Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Electroacupuncture at Lower He-Sea and Front-Mu Acupoints Ameliorates Insulin Resistance in Type 2 Diabetes Mellitus by Regulating the Intestinal Flora and Gut Barrier
Authors Wang H ![]() , Chen X, Chen C, Pan T, Li M, Yao L
, Chen X, Chen C, Pan T, Li M, Yao L ![]() , Li X
, Li X ![]() , Lu Q, Wang H, Wang Z
, Lu Q, Wang H, Wang Z
Received 6 June 2022
Accepted for publication 16 July 2022
Published 30 July 2022 Volume 2022:15 Pages 2265—2276
DOI https://doi.org/10.2147/DMSO.S374843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Haili Wang,1,* Xinhua Chen,2,* Chunhai Chen,2 Ting Pan,1 Mengyuan Li,1 Lin Yao,1 Xuefeng Li,1 Qi Lu,1 Hongfeng Wang,3 Zhaohui Wang1,4
1School of Acupuncture-Moxibustion and Tuina, Changchun University of Chinese Medicine, Changchun, Jilin, 130117, People’s Republic of China; 2Department of Acupuncture and Moxibustion, Affiliated Hospital of Changchun University of Chinese Medicine, Changchun, Jilin, 130021, People’s Republic of China; 3Changchun University of Chinese Medicine, Changchun, Jilin, 130117, People’s Republic of China; 4Bao’an Authentic TCM Therapy Hospital, Shenzhen, 518101, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongfeng Wang, Changchun University of Chinese Medicine, Changchun, Jilin, 130117, People’s Republic of China, Tel/Fax +86 431 86172008, Email [email protected] Zhaohui Wang, School of Acupuncture-Moxibustion and Tuina, Changchun University of Chinese Medicine, Changchun, Jilin, 130117, People’s Republic of China, Tel/Fax +86 431 8687856, Email [email protected]
Introduction: The study objective was to investigate the effects of electroacupuncture performed at the he-sea and front-mu acupoints on the intestinal microflora and intestinal barrier in db/db mice and to explore the related mechanism in type 2 diabetes mellitus.
Methods: Db/m mice in the normal control group (NOC), electroacupuncture group (EA), metformin group (MET) and T2DM group (T2DM) were used as model controls, and db/db mice were used in all three groups, with 8 mice in each group. The treatment period was 2 weeks. Fasting blood glucose (FBG) and triglyceride (TG) levels were measured. Lipopolysaccharide (LPS) and tumor necrosis factor-α (TNF-α) levels were detected by enzyme-linked immune sorbent assay (ELISA). The ileal tissue was stained with hematoxylin-eosin staining (H&E), and histopathological changes were observed under a light microscope. Illumina sequencing was used to analyze the V4 region of the 16S rRNA gene to evaluate the effect of EA on the intestinal flora.
Results: Our results suggest that EA treatment can reduce the expression of diabetes-related markers, with an effect similar to that of metformin. After EA intervention, the abundance of Firmicutes and the ratio of Firmicutes to Bacteroidetes increased, while the abundances of Bacteroidetes and Eubacterium decreased. In addition, the serum levels of LPS and TNF-α in the electroacupuncture group were downregulated, and ileal tissue damage was alleviated under an electron microscope.
Conclusion: EA combined with acupoints can restore the intestinal flora structure, decrease the blood LPS level, reduce levels of inflammation, maintain the integrity of the intestinal barrier, and play a therapeutic role in the treatment of T2DM, mainly by increasing the abundance of Firmicutes and the ratio of Firmicutes to Bacteroidetes and decreasing the abundances of Bacteroidetes and Eubacterium.
Keywords: type 2 diabetes mellitus, lower he-sea and front-mu acupoints, gut microbiota, gut barrier
Introduction
Diabetes mellitus (DM) is a metabolic clinical syndrome characterized by long-term hyperglycemia, and its development is mainly due to two factors: insulin deficiency in pancreatic beta cells and insulin resistance.1,2 Type 2 diabetes mellitus (T2DM) patients account for the majority of the total number of people with diabetes with a proportion of over 95%.3 It is estimated that by 2045, the number of people living with diabetes will reach 700 million, posing a global health risk.4
The gut microbiome is a complex system of trillions of bacteria, fungi and viruses.5 The intestinal microbiota plays a variety of roles in host metabolism, such as promoting immunity6 and maintaining lipid metabolism homeostasis,7 which contribute to the occurrence and development of diabetes.8 The human intestine is an important barrier, and the intestinal flora, as a relatively complete ecosystem, can affect the function of the intestinal mucosal barrier.9,10 When the metabolic status of T2DM patients is abnormal, the intestinal microbiota is unbalanced, the intestinal epithelial cell structure is destroyed, intestinal mucosal permeability is increased, the release of LPS is promoted, and inflammatory factors enter the circulation, ultimately leading to a weak inflammatory state.11 A low-grade inflammatory state is an important factor causing insulin resistance.12 The prevention of inflammatory diseases may be an effective way to improve insulin resistance.13 Therefore, reducing levels of inflammation and maintaining the integrity of the intestinal microflora and intestinal mucosal barrier are very important in improving insulin resistance and T2DM treatment.14
Studies have shown that acupuncture not only promotes weight loss and hypoglycemia in patients with T2DM but also improves insulin resistance and regulates the levels of metabolic indicators, thus improving and treating type 2 diabetes.15,16 ST36 (Zusanli) is the lower he-sea acupoint of the gastric meridian. RN12 (Zhongwan) is the gastric meridian point; this point has a large number of Zang qi collections and is used for the treatment of fu disease. Acupoint compatibility refers to the fact that in acupuncture treatment, when two or more acupoints are used simultaneously, the curative effect can be enhanced. ST36 and RN12 are good targets for the treatment of fu disease.17 Our research group18,19 has confirmed that electricity can regulate inflammation and insulin resistance and that electroacupuncture can regulate the function of Zang-Fu organs. In this experiment, the effect of electrical treatment on the composition of the intestinal microflora in db/db mice was studied, and H&E staining of the ileum was performed to detect serum LPS and TNF-α levels with the aim of studying the effects of combined electroacupuncture and acupoints on the intestinal microflora, intestinal barrier and inflammation in type 2 diabetes mellitus and to further explore the potential mechanism.
