Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Electroencephalogram alpha asymmetry in patients with depressive disorders: current perspectives
Authors Kaiser AK, Gnjezda MT, Knasmüller S, Aichhorn W
Received 22 December 2017
Accepted for publication 10 April 2018
Published 11 June 2018 Volume 2018:14 Pages 1493—1504
DOI https://doi.org/10.2147/NDT.S137776
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Andreas Kurt Kaiser,1 Maria-Theresa Gnjezda,1 Stephanie Knasmüller,1 Wolfgang Aichhorn2
1Department of Clinical Psychology, Salzburger Landeskliniken Betriebs-GesmbH, Christian-Doppler-Klinik, Paracelsus Medical University, Salzburg, Austria; 2Department of Psychiatry, Salzburger Landeskliniken Betriebs-GesmbH, Christian-Doppler-Klinik, Paracelsus Medical University, Salzburg, Austria
Purpose: Electroencephalogram (EEG) alpha asymmetry (AA) in depressive disorders has been of interest over the last few decades, but it continues to remain unclear whether EEG AA can discriminate between healthy and depressive individuals.
Materials and methods: A systematic literature search for papers addressing EEG AA using the keywords alpha asymmetry, depression, and EEG was performed in PubMed. All studies were checked for sample size, gender, handedness, reference, recording protocol, EEG band range, impedance, type of analysis, drugs, and comorbidity.
Results: A total of 61 articles were found, of which 44 met our inclusion criteria. They have been consecutively analyzed in respect of methodology and results. Approximately 25% (11/44) of the studies did not mention or ignored handedness, 41% (18/44) of the studies used data with only self-reported handedness, and only 34.1% (15/44) of all studies tested handedness. Only 35% (15/44) of the studies reported pharmacological treatment, and only 35% (15/44) of the studies controlled for medication. A total of 52% (23/44) of the studies reported comorbidity, and only 30% (13/44) of the studies controlled for comorbidity. Only 29.6% (13/44) of the studies reported education. In all, 30.5% (13/44) of the studies analyzed group differences and correlations, while 15.9 (7/44) of the studies used only correlational analyses. A total of 52.3% (23/44) of the studies analyzed only group differences. Alpha range was fixed (8–13 Hz) in 59.1% (26/44) of all studies. Reference to common average was used in seven of 44 studies (15.9%). In all, nine of 44 (20.5%) studies used the midline central position as reference, 22 of 44 (50%) studies used the ear or the mastoid as reference, and four of 44 (9.1%) studies used the nose as reference.
Conclusion: Discriminative power of EEG AA for depressed and healthy controls remains unclear. A systematic analysis of 44 studies revealed that differences in methodology and disregarding proper sampling are problematic. Ignoring handedness, gender, age, medication, and comorbidity could explain inconsistent findings. Hence, we formulated a guideline for requirements for future studies on EEG AA in order to allow for better comparisons.
Keywords: alpha asymmetry, depression, electroencephalogram, EEG, depressive disorders, review
Introduction
Over the last few decades, a lot of research concerning electroencephalogram (EEG) alpha asymmetry (AA) in depressive disorders (DD) has been conducted. EEG is of interest in respect of diagnosis of DD, with a special focus on frontal EEG AA,1,2 as it is believed to be a useful biomarker for depression.1–3 EEG AA is usually calculated by subtracting the right-side EEG power estimates from the respective counterpart on the other side. While normal controls have more right-sided frontal alpha power, depressive patients seem to have comparatively higher left frontal alpha power.1,2,4 Cortical activity is related to reduced EEG power, which is reflected in left frontal hypoactivation in depressed subjects and as a deficit in approach mechanisms.5 On the other hand, higher alpha power could be interpreted as correlate of active inhibition rather than cognitive idleness.6–8 Several meta-analyses attempted to shed light on the usefulness of EEG AA for diagnostic purposes.9,10 While Gold et al8 concluded that there is sufficient reliability of frontal AA, correlations with depression scales were small and nonsignificant. The most recent meta-analysis including 883 major depressed patients and 2,161 controls found only a nonsignificant effect size for EEG AA in respect of major DD.10 Gender, age, and severity of depression were especially identified as covariates of EEG AA.10
While many studies focus on depressive symptoms, there are, however, several subtypes of DD in terms of symptoms, duration, and etiology. In clinical routine, DD are diagnosed by a physician using ICD-10,11 Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV),12 or Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V)13 criteria. Depression scales are common for further specification of symptomatology and as diagnostic tools.
Another issue worth considering is the fact that most studies include only young patients,14 and studies including older individuals were not able to replicate the diagnostic validity of EEG AA.15–17 One major problem in this context might be publication bias, which makes it hard to publish negative results on EEG AA and leads to overinterpretation of results. Another interesting aspect is the fact that most studies deal with female individuals and not with males. Since frontal AA was found to be more consistent in women,18 many studies focus only on females.
