Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Electroconvulsive Therapy Practice in Thailand: A Nationwide Survey
Authors Kittayarak K, Ittasakul P ![]()
Received 9 August 2022
Accepted for publication 14 October 2022
Published 31 October 2022 Volume 2022:18 Pages 2477—2484
DOI https://doi.org/10.2147/NDT.S385598
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yu-Ping Ning
Kannapas Kittayarak, Pichai Ittasakul
Department of Psychiatry, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Pichai Ittasakul, 270 Rama VI Road, Ratchathewi, Bangkok, 10400, Thailand, Tel +662-2011478, Fax +662-200-3277, Email [email protected]
Objective: To determine the characteristics of electroconvulsive therapy (ECT) practice in Thailand.
Methods: A cross-sectional survey of ECT practice in Thailand was conducted. A questionnaire was sent to all 34 hospitals providing ECT services nationwide. ECT staff of each hospital were asked to complete the questionnaire.
Results: All 34 hospitals responded to the survey. The most common diagnosis was schizophrenia (5,958 patients/year), followed by bipolar disorder (982 patients/year) and major depressive disorder (869 patients/year). Brief pulse device was used in all hospitals. Bitemporal ECT was the most common type of electrode placement (88.2%), followed by bifrontal (44.1%) and right unilateral (38.2%) placement. The initial dose was determined by titration method in 24 hospitals (70.6%) and by age-based method in the remainder (29.4%). Modified ECT was always used in 25 hospitals (73.5%), including all university hospitals, 6 psychiatric hospitals (17.6%) and 10 general hospitals (29.4%). The primary anesthetics used were thiopentone (60.7%) and propofol (39.3%). Regarding acute ECT, ECT was performed three times per week in most hospitals (91.2%). The number of acute ECT treatment sessions in most hospitals was in the range of 4– 6. In total, 22 hospitals (64.7%) performed continuation/maintenance ECT. Headache was the most common adverse event, followed by cognitive side effects and myalgia.
Conclusion: ECT practice in Thailand has developed over the past two decades in many aspects. The most notable change is that the majority of patients are now treated with modified ECT. In addition, pre-treatment investigations, use of a device providing a brief pulse, unilateral electrode placement, and the monitoring of parameters during treatment are now used more widely in practice to maximize treatment efficacy while minimizing side effects. However, certain aspects of ECT can still be improved; promoting ECT education among psychiatrists and psychiatry residents could improve the quality of practice, for example.
Keywords: electroconvulsive therapy, acute ECT, continuation ECT, maintenance ECT, survey, Thailand
Introduction
Electroconvulsive therapy (ECT) was introduced in 1938 by Ugo Cerletti and Lucio Bini.1,2 After successful use had been demonstrated, ECT was widely implemented across the world, especially for the treatment of schizophrenia and mood disorders. In the 1950s, psychotropic drugs were introduced, and their use has continually increased ever since. In parallel, the popularity of ECT declined such that it became the treatment of choice only for patients who did not respond to psychotropic drugs, who required rapid symptom control, or who had conditions that respond better to ECT. The practice of ECT varies among countries: Western countries are more likely to use it to treat mood disorders, while it is applied more widely for treating schizophrenia in Asia.3–8 Anesthetic agents and muscle relaxants are more commonly used in the United States and Europe to reduce the negative effects of ECT and reduce the risk of injury, but this is not the case in Asia, Africa, Latin America, or Russia.8 Regardless of country, manufacturers, dosing strategies, and electrode placement vary among hospitals.
In Thailand, ECT was first introduced into clinical practice in 1945 by Professor Arun Paksuwan.9 It was subsequently adopted by some psychiatric, university and general hospitals providing psychiatric services at that time. The first study about general ECT practice in Thailand was conducted in the period 2001–2002.4 Of the 28 hospitals providing ECT services at that time, 2 did not participate in the study. The majority of the patients were seen in psychiatric hospitals because there were more specialists in this field in such institutions. The most prevalent diagnoses of patients selected for ECT were schizophrenia (74%), mania (8%), and depression (7%).4 Electrode placement was bilateral in all cases, and almost all treatments (94.2%) were performed without anesthetic agents because of a lack of equipment, personnel and anesthesiologists, as well as the risks posed by anesthesia, inconvenience, and economic reasons, among others.4 Unmodified ECT can induce dread and anxiety in patients, as well as post-ictal disorientation, fracture, and various other side effects.
