Back to Journals » Drug Design, Development and Therapy » Volume 19
Enhancing Diabetes Treatment: Comparing Pioglitazone/Metformin with Dapagliflozin Versus Basal Insulin/Metformin in Type 2 Diabetes
Authors Lin Y, Shi J ![]() , Yu X, Sun J, Lixia S, Dou J, Zhang M
, Yu X, Sun J, Lixia S, Dou J, Zhang M ![]() , Li X
, Li X ![]() , Tian Z, Deng H, Feng B, Su Q, Peng Y
, Tian Z, Deng H, Feng B, Su Q, Peng Y
Received 17 December 2024
Accepted for publication 1 March 2025
Published 12 March 2025 Volume 2025:19 Pages 1795—1808
DOI https://doi.org/10.2147/DDDT.S512872
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Yi Lin,1,* Jianxia Shi,1,* Xuemei Yu,2 Jiao Sun,3 Suo Lixia,4 Jiaqing Dou,5 Min Zhang,6 Xiaohua Li,7 Zhufang Tian,8 Hongyan Deng,9 Bo Feng,10 Qing Su,11 Yongde Peng1
1Department of Endocrinology and Metabolism, Shanghai General Hospital, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Central Hospital of Fengxian District, Shanghai, People’s Republic of China; 3Huadong Hospital Affiliated to Fudan University, Shanghai, People’s Republic of China; 4Shanghai Jiading Central Hospital, Shanghai Jiading Central Hospital, Shanghai, People’s Republic of China; 5Chaohu Hospital of Anhui Medical University, Chaohu, People’s Republic of China; 6Qingpu Branch of Zhongshan Hospital Affiliated to Fudan University, Shanghai, People’s Republic of China; 7Seventh People’s Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 8Xi‘an Central Hospital, Xi’an, Shanxi, People’s Republic of China; 9Wuhan Fourth Hospital, Wuhan, People’s Republic of China; 10Dongfang Hospital Affiliated to Tongji University, Shanghai, People’s Republic of China; 11Xinhua Hospital Affiliated to Shanghai Jiaotong University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongde Peng, Department of Endocrinology and Metabolism, Shanghai General Hospital, Shanghai Jiao Tong University, 100 haining Road, Shanghai, 200080, People’s Republic of China, Tel +86-13386259649, Email [email protected]
Aim: The aim of this study was to compare the efficacy and safety of fixed-dose combination (FDC) of pioglitazone and metformin supplemented with dapagliflozin (test group) with those of basal insulin supplemented with metformin (control group) in patients with inadequately controlled type 2 diabetes mellitus (T2DM).
Methods: This 16-week, prospective, randomized, open-label study enrolled patients aged 18– 75 years with glycated hemoglobin (HbA1c) levels between ≥ 8% and ≤ 11%. The primary endpoint was the proportion of patients who achieved HbA1c < 7% at week 16 without hypoglycemia or weight gain. The secondary endpoints included blood glucose, lipid profile, body weight, body mass index, inflammatory markers, bone Gla-protein, liver enzymes, and patient satisfaction.
Results: Among the full analysis set of 147 participants, no significant difference was observed in the primary endpoint between the test group and the control group. However, the test group had a higher percentage of patients who achieved HbA1c < 7% at week 16 without hypoglycemia and experienced a weight loss of ≥ 3% (31.51% vs 13.51%, P=0.009). Patients in the test group whose BMI≥ 24 kg/m2 also achieved a substantial achievement rate (36.73% vs 15.79%, P=0.014). The test group also exhibited a greater reduction in body weight and improvements in 2-hour postprandial glucose level, systolic blood pressure, and lipid profile. Notably, combination therapy did not increase the risk of hypoglycemia or weight gain. Patients in the test group were more satisfied than those in the control group with continuing to accept pioglitazone/metformin FDC combined with dapagliflozin.
Conclusion: In the absence of contraindications, pioglitazone/metformin FDC supplemented with dapagliflozin may serve as a safe and effective alternative to basal insulin combined with metformin for rectifying inadequate glucose control, as the former enables metabolic improvements without compromising safety.
Chinese Clinical Trial Registry Number: CHiCTR 2000036076. https://www.chictr.org.cn/showproj.html?proj=58825.
Keywords: dapagliflozin, pioglitazone/metformin FDC, type 2 diabetes, metformin, insulin
Introduction
Type 2 diabetes mellitus (T2DM) is a chronic metabolic disorder that affects millions of people worldwide and requires lifelong treatment. Metformin is a commonly used oral hypoglycemic agent that can be used in combination with many other hypoglycemic agents. Current guidelines recommend that metformin treatment be continued after the initiation of insulin (usually basal insulin) treatment,1,2 as it improves glycemic control, reduces the overall insulin dose required more effectively than insulin alone,3 without increasing the incidence of hypoglycemia and weight gain.4,5 In China, patients with T2DM who had previously experienced inadequate glycemic control with oral antidiabetic drugs showed improved glycemic control, potentially required lower insulin doses, and experienced less weight gain after adopting basal insulin therapy with metformin compared to those who underwent basal insulin therapy without metformin.6
While the timely addition of insulin to oral therapy for T2DM has been recommended for preventing complications by providing strict glycemic control and β-cell protection, a significant number of patients who suffer from inadequate glucose control delay insulin therapy because of concerns about hypoglycemia, weight gain, or injection administration, and such concerns might also negatively impact patient adherence to insulin therapy.7 As T2DM is a progressive disease, the initial therapy frequently proves inadequate in achieving optimal glycemic control, necessitating the use of add-on therapies. Fixed-dose combination (FDC) therapy can be an invaluable tool for helping patients effectively meet glycemic targets.8 To improve treatment outcomes and patient compliance, combination of pioglitazone and metformin or their FDC has been proven a greater reductions in glucose level, with no increase in adverse events (AEs), than when the individual therapies are used separately.9–11 Moreover, in a study of treatment-naïve patients with T2DM, pioglitazone/metformin FDC was shown to have similar or more favorable effects on circulating biomarkers of cardiovascular disease (CVD) compared with each monotherapy.12
Pioglitazone, an antidiabetic drug in the thiazolidinedione (TZD) class, is often used in combination with metformin to improve insulin sensitivity. It selectively activates peroxisome proliferator-activated receptor gamma (PPARγ), thereby regulating the transcription of multiple insulin-related genes involved in glucose and lipid metabolism.13 While pioglitazone exerts significant effects in diabetes treatment, there are concerns about potential adverse reactions to this drug, such as edema and weight gain.14 Edema formation may be related to the specific mechanisms of TZDs, such as vascular permeability and fluid retention,15 while weight gain may be associated with the expression of PPARγ in various tissues and fat redistribution.16,17
Dapagliflozin, a hypoglycemic agent commonly used in clinical practice, reduces renal glucose reabsorption by inhibiting sodium–glucose cotransporter 2 (SGLT-2), thus lowering the renal threshold for glucose, promoting the excretion of excess glucose in the urine, effectively improving fluid retention, and accelerating heat consumption in the body.18 Recent studies have shown that the combination of pioglitazone and dapagliflozin not only reduces glycated hemoglobin (HbA1c) levels in patients with T2DM, alleviates oxidative stress, and reduces the risk of ketoacidosis and hypoglycemia, but also mitigates edema and fluid retention and improves weight gain issues caused by pioglitazone.19,20
The combination of pioglitazone/metformin FDC and dapagliflozin is believed to effectively control glycometabolism and reduce the incidence of weight gain and edema. While one study compared the use of pioglitazone/metformin FDC and dapagliflozin to a placebo,21 no studies have yet compared the use of this FDC to that of insulin combined with metformin. Therefore, this study aimed to compare the effectiveness and safety of pioglitazone/metformin FDC supplemented with dapagliflozin to those of basal insulin supplemented with metformin in patients with T2DM and inadequate glycemic control.
