Back to Journals » Psychology Research and Behavior Management » Volume 16
Enacted Stigma Influences Bereavement Coping Among Children Orphaned by Parental AIDS: A Longitudinal Study with Network Analysis
Authors Chen C ![]() , Wu Q, Zhao J, Zhao G, Li X, Du H, Chi P
, Wu Q, Zhao J, Zhao G, Li X, Du H, Chi P ![]()
Received 21 June 2023
Accepted for publication 27 October 2023
Published 7 December 2023 Volume 2023:16 Pages 4949—4958
DOI https://doi.org/10.2147/PRBM.S423707
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Chuqian Chen,1,* Qinglu Wu,2,* Junfeng Zhao,3 Guoxiang Zhao,4 Xiaoming Li,5 Hongfei Du,2 Peilian Chi6,7
1Department of Medical Humanities, Southeast University, Nanjing, Jiangsu, People’s Republic of China; 2Institute of Advanced Studies in Humanities and Social Sciences, Beijing Normal University, Zhuhai, Guangdong, People’s Republic of China; 3Institute of Psychology and Behavior, Henan University, Kaifeng, Henan, People’s Republic of China; 4Department of Psychology, Henan Normal University, Xinxiang, Henan, People’s Republic of China; 5Department of Health Promotion, Education, and Behavior, University of South Carolina, Columbia, SC, USA; 6Department of Psychology, Faculty of Social Sciences, University of Macau, Macau, People’s Republic of China; 7Centre for Cognitive and Brain Sciences, University of Macau, Macau, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peilian Chi, Department of Psychology, Faculty of Social Sciences, University of Macau, Mailing: E21-3049, Macau, 999078, People’s Republic of China, Tel +853 8822-4025, Email [email protected]
Purpose: The study aims to understand how enacted stigma influences bereavement coping at the style (scale) level and the specific pathways at the strategy (item) level.
Methods: The longitudinal data of 755 children orphaned by parental Acquired Immune Deficiency Syndrome (AIDS) in rural China were used. Grief processing and deliberate grief avoidance were measured at wave 1 (baseline) and wave 2 (one-year follow-up) to reflect bereavement coping in the contexts of being with family members, being with friends, being with community members, and being alone. Enacted stigma that measured at wave 1 was used to assess the experienced stigma of these AIDS-orphaned children. Network analyses were run following regressions.
Results: Controlling for demographics and baseline-level bereavement coping, multivariate regressions revealed that enacted stigma at wave 1 significantly predicted grief processing and deliberate grief avoidance at wave 2. Network analyses showed that, for grief processing, stigma increased searching for meaning alone and with friends and expressing feelings to community members, which then provoked the same strategy across contexts. Meanwhile, stigma triggered the deliberate grief avoidance network by initially suppressing the expression of feelings to community members.
Conclusion: Enacted stigma contributes to bereavement coping. Stigma stirs up complex feelings but forces AIDS-orphaned children to suppress expressions, and it increases needs to process grief through meaning making but cuts supporting forces by promoting avoidance. Interventions are imperative to reduce stigma, improve emotion regulation, and facilitate meaning making for people bereaved by stigmatized deaths.
Keywords: enacted stigma, bereavement coping, AIDS, orphans, network analysis, parental loss
Introduction
Stigma is the “co-occurrence of labelling, stereotyping, separation, status loss, and discrimination”.1 Stigma experienced by an individual could be categorized into enacted stigma (overt), perceived stigma (awareness of others’ attitudes), and internalized stigma (inner shame and self-discrimination).2,3 For people who lost loved ones to Acquired Immunodeficiency Syndrome (AIDS), all types of stigma are salient in their bereavement experiences.4–6 Such stigma is especially harmful for children due to their frailty.7 Children orphaned by parental AIDS (AIDS-orphaned children) are usually ignored, rejected, and referred to in derogatory manners8 as people fear about infection through contact with them and interpret their misbehaviors as being like their deceased parent.7 Responding to stigma with silence, secrecy, and withdrawal, AIDS-orphaned children’s perceived social support drops, psychological distress increases,9 and self-hatred10 grows. All these factors add an immense weight to the already overwhelming process of bereavement for children.11
Stigma links to a series of negative bereavement outcomes. Higher perceived stigma relates to more intense global psychological distress,12 depression,5 trauma, and problematic grief13 among people bereaved for stigmatized death. Among them, grief deserves greater attention because it is the most direct outcome of bereavement.14 For people whose loved ones died from AIDS, more intense grief was found to be cross-sectionally associated with perceived stigma in South Africa15 and internalized stigma in China.6 Despite their meaningful findings, previous studies have mainly focused on stigma’s impacts on bereavement outcomes (eg, grief intensity) rather than bereavement coping (eg, grief processing and deliberate grief avoidance). Moreover, little attention has been given to the influence of enacted stigma. Theoretically, enacted stigma was found, among people stigmatized by epilepsy,16 breast cancer,17 and same-sex sexual behavior,18 to be the source of the perceived stigma and internalized stigma that induced psychological distress and poor adjustment. Practically, as a subjective indicator that could be measured by specific behaviors and events, enacted stigma could be easily identified to inform in-time intervention. Under such circumstances, it would also be meaningful to investigate the role of enacted stigma in bereavement.
