Back to Journals » Advances in Medical Education and Practice » Volume 15
Emergency Physicians’ Knowledge, Attitudes, and Practices Related to Psychiatric Emergencies in Makkah’s General Hospitals in Saudi Arabia: A Cross-Sectional Study
Authors Ali RM ![]() , Aljabri AA
, Aljabri AA ![]() , Hariri NH
, Hariri NH ![]() , Bokhari GS
, Bokhari GS ![]() , Alturkistani SA
, Alturkistani SA ![]() , Albishri NA
, Albishri NA ![]() , Alzahrani HA
, Alzahrani HA ![]() , Alghamdi SA
, Alghamdi SA ![]() , Alhazmi RT
, Alhazmi RT ![]() , Alfalogy EH
, Alfalogy EH ![]()
Received 12 February 2024
Accepted for publication 14 May 2024
Published 22 May 2024 Volume 2024:15 Pages 433—446
DOI https://doi.org/10.2147/AMEP.S463479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Raghad M Ali,1 Abdulkarim A Aljabri,1 Nahla H Hariri,2 Ghadi S Bokhari,1 Shahad A Alturkistani,1 Nidaa A Albishri,1 Hamza A Alzahrani,1 Shuruq A Alghamdi,3 Renad T Alhazmi,1 Enas H Alfalogy2,4
1College of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 2Community Medicine and Pilgrims Healthcare Department, College of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 3Directorate of Health Affairs, Eradah Complex for Mental Health, Jeddah, Saudi Arabia; 4Family Medicine Department, Faculty of Medicine, Suez -Canal University, Ismalia, Egypt
Correspondence: Nahla H Hariri, Community Medicine and Pilgrims Healthcare Department, College of Medicine, Umm Al-Qura University, Makkah, 21955, Saudi Arabia, Email [email protected]
Purpose: This study aims to assess the knowledge, attitudes, and practices of emergency physicians (EPs) related to psychiatric emergencies (PEs) in Makkah’s general hospitals.
Sample and Methods: This study was an observational cross-sectional study using an online survey distributed to 138 EPs in the emergency departments (EDs) of six public hospitals in Makkah City, Saudi Arabia, between March 15 and May 1, 2023. A convenience sample was used for data collection. The questionnaire was developed after related surveys in the literature were reviewed.
Results: 59.9% of the physicians were aged 20– 30 years. Most (68.8%) worked in hospitals that had psychiatric facilities. Regarding knowledge, only 30% of the emergency doctors were considered knowledgeable: the majority could identify PEs (79.7%), perform mental status examinations (71.0%), distinguish physical and mental symptoms (66.7%), and communicate with psychiatric patients (58.0%). However, only 52.9% could initiate management plans by prescribing psychiatric medication to patients. In relation to attitude, most physicians disagreed with the idea that healthcare practitioners do not need to advocate for psychiatric patients (67.4%), but many (62.3%) assumed that they do not have the responsibility to manage psychiatric patients, and they felt that conducting psychiatric evaluations in public hospitals is challenging because of the busy environment there. As regards practice, mentally ill patients (60.9%) were managed or referred by practices, and 56.5% of the EPs advised these patients upon discharge.
Conclusion: The study showed that EPs have positive attitudes toward psychiatric patients, but their knowledge varied based on age, occupation levels, and years of experience. There were significant knowledge gaps, particularly regarding effective communication with psychiatric patients. Additionally, many EPs manage psychiatric patients without being aware of the psychiatric resources in their hospital. Improving medical school curricula and postgraduate training can enhance care. However, more research in this field is needed.
Keywords: emergency departments, psychiatric patients, public hospitals, mental status examination
Introduction
Psychiatric emergencies (PEs) refer to the sudden onset of behaviour, thought, or mood disturbances. If left untreated, they can be harmful to the patient or to others.1–3 PEs are categorized in two ways: major, when the patient’s life is in danger or there is no threat to the patient’s life but the patient is severely incapacitated; and minor, when neither of these scenarios applies.4 Major PEs consist of various disorders that are divided into two principal classes, namely, acute excitement with psychomotor agitation and self-destructive or suicidal behavior.1,4 The major PEs that have been reported in the emergency department (ED) include suicide, aggression, delirium, drug overdose and withdrawal, acute psychosis, serotonin syndrome, and neuroleptic malignant syndrome. Reactions to disasters, rape, grieving reactions, and panic attacks are minor PEs.4
There is little information about the occurrence of psychiatric emergencies in non-psychiatric settings, such as general hospitals, and how they are diagnosed and treated.5 The prevalence of PEs has been estimated in several studies to range from 10% to 60%,6 with the variation in prevalence due to multiple methodological deficiencies in these studies. The fundamental basis on which a PE can be identified is still the history and physical examination: the data collected must include, at a minimum, complete vital signs; a history that includes any records of mental illness, drugs, substances, and mood disorders; a mental status exam; and additional testing as suggested by the presentation. Symptoms include the auditory hallucinations and paranoia that come with psychosis and the insomnia, impulsiveness, and grandiosity that accompany mania. Symptoms such as dysphoria, family and personal stress, or marital troubles are rarely severe, although they are typically seen in the emergency setting.
