Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Emphysema Phenotype and 1‑Year Readmission Risk After Acute Exacerbation of COPD: A Real-World Study Using Propensity Score-Based Methods
Authors Fu C ![]() , Wu Y, Huang A, Chen G, Hu Y
, Wu Y, Huang A, Chen G, Hu Y ![]()
Received 6 April 2026
Accepted for publication 28 May 2026
Published 4 June 2026 Volume 2026:21 614880
DOI https://doi.org/10.2147/COPD.S614880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Chengfeng Fu,1,2,* Yanling Wu,1,* Aixia Huang,1 Guangxi Chen,1 Ying Hu1
1Respiratory and Critical Care Medicine, The Second People’s Hospital of Banan District, Chongqing, 400054, People’s Republic of China; 2Department of Respiratory Medicine, The Second Affiliated Hospital, Chongqing Medical University, Chongqing, 400010, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guangxi Chen, Email [email protected] Ying Hu, Email [email protected]
Background: The association between emphysema phenotype and readmission risk after acute exacerbation of chronic obstructive pulmonary disease (AECOPD) remains unclear. This real‑world study evaluated this association with rigorous confounding control.
Methods: This retrospective cohort study included patients hospitalized for AECOPD (2023). Emphysema was diagnosed by chest CT. The outcome was 1‑year acute exacerbation‑related readmission. Propensity score matching (PSM), multiple-weighting methods, doubly robust analysis, Schoenfeld residuals test, Kaplan‑Meier curves, and subgroup analyses were used.
Results: Among 875 patients, PSM yielded 171 matched pairs. Emphysema was associated with higher readmission risk in adjusted analysis (HR=1.64, 95% CI:1.17– 2.32, p=0.005), and after PSM (HR=1.81, 95% CI:1.22– 2.68, p=0.003). Results were consistent across all weighting methods. The Schoenfeld test satisfied the proportional hazards assumption. Kaplan‑Meier curves showed significantly lower readmission‑free survival in the emphysema group. Subgroup analyses revealed a stronger association in patients not using inhaled corticosteroids.
Conclusion: Emphysema was associated with a higher risk of 1‑year readmission after AECOPD. The emphysema phenotype may aid risk stratification and guide individualized therapy, though these findings should be interpreted cautiously.
Keywords: AECOPD, emphysema, readmission, propensity score matching
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of hospitalization due to recurrent exacerbations and imposes a major burden on healthcare expenditure.1 In China, COPD has become the third leading cause of death, placing substantial economic and social strain on the healthcare system.2,3 Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is characterized by rapid worsening of symptoms, including dyspnea, cough, and increased sputum production, typically triggered by respiratory infections and air pollution.4 These exacerbations not only represent a major determinant of adverse outcomes but are also closely associated with elevated readmission rates.1,5 Hospitalization for AECOPD accelerates lung function decline, impairs quality of life, increases the risk of future exacerbations, and raises mortality. AECOPD is a critical factor influencing the health and prognosis of patients with COPD. Approximately 40% of patients experience readmission within one year after discharge.6 Frequent readmissions are associated with poor patient outcomes, as well as a significant increase in family economic burden and healthcare resource utilization. Patients with AECOPD often have coexisting chronic disease progression and recurrent exacerbations, which significantly increase the risk of hospital readmission.7 AECOPD poses a major challenge in disease management, with considerable adverse effects on patient health, readmission rates, and the overall disease trajectory. Early identification of high‑risk patients, clarification of risk factors for AECOPD readmission, and implementation of targeted interventions are essential for reducing readmission rates and improving patient prognosis.
Emphysema is an important phenotype of COPD, characterized by destruction of the air spaces distal to the terminal bronchioles.8 Advances in imaging technology have evolved from an adjunctive tool to a core component in COPD research and clinical care.9 It represents a clearly identifiable imaging feature on chest CT that can be readily assessed in routine practice; it is closely associated with decline in lung function, reduced exercise tolerance, and increased mortality.10–13 Pathophysiologically, the irreversible parenchymal destruction, persistent airway inflammation, and reduced physiological reserve that characterize emphysema may lower the threshold for acute exacerbations and impair post‑discharge recovery, thereby increasing susceptibility to readmission. However, its independent impact on the risk of readmission after discharge in patients with AECOPD remains controversial.14 Although the clinical significance of emphysema has been widely recognized, existing studies evaluating its association with readmission risk often have limitations. Some studies have reported a significant association between emphysema and higher readmission rates, whereas other systematic reviews and meta-analyses have found that the reported risk factors vary considerably across studies and regions,15 with no consistent independent effect identified for emphysema.16 While factors such as smoking history and prior hospitalizations significantly increased readmission risk, the conclusions regarding emphysema itself as an independent risk factor remained heterogeneous.16 These discrepancies may arise from heterogeneity in study design, including inadequate control of confounding factors, limited sample sizes, differences in patient selection criteria, varying follow-up durations, inconsistent outcome definitions, and insufficient consideration of potential effect modifiers such as inhaled corticosteroid (ICS) use. Therefore, in a real‑world setting, adopting more rigorous statistical methods to control for confounding, comprehensively assessing the independent effect of the emphysema phenotype on readmission risk in AECOPD patients, and exploring potential effect modifiers are of great clinical and scientific value.
Based on this, the present study applied propensity score matching (PSM), multivariable Cox regression, multiple-weighting methods, and doubly robust analysis to achieve more rigorous confounding control than has been typical in previous research, thereby providing more robust evidence regarding the independent effect of emphysema on readmission risk in a real-world setting. In addition, through systematic subgroup analyses, the study explored whether the association is modified by clinically relevant factors, including ICS use. The aim is to provide more robust evidence‑based support for risk stratification and individualized management of AECOPD patients.
Materials and Methods
Study Design and Population
The study was a single‑center retrospective cohort study conducted at the Second People’s Hospital of Banan District, Chongqing, China, which is a Grade II‑A general hospital. We consecutively enrolled patients with AECOPD who were hospitalized for the first time in the Department of Respiratory and Critical Care Medicine between January 2023 and December 2023. Inclusion criteria were a primary diagnosis of AECOPD based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) clinical criteria (progressive dyspnea, chronic cough or sputum production, and a history of exposure to risk factors), documented by International Classification of Diseases, Tenth Revision (ICD-10) codes J44.001 or J44.101, and age ≥40 years. Exclusion criteria were severely missing clinical data; presence of other active pulmonary diseases (eg., tuberculosis, lung cancer, interstitial lung disease); and immunodeficiencies or long‑term use of immunosuppressants. All patients were followed up for one year after discharge, with the follow‑up end date of December 31, 2024. Initially, 1025 patients were screened, and after applying the exclusion criteria, 875 patients were included in the final statistical analysis (Supplemental Figure S1).