Nowadays, more psychiatrists, anesthesiologists and anesthesiology nurses are available. Moreover, there is more knowledge about diseases, treatments, and procedures than ever before. In 2013, a public health policy was established to reduce physical and mental trauma among ECT patients, and to destigmatize the treatment. We believe that the overall practice of ECT in Thailand has evolved markedly since the first survey was conducted 17 years ago, and conducted this study to characterize current ECT practice in Thailand and aid further development of Thai ECT services.
Materials and Methods
Setting and Study Design
The study protocol was approved by the Human Research Ethics Committee of the Faculty of Medicine, Ramathibodi Hospital, Mahidol University (COA. No.: MURA2021/578). We conducted a cross-sectional survey of ECT practice in Thailand in October 2021 by sending a questionnaire to all 34 hospitals in the database of the Psychiatric Association of Thailand. We requested that staff providing ECT services at each hospital complete the questionnaire. Informed consent was obtained from all respondents at the beginning of the survey, which was conducted according to the Declaration of Helsinki and Good Clinical Practice guidelines.10
Questionnaire
The questionnaire (see Supplementary File) was developed inhouse on the basis of a review of the literature3,4,6,7,11–16 and approved by psychiatrists working at Ramathibodi Hospital. The questionnaire was divided into six sections covering the characteristics of ECT services, ECT administration, anesthetic procedures, acute-course ECT, continuation/maintenance ECT, and patient assessments during ECT. The questionnaire, which takes around 30–45 minutes to complete, was originally developed in Thai. The draft questionnaire was sent to staff providing ECT service in our hospital for evaluation of the clarity of the questions and completion time; it was then revised in response to staff comments.
ECT Services
Data pertaining to the ECT services of the hospitals were obtained in the first section of the questionnaire, including case types and diagnoses, indications for ECT, the individual supervising the informed consent process, pre-treatment investigations, the location in which treatments were carried out, and the treatment guidelines (if any). The average number of patients receiving treatment and cost of each session were also determined.
ECT Administration
The ECT administration section includes questions about the person who administered it, the type and brand of ECT device used, electrode placement, pulse width, patient monitoring procedures, and pharmacological management during the treatment.
Anesthetic Procedures
This section contains questions about the anesthetic procedure and use of modified ECT procedures. Information about the person responsible for providing the anesthesia was obtained, as well as the anesthetic agents and muscle relaxants used during the procedure.
Acute-Course ECT
Information about acute-course ECT was obtained, including the average number of treatments done for each diagnosis, intervals between treatments, and the protocol for efficacy evaluation and terminating the course.
Continuation/Maintenance ECT
Information was obtained on continuation/maintenance ECT treatments from hospitals providing this service, including the diagnoses of the patients and whether a specific protocol was followed.
Patient Assessments During ECT
Information about the tools used for symptom and cognitive function assessments during ECT, and the side effects of treatment, was obtained in the final questionnaire section.
Statistical Analysis
Nominal data are summarized as numbers and percentages, while continuous data are summarized as mean ± standard deviation or median and interquartile range, depending on the normality of the data distribution. All statistical analyses were performed using SPSS software (version 26.0 for Windows; IBM Corp., Armonk, NY, USA).
Results
We received responses from all 34 hospitals providing ECT services in Thailand. The hospitals are distributed throughout the country: 10 (29.4%) are in the central part, 11 (32.4%) in the northeastern region, 6 (17.6%) in the northern region, 5 (14.7%) in the southern region, 1 (2.9%) in the eastern region, and 1 (2.9%) the western region. There were 13 (38.2%) psychiatric hospitals, 12 (35.3%) general hospitals, and 9 (26.5%) university hospitals; the average number of psychiatric beds in these three types of hospital is 23 ± 7 (range: 12–30), 305 ± 196 (range: 90–750), and 22 ± 18 (range: 11–70), respectively.
Characteristics of ECT Services
Nineteen hospitals (55.9%) had psychiatrists specifically providing ECT services. Most hospitals (n = 26; 76.5%) had ECT guidelines, especially psychiatric hospitals. Twenty-three hospitals (67.6%) performed ECT on special populations, including patients aged < 12 years (n = 1), adolescents (aged 13–17 years; n = 16), elderly patients (n = 22), and pregnant women (n = 9).
