")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Elevated ApoB/apoA-1 is Associated with in-Hospital Mortality in Elderly Patients with Acute Myocardial Infarction
Authors Chen Y , Chen S, Han Y, Xu Q, Zhao X
Received 4 August 2023
Accepted for publication 21 October 2023
Published 3 November 2023 Volume 2023:16 Pages 3501—3512
DOI https://doi.org/10.2147/DMSO.S433876
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Yan Chen, Shengyue Chen, Yuanyuan Han, Qing Xu, Xin Zhao
Department of Cardiology, The Second Hospital of Dalian Medical University, Dalian, People’s Republic of China
Correspondence: Xin Zhao, Department of Cardiology, The Second Hospital of Dalian Medical University, No. 467 Zhongshan Road, Shahekou District, Dalian, 116023, People’s Republic of China, Tel +86-0411-84671291, Email [email protected]
Background: Apolipoprotein B/apolipoprotein A-1 (apoB/apoA-1) has been shown to be strongly associated with the risk of future cardiovascular disease, but the association between apoB/apoA-1 and the risk of in-hospital death in elderly patients with acute myocardial infarction(AMI) is inconclusive.
Aim: To investigate the association between apoB/apoA-1 and the risk of in-hospital death in elderly patients with AMI.
Methods: From December 2015 to December 2021, a total of 1495 elderly AMI patients (aged ≥ 60 years) with complete clinical history data were enrolled in the Second Hospital of Dalian Medical University. Outcome was defined as all-cause mortality during hospitalization. Multivariate logistic regression and restricted spline cubic (RCS) models were used to evaluate the association between apoB/apoA-1 and in-hospital mortality risk, respectively. Receiver operating characteristic(ROC) curves were used to evaluate the predictive value of apoB/apoA-1 for in-hospital mortality events. Discordance analysis was performed when apoB/apoA-1 and LDL-C/HDL-C were not in concordance.
Results: (1) A total of 128 patients (8.6%) died during hospitalization. Patients in the death group had higher apoB/apoA-1 than those in the non-death group, but lower apoA-1 levels than those in the non-death group, and the difference was statistically significant (P < 0.05); (2) Multivariate logistic regression analysis showed that apoB/apoA-1 was associated with the risk of in-hospital death in elderly AMI patients [Model 3 OR = 3.524 (1.622– 7.659), P = 0.001]; (3) ROC curve analysis showed that apoB/apoA-1 (AUC = 0.572, P = 0.011) had some predictive value for the risk of in-hospital death in elderly AMI patients; (4) RCS models showed a linear dose-response relationship between apoB/apoA-1 and in-hospital death after adjusting for confounders (P for non-linearity = 0.762).
Conclusion: ApoB/apoA-1 is associated with the risk of in-hospital death in elderly patients with AMI, and is superior to other blood lipid parameters and blood lipid ratio.
Keywords: elderly, apolipoprotein, acute myocardial infarction, in-hospital death, restricted cubic splines
Introduction
Acute myocardial infarction (AMI) is a common and critical cardiovascular emergency. If patients cannot receive timely treatment, could be changed to heart failure and subsequent death. The rapid development of percutaneous coronary intervention (PCI) has significantly reduced the mortality and morbidity of AMI. However, previous studies have shown that mortality within 12 months in patients with AMI is approximately 10%,1,2 and the risk of in-hospital mortality is approximately 4% to 12%.3 Elderly patients with AMI have been one of the priorities in clinical diagnosis and treatment because the risk of death during hospitalization in such patients increases significantly with age. Therefore, it is necessary to find a convenient and accurate index to predict the risk of death during hospitalization in elderly AMI patients.
Dyslipidemia has been considered to be one of the most important causes of atherosclerotic cardiovascular disease (ASCVD), and low-density lipoprotein cholesterol (LDL-C) has been paid much attention among many lipid parameters.4 However, many studies have shown that apolipoprotein B/apolipoprotein A-1 (apoB/apoA-1) is superior to LDL-C in predicting the risk of cardiovascular disease.5,6 Physiologically, each very low-density lipoprotein (VLDL), intermediate-density lipoprotein (IDL), low-density lipoprotein (LDL), and lipoprotein (α) particle contains an apoB molecule, so apoB in plasma represents the sum of almost all atherogenic particles in the body,7–9 while apoA-1 is the main apolipoprotein in high-density lipoprotein (HDL) particles and is considered to have an anti-atherosclerotic effect.10 Compared with apoB and apoA-1, apoB/apoA-1 reflects the balance between atherogenic and anti-atherogenic factors in the body in the form of a combination of two apolipoproteins.11 The results of the AMORIS (Apolipoprotein-related Mortality Risk) study12 and the INTERHEART study5 indicate that apoB/apoA-1 is an important predictor of future coronary events. However, few studies have investigated the association between apoB/apoA-1 and the risk of in-hospital mortality in AMI patients, especially in elderly AMI patients.
Therefore, the aim of this study was to investigate the association between apoB/apoA-1 and the risk of in-hospital mortality in elderly AMI and whether there is a dose-response relationship for this association.