Materials and Methods
Animals
Twenty-four male db/db mice and eight db/m mice (18–23 g, 6–7 weeks) with specific pathogen-free (SPF) status were selected for this study. The mice were provided by Changzhou Kavins Experimental Animal Co., Ltd. (License No. SCXK (Su) 2016–0010). The mice were raised in the animal room of the Chuangshi Building at Changchun University of Chinese Medicine. The temperature was maintained at 22 ± 2 ℃, and the relative humidity was 50–60%. Sterilized food and water were provided ad libitum. The cage and cushion materials were autoclaved, and the cage and animal room were cleaned and disinfected regularly for adaptive feeding for 1 week. Twenty-four db/db mice were randomly divided into the electroacupuncture group (EA) (n=8) for electroacupuncture treatment, the metformin drug group (MET) (n=8) for drug therapy, and the type 2 diabetes mellitus group (T2DM) (n=8) as the model control group, and 8 db/m mice were used as the normal control group (NOC) (n=8). All animal experiments were conducted in accordance with China’s Animal Care Guidelines and internationally recognized standards for the use of experimental animals, and they were reviewed and approved by the Ethics Committee of Animal Experiments of Changchun University of Chinese Medicine (Ethics Code: 2021206).
Animal Treatment
In the EA group, the ST36 (bilateral) and RN12 acupuncture points were identified according to the experimental acupuncture point map.20 Acupuncture needles were obtained from Andy Medical Equipment Co., Ltd. (Guizhou, China). After anesthesia was administered with 1% isoflurane (Shenzhen Rayward Life Technology Co., Ltd., Shenzhen), electroacupuncture at ST36 and RN12 was performed 3 mm deep. A Huatuo SDZ-V electroacupuncture apparatus (Suzhou Medical Device Factory, China) was used to connect the same side of the acupuncture point with a 3 Hz (frequency ratio 1:5) expansion wave, with a current of 1 mA. The amount of stimulation was measured according to the endurance of the mice. Each electroacupuncture treatment lasted 20 minutes. In the MET group, metformin (Sino-American Shanghai Squibb Pharmaceutical Ltd., National Batch Number: H20023370) was administered orally at 200 mg/kg/d.21 Animals in the T2DM group and NOC group were not treated. The experimental treatment was administered 6 days a week with 1 rest day for 2 consecutive weeks. Before treatment and on rest days after treatment, the mice were weighed, and FBG levels were measured with a glucose meter (OneTouchTwo, Roche, Germany). Stool samples from 4 randomly selected mice were collected in sterile cryopreservation tubes on the second rest day (7 am to 11 am) after 2 weeks of treatment. The samples were placed in a −80 ℃ freezer for analysis. After the feces were collected, the mice were fasted for 12 hours beginning at 8 p.m. on the same day, and the oral glucose tolerance test (OGTT) was performed at 8 a.m. the next day. Glucose levels in caudal vein blood samples were measured immediately after oral disinfection of glucose solution (2 g/kg, Sigma–Aldrich, USA) and then at 0, 0.5, 1, 1.5, and 2 hours. The area under the curve (AUC) that was achieved using the OGTT values was calculated from the measured values. After the above tests were completed, the mice were anesthetized, blood was collected, and ileum tissues from 4 mice were randomly collected (Figure 1).
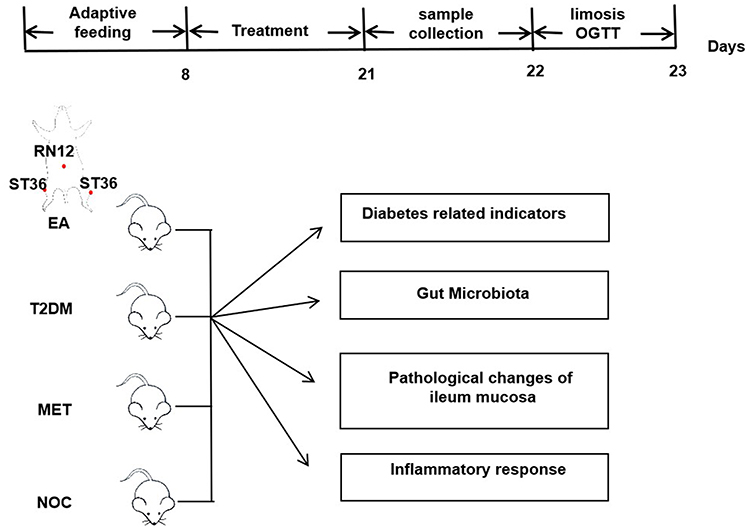 |
Figure 1 Flow chart of the experiment. |
Determination of Diabetes-Related Indices and Detection of LPS and TNF-α Levels by ELISA
Serum insulin, serum total cholesterol (TC), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C), and high-density lipoprotein cholesterol (HDL-C) levels were determined. A mouse TNF-α ELISA Kit (Beyotime) was used to determine the serum concentrations of TNF-α (Huangshi Yanke Biotechnology Co., Ltd., Product number: CK-E20852) and LPS (Huangshi Yanke Biotechnology Co., Ltd., Product number: CK-E31044). The insulin resistance (HOMA IR) index was calculated as (FBG value × FINS value)/22.5.
16S rDNA Sequencing
Primers 515F (5ʹ-GTGYCAGCMGCCGCGGTAA-3ʹ) and 806R (5ʹ-GGACTACHVGGGTWTCTAAT-3ʹ) were used to amplify a slightly modified version of the V4 region of the gene for the bacterial small subunit (16S) rRNA. The 5ʹ primer ends were affixed with a specific barcode for each sample and a universal sequencing primer. After PCR amplification, the purified amplicon was collected for normalization and peer sequencing (2 × 250) using a standard Illumina HiSeq 2500 platform protocol.
Histopathological Examination
The fixed ileal tissue was removed, dehydrated using conventional methods, embedded in paraffin, and sliced at a thickness of 5 µm. Observation was performed under an optical microscope (Nikon, Nikon Eclipse E100, Japan).
Statistical Analysis
Data are expressed as the mean ± standard error (SD) for each group. ANOVA was used to detect differences in each group, and the LSD test was used for multiple groups. Results with P values of < 0.05 were considered statistically significant.
Results
Diabetes-Related Indicators in db/db Mice
We evaluated the effect of electrotherapy on insulin resistance and dyslipidemia. After 2 weeks of intervention, food intake and water intake, body weight and blood glucose levels were lower in the EA and MET groups than in the model group (Figure 2A–D). The OGTT curve showed that fasting glucose levels were lower in the EA and MET groups than in the T2DM group at different time points (Figure 2E). In addition, the AUC in the T2DM group was higher than that in the EA group and MET group (Figure 2F). There was no significant difference between the EA group and MET group. These results suggest that EA can improve abnormal glucose tolerance in db/db mice, similar to the effect of MET.
