")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Elevated BUN Upon Admission as a Predictor of in-Hospital Mortality Among Patients with Acute Exacerbation of COPD: A Secondary Analysis of Multicenter Cohort Study
Authors Zhang J, Qin Y, Zhou C, Luo Y, Wei H, Ge H, Liu HG, Zhang J, Li X, Pan P, Yi M, Cheng L, Liu L, Aili A, Peng L , Liu Y, Pu J, Yi Q , Zhou H
Received 11 March 2023
Accepted for publication 9 July 2023
Published 13 July 2023 Volume 2023:18 Pages 1445—1455
DOI https://doi.org/10.2147/COPD.S412106
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Min Zhang
Jiarui Zhang,1,* Yichun Qin,2,* Chen Zhou,3 Yuanming Luo,4 Hailong Wei,5 Huiqing Ge,6 Hui-Guo Liu,7 Jianchu Zhang,8 Xianhua Li,9 Pinhua Pan,10 Mengqiu Yi,11 Lina Cheng,11 Liang Liu,12 Adila Aili,1 Lige Peng,1 Yu Liu,1 Jiaqi Pu,1 Qun Yi,1,13,* Haixia Zhou1,*
1Department of Respiratory and Critical Care Medicine, West China Hospital, Sichuan University, Chengdu, Sichuan Province, People’s Republic of China; 2State Key Laboratory of Oral Diseases and National Clinical Research Center for Oral Diseases, West China Hospital of Stomatology, Sichuan University, Chengdu, People’s Republic of China; 3West China School of Medicine, West China Hospital, Sichuan University, Chengdu, Sichuan Province, People’s Republic of China; 4State Key Laboratory of Respiratory Disease, Guangzhou Medical University, Guangzhou, Guangdong Province, People’s Republic of China; 5Department of Respiratory and Critical Care Medicine, People’s Hospital of Leshan, Leshan, Sichuan Province, People’s Republic of China; 6Department of Respiratory and Critical Care Medicine, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang Province, People’s Republic of China; 7Department of Respiratory and Critical Care Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei Province, People’s Republic of China; 8Department of Respiratory and Critical Care Medicine, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei Province, People’s Republic of China; 9Department of Respiratory and Critical Care Medicine, The First People’s Hospital of Neijiang City, Neijiang, Sichuan Province, People’s Republic of China; 10Department of Respiratory and Critical Care Medicine, Xiangya Hospital, Central South University, Changsha, Hunan Province, People’s Republic of China; 11Department of Emergency, First People’s Hospital of Jiujiang, Jiujiang, Jiangxi Province, People’s Republic of China; 12Department of Respiratory and Critical Care Medicine, The Affiliated Hospital of Chengdu University, Chengdu, Sichuan Province, People’s Republic of China; 13Sichuan Cancer Hospital, University of Electronic Science and Technology of China, Chengdu, Sichuan Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haixia Zhou; Qun Yi, Department of Respiratory and Critical Care Medicine, West China Hospital, Sichuan University, Guo-Xue-Xiang 37#, Wuhou District, Chengdu, Sichuan Province, 610041, People’s Republic of China, Tel/Fax +86-28-85422571, Email [email protected]; [email protected]
Background: High blood urea nitrogen (BUN) is observed in a subset of patients with acute exacerbation of COPD (AECOPD) and may be linked to clinical outcome, but findings from previous studies have been inconsistent.
Methods: We performed a retrospective analysis of patients prospectively enrolled in the MAGNET AECOPD Registry study (ChiCTR2100044625). Receiver operating characteristic (ROC) was used to determine the level of BUN that discriminated survivors and non-survivors. Univariate and multivariate Cox proportional hazards regression analyses were performed to assess the impact of BUN on adverse outcomes.
Results: Overall, 13,431 consecutive inpatients with AECOPD were included in this study, of whom 173 died, with the mortality of 1.29%. The non-survivors had higher levels of BUN compared with the survivors [9.5 (6.8– 15.3) vs 5.6 (4.3– 7.5) mmol/L, P < 0.001]. ROC curve analysis showed that the optimal cutoff of BUN level was 7.30 mmol/L for in-hospital mortality (AUC: 0.782; 95% CI: 0.748– 0.816; P < 0.001). After multivariate analysis, BUN level ≥ 7.3 mmol/L was an independent risk factor for in-hospital mortality (HR = 2.099; 95% CI: 1.378– 3.197, P = 0.001), also for invasive mechanical ventilation (HR = 1.540; 95% CI: 1.199– 1.977, P = 0.001) and intensive care unit admission (HR = 1.344; 95% CI: 1.117– 1.617, P = 0.002). Other independent prognostic factors for in-hospital mortality including age, renal dysfunction, heart failure, diastolic blood pressure, pulse rate, PaCO2 and D-dimer.