The acute manifestations of PEs require immediate treatment to improve a patient’s subjective symptoms and prevent behaviors that could harm the patient or others. Evidence shows that approximately 60% of PEs cases require medical attention but do not present in psychiatric facilities.1,7 Data collected by The National Hospital Ambulatory Medical Care Survey revealed that in the period 2017–2019, the ED visit rate of adults with mental health issues was 52.9 per 1000 adults.8 According to an Australian Government report, the number of people seeking help for mental health issues climbed from 136,026 in 2004/5 to 303,340 in 2018/9. Additionally, the proportion of ED visits linked to mental health rose from 2.9% to 3.6% of all visits during the same period.9 However, it is probable that these numbers underestimate the number of mental health-related visits to the ED.
Psychiatric patients therefore visit EDs in the event of crises.2 In addition, individuals seeking professional help for psychiatric or mental health problems require insight and motivation from EPs. The treatment of such situations makes considerable demands on the physician’s personality and conduct and also requires them to have necessary medical skills,5 which is even more challenging, given the low level of general knowledge and awareness in society regarding psychiatric and mental health issues. Furthermore, ED triage procedures and resources may not be optimal for managing mental illnesses, as PEs differ significantly from other emergencies in terms of the predominantly syndromal classification of symptoms, the lack of algorithms, and, ultimately, the individual experiences of EPs.4
PEs are as critical and vital as medical emergencies, although psychiatric patients are given less attention than individuals with physical health issues.10,11 Recent evidence indicates that the evaluation of patients’ mental well-being is infrequently conducted in EDs, primarily because insufficient hospital resources are allocated for psychiatric patients or due to the physician’s subjective bias based on personal experiences.12 It is the responsibility of the staff, who have varying degrees of training and expertise in handling mental illnesses, to take care of these individuals.12 EPs need psychiatric knowledge and an understanding of biopsychosocial issues in addition to general medical and emergency medicine skills.5 An assessment of the awareness, knowledge, and attitude of EPs in EDs will yield valuable insights into the areas that require improvement to ensure optimal medical care for patients in the ED.
Several studies have been conducted worldwide among EPs to assess their knowledge of and confidence in managing PEs. A recent study in Germany identified the issues that affect how emergency medical and psychiatric care institutions engage with mentally ill patients. The study found that 36.7% of EPs do not believe that they are adequately qualified to treat PEs and, remarkably, that many of them would seek telephone contact with acute psychiatric hospitals.13 A survey conducted in the US Midwest to assess EPs’ attitudes and practices found that 39.5% of them also feel inadequately trained to manage PEs, while 92.3% said that additional mental health resources would be beneficial for their facility.14 In India, 83.8% of the physicians examined in one study said that there are no mental health policies in their departments.12 Two similar studies, one in the United States and another in Australia, have concluded that EPs working in EDs need more knowledge and confidence and require more training.15,16
In Saudi Arabia, few studies have investigated PEs. In 2000, a study showed that 57.7% of index individuals were handled at the ED and provided with a mental outpatient appointment. Approximately 22% of the index individuals were admitted to the psychiatric unit, with mood disorders being the most prevalent condition.17 In 2020, a study reported that half of the EPs studied employed techniques for diagnosing persons with mental health disorders and that 54% were affected by their personal experiences. The same study found that 65% of EPs have seen that families may not readily accept recommendations for a psychiatric referral.18
Currently, there is limited information regarding how EPs in Saudi Arabia administer emergency care for psychiatric emergencies. Given this background, our study aims to evaluate the knowledge, attitudes, and practices of EPs toward PEs in Makkah, Saudi Arabia.
Materials and Methods
Study Design, Study Population, and Sampling
This observational cross-sectional study was carried out from March 15 to May 1, 2023. The study was conducted in Makkah, Saudi Arabia. Specifically, it was carried out in the following hospitals’ EDs: King Abdullah Medical City, King Faisal Hospital, King Abdulaziz Hospital, Al-Noor Specialist Hospital, Security Forces Hospital, and Herra General Hospital. All ED physicians available in these hospitals at the time of data collection were invited to participate in the study. The study aimed to include all EPs working in the EDs, such as residents, specialists, and consultants, at the aforementioned six general hospitals in Makkah, Saudi Arabia. Interns and rotating doctors from other specialties were excluded from the study.
Potential research subjects were approached for their verbal consent to participate in the study, after which consenting participants were administered the questionnaires in electronic form for data to be collected. The research team provided iPads to the physicians to ensure standardized and convenient questionnaire completion. On average, it took 10 minutes to complete the questionnaires. The data collectors were trained for one day on how to conduct the questionnaire administration process. They were assigned and distributed to six hospitals, ensuring that convenience sampling was used to recruit from each EP team to cover different shifts.