While age and gender data are easily obtained, handedness needs specific testing. Simple verbal information about the presumed handedness does not give valid information about hemispheric lateralization. The Edinburgh Handedness Inventory19 can be used for proper documentation. Jesulola et al20 did not report handedness and argued that hemispheric brain dominance is not only determined by handedness. Approximately 61%–70% of left-handed people have left hemispheric dominance.21,22 As mentioned before, age seems to be a covariate of EEG AA, which raises the question if cognition is also a covariate. Cognition of participants is mostly ignored, although evidence for alpha 1 power correlation with cognitive abilities was found.23 Alpha power and theta power are correlated with memory decline24,25 and cognitive decline.26 Aging must be considered in respect of EEG AA, as there are specific age-related changes that could explain why EEG AA changes are not found in geriatric patients.16 One important theory, the right hemi-aging hypothesis, proposes that the right hemisphere is more affected by age-related changes.27 This kind of hemispheric difference could also affect AA. Cabeza28 established the “hemispheric asymmetry reduction in old adults” model, which assumes that hemispheric asymmetry is reduced during cognitive performance and reflects compensatory mechanisms. A third theory named “compensation-related utilisation of neural circuits hypothesis” states that elderly individuals activate additional brain regions not only from the contralateral hemisphere.29 Closely related to cognitive ability is education, which could be easily ascertained and might as well affect EEG measures. Furthermore, educational biases between groups need to be ruled out in addition to gender, age, and cognition. Even sexual motivation seems to affect frontal AA,30 expressed in a positive relationship between self-reported mental sexual arousal and a more left-sided AA. While most studies report findings on EEG AA, it is hard to find a consensus on what the alpha band range is. Some studies use fixed ranges, while others use individual alpha bands.31 Evidence for age-related individual alpha frequency changes can be found, and also for smaller amplitudes in older adults.32 Controlling for drugs is another important possible confounder in studies on EEG AA. While many studies15,16,85 describe medication taken by the probands, any effects on the recorded EEG are simply ignored.
Summarizing the findings on EEG AA, it becomes evident that diagnostic validity is limited. One reason for this limitation could be the poor quality of some studies on EEG AA; also sample selection seems to affect the outcome. The aim of this review was to sum up methods used in studies on EEG AA and discuss potential flaws, which devalue the outcome and cannot help to shed light on the diagnostic validity of EEG AA. Not only handedness, gender, age, and education ought to be addressed but also culture, medication, and cognition need to be considered. A list of minimal requirements needs to be created in order to improve the quality of future studies on EEG AA and make the results comparable.
Materials and methods
Search procedure and characteristics of identified studies
On 13 July 2017, a search of PubMed was conducted using the combination of the following keywords in title and abstract: alpha asymmetry, depression, and EEG. Overall, the search resulted in finding 61 articles. Only studies that determined asymmetry on the basis of EEG data were included. Inclusion criteria for this review were a focus on EEG AA and affective disorders. Studies whose research focus was on the analysis of other EEG correlates instead of AA and/or other mental disorders or main symptoms that did not include depression symptoms were excluded. No study was excluded due to methodological limitations, but rather because it missed the proposed research topic. In the next step, cultural background, type of study, sample size, percentage of right-handers, and number of female participants were collected. Furthermore, we collected data on education, reference style, recording protocol and length, as well as impedance and alpha band range. Moreover, “controlling for handedness” and “controlling for drugs” were added. All collected data were transferred to Microsoft Excel 2016. Descriptive data analysis was performed using IBM SPSS Statistics 24.
Results
A total number of 61 publications were found using the following search criteria in PubMed (https://www.ncbi.nlm.nih.gov/pubmed/): (alpha asymmetry[Title/Abstract]) AND (depression[Title/Abstract]) AND (eeg[Title/Abstract]).
In all, 17 studies were excluded from further analysis since they did not fully meet search criteria.33–49 From the remaining 44 studies published between 1996 and 2017, we collected data on the methods used.
Topical heterogeneity of included literature
While all studies included in this study addressed EEG AA in DD, most of the studies tried to test the validity of EEG AA as a surrogate marker for depression and claimed to show evidence for that.4,50–56 Some of the studies addressed specific topics such as melancholia and EEG AA.57 It is inferred that it remains unclear whether this can be used as a surrogate marker or not.8,10,20,58 Anxiety was found to be correlated with the most evident relative change in frontal alpha asymmetry in one study.54 Some studies only proved EEG AA findings for anxiety and not for depression.59 EEG AA changes were found only in schizophrenia and depression and not in other clinical disorders.60 In addition, a general decrease in EEG power in all frequency bands in depression61 as well as a lowered frontal EEG power in rumination was found.62 Shyness was also a criterion and was able to predict greater relative right frontal AA only after controlling for depressive mood63 and self-esteem, which was found to be a mediator of EEG AA only in its explicit type.64 In suicide attempters, greater alpha power over the left hemisphere was found.65 One study addressed activity level in general, which might be correlated to EEG AA.66 Some interventional studies also proved a shift in EEG AA.35,67–69 A prediction of the course of depression was not possible with EEG AA.70 There was also a focus on whether EEG AA is a state or trait marker for depression,16,71,72 which still remains undetermined.72 A large number of the studies were not able to prove the diagnostic reliability of EEG AA.73–75 In particular, findings on correlations between depression scores and EEG AA were inconsistent.8,79 Studies that addressed age had difficulties in validating previous findings on EEG AA.16,17,80 Especially in young people and the oldest olds, previous EEG AA findings were not able to be replicated.16,17 Other factors such as cortical thickness as a mediator of AA could be ruled out.81 Cognition was discussed as a possible moderator of EEG AA.15–17,82,83 Hereditary effects might play a role,84 but it was found that less left frontal activity at lateral sites was only associated with lifetime major depressive disorder (MDD) in offspring and not in parental MDD.47 The issue of drug effects on EEG AA was discussed.85 It was also argued that conventional EEG analysis lacks temporal and spatial precision.56
Methodological analysis
In Table 1, a comparison of methods in all publications is provided. While most studies tried to focus on EEG AA correlates of depression, the samples were small and, in many cases, not representative. Using students as probands is common as is the use of nonclinical samples. A transfer of the evidence data to clinical patients is often not possible since no clinical samples were used for analysis. Most of the studies used only female participants. The classification of depressive status was measured using depression scores or symptom ratings according to ICD-10 and DSM-IV. Recording length varied between 2 and 8 minutes. The reference points for EEG measurement were placed on the ear, mastoid, nose, or the midline central position (Cz) in most of the studies. In detail, reference to common average (CA) was used in seven of 44 studies (15.9%), while nine of 44 (20.5%) studies used Cz as reference. Half of all studies (22/44) used the ear or the mastoid as reference, and four of 44 (9.1%) studies used the nose as reference.