Bereavement Coping and Its Social Nature
Bereavement coping refers to “processes, strategies, or styles of managing the situation in which bereavement places the individual”.19 From the social constructionism perspective, bereavement coping processes involve both social and individual levels, and they manifest in a specific cultural and historical frame.20
Bereavement coping includes grief processing and deliberate grief avoidance.21 Grief processing means to accept the reality of loss, experience the pain, adjust to life without the deceased person, emotionally relocate the deceased person and move on, and deliberate grief avoidance is to avoid all reminders of the loss on purpose to prevent the sufferings of moving forward without the loved one.21 Both processing and avoidance styles shape bereavement outcomes.22 Grief processing correlated longitudinally with more severe distress and poorer perceived health among the bereaved,23 and deliberate grief avoidance was found to contribute to the persistence of complicated grief.24
Bereavement coping has an inherent social nature. People’s coping styles differ across social contexts. For instance, both Chinese and American bereaved individuals showed less grief processing with friends than with family or while alone.25 In addition, bereaved individuals adjust their styles according to perceived social acceptance of public mourning displays.26 People bereaved for stigmatized deaths are very cautious about disclosing to people around them,27 and some express grief to strangers in online forums instead.28
Although it has been developed in previous studies that both stigma and bereavement coping share significant links with bereavement outcomes,6,15,22 whether stigma influences bereavement coping has never been explored. Moreover, bereavement coping was viewed as a single construct and analyzed mainly at the style (eg, processing/avoidance) rather than the strategy level (eg, search for meaning to process grief/not talk about the deceased to avoid process grief), and its social nature is rarely considered. Given that the social context of bereavement coping is important and that stigma has the potential to influence bereavement coping at the strategy level, it is important to understand how specific coping strategies are linked with risk factors, such as stigma and how social contexts make a difference.
The Network Perspective
From a network perspective of psychopathology, mental disorders are not single latent constructs but networks of symptoms that mutually interact and are reciprocally reinforcing,29 and symptom construct rather than reflect disorders.30 In a network model, symptoms are represented by nodes, and between-symptom connections are shown as edges.30 Major life events could activate disorder networks through specific symptom nodes, and different events trigger the same disorder network through distinct pathways.31
In recent years, network analyses have been applied to see links between coping strategies and adaptation outcomes.32 Among bereaved earthquake survivors in China, maladaptive coping strategies such as self-blame linked positively with post-traumatic stress disorder symptoms, while adaptive coping strategies such as positive reframing linked closely with post-traumatic growth elements.33 Until now, links between risk factors, such as stigma and bereavement coping have never been studied with the network approach.
The Present Study
In previous studies,6,15 how stigma influences bereavement coping was underexplored, and the strategy-level mechanism from stigma, specifically enacted stigma, to bereavement coping remains unknown. Social contexts in which coping takes place have not received enough attention, longitudinal analyses are rare, and most explorations focused on adults. Addressing all these gaps, the present study intended to investigate the influence of enacted stigma on bereavement coping at both the style and strategy levels. A longitudinal design was adopted, and context-related bereavement coping was measured among AIDS-orphaned children.
Materials and Methods
Study Design and Participants
The present study was part of a larger research project on the psychological adjustment of children affected by parental human immunodeficiency virus (HIV)/AIDS.34 The current study included 755 AIDS-orphaned children aged between 6 and 18 years. Children’s understanding of the five elements of death, namely universality, irreversibility, causality, nonfunctionality, and noncorporeal continuation, gradually develops with age.35 From 6 years on, most children can understand the five subcomponents to varying degrees,36 and those who had bereaved for family members have a more mature understanding.37 In this case, it is assumed that children in the present study are capable of comprehending the death-related topic under discussion and answer reasonably regarding their bereavement coping. Detailed information on the sample and recruitment is reported elsewhere.34,38 Briefly, the children were recruited from community settings (orphanages and family or kinship care settings) in two rural counties in central China where a large number of residents were infected with HIV due to unhygienic blood collection.34 One child per family was randomly recruited. Baseline data were collected from 2006 to 2007 (wave 1), with follow-ups after 1 year (wave 2) and 2 years (wave 3). Interviewers read questions for children who were too young or had limited literacy and recorded their oral responses.
Regarding the sample size, at least 55 participants were needed for the multivariate analysis (G*Power:39 two tails, 8 predictors, effect size f2 = 0.15, α= 0.05, power = 0.80) and 500 for the 29-node network analysis.40 Therefore, at least 500 participants were needed for this study. Data from the first two waves were used in the analyzes, since bereavement coping (dependent variable) was not measured in wave 3. There were 755 orphans at wave 1, and 552 of them reported bereavement coping at wave 2. This manuscript followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for reporting observational studies.41
Variables and Measures
Enacted stigma was measured by the scale that Zhao et al34 developed specifically for children affected by HIV/AIDS. The 14-item scale in Chinese focuses on whether the children had experienced some stigmatization acts and prejudice from others and the consequences of such stigmatization and prejudice (eg, “physically abused by other people or other kids” and “I was hurt by how people looked at me or talked to me”) (1 = never, 5 = always). The Cronbach’s α for enacted stigma in wave 1 (ES1) was 0.869 in this study.