Sample Size Calculation
With a population of 202 EPs in Makkah hospitals,19 a confidence level of 95%, a margin of error of 5%, and a response distribution of 50%, the minimum recommended sample size for this study was 133 according to the software Sample Size Calculator (Raosoft, Inc., Seattle, WA, USA). Accordingly, a sample size of 133 participants was needed for this study.
Study Assessment Tools
The research objective was to gather information about the physicians’ knowledge, attitudes, and practices regarding PEs. Therefore, we designed a questionnaire after conducting a thorough literature review and gathering relevant questions from previous studies.12–14,16,20 The questionnaire was reviewed by two emergency consultants and two psychiatric consultants for content and face validity, practicability, and interpretation of answers. Then, to ensure the quality of the questions, an emergency consultant and a psychiatric consultant reviewed the questionnaire to assess the practicability, validity, and interpretation of answers. A pilot study with 20 volunteers was then conducted to test the survey’s clarity and wording. The question wording and layout were modified based on feedback from the respondents.
The questionnaire was structured into three sections. The first section was a voluntary consent form. The second section focused on sociodemographic data, which included 11 questions on age, gender, marital status, nationality, workplace (King Abdullah Medical City, King Faisal Hospital, King Abdulaziz Hospital, Al-Noor Specialist Hospital, Security Forces Hospital, or Herra General Hospital), occupation level (junior service, senior service, junior resident, senior resident, registrar, or consultant), years of experience (less than five years, 5–10 years, 11–15 years, 16–20 years, or more than 20 years), presence of certified training in psychiatry (outside medical school), where the term “certified training” in psychiatry refers to any elective psychiatry training that the practitioner has taken outside the mandatory curriculum of psychiatry in medical school, indicating the time when the training was taken (during summer training, during postgraduate studies, during an elective ER rotation, during a hospital-provided course, during a professional course outside the workplace, or other), average number of psychiatric patients seen in one shift (0, 1–2, 3–4, or more than four patients), and whether the hospital had a psychiatric department.
The third section, assessing the EPs’ knowledge, attitudes, and practices, consisted of three parts. The first part had five questions to assess the physicians’ knowledge, with “yes”, “no”, or “uncertain” as the response options. The second part had nine questions to assess the EPs’ attitudes toward training and PE patients; the answer choices were “agree”, “disagree”, or “neutral”, with one having a multiple-choice option. The third part, which had 14 questions to evaluate the physicians’ practices, used the question-and-answer format, with responses such as “yes”, “no”, and “uncertain” and with multiple checkboxes and multiple-choice options provided.
Ethical Approval
This study was approved by the medical ethical committee at Umm Al-Qura University (HAPO-02-K-012-2023-03-1487) under the Declaration of Helsinki. After the objectives and methodology of the study were explained, consent from the participants was obtained by answering the first question: “Do you agree to participate in this study?”. The participants were told that their identifying information would not be collected and that all responses would be kept confidential.
Statistical Analysis
Statistical analysis was performed using RStudio (R version 4.2.2). Data were described using frequencies and percentages for categorical variables or medians and interquartile ranges (IQRs) for numerical variables. An overall knowledge score was computed by summing five items that reflected self-reported knowledge regarding selected items. We used the Kruskal–Wallis or the Wilcoxon rank sum test to assess differences in knowledge scores across different demographic and occupational characteristics. Significantly associated variables were incorporated into a multivariable generalised linear regression model to explore the independent predictors of knowledge. The results were presented as beta coefficients and 95% confidence intervals. A p-value of < 0.05 indicated statistical significance.
Results
Demographic and Occupational Characteristics
A total of 138 EPs responded to the questionnaires. Of the participants, 59.9% were between the ages of 20 and 30, 71.0% were male, and 43.5% were single. The majority of the physicians (68.8%) worked in hospitals with psychiatric departments, and 30.4% worked at Al Noor Hospital. Almost one-third of the participants were in junior service, 62.3% had less than five years of ED experience, and 88.4% had not received certified training in psychiatry. Furthermore, 58.4% reported having undergone their most recent training in psychiatry as medical students and 64.5% (Table 1) saw an average of one to two patients whose chief complaints were psychiatric during their shifts.