According to the national Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects, the use of anonymized retrospective data in this study posed no risk to patients and met the criteria for exemption from ethical review. The Ethics Committee of our hospital approved the exemption of ethical review for this study (approval No. 2025‑KL‑022). This study was conducted in accordance with the principles of the Declaration of Helsinki (revised in 2013). The results were reported in accordance with the STROBE statement.17
Variables
The outcome variable was the readmission rate due to acute exacerbation of COPD within one year. Readmission data were collected not only from the index hospital’s electronic medical record system but also through the Chongqing Municipal Medical Examination and Mutual Recognition System, a regional platform that enables retrieval of hospitalization and visit records from public hospitals across the municipality. This dual-source approach was intended to capture readmissions to other public hospitals within Chongqing.
The diagnosis of emphysema was based on chest computed tomography (CT) findings. Two experienced imaging specialists independently assessed emphysema changes (eg, low‑attenuation areas and parenchymal destruction) by visual evaluation, combined with clinical characteristics and chest CT results, to perform a standardized clinical assessment.
Based on the literature and clinical knowledge,18,19 potential confounding variables included: demographic characteristics (age, sex, height, weight); smoking status (never, former, current), with calculation of pack‑years; comorbidities (hypertension, diabetes, chronic bronchitis, coronary heart disease); laboratory indicators (platelet count, D‑dimer, fibrinogen, albumin, blood urea nitrogen, creatinine) obtained within 24 hours of admission; and treatment‑related factors (ICS use). Chronic bronchitis was defined clinically as chronic productive cough for at least three months per year for two consecutive years.
Statistical Analysis
Categorical variables were expressed as percentages (%) and analyzed using the chi‑square test. Continuous variables with a normal distribution were expressed as mean ± standard deviation (SD) and analyzed using one‑way analysis of variance (ANOVA). Continuous variables that did not follow a normal distribution were described as median (interquartile range) and compared using the Kruskal‑Wallis test.
Cox proportional hazards regression models were used to assess the association between emphysema and the risk of 1‑year readmission, calculating hazard ratios (HRs) and their 95% confidence intervals (CIs). To control for confounding and test the robustness of the results, three multivariable models were constructed sequentially: Model 1 adjusted for sex, age, height, and weight; Model 2 further adjusted for smoking status, pack‑years, hypertension, diabetes, chronic bronchitis, and coronary heart disease; Model 3 additionally adjusted for platelet count, D‑dimer, fibrinogen, albumin, blood urea nitrogen, creatinine, and ICS use.
The proportional hazards assumption of the Cox models was tested using Schoenfeld residuals. Kaplan‑Meier survival curves were plotted, and differences in survival between groups were compared using the log‑rank test. Multiple imputation was used to handle missing covariate data.
To evaluate the consistency of the association across different subgroups, subgroup analyses were performed according to sex, age (<65 years, ≥65 years), smoking status (never, former, current), presence or absence of chronic bronchitis, presence or absence of coronary heart disease, and ICS use.
PSM and multiple propensity score‑based methods were employed to control for confounding bias. Matching variables included sex, age, height, weight, smoking status, pack‑years, hypertension, diabetes, chronic bronchitis, coronary heart disease, platelet count, D‑dimer, fibrinogen, albumin, blood urea nitrogen, creatinine, and ICS use. A caliper of 0.2 was used for 1:1 nearest‑neighbor matching, and a standardized mean difference (SMD) <0.2 was considered to indicate adequate balance between groups. The discriminative ability of the PSM model was evaluated using receiver operating characteristic (ROC) curve analysis. To further validate the robustness of the results, we applied inverse probability of treatment weighting (IPTW), standardized mortality ratio weighting (SMRW), propensity score adjusted weighting (PSAW), and overlap weighting (OW).20,21
Traditionally, when regression analysis or propensity score models are used to estimate causal effects, unbiased estimates are obtained only when both statistical models are correctly specified. Doubly robust analysis combines a multivariable regression model with a propensity score model to estimate the association and causal effect of exposure on outcome, thereby yielding unbiased effect estimates. Therefore, to ensure the accuracy of our results, we further confirmed the association between emphysema and readmission risk using doubly robust analysis.22
To assess the sensitivity of our results to potential unmeasured confounding, we calculated E‑values. All statistical analyses were performed using R software (version 4.2.2, R Foundation for Statistical Computing, Vienna, Austria) and Free Statistics data analysis platform (Beijing, China). A two‑sided P‑value <0.05 was considered statistically significant.
Results
A total of 875 patients with AECOPD were included in the analysis, of whom 675 (77.1%) were in the emphysema group and 200 (22.9%) in the non‑emphysema group. After PSM, 171 pairs of patients were successfully matched, and baseline characteristics were well balanced between the two groups (Figure 1). After matching, the SMDs for all covariates were <0.2, except for chronic bronchitis and albumin, which still showed some differences (SMD = 0.244 and 0.248, respectively) (Table 1). ROC curve analysis showed that the area under the curve (AUC) of the PSM model was 77.9%, indicating good discriminative ability of the matching variables for group allocation (Figure 2).
