Back to Journals » International Journal of General Medicine » Volume 17
Elevated Activated Partial Thromboplastin Time as a Predictor of 28-Day Mortality in Sepsis-Associated Acute Kidney Injury: A Retrospective Cohort Analysis
Authors Lin C ![]() , Wang J
, Wang J ![]() , Cai K
, Cai K ![]() , Luo Y, Wu W
, Luo Y, Wu W ![]() , Lin S
, Lin S ![]() , Lin Z, Feng S
, Lin Z, Feng S ![]()
Received 14 January 2024
Accepted for publication 21 April 2024
Published 30 April 2024 Volume 2024:17 Pages 1739—1753
DOI https://doi.org/10.2147/IJGM.S459583
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor David E. Stec
Chen Lin,1 Jing Wang,2 Kexin Cai,2 Yuqing Luo,2 Wensi Wu,1 Siming Lin,2 Zhihong Lin,2 Shaodan Feng2
1Department of Emergency, The Third Affiliated People’s Hospital, Fujian University of Traditional Chinese Medicine, Fuzhou, 350108, People’s Republic of China; 2Department of Emergency, The First Affiliated Hospital, Fujian Medical University, Fuzhou, 350005, People’s Republic of China
Correspondence: Zhihong Lin; Shaodan Feng, Department of Emergency, The First Affiliated Hospital, Fujian Medical University, Fuzhou, 350005, People’s Republic of China, Tel +86 59187981975, Email [email protected]; [email protected]
Purpose: To address the critical mortality rates among sepsis-associated acute kidney injury (SA-AKI) patients, early prognosis is vital. This study investigates the relationship between coagulation indices and the 28-day mortality rate in patients with SA-AKI.
Patients and Methods: This study was a retrospective cohort analysis including patients with SA-AKI admitted to the First Hospital of Fujian Medical University as a training cohort (n = 119) and patients admitted to the Third People’s Hospital of Fujian University of Traditional Chinese Medicine as a validation cohort (n = 51). We examined the relationship between coagulation indices and 28-day mortality in SA-AKI, the cumulative mortality at different activated partial thromboplastin time (APTT) levels, and the nonlinear relationship between APTT and 28-day mortality. Receiver operating characteristic curves were plotted, and the area under the curve was calculated to assess the predictive power of APTT. Finally, subgroup analyses were performed to assess the robustness of the association.
Results: Overall, 119 participants with a mean±standard deviation age of 70.47± 15.20 years were included in the training cohort: 54 died, 65 survived. According to univariate and multivariate COX regression analyses, APACHE II score, CRP level, Lac level, and APTT level were independent risk factors for 28-day adverse prognosis. After controlling for some variables, an elevated baseline APTT (≥ 37.7 s) was associated with an elevated risk of 28-day mortality (HR, 1.017; 95% CI, 1.001– 1.032), and Kaplan–Meier analyses further confirmed the increased mortality in the group with a higher APTT. The same results were shown when the validation cohort was analyzed (HR, 1.024; 95% CI, 0.958– 1.096). Subgroup analyses showed the stability of the association between APTT and poor prognosis in SA-AKI.
Conclusion: In essence, APTT elevation is synonymous with increased 28-day mortality rates, indicating a poor prognosis in SA-AKI scenarios.
Keywords: APTT, prognosis, retrospective studies, critical illness
Introduction
Sepsis, a life-threatening condition arising from a dysregulated host response to infection, is predominant in inducing mortality in patients with severe trauma, burns, shock, or those undergoing major surgery.1 Representing a prevalent cause of morbidity and mortality, it significantly impacts patients in emergency departments and intensive care units (ICU).2 A frequent complication of sepsis is acute kidney injury (AKI),3,4 with the kidney being notably susceptible, displaying a prevalence of approximately 11–31% in septic conditions.5 This susceptibility is closely linked with the patients’ short-term prognosis.6 Sepsis-associated AKI (SA-AKI), a variant of AKI, compounds morbidity and mortality rates, especially in critically ill patients,7 and its advancement escalates the risk of developing chronic kidney disease (CKD), necessitating renal replacement therapy (RRT).8
Numerous clinical investigations9,10 into the etiology of SA-AKI have been conducted, yet a consensus on its underlying causes remains elusive. However, a constellation of mechanisms is posited to drive the progression of AKI in patients with sepsis. These mechanisms encompass an excessive inflammatory response, changes in autophagic flux, and changes in complement system activation, programmed cell death pathways, and the development of microcirculatory disruptions.11–13 This complex progression of AKI within the septic milieu contributes to the challenges associated with the clinical diagnosis of AKI, compounded by the inherent difficulties in delineating the specific pathophysiological trajectory of SA-AKI. This is further complicated by the absence of a clearly defined pathogenetic sequence linking sepsis to AKI, making the elucidation of these mechanisms predominantly reliant on insights gleaned from animal models.7
Research reveals that patients with SA-AKI exhibit elevated organ function scores, increased mortality rates, and an increased need for vasoactive drugs and respiratory support, alongside inflated hospitalization expenses, compared to those with sepsis alone.14,15 The contemporary therapeutic landscape lacks advanced ameliorative strategies for sepsis-related AKI, with interventions predominantly aimed at mitigating exposure to renal injury factors, enhancing renal microcirculation, managing primary infection foci, and optimizing fluid loading. Consequently, the early identification of patients with SA-AKI and an unfavorable prognosis is imperative.16 Nonetheless, numerous elements interplay in dictating the intricate pathogenesis, prognosis, and eventual clinical outcomes of SA-AKI.17–19 Early prediction of disease severity and prognosis through initial clinical manifestations and test markers enables early interventions, mitigating mortality rates.20
It has been discerned that coagulation dysfunction is integral in the progression of sepsis and AKI, underlining its significant role in SA-AKI.21–23 The ambiguity surrounding the correlation of coagulation indices with short-term prognosis and clinical outcomes necessitates the execution of this retrospective cohort study, aimed at elucidating the association between coagulation indices and 28-day mortality rate in patients with SA-AKI.
Materials and Methods
Study Design and Patient Selection
Clinical data from patients with sepsis admitted to the ICUs of the First Hospital Affiliated to Fujian Medical University and the Third People’s Hospital Affiliated to Fujian University of Traditional Chinese Medicine from January 2019 to December 2021 and from January 2019 to December 2022 were collected for a retrospective cohort study. Anonymized clinical data were obtained from the electronic medical records systems of both organizations. Upon admission, there were 276 patients in the First Hospital Affiliated to Fujian Medical University and 106 patients in the Third People’s Hospital Affiliated to Fujian University of Traditional Chinese Medicine were diagnosed with sepsis according to the definition of Sepsis-3.0 (Figure 1).1 During their hospital stay, the diagnosis of AKI was made using the Kidney Diseases Improving Overall Prognosis (KDIGO) criteria:24 The reference (baseline) serum creatinine (SCr) level was defined as the lower value between (1) the median of the inpatient and outpatient SCr measurements during the previous 12 months and (2) the first SCr measurement during the qualifying hospitalization.25 Patients older than 18 years were also included in this study. Patients were excluded according to the following criteria: (1) hospitalized for less than 24 hours; (2) history of hemodialysis prior to admission; (3) previous CKD; (4) previous kidney transplant; (5) use of nephrotoxic drugs; (6) presence of diseases that may affect coagulation, such as malignant tumors, hematologic diseases, and autoimmune diseases; (7) presence of acute or chronic liver failure; (8) undergoing anticoagulation therapy; (9) pregnant and lactating women.
