Back to Journals » Nature and Science of Sleep » Volume 15
Electroencephalographic Changes in Sleep During Acute and Subacute Phases After Sports-Related Concussion
Authors Stevens DJ ![]() , Appleton S
, Appleton S ![]() , Bickley K
, Bickley K ![]() , Holtzhausen L, Adams R
, Holtzhausen L, Adams R ![]()
Received 16 November 2022
Accepted for publication 15 March 2023
Published 19 April 2023 Volume 2023:15 Pages 267—273
DOI https://doi.org/10.2147/NSS.S397900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
David J Stevens,1 Sarah Appleton,1 Kelsey Bickley,1 Louis Holtzhausen,2– 4 Robert Adams1,5
1Sleep Health, Flinders Health and Medical Research Institute, Flinders University, Bedford Park, South Australia, Australia; 2Aspetar Orthopaedic and Sports Medicine Hospital, Doha, Qatar; 3Section Sports Medicine, Faculty of Health Science, University of Pretoria, Pretoria, South Africa; 4Department of Exercise and Sport Science, University of the Free State, Bloemfontein, South Africa; 5Respiratory and Sleep Services, Southern Adelaide Local Health Network, Bedford Park, South Australia, Australia
Correspondence: David J Stevens, Sleep Health, Flinders Health and Medical Research Institute, Flinders University, Level 2a, 5 Laffer Dve, Bedford Park, South Australia, 5041, Australia, Tel +61 7306 1816, Email [email protected]
Purpose: Little is known about sleep after a concussion, a form of mild traumatic brain injury. Given the importance of sleep for both maintaining brain health and recovery from injury, we sought to examine sleep acutely and subacutely after concussion.
Methods: Athletes who experienced a sports-related concussion were invited to participate. Participants underwent overnight sleep studies within 7 days of the concussion (acute phase), and again eight-weeks after the concussion (subacute phase). Changes in sleep from both the acute and subacute phases were compared to population normative values. Additionally, changes in sleep from acute to subacute phase were analysed.
Results: When compared to normative data, the acute and subacute phases of concussion showed longer total sleep time (p < 0.005) and fewer arousals (p < 0.005). The acute phase showed longer rapid eye movement sleep latency (p = 0.014). The subacute phase showed greater total sleep spent in Stage N3% (p = 0.046), increased sleep efficiency (p < 0.001), shorter sleep onset latency (p = 0.013), and reduced wake after sleep onset (p = 0.013). Compared to the acute phase, the subacute phase experienced improved sleep efficiency (p = 0.003), reduced wake after sleep onset (p = 0.02), and reduced latencies for both stage N3 sleep (p = 0.014) and rapid eye movement sleep (p = 0.006).
Conclusion: This study indicated sleep during both the acute and subacute phases of SRC was characterised by longer and less disrupted sleep, along with improvements in sleep from the acute to subacute phases of SRC.
Keywords: mild traumatic brain injury, somnolence, neural trauma, nocturnal activity
Plain Language Summary
Sleep plays an important role in recovery from trauma to the brain. Whilst it is well established that sleep is severely affected after major brain injuries, little is known about how concussions, a form of mild traumatic brain injury, affects sleep. We examined changes in sleep from straight after concussion to 8 weeks later and also compared them with population normative values. Sleep was measured using gold standard electroencephalography (EEG), which measures brain waves. This allowed for an accurate measure of sleep duration, quality, and the stages of sleep. The results indicate that the participants in this study, all of whom experienced a concussion, slept better compared to the population normative values. Furthermore, sleep appeared to further improve 8 weeks after concussion when compared to sleep immediately after concussion. This included more sleep, better sleep quality, and even more deep sleep, which is pivotal for repairing the brain. We speculate that the improvement in sleep was an attempt by the brain to heal itself. More research is needed in a larger population to confirm this speculation.
Introduction
A concussion is a form of mild traumatic brain injury caused by biomechanical trauma to the head, such as a direct impact, or a sudden acceleration, deceleration, and/or rotation of the head, irrespective of whether a person lost consciousness.1 Biomechanical trauma causes damage to neuronal axons, which in turn results in errant brain activation patterns.