Methods
Study Population
This was a single-center, retrospective and observational study of 1495 elderly patients 60 years of age and older with AMI who were hospitalized at the Second Hospital of Dalian Medical University from December 2015 to December 2021. This study is an observational study, in which patients informed consent can be exempted and ethical requirements in the Declaration of Helsinki have been met, and has been approved by the Ethics Committee of the Second Hospital of Dalian Medical University (No. 2023–118). Inclusion criteria: 1. Age ≥ 60 years; 2. Diagnosis of acute myocardial infarction (including NSTEMI and STEMI) at admission.13,14 Exclusion criteria: 1. Patients with the following conditions: Familial hypercholesterolemia, hyperthyroidism or hypothyroidism, nephrotic syndrome, Cushing syndrome; 2. Patients with severe coronary artery disease, requiring cardiac bypass surgery or having previously undergone cardiac bypass surgery less than half a year; 3. Life expectancy less than half a year.
Data Collection, Processing and Outcome Definition
The clinical characteristics, medical history, and laboratory test results of the patients at admission and during hospitalization were collected from the electronic medical record system. The laboratory tests performed at admission mainly included liver and kidney function, blood lipid, serum ion levels, and myocardial enzyme levels. Venous blood samples were collected after fasting for at least 12 h and assayed within 24 h of admission. Lipid parameters, including apoB and apoA-1, were measured directly by a homogeneous method under fasting conditions. The drug use during hospitalization was also recorded, including lipid-lowering drugs, β-blockers, ACEI/ARBs, and aspirin. The outcome was defined as all-cause mortality during hospitalization.
Statistical Analysis
Data were processed by SPSS (version 26.0, IBM Corp. in Armonk, NY. www.ibm.com/products/spss-statistics), MedCalc (version 20.022, MedCalc Software Ltd, Ostend, Belgium. www.medcalc.org), R(version 4.2.1, R Core Team 2020, Vienna, Austria. www.r-project.org). For categorical variables, data were described as frequencies or percentages. For continuous variables, data were presented as mean ± standard deviation if normal distribution was met; otherwise, data were presented as quartiles [median (quartiles 25, 75%)]. If continuous data satisfied normality, comparisons between two or more groups were analyzed by t-test or ANOVA; otherwise, nonparametric tests were used. Categorical variables were compared using Fisher ‘s exact test or Chi-square test. Receiver operating characteristic (ROC) curves were used to explore the performance of apoB/apoA-1. Multivariate logistic regression was used to analyze the association between apoB/apoA-1 and outcome events. In addition, restricted cubic splines (RCS) were used to explore the dose-response relationship between apoB/apoA-1 and in-hospital mortality. A discordance analysis was further performed to quantify the association of apoB/apoA-1 and LDL-C/HDL-C with In-hospital death when the two ratios were not in concordance. P < 0.05 was considered statistically significant.
Results
Sample Characteristics
The cohort of the study is baseline in Table 1. A total of 1495 elderly patients with AMI were included in this retrospective study, and a total of 128 deaths (8.6%) were recorded during hospitalization. The mean age and proportion of females in the death group (mean age 79.80 ± 8.69, 46.1% female) were higher than those in the non-death group (72.59 ± 8.34, 39.2% female). Among the lipid related parameters, apoB/apoA-1 levels were higher in patients who died than in patients without death[0.75 (0.60, 1.00) vs 0.72 (0.57, 0.88)]; apoA-1 and TG levels were lower in patients who died than in patients without death, and the difference was statistically significant (P < 0.05).
 |
Table 1 Basic Characteristics of Enrolling Patients |
Associations of apoB/apoA-1 with Risk of in-Hospital Mortality in Elderly Patients with AMI
Logistic regression analysis was used to analyze the factors affecting in-hospital death in elderly AMI patients. Univariate logistic regression showed that age, apoB/apoA-1, diabetes, type of AMI (including NSTEMI and STEMI, NSTEMI as reference), heart failure, cardiac troponin I(CTNI) and eGFR class were positively associated with the risk of in-hospital death in elderly AMI patients, as detailed in Table 2. We developed three logistic regression models based on the results of univariate logistic analysis. Model 1 was not adjusted for any confounders, model 2 was adjusted for sex and age. Model 3 was adjusted for body mass index(BMI), type of AMI, eGFR, CTNI, presence of heart failure, diabetes, PCI during hospitalization, history of stroke, and in-hospital medication (Aspirin use and Statins use) on the basis of model 2. Multivariate logistic regression results showed that apoB/apoA-1 was associated with the risk of in-hospital death in elderly AMI patients [Model 3 OR = 3.524 (1.622–7.659), P = 0.001], as detailed in Table 3. We also evaluated the association between common clinical lipid parameters and the risk of death during hospitalization in elderly AMI patients in a multivariate logistic regression model. Except for apoA-1, other lipid indicators or lipid ratios were not correlated with the risk of death during hospitalization, as detailed in Supplementary Table 1.