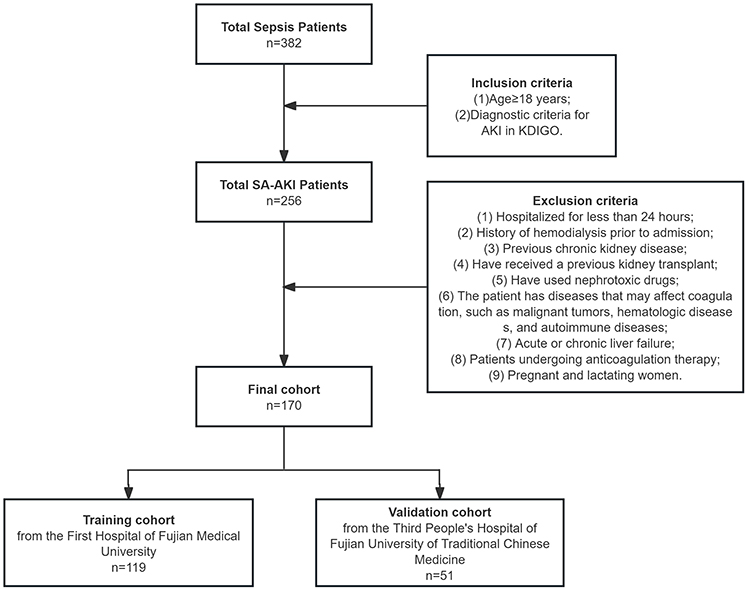 |
Figure 1 Flow diagram of patient enrolment. |
In accordance with the ethical guidelines and standards outlined in the Declaration of Helsinki, we hereby confirm that our study fully complies with these principles. The ethics committee of the First Affiliated Hospital of Fujian Medical University approved this study, and the ethics committee provided the ethical approval (Approval No.: Min Medical University Attached Ethics Medical Research [2022] 244). This study was approved by the ethics committee of the Third People’s Hospital affiliated with Fujian University of Traditional Chinese Medicine (Approval No.: 2024KS-56-1). The ethics committee approved a waiver of consent from the patients because the study did not include any therapeutic intervention and the plan was to conduct a retrospective study of SA-AKI patients.
Diagnostic Criteria
We employed the KDIGO criteria to define AKI cases as follows:1 (1) an increase in SCr level by ≥ 0.3 mg/dL (≥ 26.5 µmol/L) within 48 h; or (2) an increase in SCr level to ≥ 1.5 times the baseline level, which is known or presumed to have occurred within the previous 7 days; or (3) a urine volume < 0.5 mL/kg/h for 6 h. Moreover, AKI was classified into three stages: Stage 1, SCr level increased to 26.5 µmol/L or increased by 1.5–1.9 times the baseline level, or a urine volume < 0.5 mL/(kg/h) lasting for 6–12 h; Stage 2, SCr level increased by 2–2.9 times the baseline level or a urine volume < 0.5 mL/(kg/h), lasting > 12 h; Stage 3, SCr level increased by > 3 times the baseline level or increased to 354 µmol/L or RRT was required. The diagnostic criteria for disseminated intravascular coagulation (DIC), as established by the International Society on Thrombosis and Hemostasis, rely on a scoring system that considers the following parameters: (1) platelet count (PLT); (2) D-dimer or fibrin degradation product; (3) prothrombin time (PT); and (4) fibrin. A score of ≥ 5 is indicative of overt DIC.26 For the early detection of patients with concurrent sepsis and DIC, the sepsis-induced coagulopathy (SIC) scoring system was introduced in 2017 (Table S1).27 Patients with a SIC score of ≥ 4 have an elevated risk of overt DIC. Abnormal coagulation parameters were defined as: (1) PLT < 100.00×10^9/L; (2) thrombin time (TT) > 15.00 s; (3) PT > 15.00 s; and (4) activated partial thromboplastin time (APTT) > 40.00 s. Multiple organ dysfunction syndrome (MODS) was described as the acute, potentially reversible dysfunction of two or more organ systems.28
Relevant Variables and Study Endpoints
We first included 119 cases from the First Affiliated Hospital of Fujian Medical University as a test set and 51 cases from the Third People’s Hospital of Fujian University of Traditional Chinese Medicine as a validation set. Then, we considered multiple categories of variables: (1) demographic and admission data, which covered age, sex, AKI stage, pathogen status, and admission score; (2) clinical events, which comprised septic shock, abnormal coagulation parameters, MODS, SIC, and DIC; (3) the evaluation of a patient’s condition upon admission was gauged using the Sequential Organ Failure Assessment (SOFA) and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores; (4) sites of infection were identified as the lungs, abdominal cavity, urinary tract, soft tissues of the skin, and bloodstream; (5) underlying health conditions considered were hypertension, diabetes, and malignant cancer; (6) infectious agents documented included gram-negative bacteria, fungi, and noninfectious organisms; (7) medical interventions applied were RRT, vasoactive drugs, and mechanical ventilation; and (8) laboratory parameters recorded at the time of SA-AKI diagnosis consisted of PLT, C-reactive protein (CRP), procalcitonin, total bilirubin (TBIL), direct bilirubin (DBIL), alanine aminotransferase (ALT), alanine transaminase (AST), urea, SCr, N-terminal brain natriuretic peptide precursor, D-dimer, PT, APTT, TT, fibrinogen, and international normalized ratio (INR). When a patient’s results for multiple parameters were available within 24 hours of admission, the earliest dataset was prioritized. The primary endpoint of our research was the 28-day mortality rate.
Statistical Analysis
For our analysis, various methods were employed based on the nature of the data: (1) all continuous measures underwent normality tests; normally distributed data were denoted as mean ± standard deviation, while non-normally distributed data were indicated as median and interquartile range. Counts were represented as frequency (n) and percentage (%); (2) one-way analysis of variance or t-tests were used to analyze normally distributed continuous variables, aiming to discern differences between groups; (3) the Kruskal–Wallis test was used for non-normally distributed continuous variables, while the chi-square test was used for categorical data; (4) to assess the correlations between demographics, admission procedures, laboratory outcomes, and the 28-day mortality rate, a univariate Cox proportional risk model was employed; (5) further, a multivariate Cox proportional hazards model was crafted through stepwise regression analysis to inspect the relationship between APTT and 28-day mortality rate, with its predictive potency gauged using the area under the curve (AUC); (6) survival probabilities across diverse APTT level groups were juxtaposed using Kaplan–Meier curves; and (7) stratified and interaction assessments were performed, focusing on various factors such as sex, age, patterns of use of RRT, vasoactive drugs, mechanical ventilation, and conditions such as septic shock, blood clotting anomalies, alongside stages of DIC, SIC, and AKI.
In our dataset, less than 5% of the covariates exhibited missing entries. Given the low proportion of missing data, no imputations were deemed necessary. All subsequent analyses were performed using R software and SPSS Statistics, version 26.0 (IBM Corp., Armonk, NY, USA), and P values below 0.05 were considered statistically significant.