There has been growing concern surrounding the long-term health risks of concussions. Acutely, concussions often result in neurological, psychological, and cognitive deficits.2 Long-term epidemiological evidence indicates a link between repeated concussions and chronic traumatic encephalopathy (CTE), a neurodegenerative condition caused by the accumulation of amyloid-β and τ-proteins plaques.3
Healthy sleep plays an important role in maintaining neural health. The glymphatic process that occurs during Stage N3 sleep (also known as slow wave, or deep, sleep) clears the brain of amyloid-β and τ-proteins plaques.4 Even a single night of sleep disruption reduces the effectiveness of the glymphatic process.5 When coupled with preliminary evidence that poor sleep during the months preceding a concussion is associated with poorer cognition and emotional problems, it is important that the effect of concussion on sleep is carefully examined.
Yet research examining the effect of concussion on sleep is relatively limited. A review highlighted the majority of studies examining the effect of concussion on sleep through subjective measures.6 Two studies utilising actigraphy failed to show any differences between those with concussion, and those without concussion.7,8 Additionally, Raikes et al did not show any differences in actigraphy measured sleep from the acute post-concussion phase, which was measured within 4 days of the injury, to the subacute phase of the injury.7 Whilst actigraphy is useful for longitudinal measurements of sleep, it is limited in only being able to measure total sleep time, sleep efficiency, and sleep onset latency. Few studies have measured sleep after concussion by electroencephalography (EEG), which is the gold standard measurement of sleep. Gosselin et al show no differences in EEG measured sleep in 10 people who had experienced a sports-related concussion (SRC) within the previous 12 months compared to 10 people who had not experienced an SRC.9 Sleep was measured between 1 and 11 months post-concussion. Therefore, any acute affects of concussion on sleep could not be determined. Rao et al also showed no changes in EEG-measured sleep between a group of seven people who had experienced concussion and seven people who had not experienced a concussion (although there was a trend towards reduced duration of Stage N2 sleep).10 Whilst sleep was measured within a week of injury, there were no follow-up measures of sleep to examine for changes throughout recovery from concussion. Mantua et al showed prolonged rapid eye movement (REM) latency and reduced REM sleep as a proportion of overall sleep, in 14 people who had experienced an SRC when compared to age and gender matched control group,11 however, sleep was measured several years after the concussion.
Therefore, this study sought to objectively examine sleep by EEG during both the acute (within 7 days) and subacute (8 weeks after injury) phases after an SRC. These were compared to published age and gender-matched normative data.12 Given the preliminary evidence suggesting sleep is impaired after a concussion, coupled with studies showing impaired sleep after moderate-to-severe traumatic brain injuries,13 we hypothesized that sleep during both the acute and subacute phases after an SRC would be impaired compared to normative data. We also sought to examine for any changes in sleep from the acute to subacute phase of SRC. As no study has undertaken longitudinal measures of sleep after a concussion, no directional hypothesis was formulated.
Materials and Methods
Participants
People with SRC were invited to participate. Participants were referred from a specialized sports and exercise medicine clinic. Exclusions to participation included known, uncontrolled sleep problems, known neurological issues, or uncontrolled psychological problems. Participants were reimbursed $250 for participating. In compliance with the Declaration of Helsinki, this study received approval from the Flinders University Human Research Ethics Committee (protocol 8569), with informed, signed consent obtained prior to study commencement.
Measurements
Overnight sleep was measured by a single-channel EEG (F3-M2), with oculomotor and chin muscle movement to help with sleep staging (Embletta X100, Natus Medical, Ca., USA). Single-channel EEG is commonly used for in-home studies.14 Overnight studies occurred in the participants' own beds. EEG equipment was set up by research staff, with the equipment programmed to start upon a successful setup. Scoring was conducted by a single sleep technologist and measures included total sleep time, sleep onset latency, REM onset latency, percent of sleep in Stages N1, N2, N3, and REM, sleep efficiency, and arousal index. Post-concussion symptomology was measured using the Sports Concussion Assessment Tool version 5 (SCAT-5).15 The SCAT-5 is the most commonly used concussion assessment tool and has a high test–retest reliability (overall score Spearman’s ρ = 0.85, severity score Spearman’s ρ = 0.84, see Hannien et al for further psychometric properties16). The SCAT-5 symptoms was completed by the participant in the presence of research staff, immediately prior to the EEG setup.