 |
Table 2 Univariate Analysis of Factors Affecting in-Hospital Mortality in Elderly Patients with AMI |
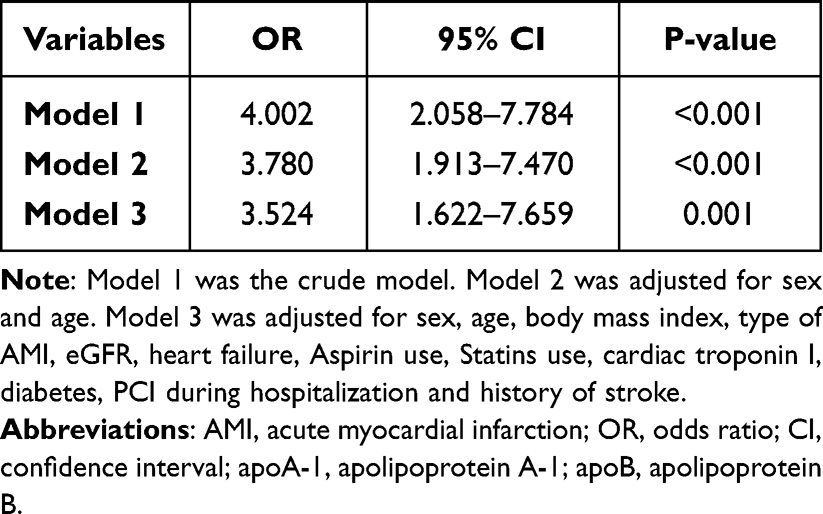 |
Table 3 Multivariate Logistic Regression Analysis of ApoB/apoA-1 and in-Hospital Mortality in Elderly Patients with AMI |
Predictive Value of apoB/apoA-1 for the Risk of in-Hospital Mortality in Elderly Patients with AMI
ROC curves were used to evaluate the predictive value of apoB/apoA-1 for in-hospital mortality in elderly patients with AMI. The results showed that the AUC of apoB/apoA-1 were 0.572 (95% CI 0.547–0.597, P = 0.011). The optimal cut-off levels of apoB/apoA-1 were 0.938 (Sensitivity = 32.81%, Specificity = 82.44%). In addition, we assessed whether apoB/apoA-1 has differential predictive power for elderly patients with NSTEMI or STEMI. The results showed that there was no difference in the predictive ability of apoB/apoA-1 for in-hospital mortality risk between elderly patients with NSTEMI and STEMI (P for difference between areas = 0.341), as detailed in Figure 1.
 |
Figure 1 The ROC analysis of apoB/apoA-1 predicting in-hospital death in elderly AMI patients. (A) The ROC analysis of apoB/apoA-1 predicting in-hospital death in elderly AMI patients; (B) Comparison of the predictive ability of apoB/apoA-1 on the risk of in-hospital mortality between elderly STEMI patients and NSTEMI patients. Abbreviations: AMI, acute myocardial infarction; NSTEMI, non-ST segment elevation myocardial infarction; STEMI, ST segment elevation myocardial infarction. apoA-1, apolipoprotein A-1; apoB, apolipoprotein B. |
Dose-Response Relationship Between Apolipoprotein-Related Markers and Risk of in-Hospital Mortality in Elderly Patients with AMI
The relationship between apolipoprotein-related parameters (apoB, apoA-1, and apoB/apoA-1) and the risk of in-hospital death in elderly patients with AMI was assessed by RCS, as detailed in Figure 2. The results showed a linear dose-response relationship between apoB/apoA-1 and outcome events (P for non-linearity = 0.119), which remained when confounders were adjusted (P for non-linearity = 0.762). This suggests that with increasing apoB/apoA-1, there is also an increased risk of in-hospital mortality in older patients with AMI. However, there was a non-linear dose-response relationship between apoA-1 and outcome events, roughly in an “L” pattern (P for adjusted non-linearity = 0.009).
 |
Figure 2 Dose-response relationship between apolipoprotein-related markers and in-hospital mortality in elderly patients with AMI. (A) Unadjusted dose-response relationship between apoB and in-hospital mortality in elderly patients with AMI; (B) Adjusted dose-response relationship between apoB and in-hospital mortality in elderly patients with AMI; (C) Unadjusted dose-response relationship between apoA-1 and in-hospital mortality in elderly patients with AMI; (D) Adjusted dose-response relationship between apoA-1 and in-hospital mortality in elderly patients with AMI; (E) Unadjusted dose-response relationship between apoB/apoA-1 and in-hospital mortality in elderly patients with AMI; (F) Adjusted dose-response relationship between apoB/apoA-1 and in-hospital mortality in elderly patients with AMI. Adjusted factors include sex, age, BMI, type of AMI, eGFR, cardiac troponin I(CTNI), presence of heart failure, diabetes, PCI during hospitalization, history of stroke, and in-hospital medication (Aspirin use and Statins use). Abbreviations: AMI, acute myocardial infarction. apoA-1, apolipoprotein A-1; apoB, apolipoprotein B. |
Discordance Analysis of apoB/apoA-1 and LDL-C/HDL-C
Spearman correlation analysis was performed for lipid parameters included in the baseline data, as shown in Figure 3. The results showed that apoB/apoA-1 had the highest correlation with LDL-C/HDL-C (R = 0.82, P < 0.001), which exceeded the correlation between apoB/apoA-1 and other lipid parameters. Concordance quantifies the variance of one variable at any level to the other. In fact, two variables can be highly correlated but be highly discordant, ie They do not correspond well, either they are too high or too low compared with the other variable. Therefore, we analyzed the discordance between apoB/apoA-1 and LDL-C/HDL-C. Discordance and concordance was defined by calculating the respective medians for apoB/apoA-1 and LDL-C/HDL-C: concordance was defined if both were < or ≥ their respective medians, and vice versa. The associations between discordance and risk of in-hospital mortality in older patients with AMI were assessed by multivariate logistic regression models. Although discordance (apoB/apoA-1 ≥ medianapoB/apoA-1 and LDL-C/HDL-C < medianLDL-C/HDL-C) may be associated with outcome events before adjustment for confounders [Model 1 OR = 1.892(1.104–3.243), P = 0.020], this association disappeared after adjustment for confounding factors [Model 3 OR = 1.139 (0.575–2.253), P = 0.709], as detailed in Table 4.
