Back to Journals » Infection and Drug Resistance » Volume 19
Epidemiology, Antimicrobial Resistance, and Seasonal Dynamics of Respiratory Bacterial Pathogens in a Saudi Tertiary Care Hospital (2023–2025)
Authors Alzahrani AJ, El-Shahidy S, Lahyani A, Al Hussain A, Al Olayan B, Alruwais N, Hagras SAA ![]() , Al Faran A, Khojah OT
, Al Faran A, Khojah OT
Received 19 March 2026
Accepted for publication 6 July 2026
Published 14 July 2026 Volume 2026:19 610414
DOI https://doi.org/10.2147/IDR.S610414
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Ahmed J Alzahrani,1,2 Samar El-Shahidy,2,3 Amina Lahyani,2 Ahmed Al Hussain,2 Bilal Al Olayan,2 Nada Alruwais,2 Soheir AA Hagras,4,5 Ahmed Al Faran,2,6 Osamah T Khojah7,8
1College of Medicine, Al-Imam Mohammed Ibn Saud Islamic University, Riyadh, Saudi Arabia; 2Laboratory Department, Dr. Sulaiman Al-Habib Medical Group, Riyadh, Saudi Arabia; 3Faculty of Science, Suez Canal University, Ismailia, Egypt; 4Pharmacy Department, Al Nahda College, Riyadh, 13255, Saudi Arabia; 5Department of Drug Radiation Research, National Center for Radiation Research and Technology (NCRRT), Egyptian Atomic Energy Authority, Cairo, Egypt; 6KSUF, Basic Sciences Department, College of Medicine, Shaqara University, Shaqara, Saudi Arabia; 7Department of Pathology, College of Medicine, King Saud University, Riyadh, 24 11472, Saudi Arabia; 8Chief Medical Officer Office, Laboratory Department, Dr. Sulaiman Al Habib Medical Group, Riyadh, 11643, Saudi Arabia
Correspondence: Ahmed J Alzahrani, Email [email protected] Samar El-Shahidy, Email [email protected]; [email protected]
Background: Respiratory tract infections (RTIs) remain a major cause of morbidity and mortality, particularly among hospitalized and critically ill patients. The increasing prevalence of multidrug-resistant organisms (MDROs) complicates treatment and highlights the need for local surveillance to guide antimicrobial stewardship. This study investigated the epidemiology, antimicrobial resistance patterns, and seasonal trends of respiratory bacterial pathogens in a tertiary care hospital in Riyadh, Saudi Arabia.
Methods: A retrospective observational study was conducted on 5582 respiratory specimens collected between January 2023 and December 2025. Samples included tracheal aspirates, sputum, bronchoalveolar lavage, throat swabs, pleural fluids, ear swabs, and nasal swabs. Bacterial identification and antimicrobial susceptibility testing were performed using the VITEK® 2 Compact system and interpreted according to CLSI M100-S35 guidelines. Statistical analyses included Chi-square tests and logistic regression.
Results: Culture positivity was 38.6% (2154/5582), with tracheal aspirates and sputum accounting for the most positive specimens. The predominant pathogens were Pseudomonas aeruginosa (31.9%), Klebsiella spp. (21.3%), Staphylococcus aureus (10.2%), Serratia marcescens (6.3%), Escherichia coli (5.7%) and Acinetobacter baumannii (5.5%). Culture positivity increased significantly with age (p< 0.001), with Gram-negative bacteria predominating in older patients. MDROs were slightly prevalent, including, carbapenem-resistant organisms (22.9%) and ESBL producers (12.3%). The highest MDRO burden occurred in intensive care and other high-acuity wards. Seasonal analysis demonstrated a significant increase in MDRO prevalence during the summer months, with carbapenem-resistant Gram-negative pathogens rising from 18.2% in the winter to 28.7% in the summer (OR 1.82, 95% CI: 1.45– 2.28; p< 0.001).
Conclusions: Respiratory pathogens in this Saudi tertiary care hospital exhibited a high prevalence of multidrug resistance, particularly among Gram-negative bacteria and in critical care settings. Seasonal increases in resistance during the summer months suggest the need for intensified infection control measures, strengthened antimicrobial stewardship, and ongoing surveillance to reduce MDRO transmission and optimize patient outcomes.
Keywords: antimicrobial resistance, respiratory tract infections, multidrug-resistant organisms, carbapenem resistance, ESBL, seasonal dynamics, antimicrobial stewardship, Saudi Arabia, Pseudomonas aeruginosa, Klebsiella pneumoniae
Introduction
Respiratory tract infections (RTIs) remain a major cause of morbidity and mortality worldwide, particularly among hospitalized and critically ill patients.1,2 The growing burden of multidrug-resistant organisms (MDROs) has significantly complicated the management of these infections by limiting effective therapeutic options, prolonging hospital stays, and increasing mortality.3,4 Among the most clinically important pathogens are carbapenem-resistant Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacterales, which are classified by the World Health Organization as critical priority pathogens requiring urgent attention.5 However, despite their clinical importance, limited data exist on the temporal and seasonal behavior of multidrug-resistant respiratory pathogens, particularly in Saudi Arabia.
Antimicrobial resistance (AMR) represents a major global health challenge and is particularly prominent in the Middle East region.6–8 In Saudi Arabia, increasing rates of resistance among respiratory pathogens have been reported, with intensive care units (ICUs) representing a high-risk setting where carbapenem-resistant Enterobacterales and multidrug-resistant Acinetobacter baumannii are frequently encountered.9,10 These trends highlight a growing national burden; however, comprehensive institution-based surveillance data remain limited, especially those evaluating resistance patterns across different respiratory specimen types and clinical care settings.11
The most commonly implicated bacterial pathogens in respiratory tract infections among hospitalized patients include Pseudomonas aeruginosa, Klebsiella pneumoniae, Acinetobacter baumannii, Escherichia coli, and Staphylococcus aureus.12,13 These organisms exhibit diverse and complex resistance mechanisms, including carbapenemase production, extended-spectrum β-lactamase (ESBL) production, methicillin resistance, as well as alterations in membrane permeability and efflux pump activity.14–18 Collectively, these mechanisms contribute to limited treatment options and are associated with adverse clinical outcomes. Understanding these pathogens and their resistance profiles is essential for interpreting local epidemiological trends and guiding empirical therapy.