Protocol
Participants underwent two nights of testing. The first night occurred within 7 days of the SRC, whilst the second night occurred eight-weeks later. For both testing nights, participants underwent the SCAT-5, and were then set up for the overnight EEG-sleep study in their homes. Recording commenced during the setup visit, with participants recording when they went to bed, and when they attempted to fall asleep.
Data Analysis
Age and gender matched normative data were generated using a published, online calculator (https://omc.ohri.ca/psgnorms/) based on a meta-analysis of population normative values of 5273 healthy adults (no known acute or chronic health problems at the time of the recording) from 169 studies.12 The age and gender matched results are presented in Supplementary S1. The use of normative data meant no adjusted analyses occurred.
Data was analysed in SPSS (v28, IBM, NY, USA). Symptomology data from the SCAT-5 was reported as percentages. As it was hypothesized that sleep would be impaired during both the acute and subacute phases after an SRC when compared to normative data, a one-sided, independent-sample t-test was used (with homogeneity tests and appropriate p-value reporting). As no directional hypothesis could be formulated to examine changes in EEG measured sleep from acute (within 7-days) and subacute (8-weeks post injury), a two-sided, paired-sample t-test was used. Significance for all analyses was set at p = 0.05, with effect sizes (Cohen’s D [d]) reported.
Results
Participants
Out of 17 participants who initially expressed interest, 10 participants consented to participate. Six were unable to partake due to COVID-related restrictions, whilst another chose not to partake. Descriptive statistics of those who participated (age, body mass index, and concussion history) are presented in Table 1.
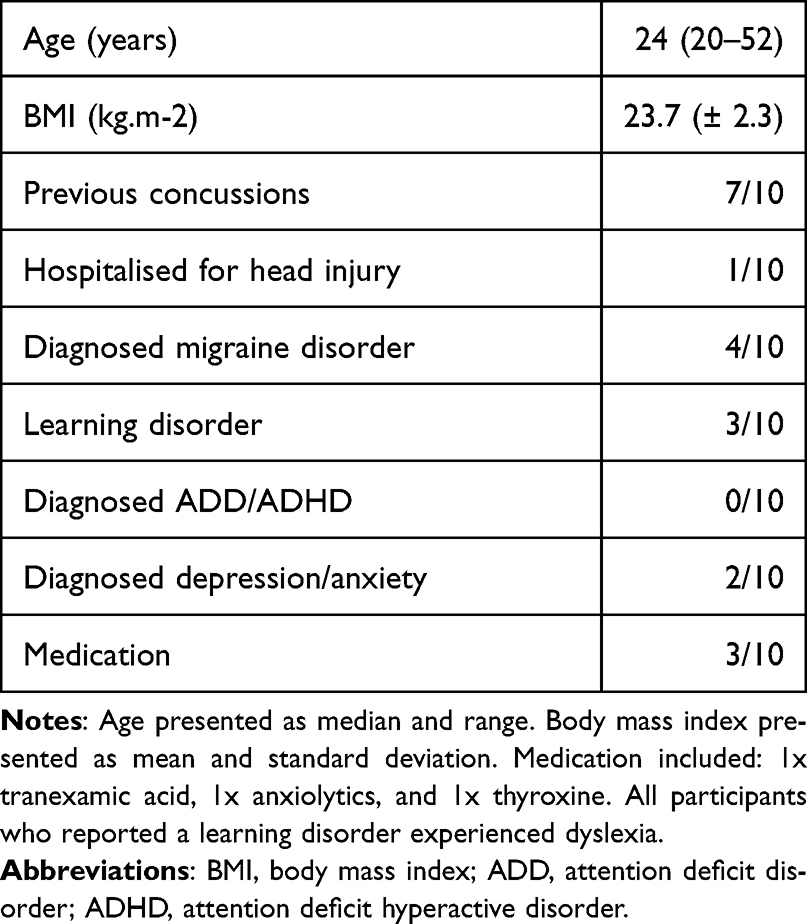 |
Table 1 Demographic Data and Concussion History |
Concussion Symptomology
During the acute post-SRC phase, participants reported a median of 11 symptoms (range 3–19), with a median score of 21 (range 3–45). During the subacute post-SRC phase, participants reported a median of four symptoms (range 0–13), with a median overall symptom score of 5 (range 0–23).