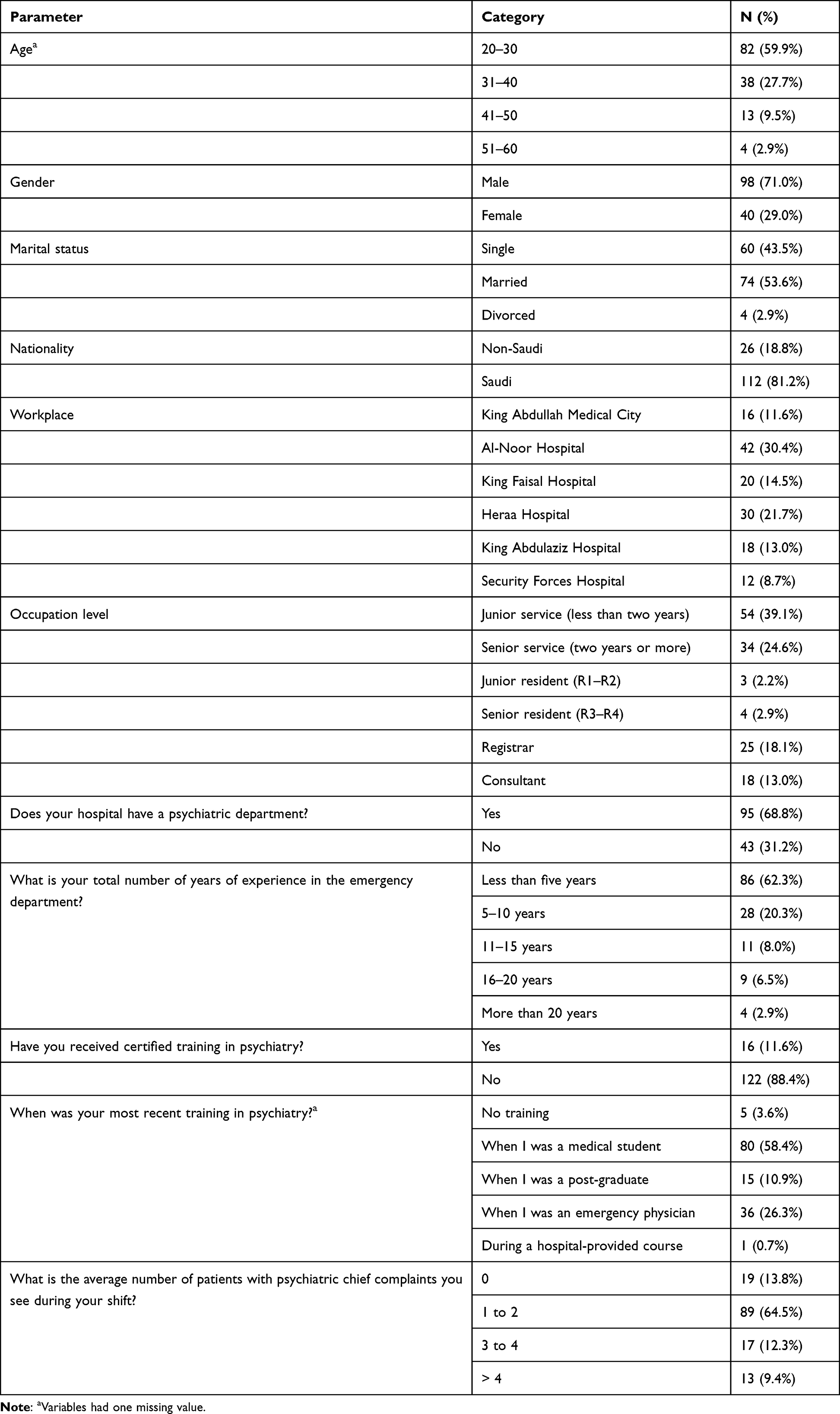 |
Table 1 Participants’ Demographic and Occupational Characteristics |
Knowledge of Psychiatric Emergencies
The evaluation of the EPs’ levels of knowledge showed that 30% (n = 42) correctly answered the five questions. The majority of the physicians reported being able to identify PEs (79.7%), perform mental status examinations of psychiatric patients (71.0%), and differentiate between physical and mental illnesses (66.7%) and that they knew communication techniques for dealing with psychiatric patients (58.0%). However, only 52.9% (Table 2) knew how to prescribe initial treatments for psychiatric patients. The median composite knowledge score was 4.0 (IQR = 2–5). Table 3 shows that self-reported knowledge differed based on age (p = 0.023), occupation level (p < 0.001), years of experience in the ED (p = 0.001), certified training in psychiatry (p = 0.027), and time of most recent psychiatric training (p < 0.001). However, when analyzed with multivariable regression, none of these factors was found to be an independent predictor (Table 4).