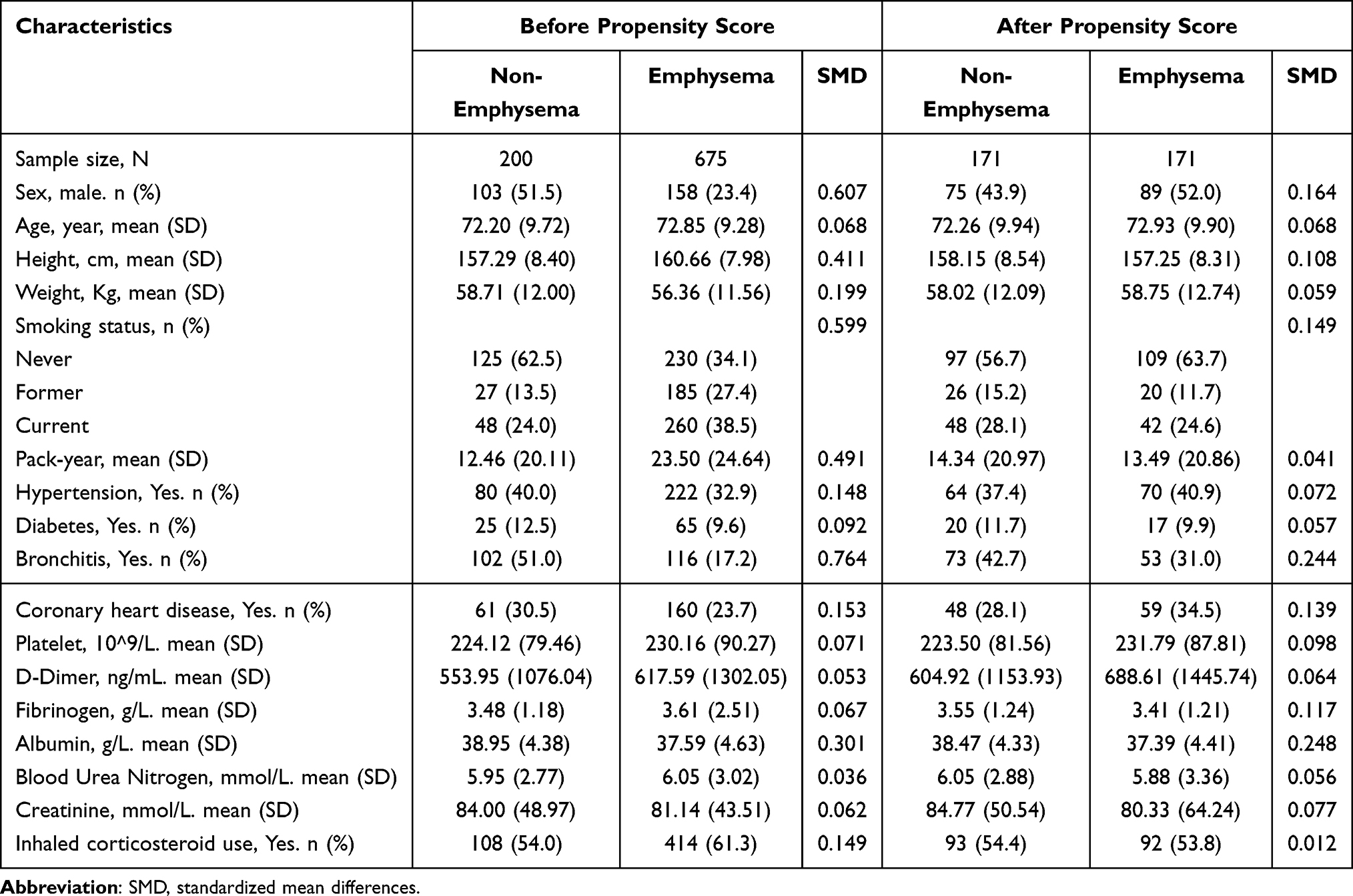 |
Table 1 Participant Characteristics by Emphysema Groups Before and After Propensity Score Matching (PSM) |
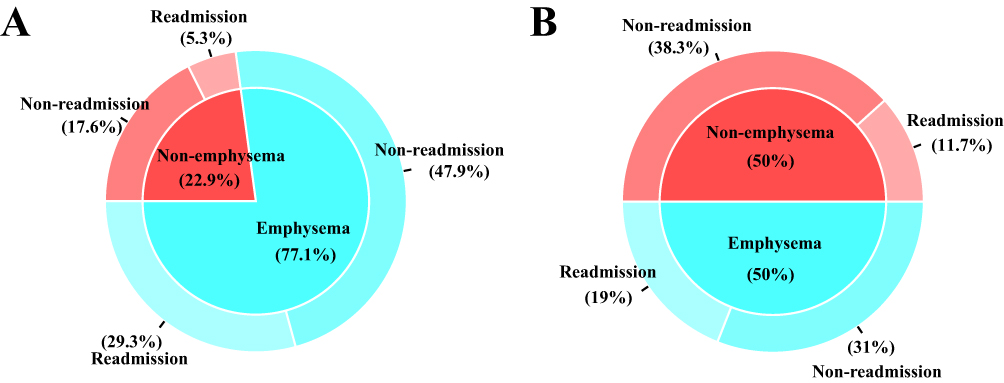 |
Figure 1 Comparison of the proportion of emphysema and non-emphysema patients and the 1-year readmission rate before (A) and after (B) propensity score matching (PSM). |
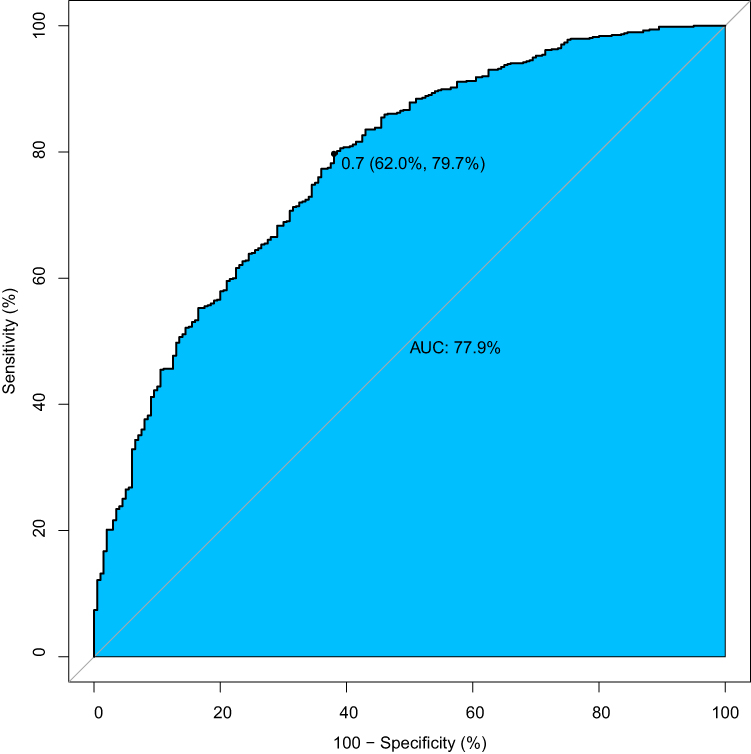 |
Figure 2 Receiver operating characteristic (ROC) curve for readmission. |
During the 1-year follow‑up period, 302 patients (34.5%) experienced readmission due to acute exacerbation. Cox regression analysis showed that in the unadjusted model, the risk of readmission was significantly higher in the emphysema group than in the non‑emphysema group (HR = 1.84, 95% CI: 1.34–2.52, P < 0.001). After stepwise adjustment for confounders, the association remained robust (Model 3: HR = 1.64, 95% CI: 1.17–2.32, P = 0.005) (Table 2). After PSM, the HR for the association between emphysema and readmission risk was 1.81 (95% CI: 1.22–2.68, P = 0.003). Using multiple-weighting methods (IPTW, SMRW, PSAW, and OW), the effect estimates remained consistent. The doubly robust analysis also yielded a stable result (HR = 1.77, 95% CI: 1.17–2.66, P = 0.006) (Table 2). E‑value analysis showed that the minimum strength of association that an unmeasured confounder would need to have with both exposure and outcome to explain away the observed effect was 2.33, suggesting that the results were robust to potential unmeasured confounding (Supplemental Figure S2).
