217487. doi:10.1371/journal.pone.0217487
43. Nowak N, Skupien J, Smiles AM, et al. Markers of early progressive renal decline in type 2 diabetes suggest different implications for etiological studies and prognostic tests development. Kidney Int. 2018;93(5):1198–1206. doi:10.1016/j.kint.2017.11.024
44. Coresh J, Turin TC, Matsushita K, et al. Decline in estimated glomerular filtration rate and subsequent risk of end-stage renal disease and mortality. JAMA. 2014;311(24):2518–2531. doi:10.1001/jama.2014.6634
45. Patel N, Golzy M, Nainani N, et al. Prevalence of various comorbidities among veterans with chronic kidney disease and its comparison with other datasets. Ren Fail. 2016;38(2):204–208. doi:10.3109/0886022x.2015.1117924
46. Oliver JD, Nee R, Grunwald LR, et al. Prevalence and characteristics of CKD in the US military health system: a retrospective cohort study. Kidney Med. 2022;4(7):100487. doi:10.1016/j.xkme.2022.100487
47. Chen TK, Knicely DH, Grams ME. Chronic kidney disease diagnosis and management: a review. JAMA. 2019;322(13):1294–1304. doi:10.1001/jama.2019.14745
48. Kovesdy CP. Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl. 2022;12(1):7–11. doi:10.1016/j.kisu.2021.11.003
49. Centers for Disease Control and Prevention. Kidney disease surveillance system: prevalence of Chronic Kidney Disease (CKD); 2023. Available from: https://nccd.cdc.gov/ckd/default.aspx.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.