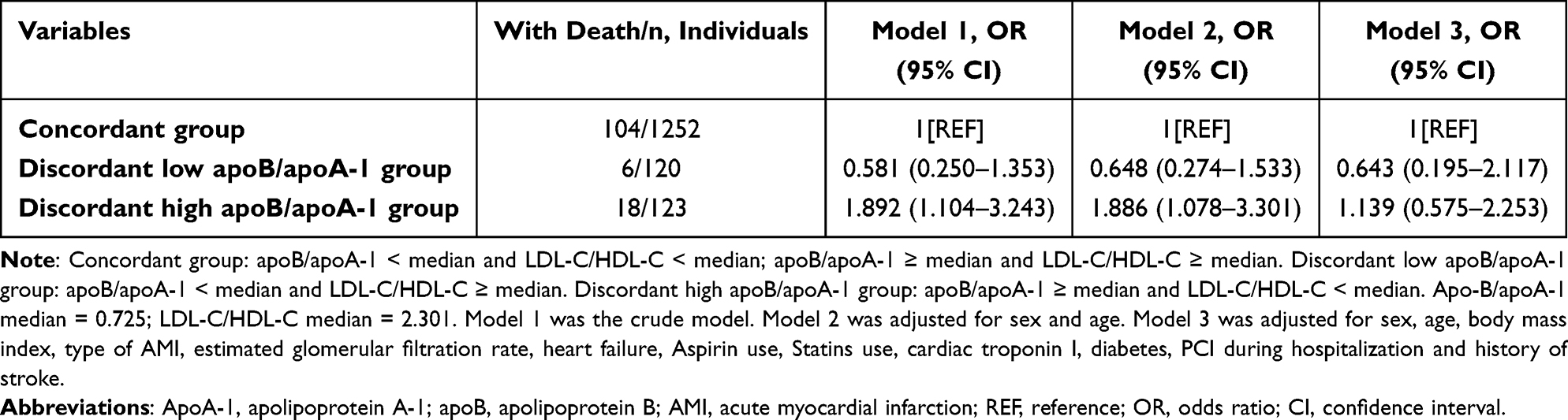 |
Table 4 Multivariate Logistic Regression Analysis Between Discordance Between ApoB/apoA-1 and LDL-C/HDL-C and Risk of in-Hospital Mortality in Elderly AMI Patients |
 |
Figure 3 Spearman correlation analysis between each pair of lipid measures. Abbreviations: TC, total cholesterol; TG, triglyceride; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; NHDL-C, non-high-density lipoprotein cholesterol; RC, remnant cholesterol; apoA-1, apolipoprotein A-1; apoB, apolipoprotein B. Notes: Asterisk (*) indicates whether the association between the two lipid parameters is statistically significant. The color of the squares indicates the strength of the correlation between the two lipid parameters, and darker colors represent the stronger correlation between the two, and vice versa. None*P > 0.05; ***P < 0.001. |
Discussion
In this retrospective study of 1495 elderly patients with AMI, we investigated the association between apoB/apoA-1 and the risk of in-hospital death in elderly patients with AMI. Univariate logistic regression showed that apoB/apoA-1 was associated with the risk of in-hospital death in elderly patients with AMI (OR = 4.002 (2.058–7.784), P < 0.001). Subsequently, we adjusted for some confounding factors that may influence outcome by multivariate logistic regression and showed that apoB/apoA-1 remained strongly associated with the risk of in-hospital mortality in elderly patients with AMI [Model 3 OR = 3.524 (1.622–7.659), P = 0.001]. The results of ROC curve analysis showed that apoB/apoA-1 could also be used to predict the occurrence of in-hospital death events in elderly AMI patients. We also further investigated the dose-response relationship of apoB/apoA-1 with the risk of in-hospital mortality in elderly AMI patients based on the RCS model for the first time, and the results showed that the risk of in-hospital mortality in elderly AMI patients also showed a linear trend to increase when apoB/apoA-1 increased. Finally, we found that apoB/apoA-1 showed the strongest association with LDL-C/HDL-C (R = 0.82, P < 0.001). Because highly correlated two variables can also be highly inconsistent (poor correspondence between the two variables),11 discordance between apoB/apoA-1 and LDL-C/HDL-C was further analyzed, but discordance between high apoB/apoA-1 and low LDL-C/HDL-C was not associated with outcome events after multivariate adjustment [Model 3 OR = 1.139 (0.575–2.253), P = 0.709], which may be due to the small sample size in this group.