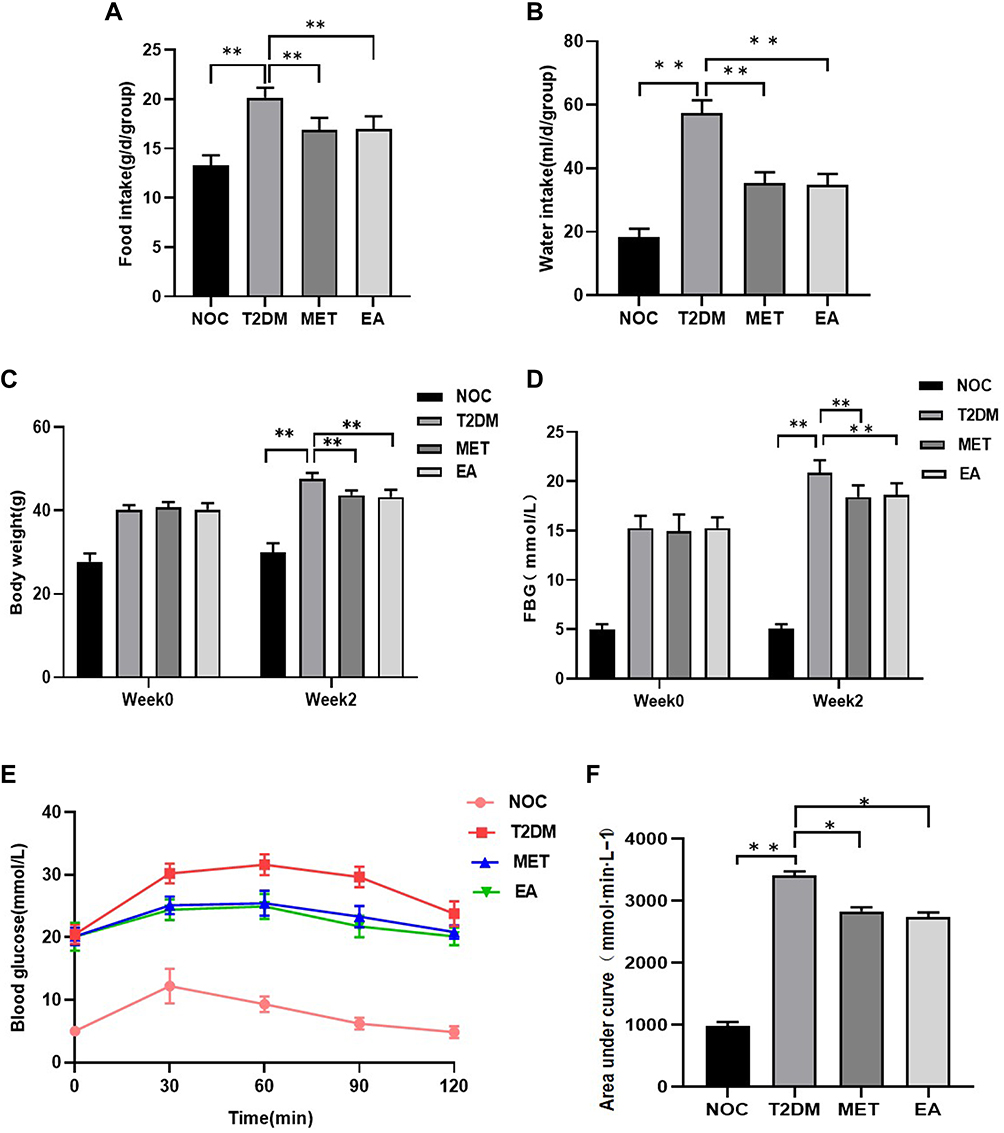 |
Figure 2 General indicators of diabetes in each group. (A) Food intake. (B) Water intake. (C) Body weight. (D) FBG levels. (E) OGTT. And (F) AUC. Data are shown as the mean ± SD values. *P < 0.05, **P < 0.01 (n = 8). |
After 2 weeks of intervention, the fasting insulin level and Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) index values in the EA group and MET group were lower than those in the T2DM group (Figure 3A and B). TC and TG levels decreased (Figure 3C and D), HDL-C levels significantly increased (Figure 3E), and LDL-C levels significantly decreased (Figure 3F). The effects were similar in the EA group and the MET group. These findings suggested that dyslipidemia and islet resistance in T2DM can be improved after EA and MET treatment. There was no difference in improvement between the two groups.
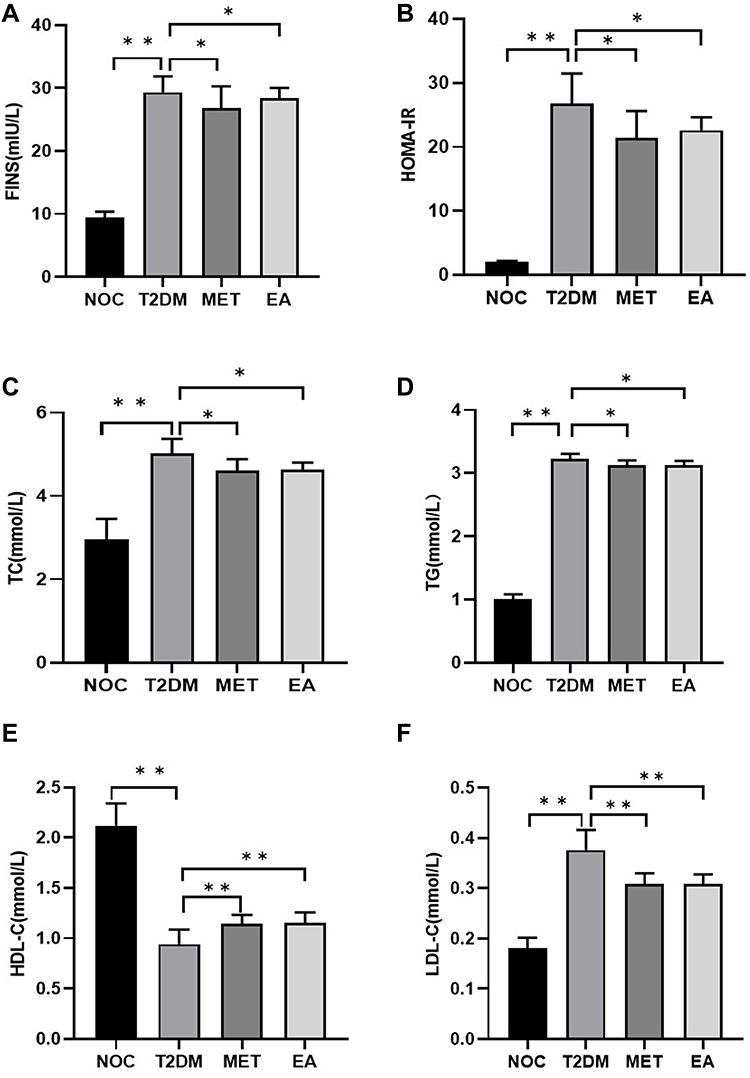 |
Figure 3 Related indicators of diabetes mellitus in each group. (A) FINS. (B) HOMA-IR. (C) TC levels. (D) TG levels. (E) HDL-C levels. (F) LDL-C levels. Data are shown as the mean ± SD values. *P < 0.05, **P < 0.01 (n = 8). |
Regulation of the Intestinal Microflora by Electroacupuncture
Obvious clustering for each group was shown by principal component analysis (PCA) based on the Bray–Curtis distance (Figure 4A). The relative abundances of the first two primary phyla (Firmicutes and Bacteroidetes) in each group changed significantly (Figure 4B and C). The Firmicutes abundance was lower in the T2DM group than in the NOC group, while the Bacteroidetes abundance was higher (Figure 4D). After EA and MET treatment for 2 weeks, Firmicutes abundance was higher and Bacteroidetes abundance was lower in the EA and MET groups than in the T2DM group (Figure 4E and F); in addition, the ratio of Firmicutes to Bacteroidetes increased after EA and MET treatment for 2 weeks (Figure 4G). We also found specific changes at the genus level in the intestinal microbiome. We found changes in a variety of bacteria, especially Eubacterium (Figure 5A). The abundances of Eubacterium in the T2DM groups were significantly higher than that in the NOC group. After EA treatment for 2 weeks, Eubacterium abundance was lower in the EA groups than in the T2DM group, while there was no significant difference in the abundance of Eubacterium between the T2DM groups after MET treatment (Figure 5B). In conclusion, taxonomic analysis suggests that EA treatment can modulate the structure of the dysregulated intestinal flora in T2DM mice and restore it to a normal state.