Informed consent for ECT was obtained from patients or family members in all hospitals. In seven psychiatric hospitals, if the patients or their relatives were unable to give consent, the decision to perform ECT was made by institutional committees, in accordance with the Thai Mental Health Act of 2008.
ECT was performed in a special ECT unit in all psychiatric hospitals. In general and university hospitals, ECT was performed in locations including inpatient and outpatient departments, operation rooms, and post-anesthesia care units.
The number of ECT-treated patients per year are shown in Table 1 according to diagnosis. The most common diagnosis was schizophrenia, followed by bipolar disorder and major depressive disorder. Reasons for ECT treatment included drug resistance, high suicidal risk, aggressive behaviors, history of a good response to ECT, poor oral intake, and medication intolerance.
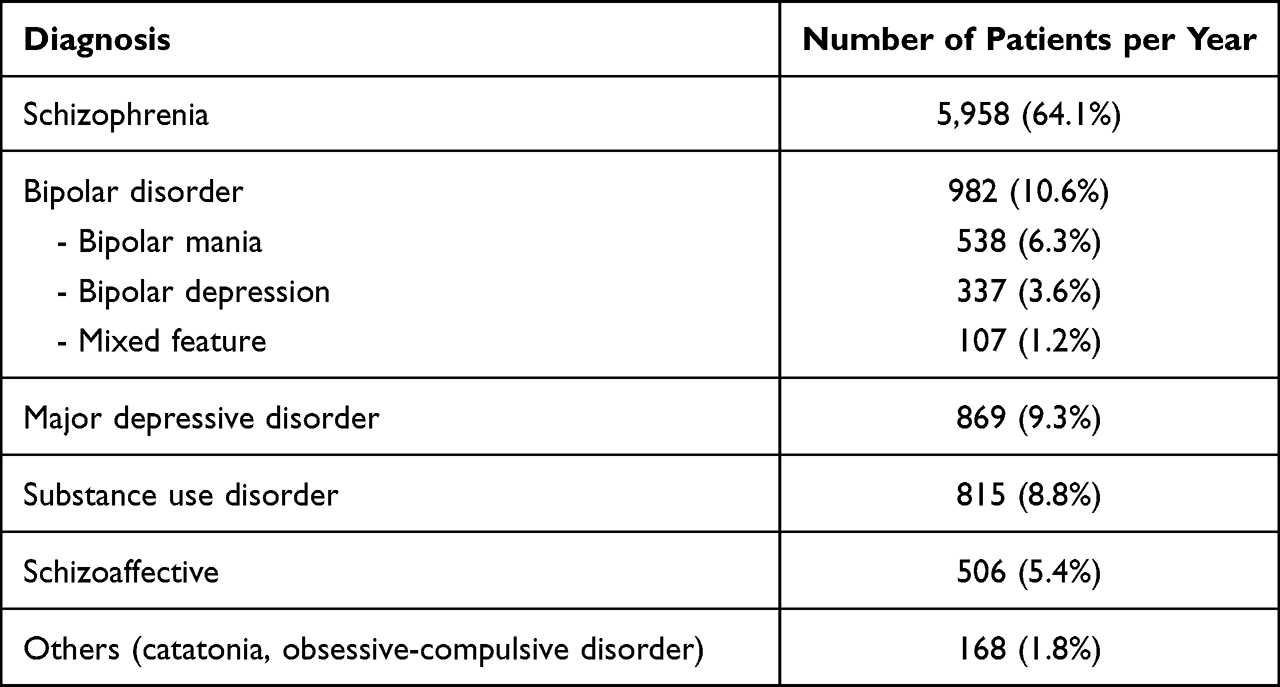 |
Table 1 The Number of ECT-treated Patients per Year in Thailand |
For pre-treatment investigations, a complete blood count (CBC) was routinely ordered in all hospitals. Electrolytes (97.1%, n = 33), renal panels (76.5%, n = 26), electrocardiograms (88.2%, n = 30), and chest X-rays (94.1%, n = 32) were also checked/performed in most hospitals. The liver function and anti-HIV tests, among other investigations, varied among hospitals.
The average price of ECT was 64 ± 33 US dollars (range: 8–152.5 US dollars) per ECT session.