Materials and Methods
Study Design
A 16-week, randomized, controlled, multicenter, open-label clinical trial was conducted at 11 hospitals in China. The primary trial center was Shanghai First People’s Hospital. Collaborating trial centers included Shanghai Tongji University Affiliated Dongfang Hospital, Shanghai Jiao Tong University School of Medicine Affiliated Xinhua Hospital, Fudan University Affiliated Huadong Hospital, Shanghai University of Traditional Chinese Medicine Affiliated Seventh People’s Hospital, Shanghai Fengxian District Central Hospital, Fudan University Affiliated Zhongshan Hospital Qingpu Branch, Beijing Wangjing Hospital, the China Academy of Chinese Medical Sciences, Shaanxi Provincial People’s Hospital, and Hubei Shiyan Taihe Hospital. At these 11 centers, the researchers strictly adhered to the inclusion and exclusion criteria set by the primary center, and all participants were fully informed about their physical conditions, disease diagnoses, and treatment plans, as well as the potential risks and complications that may arise during the study process. Prior to the start of the trial, the protocol was registered (Chinese Clinical Trial Registration Number: CHiCTR2000036076).
The aim was to compare the efficacy and safety of pioglitazone/metformin FDC supplemented with dapagliflozin to those of basal insulin combined with metformin in patients with poorly controlled T2DM. The data were collected in accordance with a standardized protocol to ensure accuracy and completeness. Abnormal values were carefully reviewed and processed to ensure the data’s reliability. All data were anonymized to protect the privacy of the subjects.
This study was approved by the Ethics Committee of Shanghai General Hospital (Approval Number: [2022]102) and by other medical centers. All study procedures were conducted in accordance with the Helsinki Declaration of 1964 (as revised in 2013). All subjects signed an informed consent form after being made fully aware of the research content and risks. To ensure the quality and reliability of the study, we adopted a series of quality control measures, including regular training and assessment of research personnel, calibration and maintenance of the experimental equipment, and strict quality checks of the experimental data.
Participants
Between December 6, 2020, and September 3, 2021, 201 patients underwent eligibility screening, with 153 patients ultimately included in the randomization. Using an interactive web response system, the patients were randomly assigned to a group that received pioglitazone/metformin FDC combined with dapagliflozin (78 patients) or to a group administered basal insulin combined with metformin (75 patients). Once participants without medication records were excluded, 74 and 73 patients were ultimately included in the full analysis set (FAS), respectively (Figure 1).
 |
Figure 1 Patient flow. |
The inclusion criteria for the trial specified participants aged between 18 and 75 years who were newly diagnosed (within three months prior to enrollment and without pharmacological treatment) or had been previously treated with hypoglycemic agents for a duration of ≥ 3 months (excluding those who had used thiazolidinediones, SGLT-2 inhibitors, insulin, or more than three oral hypoglycemic agents in the past six months) and, in both cases, had poorly controlled glycemia, represented by HbA1c levels between 8.00% (60.60 mmol/mol) and 11.00% (83.30 mmol/mol). The exclusion criteria ruled out patients with type 1 diabetes or other special types of diabetes, abnormal liver function, renal impairment, pregnancy, fasting C-peptide levels ≤ 400 pmol/L, severe chronic gastrointestinal diseases, severe heart disease, or hypertension.
Intervention Measures and Control Conditions
The subjects in the test group underwent a 16-week treatment with the pioglitazone/metformin FDC (15 mg/500 mg; produced by Hangzhou Zhongmei Huadong Pharmaceutical Co., Ltd), which was taken three times daily with meals until the end of the 16-week follow-up. If the patients could not tolerate the full dose, the frequency was reduced to twice daily and then adjusted back to three times daily based on the patient’s specific condition. Additionally, dapagliflozin (10 mg, AstraZeneca) was administered once daily, at an initial dose of 5 mg per week for the first week, followed by an increase to 10 mg from the second week onward until the end of the 16-week follow-up.
Subjects in the control group received a 16-week treatment consisting of insulin-based therapy combined with metformin hydrochloride for glycemic control. Specifically, metformin hydrochloride tablets (500 mg, Merck & Co., Inc). were taken three times daily with meals for 16 weeks (or twice a day if not well tolerated). Additionally, insulin glargine was administered via subcutaneous injections before bedtime, with an initial dose of 10 IU per day for the first three days. Subsequently, the dose was adjusted every three days based on the patient’s self-measured fasting blood glucose level. The medication was continued for 16 weeks, with insulin dose adjustments based on fasting blood glucose levels: 2 IU of insulin were upregulated for 5.60–6.60 mmol/L, + 4 IU for 6.70–7.70 mmol/L, + 6 IU for 7.80–9.90 mmol/L, and + 8 IU for ≥ 10.00 mmol/L.
During the study, patients were advised to maintain their usual diet and physical activity levels as per their baseline habits. Calorie intake and physical exercise were not strictly controlled but were monitored through regular follow-ups to ensure no significant changes occurred that could affect the study outcomes.
Observational Indicators and Outcome Measures
Before enrollment and at the end of the 16th week, HbA1c and fasting C-peptide levels were measured, blood and urine routines were performed, and blood biochemistry and electrocardiogram results (ECG) were evaluated. Inflammatory markers, 2-hour postprandial blood glucose (2h PPBG), brain natriuretic peptide (BNP), and bone Gla-protein (BGP) levels were recorded at weeks 0, 12, and 16. Fasting venous blood glucose levels were recorded upon enrollment, at week 0, and at week 16. Fasting capillary blood glucose levels were recorded at weeks 4, 8, and 12.
The primary endpoint of this study was the proportion of participants who achieved a composite endpoint at week 16, defined as HbA1c < 7% (53.00 mmol/mol) without hypoglycemia or weight gain. Secondary endpoints included HbA1c, fasting blood glucose, 2h PPBG, fasting C-peptide, homeostatic model assessment of insulin resistance (Homa-IR) results, homeostatic model assessment of beta-cell function (Homa-islet) results, diastolic blood pressure (DBP), and systolic blood pressure (SBP); lipid profiles, including triglycerides (TG), total cholesterol (TC), free fatty acids (FFA), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C); and inflammatory markers, including C-reactive protein (CRP) and interleukin-6 (IL-6) levels, body weight, body mass index (BMI), BNP, ECG, BGP, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and echocardiogram results (Echo). Hypoglycemia in this study was categorized as follows: 1) Severe hypoglycemia: This refers to a condition in which patients require assistance from others to obtain carbohydrates, glucagon, or other resuscitative measures. 2) Documented symptomatic hypoglycemia: This occurs when patients exhibit typical symptoms of hypoglycemia, and their plasma glucose concentration is less than or equal to 70 mg/dL (3.90 mmol/L). 3) Asymptomatic hypoglycemia: This refers to a condition in which patients do not exhibit typical symptoms of hypoglycemia, but their blood glucose level is still less than or equal to 70 mg/dL (3.90 mmol/L). Other endpoints included liver function, incidence of AEs (adverse gastrointestinal reactions, edema, and other AEs judged by the investigators to be related to the treatment medication), and diabetes treatment satisfaction (based on Diabetes Treatment Satisfaction Questionnaire scores).22
Sample Calculation
Based on prior research findings, the control group was expected to have a compliance rate of 40.00%, while the test group was expected to achieve a compliance rate of 65.00%, considering that their HbA1c levels were below 7.00% and there was no hypoglycemia or weight gain. To be able to detect a significant difference between the treatments in the test group and the control group with 80.00% power (β = 0.20) and an α level of 0.05, 60 subjects were required in each group. A 20% shedding rate was predicted, so at least 150 patients were proposed for inclusion.