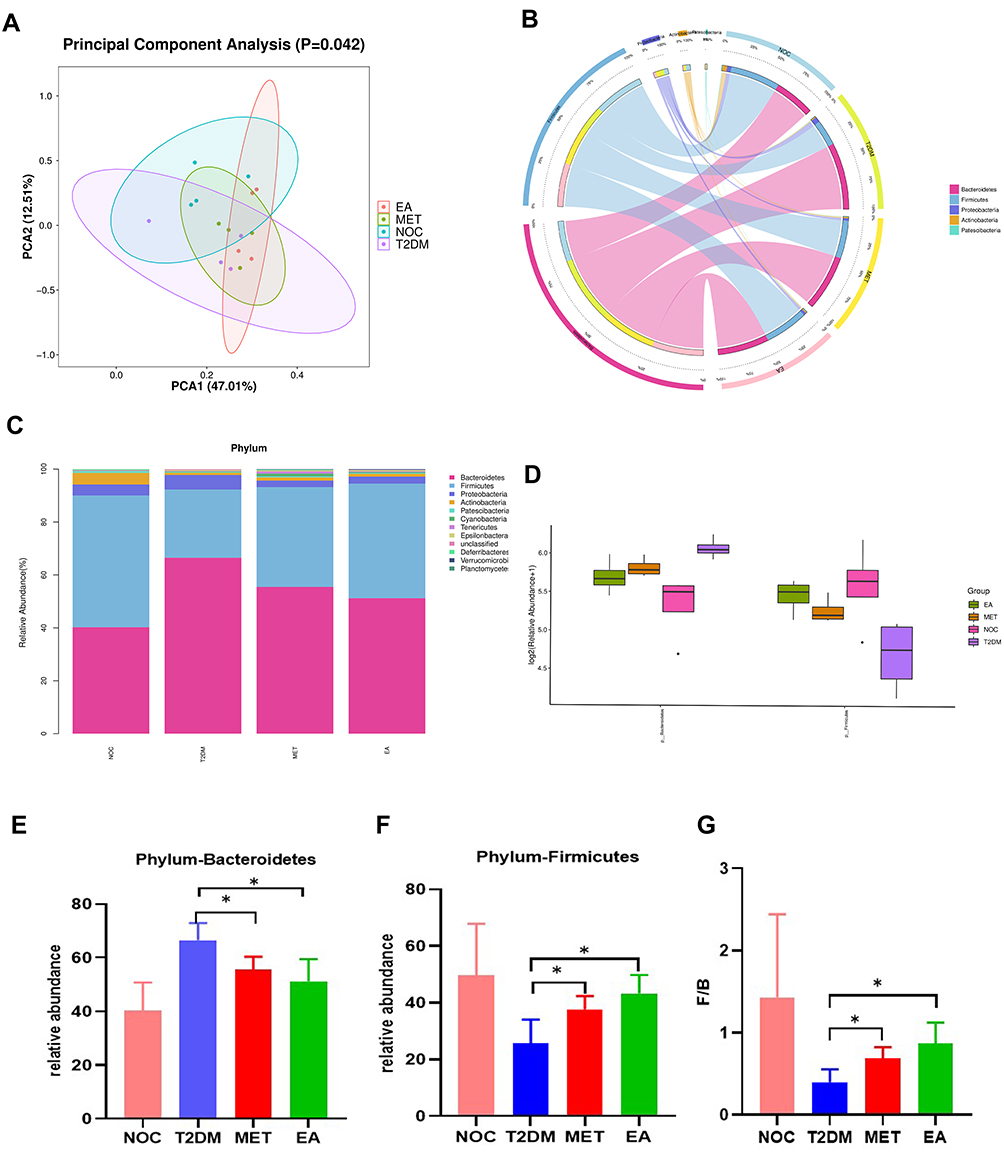 |
Figure 4 Diversity of fecal microbiota between groups (phylum level). (A) PCA. (B) Circos. (C) Stacked bar chart. (D) Bar plot difference analysis. (E) Bacteroidetes. (F) Firmicutes. (G) Firmicutes/Bacteroidetes. Data are shown as the mean ± SD values. *P < 0.05 (n = 4). |
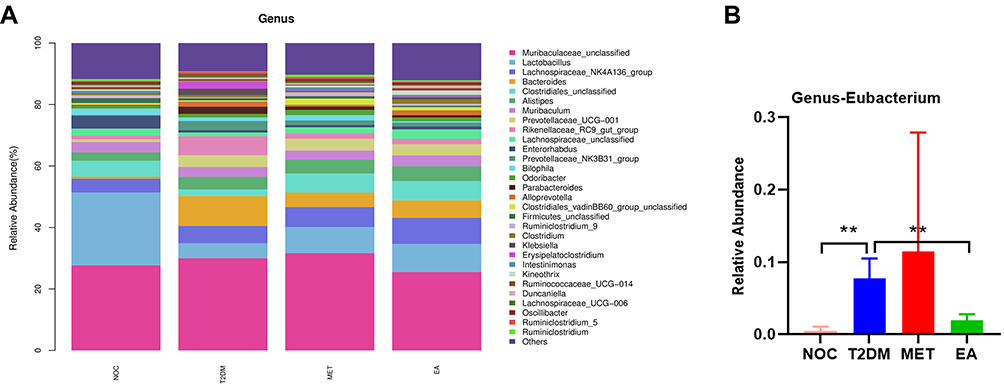 |
Figure 5 Differences in the composition of the gut microbiota at the genus level among each group. (A) Stacked bar chart. (B) Eubacterium. Data are shown as the mean ± SD values, **P < 0.01 (n = 4). |
Ileal Tissue Damage Was Repaired by Electroacupuncture, and Serum LPS and TNF-α Levels Were Downregulated
In the NOC group, the villi of the colon tissue were arranged neatly and exhibited a normal structure. Unlike those in the NOC group, the villi in the T2DM group were disordered, with marked mucosal inflammation, goblet cell and epithelial damage, and marked inflammatory cell infiltration (red arrow). Unlike in the T2DM group, the integrity of the intestinal barrier was significantly improved in the EA group and MET group, and levels of inflammatory cell infiltration were reduced (Figure 6A). In addition, serum LPS and TNF-α levels were measured to assess systemic inflammation. Serum LPS and TNF-α concentrations in the T2DM group were significantly higher than those in the NOC group, but after 2 weeks of treatment with EA and MET, LPS and TNF-α concentrations were significantly lower, with no significant difference between the two groups, suggesting that EA and MET reduce the levels of systemic inflammation and repair intestinal wall damage (Figure 6B and C).