 |
Table 2 Knowledge of Psychiatric Emergencies |
 |
Table 3 Differences in the Physicians’ Self-Reported Knowledge Scores in the Study |
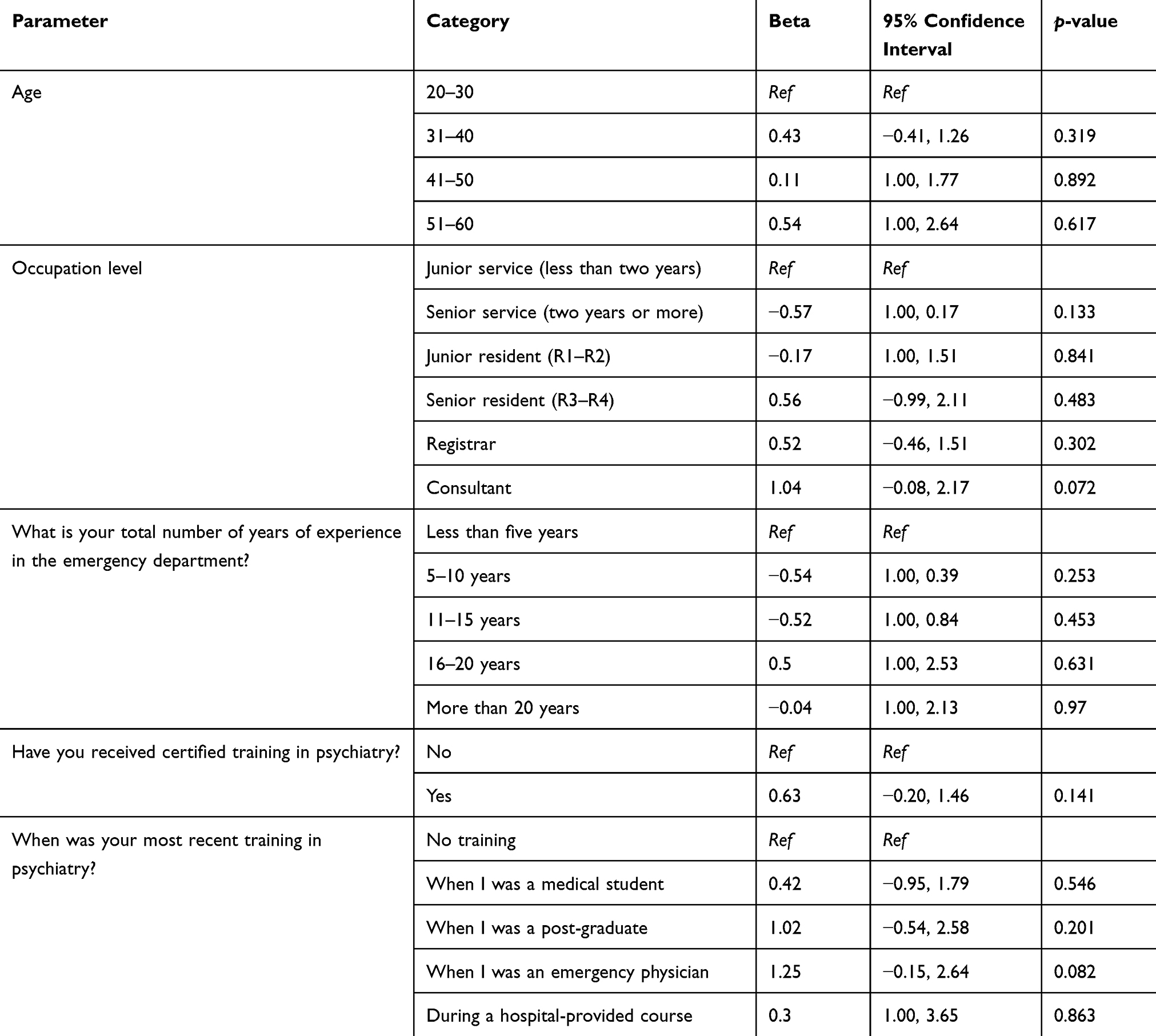 |
Table 4 Results of the Multivariable Regression Analysis for the Independent Predictors of Self-Reported Knowledge |
Physicians’ Attitudes Toward Psychiatric Emergencies
In terms of attitudes, most physicians disagreed with the idea that healthcare providers do not need to be advocates for people with mental illnesses (67.4%) and that EPs have no role in managing psychiatric patients (62.3%). However, most agreed that evaluating psychiatric patients in a busy environment is difficult (62.3%; Figure 1) and that the presence of psychiatric facilities could assist in managing psychiatric patients (68.1%).