Results
Population Characteristics
Of the 276 individuals meeting the Sepsis-3 criteria upon initial admission, 119 eligible patients with SA-AKI with complete follow-up information were included in the 28-day prognostic cohort study, and these patients were included in the training cohort. Table 1 summarizes the characteristics of these patients. Based on a 28-day survival analysis, 65 patients (54.62%) were in the survival group, and 54 (45.38%) in the death group, leading to a 28-day mortality rate of 45.38% (54/119). The cohort comprised 72 males (60.50%) and 47 females (39.50%), resulting in a male-to-female ratio of 1.53:1. Their age ranged from 27 to 95 years with an average of 70.47 ± 15.20 years. The primary sites of infection were the lungs (62.18%), abdominal cavity (20.17%), urinary tract (23.53%), skin and soft tissue (5.88%), hematologic (12.60%), and simultaneous infections at two or more sites (25.21%). Pathogens identified were gram-negative bacteria (65.55%), gram-positive bacteria (21.85%), fungal infections (25.21%); in 30 cases (25.21%), no infectious organisms were detected.
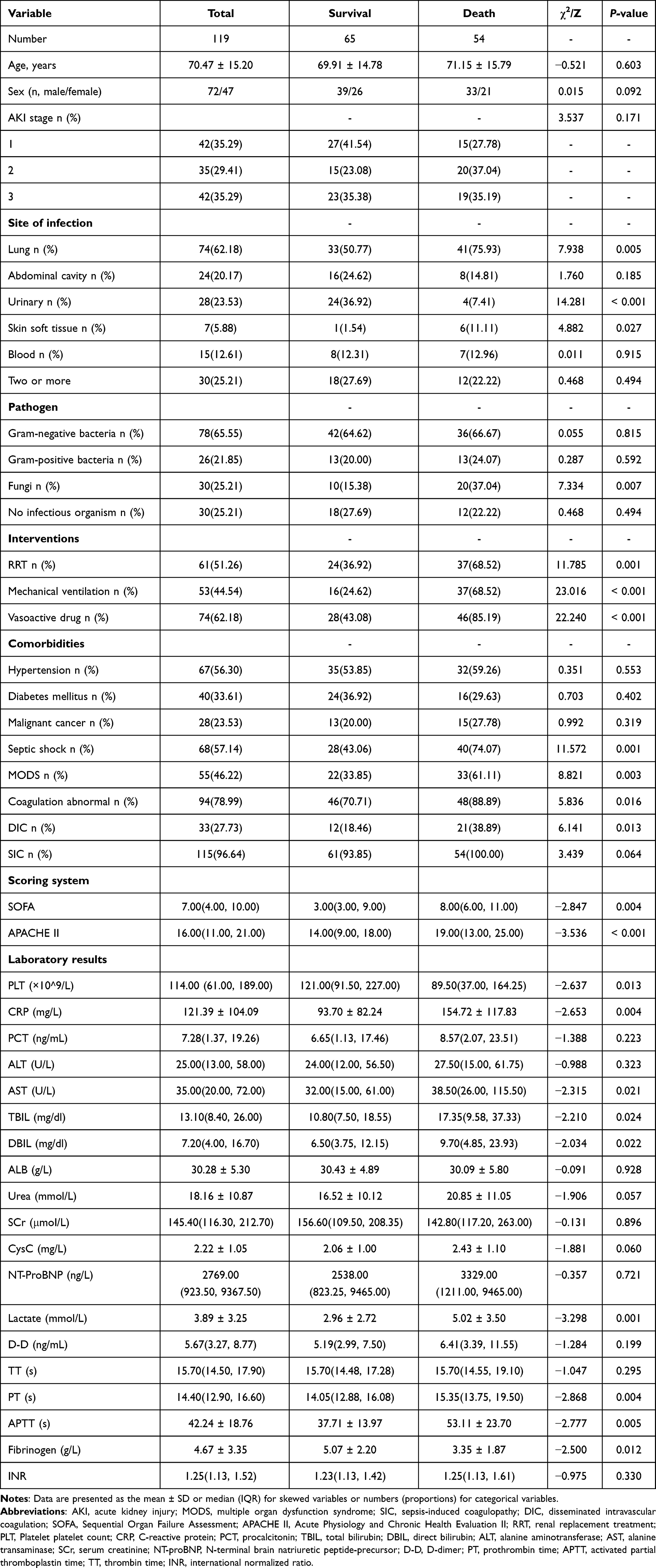 |
Table 1 Baseline Characteristics of the Participants and Outcome Parameters |
In terms of clinical treatment, usage rates for RRT, mechanical ventilation, and vasoactive drugs were higher in the death group than in the survival group. Simultaneously, the death group exhibited a higher incidence of septic shock, coagulation abnormalities, DIC, and MODS than did the survival group (P < 0.05). The SOFA and APACHE II scores in the death group were higher than those in the survival group (P < 0.01). In the death group, markers including CRP, AST, TBIL, DBIL, lactate, PT, and APTT levels were higher, while PLT and fibrinogen levels were lower than those in the survival group (P < 0.05).
In the validation cohort, we selected 51 patients with SA-AKI who were eligible and had complete follow-up information to be included out of 106 patients who met the Sepsis-3 criteria on admission. Comparing the training cohort with the validation cohort, there was a statistical difference only between a history of concomitant hypertension and serum lactate levels (P < 0.05; Table S2).
Cox Regression Analysis
After comparing the death group with the survival group and selecting for P values < 0.05, sex and age underwent univariate Cox regression analysis. The analysis revealed that RRT usage (hazard ratio [HR] = 0.547, 95% CI 0.320–0.935, P = 0.027), mechanical ventilation (HR = 3.382, 95% CI 1.898–6.027, P < 0.001), vasoactive drug usage (HR = 4.459, 95% CI 2.097–9.479, P < 0.001), and the laboratory parameters PLT (HR = 0.996, 95% CI 0.992–0.999, P = 0.028), PT (HR = 1.034, 95% CI 1.006–1.061, P = 0.015), and APTT (HR = 1.019, 95% CI 1.007–1.031, P = 0.002) were risk factors influencing 28-day mortality in SA-AKI patients. When univariate cox regression analyses were performed for pathogen classification, a negative correlation was found between only undetected pathogens and a 28-day prognosis (Table S3). When these risk factors were further analyzed using multivariate Cox stepwise regression, it was found that APACHE II (HR = 1.047, 95% CI 1.003–1.093, P = 0.036), CRP (HR = 0.008, 95% CI 1.001–1.007, P = 0.010), Lac (HR = 1.107, 95% CI 1.022–1.198, P = 0.012), and APTT (HR = 1.022, 95% CI 1.006–1.038, P = 0.007) were independent risk factors for 28-day mortality in SA-AKI patients. The findings are detailed in Table 2. A multivariate model of APTT was constructed, with the initial model being unadjusted. Model 1 was adjusted for Lac level, APACHE II score, and CRP level. In the initial model, the HR and 95% CI for both low and high APTT groups were 1.023 (0.940–1.113) and 1.017 (1.001–1.032), respectively. Upon adjustment in Model 1, these values shifted to 0.999 (0.917–1.088) and 1.030 (1.009–1.050), respectively, as shown in (Table S4).