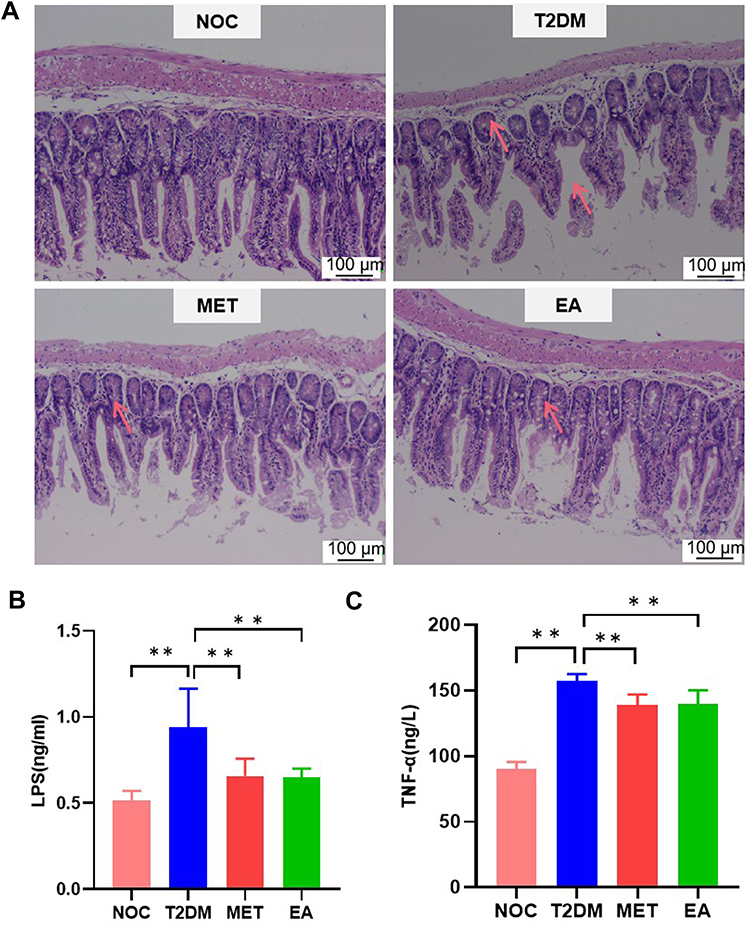 |
Figure 6 Pathological images of the ileum and serum inflammatory factors in each group. (A) H&E staining (n=4). Serum LPS (B) and TNF-α (C) levels were detected with ELISA kits. Data are shown as the mean ± SEM. **p < 0.01 (n = 8). |
Correlations Between the Gut Microbiota and Metabolic Parameters in T2DM
Correlation heatmap analysis was used to evaluate the correlations between intestinal microbiota and T2DM-related indexes, including body weight, FBG levels, FINS, HOMA-IR, TC levels, TG levels, LDL-C levels, HDL-C levels, LPS levels, and TNF-α levels (Figure 7). According to the heatmap, Firmicutes abundance and F/B were negatively correlated with T2DM-related indices (contrary to HDL-C), while Bacteroidetes abundance was positively correlated with T2DM-related indices (contrary to HDL-C) (contrary to HDL-C).