Bereavement coping was measured by the 18-item grief processing scale and the 10-item deliberate grief avoidance scale by Bonanno et al.23 The grief processing scale measures the frequencies of using five strategies, namely, thinking about the deceased, searching for meaning, having positive memories of the deceased, talking about the deceased, and expressing feelings about the deceased. The deliberate grief avoidance scale measures frequencies of three strategies, including avoiding thinking about the deceased, avoiding talking about the deceased, and avoiding expressing feelings. All eight strategies were phrased in the contexts of family members, friends, and community members. All strategies except talking about the deceased and expressing feelings about the deceased were measured in the context of being alone. The 28 bereavement coping (processing and avoidance) items were measured with a 5-point response option (from 1 = “almost never” to 5 = “almost constantly”). The Cronbach’s α for wave 1 grief processing (GP1), wave 1 deliberate grief avoidance (GA1), wave 2 grief processing (GP2), and wave 2 deliberate grief avoidance (GA2) were 0.920, 0.873, 0.928, and 0.895, respectively.
For demographics, age, sex, orphan type (single orphan or double orphan) and living condition (in an orphanage or with family) of the AIDS-orphaned children, as well as the education levels and occupations of both parents, were recorded. A family socioeconomic status (SES) score was calculated as the sum (ranging from 0 to 4) of the education score (1 = greater than elementary school, 0 = others) and occupation score (1 = engaged in a nonfarming occupation, 0 = others) of each parent.42
Statistical Analysis
First, descriptive analyses were run for all variables in SPSS. T-tests were run to detect differences between the retained participants and dropouts in age, family SES score, and ES1, GP1, and GA1 scores, and chi-square tests were used to test differences in sex, orphan type, and living condition. Correlational coefficients between ES1, GP1, GA1, GP2, and GA2 were calculated.
Second, two multivariate regressions were run in the R package mice with GP2 and GA2 as the dependent variables, ES1 as the independent variable, and age, sex, orphan type, living condition, family SES, GP1, and GA1 as control variables. Orphan type and living condition were transformed into dummy variables. Missing data were handled with multiple imputation.
Third, a network model was estimated using the R package bootnet. The model involved the ES1 node (total score) and the 28 GP2 and GA2 nodes (item score). The network analysis was run following the steps proposed by Epskamp, Borsboom and Fried.43 The relationship between two nodes was calculated after controlling for the influence of all other nodes. Sparse Gaussian graphical models with the graphical lasso were adopted,44 and the tuning parameters were chosen using the extended Bayesian information criterion (EBIC). Bootstrapping (nBoots = 1000) was used to test centrality stability and edge differences. Full Information Maximum Likelihood was applied to deal with missing data. Afterward, a 36-node model that contained an additional seven control variable nodes (age, sex, orphan type, living condition, family SES, GP1, and GA1) was run following the same steps of the 29-node model to explore whether the stigma-coping network structure changes profoundly after control variables are involved.
Results
Descriptive Analysis
The 755 AIDS-orphaned children (male: n = 403, 51.4%; female: n = 352, 46.6%) were 13.16 of age on average (n = 752, Range: 6–18, SD = 2.20) at wave 1, and 453 and 180 of them were single and double orphans, respectively. A total of 76.7% (n = 579) of them lived with family, while 23.3% (n = 176) lived in orphanages. The mean family SES score was 1.77 (n = 612, Range: 0–4, SD = 1.15).
No difference existed between the retained participants and dropouts in sex, ES1, GP1, or GA1 scores. However, the dropouts were older (t = 1.868, df = 750, p < 0.001) and had lower family SES scores (t = −0.293, df = 610, p = 0.005), and they were more likely to be single orphans (84.1% VS 76.4%, X2 = 4.276, df = 1, p = 0.046) and live with family (87.2% VS 72.8%, X2 = 17.134, df = 1, p  0.001). The outcomes of the descriptive analyses and correlational analyses are in Table 1. ES1 significantly correlated with GP2 and GA2.
0.001). The outcomes of the descriptive analyses and correlational analyses are in Table 1. ES1 significantly correlated with GP2 and GA2.