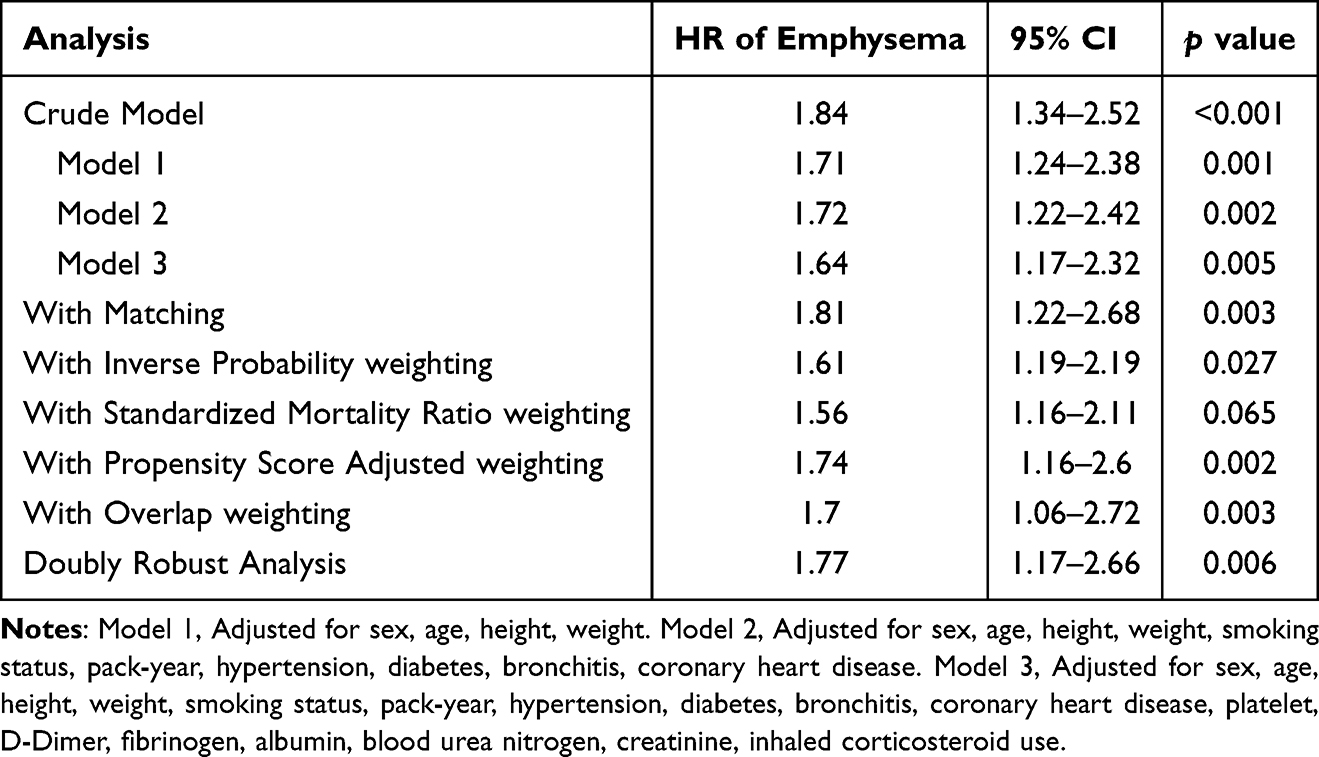 |
Table 2 Associations Between Emphysema and the Outcome in the Crude Analysis, Multivariable Analysis, and Propensity-Score Analyses |
The Schoenfeld residual test indicated that the proportional hazards assumption was satisfied in all models (Supplemental Figure S3). Kaplan‑Meier survival curves showed that the readmission‑free survival rate was significantly lower in the emphysema group than in the non‑emphysema group, both before and after PSM (Figure 3) (log‑rank P < 0.05).
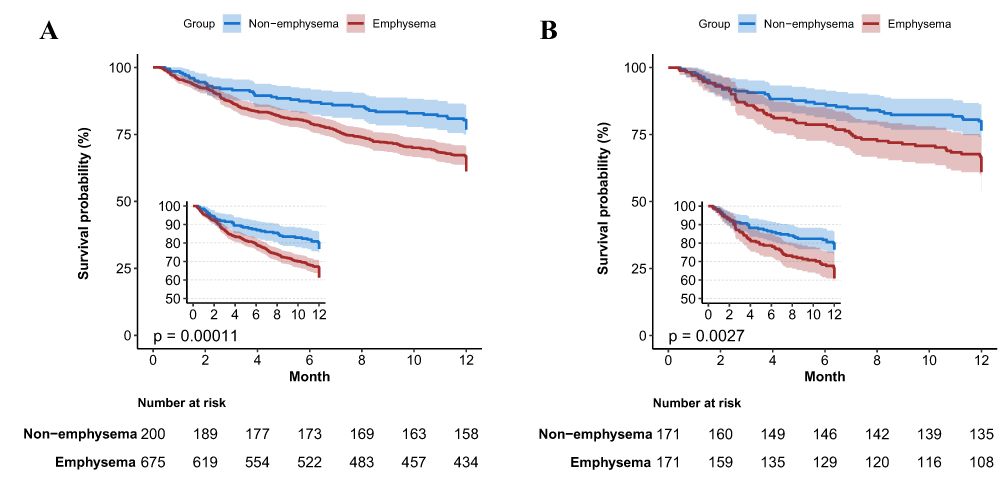 |
Figure 3 Kaplan-Meier survival curve of readmission for patients with AECOPD before (A) and after (B) propensity score matching (PSM). |
Forest plots displayed the results of subgroup analyses (Figure 4). Subgroup analyses before matching showed that the association between emphysema and readmission risk was more pronounced in males (HR = 1.79), patients aged ≥65 years (HR = 1.59), those with chronic bronchitis (HR = 2.22), those with coronary heart disease (HR = 1.97), and those not using ICS (HR = 2.21). However, no significant interactions were observed across subgroups (all interaction P > 0.05) (Table 3). Subgroup analyses after matching yielded generally similar results. Notably, in the subgroup not using ICS, the association between emphysema and readmission risk was further strengthened (HR = 3.31, 95% CI: 1.59–6.86, P = 0.001), with an interaction P‑value of 0.03, suggesting that ICS use appeared to modify the association between emphysema and readmission in patients with emphysema (Table 4). All subgroup analyses, especially those conducted in the smaller post‑matching cohort, should be considered exploratory and hypothesis‑generating. Estimates in subgroups with limited sample sizes are inherently unstable and should be interpreted with caution.