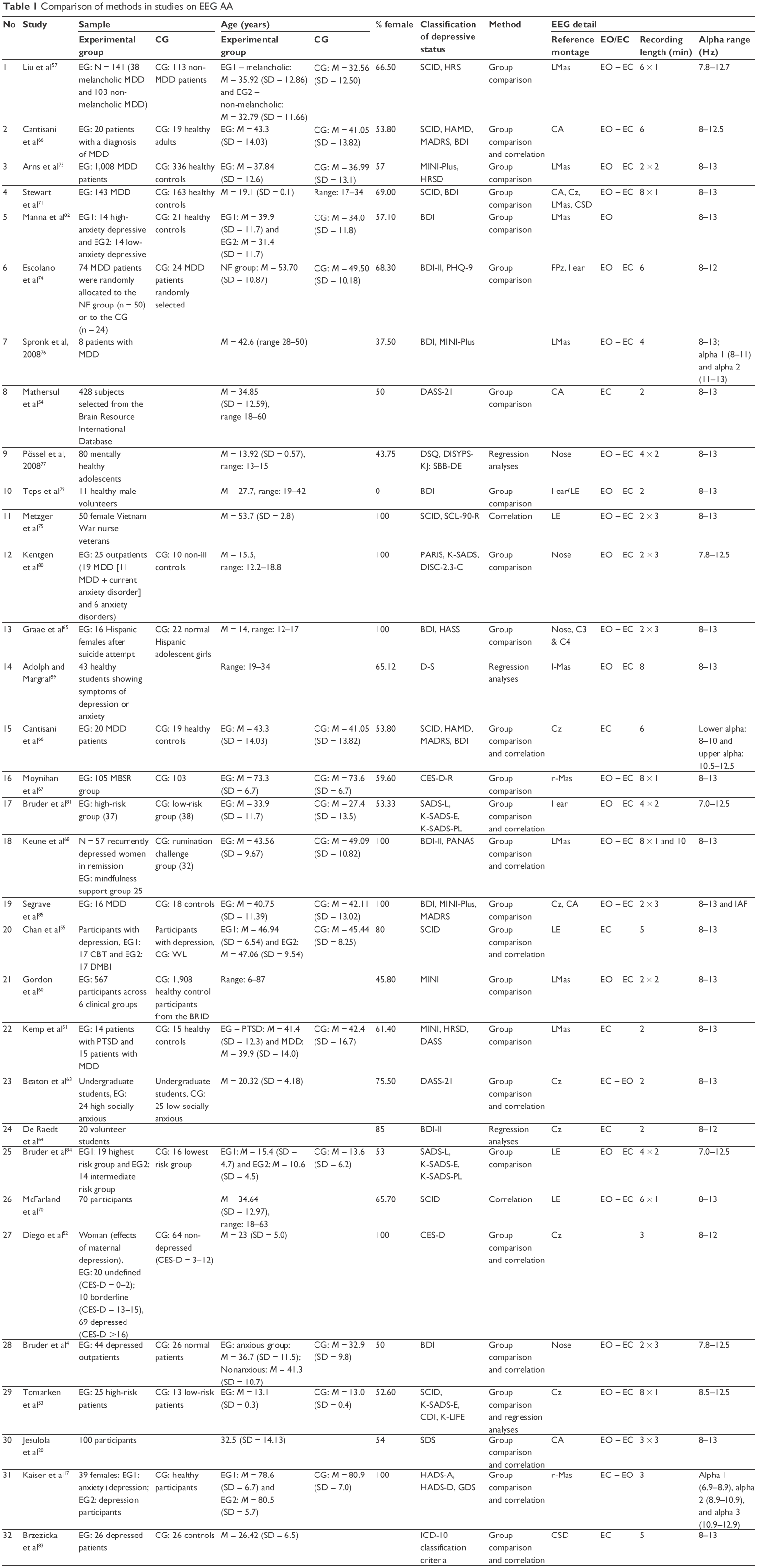 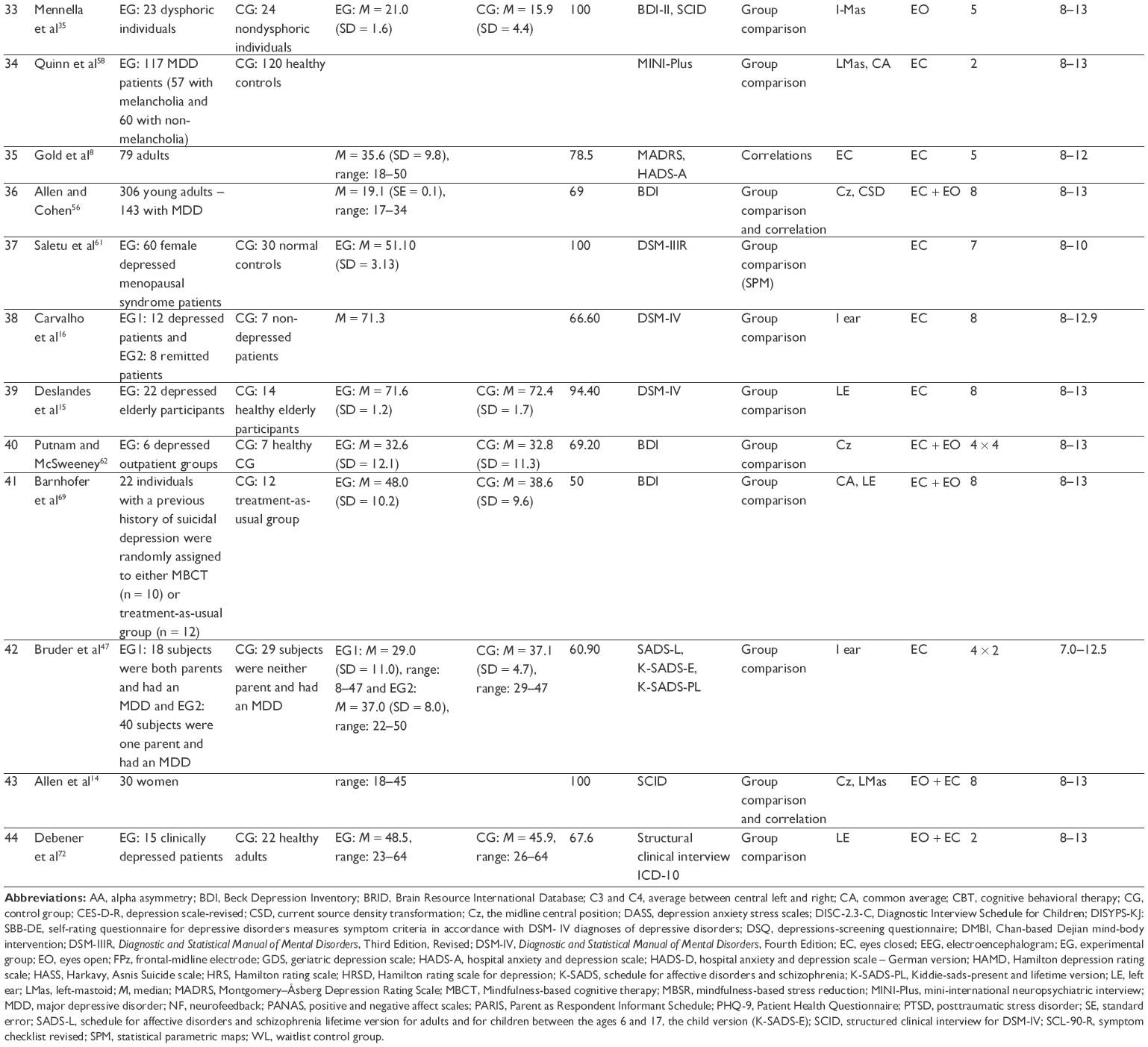 | Table 1 Comparison of methods in studies on EEG AA |
Re-referencing was also common in some cases. Statistical analysis relied on correlational analysis and analyses of variance (ANOVAs) in most of the studies. Analysis of group differences and correlation was performed in 30.5% of studies, correlational analysis was performed only in 15.9% of studies, and group differences were performed in 52.3% of studies. The alpha band range was mostly fixed at 8–13 Hz (26/44 studies). Concerning the controlling for common known confounders (Table 2), we found that 11 of 44 studies did not mention or even ignored the handedness of the participants. Only 15 studies relied on data of participants with tested handedness, while 18 studies relied on self-reported handedness. Regarding pharmacological treatment, only 15 of 44 (35%) studies reported this, and only 35% of the studies controlled for drugs in statistical analysis. Comorbidity was reported in 52% studies, and 30% studies controlled for it. Educational status was reported in 29.6% of all studies. Only nine of 44 (20.5%) studies included an additional task condition in the recording protocol. No study controlled for all common known confounders (Table 2).
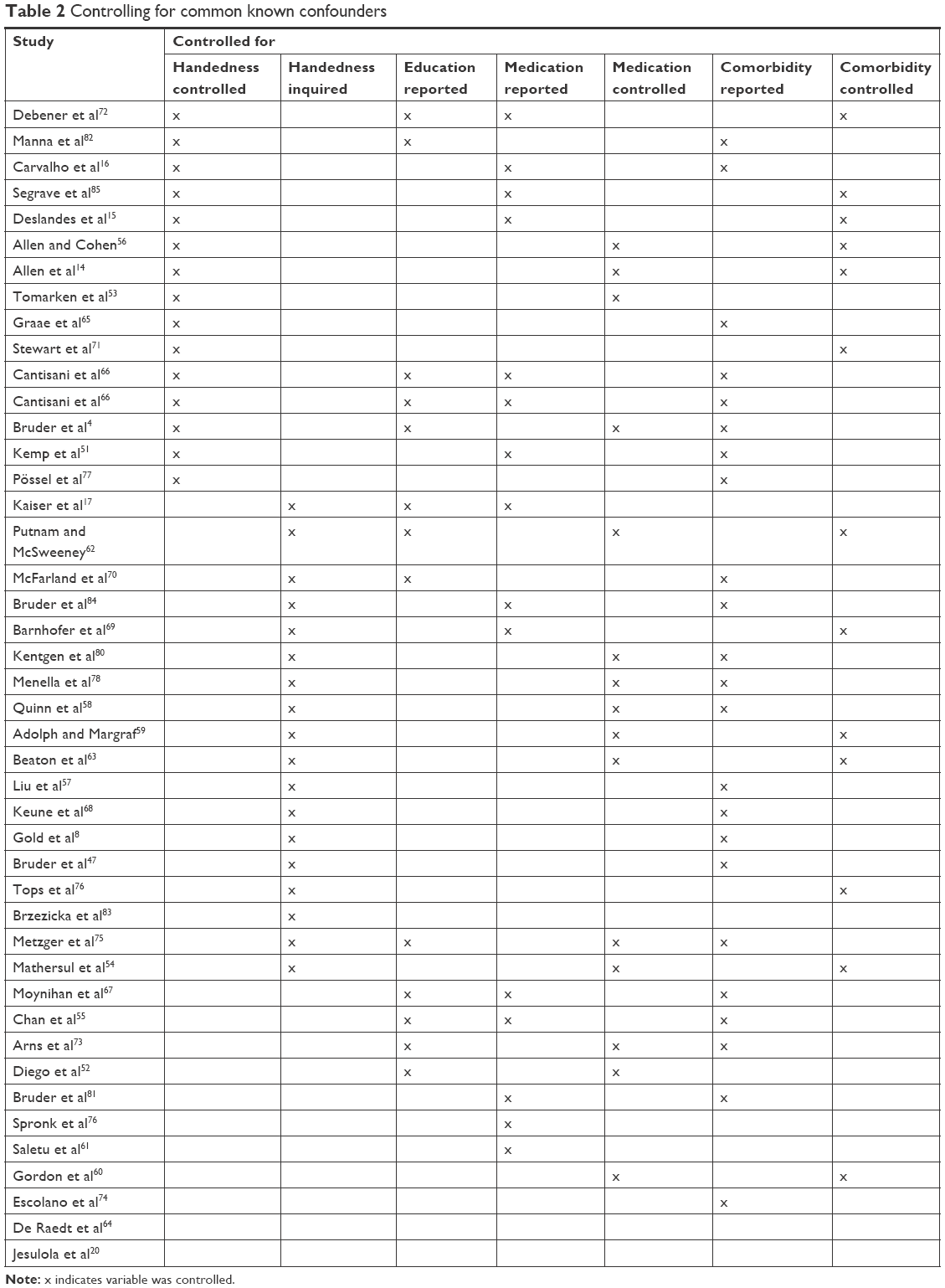 | Table 2 Controlling for common known confounders |
Discussion
We conducted a systematic review on EEG AA in patients with DD, which is still discussed as a possible biomarker for depression.1–3 However, the use of EEG AA as a surrogate marker for depression still remains unclear,9,10 which is not surprising if we take a closer look on the methodological quality of studies concerning EEG AA. The issues of small sample sizes and quality have been discussed repeatedly.8–10 In our analysis, we found that many studies on EEG AA do not consider common known confounders, which could have a tremendous effect on the recorded EEG data.
Taking a closer look at meta-analyses,9,10 we found that most of the analyzed studies differ in sample age, education, gender, handedness, medication, clinical symptoms and severity, and comorbidity. EEG AA was tested as a biomarker for melancholia,57 with unclear validity.8,10,20,58 EEG AA seems to be the most robust in anxiety.54,59 In depression, a general decrease in EEG power can be found,61 which is a sign of cortical activity. This can also be found in rumination.62 Interventional studies have also been analyzed, which could prove a shift in EEG AA.35,67–69
Future studies on EEG AA need to focus on specific changes in the course of depression, which could also help answer the question if EEG AA is a state or trait marker for depression, which still remains unclear.72 If EEG AA is used as a diagnostic measure for clinical depression, we will need normative data. A simple lateralization measure of activity or idleness in the brain cannot be used across different genders, age, educational levels, left- and right-handedness, and medicated and not medicated individuals. In comparison to common correlational analysis and group comparison with ANOVAs, modern statistical analysis methods, such as peri-burst metrics, could help overcome the lack of temporal and spatial precision.56
A consensus of proper sampling and controlling for confounders has to be found in order to validate or reject the hypothesis of EEG as a surrogate marker or marker for treatment response. The following section lists the minimal requirements for studies on EEG AA.
Guidelines for future studies on AA