Klebsiella pneumoniae represents one of the most clinically significant multidrug-resistant Gram-negative pathogens contributing to hospital-acquired respiratory infections. Its increasing antimicrobial resistance, including ESBL and carbapenem-resistant phenotypes, has been widely reported in both regional and global settings, highlighting its evolving threat in healthcare-associated infections.19–25 Recent studies have also emphasized the urgent need for alternative therapeutic strategies beyond conventional antibiotics, including antimicrobial coatings, biogenic nanoparticles, and anti-biofilm approaches targeting device-associated infections.19–25
Beyond resistance mechanisms, emerging evidence suggests that AMR may also demonstrate seasonal and temporal variation.26,27 Fluctuations in resistant respiratory pathogens have been reported and may be influenced by environmental factors, seasonal variations in viral infections, antimicrobial prescribing behavior, and healthcare utilization patterns.26,28–33 However, longitudinal studies evaluating seasonal dynamics of respiratory MDROs remain scarce, particularly within Saudi Arabia. This represents an important gap in knowledge, as understanding temporal trends may support optimization of antimicrobial stewardship strategies and infection prevention interventions.
Accordingly, institution-specific surveillance is essential to guide empirical treatment decisions and support antimicrobial stewardship and infection control programs. This study aimed to characterize the epidemiology and antimicrobial resistance patterns of respiratory bacterial pathogens, including multidrug-resistant phenotypes, and to evaluate their seasonal trends in respiratory specimens collected from a tertiary care hospital in Riyadh, Saudi Arabia, between 2023 and 2025. By providing comprehensive longitudinal surveillance data, this study addresses key gaps in local evidence and represents one of the few studies in Saudi Arabia to systematically evaluate seasonal dynamics of respiratory MDROs.
Materials and Methods
Study Design and Setting
This retrospective observational surveillance study was conducted at Dr. Sulaiman Alhabib Hospital, a 300-bed tertiary care hospital in Riyadh, Saudi Arabia. The hospital serves as a major referral center for complex medical and surgical cases, with specialized intensive care units (ICU), coronary care units (CCU), medical wards, surgical wards, pediatric units, and emergency departments. The study period extended from January 1, 2023, to December 31, 2025, encompassing three complete calendar years to capture seasonal variation and temporal trends.
Specimen Collection and Processing
All respiratory specimens submitted to the hospital microbiology laboratory as part of routine clinical care during the study period were included in the analysis. Specimen types included tracheal aspirates, sputum (expectorated or induced), bronchoalveolar lavage (BAL) fluid, throat swabs, pleural fluid, ear swabs, and nasal swabs.
Specimens were collected by trained healthcare personnel following standard clinical protocols. Tracheal aspirates were obtained using sterile suction catheters from endotracheal or tracheostomy tubes. Sputum samples were collected after instructing patients to rinse their mouths and provide deep cough specimens into sterile containers. BAL samples were collected during bronchoscopy procedures under sterile conditions.
To ensure specimen quality, samples were excluded if they were deemed inadequate based on laboratory quality criteria, including gross contamination, insufficient volume, or poor-quality sputum (eg, excessive epithelial cell contamination indicating oropharyngeal origin). Duplicate isolates and contaminated cultures were also excluded from analysis.
Ear swabs were included as they may yield bacterial pathogens commonly associated with upper respiratory tract infections and otolaryngological infections such as otitis media. These represented a minor proportion of total specimens and were analyzed within the broader respiratory pathogen dataset.
All specimens were transported to the microbiology laboratory within 2 hours of collection and were processed immediately or stored at 4°C if delayed.
Isolates were interpreted as clinically significant based on standard microbiological reporting practices and growth of potential respiratory pathogens. Only non-duplicate clinically relevant isolates were included in the final analysis. Repeated isolates of the same bacterial species recovered from the same patient during the same clinical episode were excluded from the analysis. In cases of polymicrobial infection, different bacterial species isolated from the same patient were retained and analyzed separately as distinct isolates. Furthermore, patient readmissions were considered separate clinical episodes, and isolates obtained during a subsequent admission were eligible for inclusion Due to the retrospective laboratory-based design and lack of detailed clinical and radiological data, definitive differentiation between colonization and infection could not be systematically performed.
Bacterial Identification and Antimicrobial Susceptibility Testing
Specimens were inoculated onto appropriate culture media including blood agar, chocolate agar, and MacConkey agar, and incubated at 35–37°C in 5% CO2 (for fastidious organisms) or ambient air for 24–48 hours. Bacterial identification and antimicrobial susceptibility testing (AST) were performed using the VITEK® 2 Compact automated system (bioMérieux, Marcy-l’Étoile, France) with appropriate identification cards (GN, GP, YST) and AST cards (AST-N417, AST-P67, AST-GP80) according to the manufacturer’s instructions.34
Minimum inhibitory concentration (MIC) values were determined for relevant antimicrobial agents based on pathogen type. For Gram-negative organisms, tested agents included β-lactams (penicillins, cephalosporins, carbapenems), fluoroquinolones, and aminoglycosides. For Gram-positive organisms, tested agents included β-lactams, vancomycin, linezolid, daptomycin, and other agents as appropriate. Disk diffusion testing was performed as confirmatory testing when indicated, following CLSI guidelines.
All MIC values and disk diffusion zone diameters were interpreted according to the Clinical and Laboratory Standards Institute (CLSI) Performance Standards for Antimicrobial Susceptibility Testing, 35th Informational Supplement (M100-S35, 2025).35 The VITEK® 2 interpretive software was automatically updated in accordance with each new CLSI edition released during the study period (2023–2025), ensuring standardized and time-appropriate breakpoint interpretation across all isolates. For analysis purposes, intermediate susceptibility results were grouped with resistant isolates and reported as non-susceptible.
Quality control was performed using reference strains (Escherichia coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853, Staphylococcus aureus ATCC 29213, Enterococcus faecalis ATCC 29212) according to CLSI recommendations.
ESBL-producing and Carbapenem Resistant organisms were identified based on phenotypic antimicrobial susceptibility profiles generated by the VITEK® 2 Compact system and interpreted according to CLSI guidelines. Molecular confirmation of resistance genes was not performed.
Definitions
Culture Positivity
Growth of clinically significant bacterial pathogens from respiratory specimens, excluding normal respiratory flora and contaminants. Specimens with mixed flora or growth of probable contaminants (eg, coagulase-negative staphylococci, viridans streptococci, Corynebacterium spp., Candida spp.) were classified as culture-negative unless clinical correlation suggested pathogenic significance.
Multidrug Resistance (MDR)
Non-susceptibility to at least one agent in three or more antimicrobial categories, according to standardized international definitions.36
Extensive Drug Resistance (XDR)
Non-susceptibility to at least one agent in all but two or fewer antimicrobial categories.37
Carbapenem Resistance
Resistance to imipenem, meropenem, or doripenem based on CLSI breakpoints.
Extended-Spectrum β-Lactamase (ESBL) Producers
Organisms demonstrating ESBL phenotype based on CLSI screening and confirmatory criteria (ceftazidime or cefotaxime resistance with ≥5mm zone diameter increase in combination with clavulanic acid).
Methicillin-Resistant Staphylococcus aureus (MRSA)
S. aureus resistant to oxacillin or cefoxitin based on CLSI breakpoints.
Seasonal Classification
Winter (December–February), Spring (March–May), Summer (June–August), Autumn (September–November), based on Riyadh climatic patterns.