Conclusion: BUN is an independent risk factor for in-hospital mortality in inpatients with AECOPD and may be used to identify serious (or severe) patients and guide the management of AECOPD.
Clinical Trial Registration: MAGNET AECOPD; Chinese Clinical Trail Registry NO.: ChiCTR2100044625; Registered March 2021, URL: http://www.chictr.org.cn/showproj.aspx?proj=121626.
Keywords: AECOPD, inpatients, blood urea nitrogen, mortality, adverse outcomes
Introduction
Chronic obstructive pulmonary disease (COPD) is a common disease that is characterized by persistent airflow limitation and recurrent exacerbations.1,2 It is a leading cause of morbidity and mortality worldwide and induces a substantial health and economic burden.3,4 Acute exacerbation of COPD (AECOPD) is defined as periodic deterioration of respiratory symptoms, resulting in the need for urgent care or hospitalization and a decline in the quality of life.5 Early identification of severe patients with high-risk of mortality is crucial, as it can help physician choose appropriate treatment strategies and reduce in-hospital mortality.6,7
Some clinical studies have identified multiple risk factors for mortality in patients with AECOPD, including dyspnoea, eosinopenia, pulmonary consolidation, acidaemia, atrial fibrillation and renal function.8,9 Blood urea nitrogen (BUN) is a traditional biomarker of renal function and has been reported to be associated with the poor prognosis of ischemic stroke, cardiovascular disease, coronavirus disease 2019 (COVID-19), acute pancreatitis and pneumonia.10–14 BUN has been linked to the poor clinical prognosis of AECOPD, but the findings have been inconsistent. A study from Canada found that elevated BUN level with a cutoff value of 12 mmol/L increased mortality,15 and a recent Chinese observation reported that an elevated BUN/ALB ratio was a strong and independent predictor of in-hospital and 90-day all-cause mortality in patients with AECOPD,16 whereas investigations conducted in Australia showed that BUN level was not an independent predictor of short-term or long-term adverse outcomes.17 Therefore, the relationship between BUN and the prognosis of AECOPD and the cutoff value of BUN in patients with AECOPD with a high risk of mortality remains unclear.
We performed a retrospective analysis of data from a multicenter study to investigate the role of BUN in prediction of in-hospital mortality and other adverse outcomes in AECOPD inpatients.
Methods
Study Design and Participants
Participants were included from MAGNET AECOPD (MAnaGement aNd advErse ouTcomes in inpatients with acute exacerbation of COPD) Registry study (ChiCTR2100044625) in China; the registry included patients as a prospective, noninterventional, multicenter cohort study. The original study enrolled consecutive adult inpatients diagnosed with AECOPD among ten major hospitals (including West China Hospital, Guangzhou Medical University, Xiangya Hospital, Tongji and Union Hospitals of Huazhong University of Science and Technology, People’s Hospital of Leshan, Sir Run Run Shaw Hospital, the First People’s Hospital of Neijiang City, the First People’s Hospital of Jiujiang, and the Affiliated Hospital of Chengdu University) in China between September 2017 and July 2021, while this is a retrospective analysis of patients prospectively enrolled in the MAGNET AECOPD Registry study. This study was approved by the Ethics Committee of the ten academic medical centers that participated in accordance with the Declaration of Helsinki, and written informed consent was obtained from all the participants.
The diagnosis of AECOPD was based on the following criteria in all the ten medical centers that participated: (1) a history of COPD defined according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria;18 and (2) an acute worsening of respiratory symptoms resulting in additional therapy. The exclusion criteria were as follows : (1) patients with missing records of BUN on admission; (2) patients requiring immediate cardiopulmonary resuscitation; and (3) patients with gastrointestinal bleeding. BNU was detected for each patient within 24 h of admission. We compared the differences in BUN between survivors and non-survivors and investigated the potential predictors for mortality in these hospitalized patients with AECOPD.
Data Collection
For this study, clinical data of participants were collected with standardized case report form, including baseline demographics, frequency of hospitalization due to AECOPD in the past year, comorbidities, vital signs, laboratory and radiologic findings, and clinical outcomes, as described previously.19 The data collectors received in-depth training, and all data were checked by two investigators (JZ and CZ) to ensure the reliability of the information. The main clinical endpoint was all-cause in-hospital mortality. The secondary outcomes included invasive mechanical ventilation and intensive care unit (ICU) admission during hospital stay.