Future studies on EEG AA ought to include the following commonly known confounders and recording protocols (controlling implies statistical consideration):
- clinical samples;
- controlling for handedness with a handedness inventory (eg, Edinburgh Handedness Inventory);
- controlling for drugs and point of taking;
- controlling for gender;
- controlling for age;
- controlling for cognition with cognitive test or screening;
- controlling for education;
- controlling for comorbidity with clinical screening; and
- EEG protocol including task and resting state condition.
Conclusion
We conducted a literature search on EEG AA in DD and found that methodological flaws could account for the unclear results. Some of the studies do not take into consideration commonly known confounders such as education, age, gender, handedness, drugs, and comorbidity. We have designed a list of requirements to improve the quality of future studies on EEG AA, thus allowing a better comparison of results.
Author contributions
AK Kaiser was responsible for conception and design of the study and analysis of the review. He was also responsible for most of the written text and final approval. M-T Gnjezda was responsible for the concept, aquisition of data, and interpretation of the review. S Knasmüller was responsible for the concept and analysis of the review and tables. W Aichhorn was responsible for the concept and analysis of the review. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Henriques JB, Davidson RJ. Regional brain electrical asymmetries discriminate between previously depressed and healthy control subjects. J Abnorm Psychol. 1990;99(1):22–31. | ||
Schaffer CE, Davidson RJ, Saron C. Frontal and parietal electroencephalogram asymmetry in depressed and nondepressed subjects. Biol Psychiatry. 1983;18(7):753–762. | ||
Leiser SC, Dunlop J, Bowlby MR, Devilbiss DM. Aligning strategies for using EEG as a surrogate biomarker: a review of preclinical and clinical research. Biochem Pharmacol. 2011;81(12):1408–1421. | ||
Bruder GE, Fong R, Tenke CE, et al. Regional brain asymmetries in major depression with or without an anxiety disorder: a quantitative electroencephalographic study. Biol Psychiatry. 1997;41(9):939–948. | ||
Henriques JB, Davidson RJ. Left frontal hypoactivation in depression. J Abnorm Psychol. 1991;100(4):535–545. | ||
Cooper NR, Croft RJ, Dominey SJ, Burgess AP, Gruzelier JH. Paradox lost? Exploring the role of alpha oscillations during externally vs. internally directed attention and the implications for idling and inhibition hypotheses. Int J Psychophysiol. 2003;47(1):65–74. | ||
Klimesch W, Sauseng P, Hanslmayr S. EEG alpha oscillations: the inhibition-timing hypothesis. Brain Res Rev. 2007;53(1):63–88. | ||
Gold C, Fachner J, Erkkila J. Validity and reliability of electroencephalographic frontal alpha asymmetry and frontal midline theta as biomarkers for depression. Scand J Psychol. 2013;54(2):118–126. | ||
Thibodeau R, Jorgensen RS, Kim S. Depression, anxiety, and resting frontal EEG asymmetry: a meta-analytic review. J Abnorm Psychol. 2006;115(4):715–729. | ||
van der Vinne N, Vollebregt MA, Arns M. Frontal alpha asymmetry in depression: fact or fiction? A meta-analysis. Neuroimage Clin. 2017;16:79–87. | ||
Dilling H, Mombour W, Schmidt MH, Organization WH. Internationale Klassifikation psychischer Störungen: ICD-10. (Kapitel V). F, klinisch-diagnostische Leitlinien; 1991. [International classification of diseases: ICD-10 Chapter V (F), Clinical-diagostic Guidelines, World Health Organization]. Bern: Huber. German. | ||