Compared with LDL-C, apoB provides more information about the risk of cardiovascular disease in patients, which is determined by its physiological properties. Simply put, LDL can be divided into two subtypes: small-dense LDL (sd-LDL) and large floating LDL. But sd-LDL particles tend to be more dangerous than large, floating LDL particles. Because sd-LDL particles are more easily oxidized and promote inflammatory responses and plaque growth, exacerbating cardiovascular disease risk.15–18 When the body ‘s LDL is dominated by sd-LDL, the body needs the liver to make enough LDL to carry cholesterol, and there is an apoB molecule on each LDL surface, so apoB reflects the content of sd-LDL in the body to a certain extent.11 When LDL-C levels are the same in both patients, if sd-LDL particles predominate in one patient and large buoyant LDL particles in the other, the risk of potential cardiovascular disease is significantly different despite the same LDL-C levels in both patients,19 which is one of the important reasons why apoB is more predictive of the risk of cardiovascular disease in patients than LDL-C. ApoA-1 transports HDL particles, which have anti-inflammatory, antioxidant, antithrombotic, and vasodilator effects and are critical in the anti-atherosclerotic process,20–22 and therefore tends to provide more information about the risk of cardiovascular disease than HDL-C. ApoB/apoA-1 actually reflects the balance between atherogenic and anti-atherosclerotic factors in the human body and is more significant than apoB, apoA-1, and other common lipid parameters alone to predict cardiovascular disease risk.11 The AMORIS study12 is the first cohort study to systematically evaluate the long-term risk of apoB, apoA-1, and apoB/apoA-1 with cardiovascular disease, and its results suggest that apoB/apoA-1 is very closely related to the risk of myocardial infarction, stroke, and other cardiovascular diseases. Similar results were also described in the INTERHEART study,5 which found the strongest association between apoB/apoA-1 and AMI (OR = 3.25, 99% CI 2.81–3.76). Walldius et al found that apoB/apoA-1 was associated with major adverse cardiovascular events(MACEs).23 Steyn et al6 found that apoB/apoA-1 was more strongly associated with AMI than LDL-C and other lipid ratios (South African population), which is similar to that found in the overall INTERHEART population. Similar conclusions were reached by the findings of Goswami et al,24 who found that apoB/apoA-1 identified CAD risk more than other lipid ratios (TC/HDL-C, NHDL-C/HDL-C, LDL-C/HDL-C). In addition, several studies have demonstrated that apoB/apoA-1 is a strong predictor of future coronary events in people initially free of coronary artery disease.25–28 Li et al observed that apoB/apoA-1 was also associated with total occlusion in CAD patients (OR = 2.590, 95% CI 2.049–3.274).29 In recent years, some studies have also shown that apoB/apoA-1 is associated with the severity of coronary artery disease,30,31 aortic valve stenosis,32 aortic stenosis,33 and poor prognosis of acute ischemic stroke.34 But few studies have investigated the relationship between apoB/apoA-1 and short-term prognosis in AMI patients, especially in this critical population of elderly AMI patients. Our findings suggest that apoB/apoA-1 is strongly associated with in-hospital mortality in elderly AMI patients. Other lipid parameters did not appear to be associated with outcome events in our study, and we considered that this may be related to the fact that most patients were taking lipid-lowering drugs chronically, thereby weakening the association of some common lipid parameters with outcome events, such as LDL-C and NHDL-C. In addition, it may also be related to the higher age of our enrolled patients, and previous studies have shown that the association between LDL-C, TC, TG and cardiovascular events is weakened by increasing patient age,11,35,36 perhaps because elderly AMI patients usually have other diseases, such as heart failure, renal insufficiency, diabetes, hypertension, etc., which are closely related to the risk of in-hospital death in elderly AMI patients. Of course, it may also be related to the relatively small number of patients who died during hospitalization in our study. Some previous studies have shown that apoB/apoA-1 is associated with atherosclerosis progression when it is > 0.74,37 and the results of the AMORIS study12 and INTERHEART study5 defined apoB/apoA-1 > 0.70 as a moderate risk of cardiovascular disease. Similarly, our RCS models suggest that the risk of in-hospital mortality in elderly AMI patients increases with increasing apoB/apoA-1 when apoB/apoA-1 is > 0.73. In conclusion, we believe that the association between apoB/apoA-1 and the risk of in-hospital death in elderly AMI patients may be due to the fact that apoB/apoA-1 represents a trend of atherosclerosis and anti-atherosclerosis in human body,11 and the process of atherosclerosis is always accompanied by the progression of inflammation.38–40 Therefore, high apoB/apoA-1 not only indicates the predominance of atherogenic factors in vivo, but may also indicate the enhancement of inflammatory response in vivo. Previous studies have also shown that certain inflammatory markers are significantly associated with in-hospital mortality in elderly patients with acute myocardial infarction.41–43 Of course, this hypothesis needs to be tested with larger samples. When we identify these high-risk patients through apoB/apoA-1, we can use some feasible measures to reduce their risk of death in clinical treatment, such as earlier revascularization, more refined care strategies, and the use of mechanical adjuvant therapy if necessary.13,44 In addition, apoB/apoA-1 can be measured and used in non-fasting conditions.45 We can measure apoB/apoA-1 as soon as possible after admission in patients with AMI to assess the risk of death during hospitalization. It is worth mentioning that some factors associated with PCI are closely related to the risk of in-hospital mortality in AMI patients, such as the incidence of perioperative complications,46 whether radial artery puncture is performed,47 the experience of the operator, and whether the puncture was performed through the radial artery.48 Whether adding the above factors can affect the association between apoB/apoA-1 and in-hospital death in elderly patients with AMI needs to be further explored in subsequent studies.