Statistical Analysis
Continuous variables are summarized as the mean ± standard deviation or interquartile range [IQR] and were compared with the t-test or Mann–Whitney U-test. Categorical variables are expressed as n (%) and were compared with the chi-squared test. Receiver operating characteristic (ROC) analysis was used to determine the optimal BUN level that predicted in-hospital mortality. Univariate and multivariate Cox regression analyses were used to assess the impact of potential risk factors on survival, and hazard ratios (HR) and 95% confidence interval (95% CI) were calculated to evaluate the degree of influence of these variables. Analyses of the survival time of AECOPD patients with different levels of BUN were performed using Kaplan–Meier and log-rank methods. P < 0.05 was deemed statistically significant. All analyses were conducted using SPSS version 21.0.
Results
Demographic and Clinical Characteristics of Included Patients
A total of 14,007 consecutive patients enrolled in the MAGNET AECOPD Registry study, 13,431 patients with AECOPD included in the analysis. The main reasons for exclusion were as follows: (1) BUN level was not recorded (n = 470); (2) patients requiring immediate cardiopulmonary resuscitation (n = 2); (3) patients with gastrointestinal bleeding (n = 104). Overall, 173 (1.29%) patients were died during hospitalization, 416 (3.1%) patients used invasive mechanical ventilation, and 968 (7.2%) patients were treated in the ICU during their hospital stay. The flow chart of the study is shown in Figure 1.
 |
Figure 1 Flow chart of the study. |
The characteristics of survivors and non-survivors are summarized in Table 1. The non-survivors were significantly older than the survivors. Additionally, there were more patients who had to be hospitalized frequently due to AECOPD in the past year in the non-survivor group. Some comorbidities were more common in the non-survivor group, including hypertension, diabetes, renal dysfunction, pneumonia, and heart failure (all P < 0.05). The pulse rate in the non-survival group was faster than that in the survival group, and the non-survivors had a lower level of systolic blood pressure and diastolic blood pressure. The non-survivors had higher white blood cell (WBC) counts and D-dimer level as well as lower hemoglobin and eosinophil percentage (all P < 0.05). Serum BUN level was higher in the non-survivor group, and the difference was statistically significant [9.5 (6.8–15.3) vs 5.6 (4.3–7.5) mmol/L, P < 0.001]. There was no difference in respiratory rate, PaO2, lactic acid, uric acid or fibrinogen between the survivor group and the non-survivor group (all P > 0.05).