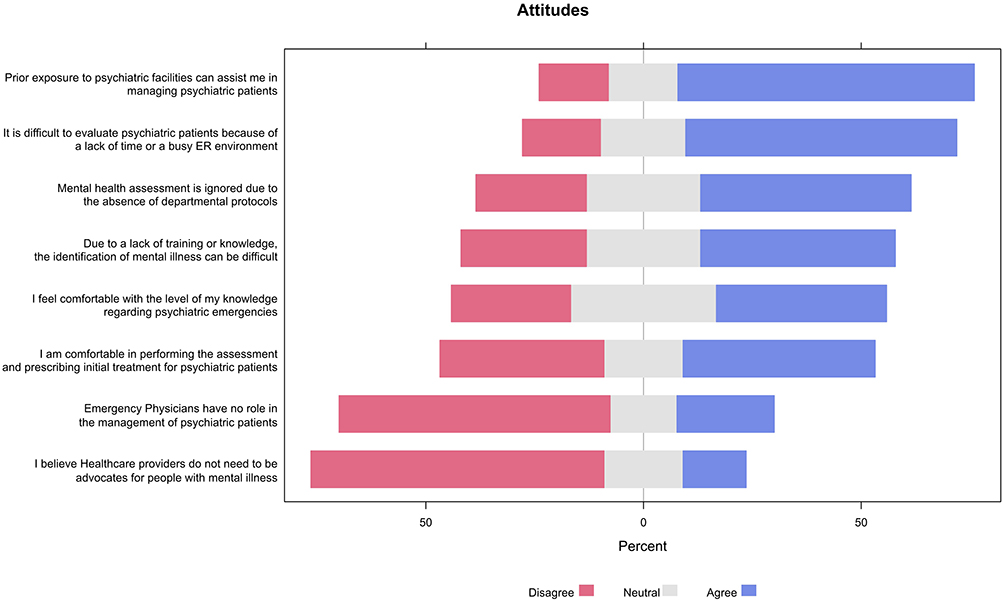 |
Figure 1 Physicians’ responses to the attitude items. |
Physicians’ Practices Regarding Psychiatric Emergencies
Regarding practices, 60.9% of the EPs were aware of the presence of management/referral policy in their department for mentally ill patients, whereas approximately half (56.5%) gave discharge advice to these patients. EPs provided discharge advice to patients during PEs to ensure their safety, facilitate access to appropriate care, and promote recovery and well-being. This advice differs from standard medical advice and may be influenced by the physician’s considerations. The advice may include counseling the patient and their family, educating them about the condition, providing advice on how to prevent future relapses (such as avoiding triggers and giving instructions regarding their psychiatric medication use), and advising the patient to seek a psychologist or psychiatrist for further help, either through outpatient clinics or specialized facilities. About 54.3% (Table 5) performed their own independent psychiatric evaluations of the patients, even if someone else had performed the initial evaluation. Moreover, the majority of the physicians (60.1%) reevaluated patients every two hours when suicidal patients came under their care, and 75.4% (Table 5) did the same for cardiac patients under their care. Notably, 66.7% of the physicians ordered routine laboratory investigations of psychiatric patients; the most common laboratory tests routinely ordered for psychiatric patients were complete blood count (93.5%), liver function tests (82.6%), and fingerstick glucose testing (72.8%; Figure 2).
 |
Table 5 Psychiatric Emergency Practices |
 |
Figure 2 Proportions of the laboratory tests performed by the physicians for their psychiatric patients. |
Discussion
In this study, we assessed the knowledge, attitudes, and practices of EPs in managing PEs in Makkah’s general hospitals. A total of 138 physicians from six hospitals responded to the survey, 30.4% of whom were from Al Noor Hospital. Most physicians were Saudi men, and over half were relatively young, aged 20–30 years old.
The results in this study revealed that the physicians’ knowledge varied significantly based on their ages, occupation levels, years of experience in the ED, certified training in psychiatry, and time of recent psychiatric training. Most respondents said that they knew how to identify PEs and could differentiate physical from mental illnesses. Furthermore, 71% of EPs know about mental status examinations or assessments. This finding is in line with a previous study that showed that half of the EPs considered employed methods to diagnose individuals with mental health disorders.18 A significant number of the respondents knew about communication techniques for dealing with psychiatric patients or how to prescribe initial treatments. This finding is similar to that of Bhargav et al, whose study found that a significant majority of EPs (over 85%) are aware of the serious consequences that mental health issues impose on healthcare systems.12 Furthermore, more than 79% of the EPs in the current study had encountered patients with mental illnesses within the ED setting, and 52% of physicians had prescribed initial psychiatric emergency medications. In contrast, a previous study reported a significant majority (over 85%) rarely engaged in the assessment of their patients’ mental health conditions. The majority (over two thirds) lacked knowledge of the diagnostic criteria for depression, and a mere 14% had received any form of training in effectively treating mental health issues in patients.12 In another study, junior ED doctors were investigated before they started their ED placements and before they were provided with psychiatry training. Over half of the 32 doctors surveyed reported lacking the necessary skills, knowledge, and confidence to assess and manage mental health patients.20 Similarly, more than one third of our respondents were at the junior occupation level and had received recent psychiatric training while in medical school but still showed deficiencies in their knowledge and skills. Furthermore, the cited study included more junior physicians, that is, those aged 20–30, as most participants were at the service level (general practitioners).