This study has the following limitations: First, it is a single-center study and its results may be influenced by patient selection bias. Second, we failed to obtain results on the long-term prognosis of patients discharged normally. Finally, case-control studies could not identify a causal relationship between apoB/apoA-1 and the risk of in-hospital mortality in elderly AMI patients.
Conclusion
Our findings suggest that apoB/apoA-1 is strongly associated with the risk of in-hospital mortality in older patients with AMI, but this association has not been found in other traditional lipid parameters. In addition, we found a linear dose-response relationship between apoB/apoA-1 and in-hospital mortality in elderly patients with AMI. As the apoB/apoA-1 ratio increases, the risk of in-hospital mortality also increases. Clinicians may consider using apoB/apoA-1 as risk stratification marker for elderly inpatients with AMI to better improve their short-term prognosis.
Patient Privacy Protection Statement
We desensitized all the data that can be used to identify patient personal information, such as their names, hospitalization ID and telephone numbers, to protect the privacy of patients.
Data Sharing Statement
The data that support the results of this study are available from the corresponding author upon reasonable request.
Statement of Ethics
The study protocol has been reviewed and approved by the Ethics Committee of the Second Hospital of Dalian Medical University. The need for informed consent was waived for the following reasons: (1) The purpose of the study was important; (2) The possible risk to patients was not higher than the minimum one; (3) The waiver of informed consent would not adversely affect the rights and health of patients; (4) The patients’ privacy and personal identity information were well protected. We have desensitized the patient ‘s personal identity to protect patient privacy. The protocol of the study is compliant with Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Pedersen F, Butrymovich V, Kelbæk H, et al. Short- and long-term cause of death in patients treated with primary PCI for STEMI. J Am Coll Cardiol. 2014;64(20):2101–2108. doi:10.1016/j.jacc.2014.08.037
2. Fokkema ML, James SK, Albertsson P, et al. Population trends in percutaneous coronary intervention: 20-year results from the SCAAR (Swedish coronary angiography and angioplasty registry). J Am Coll Cardiol. 2013;61(12):1222–1230. doi:10.1016/j.jacc.2013.01.007
3. Kristensen SD, Laut KG, Fajadet J, et al. Reperfusion therapy for ST elevation acute myocardial infarction 2010/2011: current status in 37 ESC countries. Eur Heart J. 2014;35(29):1957–1970. doi:10.1093/eurheartj/eht529
4. Ference BA, Ginsberg HN, Graham I, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European atherosclerosis society consensus panel. Eur Heart J. 2017;38(32):2459–2472. doi:10.1093/eurheartj/ehx144
5. McQueen MJ, Hawken S, Wang X, et al. Lipids, lipoproteins, and apolipoproteins as risk markers of myocardial infarction in 52 countries (the INTERHEART study): a case-control study. Lancet. 2008;372(9634):224–233. doi:10.1016/S0140-6736(08)61076-4
6. Steyn K, Sliwa K, Hawken S, et al. Risk factors associated with myocardial infarction in Africa: the INTERHEART Africa study. Circulation. 2005;112(23):3554–3561. doi:10.1161/CIRCULATIONAHA.105.563452
7. Langlois MR, Sniderman AD. Non-HDL cholesterol or apoB: which to Prefer As A Target For The Prevention Of Atherosclerotic Cardiovascular Disease? Curr Cardiol Rep. 2020;22(8):67. doi:10.1007/s11886-020-01323-z
8. de Nijs T, Sniderman A, de Graaf J. ApoB versus non-HDL-cholesterol: diagnosis and cardiovascular risk management. Crit Rev Clin Lab Sci. 2013;50(6):163–171. doi:10.3109/10408363.2013.847897
9. Carr SS, Hooper AJ, Sullivan DR, Burnett JR. Non-HDL-cholesterol and apolipoprotein B compared with LDL-cholesterol in atherosclerotic cardiovascular disease risk assessment. Pathology. 2019;51(2):148–154. doi:10.1016/j.pathol.2018.11.006
10. Schaefer EJ, Lamon-Fava S, Cohn SD, et al. Effects of age, gender, and menopausal status on plasma low density lipoprotein cholesterol and apolipoprotein B levels in the Framingham Offspring Study. J Lipid Res. 1994;35(5):779–792. doi:10.1016/S0022-2275(20)39173-2
11. Walldius G, Jungner I. The apoB/apoA-I ratio: a strong, new risk factor for cardiovascular disease and a target for lipid-lowering therapy--a review of the evidence. J Intern Med. 2006;259(5):493–519. doi:10.1111/j.1365-2796.2006.01643.x