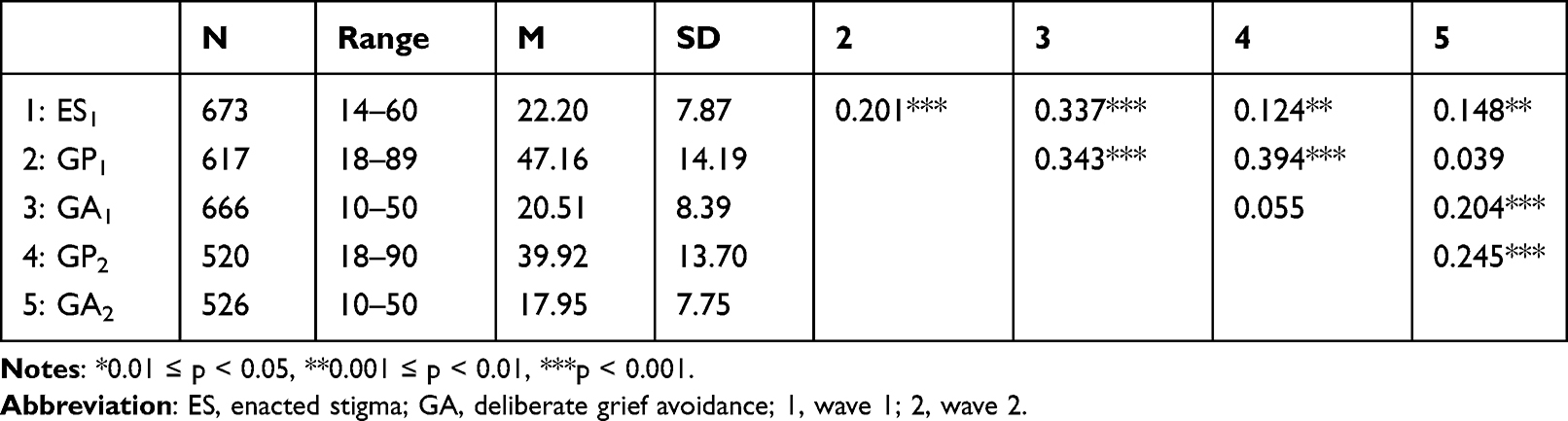 |
Table 1 Descriptive and Correlational Analyses (Total Score) |
Multivariate Regressions
The two regressions with GP2 and GA2 as the dependent variables generated similar findings (Table 2). After controlling for age, sex, orphan type, living condition, family SES, GP1, and GA1, higher ES1 significantly predicted higher GP2 (B = 0.222, p = 0.017, R2 = 0.210) and higher GA2 (B = 0.124, p = 0.023, R2 = 0.101).
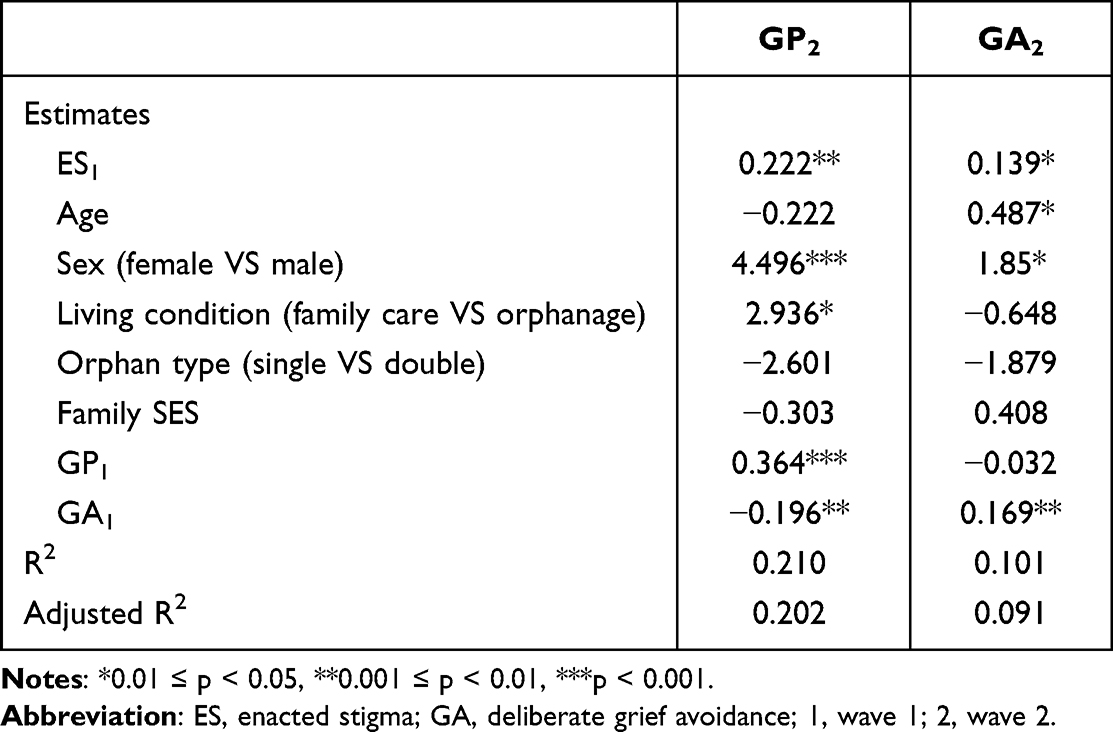 |
Table 2 Detailed Finding of Multivariate Regressions |
The Network Analysis
In the 29-node model, 133 out of the 406 edges were nonzero, and their mean weight was 0.032. The maximum drop proportions to retain a correlation of 0.7 in at least 95% of the sample were 0.75 and 0.75 for edge and strength, respectively. According to the criteria by Epskamp, Borsboom and Fried,43 the model was reliable. Figure 1 shows the distribution of strategies (blue edges have positive weights, and red edges have negative weights). Edge characters can be found in Figure S1 of the Supplementary Document.
 |
Figure 1 Symptom network of enacted stigma and bereavement coping. Notes: Blue edges have positive weights, and red edges have negative weights. Edge thickness is proportional to the edge weight. Processing: 1P: Think about your deceased parent; 2P: Search for some reason, meaning, or way to make sense of your loss; 3P: Have positive memories of your deceased parent; 5P: Talk about your deceased parent; 7P: Show your feelings about your deceased parent. Avoidance: 4A: Avoid thinking about your deceased parent; 6A: Avoid talking about your deceased parent; 8A: Avoid showing your feelings about your deceased parent. Contexts: H1: Family member; H2: Friends; H3: Community members; H4: Alone. Stigma: Enacted stigma. |
In Figure 1, grief processing items form separate strategy-based clusters. One strategy in a specific context was more likely to link to the same strategy across contexts rather than other strategies in the same context. However, deliberate grief avoidance items formed one general network, and they were linked across both strategies and contexts.