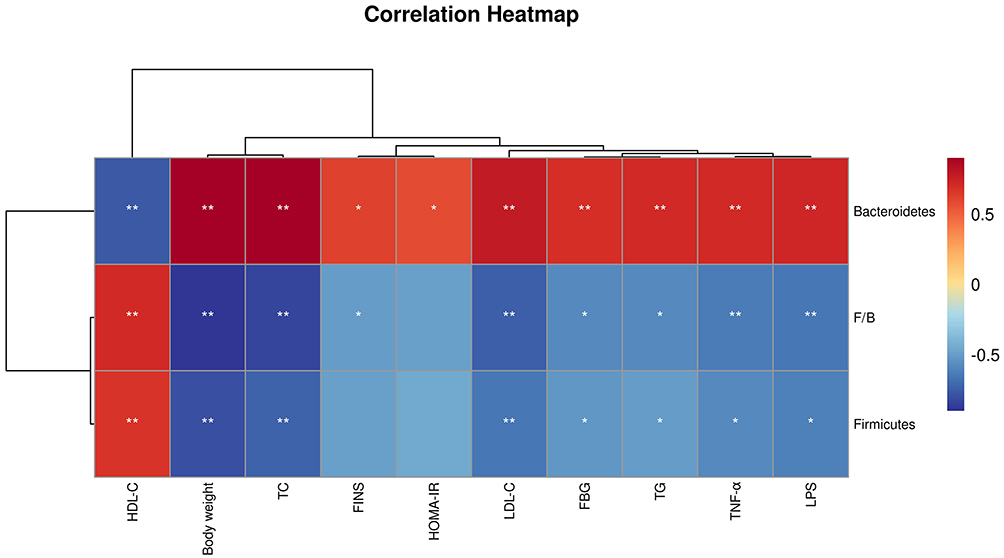 |
Figure 7 The correlation analysis matrix between related factors and intestinal flora changes in T2DM mice was based on the Pearson correlation value. *P < 0.05, **P < 0.01 indicates significant correlation. |
Discussion
The basic pathogenic mechanism underlying DM is dryness-heat due to yin deficiency.22 In recent years, there has been research progress on the therapeutic effect of acupuncture on T2DM and insulin resistance (IR). ST36 is the lower he-sea acupoint of the gastric meridian, which can regulate the function of meridians and eliminate pathogens. RN12 is the front-mu acupoint, with the effects of nourishing Yin, nourishing blood, and nourishing blood function. In this study, the combination of the lower he-sea and front-mu acupoints, which is one of the commonly used acupoint selection methods in acupuncture treatment, was mainly used for the treatment of corresponding fu diseases. Therefore, the combination of the lower he-sea and front-mu acupoints were selected in this study as targets for treating type 2 diabetes.23
Db/db mice exhibit the characteristics of T2DM and are ideal animal models for the experimental study of T2DM. They are widely used in animal experiments.24 Therefore, we observed the effects of electroacupuncture performed at the lower he-sea and front-mu acupoints on the intestinal flora and intestinal barrier of db/db mice and explored the mechanism of action related to T2DM treatment. Previous studies have shown that after db/db mouse feces were transplanted into germ-free mice, the body weight and blood glucose levels of the mice increased, and the blood lipids were abnormal.25 In this study, the body weight and blood glucose levels of the mice in the T2DM group increased, and the blood lipids were abnormal, which was consistent with the results of previous studies. In this experiment, after EA and MET treatment, all the above indicators were alleviated (Figure 2A–D), and glucose tolerance and dyslipidemia were improved (Figure 3C–F). In addition, decreased serum insulin levels and improved insulin resistance were observed (Figure 3A and B). Insulin resistance is one of the main pathologies underlying T2DM. Due to excessive levels of proinflammatory cytokines, insulin resistance leads to impaired glucose transport and increased fat decomposition. Due to the activation of the insulin response or insufficient insulin production, the body reacts by inappropriately increasing glucagon levels, which further leads to hyperglycemia.26 Metformin is currently the most commonly used treatment for T2DM. Patients with diabetes or who are obese or overweight can effectively reduce blood glucose levels, lose weight and improve insulin resistance, which has a good therapeutic effect in patients with diabetes or obese diabetes.27 In this study, the efficacy of electroacupuncture performed at the lower he-sea and front-mu acupoints was similar to that of MET in terms of weight loss, hypoglycemia, and improvement of insulin resistance, suggesting that electroacupuncture performed at the lower he-sea and front-mu acupoints had a good ability to provide mechanical therapy for T2DM, which was consistent with the results of previous studies.28,29
The intestinal flora is located on the surface of the intestinal mucosa, and it is indispensable for human growth and development, physiological processes and even disease states. The gut microbiota consists of approximately 500–1000 species of bacteria.30 The healthy intestinal flora mainly includes Firmicutes, Bacteroidetes, Proteobacteria and Actinobacteria at the phylum level. The intestinal flora is involved in the occurrence and development of insulin resistance and T2DM.31 It was found that the abundance of Firmicutes in the T2DM group was significantly lower than that in normal controls, and the abundance of Bacteroidetes was higher. The study also found that in T2DM patients, the ratio of Bacteroidetes to Firmicutes was significantly positively correlated with blood glucose concentration.32 In this study, assessments of the composition of the intestinal flora showed that, at the phylum level, Firmicutes abundance was higher and Bacteroides abundance was lower in the EA groups than in the T2DM group, (Figures 4E and F), and the ratio of Firmicutes/Bacteroides was higher (Figure 4G). At the genus level, Eubacterium abundances in the T2DM groups were significantly higher and lower after EA treatment than those in the T2DM group, while there was no significant difference in the Eubacterium abundance between the T2DM groups after MET treatment (Figure 5B). At the phylum level and genus level, the intestinal flora of db/db mice in the EA group was more similar to that in the NOC group than the intestinal flora in the T2DM group. In conclusion, electroacupuncture performed at the lower he-sea and front-mu acupoints can be used to regulate the composition of the intestinal microflora in T2DM mice and make it close to its normal state.
LPS is an endotoxin that is present in the cell wall of gram-negative bacteria. T2DM under the condition of abnormal glucose metabolism in patients with imbalances in the intestinal microflora and specifically in intestinal epithelial cells can damage the intestinal structure; increase the permeability of the intestinal mucosa; impair the intestinal barrier; promote the release of LPS and the production of a large number of inflammatory cytokines, such as TNF-α, cause intestinal inflammation; induce the entry of inflammatory factors into the circulatory system, leading to a systemic low-grade inflammatory state; and decrease insulin sensitivity.33–35 In addition, LPS, when present in excess, binds to the CD14 protein as a ligand and binds Toll-like receptor 4 (TLR-4) to activate transcription factors, such as nuclear transcription factor-κB, to generate immune responses and induce inflammatory responses.36 Furthermore, CD14/TLR4 knockout mice were found to be more sensitive to insulin than wild-type control mice.37 Fei et al38 induced insulin resistance via subcutaneous injection of endotoxin in mice and transplanted endotoxin-containing bacteria from the intestinal tract of obese mice into the intestinal tract of sterile mice, resulting in insulin resistance in sterile mice. Huang et al33 found that increased intestinal mucosal permeability leads to more endotoxin entering the blood, which is one of the causes of diabetes in mice. Therefore, increased LPS levels trigger an inflammatory response, increase intestinal mucosal permeability, cause insulin resistance, and ultimately lead to the occurrence and development of diabetes. In our study, ileal tissue from T2DM mice was severely damaged, as indicated by electron microscopy. After EA treatment, ileal tissue damage was improved, as indicated by electron microscopy (Figure 6A). In addition, LPS and TNF-α levels in the circulation were decreased in the EA groups (Figures 6B and C). Firmicutes abundance and F/B were negatively correlated with LPS and TNF-α levels, while Bacteroidetes abundance was positively correlated with LPS and TNF-α levels (Figure 7). These results suggest that EA can reduce inflammation, repair the integrity of the intestinal barrier and regulate the structure of the intestinal flora, thus alleviating diabetes. These findings are consistent with those observed in previous studies.39,40
A literature review showed that acupuncture performed at specific acupoints, including ST36, showed anti-inflammatory properties.41 Another study showed that EA performed at the Zusanli point protects the intestinal barrier by regulating the gut microbiome.42 RN12 plays a benign role in weight loss and gastrointestinal motility.43 According to our experimental results, we believe that electroacupuncture performed at lower he-sea and front-mu acupoints, probably by regulating the intestinal flora, repaired the intestinal structure of intestinal epithelial cells and reduced the permeability of the intestinal mucosa to prevent a large number of lipopolysaccharides from entering the body circulation, thus improving the general, low-grade inflammatory state and eventually improving insulin resistance.