Data Collection
Data were extracted from the hospital laboratory information system (LIS) and electronic medical records (EMR). For each positive culture, the following data were collected:
- Patient demographics: age, gender
- Specimen type and collection date
- Ward/unit of origin (ICU, CCU, medical ward, surgical ward, pediatric ward, emergency department, outpatient)
- Bacterial identification (genus and species)
- Antimicrobial susceptibility results (MIC values and interpretation)
- Resistance phenotypes (MDR, XDR, carbapenem resistance, ESBL, MRSA)
Age was categorized into clinically relevant groups: preschool (0–5 years), school-age (6–12 years), adolescent (13–18 years), young adult (19–40 years), middle-aged adult (41–64 years), and geriatric (≥65 years).
To avoid duplicate reporting, repeat isolates of the same bacterial species recovered from the same patient within a 30-day period were excluded. Different bacterial species isolated from the same patient during the same clinical episode were retained and analyzed separately to account for polymicrobial infections. Patient readmissions were considered separate clinical episodes, and isolates recovered during subsequent admissions were included in the analysis.
Statistical Analysis
Data were compiled and analyzed using Microsoft Excel (Data Analysis Toolpak) and the RealStatistics add-in.38 Descriptive statistics were used to summarize all variables. Categorical variables were presented as frequencies and percentages, while continuous variables were expressed as means ± standard deviations or medians with interquartile ranges, depending on data distribution.
Univariate analyses were performed using the Chi-square test or Fisher’s exact test, as appropriate, to assess associations between categorical variables, including pathogen distribution, antimicrobial resistance patterns, ward location, age groups, gender, and seasonal variation. A p-value of <0.05 was considered statistically significant.
For temporal and seasonal analyses, monthly culture positivity rates and multidrug-resistant organism (MDRO) prevalence were calculated and evaluated across the study period. Seasonal comparisons were performed using Chi-square tests, with odds ratios (OR) and 95% confidence intervals (CI) calculated to quantify differences in MDRO prevalence between seasons, using winter as the reference category.
Binary logistic regression analysis was applied where appropriate to assess the association between MDRO occurrence and independent variables, including season, ward type, and patient demographic factors. Results were reported as crude or adjusted odds ratios as applicable.
Given the large sample size (5582 specimens and 2154 positive cultures), the study had sufficient statistical power to detect clinically meaningful differences in proportions between groups (eg, approximately 10% absolute differences in resistance rates) at a significance level of α = 0.05, based on chi-square distribution assumptions.39
Because of the exploratory nature of this surveillance study and the multiple comparisons performed across pathogens, antibiotics, wards, and seasons, unadjusted p-values were reported. Findings were interpreted in the context of clinical relevance and consistency with existing literature, with acknowledgment of the potential for type I error in subgroup analyses.
Ethical Considerations
This study was approved by the Institutional Review Board of Dr. Sulaiman Alhabib Medical Group (Approval RC 25.08.75). As a retrospective analysis of de-identified laboratory surveillance data collected as part of routine clinical care, the requirement for informed consent was waived. All patient data were de-identified prior to analysis, and no protected health information was included in the dataset. Data were stored on password-protected institutional servers with access restricted to authorized study personnel.
Results
Overall Culture Positivity and Specimen Distribution
Of 5582 respiratory specimens analyzed between January 2023 and December 2025, 2154 (38.6%) yielded clinically significant bacterial growth. The remaining 3428 specimens (61.4%) were culture-negative, showed normal respiratory flora only, or grew probable contaminants.
Among culture-positive specimens, tracheal aspirates accounted for 974/2154 (45.2%), followed by sputum 707/2154 (32.8%), bronchoalveolar lavage 245/2154 (11.4%), throat swabs 128/2154 (5.9%), pleural fluid 58/2154 (2.7%), nasal swabs 28/2154 (1.3%), and ear swabs 14/2154 (0.7%). Tracheal aspirates and sputum together accounted for 78.0% of all positive cultures.
Pathogen Distribution
A total of 2154 bacterial isolates were recovered from culture-positive specimens (Table 1). Pseudomonas aeruginosa was the most frequently isolated pathogen (31.9%), followed by Klebsiella species (21.3%), Staphylococcus aureus (10.2%), Serratia marcescens (6.3%), Escherichia coli (5.7%) and Acinetobacter baumannii (5.5%). Gram-negative bacteria accounted for 82% of all isolates, whereas Gram-positive bacteria accounted for 18%.
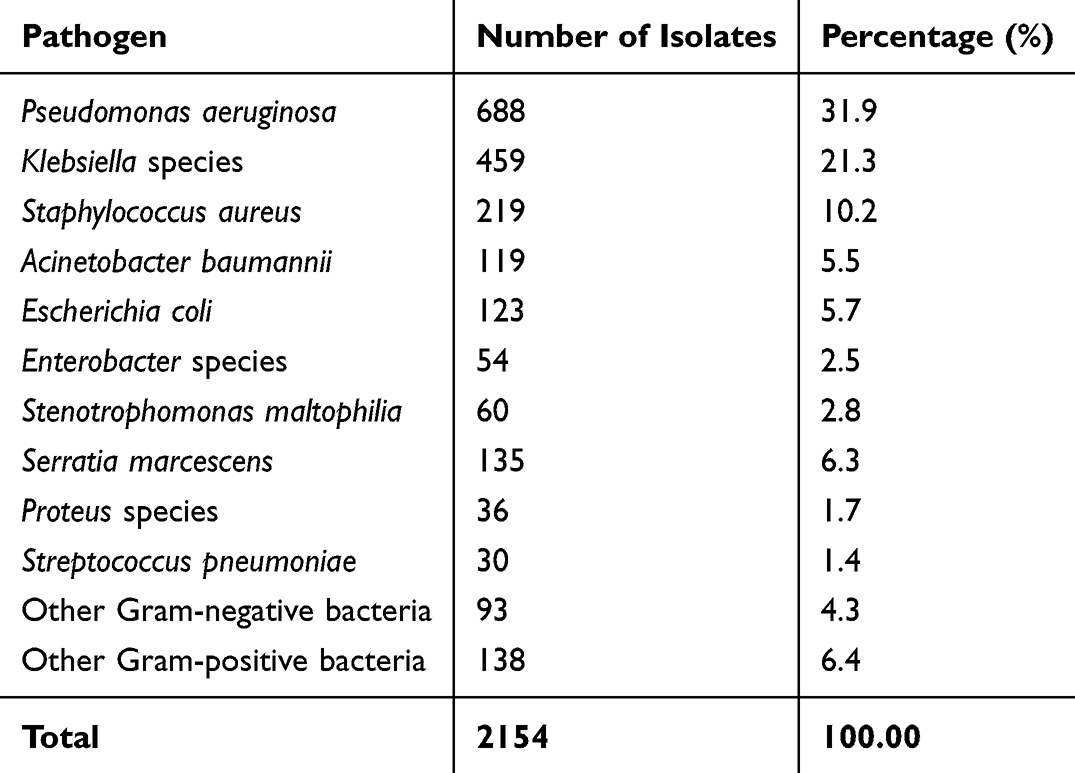 |
Table 1 Distribution of Bacterial Pathogens from Respiratory Specimens (N=2154) |
Age and Gender Distribution
Culture positivity increased significantly with age (p<0.001), ranging from 8.9% among preschool children to 51.5% among geriatric patients:
- Preschool (0–5 years): 8.9% (42/472)
- School-age (6–12 years): 12.3% (38/309)
- Adolescent (13–18 years): 18.7% (29/155)
- Young adult (19–40 years): 28.4% (287/1011)
- Middle-aged adult (41–64 years): 42.1% (756/1796)
- Geriatric (≥65 years): 51.5% (1002/1945)
The geriatric population accounted for 46.5% of all positive cultures.