Four bereavement coping items shared nonzero edges with enacted stigma: H4.2P (Search for some reason, meaning, or way to make sense of the loss alone), H2.2P (Search for some reason, meaning, or way to make sense of the loss with friends), H3.7P (Show feelings about the deceased parent with community members), and H3.8A (Avoid showing feelings about the deceased parent with community members). Bootstrap analysis detected no significant differences among the four edge weights.
From the findings about the network distribution of grief processing items and deliberate grief avoidance items (how grief processing items link to each other) and these items’ links with the stigma node (how enacted stigma links to specific grief processing items), two stigma-processing pathways (stigma – searching for meaning alone/with friends – searching for meaning across contexts; stigma – feeling expressions with community – feeling expressions across contexts) and one stigma-avoidance pathway (stigma – avoidance of feeling expressions with community – all avoidance strategies across contexts) were identified.
Network analysis of the 36-node model generated similar findings in terms of node distribution, edge weight and node strength, and model reliability to the 29-node model. Detailed outcomes of the 36-node model are shown in the Supplementary Document and Figure S2 demonstrates its symptom distribution.
Discussion
Using large-sample (n = 755) longitudinal data from Chinese AIDS-orphaned children, this is the first study to reveal the influence of stigma on bereavement coping. Combining multivariate regressions with network analysis, explorations were conducted at two distinct levels, and attention was given to social contexts. At the style level, higher enacted stigma significantly predicted more grief processing and deliberate grief avoidance in the AIDS-orphaned children one year later. At the strategy level, stigma triggered two networks in specific pathways. Our findings contribute greatly to the theoretical understanding of the effect of stigmatized deaths on bereavement and support the use of network analysis in future studies in the field.
The Style Level
The style-level findings show that how orphans are treated in their social network influences how they deal with bereavement. The developmental challenges of incomplete individuation and dependency on caregivers45 and the lack of coping experiences46 make children especially susceptible to adverse environmental conditions.
In previous studies, both stigma12 and bereavement coping styles, such as grief processing and avoidance were found to link positively with negative bereavement outcomes.47 By revealing stigma’s predictive effects on bereavement coping, present findings indicate coping’s potential mediating role in the relationship between stigma and bereavement outcomes.
The Strategy Level
In the network model, while grief processing is linked mainly within the same strategy across contexts, avoidance could be triggered across both strategies and contexts. Processing grief is especially difficult, exhausting, and confusing for children,48 so they may find it easier to try one coping strategy at a time. In contrast, when trying to avoid reminders of the loss, distance should be kept from any relevant clues, including emotions, thoughts, and conversations.
The Stigma-Processing Pathway
For grief processing, enacted stigma mainly connected to searching for meaning. Facing stigmatized deaths, children can have contradictory feelings of anger and abandonment as well as love and affection towards their deceased parents,49 and meaning making may help form counternarratives.50 Moreover, meaning making may help children construct continuing bonds to gain strength through inner guides (“What would he or she suggest that I do?”)46 to deal with enacted stigma.
Stigma-triggered meaning making began in contexts where AIDS-orphaned children were alone and with friends. Making sense of the loss alone would be safe. When support is needed, the rest of the grieving family may be too sad to provide help, while peers who are not directly involved with the death are more available.51
Enacted stigma also leads to more feeling expression, starting when AIDS-orphaned children are with community members. Stigma could serve as a loss reminder that evokes grief reactions.52 Since most of the stigma experiences measured in this study (eg, physical abuse or being called bad names by others) were more likely to be enacted by community members than family or friends, more grief reactions would be stirred up in those contexts. As sustaining emotions during bereavement are particularly hard for children,45 more expression is inevitable. This, in turn, could increase feeling expressions across contexts.
The Stigma-Avoidance Pathway
Although enacted stigma brings unavoidable feeling outbursts, it also contributes to intentional feeling suppression. Stigma triggers the whole avoidance network through “avoiding expressing feelings with community members”. This makes sense because a gradual avoidance process should start from with the most sensitive topic and the least intimate group. Avoidance measures like social withdrawal and emotion suppression may be used to manage embarrassment and stigma.53
A Paradox
The two pathways revealed a paradoxical picture. Enacted stigma stirs up complex feelings in orphans but forces them to suppress expressions. It creates stronger needs for meaning making but cuts supporting forces by promoting avoidance. Similar difficulties were vaguely mentioned in previous qualitative explorations regarding stigmatized deaths.54 For the first time, this study revealed how such a paradox forms quantitatively at the style and the strategy levels.
Limitations
As participants were recruited from a specific group in a certain region and only one type of stigma was measured, the generalizability of the findings is limited. In addition, the data are not recent enough. Nevertheless, as the study focused on the relationships between variables rather than the prevalence, the findings may not have been seriously distorted.