In the future, we hope to target the intestinal flora to provide more therapeutic options for acupuncture in the treatment of diabetes. Thus far, the clinical treatment of diabetes mainly involves hypoglycemic drugs, but they have side effects, such as low blood sugar levels and nausea. Traditional Chinese medicine acupuncture treatment exhibits very good control of blood sugar levels, with few side effects, and it is inexpensive and easily accepted by patients. In the future, we hope that more in-depth studies from the perspective of the intestinal flora will provide more targets for the treatment of T2DM with acupuncture.
Conclusions
Electroacupuncture performed at the lower he-sea and front-mu acupoints mainly targets the thick cell wall of bacteria (with effects on gram-negative and gram-positive bacterial abundance) by upregulating the abundance of Firmicutes (gram-positive) and downregulating the abundance of Bacteroidetes (gram-negative) to restore the structure of the intestinal flora, reduce the circulating level of LPS, and reduce levels of inflammation to maintain the integrity of the intestinal barrier for the treatment of T2DM. Therefore, in this study, EA technology was used in the treatment of T2DM, confirming that it has a similar therapeutic effect to that achieved using metformin. Furthermore, the intestinal flora was targeted to elucidate the mechanism of action underlying the effects of electroacupuncture performed at the lower he-sea and front-mu acupoints in the treatment of T2DM.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgments
We thank the National Natural Science Funding of China (81774393), the Natural Science Foundation of Jilin Province (20200201612JC, 20210101191JC).
Disclosure
The authors declare no conflict of interest.
References
1. Roden M, Shulman GI. The integrative biology of type 2 diabetes. Nature. 2019;576(7785):51–60. doi:10.1038/s41586-019-1797-8
2. Pearson ER. Type 2 diabetes: a multifaceted disease. Diabetologia. 2019;62(7):1107–1112. doi:10.1007/s00125-019-4909-y
3. Elkhidir AE, Eltaher HB, Mohamed AO. Association of lipocalin-2 level, glycemic status and obesity in type 2 diabetes mellitus. BMC Res Notes. 2017;10(1):285. doi:10.1186/s13104-017-2604-y
4. Cho NH, Shaw JE, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
5. Eckburg PB, Bik EM, Bernstein CN, et al. Diversity of the human intestinal microbial flora. Science. 2005;308(5728):1635–1638. doi:10.1126/science.1110591
6. Bender E. Could a bacteria-stuffed pill cure autoimmune diseases? Nature. 2020;577(7792):S12–S13. doi:10.1038/d41586-020-00197-z
7. Chen JJ, Xie J, Zeng BH, et al. Absence of gut microbiota affects lipid metabolism in the prefrontal cortex of mice. Neurol Res. 2019;41(12):1104–1112. doi:10.1080/01616412.2019.1675021
8. Portincasa P, Bonfrate L, Vacca M, et al. Gut microbiota and short chain fatty acids: implications in glucose homeostasis. Int J Mol Sci. 2022;23(3):1105. doi:10.3390/ijms23031105
9. Shin W, Kim HJ. Intestinal barrier dysfunction orchestrates the onset of inflammatory host-microbiome cross-talk in a human gut inflammation-on-a-chip. Proc Natl Acad Sci USA. 2018;115(45):E10539–E10547. doi:10.1073/pnas.1810819115
10. Hiippala K, Jouhten H, Ronkainen A, et al. The potential of gut commensals in reinforcing intestinal barrier function and alleviating inflammation. Nutrients. 2018;10(8):988. doi:10.3390/nu10080988
11. Liu T, Wu Y, Wang L, et al. A more robust gut microbiota in calorie-restricted mice is associated with attenuated intestinal injury caused by the chemotherapy drug cyclophosphamide. mBio. 2019;10(2):e02903–18. doi:10.1128/mBio.02903-18
12. Almuraikhy S, Kafienah W, Bashah M, et al. Interleukin-6 induces impairment in human subcutaneous adipogenesis in obesity-associated insulin resistance. Diabetologia. 2016;59(11):2406–2416. doi:10.1007/s00125-016-4031-3
13. Rehman K, Akash MSH, Liaqat A, et al. Role of interleukin-6 in development of insulin resistance and Type 2 diabetes mellitus. Crit Rev Eukaryot Gene Expr. 2017;27:229–236. doi:10.1615/CritRevEukaryotGeneExpr.2017019712
14. Wu W, Liu L, Zhu H, et al. Butyrolactone-I, an efficient alpha-glucosidase inhibitor, improves type 2 diabetes with potent TNF-alpha-lowering properties through modulating gut microbiota in db/db mice. FASEB J. 2019;33(11):12616–12629. doi:10.1096/fj.201901061R
15. Chen C, Liu J, Sun M, et al. Acupuncture for type 2 diabetes mellitus: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Clin Pract. 2019;36:100–112. doi:10.1016/j.ctcp.2019.04.004
16. Liu M, Chen J, Ren Q, et al. Acupuncture and related techniques for type 2 diabetes mellitus: a systematic review protocol. Medicine. 2019;98(2):e14059. doi:10.1097/MD.0000000000014059
17. Wang ZH, Zhang JJ, Wang FC. [Effect of different acupoint prescriptions on prevention and treatment of stress gastric ulcer]. Zhongguo Zhen Jiu. 2014;34(2):149–151. [王朝辉,张娇娇,王富春. 不同腧穴配伍防治应激性胃溃疡的效应规律[J]. 中国针灸,2014,34(02):149-151.] Chinese. PMID: 24796050
18. Li L, Zang H, Jiang Y, et al. Acupuncture at back-shu and front-mu acupoints prevents gastric ulcer by regulating the TLR4/MyD88/NF-κB signaling pathway. Evid Based Complement Alternat Med. 2021;2021:8214052. doi:10.1155/2021/8214052
19. Zhang L, Chen X, Wang H, et al. Adjusting internal organs and dredging channel”electroacupuncture ameliorates insulin resistance in type 2 diabetes mellitus by regulating the intestinal flora and inhibiting inflammation. Diabetes Metab Syndr Obes. 2021;14:2595–2607. doi:10.2147/DMSO.S306861
20. Liu S, Guo R, Liu F, et al. Gut microbiota regulates depression-like behavior in rats through the neuroendocrine-immune mitochondrial pathway. Neuropsychiatr Dis Treat. 2020;16:859–869. doi:10.2147/NDT.S243551
21. Jia W, Bai T, Zeng J, et al. Combined administration of metformin and atorvastatin attenuates diabetic cardiomyopathy by inhibiting inflammation, apoptosis, and oxidative stress in type 2 diabetic mice. Front Cell Dev Biol. 2021;9:634900. doi:10.3389/fcell.2021.634900
22. Zheng W, Wang G, Zhang Z, et al. Research progress on classical traditional Chinese medicine formula Liuwei Dihuang pills in the treatment of type 2 diabetes. Biomed Pharmacother. 2020;121:109564. doi:10.1016/j.biopha.2019.109564
23. Yang M. [Clinical study on effect of lower he-front Mu acupoint Method on insulin motilin levels in patients with diabetic gastroparesis]. Changchun Univ Chin Med. 2017. [杨明. 合募配穴法对糖尿病胃轻瘫患者胰岛素用量及胃动素水平影响的临床研究[D].长春中医药大学, 2017]. Chinese.