Overnight Sleep Metrics
Sleep data for both the acute and subacute phases of SRC, as well as the normative data, are presented in Table 2. No EEG data was lost for any participant; however, one participant lost electrocardiograph (ECG) measures, whilst another lost pulse oximetry, both on subacute nights.
 |
Table 2 Sleep Measures During Acute (Within 7 Days) and Subacute (Within 8 Weeks) Phases, as Well as Normative Values |
When comparing the acute sleep metrics to the normative data, the t-tests indicated that those with SRC experienced significantly longer total sleep time (t9.4 = 3.2, p = 0.005, d = 1.42), significantly fewer arousals (t18 = 4.8, p < 0.001, d = 2.07), and significantly longer REM latency (t9.1 = 2.6, p = 0.014, d = 1.17). Further, there was a trend towards significantly increased percent of the total sleep spent in Stage N3 sleep (t9.04 = 1.7, p = 0.059, d = 0.77). No other significant differences were shown.
When comparing the subacute sleep metrics to the normative data, the t-tests indicated those with SRC experienced significantly longer total sleep time (t9.5 = 3.9, p = 0.002, d = 1.76), reduced percent of the total sleep time spend in Stage N1 sleep (t9.4 = 2.9, p = 0.009, d = 1.28), increased percent of the total sleep spent in Stage N3 sleep (t9.1 = 1.9, p = 0.046, d = 0.84), increased sleep efficiency (t18 = 5.6, p < 0.001, d = 2.43), fewer arousals (t11.4 = 3.1, p = 0.005, d = 1.35), shorter sleep onset latency (t9.3 = 2.7, p = 0.013, d = 1.19), and reduced wake after sleep onset (t18 = 2.5, p = 0.013, d = 1.08). No other significant differences were shown.
When examining changes in sleep from acute to subacute SRC, the t-tests showed that compared to the acute phase of SRC, the subacute phase of SRC experienced significantly improved sleep efficiency (t9 = 4.1, p = 0.003, d = 1.3), reduced wake after sleep onset (t9 = 2.8, p = 0.02, d = 0.89), and reduced latencies for both stage N3 sleep (t9 = 3.1, p = 0.014, d = 0.97) and stage REM sleep (t9 = 3.5, p = 0.006, 1.12). No other significant differences were shown.
Discussion
This is the first study to examine overnight EEG during the acute (within 7 days) and subacute (8 weeks) phases after SRC. Sleep during both the acute and subacute phases of SRC was characterized by longer and less disrupted sleep when compared to population normative values.12 These results were not in accordance with our hypothesis that sleep would be impaired compared to normative data values. There was also an improvement in sleep, from the acute to subacute phase of SRC.