Practical Implications and Future Studies
In practice, it is imperative to reduce the HIV/AIDS stigma through public education and awareness, and support should be provided to bereaved individuals who suffer from enacted stigma to reduce alienation, shame, misunderstandings, and ambiguity.55 Preventing enacted stigma from interfering with people’s acceptance of the death and moving on with the loss is of paramount importance, for which meaning-oriented interventions could be applied.56 For children, practitioners could involve the surviving parent or primary caregivers to promote adaptive coping towards stigma and grief.57
Future studies could explore the style-level and strategy-level mediation pathways of “stigma – bereavement coping – grief outcomes”. Investigating the moderation effects of some protective factors that could buffer the negative effects of enacted stigma would also be useful. Interventions with randomized controlled trial designs could aim to break the link between enacted stigma and maladaptive bereavement coping. Moreover, the dyadic coping between the surviving parent and the child under the shadow of stigma would also provide insights.
Conclusion
Enacted stigma influences bereavement coping. At the style level, higher enacted stigma significantly predicted more grief processing and deliberate grief avoidance in the AIDS-orphaned children one year later. At the strategy level, enacted stigma stirs up complex feelings but forces AIDS-orphaned children to suppress expressions, and it increases the need to process grief through meaning making but cuts supporting forces by promoting avoidance. Interventions are imperative to reduce enacted stigma, improve emotion regulation, and facilitate meaning making for people bereaved by stigmatized deaths.
Abbreviations
AIDS, acquired immune deficiency syndrome; HIV, human immunodeficiency virus; PTSD, post-traumatic stress disorder; SES, socioeconomic status.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Dr Peilian Chi (email: [email protected]) upon reasonable request.
Ethics Approval and Informed Consent
The present study complies with the Declaration of Helsinki. All procedures involving human subjects were approved by the Institutional Review Boards or the research ethics committee at Wayne State University (HIC# 099205B3F), Henan University (1R01MH76488-01), and University of Macau (MYRG2017-00173-FSS). For children’s participation, written assent or oral assent was obtained from the children, and written or oral consent was obtained from their caregivers or legal guardians.
Consent for Publication
The authors confirm that the details of any images, videos, recordings, etc., can be published, and that the persons providing consent have been shown the article contents to be published.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was support by the [Science and Technology Development Fund (FDCT)] under grant [number 0095/2022/AFJ] and [number 0087/2021/A]; [National Institute of Nursing Research] under Grant [R01NR13466]; [Start-Up Fund of Beijing Normal University at Zhuhai] under Grant [number 310432101]; and [Southeast University Zhishan Young Scholars Support Program]. None of the sponsors involved in study design, the collection, analysis and interpretation of data, the writing of the report or the decision to submit the article for publication.
Disclosure
The authors report there are no competing interests to declare.
References
1. Link BG, Phelan JC. Conceptualizing stigma. Annu Rev Socio. 2001;27(1):363–385. doi:10.1146/annurev.soc.27.1.363
2. Tse WF, Huang W. Stigma among HIV/AIDS patients in China. HIV AIDS Rev. 2017;16(1):11–17. doi:10.5114/hivar.2017.65921
3. Herek GM, Gillis JR, Cogan JC. Internalized stigma among sexual minority adults: insights from a social psychological perspective. J Couns Psychol. 2009;56(1):32–43. doi:10.1037/a0014672
4. Houck JA. A comparison of grief reactions in cancer, hiv/aids, and suicide bereavement. J HIV/AIDS Soc Serv. 2007;6(3):97–112. doi:10.1300/J187v06n03_07
5. Chi P, Li X, Zhao J, Zhao G. Vicious circle of perceived stigma, enacted stigma and depressive symptoms among children affected by HIV/AIDS in China. AIDS Behav. 2014;18(6):1054–1062. doi:10.1007/s10461-013-0649-z
6. Yu NX, Chow AYM, Chan CLW, Zhang J, Stewart SM. Stigma never dies: mourning a spouse who died of AIDS in China. Psychiatry Research. 2015;230(3):968–970. doi:10.1016/j.psychres.2015.10.034
7. Meini B, Tognetti Bordogna M. The impact of HIV-related stigma on children orphaned by AIDS or living with seropositive caregivers. Int Rev Soc. 2018;28(3):541–555. doi:10.1080/03906701.2018.1529090
8. Harms S, Jack S, Ssebunnya J, Kizza R. The orphaning experience: descriptions from Ugandan youth who have lost parents to HIV/AIDS. Child Adolesc Psychiatry Ment. 2010;4(1):6. doi:10.1186/1753-2000-4-6
9. Yassin Z, Erasmus C, Frantz J. HIV-related stigma and the psychosocial well-being of children orphaned by AIDS: a systematic review. Vulnerable Child Youth Stud. 2018;13(3):247–258. doi:10.1080/17450128.2018.1457193
10. Xu T, Yan Z, Duan S, Wang C, Rou K, Wu Z. Psychosocial well-being of children in hiv/aids-affected families in southwest china: a qualitative study. J Fam Stud. 2009;18(1):21–30. doi:10.1007/s10826-008-9202-5
11. Thupayagale-Tshweneagae G, Benedict S. The burden of secrecy among South African adolescents orphaned by HIV and AIDS. Issues Ment Health Nurs. 2011;32(6):355–358. doi:10.3109/01612840.2011.576128
12. Evans A, Abrahamson K. The influence of stigma on suicide bereavement: a systematic review. J Psychosoc Nurs Ment Health Serv. 2020;58(4):21–27. doi:10.3928/02793695-20200127-02
13. Hanschmidt F, Treml J, Klingner J, Stepan H, Kersting A. Stigma in the context of pregnancy termination after diagnosis of fetal anomaly: associations with grief, trauma, and depression. Arch Womens Ment Health. 2018;21(4):391–399. doi:10.1007/s00737-017-0807-9
14. Stroebe MS, Hansson RO, Schut H, Stroebe W. Bereavement research: contemporary perspectives. In: Handbook of Bereavement Research and Practice: Advances in Theory and Intervention. American Psychological Association; 2008:3–25.