Saß H, Wittchen H-U, Zaudig M, Houben I. American Psychiatric Association. Diagnostisches und statistisches Manual psychischer Störungen DSM-IV: übersetzt nach der vierten Auflage des Diagnostic and statistical manual of mental disorders der American Psychiatric Association. [DSM-IV-TR – Diagnostic and Statistical Manual of Psychiatic Disorders – Textrevision. (2003). Göttingen: Hogrefe. Oxford: Verlag für Psychologie, Göttingen: Hogrefe; 2003. German. | ||
American Psychiatric Association. Diagnostisches und statistisches Manual psychischer Störungen–DSM-5®. [American Psychiatric Association. Diagnostic and statistical manual of mental disorders-5th ed]. Washington, DC: Oxford: Hogrefe Verlag; 2013. German. | ||
Allen JJ, Urry HL, Hitt SK, Coan JA. The stability of resting frontal electroencephalographic asymmetry in depression. Psychophysiology. 2004;41(2):269–280. | ||
Deslandes AC, de Moraes H, Pompeu FA, et al. Electroencephalographic frontal asymmetry and depressive symptoms in the elderly. Biol Psychol. 2008;79(3):317–322. | ||
Carvalho A, Moraes H, Silveira H, et al. EEG frontal asymmetry in the depressed and remitted elderly: is it related to the trait or to the state of depression? J Affect Disord. 2011;129(1–3):143–148. | ||
Kaiser AK, Doppelmayr M, Iglseder B. Electroencephalogram alpha asymmetry in geriatric depression: valid or vanished? Z Gerontol Geriatr. 2016;51(2):200–205. | ||
Stewart JL, Bismark AW, Towers DN, Coan JA, Allen JJ. Resting frontal EEG asymmetry as an endophenotype for depression risk: sex-specific patterns of frontal brain asymmetry. J Abnorm Psychol. 2010;119(3):502–512. | ||
Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia. 1971;9(1):97–113. | ||
Jesulola E, Sharpley CF, Agnew LL. The effects of gender and depression severity on the association between alpha asymmetry and depression across four brain regions. Behav Brain Res. 2017;321:232–239. | ||
Segalowitz SJ, Bryden M. Individual differences in hemispheric representation of language. In: Language Functions and Brain Organization. NY: Academic Press, Inc; 1983:341–372. | ||
Clarke C. Neurology: A Queen Square Textbook. Hoboken: John Wiley & Sons; 2016. | ||
Gianotti LR, Kunig G, Lehmann D, et al. Correlation between disease severity and brain electric LORETA tomography in Alzheimer’s disease. Clin Neurophysiol. 2007;118(1):186–196. | ||
Klimesch W. EEG alpha and theta oscillations reflect cognitive and memory performance: a review and analysis. Brain Res Brain Res Rev. 1999;29(2–3):169–195. | ||
Hanslmayr S, Staudigl T, Fellner MC. Oscillatory power decreases and long-term memory: the information via desynchronization hypothesis. Front Hum Neurosci. 2012;6:74. | ||
van der Hiele K, Vein AA, Reijntjes RH, et al. EEG correlates in the spectrum of cognitive decline. Clin Neurophysiol. 2007;118(9):1931–1939. | ||
Dolcos F, Rice HJ, Cabeza R. Hemispheric asymmetry and aging: right hemisphere decline or asymmetry reduction. Neurosci Biobehav Rev. 2002;26(7):819–825. | ||
Cabeza R. Hemispheric asymmetry reduction in older adults: the HAROLD model. Psychol Aging. 2002;17(1):85–100. | ||
Berlingeri M, Danelli L, Bottini G, Sberna M, Paulesu E. Reassessing the HAROLD model: is the hemispheric asymmetry reduction in older adults a special case of compensatory-related utilisation of neural circuits? Exp Brain Res. 2013;224(3):393–410. | ||
Prause N, Staley C, Roberts V. Frontal alpha asymmetry and sexually motivated states. Psychophysiology. 2014;51(3):226–235. | ||
Doppelmayr M, Klimesch W, Pachinger T, Ripper B. Individual differences in brain dynamics: important implications for the calculation of event-related band power. Biol Cybern. 1998;79(1):49–57. | ||