ECT Administration
A psychiatrist or psychiatric resident was responsible for performing ECT and administering the electrical charges in all hospitals. A device providing a brief pulse (0.5–1 ms) was used in all 34 hospitals, although some (8.8%, n = 3) reported using an ultra-brief pulse (0.25–0.3 ms) more frequently. None of the hospitals used devices that can produce sine waves. Device models included spECTrum 5000Q (MECTA, Lake Oswego, OR, USA) (n = 18 hospitals; 52.9%), Thymatron System IV (Somatics, LLC, Lake Bluff, IL, USA) (n = 17; 50%), and spECTrum 5000M (MECTA) (n = 4; 11.8%). The Σigma device (MECTA) was used in one (2.9%) university hospital.
Regarding electrode placement and dosing strategy, bitemporal ECT was the most commonly used approach (n = 30 hospitals; 88.2%). The stimulus intensity was determined by the titration method in most hospitals (n = 24; 70.6%) (Table 2).
 |
Table 2 Electrode Placement and Dosing Strategy |
Reasons for dose increases included inadequate seizure (n = 34 hospitals; 100%) and a lack of clinical improvement (n = 10; 29.4%).
Guidelines for managing patients’ current medications before ECT were followed by 17 hospitals (50%). Among those hospitals, drugs that had to be discontinued before starting the treatment (according to the guidelines) included anticonvulsants (n = 15; 88.2%), benzodiazepines (n = 15; 88.2%), lithium (n = 13; 76.5%), antipsychotics (n = 6; 35.3%), antidepressants (n = 3; 17.6%), and anticholinergics (n = 1; 5.9%). Changes in psychotropic drugs during ECT were made in most hospitals (n = 28; 82.4%).
During ECT, blood pressure, heart rate, and pulse oximetry were monitored in all hospitals, while EEG was monitored in all university hospitals and some of the other hospitals (n = 29; 85.3%). ECG, motor seizures, the bispectral index, and carbon dioxide were monitored in 28 (82.4%), 26 (76.5%), 3 (8.8%), and 4 hospitals (11.8%), respectively.
Modified ECT was always used in 25 hospitals (73.5%), including all university hospitals, 6 psychiatric hospitals (17.6%) and 10 general hospitals (29.4%). Three psychiatric hospitals (8.8%) used both modified and unmodified ECT in certain cases. Two general (5.8%) and four psychiatric hospitals (11.8%) used unmodified ECT in all cases. The reasons for using unmodified ECT are listed in Table 3.
 |
Table 3 Reasons of Unmodified ECT |
Anesthesia in Modified ECT
Preanesthetic assessment and anesthetic procedures were performed by an anesthesiologist or anesthesiology nurse in most hospitals. However, in most psychiatric hospitals, anesthesia was provided by nurse anesthetists only. The primary anesthetics used were thiopentone (n = 17 hospitals; 60.7%) and propofol (n = 11; 39.3%). Ketamine, etomidate, and fentanyl were only used in university hospitals. All hospitals used succinylcholine as the muscle relaxant. Preoxygenation was performed in all except one general hospital. Hyperventilation was performed in 20 hospitals (71.4%). Two hospitals (5.9%) reported the use of endotracheal tube intubation for modified ECT in some cases, such as patients with a difficult airway, pregnancy, or unstable vital signs.
Acute-Course ECT
Regarding acute treatment for schizophrenia or schizoaffective disorder, 21 hospitals reported the use of 4–6 ECT sessions on average; the next most common amount was 10–12 sessions (n = 8 hospitals), followed by 7–9 sessions (n = 6), 1–3 sessions (n = 3), and > 12 sessions (n = 2). For major depressive disorder and bipolar disorder, the pattern was similar, with ECT being performed three times per week in most hospitals (n = 31; 91.2%). The response to ECT was reportedly assessed after 4.4 ± 1.5 sessions, and reasons for discontinuation included intolerable side effects (n = 28; 82.4%), clinical improvement (n = 27; 79.4%), a lack of response to ECT (n = 15; 44.1%), and a plateau in the response (n = 7; 20.6%).
Continuation/Maintenance ECT
In total, 22 (64.8%) hospitals performed continuation/maintenance ECT, most commonly for schizophrenia (followed by bipolar disorder, schizoaffective disorder, major depressive disorder, and organic psychosis). There were no clear guidelines for continuation/maintenance ECT in most hospitals (n = 18; 52.9%).