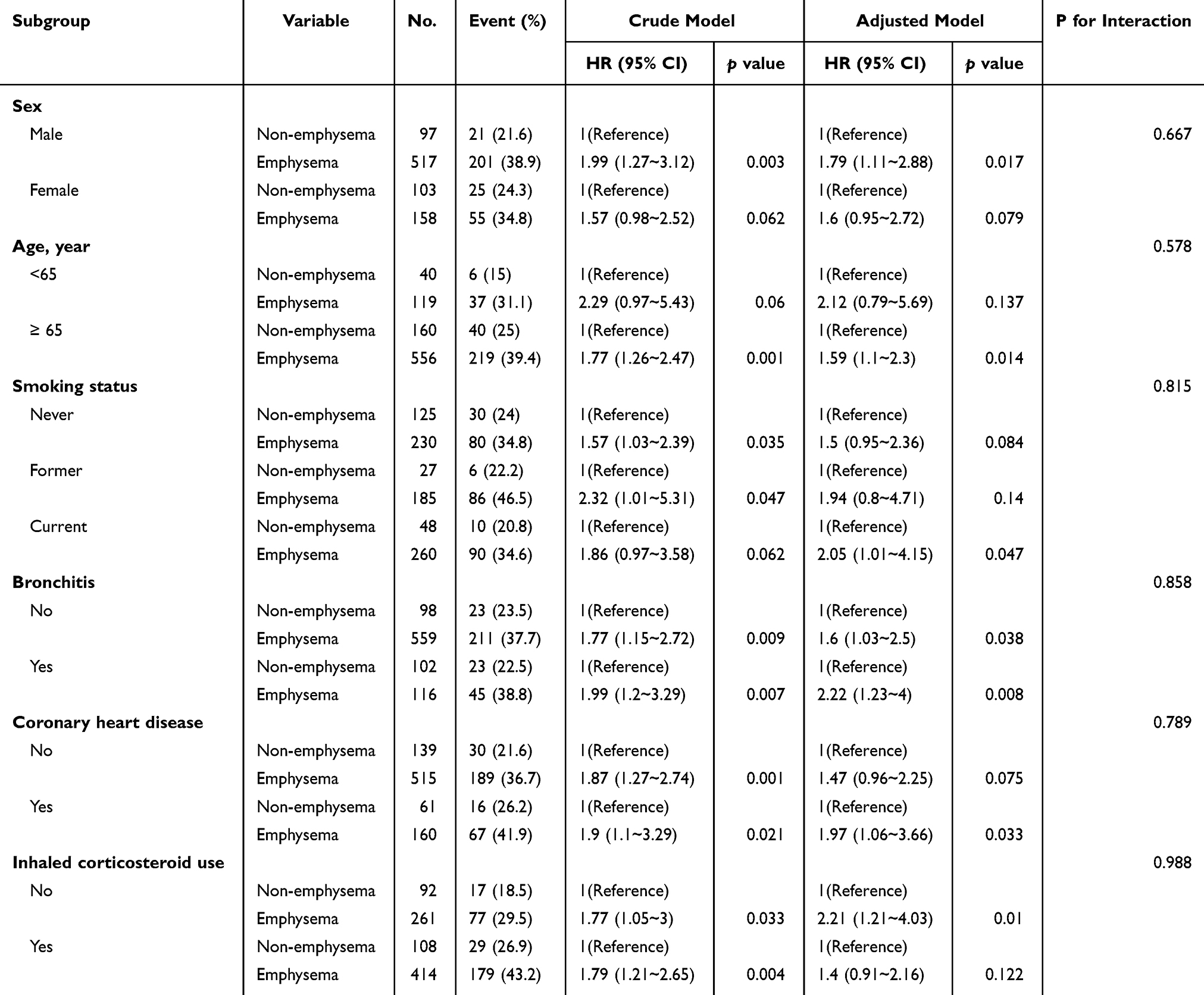 |
Table 3 Subgroup Analysis Before Propensity Score Matching (PSM) |
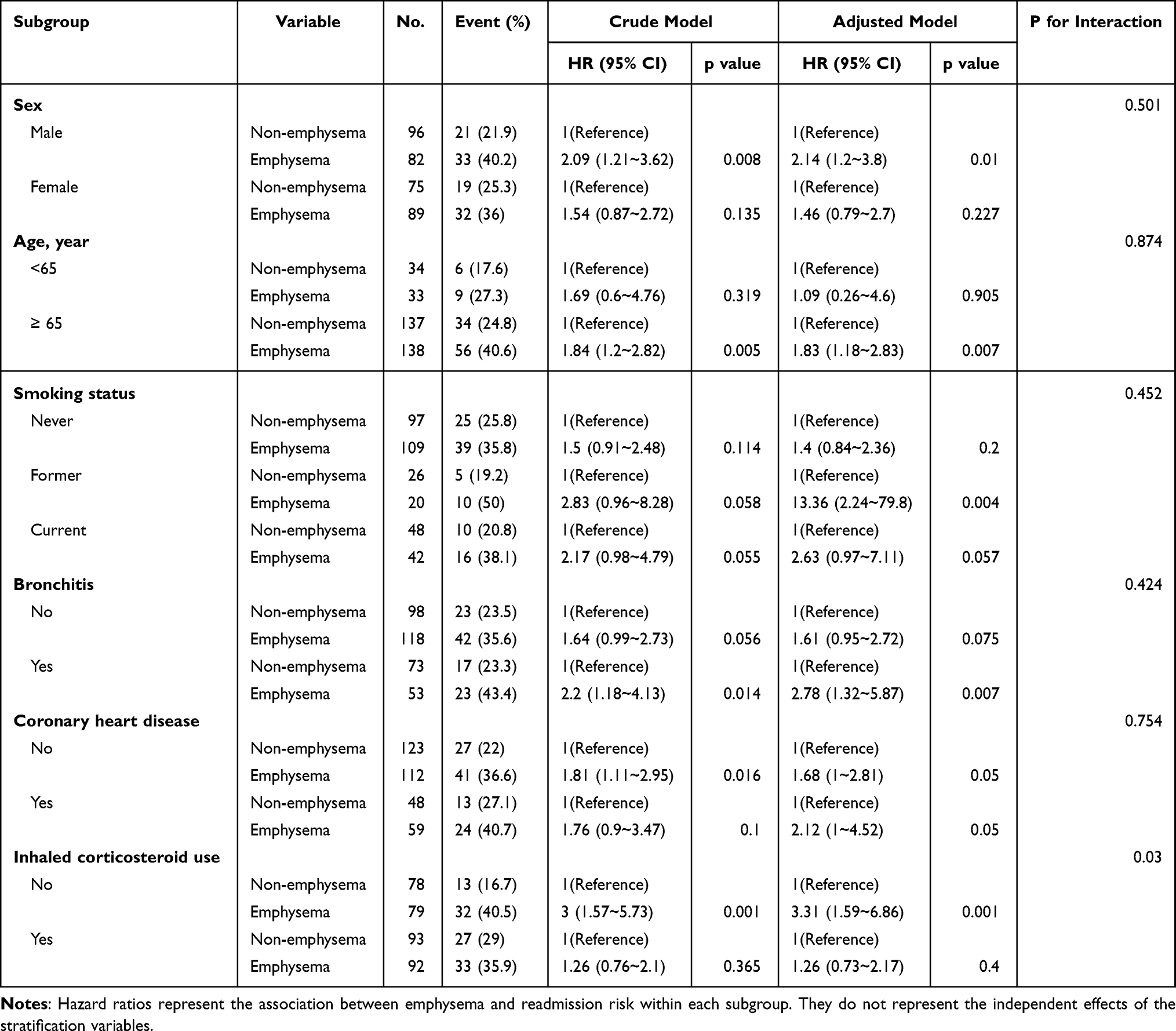 |
Table 4 Subgroup Analysis After Propensity Score Matching (PSM) |
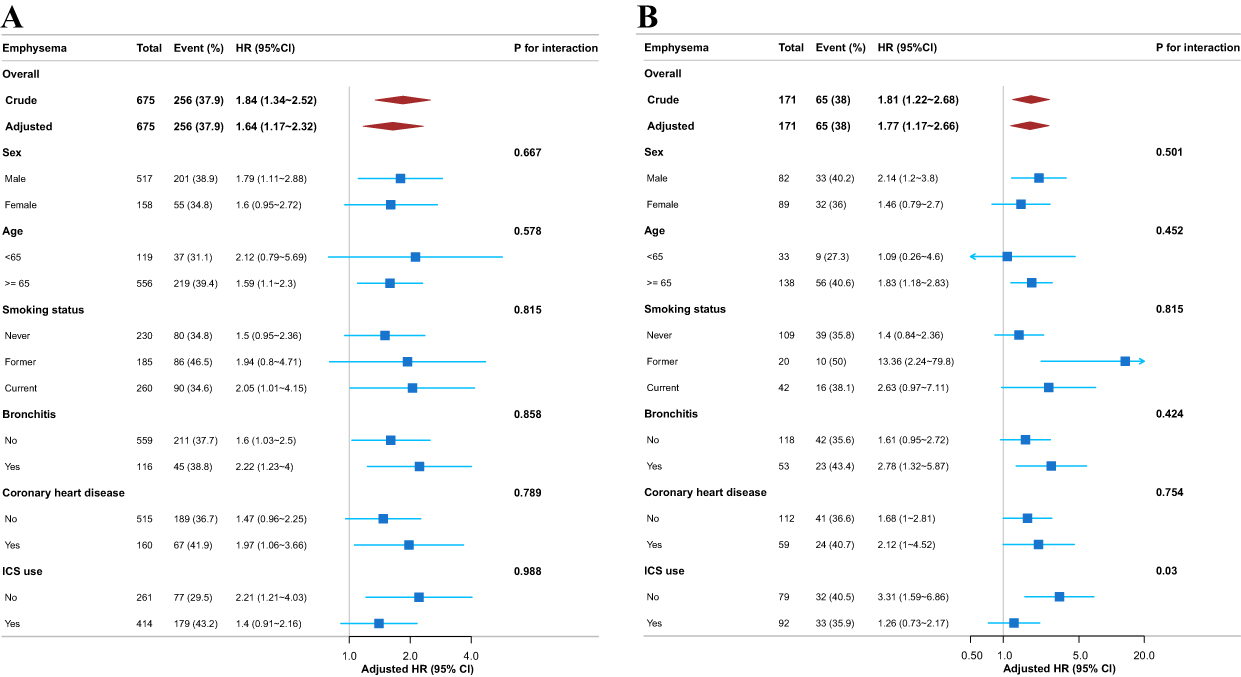 |
Figure 4 Subgroup analysis evaluating the association between emphysema and the 1-year readmission risk in patients with AECOPD before (A) and after (B) propensity score matching (PSM). |
Discussion
This study, based on real‑world clinical data and employing PSM and multiple-weighting methods, systematically evaluated the association between the emphysema phenotype and the risk of acute exacerbation‑related readmission within one year after discharge in patients with AECOPD. The results showed that the risk of one year readmission was significantly higher in patients with emphysema than in those without emphysema.
Previous studies on the association between emphysema and readmission risk in COPD patients have yielded inconsistent findings. Some studies have demonstrated a significant association between the emphysema phenotype and readmission risk. Cerezo Lajas et al compared patients with high‑frequency readmission (≥2 times within 30 days) and those with low‑frequency readmission (0–1 time) and found that the proportion of the emphysema phenotype was higher in the high‑frequency readmission group, with a significantly increased readmission risk in patients with the emphysema phenotype.23 Similarly, Andres Gimenez Velando et al reported that among patients readmitted within 1 month and 3 months after discharge, the proportion of the exacerbator with emphysema phenotype was significantly higher than that in the non‑readmission group, further supporting the association between emphysema and readmission.24 However, other studies have not found an independent association of emphysema. A systematic review by Njoku et al15 which included 57 studies from 30 countries, explicitly noted that the reported factors associated with readmission varied across studies, and that this variation may reflect differences in regional healthcare environments, accessibility of community services, and patient population characteristics. The review pointed out that risk factors for COPD‑related readmission “cannot be generalised”, and that interventions should be tailored to the local healthcare context. Moreover, a meta‑analysis in Asian populations showed that although factors such as smoking history, pulmonary heart disease, nutritional disorders, male sex, and multiple prior hospitalizations significantly increased readmission risk,16 the conclusions regarding emphysema itself as an independent risk factor remained heterogeneous across studies. These discrepancies may arise from heterogeneity in study design, including differences in patient selection criteria, sample size, degree of control for confounders, follow‑up duration, and outcome definitions. The present study addressed baseline differences between groups through PSM and validated the robustness of the results using multiple propensity score‑based weighting methods, thereby partially remedying the limitations of previous studies.