Pathogen distribution varied by age group. Among pediatric patients (0–12 years), Staphylococcus aureus (32.5%) and Streptococcus pneumoniae (15.0%) were most common. Among adults (19–64 years), Pseudomonas aeruginosa (33.8%) and Klebsiella species (22.1%) predominated, whereas among geriatric patients, Pseudomonas aeruginosa (34.2%), Klebsiella species (23.7%), and Acinetobacter baumannii (15.8%) were most frequently isolated.
Males accounted for 58.2% (1254/2154) of positive cultures and females for 41.8% (900/2154), with a male-to-female ratio of 1.39:1. This difference was statistically significant (p=0.003).
Ward-Specific Distribution
The distribution of culture-positive specimens and multidrug-resistant organisms (MDROs) by hospital ward is shown in Table 2.
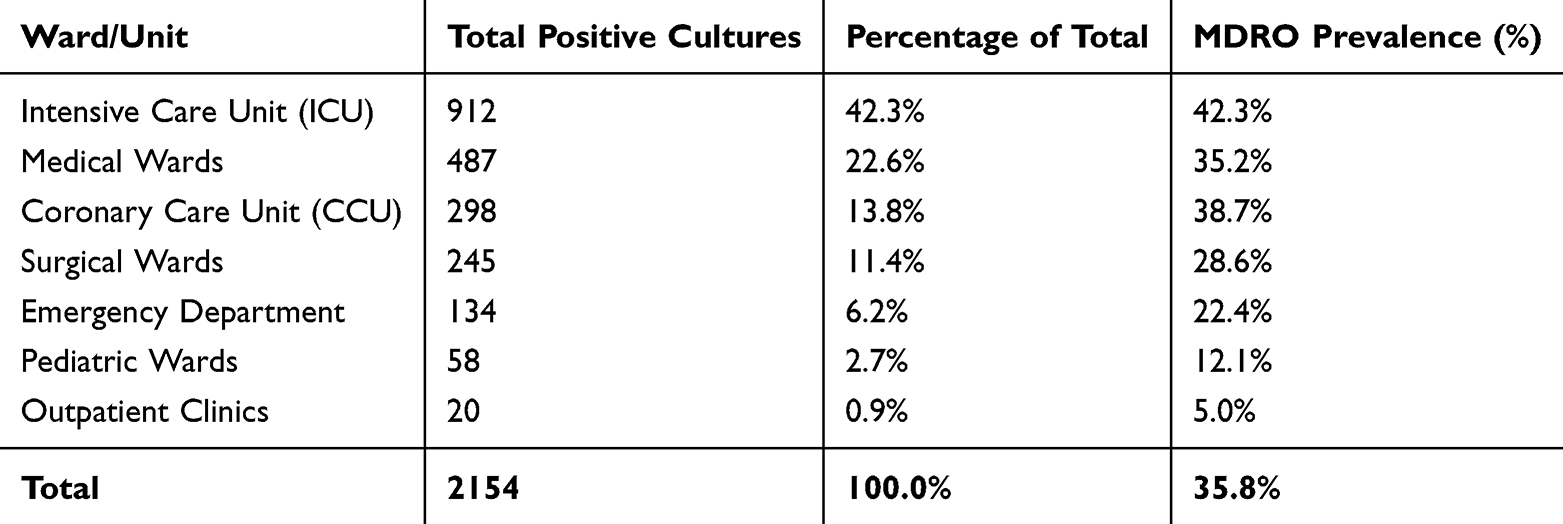 |
Table 2 Ward-Specific Distribution of Culture-Positive Specimens and MDRO Prevalence |
The ICU contributed 42.3% of all culture-positive isolates and demonstrated the highest MDRO prevalence among positive ICU cultures (42.3%), followed by the CCU (38.7%) and medical wards (35.2%). High-acuity units (ICU, CCU, and medical wards) accounted for 78.7% of all positive cultures and 82.4% of all MDROs.
Antimicrobial Resistance Patterns
Gram-Negative Pathogens
Antimicrobial resistance profiles of major Gram-negative pathogens are summarized in Table 3. MDROs were highly prevalent, including, carbapenem-resistant organisms (22.9%) and ESBL producers (12.3%).
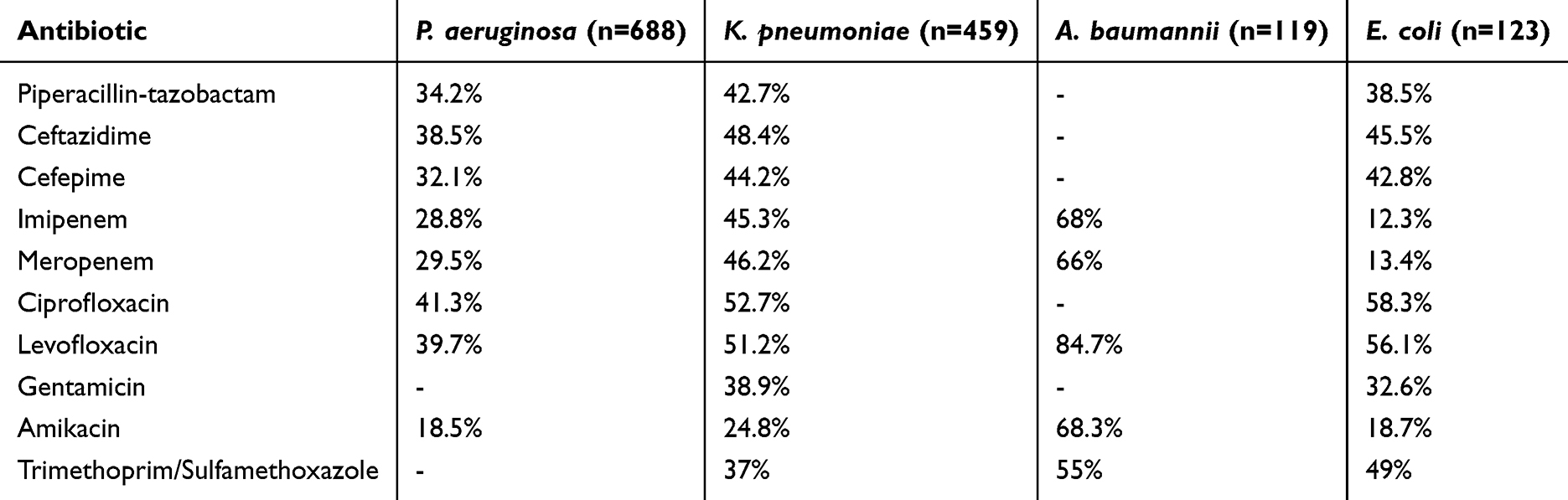 |
Table 3 Antimicrobial Resistance Rates for Major Gram-Negative Pathogens |
Carbapenem resistance rates were 32.5% for Klebsiella pneumoniae, and 4.9% for Escherichia coli.