Assessing Patients During ECT
Eighteen hospitals (52.9%) assessed patients clinically using various assessment tools before and after ECT, fifteen (44.1%) did not perform any assessments and one (2.9%) performed assessments only before treatment. Various assessment tools were used, including the Brief Psychiatric Rating Scale (BPRS),17 Positive and Negative Syndrome Scale (PANSS),18 Young Mania Rating Scale (YMRS),19 Hamilton Depression Rating Scale (HAM-D),20 Montgomery–Åsberg Depression Rating Scale (MADRS),21 Health of the Nation Outcome Scales (HoNOs),22 and Clinical Global Impression (CGI) scale.23 Twelve hospitals assessed patients’ cognitive function using the Thai Mental State Examination (TMSE),24 Mini-Mental State Examination–Thai version (MMSE-Thai)25 and/or Montreal Cognitive Assessment–Thai version (MoCA-T),26 while 22 (64.7%) hospitals did not perform any cognitive assessments. Regarding the side effects of ECT, headache was the most frequent, followed by cognitive side effects and myalgia. Other side effects included cardiovascular problems, delirium, oral cavity trauma, and “others” (eg, falling and bone fractures). No deaths were reported.
Discussion
In this nationwide survey of ECT practice in Thailand, we received responses from all hospitals providing ECT services throughout the country. The study was performed almost 20 years after that of Chanpattana and Kramer,4 which was the first of its kind, and provides an up-to-date picture of ECT practice in Thailand. Currently, 34 hospitals offer ECT services in Thailand, compared with 28 in the previous survey. Even though the hospitals are widely distributed throughout the country, and have increased in number, they remain concentrated in certain areas. For example, 7 of the 10 hospitals in the central part of the country are located in Bangkok. The unequal distribution of hospitals providing ECT services means that accessibility remains relatively low for some people.
According to our results, the most common diagnosis of patients receiving ECT is still schizophrenia (64.1%), followed by bipolar disorder (10.6%) and major depressive disorder (9.3%). These trends are similar to those in Asia overall3,5,14 but differ from those in the USA, Australia and New Zealand, and most other Western countries,8,11–13,15,16 in which affective disorders are more common. The severity of the symptoms of schizophrenia, which require rapid control, may explain the high proportion of such patients in our survey.
Pre-treatment investigations were provided by most of the hospitals in our survey and included CBC, renal panels, electrolyte tests, electrocardiogram, and, if necessary, chest X-ray, similar to many countries in Europe.27 We suggest that standardized guidelines be developed for all hospitals to enhance patient safety during ECT.
Our results showed that modified ECT is being used significantly more often today compared with 2002.4 This can be attributed to increasing numbers of anesthesiologists and anesthesiology nurses, in accordance with public health policy enacted in 2013 to better treat the physical and mental problems of trauma patients and destigmatize ECT. In most of the psychiatric hospitals surveyed herein, anesthesia was performed mainly by anesthesiology nurses, which does not accord with international guidelines.28 The general lack of anesthesiologists in psychiatric hospitals necessitated that nurses be trained to perform anesthetic procedures. According to our survey, thiopental is still the most common anesthetic drug used in Thailand, although the use of propofol has increased. Methohexital remains unavailable.
The number of ECT sessions typically performed was quite low in our survey, inconsistent with a study reporting that an average of 11.8 ± 4.7 sessions were required to achieve remission in Thai psychiatric patients.29 Fifteen of the hospitals surveyed herein cited nonresponse to ECT among the reasons for discontinuation of treatment; we assume that, in some of the cases, treatment may have been stopped too early.
None of the hospitals in our survey used devices that can produce sine waves; brief and ultra-brief pulses were used instead. Regarding the stimulation method, our results indicate that dose titration is being increasingly used. Regarding electrode placement, bilateral ECT was typically used, albeit not exclusively (in contrast to the 2002 survey).4 Unilateral ECT was used to reduce the cognitive side effects of ECT.30
Despite the recommendations of the Royal College of Psychiatrists (London, UK),31 most of the hospitals that we surveyed do not use any tools to monitor patients’ clinical and cognitive function; this is important when evaluating treatment efficacy, and to detect and monitor patients at risk of cognitive impairment.
Some potential limitations of our research should be noted. First, rather than conducting an audit, data were obtained from representative ECT staff at each participating hospital, and the outcomes may not fully reflect real practice. Second, given the self-administered nature of the survey, misinterpretation of certain questions cannot be ruled out. Third, no data were obtained regarding patient characteristics, ECT utilization, the response rate, or difficulties experienced by hospitals in providing ECT services; further research is therefore required.