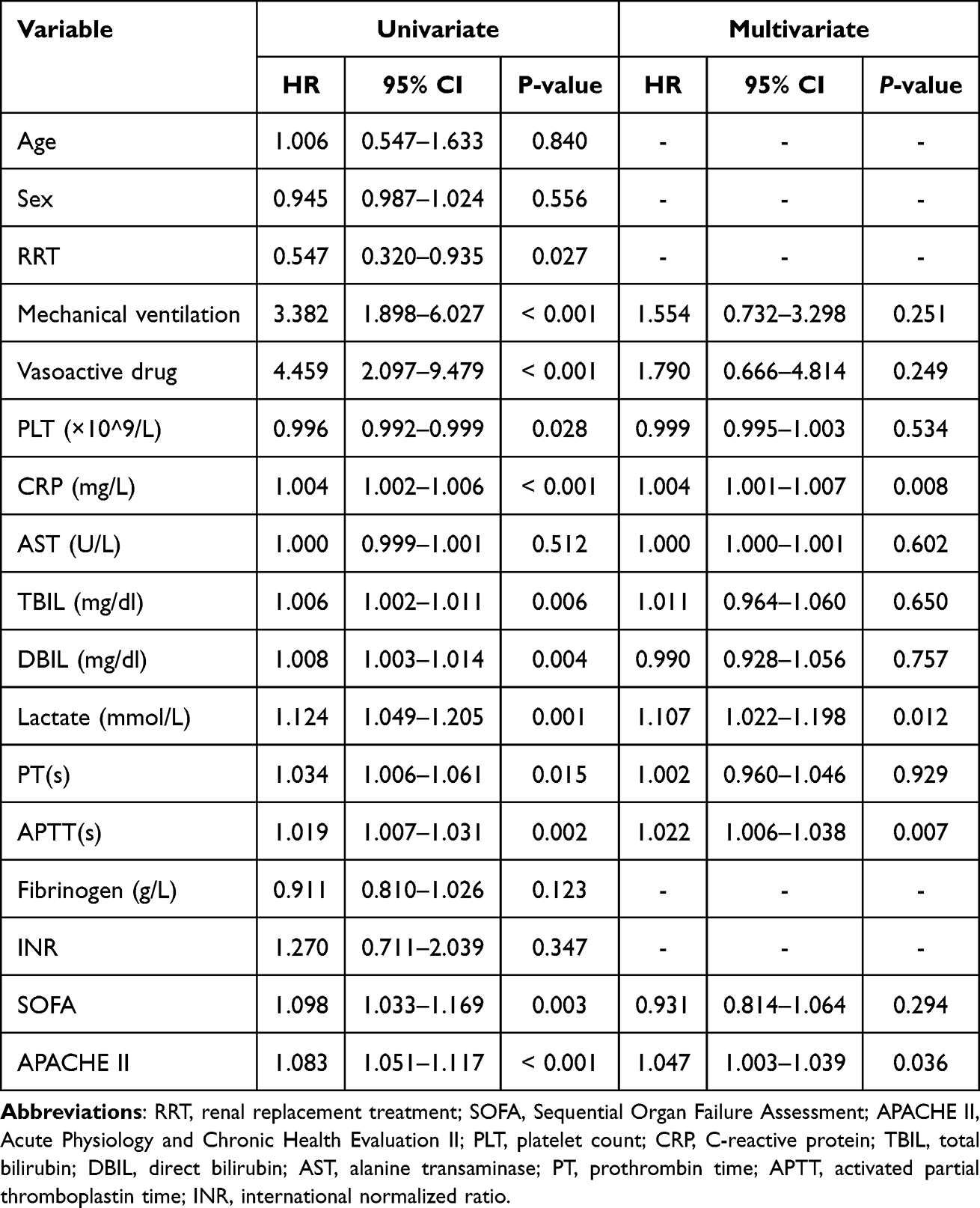 |
Table 2 Cox Analysis of Risk Factors for 28-Day Mortality in Patients with SA-AKI |
APTT and 28-Day Mortality
In the training cohort, a restriction cubic spline (RCS) analysis revealed a nonlinear relationship between APTT (log2) and the 28-day mortality rate. For APTT levels below 37.7 s, the risk of death remained consistent. However, for APTT values of 37.7 s and above, the risk of death increased concurrently with the APTT levels (Figure 2A). The results were similar in the validation cohort, except that this turning point occurred at an APTT level of 38.8 s (Figure 2B).
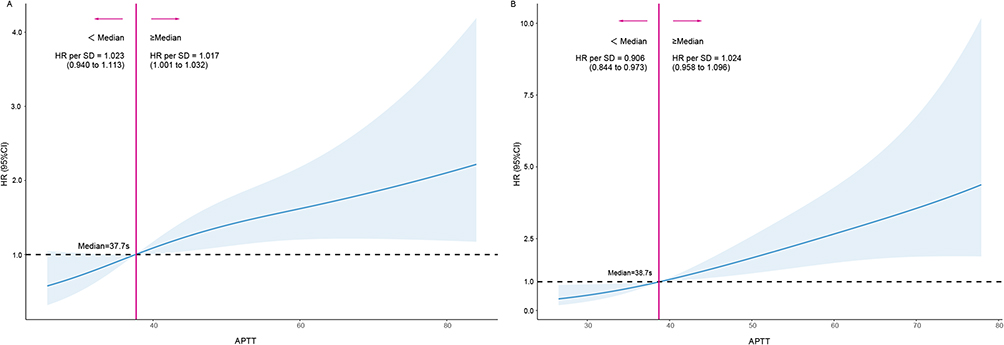 |
Figure 2 Restriction cubic spline (RSC) analysis of the association between log-transformed APTT and 28-day mortality. (A) RCS curves in the training cohort. The HR of the median was used as baseline, 37.7 s for log-transformed activated partial thromboplastin time (APTT). (B) RCS curves in the validation cohort. The HR of the median was used as baseline, 37.7 s for log-transformed APTT. Hazard ratios are indicated by solid lines and 95% CIs by shaded areas. |
To analyze the cumulative survival in-depth, we divided the patients in both the training and validation cohorts into two groups based on the median APTT value (37.7 seconds): a high-APTT group (≥ 37.7 seconds) and a low-APTT group (< 37.7 seconds). Kaplan–Meier survival curves showed that the 28-day cumulative survival rates in the training cohort were 42.11% and 66.13% for the high-APTT and low-APTT groups, respectively. Notably, high APTT was associated with decreased 28-day survival, which decreased further with increasing APTT (Log-rank2 = 4.7, P = 0.012, Figure 3A). We observed the same pattern in the validation cohort (Log-rank2 = 10.81, P = 0.001, Figure 3B).
 |
Figure 3 Kaplan–Meier survival curve for activated partial thromboplastin time (APTT). Kaplan–Meier analysis was performed to compare the 28-day survival (overall survival [OS]) rate between the high- and low-APTT groups using p-values from the Log rank test. (A) Kaplan–Meier survival curve in the training cohort. High APTT was associated with poor prognosis (P = 0.012). (B) Kaplan–Meier survival curve in the validation cohort. High APTT was associated with poor prognosis (P = 0.001). |
We plotted a 3D bar chart to visualize the relationship between APTT levels and 28-day mortality (Figure 4). Patients were divided into four equal parts: Q1: APTT ≤ 31.0 s; Q2: 31.0 s < APTT ≤ 37.7 s; Q3: 37.7 s < APTT ≤ 47.7 s; and Q4: APTT > 47.7 s. In the training cohort, the 28-day mortality rates from Q1 to Q4 were 28.1%, 40.0%, 51.7%, and 64.3%, respectively. In the validation cohort, these were 44.4%, 46.4%, 66.7%, and 93.3%, respectively.