Methodologically, our study aligned closely with Roa et al’s study measuring sleep acutely within a week after concussion, but showed conflicting results.10 Rao et al showed no difference in any sleep metric between those with concussion and controls who did not have concussion. Our study showed that during the acute-post concussion phase, there was significantly longer TST, reduced arousal index (which Roa et al did not report), and longer REM onset latency during the acute phase, but did not show any significant changes in sleep stage composition. A major difference between the studies was the control group comparison. Our study compared sleep after concussion to published normative data, whilst Rao et al compared sleep in those with concussion to a gender and age matched group (although data for the control group was measured for a different experiment). Therefore, the differences in results could be due to the difference in control data. Interestingly, however, only one participant of Rao et al’s study sustained a concussion from sport, whilst four sustained concussions from assault, one was involved in a motor vehicle accident, and another had “a wooden board fall on his head”. Therefore, it is possible that the different mechanism of injury could also explain the differences in results. Rao et al did not measure undertaking further sleep measurements beyond a week after concussion, meaning comparison to the subacute phase of this study is impossible.10
The differences in timing from concussion to sleep measurements may explain contrasting results with other studies that measured sleep by EEG after concussion. Gosselin et al showed no differences in sleep between those with concussion and those who did not have concussion.9 Importantly, sleep was measured between 1 and 11 months after concussion. In contrast, Mantua et al showed those who had experienced concussion several years prior (not necessarily sports related) experienced prolonged REM latency, with reduced overall REM sleep, compared to those without concussion.11 Our study also showed significantly prolonged REM latency during the acute post-SRC phase compared to both normative data and the subacute post-SRC phase. By the subacute phase, however, there was no longer prolonged REM latency compared to the normative data. Given sleep was measured several years after concussion (which was also not sport related), it is possible that factors other than concussion can be attributed to changes in sleep.11
This is the first study that has utilised EEG to show improvements in sleep from the acute to subacute phases of concussion. A previous study utilising actigraphy showed no changes in total sleep time, sleep efficiency, and wake after sleep onset from the acute (4 days post-concussion) to the subacute (4 weeks post-concussion) phases, nor any differences in sleep metrics were shown between the 7 participants with concussion, and the 10 participants who did not have concussion.7 Given the differences in measurement of sleep, however, comparison of the results between the studies is difficult.
We speculate that longer and less disrupted sleep during both phases of SRC, when compared to normative values, and improvements in sleep from acute to subacute phases of SRC, is an attempt by the brain to minimise and repair the damage resulting from SRC. The significantly increased proportion of Stage N3 sleep during the subacute phase is potentially important. There is growing evidence that concussions may cause an accumulation of amyloid-β and τ-proteins, with multiple concussions seemingly resulting in greater accumulation.17 The glymphatic process, which occurs during Stage N3 sleep, removes these plaques.4 A rat study showed both pharmacological and behavioural interventions, which increased Stage N3 sleep improved axonal recovery from TBI.18 Similarly, increases in sleep efficiency and TST are associated with improved neurological outcomes in traumatic and acquired brain injury, such as stroke.19 Therefore, we speculate that increased TST and reduced arousal index during both phases of SRC and the improved sleep efficiency during the subacute phase, are recovery mechanisms utilised by the brain to rehabilitate itself. Theses should be further explored in future research.
What is unclear is why there was an extended onset of REM sleep and Stage N3 sleep during the acute phase, significantly so for REM sleep when compared to normative values (normative data on Stage N3 latency was not calculated). It is possible that the neurochemical cascade that occurs after a concussion such as the influx of calcium into neuronal axons, interferes with sleep-stage initiation.20 This too should be explored in future research.
The participants in our study were physically active, with all concussions were sustained whilst playing sport. Moderate physical activity is enough to improve sleep quality and reduce the burden of sleep disorders.21 The normative data, from which the results of this study were compared, does not mention physical activity levels. Therefore, we cannot discount the effect of participation in physical activity on potentially contributing to the improved sleep shown after SRC in this study.
Other intrinsic factors, presented in Table 1, are unlikely to explain the results. Only two participants reported suffering from depression or anxiety, which potentially causes sleep problems.22 One participant was treated with anxiolytics, which may suppress REM sleep, and increase Stage N2 sleep.23 It is not known whether other medications, being tranexamic acid, and thyroxine, affect sleep. Three participants reported learning difficulties, all being dyslexia, which causes difficulty initiating and maintaining sleep. Yet, as the results indicated longer and less disrupted sleep when compared to population normative values and an improvement in sleep from acute to subacute post-concussion phases, it is unlikely that the intrinsic factors contributed to the sleep results shown. We also acknowledge that there is night-to-night variability of EEG measured sleep.24 Future studies should record sleep over multiple nights to minimize the potential effect of night-to-night variability.