Purdon PL, Pavone KJ, Akeju O, et al. The ageing brain: age-dependent changes in the electroencephalogram during propofol and sevoflurane general anaesthesia. Br J Anaesth. 2015;115(suppl 1):i46–i57. | ||
Reznik SJ, Nusslock R, Pornpattananangkul N, Abramson LY, Coan JA, Harmon-Jones E. Laboratory-induced learned helplessness attenuates approach motivation as indexed by posterior versus frontal theta activity. Cogn Affect Behav Neurosci. 2017;17(4):904–916. | ||
Bruder GE, Stewart JW, McGrath PJ. Right brain, left brain in depressive disorders: clinical and theoretical implications of behavioral, electrophysiological and neuroimaging findings. Neurosci Biobehav Rev. 2017;78:178–191. | ||
Mennella R, Patron E, Palomba D. Frontal alpha asymmetry neurofeedback for the reduction of negative affect and anxiety. Behav Res Ther. 2017;92:32–40. | ||
Mobius M, Lacomble L, Meyer T, et al. Repetitive transcranial magnetic stimulation modulates the impact of a negative mood induction. Soc Cogn Affect Neurosci. 2017;12(4):526–533. | ||
Gorka SM, Phan KL, Shankman SA. Convergence of EEG and fMRI measures of reward anticipation. Biol Psychol. 2015;112:12–19. | ||
Mirski A, Pachalska M, Moskala M, et al. Neuromarkers of anxiety and depression in a patient after neuro-ophthalmic surgery of the meningioma – effect of individually-tailored tDCS and neurofeedback. Ann Agric Environ Med. 2015;22(4):718–723. | ||
Moore RD, Sauve W, Ellemberg D. Neurophysiological correlates of persistent psycho-affective alterations in athletes with a history of concussion. Brain Imaging Behav. 2016;10(4):1108–1116. | ||
Baskaran A, Milev R, McIntyre RS. The neurobiology of the EEG biomarker as a predictor of treatment response in depression. Neuropharmacology. 2012;63(4):507–513. | ||
Deslandes AC, Moraes H, Alves H, et al. Effect of aerobic training on EEG alpha asymmetry and depressive symptoms in the elderly: a 1-year follow-up study. Braz J Med Biol Res. 2010;43(6):585–592. | ||
Jesulola E, Sharpley CF, Bitsika V, Agnew LL, Wilson P. Frontal alpha asymmetry as a pathway to behavioural withdrawal in depression: research findings and issues. Behav Brain Res. 2015;292:56–67. | ||
Keune PM, Wiedemann E, Schneidt A, Schonenberg M. Frontal brain asymmetry in adult attention-deficit/hyperactivity disorder (ADHD): extending the motivational dysfunction hypothesis. Clin Neurophysiol. 2015;126(4):711–720. | ||
Kremer H, Lutz FP, McIntosh RC, Devieux JG, Ironson G. Interhemispheric asymmetries and theta activity in the rostral anterior cingulate cortex as EEG signature of HIV-related depression: gender matters. Clin EEG Neurosci. 2016;47(2):96–104. | ||
Meerwijk EL, Ford JM, Weiss SJ. Resting-state EEG delta power is associated with psychological pain in adults with a history of depression. Biol Psychol. 2015;105:106–114. | ||
Meyer T, Smeets T, Giesbrecht T, et al. The role of frontal EEG asymmetry in post-traumatic stress disorder. Biol Psychol. 2015;108:62–77. | ||
Bruder GE, Tenke CE, Warner V, et al. Electroencephalographic measures of regional hemispheric activity in offspring at risk for depressive disorders. Biol Psychiatry. 2005;57(4):328–335. | ||
Gilbert DG, McClernon FJ, Rabinovich NE, et al. EEG, physiology, and task-related mood fail to resolve across 31 days of smoking abstinence: relations to depressive traits, nicotine exposure, and dependence. Exp Clin Psychopharmacol. 1999;7(4):427–443. | ||