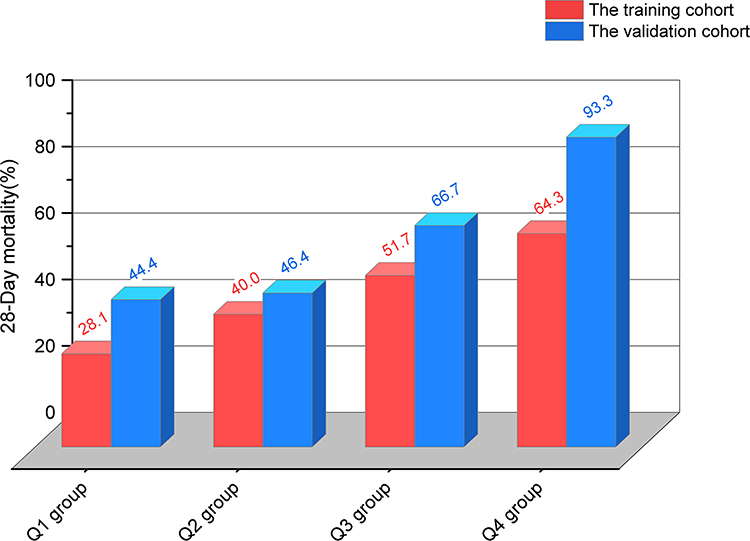 |
Figure 4 3D bar chart of activated partial thromboplastin time (APTT) and 28-day mortality. Q1 group: APTT ≤ 31.0 s; Q2 group: 31.0 s < APTT ≤ 37.7 s; Q3 group: 37.7 s < APTT ≤ 47.7 s; and Q4 group: APTT > 47.7 s. In the training cohort, the 28-day mortality rates were as follows: Q1 group: 28.1%, Q2 group: 40.0%, Q3 group: 51.7%, Q4 group: 64.3%. In the validation cohort, the 28-day mortality rates were as follows: Q1 group: 44.4%, Q2 group: 46.4%, Q3 group: 66.7%, Q4 group: 93.3%. |
Receiver Operating Characteristic Curve
Receiver operating characteristic (ROC) curves for APTT and Model 1 were constructed to predict mortality in patients with SA-AKI (Figure 5). The AUC for APTT was 0.675 (95% CI 0.566–0.784), while for Model 1, it was 0.774 (95% CI 0.684–0.866). The sensitivity rates for APTT and Model 1 were 53.3% and 62.2%, respectively, and both showed a specificity of 81.1%. We also tested the ability of APTT and Model 1 to predict mortality in patients with SA-AKI in the validation cohort. The AUC for APTT stood at 0.675 (95% CI, 0.566–0.784); for Model 1, the AUC was notably higher at 0.774 (95% CI 0.684–0.866). The sensitivity and specificity were 61.8% and 82.4% for APTT and 67.6% and 94.1% for Model 1, respectively.
 |
Figure 5 Restriction cubic spline (RSC) curves for predicting 28-day mortality in the training and validation cohorts. (A) ROC curves for activated partial thromboplastin time (APTT) and Model 1 in the training cohort. (B) ROC curves for APTT and Model 1 in the validation cohort. Variables included in model 1: APACHE II score, c-reactive protein (CRP), procalcitonin (PCT), platelet count (PLT), and D-dimer levels. |
Subgroup Analysis
Table 3 shows the correlation between APTT and 28-day mortality across different patient statuses. An interaction was found between RRT usage and sepsis-related coagulation dysfunction (P < 0.05). However, other subgroups revealed no significant interactions (P < 0.05). Among patients with stage 2 AKI, the predictive power of APTT for 28-day mortality was less robust than among patients with stages 1 and 3 AKI. The HRs for stages 1, 2, and 3 AKI were 1.018 (95% CI 1.002–1.035, P < 0.05), 1.008 (95% CI 0.970–1.047, P = 0.088), and 1.026 (95% CI 1.003–1.049, P < 0.05), respectively.
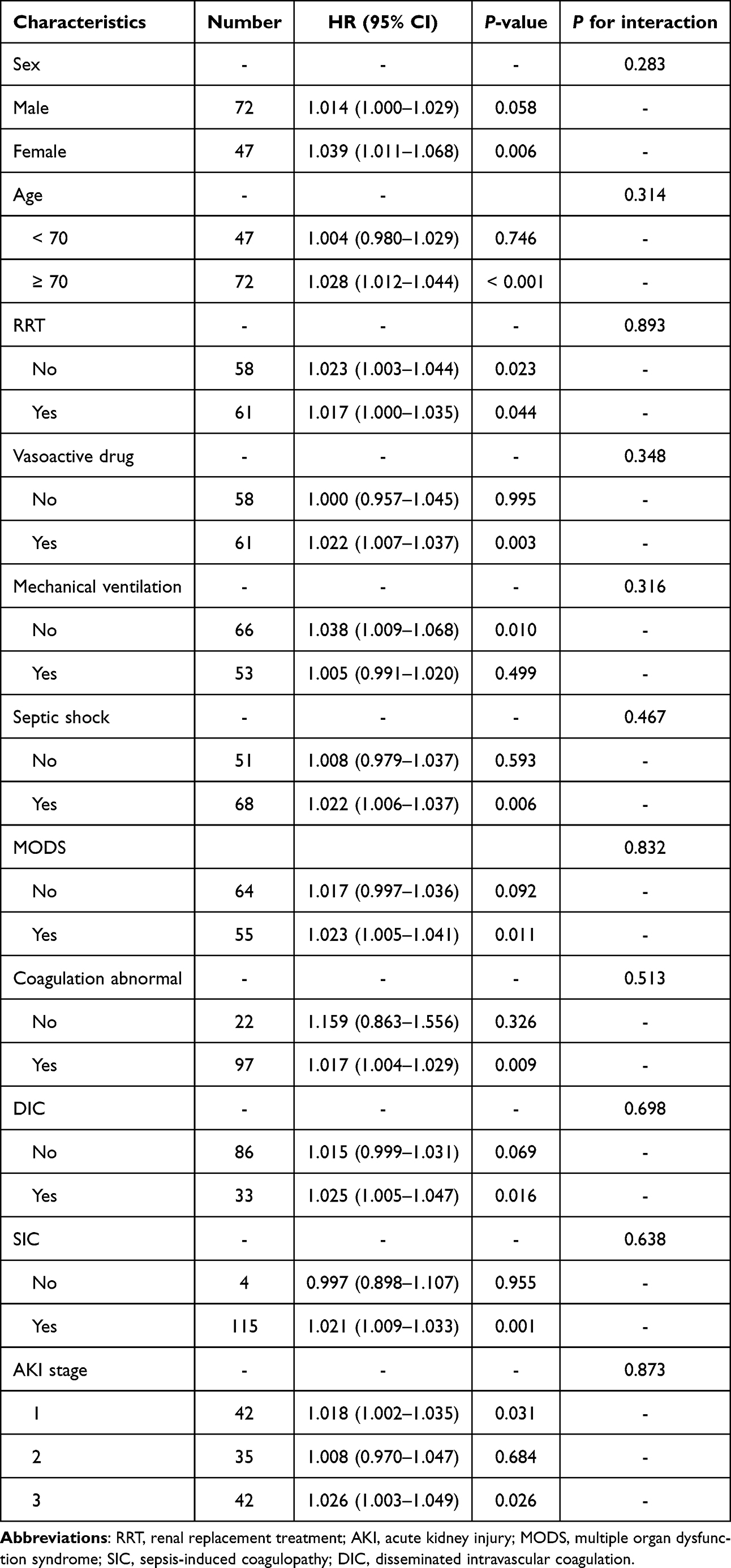 |
Table 3 Subgroup Analysis of the Association Between APTT and 28-Day Mortality |
Discussion
Sepsis can affect multiple body organs due to its rapid onset and swift progression. AKI has been observed in approximately 31.2% to 70.0% of sepsis patients,29,30 and this condition also stands as an independent risk factor for death in these individuals, imposing a significant economic strain on patients and their families. Existing research31–33 has documented an overall mortality rate of 30% to 70% in patients with sepsis-related acute kidney injury. The present results showed an overall mortality rate of 51.8% in all 170 patients with SA-AKI, which is consistent with the results of previous studies. Additionally, we observed that SA-AKI patients in the death group exhibited a higher risk of septic shock than did those in the survival group. This aligns with the findings of Ranieri’s et al,34 suggesting that patients with sepsis and hypocoagulation together with increased hemorrhage potential had higher morbidity and mortality rates. Identifying prognostic risk indicators in SA-AKI patients is paramount to assess disease progression accurately and to ensure immediate, effective interventions. Meanwhile, there was no statistical difference in most of the variables between the training and validation cohorts, meaning there was a certain degree of homogeneity in most of the indicators between the two groups, which speaks to the generalizability of the results.