Statistical Analysis
The FAS population included subjects who met the eligibility criteria, were randomized, and received at least one intervention dose. The safety population was defined as subjects who received at least one intervention dose. Missing data were treated as nonresponsive. Continuous variables following a Gaussian distribution are presented as means (95% confidence interval [CI]) and analyzed with independent sample t-tests. Non-normally distributed continuous variables are represented as medians (interquartile range) and compared using the Mann–Whitney U-test. Categorical variables are expressed as numbers (percentages). Pearson’s χ²-test was applied for comparisons with expected cell frequencies ≥5; otherwise, Fisher’s exact test was used. The primary endpoint comparison between the groups was performed using Pearson’s χ²-test. Post hoc analyses based on BMI and weight loss were conducted when the primary endpoint was not statistically significant. Statistical analysis was conducted using SAS 9.4 software. All statistical tests used in the study were two-sided, and a P value of < 0.05 was considered statistically significant.
Results
Baseline Characteristics
The average patient ages were 54.20 ± 11.32 years in the control group and 54.35 ± 11.24 years in the test group. Most of the baseline characteristics, including BMI and HbA1c, were comparable between the two groups, except for body weight (P = 0.045), heartbeats per minute (P = 0.031), and tobacco and alcohol use (P = 0.031 and 0.033, respectively), which were all higher in the control group. Although the baseline data for smoking and alcohol consumption were imbalanced, no differences were observed in the baseline values of the associated indicators, such as AST, ALT, and IL-6 (Table 1).
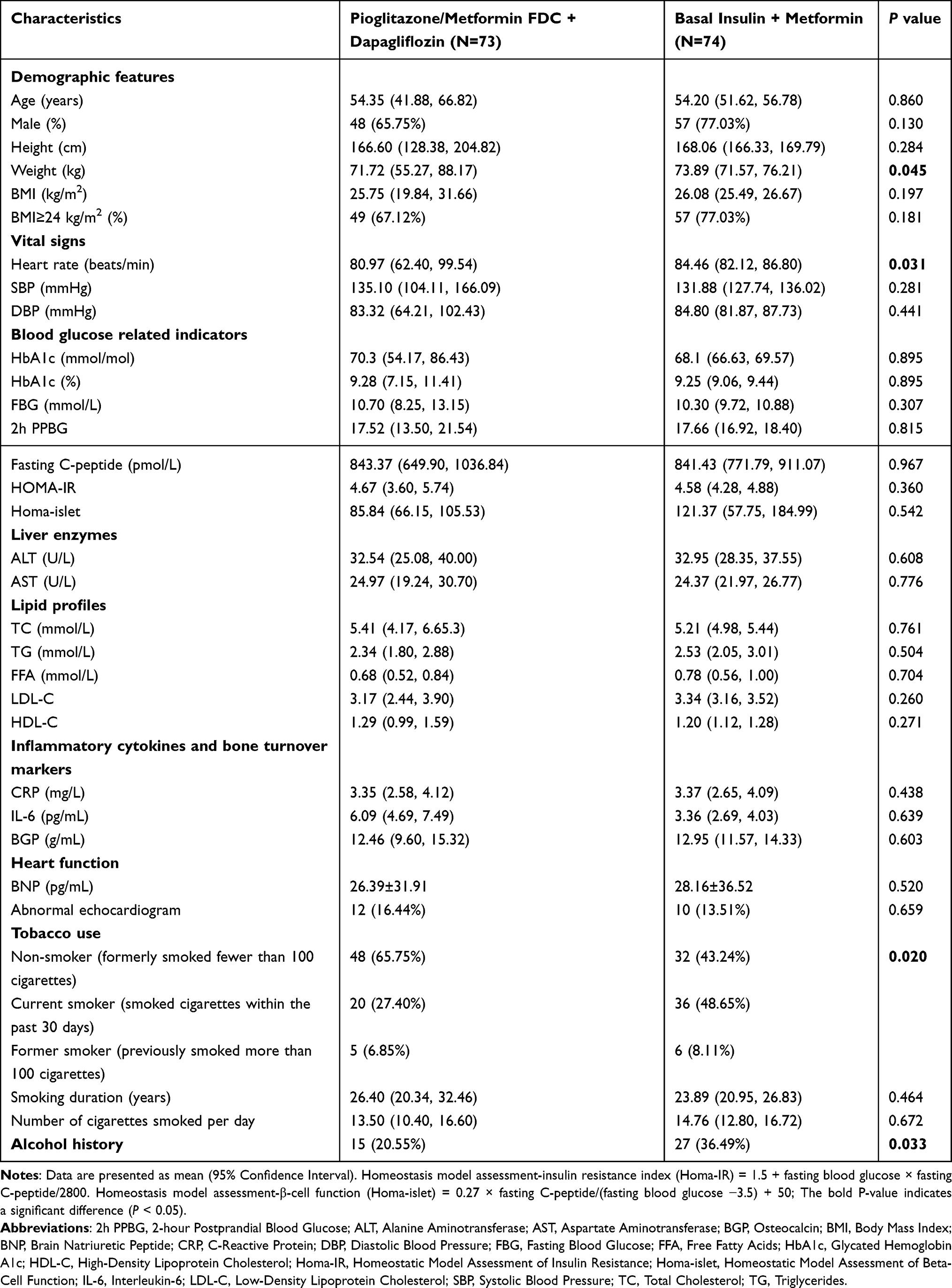 |
Table 1 Patient Demographics and Disease Characteristics at Baseline |
Efficacy
Primary Endpoints
As shown in Table 2, at week 16, there was no significant difference in the proportion of patients who achieved the primary endpoint between the test (43.84%) and control groups (37.84%). We then conducted post hoc analyses based on BMI and weight reduction. The percentage of patients in the test group (31.51%) who reached the target HbA1c level without developing hypoglycemia and experienced a weight loss of ≥ 3.00% was significantly higher than that in the control group (13.51%; P = 0.009). In the population with BMIs ≥ 24.00 kg/m², the proportion of subjects in the test group (36.73%) who achieved the target HbA1c level without developing hypoglycemia and experienced a weight loss of ≥ 3.00% was significantly higher than that in the control group (15.79%; P = 0.014; Figure 2).