The biological mechanisms linking emphysema to increased readmission risk are multifactorial. Emphysema is characterized by irreversible parenchymal destruction, persistent airway inflammation, and reduced physiological reserve, which collectively lower the threshold for exacerbations triggered by respiratory infections or air pollution.25,26 Recent proteomic evidence further suggests that patients with emphysema-predominant COPD exhibit distinct molecular profiles involving immune regulatory mediators and extracellular matrix remodeling pathways, which may sustain a higher baseline inflammatory state even after resolution of acute exacerbations.27,28 In addition, respiratory muscle dysfunction and malnutrition, which are common in patients with emphysema, may delay post-discharge recovery and contribute to the risk of recurrent events.29,30
A notable finding of this study was the significant effect modification by ICS use on the association between emphysema and readmission risk (interaction P = 0.03). In the subgroup of patients not using ICS, emphysema was associated with a markedly higher readmission risk (HR = 3.31, 95% CI: 1.59–6.86, P = 0.001), whereas no significant association was observed among ICS users (HR = 1.26, 95% CI: 0.73–2.17, P = 0.400). This pattern suggests that ICS therapy may mitigate the excess readmission risk conferred by the emphysema phenotype. Several mechanisms may explain this effect modification. First, ICS have well‑established anti‑inflammatory effects, reducing airway and parenchymal inflammation that is persistently elevated in emphysema patients.27,31 Second, ICS reduce the frequency of moderate‑to‑severe exacerbations, which may directly lower readmission risk.32 Third, the differential response to ICS between emphysema and non‑emphysema patients may reflect underlying molecular heterogeneity, as suggested by recent proteomic studies identifying distinct inflammatory pathways in emphysema‑predominant COPD.32
This study provides an imaging phenotype‑based quantitative basis for risk stratification in patients with AECOPD. Emphysema, as a clearly identifiable phenotypic feature on chest CT, may assist in the early clinical identification of patients at high risk for readmission. Based on the findings of this study, the following strategies may be considered in clinical practice: performing chest CT imaging assessment in patients with AECOPD to evaluate the presence and severity of emphysema; strengthening post‑discharge follow‑up management for patients with emphysema, particularly those not using ICS or those with comorbid chronic bronchitis or coronary heart disease; and considering the emphysema phenotype as a reference factor in ICS clinical decision‑making when formulating inhaled treatment regimens. The clinical value of these strategies needs to be further validated by prospective interventional studies.
The main strengths of this study include: first, the use of real‑world clinical data with a relatively large sample size, providing adequate representativeness; second, the application of PSM, multiple propensity score‑based weighting methods, and doubly robust analysis to control for confounding, thereby enhancing the reliability of the results; third, systematic subgroup analyses to identify potential effect modifiers; and fourth, the use of E‑value analysis to assess the potential impact of unmeasured confounding, which improved the robustness of the conclusions.
This study also has several limitations. First, and most importantly, COPD severity indicators, including GOLD stage, spirometric indices (FEV1% predicted), symptom scores, and prior exacerbation history, were not systematically available in our dataset. Because emphysema phenotype is closely correlated with underlying COPD severity, the observed association between emphysema and readmission risk may be partly attributable to residual confounding by unmeasured disease severity. The E-value analysis provides some quantitative context for the robustness of the findings, but future studies incorporating comprehensive severity measures are essential to validate these results. Second, the assessment of emphysema was based on visual evaluation of imaging reports rather than quantitative CT analysis, which may introduce some degree of classification bias. Furthermore, specific emphysema subtypes were not systematically reported and could not be examined. Third, follow‑up data were derived from electronic medical records, which may be subject to loss to follow‑up or incomplete documentation, potentially leading to information bias in outcome ascertainment. Fourth, the assessment of ICS use was based on medication records during hospitalization without data on acute systemic corticosteroid or antibiotic use, other inhaled therapies (such as Long-Acting Muscarinic Antagonists, Long-Acting Beta2-Agonists, or triple therapy), discharge prescriptions, or post-discharge adherence and persistence, which may have introduced bias in the estimation of effect modification. Fifth, although readmissions were tracked through both the index hospital’s records and the Chongqing municipal medical record system (covering public hospitals), admissions to private or out-of-city hospitals may have been missed, potentially underestimating the true readmission rate.
Conclusion
In this real‑world study, the emphysema phenotype was associated with a higher risk of acute exacerbation‑related readmission within 1-year after discharge in patients with AECOPD, and this association remained consistent across multivariable adjustment, PSM, and multiple propensity score‑based weighting methods. However, given the single‑center design, potential for residual confounding by unmeasured COPD severity, and incomplete clinical and pharmacological data, these findings should be interpreted cautiously. Future prospective, multicenter studies incorporating comprehensive clinical variables are needed to validate these results and explore their clinical translation pathways.
Data Sharing Statement
Data are available from the corresponding author Ying Hu upon reasonable request and with consent.
Ethics Approval
This is an observational study. The Ethics Committee of the Second People’s Hospital of Banan District approved the exemption of ethical review for this study (approval No. 2025‑KL‑022).
Acknowledgments
The authors sincerely thank the clinical scientist team for their statistical analysis support.
Funding
This work was supported by the Scientific Research Project of Banan District, Chongqing, China and by grant number 2026ZDXM008.
Disclosure
The authors declare no competing interests in this work.