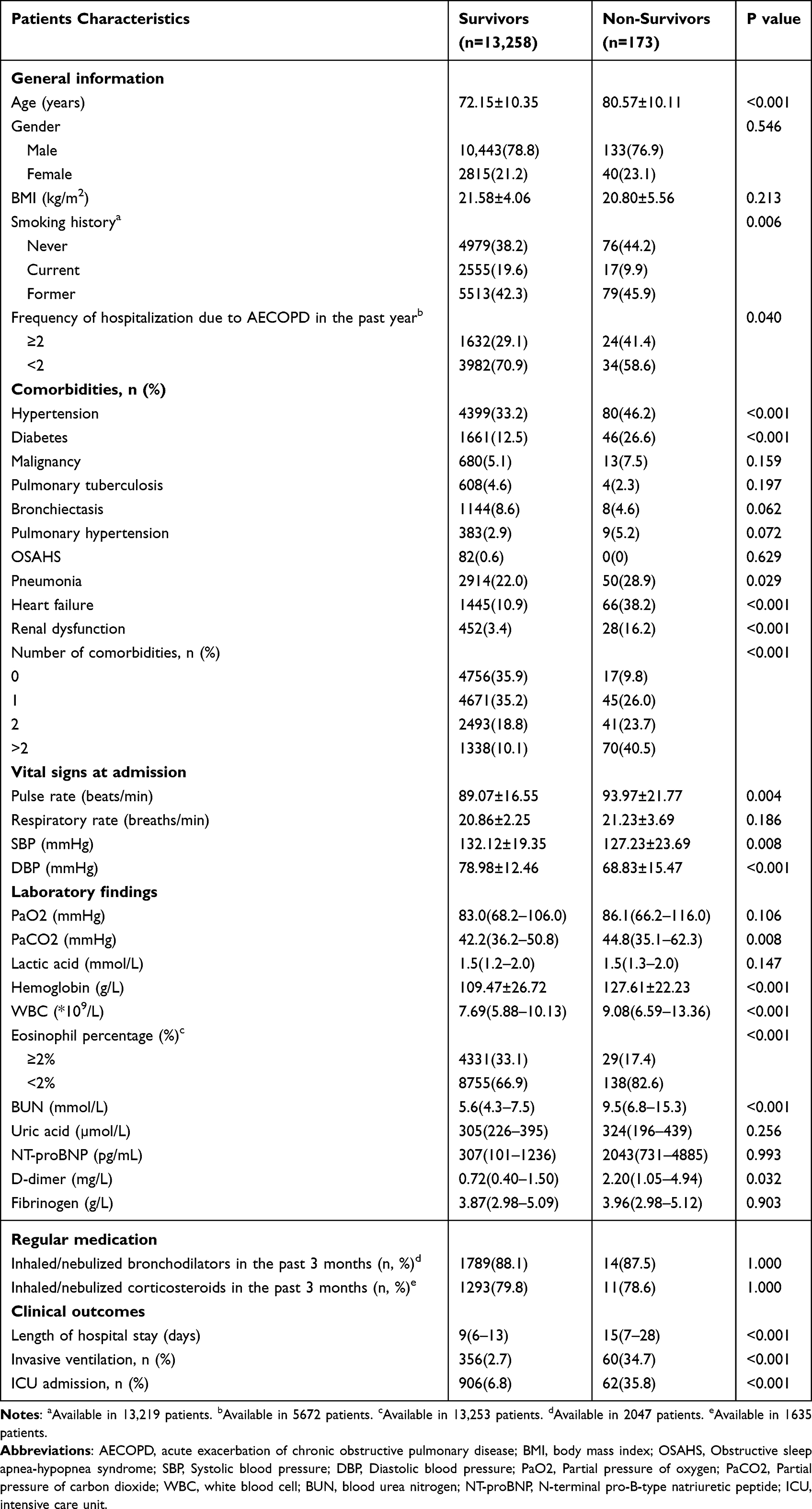 |
Table 1 Demographics and Clinical Characteristics of Patients with AECOPD Grouped by Mortality |
Associations Between BUN Level and Clinical Prognosis
ROC curve analysis showed that the optimal cutoff value of BUN level was 7.30 mmol/L for hospital mortality (AUC: 0.782; 95% CI: 0.748–0.816; P < 0.001) (Figure 2), with a sensitivity of 0.711 and a specificity of 0.726. The study cohort was stratified into two groups according to the BUN level. There were 3762 patients with BUN level ≥7.30 mmol/L and 9669 with BUN level <7.30 mmol/L. The characteristics in the patients with BUN level ≥7.30 mmol/L and BUN level <7.30 mmol/L are summarized and compared in Supplementary Table S1. Patients with BUN ≥ 7.30 mmol/L had higher rates of in-hospital mortality (3.3% vs 0.5%, P < 0.001), invasive mechanical ventilation (6.6% vs 1.7%, P < 0.001) and ICU admission (12.4% vs 5.2%, P < 0.001). In addition, a high level of BUN was associated with a longer length of stay (LOS) (10 vs 9 days, P < 0.001).
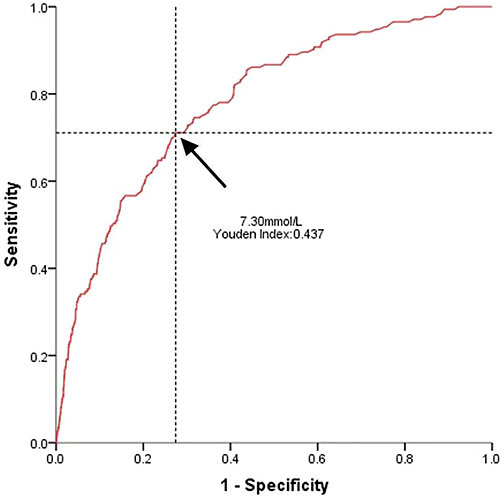 |
Figure 2 The ROC curve of BUN as a predictor of mortality in patients with AECOPD. |
Independent Risk Factors of in-Hospital Mortality of AECOPD
Univariable and multivariable Cox proportional hazard regressions were performed to evaluate the predictive factors related to mortality of AECOPD (Table 2). In univariable analysis, age, diabetes, renal dysfunction, heart failure, systolic blood pressure, diastolic blood pressure, pulse rate, PaCO2, hemoglobin, white blood cell, eosinophil percentage <2%, D-dimer, and BUN level ≥7.3 mmol/L were observed as potential prognostic factors of in-hospital mortality. After multivariate analysis, BUN level ≥7.3 mmol/L (HR = 2.099; 95% CI: 1.378–3.197, P = 0.001) was identified as an independent risk factor of in-hospital mortality. Other independent prognostic factors including older age (HR = 1.028; 95% CI: 1.008–1.049, P = 0.005), renal dysfunction (HR = 2.021; 95% CI: 1.319–3.095, P = 0.001), heart failure (HR=1.688; 95% CI: 1.148–2.483, P = 0.008), higher diastolic blood pressure (HR = 0.957; 95% CI: 0.941–0.973, P < 0.001), faster pulse rate (HR = 1.018; 95% CI: 1.008–1.028, P = 0.001), increased PaCO2 (HR = 1.016; 95% CI: 1.006–1.026, P = 0.001) and D-dimer (HR = 1.005; 95% CI: 1.000–1.009, P = 0.03) (Table 2).