Conclusions
Our survey showed that ECT practice in Thailand has developed over the past two decades in many aspects. The most notable change is that the majority of patients are now treated with modified ECT. Moreover, pre-treatment investigations, brief pulses, unilateral electrode placement, and monitoring of treatment parameters are being used more often to maximize treatment efficacy while minimizing side effects. However, standard treatment protocols are not being adhered to in all respects; for example, it is likely that acute ECT treatment is being stopped prematurely in some cases. Improving ECT education for psychiatrists and psychiatry residents could improve the standard of care. We suggest that training nurses in the performance of anesthesiology may improve the accessibility of ECT services in some parts of Thailand, given the lack of availability of anesthetists; anesthesia training for psychiatrists could also be an option. The provision of support by the Royal College of Psychiatrists for the implementation of ECT services in certain parts of Thailand would be useful, as would the formation of, and subsequent monitoring of adherence to, standards for ECT. Finally, our research focused on ECT practice before the coronavirus disease 2019 outbreak. Some medical practices, especially ones involving anesthetics, were modified during the pandemic; further study could focus on the impact of the pandemic on ECT practice.
Data Sharing Statement
The data presented in this study are available upon request from the corresponding author.
Informed Consent Statement
All participants provided written informed consent.
Acknowledgments
We would like to thank the staff at the Electroconvulsive Therapy Clinic of Ramathibodi Hospital for their assistance with the data collection, and all other ECT staff who completed the questionnaire. We also thank Michael Irvine, PhD, from Liwen Bianji (Edanz) (www.liwenbianji.cn) for editing the English text of a draft of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors received salary support from Mahidol University, Bangkok, Thailand. Pichai Ittasakul received lecture honoraria from Jassen, Pfizer, and Sumitomo Dainippon Pharma. The authors report no other conflicts of interest in this work.
References
1. Gazdag G, Ungvari GS. Electroconvulsive therapy: 80 years old and still going strong. World J Psychiatry. 2019;9(1):1–6. doi:10.5498/wjp.v9.i1.1
2. Endler NS. The origins of electroconvulsive therapy (ECT). Convuls Ther. 1988;4(1):5–23.
3. Chanpattana W, Kojima K, Kramer BA, Intakorn A, Sasaki S, Kitphati R. ECT practice in Japan. J ECT. 2005;21(3):139–144. doi:10.1097/01.yct.0000169503.80981.c9
4. Chanpattana W, Kramer BA. Electroconvulsive therapy practice in Thailand. J ECT. 2004;20(2):94–98. doi:10.1097/00124509-200406000-00004
5. Chanpattana W, Kramer BA, Kunigiri G, Gangadhar BN, Kitphati R, Andrade C. A survey of the practice of electroconvulsive therapy in Asia. J ECT. 2010;26(1):5–10. doi:10.1097/YCT.0b013e3181a74368
6. Kaliora SC, Braga RJ, Petrides G, Chatzimanolis J, Papadimitriou GN, Zervas IM. The practice of electroconvulsive therapy in Greece. J ECT. 2013;29(3):219–224. doi:10.1097/YCT.0b013e31827e0d49
7. Sienaert P, Dierick M, Degraeve G, Peuskens J. Electroconvulsive therapy in Belgium: a nationwide survey on the practice of electroconvulsive therapy. J Affect Disord. 2006;90(1):67–71. doi:10.1016/j.jad.2005.09.016
8. Leiknes KA, Jarosh-von Schweder L, Høie B. Contemporary use and practice of electroconvulsive therapy worldwide. Brain Behav. 2012;2(3):283–344. doi:10.1002/brb3.37
9. Chanpattana W. One hundred twenty years of mental health care in Thailand and the development of electroconvulsive therapy. J ECT. 2010;26(1):11–13. doi:10.1097/YCT.0b013e3181c185f9
10. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
11. Antosik-Wójcińska AZ, Dominiak M, Mierzejewski P, et al. Changes in the practice of electroconvulsive therapy in Poland: a nationwide survey comparing data between 2005 and 2020. Neuropsychiatr Dis Treat. 2021;17:605–612. doi:10.2147/ndt.S296210