Saletu B, Brandstatter N, Metka M, et al. Double-blind, placebo-controlled, hormonal, syndromal and EEG mapping studies with transdermal oestradiol therapy in menopausal depression. Psychopharmacology (Berl). 1995;122(4):321–329. | ||
Cantisani A, Koenig T, Stegmayer K, et al. EEG marker of inhibitory brain activity correlates with resting-state cerebral blood flow in the reward system in major depression. Eur Arch Psychiatry Clin Neurosci. 2016;266(8):755–764. | ||
Kemp AH, Griffiths K, Felmingham KL, et al. Disorder specificity despite comorbidity: resting EEG alpha asymmetry in major depressive disorder and post-traumatic stress disorder. Biol Psychol. 2010;85(2):350–354. | ||
Diego MA, Field T, Hernandez-Reif M. CES-D depression scores are correlated with frontal EEG alpha asymmetry. Depress Anxiety. 2001;13(1):32–37. | ||
Tomarken AJ, Dichter GS, Garber J, Simien C. Resting frontal brain activity: linkages to maternal depression and socio-economic status among adolescents. Biol Psychol. 2004;67(1–2):77–102. | ||
Mathersul D, Williams LM, Hopkinson PJ, Kemp AH. Investigating models of affect: relationships among EEG alpha asymmetry, depression, and anxiety. Emotion. 2008;8(4):560–572. | ||
Chan AS, Han YM, Sze SL, Wong QY, Cheung MC. A randomized controlled neurophysiological study of a Chinese Chan-based mind-body intervention in patients with major depressive disorder. Evid Based Complement Alternat Med. 2013;2013:812096. | ||
Allen JJ, Cohen MX. Deconstructing the “resting” state: exploring the temporal dynamics of frontal alpha asymmetry as an endophenotype for depression. Front Hum Neurosci. 2010;4:232. | ||
Liu H, Sarapas C, Shankman SA. Anticipatory reward deficits in melancholia. J Abnorm Psychol. 2016;125(5):631–640. | ||
Quinn CR, Rennie CJ, Harris AW, Kemp AH. The impact of melancholia versus non-melancholia on resting-state, EEG alpha asymmetry: electrophysiological evidence for depression heterogeneity. Psychiatry Res. 2014;215(3):614–617. | ||
Adolph D, Margraf J. The differential relationship between trait anxiety, depression, and resting frontal alpha-asymmetry. J Neural Transm (Vienna). 2017;124(3):379–386. | ||
Gordon E, Palmer DM, Cooper N. EEG alpha asymmetry in schizophrenia, depression, PTSD, panic disorder, ADHD and conduct disorder. Clin EEG Neurosci. 2010;41(4):178–183. | ||
Saletu B, Anderer P, Saletu-Zyhlarz GM. EEG topography and tomography (LORETA) in diagnosis and pharmacotherapy of depression. Clin EEG Neurosci. 2010;41(4):203–210. | ||
Putnam KM, McSweeney LB. Depressive symptoms and baseline prefrontal EEG alpha activity: a study utilizing ecological momentary assessment. Biol Psychol. 2008;77(2):237–240. | ||
Beaton EA, Schmidt LA, Ashbaugh AR, Santesso DL, Antony MM, McCabe RE. Resting and reactive frontal brain electrical activity (EEG) among a non-clinical sample of socially anxious adults: does concurrent depressive mood matter? Neuropsychiatr Dis Treat. 2008;4(1):187–192. | ||
De Raedt R, Franck E, Fannes K, Verstraeten E. Is the relationship between frontal EEG alpha asymmetry and depression mediated by implicit or explicit self-esteem? Biol Psychol. 2008;77(1):89–92. | ||
Graae F, Tenke C, Bruder G, et al. Abnormality of EEG alpha asymmetry in female adolescent suicide attempters. Biol Psychiatry. 1996;40(8):706–713. | ||
Cantisani A, Koenig T, Horn H, Muller T, Strik W, Walther S. Psychomotor retardation is linked to frontal alpha asymmetry in major depression. J Affect Disord. 2015;188:167–172. | ||
Moynihan JA, Chapman BP, Klorman R, et al. Mindfulness-based stress reduction for older adults: effects on executive function, frontal alpha asymmetry and immune function. Neuropsychobiology. 2013;68(1):34–43. | ||