ESBL positivity was observed in 18.9% (87/459) of Klebsiella pneumoniae isolates and 65.9% (81/123) of Escherichia coli isolates.
Multidrug resistance was detected in 68% (81/119) of Acinetobacter baumannii, 58.2% (267/459) of Klebsiella pneumoniae, 42.7% (294/688) of Pseudomonas aeruginosa, and 38.2% (47/123) of Escherichia coli isolates.
Gram-Positive Pathogens
Antimicrobial resistance patterns among Gram-positive pathogens are summarized in Table 4.
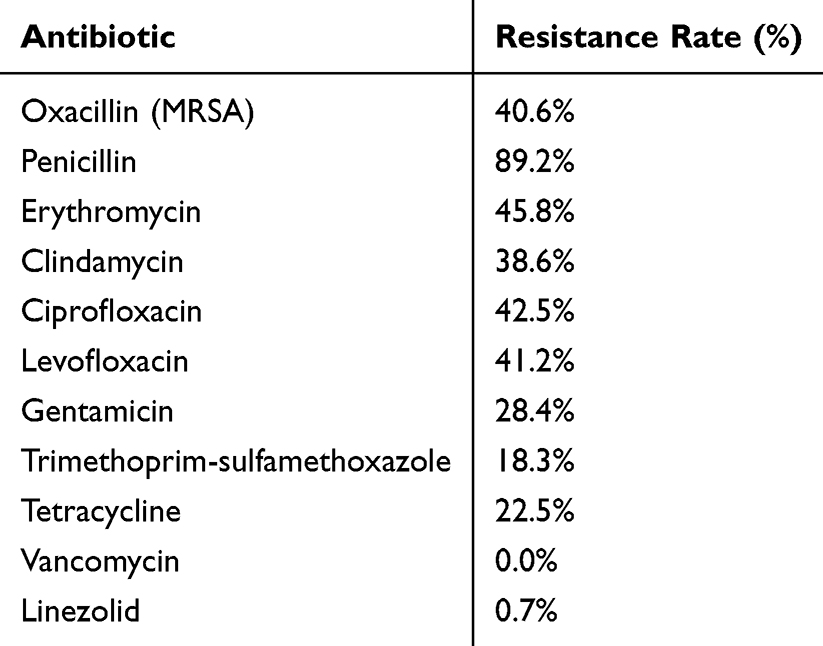 |
Table 4 Antimicrobial Resistance Rates for Staphylococcus aureus (n=306) |
Among Staphylococcus aureus isolates, 40.6% (89/219) were methicillin-resistant. Resistance to vancomycin and linezolid was rare, with susceptibility rates exceeding 99%. Fluoroquinolone resistance ranged from 41% to 43%, and penicillin resistance was observed in 89.2% of isolates.
All Streptococcus pneumoniae isolates were susceptible to vancomycin, linezolid, and levofloxacin, whereas 22.2% and 5.9% exhibited non-susceptibility to penicillin and ceftriaxone, respectively.
Seasonal and Temporal Dynamics
Monthly and Seasonal Variation
Monthly culture positivity rates ranged from 32.1% to 45.8% and demonstrated significant seasonal variation (p<0.001) (Table 5).
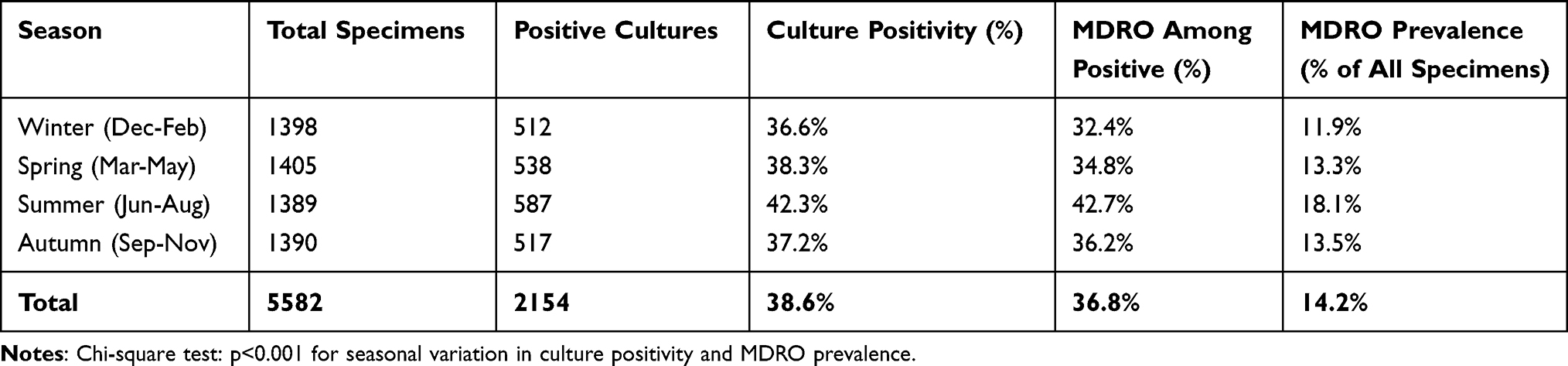 |
Table 5 Seasonal Distribution of Culture Positivity and MDRO Prevalence |
Culture positivity was higher during summer (42.3%) than winter (36.6%) (OR 1.27, 95% CI: 1.09–1.48, p=0.002). MDRO prevalence also increased during summer (42.7%) compared with winter (32.4%) (OR 1.56, 95% CI: 1.26–1.93, p<0.001).
Seasonal Variation in Carbapenem Resistance
Seasonal distributions of carbapenem-resistant Gram-negative pathogens are presented in Table 6.
 |
Table 6 Seasonal Variation in Carbapenem-Resistant Gram-Negative Pathogens |
Carbapenem-resistant Gram-negative pathogens increased from 18.2% in winter to 28.7% in summer (OR 1.82, 95% CI: 1.45–2.28, p<0.001).