Indeed, the exploratory and pilot nature of this study meant there were limitations; however, these can be used to guide future research. We recruited no control group but rather utilised published normative values from an online calculator. Ideally, future studies should examine sleep prior to an SRC occurring. Participants who consented to partake appeared to only have mild SRC, given the low symptomology scores recorded on SCAT. Therefore, it is unclear whether similar results would be seen in those with more severe SRCs. A recent scoping review highlighted that roughly a third of patients who experience SRCs report worse sleep; however, no association with concussion severity was drawn.6 We speculate that severe SRCs may result in poorer objectively measured sleep. Finally, the number of participants was low. The COVID pandemic meant many sports were not played during the data collection period, thereby reducing the potential participants available, whilst adherence to COVID guidelines, including close contact isolation and social distancing, precluded the conduct of sleep studies in six potential participants. Future studies should endeavour to include other neurophysiological, and neurocognitive measures, to examine whether changes in sleep during recovery from an SRC result in changes to other aspects of SRC consequences.
Conclusion
This is the first study to objectively examine sleep at set times after concussion. The novel findings of improved sleep a during both the acute and subacute post-concussion phases are a mechanism by the brain to improve recovery from SRC. Further research should seek to replicate these findings in a larger population, with a range of symptom severity, which would ultimately guide future research examining whether sleep interventions can be used to improve recovery from SRC.
Acknowledgments
We would like to thank Wakefield Sports + Exercise Medicine Clinic, especially Dr Stephen Kennett, for their assistance with recruiting. This study received funding from the Flinders Foundation (South Australia), awarded to DJS, LH, and RA.
Disclosure
DJS receives salary from NeuroFlex Inc., which is a concussion management platform; however, this work occurred prior to DJS receiving salary from NeuroFlex, and is unrelated to the work of NeuroFlex. LH receives salary from the Aspetar Orthopedic and Sports Medicine Hospital, where he treats concussion. RA reports grants from Flinders Foundation and National Health and Medical Research Council. SA and KB report no conflicts of interest in this work.
References
1. Meaney DF, Smith DH. Biomechanics of concussion. Clin Sports Med. 2011;30(1):19–31, vii. doi:10.1016/j.csm.2010.08.009
2. Choe MC, Giza CC. Diagnosis and management of acute concussion. Semin Neurol. 2015;35(1):29–41. doi:10.1055/s-0035-1544243
3. Stein TD, Montenigro PH, Alvarez VE, et al. Beta-amyloid deposition in chronic traumatic encephalopathy. Acta Neuropathol. 2015;130(1):21–34. doi:10.1007/s00401-015-1435-y
4. Kylkilahti TM, Berends E, Ramos M, et al. Achieving brain clearance and preventing neurodegenerative diseases-A glymphatic perspective. J Cereb Blood Flow Metab. 2021;41(9):2137–2149. doi:10.1177/0271678x20982388
5. Ooms S, Overeem S, Besse K, Rikkert MO, Verbeek M, Claassen JAHR. Effect of 1 night of total sleep deprivation on cerebrospinal fluid β-amyloid 42 in healthy middle-aged men a randomized clinical trial. Article. JAMA Neurol. 2014;71(8):971–977. doi:10.1001/jamaneurol.2014.1173
6. Stevens DJ, Alghwiri A, Appleton SL, et al. Should we lose sleep over sleep disturbances after sports-related concussion? A scoping review of the literature. J Head Trauma Rehabil. 2022;37(3):E206–E219. doi:10.1097/htr.0000000000000701