Keune PM, Bostanov V, Hautzinger M, Kotchoubey B. Approaching dysphoric mood: state-effects of mindfulness meditation on frontal brain asymmetry. Biol Psychol. 2013;93(1):105–113. | ||
Barnhofer T, Duggan D, Crane C, Hepburn S, Fennell MJ, Williams JM. Effects of meditation on frontal alpha-asymmetry in previously suicidal individuals. Neuroreport. 2007;18(7):709–712. | ||
McFarland BR, Shankman SA, Tenke CE, Bruder GE, Klein DN. Behavioral activation system deficits predict the six-month course of depression. J Affect Disord. 2006;91(2–3):229–234. | ||
Stewart JL, Coan JA, Towers DN, Allen JJ. Resting and task-elicited prefrontal EEG alpha asymmetry in depression: support for the capability model. Psychophysiology. 2014;51(5):446–455. | ||
Debener S, Beauducel A, Nessler D, Brocke B, Heilemann H, Kayser J. Is resting anterior EEG alpha asymmetry a trait marker for depression? Findings for healthy adults and clinically depressed patients. Neuropsychobiology. 2000;41(1):31–37. | ||
Arns M, Bruder G, Hegerl U, et al. EEG alpha asymmetry as a gender-specific predictor of outcome to acute treatment with different antidepressant medications in the randomized iSPOT-D study. Clin Neurophysiol. 2016;127(1):509–519. | ||
Escolano C, Navarro-Gil M, Garcia-Campayo J, Congedo M, De Ridder D, Minguez J. A controlled study on the cognitive effect of alpha neurofeedback training in patients with major depressive disorder. Front Behav Neurosci. 2014;8:296. | ||
Metzger LJ, Paige SR, Carson MA, et al. PTSD arousal and depression symptoms associated with increased right-sided parietal EEG asymmetry. J Abnorm Psychol. 2004;113(2):324–329. | ||
Spronk D, Arns M, Bootsma A, van Ruth R, Fitzgerald PB. Long term effects of left frontal rTMS on EEG and ERPs in patients with depression. Clin EEG Neurosci. 2008;39(3):118–124. | ||
Pössel P, Lo H, Fritz A, Seemann S. A longitudinal study of cortical EEG activity in adolescents. Biol Psychol. 2008;78(2):173–178. | ||
Mennella R, Benvenuti SM, Buodo G, Palomba D. Emotional modulation of alpha asymmetry in dysphoria: results from an emotional imagery task. Int J Psychophysiol. 2015;97(2):113–119. | ||
Tops M, Wijers AA, van Staveren AS, et al. Acute cortisol administration modulates EEG alpha asymmetry in volunteers: relevance to depression. Biol Psychol. 2005;69(2):181–193. | ||
Kentgen LM, Tenke CE, Pine DS, Fong R, Klein RG, Bruder GE. Electroencephalographic asymmetries in adolescents with major depression: influence of comorbidity with anxiety disorders. J Abnorm Psychol. 2000;109(4):797–802. | ||
Bruder GE, Bansal R, Tenke CE, et al. Relationship of resting EEG with anatomical MRI measures in individuals at high and low risk for depression. Hum Brain Mapp. 2012;33(6):1325–1333. | ||
Manna CB, Tenke CE, Gates NA, et al. EEG hemispheric asymmetries during cognitive tasks in depressed patients with high versus low trait anxiety. Clin EEG Neurosci. 2010;41(4):196–202. | ||
Brzezicka A, Kaminski J, Kaminska OK, Wolynczyk-Gmaj D, Sedek G. Frontal EEG alpha band asymmetry as a predictor of reasoning deficiency in depressed people. Cogn Emot. 2017;31(5):868–878. | ||
Bruder GE, Tenke CE, Warner V, Weissman MM. Grandchildren at high and low risk for depression differ in EEG measures of regional brain asymmetry. Biol Psychiatry. 2007;62(11):1317–1323. | ||
Segrave RA, Cooper NR, Thomson RH, Croft RJ, Sheppard DM, Fitzgerald PB. Individualized alpha activity and frontal asymmetry in major depression. Clin EEG Neurosci. 2011;42(1):45–52. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.