 |
Table 2 Risk Factors Related to Mortality in Patients with AECOPD |
Risks for Adverse Outcomes in Association with BUN by Multivariate Analysis
Table 3 shows the risks for in-hospital mortality, invasive mechanical ventilation and ICU admission in association with BUN in the overall cohort after multivariate analysis. High on-admission BUN (≥7.30 mmol/L) remained an independent predictor in model one which was adjusted for age and sex (for in-hospital mortality: HR = 3.553, 95% CI: 2.528–4.995, P < 0.001, for invasive mechanical ventilation: HR = 2.590; 95% CI: 2.112–3.176, P < 0.001, and for ICU admission: HR = 1.734; 95% CI: 1.521–1.976, P < 0.001) and model two which was adjusted for age, diabetes, renal dysfunction, heart failure, systolic blood pressure, diastolic blood pressure, pulse rate, PaCO2, hemoglobin, white blood cell, eosinophil percentage <2% and D-dimer (for in-hospital mortality: HR = 2.099, 95% CI: 1.378–3.197, P = 0.001, for invasive mechanical ventilation: HR = 1.540; 95% CI: 1.199–1.977, P = 0.001 and for ICU admission: HR = 1.344; 95% CI: 1.117–1.617, P = 0.002).
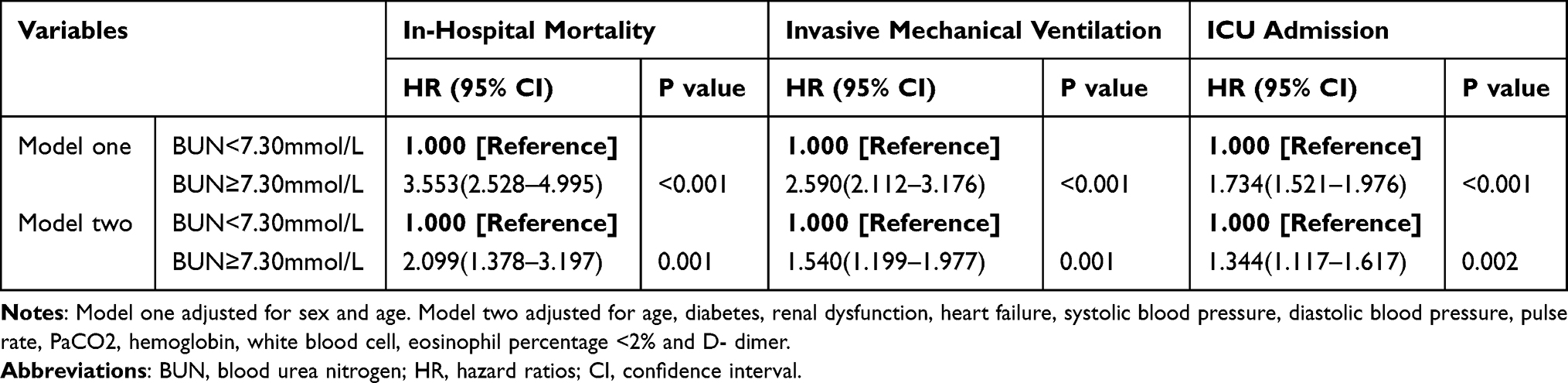 |
Table 3 Multivariate Analysis on Adverse Outcomes in Patients with AECOPD |
Kaplan–Meier Survival Analysis of the Cohort by BUN Levels
The Kaplan–Meier curve for BUN as a predictor for in-hospital mortality showed that patients with a BUN ≥ 7.30 mmol/L had a higher in-hospital mortality than patients with BUN level < 7.30 mmol/L (P < 0.001) (Figure 3).
 |
Figure 3 Kaplan–Meier curves of overall survival in patients with AECOPD with BUN level above (≥) and below (<)7.30 mmol/L. |
Discussion
In this multicenter cohort study, we observed that BUN levels were associated with in-hospital adverse outcomes in inpatients with AECOPD. BUN level ≥7.30 mmol/L was an independent risk factor for in-hospital mortality, invasive mechanical ventilation and ICU admission, which suggests elevated BUN level (≥7.30 mmol/L) may serve as a convenient indicator of the severity and poor prognosis in inpatients with AECOPD.