In our study, 79% of SA-AKI patients showed anomalies in at least one coagulation index, and irregularities were noted in one or more parameters among PLT, TT, PT, and APTT levels. Notably, the death group showed a significantly higher rate of abnormal coagulation indices than did the survival group, and their cumulative survival rate was inferior to those with normal coagulation. Furthermore, 27.73% of patients with sepsis presented with DIC at the time of their AKI diagnosis. The DIC incidence was notably higher in the death group than in the survival group. While 96.64% of SA-AKI patients exhibited combined SIC, no significant difference existed between the survival and death groups. This could be due to the SIC score’s high sensitivity,35 possibly leading to the enrolment of patients who are already in advanced SA-AKI stages. The study by Liao et al36 proposed that both SIC and overt DIC scores escalate over time, with DIC diagnosis thresholds being surpassed after those of SIC. Hence, the SA-AKI patients reaching the SIC diagnostic threshold considerably outnumbered those reaching the overt DIC threshold. Our findings reinforce the idea that coagulation disorders play a significant role in SA-AKI development and serve as crucial benchmarks for SA-AKI patients’ prognostic assessments.
The pathophysiology underlying sepsis and SA-AKI is multifaceted, encompassing changes in the function of various organs and systems. The nuances of these changes are still subjects of debate in the medical community. Contemporary research suggests that the development of SA-AKI might stem from a multi-systemic response, primarily between the coagulation and immune systems, following an invasion by pathogenic microorganisms. This protective response is the body’s natural defense against microbial threats. However, this interaction can lead to immunothrombosis and consequential organ damage.23 In sepsis, there is a pronounced release of endotoxins and inflammatory agents that compromise the vascular endothelial structure, promoting monocyte-macrophage expression and subsequent tissue damage.37 Furthermore, tissue factors released from these monocytes activate circulating factor VIIa,38 leading to the formation of a tissue–factor VIIa complex. This event marks the start of the exogenous coagulation pathway, which in turn causes hyperfibrinolysis and a reduction in coagulation factor production.39 As a result, coagulation indices often show elevated PT and INR levels but a decline in fibrinogen. Concurrently, inflammatory substances, when released by immune cells, can either directly or indirectly, cause endothelial cell damage. This process activates coagulation factor XI through the binding of coagulation factor XIIa to subendothelial collagen, triggering the endogenous coagulation pathway and subsequent thrombosis in microvascular structures.40 An increase in APTT is a typical characteristic of coagulation indices in this context. Furthermore interactions between the endogenous and exogenous coagulation pathways amplify coagulation activities. Both pathways culminate in platelet aggregation and adhesion,41 reduced fiber activity, increased hypercoagulability, and microthrombi formation in microvascular structures. This ultimately leads to renal microcirculation disorders and an increase in mortality rates.42 This aligns with our findings and suggests that anomalies in coagulation significantly influence the onset of SA-AKI43 and its eventual prognosis.
Among the measured coagulation parameters, APTT was associated with 28-day mortality rate in SA-AKI patients. Deeper investigations highlighted that an increased APTT correlated with a markedly increased mortality risk. Cox multifactorial analysis and RCS curves unveiled pronounced differences in survival rates among SA-AKI patients, especially when APTT was ≥ 37.7 s. Additionally, our subgroup analyses showed consistent prognostic values across the groups, with no interactions between APTT and other covariates. In the validation cohort, despite the identification of a turning point at an APTT of 38.8 s, this did not obscure the clarification of the relationship between APTT and the risk of 28-day mortality. This outcome could be attributed to our methodological shift towards emphasizing a HR of 1 as the pivotal threshold. Notably, within the APTT range of 37.7 s to 38.8 s, we observed a slower increase in the risk of death at 28 days, which strengthens the nuanced understanding of the predictive value of the APTT.
APTT is an essential metric for assessing the internal coagulation pathway.44 An increased APTT signifies abnormalities in coagulation factors and disruptions in internal coagulation. In our study, Cox multifactorial analysis revealed that an increased APTT is an independent risk factor for 28-day mortality in patients with SA-AKI. When assessing the cumulative survival rates through APTT stratification, it was shown that SA-AKI patients with APTT readings above 37.7 s had a death 1.75-fold risk of mortality than did their counterparts with APTT readings below 37.7 s. As the APTT lengthened, the 28-day mortality rate in SA-AKI patients increased consistently. This consistent relationship between increased APTT and poor outcomes remained even after controlling for potential confounding factors. The same result was found in the validation cohort. Previous studies45,46 have made similar observations regarding the prognostic implications of increased APTT in patients with sepsis. However, our ROC curve assessments revealed that while the predictive capabilities of APTT are fairly universal, they lack sensitivity. The accuracy of APTT as a predictive tool for SA-AKI prognosis can be enhanced when combined with parameters such as the APACHE II score, Lac, and CRP. It is worth noting that our participant pool included individuals who experienced external trauma or burns; therefore, our findings necessitate further validation in a larger sample for clarity.