Meropenem resistance in Pseudomonas aeruginosa increased from 24.1% in winter to 35.8% in summer (OR 1.76, 95% CI: 1.28–2.42, p<0.001), while carbapenem resistance in Klebsiella pneumoniae increased from 40.2% to 52.7% (OR 1.66, 95% CI: 1.18–2.33, p=0.003).
Temporal Trends
Overall culture positivity remained stable during the study period at 37.8% in 2023, 38.9% in 2024, and 39.1% in 2025 (p=0.54).
MDRO prevalence increased from 33.2% in 2023 to 37.8% in 2024 and 38.4% in 2025 (p=0.02). Carbapenem resistance in Pseudomonas aeruginosa increased from 26.3% to 31.8% over the study period (p=0.04), whereas carbapenem resistance in Klebsiella pneumoniae remained stable (p=0.62). MRSA prevalence decreased from 41.2% in 2023 to 35.7% in 2025, although this trend was not statistically significant (p=0.18).
MDRO Burden by Ward and Season
MDRO prevalence stratified by ward and season is presented in Table 7. The highest MDRO prevalence was observed among ICU isolates during the summer (48.7%), compared with 38.2% during the winter (OR 1.54, 95% CI: 1.18–2.01, p=0.001).
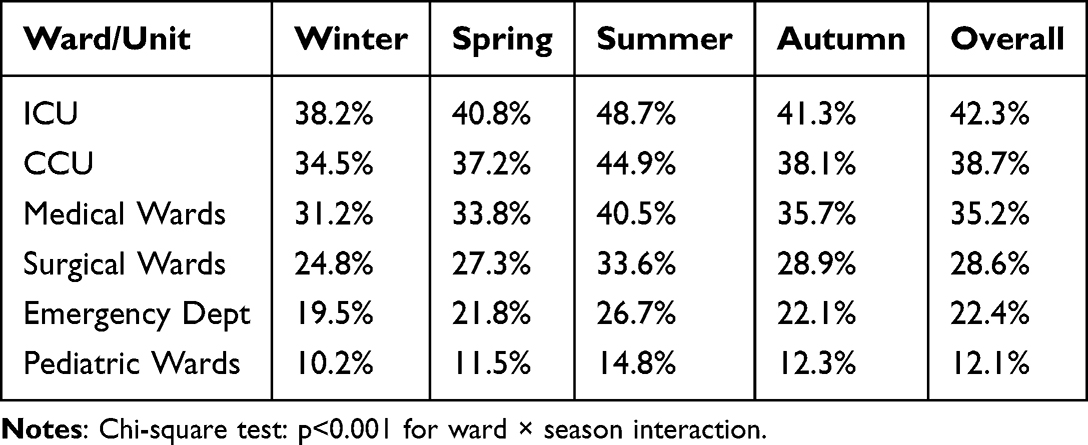 |
Table 7 MDRO Prevalence by Ward and Season (% of Positive Cultures) |
Discussion
This study provides comprehensive surveillance data on respiratory bacterial pathogens and antimicrobial resistance in a tertiary care hospital in Riyadh, Saudi Arabia. The principal findings were the predominance of Gram-negative pathogens, the high burden of multidrug resistance, particularly among A. baumannii and K. pneumoniae, and the significant seasonal increase in multidrug-resistant organisms during summer months.
Pathogen Distribution and Antimicrobial Resistance
Pseudomonas aeruginosa and Klebsiella spp. were the most frequently isolated pathogens, consistent with reports from hospitalized patients with respiratory infections in Saudi Arabia and other regions.11–13 The predominance of Gram-negative organisms, particularly among older patients and critically ill individuals, highlights their important role in healthcare-associated respiratory infections.
A major finding was the high prevalence of antimicrobial resistance among Gram-negative pathogens. Carbapenem resistance was observed in 32.5% of K. pneumoniae isolates and 4.9% of E. coli isolates, while multidrug resistance affected nearly 68% of A. baumannii isolates. These findings are consistent with reports from regional studies documenting substantial resistance among respiratory pathogens in intensive care settings.12,26
It is important to note that carbapenem resistance identified in this study was based on phenotypic susceptibility testing and does not necessarily indicate carbapenemase production. Multiple mechanisms may contribute to carbapenem resistance, including the production of carbapenemases, alterations in outer membrane permeability due to porin loss, efflux pump overexpression, and AmpC or ESBL production in combination with reduced membrane permeability. As molecular characterization and confirmatory carbapenemase detection assays were not performed, the specific resistance mechanisms could not be determined. Therefore, the carbapenem-resistant isolates reported in this study should be interpreted as phenotypically resistant organisms rather than confirmed carbapenemase producers.
Among Gram-positive organisms, MRSA accounted for 40.6% of S. aureus isolates, while vancomycin and linezolid retained excellent activity. These findings support the continued effectiveness of these agents for the treatment of serious Gram-positive respiratory infections.12,36,40
Seasonal Dynamics of Resistance
One of the most important findings of this study was the significant seasonal variation in antimicrobial resistance. Carbapenem-resistant Gram-negative pathogens increased from 18.2% in the winter to 28.7% in the summer, accompanied by a higher prevalence of MDROs during the summer months. Similar seasonal patterns have been reported in studies evaluating resistant Gram-negative pathogens, although the magnitude and timing of these fluctuations vary across geographic regions and healthcare settings.26,28–33 The mechanisms underlying these seasonal trends remain uncertain and may involve environmental conditions, antimicrobial prescribing patterns, patient case mix, and healthcare-associated transmission. Further studies incorporating environmental and antimicrobial consumption data are needed to better understand these observations.
Ward-Specific Burden and Clinical Implications
The highest MDRO burden was observed in ICU and other high-acuity units, which accounted for the majority of resistant isolates. This finding is consistent with the greater antimicrobial exposure, severity of illness, and invasive device utilization commonly encountered in these settings.11,41 The concentration of resistant pathogens in high-acuity wards highlights the importance of continuous surveillance, antimicrobial stewardship, and infection prevention measures targeted to these high-risk areas.
Strengths and Limitations
The major strengths of this study include the large sample size, inclusion of multiple respiratory specimen types, three years of continuous surveillance, and evaluation of seasonal resistance patterns. These data provide valuable baseline information on respiratory pathogen epidemiology and antimicrobial resistance in a Saudi tertiary care hospital.
A limitation of this study is the absence of molecular confirmation of antimicrobial resistance mechanisms. Resistance phenotypes were identified using routine laboratory methods, and therefore the specific genes responsible for carbapenem resistance and ESBL production could not be determined.