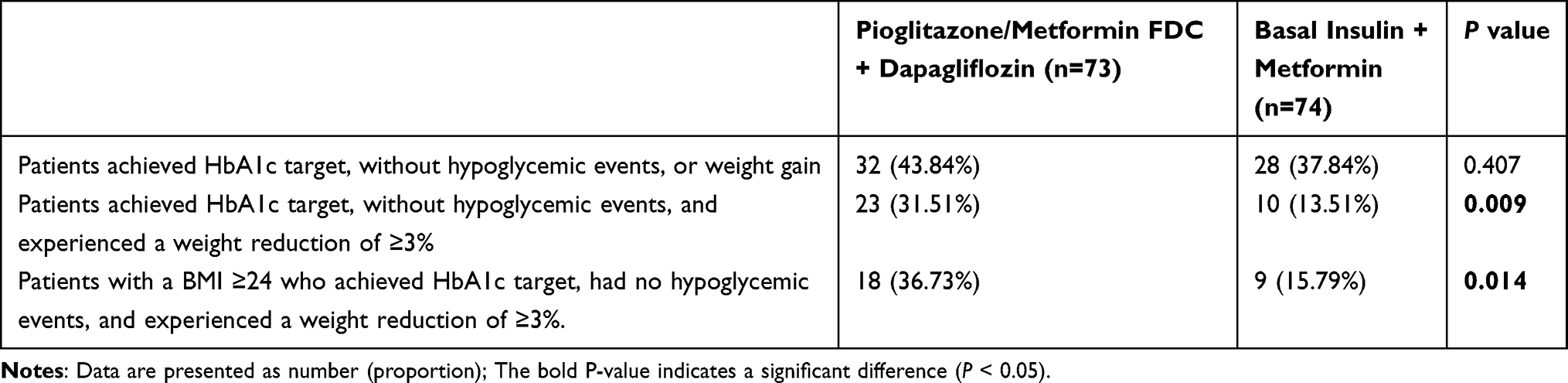 |
Table 2 Proportions of Patients Meeting the Composite Endpoints |
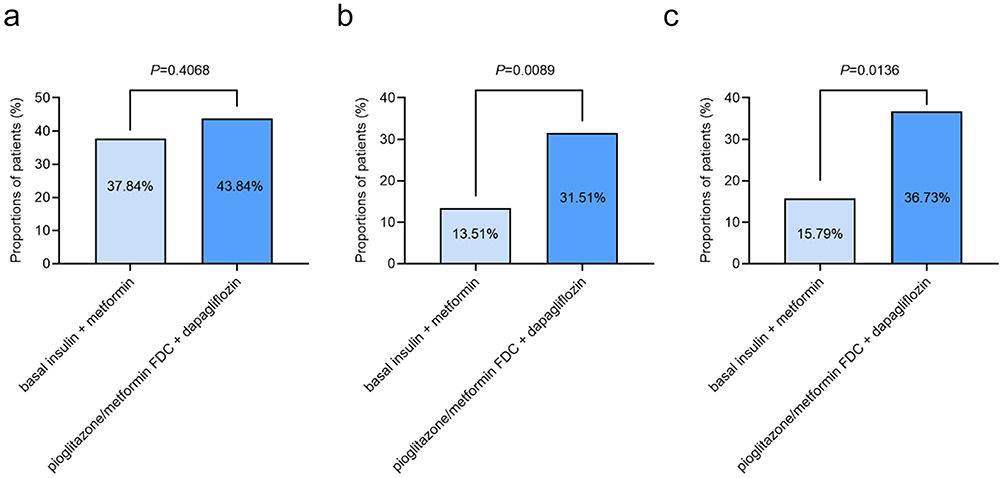 |
Figure 2 Primary endpoints. Results for the primary endpoints. (a) Patients who achieved the HbA1c target without hypoglycemic events or weight gain. (b) Patients who achieved the HbA1c target without hypoglycemic events and experienced a weight reduction of ≥ 3%. (c) Patients with BMIs ≥ 24 kg/m² who achieved the HbA1c target, had no hypoglycemic events, and experienced a weight reduction of ≥ 3%. |
Secondary Endpoints
At week 16, the metabolic, inflammatory, cardiovascular, and other effects of the pioglitazone/metformin FDC combined with dapagliflozin were evaluated against those of basal insulin combined with metformin. Relative to the baseline data, glucose metabolism, BGP, and cardiac function data were comparable in the two groups (Table 3). In the test group, a greater reduction from the baseline in SBP was found (P < 0.05). Although TG and FFA differed insignificantly between the two groups, the improvement in HDL-C relative to the baseline value (P < 0.001) was notable Patients administered FDC with dapagliflozin achieved a considerable body weight loss and BMI improvement (both P < 0.01). The reduction in IL-6 was appreciable in the test group (P = 0.035). The level of ALT was greatly reduced from the baseline value in the test group (P = 0.028). According to the satisfaction survey, overall satisfaction and responses to the question “Would you like to continue your current treatment?” scored higher in the test group than in the control group (P < 0.05, Supplementary Table 1), indicating that the patients were more accepting of the oral combination therapy than they were of the combination of injections with oral therapy.
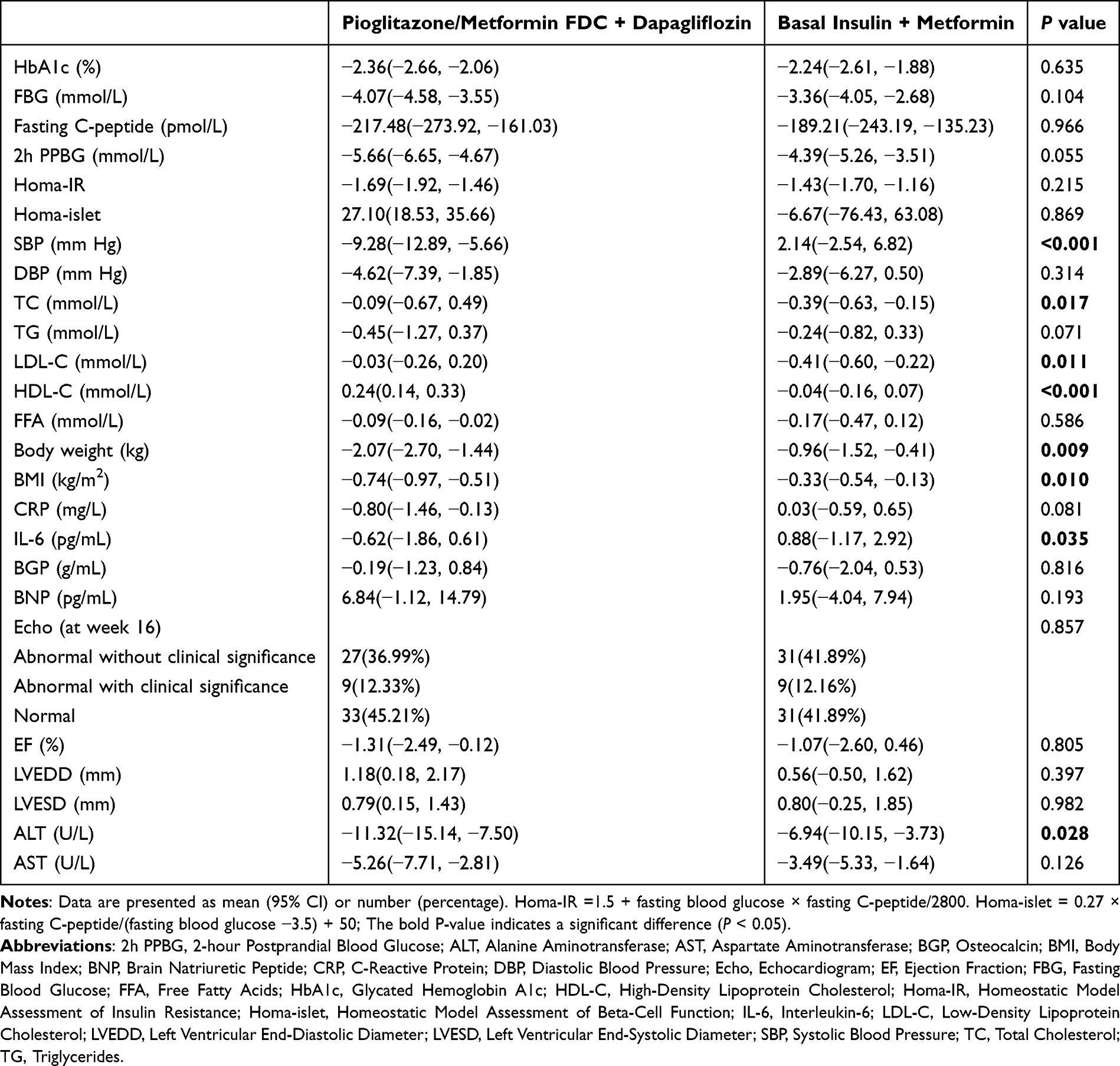 |
Table 3 Changes From Baseline in Blood Glucose Levels, Blood Pressure, Lipid Profile, Inflammatory Cytokines and Bone Turnover Markers, Cardiac Function, and Liver Enzymes at week 16 |
Adverse Events
Overall, 29 AEs were reported by 21 patients in the control group, and 26 were reported by 17 patients in the test group (P > 0.05). AEs occurred in similar proportions in the two groups. Notably, the rate of hypoglycemia was lower in the test group (2 patients, 2.74%) than in the control group (10, 13.51%), as shown in Table 4.