12. Walldius G, Jungner I, Holme I, Aastveit AH, Kolar W, Steiner E. High apolipoprotein B, low apolipoprotein A-I, and improvement in the prediction of fatal myocardial infarction (AMORIS study): a prospective study. Lancet. 2001;358(9298):2026–2033. doi:10.1016/S0140-6736(01)07098-2
13. Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393
14. Collet JP, Thiele H, Barbato E, et al. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289–1367. doi:10.1093/eurheartj/ehaa575
15. Walldius G, Jungner I. Apolipoprotein B and apolipoprotein A-I: risk indicators of coronary heart disease and targets for lipid-modifying therapy. J Intern Med. 2004;255(2):188–205. doi:10.1046/j.1365-2796.2003.01276.x
16. Marcovina S, Packard CJ. Measurement and meaning of apolipoprotein AI and apolipoprotein B plasma levels. J Intern Med. 2006;259(5):437–446. doi:10.1111/j.1365-2796.2006.01648.x
17. Sniderman AD, Furberg CD, Keech A, et al. Apolipoproteins versus lipids as indices of coronary risk and as targets for statin treatment. Lancet. 2003;361(9359):777–780. doi:10.1016/S0140-6736(03)12663-3
18. Barter PJ, Ballantyne CM, Carmena R, et al. Apo B versus cholesterol in estimating cardiovascular risk and in guiding therapy: report of the thirty-person/ten-country panel. J Intern Med. 2006;259(3):247–258. doi:10.1111/j.1365-2796.2006.01616.x
19. Duran EK, Aday AW, Cook NR, Buring JE, Ridker PM, Pradhan AD. Triglyceride-rich lipoprotein cholesterol, small dense LDL cholesterol, and incident cardiovascular disease. J Am Coll Cardiol. 2020;75(17):2122–2135. doi:10.1016/j.jacc.2020.02.059
20. Li J, Wang W, Han L, et al. Human apolipoprotein A-I exerts a prophylactic effect on high-fat diet-induced atherosclerosis via inflammation inhibition in a rabbit model. Acta Biochim Biophys Sin. 2017;49(2):149–158. doi:10.1093/abbs/gmw128
21. Yui Y, Aoyama T, Morishita H, Takahashi M, Takatsu Y, Kawai C. Serum prostacyclin stabilizing factor is identical to apolipoprotein A-I (Apo A-I). A novel function of Apo A-I. J Clin Invest. 1988;82(3):803–807. doi:10.1172/JCI113682
22. Patel S, Di Bartolo BA, Nakhla S, et al. Anti-inflammatory effects of apolipoprotein A-I in the rabbit. Atherosclerosis. 2010;212(2):392–397. doi:10.1016/j.atherosclerosis.2010.05.035
23. Walldius G, de Faire U, Alfredsson L, et al. Long-term risk of a major cardiovascular event by apoB, apoA-1, and the apoB/apoA-1 ratio-experience from the Swedish AMORIS cohort: a cohort study. PLoS Med. 2021;18(12):e1003853. doi:10.1371/journal.pmed.1003853
24. Goswami B, Rajappa M, Mallika V, Kumar S, Shukla DK. Apo-B/apo-AI ratio: a better discriminator of coronary artery disease risk than other conventional lipid ratios in Indian patients with acute myocardial infarction. Acta Cardiol. 2008;63(6):749–755. doi:10.2143/AC.63.6.2033393
25. Dunder K, Lind L, Zethelius B, Berglund L, Lithell H. Evaluation of a scoring scheme, including proinsulin and the apolipoprotein B/apolipoprotein A1 ratio, for the risk of acute coronary events in middle-aged men: Uppsala Longitudinal Study of Adult Men (ULSAM). Am Heart J. 2004;148(4):596–601. doi:10.1016/j.ahj.2004.03.021
26. van der Steeg WA, Boekholdt SM, Stein EA, et al. Role of the apolipoprotein B-apolipoprotein A-I ratio in cardiovascular risk assessment: a case-control analysis in EPIC-Norfolk. Ann Intern Med. 2007;146(9):640–648. doi:10.7326/0003-4819-146-9-200705010-00007
27. Meisinger C, Loewel H, Mraz W, Koenig W. Prognostic value of apolipoprotein B and A-I in the prediction of myocardial infarction in middle-aged men and women: results from the MONICA/KORA Augsburg cohort study. Eur Heart J. 2005;26(3):271–278. doi:10.1093/eurheartj/ehi003
28. Cremer P, Nagel D, Mann H, et al. Ten-year follow-up results from the Goettingen Risk, Incidence and Prevalence Study (GRIPS). I. Risk factors for myocardial infarction in a cohort of 5790 men. Atherosclerosis. 1997;129(2):221–230. doi:10.1016/S0021-9150(96)06030-3
29. Li T, Yuan D, Wang P, et al. Associations of lipid measures with total occlusion in patients with established coronary artery disease: a cross-sectional study. Lipids Health Dis. 2022;21(1):118. doi:10.1186/s12944-022-01733-8
30. Song Y, Yang Y, Zhang J, et al. The apoB100/apoAI ratio is independently associated with the severity of coronary heart disease: a cross sectional study in patients undergoing coronary angiography. Lipids Health Dis. 2015;14(1):150. doi:10.1186/s12944-015-0155-6