Through interaction analyses, our investigation unearthed a markedly consistent and robust association between APTT and 28-day adverse prognoses, demonstrating resilience against the influence of a multitude of risk factors. This harmonizes with prior research47 elucidating the correlation between coagulation markers, such as APTT, and the staging or prognostication of AKI, particularly within the purview of distinct illnesses like hemorrhagic fever coupled with renal syndrome. In our analysis, it was observed that APTT’s predictive capacity for 28-day mortality was much lower in patients classified under stage 2 AKI than in those with stages 1 or 3 AKI. Previous studies established a direct correlation between the severity of AKI and the subsequent increases in patient mortality rates.30 Contrary to this result, our dataset indicated an anomaly wherein mortality rates were higher in patients with stage 2 AKI than in those with stage 3 AKI. This divergence from prior findings48 could potentially be attributed to the absence of continuous dynamic surveillance of blood creatinine levels in the present study, which may have led to diminished precision in AKI staging for certain patients. Additionally, not all mortality within the present cohort could be directly ascribed to AKI, considering the high chance of sepsis leading to MODS.49,50 Therefore, the intricacies surrounding the relationship between SA-AKI and 28-day mortality warrant further investigations.
Our study had certain limitations. First this study’s retrospective design primarily concentrated on initial coagulation indices without assessing the effects of treatments during hospitalization, and we did not track data dynamically. We did not conduct a prospective study due to resource constraints, and the lack of detailed pathogen identification may have compromised our further analysis of SA-AKI outcomes. Moving forward, the goal is to engage in comprehensive research and analyses, aiming for broader multicenter studies to bolster the robustness and scope of our evaluations.
Conclusion
APTT may be an independent predictor of adverse outcomes in SA-AKI patients, especially in patients with stages 1 and 3 AKI. Increased APTT values escalated, the 28-day mortality rate proportionally increased.
Data Sharing Statement
The data underlying this article are available in the article and online Supplementary Material.
Acknowledgments
We thank the nurses and physicians who assisted with this study. We thank the First Hospital of Fujian Medical University for providing the clinical data.
Funding
This work was supported by the Fujian Provincial Science and Technology Planning Project Social Development and Technology Guiding Project (grant number: 2020Y0032) and the Fujian Provincial Health and Health Provincial Special Subsidy Funds (grant number: BPB - 2022FSD and BPB - FSD2021). The funding agencies had no role in the design and conduct of the study; collection, management, analysis, and interpretation of data; preparation, review, and approval of the manuscript; or the decision to submit the manuscript for publication.
Disclosure
The authors declare no competing interests in this work.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
2. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the global burden of disease study. Lancet. 2020;395(10219):200–211. doi:10.1016/S0140-6736(19)32989-7
3. Prowle JR. Sepsis-associated AKI. Clin J Am Soc Nephrol. 2018;13(2):339–342. doi:10.2215/CJN.07310717
4. Bouchard J, Acharya A, Cerda J, et al. A prospective international multicenter study of AKI in the intensive care unit. Clin J Am Soc Nephrol. 2015;10(8):1324–1331. doi:10.2215/CJN.04360514
5. Shum HP, Kong HH, Chan KC, Yan WW, Chan TM. Septic acute kidney injury in critically ill patients - A single-center study on its incidence, clinical characteristics, and outcome predictors. Ren Fail. 2016;38(5):706–716. doi:10.3109/0886022X.2016.1157749
6. Basu RK, Hackbarth R, Gillespie S, et al. Clinical phenotypes of acute kidney injury are associated with unique outcomes in critically ill septic children. Pediatr Res. 2021;90(5):1031–1038. doi:10.1038/s41390-021-01363-3
7. Peerapornratana S, Manrique-Caballero CL, Gomez H, Kellum JA. Acute kidney injury from sepsis: current concepts, epidemiology, pathophysiology, prevention and treatment. Kidney Int. 2019;96(5):1083–1099. doi:10.1016/j.kint.2019.05.026
8. Hoste EAJ, Kellum JA, Selby NM, et al. Global epidemiology and outcomes of acute kidney injury. Nat Rev Nephrol. 2018;14(10):607–625. doi:10.1038/s41581-018-0052-0
9. Nusshag C, Wei C, Hahm E, et al. suPAR links a dysregulated immune response to tissue inflammation and sepsis-induced acute kidney injury. JCI Insight. 2023;8(7). doi:10.1172/jci.insight.165740
10. Pickkers P, Darmon M, Hoste E, et al. Acute kidney injury in the critically ill: an updated review on pathophysiology and management. Intensive Care Med. 2021;47(8):835–850. doi:10.1007/s00134-021-06454-7
11. Zhao S, Liao J, Shen M, Li X, Wu M. Epigenetic dysregulation of autophagy in sepsis-induced acute kidney injury: the underlying mechanisms for renoprotection. Front Immunol. 2023;14:1180866. doi:10.3389/fimmu.2023.1180866
12. Wu Z, Deng J, Zhou H, et al. Programmed cell death in sepsis associated acute kidney injury. Front Med. 2022;9:883028. doi:10.3389/fmed.2022.883028
13. Morrell ED, Kellum JA, Pastor-Soler NM, Hallows KR. Septic acute kidney injury: molecular mechanisms and the importance of stratification and targeting therapy. Crit Care. 2014;18(5):501. doi:10.1186/s13054-014-0501-5
14. Poston JT, Koyner JL. Sepsis associated acute kidney injury. BMJ. 2019;364:k4891. doi:10.1136/bmj.k4891
15. Gameiro J, Fonseca JA, Jorge S, Gouveia J, Lopes JA. Neutrophil, lymphocyte and platelet ratio as a predictor of mortality in septic-acute kidney injury patients. Nefrologia. 2020;40(4):461–468. doi:10.1016/j.nefro.2019.11.006
16. Yoon SH, Choi B, Eun S, et al. Using the lactate-to-albumin ratio to predict mortality in patients with sepsis or septic shock: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci. 2022;26(5):1743–1752. doi:10.26355/eurrev_202203_28244
17. Md Ralib A, Mat Nor MB, Pickering JW. Plasma neutrophil gelatinase-associated lipocalin diagnosed acute kidney injury in patients with systemic inflammatory disease and sepsis. Nephrology. 2017;22(5):412–419. doi:10.1111/nep.12796
18. Zhou J, Bai Y, Wang X, et al. A simple risk score for prediction of sepsis associated-acute kidney injury in critically ill patients. J Nephrol. 2019;32(6):947–956. doi:10.1007/s40620-019-00625-y
19. Schmitz M, Tillmann F, Paluckaite A, et al. Mortality risk factors in intensive care unit patients with acute kidney injury requiring renal replacement therapy: a retrospective cohort study. Clin Nephrol. 2017;88(07):27–32. doi:10.5414/CN109078