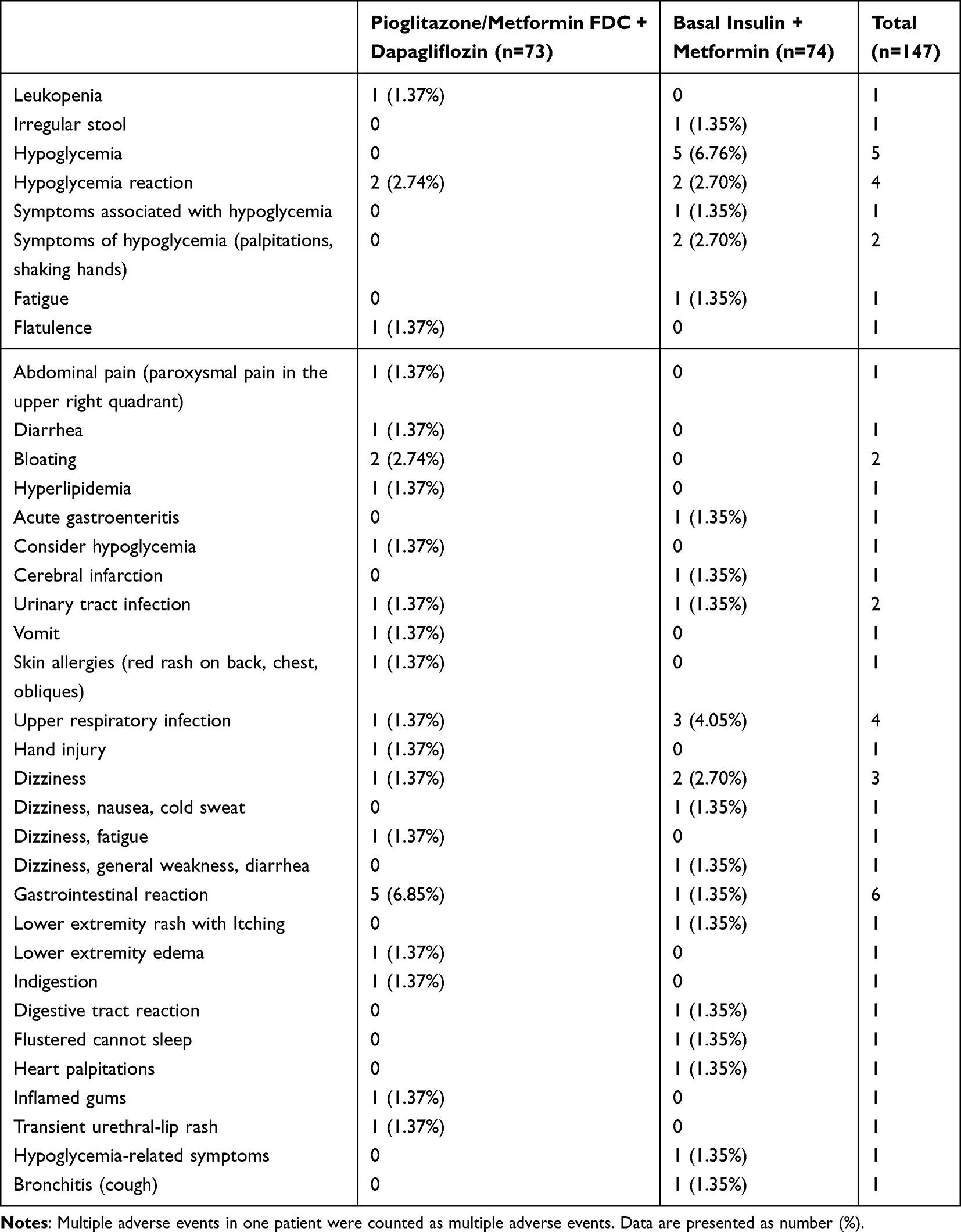 |
Table 4 Summary of Adverse Events |
Discussion
The study results indicated no significant difference between the test and control groups in the overall proportion of patients achieving HbA1c levels <7.00% without hypoglycemia or weight gain. However, a notably higher proportion of patients in the test group attained the target HbA1c without hypoglycemia and achieved a body weight reduction of ≥3.00% compared to the control group, particularly among individuals with BMIs ≥24.00 kg/m². Furthermore, the test group demonstrated meaningful improvements in SBP, lipid profiles, body weight, BMI, inflammatory markers, and liver function, along with clinically symptomatic benefits. Additionally, the incidence of hypoglycemia was substantially lower in the test group.
Patients with T2DM are often comorbid with one or more components of metabolic syndrome, such as hypertension, dyslipidemia, or obesity, which significantly increase the risk, progression rate, and harm of T2DM complications.23 Therefore, the management of T2DM should be comprehensive, including the control of blood glucose, blood pressure, blood lipids, and body weight, while avoiding the occurrence of safety events, such as hypoglycemia.24 Although some previous studies have used similar endpoints, the number is relatively limited.25 Single-drug administration often fails to simultaneously achieve all these goals, and it is usually necessary to add other drugs to compensate for their shortcomings. Many studies have shown that, compared to monotherapy with pioglitazone or metformin, the change in HbA1c from the baseline in patients treated with the FDC of pioglitazone and metformin consistently demonstrates a superior treatment effect. The pioglitazone/metformin FDC is well tolerated, with a lower or similar incidence of AEs compared to each monotherapy, but as some studies have pointed out, pioglitazone may cause weight gain.26,27 In this study, we chose to combine dapagliflozin with the pioglitazone/metformin FDC based on its known mechanism of inhibiting renal glucose reabsorption and increasing glucose excretion, thereby inducing a negative energy balance within the body and facilitating fat utilization.28–30 Metformin, on the other hand, accelerates the body’s utilization of glucose, reducing the energy supply to the body.