BUN has been reported to be associated with adverse outcomes of acute ischemic stroke, cardiovascular disease, acute pancreatitis, pneumonia, and pulmonary embolism.10–14,20–22 Some studies tried to explore relationship between BUN and the prognosis of AECOPD; however, a consensus was not reached, which might be attributed to different study populations and small sample sizes in some studies.7,15,17,23,24 For example, two studies from Canada and Netherlands demonstrated that elevated BUN level increased hospital mortality in patients with AECOPD.15,24 However, A study conducted in Australia held that BUN was not a strong and independent predictor of in-hospital and 1-year mortality in AECOPD.17 The findings on association between BUN and poor prognosis in patients with AECOPD are inconsistent even within Chinese population.7,23 In this large and multicenter cohort study conducted in China, elevated BUN levels were demonstrated to be a significant contributor to early mortality and adverse outcomes in patients with AECOPD. Additionally, the optimal cutoff value of BUN in patients with a high risk of mortality has not been consistent either across different study populations. Chen et al identified an admission BUN of 7.63 mmol/L as an optimal cutoff value to predict hospital mortality in patients with AECOPD.7 Stiell identified elevated BUN level with a cutoff value of 12 mmol/L as a high-risk biomarker which could be used to stratify the likelihood of poor outcomes in patients with AECOPD.15 Moreover, BUN > 7 mmol/L is one of six clinical parameters of CURB65 score, which has been proven effective in predicting early mortality in AECOPD and can be used to assess risk stratification.25 In this study, we determined an optimal cutoff value of BUN (7.30mmol/L) that corresponds to a higher risk of death in Chinese inpatients with AECOPD, which provided a reference value for the severity and prognosis of AECOPD in Chinese subjects.
The mechanism underlying the association between elevated BUN levels and adverse outcomes in AECOPD has not been well defined. BUN is a metabolite produced by protein, and its concentration represents the balance of excretion and reabsorption in the kidneys.11 A higher BUN could potentially be a marker of renal hypoperfusion and renal injury,22 which were closely associated with early mortality in patients with AECOPD.26,27 In our cohort, we also found higher incidence of renal dysfunction was associated with higher BUN (Supplementary Table S1). Additionally, studies have found that high BUN levels may reflect activation of the renin-angiotensin-aldosterone and sympathetic nerve systems, which impair mitochondrial function in cardiac cells.28,29 Therefore, a higher BUN may serve as an efficient biomarker of cardiac insufficiency and thus be closely related to adverse outcomes.30 In our cohort, elevated BUN level remained an independent predictor of hospital mortality after adjusted for renal dysfunction and heart failure, which indicates other mechanisms may also exist. Therefore, the mechanism linking BUN to the short-term mortality of patients with AECOPD may be complex and requires further researches.
Additionally, we found age, renal dysfunction, heart failure, diastolic blood pressure, pulse rate, PaCO2, and D-dimer were observed to be significantly associated with mortality, which were consistent with previous researches. It is well known that older population accounted for an increasing risk for adverse outcomes among hospitalized patients.31 Renal dysfunction is a frequent complication of patients admitted to the hospital for AECOPD and represented a very important predictive factor of in-hospital mortality.26 Heart failure played a role in the occurrence of worse prognosis in AECOPD, which was consistent with the study results reported by Yoshihisa A and Ahn YH.32,33 Diastolic blood pressure, instead of systolic blood pressure, and pulse pressure that as easily obtained predictors were considered to be associated with hospital mortality in patients with COPD.34 Hypercapnia often occurs in patients with AECOPD, which was defined as PaCO2>50 mmHg. PaCO2 is an independent prognostic factor of mortality in COPD and should be optimally treated.35 We also found that a higher D-dimer level was an independent risk factor for in-hospital mortality of AECOPD. D-dimer level has been previously reported to be a predictor of hospital mortality in COPD exacerbations.27,36,37
To our knowledge, this is the first large-scale multicenter cohort study to explore the association between BUN levels and adverse outcomes in inpatients with AECOPD. The consecutive inclusion of unselected inpatients with AECOPD and comprehensive collection of information, including baseline demographics, comorbidities and laboratory tests, outcomes etc., in our study ensured high data quality and true associations in the real world setting. Nevertheless, our study has several limitations. First, this was a secondary analysis of a prospectively cohort of patients with AECOPD, we could not reach all baseline characteristics. Fortunately, the proportion of excluded patients was small and the impact on our results can be neglected. Second, because patients with AECOPD generally have poor breathing status and cannot afford the pulmonary function test, and related data from stable stage were missing for many patients; thus, parameters of pulmonary function were not included into our analysis. Third, our study did not measure some laboratory data which were associated with mortality in previous studies, such as neutrophil lymphocyte ratio, and platelet lymphocyte ratio. Finally, the lack of follow-up data prevented us from further evaluating the association of BUN with long-time outcome of AECOPD patients.
Conclusions
In this large cohort study, elevation of BUN (≥7.30 mmol/L) was associated with increased risk for in-hospital mortality and other adverse outcomes in AECOPD inpatients. BUN is an easily available biomarker that may be used to identify serious patients and guide the management of AECOPD inpatients.