References
1. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–13. doi:10.1016/S0140-6736(22)00470-6
2. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
3. Meng W, Ma Y, Wu J, et al. Prevalence of treatable traits among patients with very severe COPD across STAR and GOLD classification: a multicenter cohort study. Pulmonology. 2026;32(1):2613525. doi:10.1080/25310429.2026.2613525
4. Rothnie KJ, Müllerová H, Smeeth L, Quint JK. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice–based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
5. Alqahtani JS, Njoku CM, Bereznicki B, et al. Risk factors for all-cause hospital readmission following exacerbation of COPD: a systematic review and meta-analysis. Eur Respir Rev Off J Eur Respir Soc. 2020;29(156):190166. doi:10.1183/16000617.0166-2019
6. Ruan H, Zhang H, Wang J, Zhao H, Han W, Li J. Readmission rate for acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Respir Med. 2023;206:107090. doi:10.1016/j.rmed.2022.107090
7. MacLeod M, Papi A, Contoli M, et al. Chronic obstructive pulmonary disease exacerbation fundamentals: diagnosis, treatment, prevention and disease impact. Respirol. 2021;26(6):532–551. doi:10.1111/resp.14041
8. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: gold executive summary. Am J Respir Crit Care Med. 2023;207(7):819–837. doi:10.1164/rccm.202301-0106PP
9. Koo HK, Bhatt SP. Imaging in chronic obstructive pulmonary disease: ready for prime time? Tuberc Respir Dis. 2026;89(2):143–153. doi:10.4046/trd.2025.0202
10. Castaldi PJ, Xu Z, Young KA, et al. Heterogeneity and progression of chronic obstructive pulmonary disease: emphysema-predominant and non–emphysema-predominant disease. Am J Epidemiol. 2023;192(10):1647–1658. doi:10.1093/aje/kwad114
11. Wang G, Ma A, Zhang L, et al. Acute exacerbations of chronic obstructive pulmonary disease in a cohort of Chinese never smokers goes along with decreased risks of recurrent acute exacerbation, emphysema and comorbidity of lung cancer as well as decreased levels of circulating eosinophils and basophils. Front Med. 2022;9:907893. doi:10.3389/fmed.2022.907893
12. Nguyen Hai C, Bui Duc T, Nguyen Minh T, Trinh Duc L, Tran Quyet T. Quantitative chest computed tomography in chronic obstructive pulmonary disease: assessing the role of emphysema severity and its correlation with clinical characteristics, lung function, and plasma levels of VEGF and IL-1β. Ther Adv Respir Dis. 2025;19:17534666251332469. doi:10.1177/17534666251332469
13. Yang H, Yang Y, Wang F, et al. Clinical and prognostic differences in mild to moderate COPD with and without emphysema. CHEST. 2025;167(3):724–735. doi:10.1016/j.chest.2024.10.020
14. Hartl S, Lopez-Campos JL, Pozo-Rodriguez F, et al. Risk of death and readmission of hospital-admitted COPD exacerbations: european COPD audit. Eur Respir J. 2016;47(1):113–121. doi:10.1183/13993003.01391-2014
15. Njoku CM, Alqahtani JS, Wimmer BC, et al. Risk factors and associated outcomes of hospital readmission in COPD: a systematic review. Respir Med. 2020;173:105988. doi:10.1016/j.rmed.2020.105988
16. Lin P, Shen CC, Li QP, et al. A systematic review and meta-analysis of chronic obstructive pulmonary disease in Asia: risk factors for readmission and readmission rate. BMC Pulm Med. 2024;24(1):388. doi:10.1186/s12890-024-03203-6
17. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
18. Fu CF, Shi JW, Haroon M, Luo J, Hu Y, Jiang DP. L-shaped association between dietary copper intake and chronic obstructive pulmonary disease among American adults: findings from the national health and nutrition examination survey 1999–2018. J Acad Nutr Diet. 2025;125(9):1275–1286.e3. doi:10.1016/j.jand.2025.03.012
19. Shirakawa C, Shiroshita A, Miyakoshi C, et al. Impact of rehabilitation on readmission rates in older patients with COPD with disability after hospital discharge. COPD. 2026;23(1):2593282. doi:10.1080/15412555.2025.2593282
20. Austin PC, Fine JP. Inverse probability of treatment weighting using the propensity score with competing risks in survival analysis. Stat Med. 2025;44(5):e70009. doi:10.1002/sim.70009
21. Xiong L, Zeng Z, Wang S, et al. The association of handgrip strength with all-cause and cardiovascular mortality: results from the national health and nutrition examination survey database prospective cohort study with propensity score matching. Front Nutr. 2023;10:1183973. doi:10.3389/fnut.2023.1183973
22. McCaffrey DF, Griffin BA, Almirall D, Slaughter ME, Ramchand R, Burgette LF. A tutorial on propensity score estimation for multiple treatments using generalized boosted models. Stat Med. 2013;32(19):3388–3414. doi:10.1002/sim.5753
23. Cerezo Lajas A, Gutiérrez González E, Llorente Parrado C, Puente Maestu L, Miguel-Díez J D. Readmission due to exacerbation of COPD: associated factors. Lung. 2018;196(2):185–193. doi:10.1007/s00408-018-0093-y
24. Velando AG, Pastor EC, López RC, et al. Characterization of readmissions in patients hospitalized with COPD exacerbation. Eur Respir J. 2016;48(suppl 60). doi:10.1183/13993003.congress-2016.PA4073
25. Subedi S, Guntipally M, Suwal N, et al. Cellular senescence in chronic obstructive pulmonary disease: molecular mechanisms and therapeutic interventions. Ageing Res Rev. 2025;110:102813. doi:10.1016/j.arr.2025.102813
26. Booth S, Hsieh A, Mostaco-Guidolin L, et al. A single-cell atlas of small airway disease in chronic obstructive pulmonary disease: a cross-sectional study. Am J Respir Crit Care Med. 2023;208(4):472–486. doi:10.1164/rccm.202303-0534OC
27. Zhang YH, Castaldi PJ, Bowler RP, et al. Proteomic biomarkers of emphysema-predominant and non-emphysema-predominant chronic obstructive pulmonary disease. eBioMedicine. 2025;117:105800. doi:10.1016/j.ebiom.2025.105800
28. Kim JH, Schaible N, Hall JK, et al. Multiscale stiffness of human emphysematous precision cut lung slices. Sci Adv. 2023;9(20):eadf2535. doi:10.1126/sciadv.adf2535
29. Nan Y, Zhou Y, Dai Z, et al. Role of nutrition in patients with coexisting chronic obstructive pulmonary disease and sarcopenia. Front Nutr. 2023;10:1214684. doi:10.3389/fnut.2023.1214684
30. Lu R, Gregory A, Suryadevara R, et al. Lung transcriptomics link emphysema to barrier dysfunction and macrophage subpopulations. Am J Respir Crit Care Med. 2025;211(1):75–90. doi:10.1164/rccm.202305-0793OC
31. Lea S, Higham A, Beech A, Singh D. How inhaled corticosteroids target inflammation in COPD. Eur Respir Rev. 2023;32(170):230084. doi:10.1183/16000617.0084-2023
32. Georgiou A, Ramesh R, Schofield P, White P, Harries T. Withdrawal of inhaled corticosteroids from patients with COPD; effect on exacerbation frequency and lung function: a systematic review. COPD. 2024;19:1403–1419. doi:10.2147/COPD.S436525
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence of Cardiovascular Disease and Rate of Major Adverse Cardiovascular Events in Severe Alpha-1 Antitrypsin Deficiency COPD
Ellis P, Bailey E, Choate R, Holm KE, Sandhaus RA, Turner AM, Newnham M
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:149-159
Published Date: 17 January 2024
Impact of an Integrated Medical-Nursing Clinical Pathway on 30-Day Readmission and Long-Term Prognosis in Patients with Acute Exacerbation of COPD: A Retrospective Cohort Study Using Real-World Data
Dou Y, Wang L, Wang Y, Wang J, Qin H, Wang L, Li K, Li N
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:589413
Published Date: 28 April 2026