To meet its own energy needs, the body directly consumes adipose tissue, thereby reducing its fat content.31 The combination of insulin and metformin, a powerful hypoglycemic therapy, has been recommended by many guidelines for a long time.32 However, hypoglycemia and weight gain are common adverse effects associated with insulin treatment.33 The results of the composite endpoints in this study suggest that the combination of the pioglitazone/metformin FDC and dapagliflozin has certain advantages over insulin combined with metformin in the comprehensive management of T2DM. Furthermore, while not statistically significant, the observed changes in HbA1c, fasting venous blood glucose, fasting C-peptide, 2-hour postprandial venous blood glucose, Homa-IR, and Homa-islet still suggested improvements in glucose metabolism and cellular function from pioglitazone/metformin FDC combined with dapagliflozin.
In the Chinese population, a BMI between 24.00 and 27.90 kg/m² is generally categorized as overweight, while a BMI of 28.00 kg/m² or above is considered obese.34 The pathogenesis of T2DM mainly involves defects in insulin secretion, namely absolute deficiency, insulin resistance, or utilization disorders. The key factor in its development is insulin resistance caused by overweight and obesity. Thus, obesity is an indispensable factor to consider in studying the occurrence and development of T2DM.35 In China, the proportion of patients with abdominal obesity among diabetics is close to 50%. Some studies have demonstrated that losing approximately 10 kg of weight can reduce the mortality rate of diabetic patients by about 25%.36 Over the past 30 years, the average BMI of adults in China has increased by approximately 1.8 kg/m2, the prevalence of obesity has increased by 8 times, and the prevalence of diabetes has increased by 14 times. Diabetic patients with overweight or obesity have a higher visceral fat volume than those with overweight or obesity alone.37 Based on these studies, it can be concluded that there is a strong correlation between an increase in BMI and the risk of developing T2DM. However, the complex relationship between obesity and T2DM has not been fully elucidated, and the occurrence, development, and mutual promotion of the two conditions require further investigation.
SGLT2 primarily leads to weight loss through caloric loss and osmotic diuresis. Multiple meta-analyses have shown that SGLT2 inhibitors significantly reduce body weight in elderly patients compared with placebos, with a combined weight loss effect of 1.72 kg. In elderly patients with T2DM aged 55 to 80 years, 100 or 300 mg of canagliflozin per day for 104 weeks can result in an average weight loss of 2.7 or 3.5 kg, respectively. In this study, the proportion of subjects with BMIs ≥ 24.00 kg/m2 in the test group who achieved the target HbA1c level did not experience hypoglycemia, and they lost ≥ 3.00% of their body weight when treated with the pioglitazone/metformin FDC combined with dapagliflozin, which was a significantly higher rate than that in the control group. This indicates that dapagliflozin can improve blood glucose levels while also managing body weight. In this study, we observed better glycemic control in individuals who lost more than 3% of their body weight after 16 weeks of follow-up, indicating that our approach has advantages in terms of weight management and blood glucose control.
Inflammation and liver disease are common complications associated with T2DM. Chronic inflammation is a hallmark feature of T2DM and plays a critical role in the pathogenesis and progression of the disease. This inflammatory state is associated with elevated levels of proinflammatory cytokines, such as IL-6 and CRP, which contribute to insulin resistance and impaired glucose metabolism.38 Additionally, patients with T2DM have a greater risk of developing liver diseases, including nonalcoholic fatty liver disease and nonalcoholic steatohepatitis.39 These conditions are characterized by the accumulation of fat in the liver, which can lead to inflammation, fibrosis, and liver dysfunction. Potential mechanisms linking T2DM with liver disease include insulin resistance, dyslipidemia, oxidative stress, and adipose tissue inflammation.40–42
In this study, the therapeutic combination of pioglitazone/metformin FDC with dapagliflozin had beneficial effects on inflammatory cytokines and liver enzymes. Previous studies that compared low-dose pioglitazone treatment with metformin treatment in Japanese patients with diabetes and metabolic syndrome found that the pioglitazone group exhibited significant reductions in HbA1c and HOMA-IR, as well as significant decreases in TG, AST, ALT, and hs-CRP. The metformin group showed significant decreases in HbA1c, HOMA-IR, BMI, and waist circumference.43 If we combine previous clinical research evidence with the results of this study, it suggests that the combination of pioglitazone/metformin FDC with dapagliflozin may have the potential to reduce inflammation and alleviate liver disease in patients with T2DM. This favorable outcome effectively strengthens the advantage of the combination of the pioglitazone/metformin FDC with dapagliflozin in terms of comprehensively improving the overall health status of diabetic patients.
BGP, commonly known as osteocalcin, serves as a biomarker of bone formation and is occasionally associated with bone metabolism.44 T2DM is associated with an increased risk of bone-related complications, such as osteoporosis and fractures.45 A cross-sectional study that included 250 patients with T2DM found an independent negative correlation between glycemic excursions and bone turnover markers (type 1 collagen N-terminal propeptide and a C-terminal telopeptide fragment of type I collagen).46 However, the relationship between T2DM and bone health is complex, multifaceted, and influenced by numerous factors, including age, obesity, insulin resistance, and medications used to control diabetes, which may all affect bone metabolism in patients with T2DM.47 Some studies have also suggested a potential association between TZDs and osteoporosis.48,49 This study found that there were no significant changes in BGP levels within each group or between groups after 16 weeks of treatment. This may be due to the specific population studied, the treatment regimens administered, and the duration of observation. Additionally, bone metabolism is influenced by various factors, such as age, gender, diet, and physical activity, which need to be considered comprehensively. Further research is crucial to validate these findings and clarify the long-term effects and safety of the pioglitazone and metformin FDC combined with dapagliflozin on bone health.
The main limitation of the study is its relatively small sample, which may not be fully representative of the broader population of patients with T2DM. Second, the study did not strictly monitor the calorie intake and exercise of the enrolled patients, which may have had some impact on the results. Additionally, the proportion of female patients is higher in the test group, which, although not statistically significant, may impact the overall weight loss results due to the difference in fat mass between genders. Therefore, the more significant weight loss observed in the test group should be interpreted with caution, which may be more valuable for female patients with higher BMI. Further research is needed to confirm the findings, and we will perform a more appropriate group matching or controlling for these factors.
Conclusions
The combination of pioglitazone/metformin FDC with dapagliflozin therapy could be an effective means of managing T2DM in patients with poor glycemic control and a favorable alternative to basal insulin supplemented with metformin therapy in the absence of contraindications. However, additional research is needed to further elucidate the mechanisms and long-term effects of this treatment combination, particularly regarding weight loss parameters.