7. Raikes AC, Schaefer SY. Sleep quantity and quality during acute concussion: a pilot study. Sleep. 2016;39(12):2141–2147. doi:10.5665/sleep.6314
8. Hoffman NL, O’Connor PJ, Schmidt MD, Lynall RC, Schmidt JD. Differences in sleep between concussed and nonconcussed college students: a matched case-control study. Sleep. 2019;42(2). doi:10.1093/sleep/zsy222
9. Gosselin N, Lassonde M, Petit D, et al. Sleep following sport-related concussions. Article. Sleep Med. 2009;10(1):35–46. doi:10.1016/j.sleep.2007.11.023
10. Rao V, Bergey A, Hill H, Efron D, McCann U. Sleep disturbance after mild traumatic brain injury: indicator of injury? J Neuropsychiatry Clin Neurosci. 2011;23(2):201–205. doi:10.1176/jnp.23.2.jnp201
11. Mantua J, Henry OS, Garskovas NF, Spencer RMC. Mild traumatic brain injury chronically impairs sleep- and wake-dependent emotional processing. Sleep. 2017;40(6). doi:10.1093/sleep/zsx062
12. Boulos MI, Jairam T, Kendzerska T, Im J, Mekhael A, Murray BJ. Normal polysomnography parameters in healthy adults: a systematic review and meta-analysis. Lancet Respir Med. 2019;7(6):533–543. doi:10.1016/s2213-2600(19)30057-8
13. Mathias JL, Alvaro PK. Prevalence of sleep disturbances, disorders, and problems following traumatic brain injury: a meta-analysis. Sleep Med. 2012;13(7):898–905. doi:10.1016/j.sleep.2012.04.006
14. Lucey BP, McLeland JS, Toedebusch CD, et al. Comparison of a single-channel EEG sleep study to polysomnography. J Sleep Res. 2016;25(6):625–635. doi:10.1111/jsr.12417
15. McCrory P, Meeuwisse W, Dvořák J, et al. Consensus statement on concussion in sport-The 5(th) international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med. 2017;51(11):838–847. doi:10.1136/bjsports-2017-097699
16. Hänninen T, Parkkari J, Howell DR, et al. Reliability of the sport concussion assessment tool 5 baseline testing: a 2-week test-retest study. J Sci Med Sport. 2021;24(2):129–134. doi:10.1016/j.jsams.2020.07.014
17. Gavett BE, Stern RA, McKee AC. Chronic traumatic encephalopathy: a potential late effect of sport-related concussive and subconcussive head trauma. Clin Sports Med. 2011;30(1):179–188. doi:10.1016/j.csm.2010.09.007
18. Morawska MM, Buchele F, Moreira CG, Imbach LL, Noain D, Baumann CR. Sleep modulation alleviates axonal damage and cognitive decline after rodent traumatic brain injury. J Neurosci. 2016;36(12):3422–3429. doi:10.1523/jneurosci.3274-15.2016
19. Fleming MK, Smejka T, Henderson Slater D, et al. Sleep disruption after brain injury is associated with worse motor outcomes and slower functional recovery. Neurorehabil Neural Repair. 2020;34(7):661–671. doi:10.1177/1545968320929669
20. Giza CC, Hovda DA. The new neurometabolic cascade of concussion. Neurosurgery. 2014;75 Suppl 4(4):S24–S33. doi:10.1227/neu.0000000000000505
21. Buman MP, King AC. Exercise as a treatment to enhance sleep. Am J Lifestyle Med. 2010;4(6):500–514. doi:10.1177/1559827610375532
22. Alvaro PK, Roberts RM, Harris JK. A systematic review assessing bidirectionality between sleep disturbances, anxiety, and depression. Sleep. 2013;36(7):1059–1068. doi:10.5665/sleep.2810
23. de Mendonça FMR, de Mendonça G, Souza LC, et al. Benzodiazepines and sleep architecture: a systematic review. CNS Neurol Disord Drug Targets. 2023;22(2):172–179. doi:10.2174/1871527320666210618103344
24. Williams RL, Agnew HW, Webb WB. Sleep patterns in you adults: an EEG study. Electroencephalogr Clin Neurophysiol. 1964;17:376–381. doi:10.1016/0013-4694(64)90160-9
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.