Conclusion
This study demonstrates a substantial burden of multidrug-resistant respiratory pathogens in a tertiary care hospital in Riyadh, Saudi Arabia, with Gram-negative bacteria accounting for most infections and resistance concentrated in high-acuity units. Carbapenem resistance was observed among major respiratory pathogens, particularly Klebsiella pneumoniae and E. coli. A notable finding was the significant seasonal variation in resistance patterns, with higher prevalence of multidrug-resistant organisms and carbapenem-resistant Gram-negative pathogens during the summer months. These findings highlight the importance of continuous local surveillance, antimicrobial stewardship, and targeted infection prevention measures to mitigate the spread of resistant respiratory pathogens and support evidence-based empirical therapy.
Future Directions
Future studies should incorporate molecular characterization of resistance mechanisms, multicenter surveillance, and linkage of microbiological findings with clinical outcomes. Additional investigations are warranted to better understand the environmental, epidemiological, and healthcare-related factors contributing to the observed seasonal variation in antimicrobial resistance.
Data Privacy and Confidentiality
All patient data were de-identified prior to extraction from the laboratory information system and electronic medical records. No protected health information (names, medical record numbers, dates of birth, addresses, or other identifiers) was included in the study dataset. Data were stored on password-protected institutional servers with access restricted to authorized study personnel. Data analysis was performed on de-identified datasets only.
Data Security
Electronic data were stored on secure, password-protected servers maintained by the hospital information technology department with regular backups and encryption. Access to the dataset was limited to study investigators and authorized research personnel. No data were transferred outside the institution except in de-identified, aggregated form for publication.
Data Sharing Statement
De-identified aggregate data supporting the findings of this study are available from Dr. Ahmed J Alzahrani, the corresponding author upon reasonable request and subject to institutional data sharing policies. Individual patient-level data cannot be shared due to privacy regulations.
Ethical Approval
This study was approved by the Institutional Review Board (IRB) of Dr. Sulaiman Alhabib Medical Group (RC 25.08.75). The study protocol, data collection procedures, and analysis plan were reviewed and approved prior to study initiation.
Informed Consent
As a retrospective analysis of de-identified laboratory surveillance data collected as part of routine clinical care, the requirement for informed consent was waived by the IRB in accordance with local regulations and international ethical guidelines (Declaration of Helsinki, 2013 revision). No patient contact or intervention occurred as part of this study.
Acknowledgments
The authors thank the microbiology laboratory staff at Dr. Sulaiman Alhabib Hospital for their dedication to high-quality specimen processing and antimicrobial susceptibility testing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study received no funding.
Disclosure
The authors declare no conflicts of interest related to this study. No financial or personal relationships with organizations or individuals that could inappropriately influence this work.
References
1. Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61–13. doi:10.1093/cid/ciw353
2. Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia. Eur Respir J. 2017;50(3):1700582. doi:10.1183/13993003.00582-2017
3. Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
4. Cassini A, Högberg LD, Plachouras D, et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis. Lancet Infect Dis. 2019;19(1):56–66. doi:10.1016/S1473-3099(18)30605-4
5. Tacconelli E, Carrara E, Savoldi A, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18(3):318–327. doi:10.1016/S1473-3099(17)30753-3
6. Murray CJL, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
7. Zowawi HM, Harris PN, Roberts MJ, et al. The emerging threat of multidrug-resistant Gram-negative bacteria in urology. Nat Rev Urol. 2015;12(10):570–584. doi:10.1038/nrurol.2015.199
8. Alshehry AS. Antibiotic-Resistant Bacteria in Intensive Care Units in Saudi Arabia: a Systematic Review. Middle East J Nurs. 2024;18(1):45–58.
9. Liu J, Li Y, Liu T; Pathogen Burden Among Intensive Care Unit Patients in Hail. Saudi Arabia: a Retrospective Study. Infect Drug Resist. 2023;16:3847–3858. doi:10.2147/IDR.S415830
10. Kabrah A, Khamjan NA, Alghamdi S, et al. Extended-spectrum beta-lactamase and carbapenem-resistant enterobacteriaceae in Makkah, Saudi Arabia. Ethiop J Health Sci. 2022;32(3):571–580. doi:10.4314/ejhs.v32i3.14
11. Abdalla J, Saad H, Sadeq A, et al. Narrative review of hospital-acquired pneumonia and ventilator-associated pneumonia in Gulf cooperation council countries: current status and future perspectives. Infect Dis Ther. 2023;12(5):1289–1312. doi:10.1007/s40121-023-00801-4
12. Maraki S, Stafylaki D, Kasimati A, Kapsetaki M, Scoulica E. Prevalence and Antimicrobial Resistance Trends among Lower Respiratory Tract Pathogens in Crete, Greece, 2017-2022. Infect Chemother. 2024;56(3):345–358. doi:10.3947/ic.2024.0060
13. Dung TTN, Phat VV, Vinh PV, et al. The bacterial etiology and antimicrobial susceptibility of lower respiratory tract infections in Vietnam. Ann Clin Microbiol Antimicrob. 2025;24:12. doi:10.1186/s12941-025-00818-3
14. Hammoudi Halat D, Ayoub Moubareck C. The current burden of carbapenemases: review of significant properties and dissemination among Gram-negative bacteria. Antibiotics. 2020;9(4):186. doi:10.3390/antibiotics9040186
15. Nordmann P, Poirel L. Epidemiology and diagnostics of carbapenem resistance in Gram-negative bacteria. Clin Infect Dis. 2019;69(Suppl 7):S521–S528. doi:10.1093/cid/ciz824
16. Peirano G, Pitout JDD. Extended-spectrum β-lactamase-producing enterobacteriaceae: update on molecular epidemiology and treatment options. Drugs. 2019;79(14):1529–1541. doi:10.1007/s40265-019-01180-3
17. Turner NA, Sharma-Kuinkel BK, Maskarinec SA, et al. Methicillin-resistant Staphylococcus aureus: an overview of basic and clinical research. Nat Rev Microbiol. 2019;17(4):203–218. doi:10.1038/s41579-018-0147-4
18. Poole K. Pseudomonas aeruginosa: resistance to the max. Front Microbiol. 2011;2:65. doi:10.3389/fmicb.2011.00065
19. Asokan S, Jacob T, Jacob J, et al. Klebsiella pneumoniae: a growing threat in the era of antimicrobial resistance. Microbe. 2025;7:100333. doi:10.1016/j.microb.2025.100333
20. Asokan S, Jacob T, Jacob J, AlSosowaa AA, Vijayan S. Trends in antimicrobial susceptibility patterns of Klebsiella pneumoniae isolated from clinical samples at a tertiary care hospital in Kerala, India. Next Research. 2025;2(3):100654. doi:10.1016/j.nexres.2025.100654
21. Asokan S, Jacob T, Cherian T, et al. HR-LCMS profiling, in vitro and in silico assessment of the antibacterial activities of endophytic Bacillus amyloliquefaciens NWR-14 from Piper chaba W. Hunter. Phytomedicine Plus. 2025;5(4):100885. doi:10.1016/j.phyplu.2025.100885
22. Asokan S, Sony S, Jacob T, Jisha MS, Vijayan S. Biogenic ZnO nanoparticle-coated endotracheal tubes: a study on their biocompatibility and antibacterial activity. Next Nanotechnol. 2025;8:100274. doi:10.1016/j.nxnano.2025.100274
23. Asokan S, Jacob T, Cherian T, AlSosowaa AA, Al-Mojahid FQ, Vijayan S. Biogenic ZnO nanoparticles from bacillus amyloliquefaciens NWR-14 for combating ESBL-producing Klebsiella pneumoniae. Biomed Mater Device. 2026;10:1–25.