Abbreviations
T2DM, type 2 diabetes mellitus; FDC, fixed-dose combination; AEs, adverse events; CVD, cardiovascular disease; TZD, thiazolidinedione; PPARγ, peroxisome proliferator-activated receptor gamma; SGLT-2, sodium–glucose cotransporter 2; HbA1c, glycated hemoglobin; FAS, full analysis set; ECG, electrocardiogram results; 2h PPBG, 2-hour postprandial blood glucose; BNP, brain natriuretic peptide; BGP, bone Gla-protein; Homa-IR, homeostatic model assessment of insulin resistance; Homa-islet, homeostatic model assessment of beta-cell function; DBP, diastolic blood pressure; SBP, systolic blood pressure; TG, triglycerides; TC, total cholesterol; FFA, free fatty acids; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; CRP, C-reactive protein; IL-, interleukin-6; BMI, body mass index; ALT, alanine aminotransferase; AST, aspartate aminotransferase; Echo, echocardiogram; CI, confidence interval.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Shanghai General Hospital (Approval Number: [2022]102) and by other medical centers. All study procedures were conducted in accordance with the Helsinki Declaration of 1964 (as revised in 2013). All subjects signed an informed consent form after being made fully aware of the research content and risks.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Yi Lin and Jianxia Shi are co-first authors for this study. The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. American Diabetes Association. 8. pharmacologic approaches to glycemic treatment: standards of medical care in diabetes-2018. Diabetes Care. 2018;41(Suppl 1):S73–s85. doi:10.2337/dc18-S008
2. Weng J, Ji L, Jia W, et al. Standards of care for type 2 diabetes in China. Diab Metab Res Rev. 2016;32(5):442–458. doi:10.1002/dmrr.2827
3. Beysel S, Unsal IO, Kizilgul M, Caliskan M, Ucan B, Cakal E. The effects of metformin in type 1 diabetes mellitus. BMC Endocr Disord. 2018;18(1):1. doi:10.1186/s12902-017-0228-9.
4. Flory J, Lipska K. Metformin in 2019. JAMA. 2019;321(19):1926–1927. doi:10.1001/jama.2019.3805
5. American Diabetes Association. 9. pharmacologic approaches to glycemic treatment: standards of care in diabetes-2025. Diabetes Care. 2025;48(Supplement_1):S181–s206. doi:10.2337/dc25-S009
6. Zhang P, Chen M, Zhang H, et al. Effectiveness and safety of basal insulin therapy in type 2 diabetes mellitus patients with or without metformin observed in a national cohort in China. BMC Endocr Disord. 2022;22(1):26. doi:10.1186/s12902-021-00892-6
7. Dagogo-Jack S, Frederich R, Liu J, et al. Ertugliflozin delays insulin initiation and reduces insulin dose requirements in patients with type 2 diabetes: analyses from VERTIS CV. J Clin Endocrinol Metab. 2023;108(8):2042–2051. doi:10.1210/clinem/dgac764
8. Böhm AK, Schneider U, Aberle J, Stargardt T. Regimen simplification and medication adherence: fixed-dose versus loose-dose combination therapy for type 2 diabetes. PLoS One. 2021;16(5):e0250993. doi:10.1371/journal.pone.0250993
9. Li J, Lian H. Recent development of single preparations and fixed-dose combination tablets for the treatment of non-insulin-dependent diabetes mellitus: a comprehensive summary for antidiabetic drugs. Arch Pharmacal Res. 2016;39:731–746. doi:10.1007/s12272-016-0762-4
10. Alnuaimi S, Reljic T, Abdulla FS, et al. PPAR agonists as add-on treatment with metformin in management of type 2 diabetes: a systematic review and meta-analysis. Sci Rep. 2024;14(1):8809. doi:10.1038/s41598-024-59390-z
11. Guo LX, Wang LW, Tian DZ, et al. Efficacy and safety of pioglitazone/metformin fixed-dose combination versus uptitrated metformin in patients with type 2 diabetes without adequate glycemic control: a randomized clinical trial. Diabetes Ther. 2024;15(11):2351–2366. doi:10.1007/s13300-024-01638-y
12. Perez A, Jacks R, Arora V, Spanheimer R. Effects of pioglitazone and metformin fixed-dose combination therapy on cardiovascular risk markers of inflammation and lipid profile compared with pioglitazone and metformin monotherapy in patients with type 2 diabetes. J Clin Hypertens. 2010;12(12):973–982. doi:10.1111/j.1751-7176.2010.00389.x
13. Zhao H, Zhang J, Cheng X, Nie X, He B. Insulin resistance in polycystic ovary syndrome across various tissues: an updated review of pathogenesis, evaluation, and treatment. J Ovarian Res. 2023;16(1):9. doi:10.1186/s13048-022-01091-0
14. Nesti L, Tricò D, Mengozzi A, Natali A. Rethinking pioglitazone as a cardioprotective agent: a new perspective on an overlooked drug. Cardiovasc Diabetol. 2021;20(1):109. doi:10.1186/s12933-021-01294-7
15. Giglio RV, Papanas N, Rizvi AA, et al. An update on the current and emerging use of thiazolidinediones for type 2 diabetes. Medicina. 2022;58(10):1475. doi:10.3390/medicina58101475
16. van Baak MA, Mariman ECM. Mechanisms of weight regain after weight loss — the role of adipose tissue. Nat Rev Endocrinol. 2019;15(5):274–287. doi:10.1038/s41574-018-0148-4
17. Ko KD, Kim KK, Lee KR. Does weight gain associated with thiazolidinedione use negatively affect cardiometabolic health? J Obes Metab Syndr. 2017;26(2):102–106. doi:10.7570/jomes.2017.26.2.102
18. Bolinder J, Ljunggren Ö, Johansson L, et al. Dapagliflozin maintains glycaemic control while reducing weight and body fat mass over 2 years in patients with type 2 diabetes mellitus inadequately controlled on metformin. Diabetes Obesity Metab. 2014;16(2):159–169. doi:10.1111/dom.12189
19. Peikert A, Martinez FA, Vaduganathan M, et al. Efficacy and safety of dapagliflozin in heart failure with mildly reduced or preserved ejection fraction according to age: the DELIVER trial. Circulation. 2022;15(10):e010080. doi:10.1161/CIRCHEARTFAILURE.122.010080
20. McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. New Engl J Med. 2019;381(21):1995–2008. doi:10.1056/NEJMoa1911303
21. Lim S, Lee SH, Min KW, et al. A multicentre, double-blind, placebo-controlled, randomized, parallel comparison, Phase 3 trial to evaluate the efficacy and safety of pioglitazone add-on therapy in type 2 diabetic patients treated with metformin and dapagliflozin. Diabetes Obesity Metab. 2024;26(6):2188–2198. doi:10.1111/dom.15526
22. Baccaro F, Novelli Poisson P, Arduin J, Hilliar V. Diabetes treatment satisfaction questionnaire (DTSQ) of in non-ambulatory type 2 diabetic patients. Boletin de la Asociacion Medica de Puerto Rico. 2016;108(1):57–62.
23. Ribeiro ESR, de Miranda Gauza M, Guisso MES, da Silva JON, Kohara SK. Once-weekly insulin icodec vs. once-daily insulin Glargine U100 for type 2 diabetes: a systematic review and meta-analysis of Phase 2 randomized controlled trials. Arch Endocrinol Metab. 2023;67(5):e000614. doi:10.20945/2359-3997000000614
24. Rosenstock J, Frías JP, Rodbard HW, et al. Tirzepatide vs insulin lispro added to basal insulin in type 2 diabetes: the SURPASS-6 randomized clinical trial. JAMA. 2023;330(17):1631–1640. doi:10.1001/jama.2023.20294
25. Gu T, Ma J, Zhang Q, et al. Comparative effect of saxagliptin and glimepiride with a composite endpoint of adequate glycaemic control without hypoglycaemia and without weight gain in patients uncontrolled with metformin therapy: results from the SPECIFY study, a 48-week, multi-centre, randomized, controlled trial. Diabetes Obesity Metab. 2019;21(4):939–948.