15. Boon H, Ruiter RAC, James S, van den Borne B, Williams E, Reddy P. Correlates of grief among older adults caring for children and grandchildren as a consequence of HIV and AIDS in South Africa. J Aging Health. 2010;22(1):48–67. doi:10.1177/0898264309349165
16. Lee S-A, Kim SJ, Kim HJ, et al. Family cohesion is differently associated with felt stigma depending on enacted stigma in adults with epilepsy. Epilepsy Behavior. 2020:112107446. doi:10.1016/j.yebeh.2020.107446
17. Amini-Tehrani M, Zamanian H, Daryaafzoon M, et al. Body image, internalized stigma and enacted stigma predict psychological distress in women with breast cancer: a serial mediation model. J Adv Nurs. 2021;77(8):3412–3423. doi:10.1111/jan.14881
18. Li X, Yan H, Wang W, Yang H, Li S. Association between enacted stigma, internalized stigma, resilience, and depressive symptoms among young men who have sex with men in China: a moderated mediation model analysis. Ann Epidemiol. 2021;56:1–8. doi:10.1016/j.annepidem.2021.01.001
19. Stroebe M, Schut H. The dual process model of coping with bereavement: a decade on. J Death Dying. 2010;61(4):273–289. doi:10.2190/OM.61.4.b
20. Neimeyer RA, Klass D, Dennis MR. A social constructionist account of grief: loss and the narration of meaning. Death Studies. 2014;38(8):485–498. doi:10.1080/07481187.2014.913454
21. Stroebe M, Boelen PA, van den Hout M, Stroebe W, Salemink E, van den Bout J. Ruminative coping as avoidance: a reinterpretation of its function in adjustment to bereavement. Eur Arch Psychiatry Clin Neurosci. 2007;257(8):462–472. doi:10.1007/s00406-007-0746-y
22. Stroebe M, Schut H, Boerner K. Models of coping with bereavement: an updated overview / modelos de afrontamiento en duelo: un resumen actualizado. Psychol Stud. 2017;38(3):582–607. doi:10.1080/02109395.2017.1340055
23. Bonanno GA, Papa A, Lalande K, Zhang N, Noll JG. Grief processing and deliberate grief avoidance: a prospective comparison of bereaved spouses and parents in the United States and the people’s republic of China. J Consult Clin Psychol. 2005;73(1):86–98. doi:10.1037/0022-006x.73.1.86
24. Eisma MC, Stroebe MS. Emotion regulatory strategies in complicated grief: a systematic review. Behav Ther. 2021;52(1):234–249. doi:10.1016/j.beth.2020.04.004
25. Pressman DL, Bonanno GA. With whom do we grieve? social and cultural determinants of grief processing in the United States and China. J Soc Pers Relat. 2007;24(5):729–746. doi:10.1177/0265407507081458
26. Chapple A, Ziebland S, Hawton K. Taboo and the different death? Perceptions of those bereaved by suicide or other traumatic death. Sociol Health Illn. 2015;37(4):610–625. doi:10.1111/1467-9566.12224
27. Cohen H, Samp JA. Grief communication: exploring disclosure and avoidance across the developmental spectrum. West J Commun. 2018;82(2):238–257. doi:10.1080/10570314.2017.1326622
28. Schotanus-Dijkstra M, Havinga P, van Ballegooijen W, Delfosse L, Mokkenstorm J, Boon B. What do the bereaved by suicide communicate in online support groups? A content analysis. Crisis J Crisis Interv Suic Prev. 2014;35(1):27–35. doi:10.1027/0227-5910/a000225
29. Borsboom D, Cramer AOJ. Network analysis: an integrative approach to the structure of psychopathology. Annu Rev Clin Psychol. 2013;9(1):91–121. doi:10.1146/annurev-clinpsy-050212-185608
30. McNally RJ. Network analysis of psychopathology: controversies and challenges. Annu Rev Clin Psychol. 2020;17:31–53. doi:10.1146/annurev-clinpsy-081219-092850
31. Burger J, Stroebe MS, Perrig-Chiello P, et al. Bereavement or breakup: differences in networks of depression. J Affect Disord. 2020;267:1–8. doi:doi:10.1016/j.jad.2020.01.157
32. Lass ANS, Winer ES, Collins AC, Rokke PD. The associations among distress tolerance, unhelpful coping behaviors, and symptoms of depression: a network analysis. Cognit Ther Res. 2020;44(6):1077–1090. doi:10.1007/s10608-020-10131-2
33. Peters J, Bellet BW, Jones PJ, Wu GWY, Wang L, McNally RJ. Posttraumatic stress or posttraumatic growth? Using network analysis to explore the relationships between coping styles and trauma outcomes. J Anxiety Disord. 2021;78102359. doi:10.1016/j.janxdis.2021.102359
34. Zhao J, Li X, Fang X, et al. Stigma against children affected by AIDS (SACAA): psychometric evaluation of a brief measurement scale. AIDS Behav. 2010;14(6):1302–1312. doi:10.1007/s10461-009-9629-8
35. Poltorak DY, Glazer JP. The development of children’s understanding of death: cognitive and psychodynamic considerations. Child Adolesc Psychiatr Clin N Am. 2006;15(3):567. doi:10.1016/j.chc.2006.03.003