24. Li K, Zhang L, Xue J, et al. Dietary inulin alleviates diverse stages of type 2 diabetes mellitus via anti-inflammation and modulating gut microbiota in db/db mice. Food Funct. 2019;10(4):1915–1927. doi:10.1039/C8FO02265H
25. Yu F, Jiang R, Han W, et al. Gut microbiota transplantation from db/ db mice induces diabetes-like phenotypes and alterations in Hippo signaling in pseudo germ-free mice. Aging. 2020;12(23):24156–24167. doi:10.18632/aging.104101
26. Patel TP, Rawal K, Bagchi AK, et al. Insulin resistance: an additional risk factor in the pathogenesis of cardiovascular disease in type 2 diabetes. Heart Fail Rev. 2016;21:11–23. doi:10.1007/s10741-015-9515-6
27. Zhang Q, Hu N. Effects of metformin on the gut microbiota in obesity and type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2020;13:5003–5014. doi:10.2147/DMSO.S286430
28. Xu T, Yu Z, Liu Y, et al. Hypoglycemic effect of electroacupuncture at ST25 through neural regulation of the pancreatic intrinsic nervous system. Mol Neurobiol. 2022;59(1):703–716. doi:10.1007/s12035-021-02609-1
29. Wang X, Li Q, Han X, et al. Electroacupuncture alleviates diabetic peripheral neuropathy by regulating glycolipid-related GLO/AGEs/RAGE axis. Front Endocrinol. 2021;12:655591. doi:10.3389/fendo.2021.655591
30. Gilbert JA, Blaser MJ, Caporaso JG, et al. Current understanding of the human microbiome. Nat Med. 2018;24(4):392–400. doi:10.1038/nm.4517
31. Tremaroli V, Bäckhed F. Functional interactions between the gut microbiota and host metabolism. Nature. 2012;489(7415):242–249. doi:10.1038/nature11552
32. Larsen N, Vogensen FK, van den Berg FW, et al. Gut microbiota in human adults with type 2 diabetes differs from non-diabetic adults. PLoS One. 2010;5(2):e9085. doi:10.1371/journal.pone.0009085
33. Huang J, Guan B, Lin L, et al. Improvement of intestinal barrier function, gut microbiota, and metabolic endotoxemia in type 2 diabetes rats by curcumin. Bioengineered. 2021;12(2):11947–11958. doi:10.1080/21655979.2021.2009322
34. Yuan JH, Xie QS, Chen GC, et al. Impaired intestinal barrier function in type 2 diabetic patients measured by serum LPS, Zonulin, and IFABP. J Diabetes Complications. 2021;35(2):107766. doi:10.1016/j.jdiacomp.2020.107766
35. Nascimento JC, Matheus VA, Oliveira RB, et al. High-fat diet induces disruption of the tight junction-mediated paracellular barrier in the proximal small intestine before the onset of type 2 diabetes and endotoxemia. Dig Dis Sci. 2021;66(10):3359–3374. doi:10.1007/s10620-020-06664-x
36. Monguió-Tortajada M, Franquesa M, Sarrias MR, et al. Low doses of LPS exacerbate the inflammatory response and trigger death on TLR3-primed human monocytes. Cell Death Dis. 2018;9(5):499. doi:10.1038/s41419-018-0520-2
37. Garibotto G, Carta A, Picciotto D, et al. Toll-like receptor-4 signaling mediates inflammation and tissue injury in diabetic nephropathy. J Nephrol. 2017;30(6):719–727. doi:10.1007/s40620-017-0432-8
38. Fei N, Zhao L. An opportunistic pathogen isolated from the gut of an obese human causes obesity in germfree mice. ISME J. 2013;7(4):880–884. doi:10.1038/ismej.2012.153
39. Song JX, Ren H, Gao YF, et al. Dietary capsaicin improves glucose homeostasis and alters the gut microbiota in obese diabetic ob/ob mice. Front Physiol. 2017;8:602. doi:10.3389/fphys.2017.00602
40. Van Hul M, Geurts L, Plovier H, et al. Reduced obesity, diabetes, and steatosis upon cinnamon and grape pomace are associated with changes in gut microbiota and markers of gut barrier. Am J Physiol Endocrinol Metab. 2018;314(4):E334–E352. doi:10.1152/ajpendo.00107.2017
41. Oh JE, Kim SN. Anti-inflammatory effects of acupuncture at ST36 point: a literature review in animal studies. Front Immunol. 2022;12:813748. doi:10.3389/fimmu.2021.813748
42. Wang L, An J, Song S, et al. Electroacupuncture preserves intestinal barrier integrity through modulating the gut microbiota in DSS-induced chronic colitis. Life Sci. 2020;261:118473. doi:10.1016/j.lfs.2020.118473
43. Yeh YC, Chen CC, Cheng CY, et al. The beneficial effects of moxibustion on overweight adolescent girls. Evid Based Complement Alternat Med. 2021;2021:1943181. doi:10.1155/2021/1943181
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Tang-Ping-San Decoction Remodel Intestinal Flora and Barrier to Ameliorate Type 2 Diabetes Mellitus in Rodent Model
Yin W, Zhang SQ, Pang WL, Chen XJ, Wen J, Hou J, Wang C, Song LY, Qiu ZM, Liang PT, Yuan JL, Yang ZS, Bian Y
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2563-2581
Published Date: 20 August 2022
The Association Between Sarcopenia and Diabetes: From Pathophysiology Mechanism to Therapeutic Strategy
Chen H, Huang X, Dong M, Wen S, Zhou L, Yuan X
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1541-1554
Published Date: 30 May 2023
The Role of Type 2 Diabetes Mellitus–Related Risk Factors and Drugs in Hepatocellular Carcinoma
Mai Y, Meng L, Deng G, Qin Y
Journal of Hepatocellular Carcinoma 2024, 11:159-171
Published Date: 19 January 2024