26. Singh AK, Singh R, Chakraborty PP. Diabetes monotherapies versus metformin-based combination therapy for the treatment of type 2 diabetes. Int J Gene Med. 2021;14:3833–3848. doi:10.2147/IJGM.S295459
27. Wise J. Pioglitazone seems safe and effective for patients with fatty liver disease and diabetes. BMJ. 2016;353:i3435. doi:10.1136/bmj.i3435
28. Oyama K, Raz I, Cahn A, et al. Obesity and effects of dapagliflozin on cardiovascular and renal outcomes in patients with type 2 diabetes mellitus in the DECLARE-TIMI 58 trial. Eur Heart J. 2022;43(31):2958–2967. doi:10.1093/eurheartj/ehab530
29. Sugiyama S, Jinnouchi H, Kurinami N, et al. Dapagliflozin reduces fat mass without affecting muscle mass in type 2 diabetes. J Atheroscler Thromb. 2018;25(6):467–476. doi:10.5551/jat.40873
30. Vivian EM. Dapagliflozin: a new sodium-glucose cotransporter 2 inhibitor for treatment of type 2 diabetes. Am J Health Syst Pharm. 2015;72(5):361–372. doi:10.2146/ajhp140168
31. Hayashizaki-Someya Y, Kurosaki E, Takasu T, et al. Ipragliflozin, an SGLT2 inhibitor, exhibits a prophylactic effect on hepatic steatosis and fibrosis induced by choline-deficient l-amino acid-defined diet in rats. Eur J Pharmacol. 2015;754:19–24. doi:10.1016/j.ejphar.2015.02.009
32. Elkind-Hirsch KE, Seidemann E, Harris R. A randomized trial of dapagliflozin and metformin, alone and combined, in overweight women after gestational diabetes mellitus. Ame j Obstetrics Gynecol MFM. 2020;2(3):100139. doi:10.1016/j.ajogmf.2020.100139
33. Alidrisi HA, Bohan A, Mansour AA. Barriers of doctors and patients in starting insulin for type 2 diabetes mellitus. Cureus. 2021;13(9):e18263. doi:10.7759/cureus.18263
34. Pan XF, Wang L, Pan A. Epidemiology and determinants of obesity in China. Lancet Diab Endocrinol. 2021;9(6):373–392. doi:10.1016/S2213-8587(21)00045-0
35. Jourdan T, Godlewski G, Kunos G. Endocannabinoid regulation of β-cell functions: implications for glycaemic control and diabetes. Diab Obes Metab. 2016;18(6):549–557. doi:10.1111/dom.12646
36. Amiel SA. The consequences of hypoglycaemia. Diabetologia. 2021;64(5):963–970. doi:10.1007/s00125-020-05366-3
37. Wang Y, Bolge SC, Lopez JM, Zhu VJ, Stang PE. Changes in body weight among people with type 2 diabetes mellitus in the United States, NHANES 2005-2012. Diab Educator. 2016;42(3):336–345. doi:10.1177/0145721716640096
38. Hariharan R, Odjidja EN, Scott D, et al. The dietary inflammatory index, obesity, type 2 diabetes, and cardiovascular risk factors and diseases. Obes Rev. 2022;23(1):e13349. doi:10.1111/obr.13349
39. Stanimirovic J, Radovanovic J, Banjac K, et al. Role of C-reactive protein in diabetic inflammation. Mediators Inflammation. 2022;2022:3706508. doi:10.1155/2022/3706508
40. Mettananda C, Egodage T, Dantanarayana C, et al. Identification of patients with type 2 diabetes with non-alcoholic fatty liver disease who are at increased risk of progressing to advanced fibrosis: a cross-sectional study. BMJ Open. 2023;13(1):e063959. doi:10.1136/bmjopen-2022-063959
41. Yilmaz Y, Zeybel M, Adali G, et al. TASL practice guidance on the clinical assessment and management of patients with nonalcoholic fatty liver disease. Hepatol Forum. 2023;4(Suppl 1):1–32. doi:10.14744/hf.2023.2023.0011
42. Tauil RB, Golono PT, de Lima EP, et al. Metabolic-associated fatty liver disease: the influence of oxidative stress, inflammation, mitochondrial dysfunctions, and the role of polyphenols. Pharmaceuticals. 2024;17(10):1354.
43. Kothari S, Dhami-Shah H, Shah SR. Antidiabetic drugs and statins in nonalcoholic fatty liver disease. J Clin Exp Hepatol. 2019;9(6):723–730. doi:10.1016/j.jceh.2019.06.003
44. Sanches CP, Vianna AGD, Barreto FC. The impact of type 2 diabetes on bone metabolism. Diabetol Metab Syndr. 2017;9:85. doi:10.1186/s13098-017-0278-1
45. Cipriani C, Colangelo L, Santori R, et al. The interplay between bone and glucose metabolism. Front Endocrinol. 2020;11:122. doi:10.3389/fendo.2020.00122
46. Yang J, Zheng C, Wang Y, Yang L, Liu L. Correlation between mean amplitude of glycemic excursion and bone turnover markers in patients with type 2 diabetes: a cross-sectional study. Diab Metab Syndrome Obes. 2023;16:397–407. doi:10.2147/DMSO.S388919
47. Zhou R, Guo Q, Xiao Y, et al. Endocrine role of bone in the regulation of energy metabolism. Bone Res. 2021;9(1):25. doi:10.1038/s41413-021-00142-4
48. Lim S, Kim KM, Kim SG, et al. Effects of lobeglitazone, a novel thiazolidinedione, on bone mineral density in patients with type 2 diabetes mellitus over 52 weeks. Diabetes Metab J. 2017;41(5):377–385. doi:10.4093/dmj.2017.41.5.377
49. Yang BR, Cha SH, Lee KE, Kim JW, Lee J, Shin KH. Effect of dipeptidyl peptidase IV inhibitors, thiazolidinedione, and sulfonylurea on osteoporosis in patients with type 2 diabetes: population-based cohort study. Osteoporos Int. 2021;32(9):1705–1712. doi:10.1007/s00198-020-05801-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Dapagliflozin in Southern Europe Across the Spectrum of Characteristics of Type 2 Diabetes: An International Real-World Analysis
Fadini GP, Morales C, Caballero I, González B, Tentolouris N, Consoli A
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3533-3541
Published Date: 15 November 2022
Are There Differences in Gut Microbiome in Patients with Type 2 Diabetes Treated by Metformin or Metformin and Insulin?
Dzięgielewska-Gęsiak S, Fatyga E, Piłot M, Wierzgoń A, Muc-Wierzgoń M
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3589-3599
Published Date: 18 November 2022
Ethnic Variability in Glucose and Insulin Response to Rice Among Healthy Overweight Adults: A Randomized Cross-Over Study
Sadiya A, Jakapure V, Kumar V
Diabetes, Metabolic Syndrome and Obesity 2023, 16:993-1002
Published Date: 9 April 2023
Impact of Fixed Combination of Metformin and Pioglitazone on Insulin Resistance of Patients with Type 2 Diabetes: Results of a Randomized Open-Label Study
Sun R, Yuan L, Shen Y, Shen Z, Ding B, Ma J
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2911-2919
Published Date: 20 September 2023
The Regulation of Metabolic Homeostasis by Incretins and the Metabolic Hormones Produced by Pancreatic Islets
Reed J, Bain SC, Kanamarlapudi V
Diabetes, Metabolic Syndrome and Obesity 2024, 17:2419-2456
Published Date: 13 June 2024