The reasons for this lack of knowledge are complex and require further exploration. One reason may be that most of the physicians were at the junior service level (< 0.001) and had less than five years of experience in EDs, with their most recent training in psychiatry being in medical school (< 0.001). Moreover, only a small percentage (11.6%) reported receiving certified training in psychiatry. Most physicians agreed that a lack of training makes the identification of mental illnesses difficult, which can be particularly challenging in a busy ED environment given the limited time available. This suggests the critical importance of and need for more training, continuous development, and learning among recent EPs graduates. As most respondents agreed that prior exposure to psychiatric facilities could improve their ability to manage psychiatric patients, improvement could be made by increasing exposure during medical school rotations and providing courses and workshops in psychiatry. Bedside teaching and regular case discussions can also be helpful because most EPs said that they see one to two psychiatric patients per shift on average. This finding is concurrent with the survey results of Gordon, which showed the need to implement mental health training programs for newly employed physicians working in EDs.20 The provision of training for these professionals can be effectively facilitated using liaison psychiatric services. This practice must be integrated into the instructional curriculum and be consistently adapted to the identified training requirement.12
Another study revealed that 31.4% of the physicians considered had insufficient understanding of mental diseases, while just 25.6% possessed pertinent knowledge. The study reported that 37.8% of the respondents had a positive attitude, whereas 44.7% exhibited a negative attitude towards those with mental illness. The study found a direct correlation between positive attitudes toward individuals with mental diseases and having sufficient awareness of mental illnesses, as has been previously shown.21 Healthcare workers’ unfavourable views exacerbate patients’ mental health issues and can significantly impede their recovery.22
Most EPs disagreed with the idea that healthcare providers do not have to advocate for individuals with mental illnesses and with the belief that EPs have no role in managing psychiatric patients. This finding suggests that EPs have positive attitudes toward both psychiatric patients and their responsibilities as healthcare providers. A study found that emotional, diagnostic, and logistical obstacles are exacerbated by preexisting flaws within healthcare and societal systems and contribute to and perpetuate unfavourable attitudes, expectations, and prejudices. The confluence of these processes engenders detrimental healthcare experiences for patients, physicians, and nurses, thereby potentially compromising the quality of patient treatment and the well-being of ED staff.12
In terms of practice, more than one third of the physicians reported being uncertain about or unaware of whether their hospitals had management or referral policies for mentally ill patients, even though all the general hospitals included in the study have psychiatric departments. Compared to a 2016 study in which over 80% of the physicians also reported not having such policies,12 the present study suggests that some EPs are managing psychiatric patients alone, without a psychiatrist’s help, and may be unaware of their hospitals’ psychiatric departments. Over one third also reported not having psychiatric departments. Additionally, more than half of the respondents would reevaluate suicidal patients, as they did cardiac patients, admitted to the ED after a certain period. This percentage is higher than that found by a 2021 study14 and indicates that EPs provide the same amount of care and attention to psychiatric patients as they do to other patients.
In PEs, EPs must evaluate patients experiencing acute psychological distress quickly and effectively by using proper assessment and diagnostic skills to provide urgent care and appropriate initial management. Doing so will help ensure patients’ health and safety.
Limitations of the Study
The results of this study provide limited insight into how EPs deal with PEs, as we only included Makkah’s general hospitals and excluded private hospitals or those in other cities, resulting in a small population size (n = 138). Moreover, a majority of those participating in this study were younger physicians (59.9%), aged 20–30, who had little experience of PEs. The results could have been different if the respondents had been experienced senior doctors. Furthermore, the majority of the respondents were at service level (general practitioners) because Makkah’s general hospitals have more service physicians than emergency board residents in their training programmes. Lastly, the study excluded other healthcare providers, such as nurses, psychiatrists, and physicians from other departments who are on emergency medicine rotations and may also be responsible for managing psychiatric patients; nor did it include PEs presented to outpatient departments.
Conclusion
EPs have a crucial role in managing PEs in the ED. Our study highlights the importance of evaluating their knowledge, attitudes, and practices in managing these emergencies, addressing gaps and deficiencies, and improving the level of care provided to psychiatric patients. Participants showed positive attitudes toward psychiatric patients, but their knowledge varied based on their ages, occupation levels, years of experience in the ED, and time of psychiatric training. There were significant knowledge gaps, specifically in terms of effective communication with psychiatric patients. Moreover, some EPs manage psychiatric patients independently without being aware of psychiatric resources in their hospital.
To improve the level of care provided to psychiatric patients, it is essential to enhance the medical school curriculum, offer postgraduate training or courses, and provide more communication training to EPs. Doing so will ensure they are better equipped to manage acute PEs with the same level of expertise and urgency as other emergency conditions. However, further research is still needed to conduct a more thorough assessment using more specific methods. Moreover, future studies should determine whether these findings are consistent across EPs from different regions or if there are differences.
Data Sharing Statement
All the data related to this study are available upon request.
Acknowledgments
The authors would like to express their gratitude and appreciation to all participants in the study.