36. Hopkins M. The Development of Children’s Understanding of Death. [Dissertation/Thesis]; 2014.
37. Bonoti F, Leondari A, Mastora A. Exploring children’s understanding of death: through drawings and the death concept questionnaire. Death Studies. 2013;37(1):47–60. doi:10.1080/07481187.2011.623216
38. Li X, Barnett D, Fang X, et al. Lifetime incidences of traumatic events and mental health among children affected by HIV/AIDS in rural China. J Clin Child Adolesc Psychol. 2009;38(5):731–744. doi:10.1080/15374410903103601
39. Faul F, Erdfelder E, Buchner A, Lang A-G. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
40. Kolaczyk ED, Krivitsky PN. On the question of effective sample size in network modeling: an asymptotic inquiry. Stat Sci. 2015;30(2):184–198. doi:10.1214/14-STS502
41. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (strobe) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):1623. doi:10.1371/journal.pmed.0040296
42. Chi P, Li X, Douglas B, Zhao J, Zhao G. Do children orphaned by AIDS experience distress over time? A latent growth curve analysis of depressive symptoms. Psychol Health Med. 2014;19(4–6):
43. Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50(1):195–212. doi:10.3758/s13428-017-0862-1
44. Friedman J, Hastie T, Tibshirani R. Sparse inverse covariance estimation with the graphical lasso. Biostatistics. 2008;9(3):432–441. doi:10.1093/biostatistics/kxm045
45. Li X, Naar-King S, Barnett D, Stanton B, Fang X, Thurston C. A developmental psychopathology framework of the psychosocial needs of children orphaned by HIV. J Assoc Nurses AIDS Care. 2008;19(2):147–157. doi:10.1016/j.jana.2007.08.004
46. Hansen DM, Sheehan DK, Stephenson PS, Mayo MM. Parental relationships beyond the grave: adolescents’ descriptions of continued bonds. Palliative Supportive Care. 2016;14(4):358–363. doi:10.1017/S1478951515001078
47. Boelen PA, Eisma MC. Anxious and depressive avoidance behavior in post-loss psychopathology: a longitudinal study. Anxiety Stress Coping. 2015;28(5):587–600. doi:10.1080/10615806.2015.1004054
48. Stachnik K, Kotlińska-Lemieszek A. A child after the death of a parent or another important person. Medycy Paliat. 2018;10(4):184–190. doi:10.5114/pm.2018.83275
49. Hagström AS. Suicide stigma’ renegotiated: storytelling, social support and resistance in an internet-based community for the young suicide-bereaved. Qual Soc Work. 2017;16(6):775–792. doi:10.1177/1473325016644039
50. Gillies J, Neimeyer RA. Loss, grief, and the search for significance: toward a model of meaning reconstruction in bereavement. J Constr Psychol. 2006;19(1):31–65. doi:10.1080/10720530500311182
51. Dopp AR, Cain AC. The role of peer relationships in parental bereavement during childhood and adolescence. Death Studies. 2012;36(1):41–60. doi:10.1080/07481187.2011.573175
52. Christopher ML, Julie BK, Benjamin O, Ryan MH, Robert SP. The interplay between posttraumatic stress and grief reactions in traumatically bereaved adolescents: when trauma, bereavement, and adolescence converge. Adolesc Psychiatry. 2017;7(4):266–285. doi:10.2174/2210676608666180306162544
53. Goulah-Pabst DM. Suicide loss survivors: navigating social stigma and threats to social bonds. Omega. 2021. doi:10.1177/00302228211026513
54. Demmer C, Rothschild N. Bereavement among South African adolescents following a sibling’s death from AIDS. Ajar-African J Aids Research Apr. 2011;10(1):15–24 Pii 938657583. doi:10.2989/16085906.2011.575544
55. Wood K, Chase E, Aggleton P. ‘Telling the truth is the best thing’: teenage orphans’ experiences of parental AIDS-related illness and bereavement in Zimbabwe. Soc Sci Med. 2006;63(7):1923–1933. doi:10.1016/j.socscimed.2006.04.027
56. Danvers AF, Scott BG, Shiota MN, Tein J-Y, Wolchik SA, Sandler II. Effects of therapeutic intervention on parentally bereaved children’s emotion reactivity and regulation 15 years later. Prev Sci. 2020;21(8):1017–1027. doi:10.1007/s11121-020-01142-2
57. Jiao K, Chow AYM, Chen C. Dyadic relationships between a surviving parent and children in widowed families: a systematic scoping review. Report Family Process. 2021;60(3):888. doi:10.1111/famp.12610
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.