20. Chen KF, Liu S-H, Li C-H, et al. Development and validation of a parsimonious and pragmatic CHARM score to predict mortality in patients with suspected sepsis. Am J Emerg Med. 2017;35(4):640–646. doi:10.1016/j.ajem.2016.10.075
21. Liu J, Liu Z, Zhao T, Su T, Jin Q. Thromboelastography and traditional coagulation testing in non-ICU-admitted patients with acute kidney injury: an observational cohort study. Am J Nephrol. 2023;54(5–6):208–218. doi:10.1159/000530777
22. Wu R, Wang N, Comish PB, Tang D, Kang R. Inflammasome-dependent coagulation activation in sepsis. Front Immunol. 2021;12:641750. doi:10.3389/fimmu.2021.641750
23. Iba T, Umemura Y, Wada H, Levy JH. Roles of coagulation abnormalities and microthrombosis in sepsis: pathophysiology, diagnosis, and treatment. Arch Med Res. 2021;52(8):788–797. doi:10.1016/j.arcmed.2021.07.003
24. Sawhney S, Mitchell M, Marks A, Fluck N, Black C. Long-term prognosis after acute kidney injury (AKI): what is the role of baseline kidney function and recovery? A systematic review. BMJ Open. 2015;5(1):e006497. doi:10.1136/bmjopen-2014-006497
25. Siew ED, Matheny ME. Choice of reference serum creatinine in defining acute kidney injury. Nephron. 2015;131(2):107–112. doi:10.1159/000439144
26. Wada H, Takahashi H, Uchiyama T, et al. The approval of revised diagnostic criteria for DIC from the Japanese society on thrombosis and hemostasis. Thromb J. 2017;15(1):17. doi:10.1186/s12959-017-0142-4
27. Iba T, Nisio MD, Levy JH, Kitamura N, Thachil J. New criteria for sepsis-induced coagulopathy (SIC) following the revised sepsis definition: a retrospective analysis of a nationwide survey. BMJ Open. 2017;7(9):e017046. doi:10.1136/bmjopen-2017-017046
28. Gourd NM, Nikitas N. Multiple organ dysfunction syndrome. J Intensive Care Med. 2020;35(12):1564–1575. doi:10.1177/0885066619871452
29. Zhi DY, Lin J, Zhuang H-Z, et al. Acute kidney injury in critically ill patients with sepsis: clinical characteristics and outcomes. J Invest Surg. 2019;32(8):689–696. doi:10.1080/08941939.2018.1453891
30. Hoste EA, Bagshaw SM, Bellomo R, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41(8):1411–1423. doi:10.1007/s00134-015-3934-7
31. STARRT-AKI Investigators. Timing of initiation of renal-replacement therapy in acute kidney injury. N Engl J Med. 2020;383:240–251. doi:10.1056/NEJMoa2000741
32. Cho AY, Yoon HJ, Lee KY, Sun IO. Clinical characteristics of sepsis-induced acute kidney injury in patients undergoing continuous renal replacement therapy. Ren Fail. 2018;40(1):403–409. doi:10.1080/0886022X.2018.1489288
33. Sood MM, Shafer LA, Ho J, et al. Early reversible acute kidney injury is associated with improved survival in septic shock. J Crit Care. 2014;29(5):711–717. doi:10.1016/j.jcrc.2014.04.003
34. Ranieri VM, Thompson BT, Barie PS, et al. Drotrecogin alfa (activated) in adults with septic shock. N Engl J Med. 2012;366(22):2055–2064. doi:10.1056/NEJMoa1202290
35. Loberger JM, Aban IB, Prabhakaran P. Exploration of sepsis-associated coagulopathy severity and pediatric septic shock outcomes. J Pediatr Intensive Care. 2021;10(01):38–44. doi:10.1055/s-0040-1713436
36. Liao D, Zhou F, Luo L, et al. Haematological characteristics and risk factors in the classification and prognosis evaluation of COVID-19: a retrospective cohort study. Lancet Haematol. 2020;7(9):e671–e678. doi:10.1016/S2352-3026(20)30217-9
37. Park JT, Lee H, Kee YK, et al. High-dose versus conventional-dose continuous venovenous hemodiafiltration and patient and kidney survival and cytokine removal in sepsis-associated acute kidney injury: a randomized controlled trial. Am J Kidney Dis. 2016;68(4):599–608. doi:10.1053/j.ajkd.2016.02.049
38. Foley JH, Conway EM. Cross talk pathways between coagulation and inflammation. Circ Res. 2016;118(9):1392–1408. doi:10.1161/CIRCRESAHA.116.306853
39. Levi M, Poll T. Coagulation in patients with severe sepsis. Semin Thromb Hemost. 2015;41(01):9–15. doi:10.1055/s-0034-1398376
40. Tsao CM, Ho ST, Wu CC. Coagulation abnormalities in sepsis. Acta Anaesthesiol Taiwan. 2015;53(1):16–22. doi:10.1016/j.aat.2014.11.002
41. Hurley SM, Kahn F, Nordenfelt P, et al. Platelet-dependent neutrophil function is dysregulated by M protein from streptococcus pyogenes. Infect Immun. 2015;83(9):3515–3525. doi:10.1128/IAI.00508-15
42. Watchorn J, Huang D, Bramham K, Hutchings S. Decreased renal cortical perfusion, independent of changes in renal blood flow and sublingual microcirculatory impairment, is associated with the severity of acute kidney injury in patients with septic shock. Crit Care. 2022;26(1):261. doi:10.1186/s13054-022-04134-6
43. Assinger A, Schrottmaier WC, Salzmann M, Rayes J. Platelets in Sepsis: an Update on Experimental Models and Clinical Data. Front Immunol. 2019;10:1687. doi:10.3389/fimmu.2019.01687
44. Kiflemariam FK, Tewelde AG, Hamid AM, et al. Meriandra dianthera aqueous extract and its fraction prevents blood coagulation by specifically inhibiting the intrinsic coagulation pathway: an in vitro study. J Exp Pharmacol. 2022;14:205–212. doi:10.2147/JEP.S362258
45. Chen RJ, Zhou XM, Rui QL, Wang XX. Combined predictive value of the risk factors influencing the short-term prognosis of sepsis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020;32(3):307–312. Chinese. doi:10.3760/cma.j.cn121430-20200306-00218
46. Lorente L, Martín MM, Ortiz-López R, et al. Association between septic patient mortality and blood survivin concentrations. Med Intensiva. 2023;47(2):84–89. doi:10.1016/j.medine.2021.12.017
47. Chen WJ, Du H, Hu H-F, et al. Levels of peripheral blood routine, biochemical and coagulation parameters in patients with hemorrhagic fever with renal syndrome and their relationship with prognosis: an observational cohort study. BMC Infect Dis. 2024;24(1):75. doi:10.1186/s12879-023-08777-w
48. Savaş Şen Z, Çakar N. Acute kidney injury: classification and prognosis. Turk J Pediatr. 2017. doi:10.12956/tjpd.2017.314
49. Sun GD, Zhang Y, Mo SS, Zhao MY. Multiple organ dysfunction syndrome caused by sepsis: risk factor analysis. Int J Gen Med. 2021;14:7159–7164. doi:10.2147/IJGM.S328419
50. Elke G, Bloos F, Wilson DC, Meybohm P, SepNet Critical Care Trials G. Identification of developing multiple organ failure in sepsis patients with low or moderate SOFA scores. Crit Care. 2018;22(1):147. doi:10.1186/s13054-018-2084-z
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Age-Stratified Immune-Inflammatory Profiles and Prognostic Implications of Old Patients in the ICU: A Prospective Study
Lian H, Wang G, Zhang Q, Zhao H, Wang X
Journal of Inflammation Research 2025, 18:13727-13743
Published Date: 3 October 2025
Early Identification and Risk Factors for Acute Kidney Injury Progression: A Real-World Study
Nan Z, Fan X, Guo S, Zhao CC, Yang J, Wang Y, Zhang T
Risk Management and Healthcare Policy 2026, 19:576846
Published Date: 2 February 2026