Abbreviations
COPD, chronic obstructive pulmonary disease; AECOPD, Acute exacerbation of chronic obstructive pulmonary disease; BUN, Blood urea nitrogen; COVID-19, Coronavirus disease 2019; MAGNET AECOPD, MAnaGement aNd advErse ouTcomes in inpatients with acute exacerbation of COPD Registry; GOLD, Global Initiative for Chronic Obstructive Lung Disease; ICU, intensive care unit; IQR, interquartile range; ROC, Receiver operating characteristic; HR, hazard ratio; 95% CI, 95% confidence interval; WBC, White blood cell; LOS, length of stay.
Data Sharing Statement
The datasets used and analyzed during the present study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the ten academic medical centers that participated. Written informed consent was obtained from all the participants.
Consent for Publication
The participant has consented to the submission of this article to the journal.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (82170013), the Sichuan Science and Technology Program (2022YFS0262) and the National Key Research Program of China (2016YFC1304202).
Disclosure
The authors declare that the research had no conflicts of interest.
References
1. Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370(9589):765–773. doi:10.1016/s0140-6736(07)61380-4
2. Murphy PB, Rehal S, Arbane G, et al. Effect of home noninvasive ventilation with oxygen therapy vs oxygen therapy alone on hospital readmission or death after an acute COPD exacerbation: a randomized clinical trial. JAMA. 2017;317(21):2177–2186. doi:10.1001/jama.2017.4451
3. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/s0140-6736(18)30841-9
4. Zafari Z, Li S, Eakin MN, Bellanger M, Reed RM. Projecting long-term health and economic burden of COPD in the United States. Chest. 2021;159(4):1400–1410. doi:10.1016/j.chest.2020.09.255
5. Criner GJ, Bourbeau J, Diekemper RL, et al. Prevention of acute exacerbations of COPD: American College of Chest Physicians and Canadian Thoracic Society Guideline. Chest. 2015;147(4):894–942. doi:10.1378/chest.14-1676
6. Groves D, Karsanji U, Evans RA, et al. Predicting future health risk in COPD: differential impact of disease-specific and multi-morbidity-based risk stratification. Int J Chron Obstruct Pulmon Dis. 2021;16:1741–1754. doi:10.2147/copd.S303202
7. Chen L, Chen L, Zheng H, Wu S, Wang S. The association of blood urea nitrogen levels upon emergency admission with mortality in acute exacerbation of chronic obstructive pulmonary disease. Chron Respir Dis. 2021;18:14799731211060051. doi:10.1177/14799731211060051
8. Steer J, Gibson J, Bourke SC. The DECAF score: predicting hospital mortality in exacerbations of chronic obstructive pulmonary disease. Thorax. 2012;67(11):970–976. doi:10.1136/thoraxjnl-2012-202103
9. Trudzinski FC, Alqudrah M, Omlor A, et al. Consequences of chronic kidney disease in chronic obstructive pulmonary disease. Respir Res. 2019;20(1):151. doi:10.1186/s12931-019-1107-x
10. You S, Zheng D, Zhong C, et al. Prognostic significance of blood urea nitrogen in acute ischemic stroke. Circ J. 2018;82(2):572–578. doi:10.1253/circj.CJ-17-0485
11. Lan Q, Zheng L, Zhou X, et al. The value of blood urea nitrogen in the prediction of risks of cardiovascular disease in an older population. Front Cardiovasc Med. 2021;8:614117. doi:10.3389/fcvm.2021.614117
12. Cheng A, Hu L, Wang Y, et al. Diagnostic performance of initial blood urea nitrogen combined with D-dimer levels for predicting in-hospital mortality in COVID-19 patients. Int J Antimicrob Agents. 2020;56(3):106110. doi:10.1016/j.ijantimicag.2020.106110
13. Vitale DS, Hornung L, Lin TK, et al. Blood urea nitrogen elevation is a marker for pediatric severe acute pancreatitis. Pancreas. 2019;48(3):363–366. doi:10.1097/mpa.0000000000001265
14. Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58(5):377–382. doi:10.1136/thorax.58.5.377
15. Stiell IG, Clement CM, Aaron SD, et al. Clinical characteristics associated with adverse events in patients with exacerbation of chronic obstructive pulmonary disease: a prospective cohort study. CMAJ. 2014;186(6):E193–E204. doi:10.1503/cmaj.130968
16. Zeng Z, Ke X, Gong S, et al. Blood urea nitrogen to serum albumin ratio: a good predictor of in-hospital and 90-day all-cause mortality in patients with acute exacerbations of chronic obstructive pulmonary disease. BMC Pulm Med. 2022;22(1):476. doi:10.1186/s12890-022-02258-7