12. Vera I, Sanz-Fuentenebro J, Urretavizcaya M, et al. Electroconvulsive therapy practice in Spain: a national survey. J ECT. 2016;32(1):55–61. doi:10.1097/yct.0000000000000270
13. Sienaert P, Falconieri T, Obbels J, van den Ameele H, Bouckaert F. Improving practice in electroconvulsive therapy: a nationwide survey in Belgium. J ECT. 2016;32(1):29–32. doi:10.1097/yct.0000000000000260
14. Chanpattana W, Kunigiri G, Kramer BA, Gangadhar BN. Survey of the practice of electroconvulsive therapy in teaching hospitals in India. J ECT. 2005;21(2):100–104. doi:10.1097/01.yct.0000166634.73555.e6
15. Chanpattana W. A questionnaire survey of ECT practice in Australia. J ECT. 2007;23(2):89–92. doi:10.1097/YCT.0b013e318031bc50
16. Asztalos M, Ungvari GS, Gazdag G. Changes in electroconvulsive therapy practice in the last 12 years in Hungary. J ECT. 2017;33(4):260–263. doi:10.1097/yct.0000000000000428
17. Overall JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep. 1962;10(3):799–812. doi:10.2466/pr0.1962.10.3.799
18. Nilchaikovit T, Uneanong S, Kessawai D, Thomyangkoon P. The Thai version of the Positive and Negative Syndrome Scale (PANSS) for schizophrenia: criterion validity and interrater reliability. J Med Assoc Thai. 2000;83(6):646–651.
19. Kongsakon R, Bhatanaprabhabhan D. Validity and reliability of the Young Mania Rating Scale: Thai version. J Med Assoc Thai. 2005;88(11):1598–1604.
20. Lotrakul M, Sumrithe S, Saipanish R. Reliability and validity of the Thai version of the PHQ-9. BMC Psychiatry. 2008;8. doi:10.1186/1471-244X-8-46
21. Satthapisit S, Posayaanuwat N, Sasaluksananont C, Kaewpornsawan T, Singhakun S. The comparison of Montgomery and Asberg Depression Rating Scale (MADRS Thai) to diagnostic and statistical manual of mental disorders (DSM) and to Hamilton Rating Scale for Depression (HRSD): validity and reliability. J Med Assoc Thai. 2007;90(3):524–531.
22. Phuaphanprasert B, Srisurapanont M, Silpakit C, et al. Reliability and validity of the Thai version of the Health of the Nation Outcome Scales (hoNOS). J Med Assoc Thai. 2007;90(11):2487–2493.
23. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry. 2007;4(7):28–37.
24. Dharmasaroja PA, Ratanakorn D, Nidhinandana S, Charernboon T. Comparison of computerized and standard cognitive test in Thai Memory Clinic. J Neurosci Rural Pract. 2018;9(1):140–142. doi:10.4103/jnrp.jnrp_373_17
25. Jitapunkul S, Lailert C. Mini-mental status examination: is it appropriate for screening in Thai elderly? J Med Assoc Thai. 1997;80(2):116–120.
26. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
27. Medved S, Žaja N, Gazdag G, et al. Preliminary assessment of pre-electroconvulsive therapy evaluation practices in European countries: the need for guidelines. J ECT. 2022. doi:10.1097/yct.0000000000000854
28. Weiss A, Hussain S, Ng B, et al. Royal Australian and New Zealand College of Psychiatrists professional practice guidelines for the administration of electroconvulsive therapy. Aust N Z J Psychiatry. 2019;53(7):609–623. doi:10.1177/0004867419839139
29. Ittasakul P, Vora-Arporn S, Waleeprakhon P, Tor PC. Number of electroconvulsive therapy sessions required for Thai psychiatric patients: a retrospective study. Neuropsychiatr Dis Treat. 2020;16:673–679. doi:10.2147/ndt.S244031
30. Porter RJ, Baune BT, Morris G, et al. Cognitive side-effects of electroconvulsive therapy: what are they, how to monitor them and what to tell patients. BJPsych Open. 2020;6(3):e40. doi:10.1192/bjo.2020.17
31. Royal College of Psychiatrists. ECT Accreditation Service (ECTAS): Standards for the Administration of ECT.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Continuation-Maintenance Electroconvulsive Therapy on Hospitalization: A Retrospective Mirror-Image Study
Sombatcharoen-non N, Yamnim T, Jullagate S, Ittasakul P
Neuropsychiatric Disease and Treatment 2023, 19:1427-1433
Published Date: 15 June 2023