24. Asokan S, Pandey RK, Jalil MA, et al. Biofilm associated infections on medical devices: pathogenesis, diagnostic challenges, and control strategies. Microbe. 2026;3:100712. doi:10.1016/j.microb.2026.100712
25. Asokan S, Banerjee N, Saleem M, et al. Healthcare associated infections (HAI): insights into epidemiology, microbiology, and diagnostics. Diagnostic Microbiol Infect Dis. 2026;12(3):117376. doi:10.1016/j.diagmicrobio.2026.117376
26. Ito K, Imai S, Nakamura R, Matsumoto T. Analysis of drug-resistant bacteria seasonality in Japan using financial time series analysis method: a nationwide longitudinal study. Can J Infect Dis Med Microbiol. 2025;2025:5590467. doi:10.1155/cjid/5590467
27. Fisman DN. Seasonality of infectious diseases. Annu Rev Public Health. 2007;28:127–143. doi:10.1146/annurev.publhealth.28.021406.144128
28. Burnham JP, Olsen MA, Stwalley D, et al. Infectious diseases society of America emerging infections network survey of the epidemiology of Acinetobacter baumannii infections in the United States. Open Forum Infect Dis. 2019;6(4):ofz034. doi:10.1093/ofid/ofz034
29. Liu XX, Li YH, Wang L, et al. Seasonal variation in meropenem resistance of Acinetobacter baumannii: a retrospective study. BMC Microbiol. 2024;24:89. doi:10.1186/s12866-024-03241-8
30. Itani R, Karout L, Fadlallah S, et al. Incidence and risk factors of difficult-to-treat resistant Pseudomonas aeruginosa infection in Lebanon: a case-control study. BMC Infect Dis. 2025;25:89. doi:10.1186/s12879-025-10389-4
31. Gupta V, Ye G, Olesky M, Lawrence K, Murray J, Yu K. National prevalence estimates for resistant Pseudomonas aeruginosa and Acinetobacter baumannii and the association with influenza season. Open Forum Infect Dis. 2022;9(7):ofac255. doi:10.1093/ofid/ofac255
32. Güvenir M, Kayacan CB, Köksal F. Seasonal changes and effect of climate on acinetobacter infections. Pol J Environ Stud. 2021;30(3):2479–2486. doi:10.15244/pjoes/128518
33. Ben-Amram H, Borer A, Valinsky L, et al. Biofilm formation by hospital-acquired resistant bacteria isolated from respiratory samples. J Epidemiol Glob Health. 2024;14(2):215–223. doi:10.1007/s44197-024-00215-7
34. bioMérieux. VITEK® 2 Compact: Product Information and Operating Manual. Marcy-L’étoile. France: bioMérieux; 2020.
35. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing; 35th Informational Supplement. CLSI Document M100-S35.Wayne, PA: CLSI. 2025.
36. Ingravalle F, Sanguinetti M, Posteraro B, et al. time trends in prevalence and antimicrobial resistance of respiratory pathogens in a tertiary hospital in Rome, Italy: a retrospective analysis (2018-2023). Antibiotics. 2025;14(9):932. doi:10.3390/antibiotics14090932
37. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
38. Zaiontz C. Real Statistics Resource Pack for Excel. In: Real Statistics Using Excel Website. 2023. Available from: https://www.real-statistics.com/
39. Abdul Rahman H, Noraidi AA, Hj Khalid AN, Mohamad-Adam AZ, Zahari NH, Tuming NE. Practical guide to calculate sample size for chi-square test in biomedical research. BMC Med Res Methodol. 2025;25:144. doi:10.1186/s12874-025-02584-4
40. Bazira J, Asiimwe BB, Najjuka CF, et al. Seven-year surveillance of antimicrobial resistance in respiratory pathogens at a Ugandan referral hospital: emerging trends and stewardship priorities. Afr J Thorac Crit Care Med. 2025;31(4):e3495. doi:10.7196/AJTCCM.2025.v31i4.3495
41. Halat DH, Moubareck CA, Sarkis DK. Hospital-acquired and ventilator-associated pneumonia caused by multidrug-resistant Gram-negative pathogens: understanding epidemiology, resistance patterns, and implications with COVID-19. F1000Res. 2024;12:1277. doi:10.12688/f1000research.129080.2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Molecular Characterization of Klebsiella pneumoniae Isolated from Sputum in a Tertiary Hospital in Xinxiang, China
Hao Y, Jiang Y, Ishaq HM, Liu W, Zhao H, Wang M, Yang F
Infection and Drug Resistance 2022, 15:3829-3839
Published Date: 18 July 2022
Relationship Between Drug Resistance Characteristics and Biofilm Formation in Klebsiella Pneumoniae Strains
Dan B, Dai H, Zhou D, Tong H, Zhu M
Infection and Drug Resistance 2023, 16:985-998
Published Date: 17 February 2023
Healthcare Workers’ Knowledge, Awareness, and Practices Regarding Antimicrobial Use, Resistance, and Stewardship in Saudi Arabia
Abdallah MS, Al Meanazel OT, Alruwaili MM, AlRasheed HA
Infection and Drug Resistance 2025, 18:6035-6050
Published Date: 19 November 2025
Hospital-Based Surveillance of Klebsiella pneumoniae and Other Klebsiella species in Southern Saudi Arabia (2012–2024): Escalating Carbapenem and DTR Resistance with Species-Specific Phenotypes and Genotypes
Shabi Y, Algarni AM, Binkhamis K, Al Bshabshe A, Alazraqi T, Abdullah Mohammed S, Habbash S, Alqahtani AJ, Basheer NA, Alhazmi AH, Patriquin G, Bawazeer AO, Tahtouh EI
Infection and Drug Resistance 2026, 19:554543
Published Date: 4 February 2026
Antimicrobial Resistance in Intensive Care Units in Somalia: A Commentary on Measurement Gaps and Facility-Level Priorities for Infection Prevention and Stewardship
Hassan AM, Siyad AO, Hussein AM
Infection and Drug Resistance 2026, 19:606434
Published Date: 18 May 2026