Funding
The authors have received no funding to conduct this study.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Mothibi JD. Determining the Need for Teaching on Pre-Hospital Management of Psychiatric Emergencies in the Emergency Medical Care Curriculum in South Africa. University of the Free State; 2020.
2. Wheat S, Dschida D, Talen MR. Psychiatric emergencies. Prim Care. 2016;43(2):3410–3454. doi:10.1016/j.pop.2016.01.009
3. Gerson S, Bassuk E. Psychiatric emergencies: an overview. Am J Psychiatry. 1980;137(1):1–11.
4. Sudarsanan S, Chaudhury S, Pawar A, Salujha S, Srivastava K. Psychiatric emergencies. MJAFI. 2004;60(1):59–62.
5. Mavrogiorgou P, Brüne M, Juckel G. The management of psychiatric emergencies. Dtsch Ärztebl Int. 2011;108(13):222. doi:10.3238/arztebl.2011.0222
6. Arolt V, Diefenbacher A. Psychiatrie in der klinischen Medizin: Konsiliarpsychiatrie,-psychosomatik und-psychotherapie. Springer-Verlag; 2013.
7. Rössler W, Riecher-Rössler A. Versorgungsebenen in der Notfallpsychiatrie. Das Notfall Psychiatr Buch Urban Schwarzenb. 2002;1(1):2–10.
8. Santo L, Peters ZJ, DeFrances CJ Emergency department visits for adults with mental health disorders: United States, 2017–2019. 2021.
9. Ash D, Brown P, Burvill P, et al. Mental Health Services in the Australian States and Territories. In Mental Health in Australia: Collaborative Community Practice. Oxford University Press; 2007:101–131.
10. Duncan L, Comeau J, Wang L, Vitoroulis I, Boyle MH, Bennett K. Research review: test–retest reliability of standardized diagnostic interviews to assess child and adolescent psychiatric disorders: a systematic review and meta‐analysis. J Child Psychol Psychiatr. 2019;60(1):16–29. doi:10.1111/jcpp.12876
11. Roennfeldt H, Wyder M, Byrne L, Hill N, Randall R, Hamilton B. Subjective experiences of mental health crisis care in emergency departments: a narrative review of the qualitative literature. Int J Environ Res Public Health. 2021;18(18):9650. doi:10.3390/ijerph18189650
12. Bhargav A, Subhan I, Singh N. A study on knowledge, attitude and practices of emergency physicians in management of patients with mental health disorders in the city of Hyderabad, India. Eurasian J Emerg Med. 2016;15:4.
13. Schick B, Mayer B, Jäger M, et al. Emergency medical care of patients with psychiatric disorders-challenges and opportunities: results of a multicenter survey. BMC Emerg Med. 2022;22(1):1–10. doi:10.1186/s12873-022-00722-5
14. Brodeur J, Ley AF, Bonnet M. A survey of Midwest physicians’ experiences with patients in psychiatric distress in the emergency department. JOM. 2021;121(10):773–778. doi:10.1515/jom-2021-0052
15. Sivakumar S, Weiland TJ, Gerdtz MF, Knott J, Jelinek GA. Mental health‐related learning needs of clinicians working in Australian emergency departments: a national survey of self‐reported confidence and knowledge. Emergency Med Australasia. 2011;23(6):697–711. doi:10.1111/j.1742-6723.2011.01472.x
16. Pickett J, Haas MRC, Fix ML, et al. Training in the management of psychobehavioral conditions: a needs assessment survey of emergency medicine residents. AEM E T. 2019;3(4):365–374.
17. Mahgoub OM. Psychiatric emergencies at a university teaching hospital in eastern Saudi Arabia. J Family Community Med. 2000;7(2):53–59. doi:10.4103/2230-8229.98190
18. Alruzaiza SA, Mahrous RM. Assessment of knowledge, attitude, and practice on level of awareness among pediatric emergency department visitors – Makkah City, Saudi Arabia: cross-sectional study. Int J Psychosoc Rehabil. 2020;24:5186–5202.
19. Ministry of Health. Statistical-Yearbook 2021; 2021. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/Statistical-Yearbook-2021.pdf.
20. Gordon JT. Emergency department junior medical staff’s knowledge, skills and confidence with psychiatric patients: a survey. Psychiatrist. 2012;36(5):186–188. doi:10.1192/pb.bp.111.035188
21. AlSalem M, Alamri R, Hejazi S. Nonpsychiatric healthcare professionals’ attitudes toward patients with mental illnesses in Makkah city, Saudi Arabia: a cross-sectional study. Neuropsychiatr Dis Treat. 2020;341–348. doi:10.2147/NDT.S236148
22. Wang PS, Berglund P, Olfson M, Pincus HA, Wells KB, Kessler RC. Failure and delay in initial treatment contact after first onset of mental disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry. 2005;62(6):603–613. doi:10.1001/archpsyc.62.6.603
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.