17. Kumar P, Law S, Sriram KB. Evaluation of platelet lymphocyte ratio and 90-day mortality in patients with acute exacerbation of chronic obstructive pulmonary disease. J Thorac Dis. 2017;9(6):1509–1516. doi:10.21037/jtd.2017.05.77
18. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
19. Zhou C, Yi Q, Ge H, et al. Validation of risk assessment models predicting venous thromboembolism in inpatients with acute exacerbation of chronic obstructive pulmonary disease: a multicenter cohort study in China. Thromb Haemost. 2022;122(7):1177–1185. doi:10.1055/a-1693-0063
20. Liu J, Sun LL, Wang J, Ji G. Blood urea nitrogen in the prediction of in-hospital mortality of patients with acute aortic dissection. Cardiol J. 2018;25(3):371–376. doi:10.5603/CJ.a2017.0075
21. Khoury J, Bahouth F, Stabholz Y, et al. Blood urea nitrogen variation upon admission and at discharge in patients with heart failure. ESC Heart Fail. 2019;6(4):809–816. doi:10.1002/ehf2.12471
22. Tatlisu MA, Kaya A, Keskin M, et al. The association of blood urea nitrogen levels with mortality in acute pulmonary embolism. J Crit Care. 2017;39:248–253. doi:10.1016/j.jcrc.2016.12.019
23. Li H, Zeng Z, Cheng J, et al. Prognostic role of NT-proBNP for in-hospital and 1-year mortality in patients with acute exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:57–67. doi:10.2147/copd.S231808
24. Slenter RH, Sprooten RT, Kotz D, Wesseling G, Wouters EF, Rohde GG. Predictors of 1-year mortality at hospital admission for acute exacerbations of chronic obstructive pulmonary disease. Respiration. 2013;85(1):15–26. doi:10.1159/000342036
25. Chang CL, Sullivan GD, Karalus NC, Mills GD, McLachlan JD, Hancox RJ. Predicting early mortality in acute exacerbation of chronic obstructive pulmonary disease using the CURB65 score. Respirology. 2011;16(1):146–151. doi:10.1111/j.1440-1843.2010.01866.x
26. Fabbian F, De Giorgi A, Manfredini F, et al. Impact of renal dysfunction on in-hospital mortality of patients with severe chronic obstructive pulmonary disease: a single-center Italian study. Int Urol Nephrol. 2016;48(7):1121–1127. doi:10.1007/s11255-016-1272-5
27. Hu G, Wu Y, Zhou Y, et al. Prognostic role of D-dimer for in-hospital and 1-year mortality in exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:2729–2736. doi:10.2147/copd.S112882
28. Horiuchi Y, Aoki J, Tanabe K, et al. A high level of blood urea nitrogen is a significant predictor for in-hospital mortality in patients with acute myocardial infarction. Int Heart J. 2018;59(2):263–271. doi:10.1536/ihj.17-009
29. Tajes M, Díez-López C, Enjuanes C, et al. Neurohormonal activation induces intracellular iron deficiency and mitochondrial dysfunction in cardiac cells. Cell Biosci. 2021;11(1):89. doi:10.1186/s13578-021-00605-5
30. Høiseth AD, Omland T, Hagve TA, Brekke PH, Søyseth V. NT-proBNP independently predicts long term mortality after acute exacerbation of COPD - a prospective cohort study. Respir Res. 2012;13(1):97. doi:10.1186/1465-9921-13-97
31. Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
32. Yoshihisa A, Takiguchi M, Shimizu T, et al. Cardiovascular function and prognosis of patients with heart failure coexistent with chronic obstructive pulmonary disease. J Cardiol. 2014;64(4):256–264. doi:10.1016/j.jjcc.2014.02.003
33. Ahn YH, Lee KS, Park JH, et al. Independent risk factors for mortality in patients with chronic obstructive pulmonary disease who undergo comprehensive cardiac evaluations. Respiration. 2015;90(3):199–205. doi:10.1159/000437097
34. Byrd JB, Newby DE, Anderson JA, et al. Blood pressure, heart rate, and mortality in chronic obstructive pulmonary disease: the SUMMIT trial. Eur Heart J. 2018;39(33):3128–3134. doi:10.1093/eurheartj/ehy451
35. Ahmadi Z, Bornefalk-Hermansson A, Franklin KA, Midgren B, Ekström MP. Hypo- and hypercapnia predict mortality in oxygen-dependent chronic obstructive pulmonary disease: a population-based prospective study. Respir Res. 2014;15(1):30. doi:10.1186/1465-9921-15-30
36. Husebø GR, Gabazza EC, D’Alessandro Gabazza C, et al. Coagulation markers as predictors for clinical events in COPD. Respirology. 2021;26(4):342–351. doi:10.1111/resp.13971
37. Fruchter O, Yigla M, Kramer MR. D-dimer as a prognostic biomarker for mortality in chronic obstructive pulmonary disease exacerbation. Am J Med Sci. 2015;349(1):29–35. doi:10.1097/maj.0000000000000332
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.