31. Yaseen RI, El-Leboudy MH, El-Deeb HM. The relation between ApoB/ApoA-1 ratio and the severity of coronary artery disease in patients with acute coronary syndrome. Egypt Heart J. 2021;73(1):24. doi:10.1186/s43044-021-00150-z
32. Zheng KH, Arsenault BJ, Kaiser Y, et al. apoB/apoA-I ratio and Lp(a) associations with aortic valve stenosis incidence: insights from the EPIC-Norfolk prospective population study. J Am Heart Assoc. 2019;8(16):e013020. doi:10.1161/JAHA.119.013020
33. Ivert T, Hammar N, Talbäck M, Malmström H, Leander K, Walldius G. Elevated Apolipoprotein B/A-1 ratio is associated with an increased risk of aortic stenosis: experience from the AMORIS cohort. Heart Lung Circ. 2021;30(7):1050–1057. doi:10.1016/j.hlc.2020.12.005
34. Li Z, Zhang D, Song Z, et al. Elevated ApoB/ApoA-Ι ratio is associated with poor outcome in acute ischemic stroke. J Clin Neurosci. 2023;107:138–143. doi:10.1016/j.jocn.2022.11.007
35. Parish S, Peto R, Palmer A, et al. The joint effects of apolipoprotein B, apolipoprotein A1, LDL cholesterol, and HDL cholesterol on risk: 3510 cases of acute myocardial infarction and 9805 controls. Eur Heart J. 2009;30(17):2137–2146. doi:10.1093/eurheartj/ehp221
36. Shipley MJ, Pocock SJ, Marmot MG. Does plasma cholesterol concentration predict mortality from coronary heart disease in elderly people? 18 year follow up in Whitehall study. BMJ. 1991;303(6794):89–92. doi:10.1136/bmj.303.6794.89
37. Wallenfeldt K, Bokemark L, Wikstrand J, Hulthe J, Fagerberg B. Apolipoprotein B/apolipoprotein A-I in relation to the metabolic syndrome and change in carotid artery intima-media thickness during 3 years in middle-aged men. Stroke. 2004;35(10):2248–2252. doi:10.1161/01.STR.0000140629.65145.3c
38. Ginsberg HN, Packard CJ, Chapman MJ, et al. Triglyceride-rich lipoproteins and their remnants: metabolic insights, role in atherosclerotic cardiovascular disease, and emerging therapeutic strategies-a consensus statement from the European Atherosclerosis Society. Eur Heart J. 2021;42(47):4791–4806. doi:10.1093/eurheartj/ehab551
39. Webb RJ, Mazidi M, Lip GYH, Kengne AP, Banach M, Davies IG. The role of adiposity, diet and inflammation on the discordance between LDL-C and apolipoprotein B. Nutr Metab Cardiovasc Dis. 2022;32(3):605–615. doi:10.1016/j.numecd.2021.12.004
40. Varbo A, Benn M, Tybjærg-Hansen A, Nordestgaard BG. Elevated remnant cholesterol causes both low-grade inflammation and ischemic heart disease, whereas elevated low-density lipoprotein cholesterol causes ischemic heart disease without inflammation. Circulation. 2013;128(12):1298–1309. doi:10.1161/CIRCULATIONAHA.113.003008
41. Li L, Ma Y, Geng XB, et al. Platelet-to-lymphocyte ratio relates to poor prognosis in elderly patients with acute myocardial infarction. Aging Clin Exp Res. 2021;33(3):619–624. doi:10.1007/s40520-020-01555-7
42. Ji Z, Liu G, Guo J, et al. The neutrophil-to-lymphocyte ratio is an important indicator predicting in-hospital death in AMI patients. Front Cardiovasc Med. 2021;8:706852. doi:10.3389/fcvm.2021.706852
43. Chen Y, Chen S, Han Y, Xu Q, Zhao X. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio are important indicators for predicting in-hospital death in elderly AMI patients. J Inflamm Res. 2023;16:2051–2061. doi:10.2147/JIR.S411086
44. Gheeraert PJ, De Buyzere ML, Taeymans YM, et al. Risk factors for primary ventricular fibrillation during acute myocardial infarction: a systematic review and meta-analysis. Eur Heart J. 2006;27(21):2499–2510. doi:10.1093/eurheartj/ehl218
45. Nordestgaard BG, Langlois MR, Langsted A, et al. Quantifying atherogenic lipoproteins for lipid-lowering strategies: consensus-based recommendations from EAS and EFLM. Atherosclerosis. 2020;294:46–61. doi:10.1016/j.atherosclerosis.2019.12.005
46. Rakowski T, Węgiel M, Siudak Z, et al. Prevalence and predictors of coronary artery perforation during percutaneous coronary interventions (from the ORPKI National Registry in Poland). Am J Cardiol. 2019;124(8):1186–1189. doi:10.1016/j.amjcard.2019.07.021
47. Zabojszcz M, Januszek R, Siudak Z, et al. Association between the mortality rate and operator volume in patients undergoing emergency or elective percutaneous coronary interventions. Kardiol Pol. 2020;78(2):138–146. doi:10.33963/KP.15123
48. Tokarek T, Dziewierz A, Plens K, et al. Percutaneous coronary intervention during on- and off-hours in patients with ST-segment elevation myocardial infarction. Hell J Cardiol. 2021;62(3):212–218. doi:10.1016/j.hjc.2021.01.011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.