Back to Journals » Journal of Pain Research » Volume 19
Efficacy of Governor Vessel–Based Acupuncture, Alone or in Combination with Other Therapies, for Acute Lumbar Disc Herniation: A Systematic Review and Meta-Analysis
Authors Yang S, Guo Q, Zhang M, Zhang W ![]() , Ren S
, Ren S
Received 14 December 2025
Accepted for publication 12 February 2026
Published 25 February 2026 Volume 2026:19 586965
DOI https://doi.org/10.2147/JPR.S586965
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Shuai Yang,* Qngfeng Guo,* Miao Zhang, Weiling Zhang, Shouchen Ren
Traditional Chinese Medicine Department, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weiling Zhang, Traditional Chinese Medicine Department, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050000, People’s Republic of China, Email [email protected] Shouchen Ren, Traditional Chinese Medicine Department, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050000, People’s Republic of China, Email [email protected]
Abstract: This study systematically evaluated the efficacy of Governor Vessel–based acupuncture for lumbar disc herniation (LDH) and examined whether different acupuncture paradigms or combined interventions offered additional benefits. A comprehensive search of nine major databases identified 689 records, and 15 randomized controlled trials involving 670 patients met the inclusion criteria. Meta-analysis demonstrated that Governor Vessel–based acupuncture significantly improved overall clinical effectiveness compared with control treatments (RR = 1.21, 95% CI: 1.15– 1.27), with a stable predictive interval. Pain intensity was also markedly reduced, as evidenced by a substantial decrease in visual analogue scale scores (SMD = – 1.77, 95% CI: – 2.18 to – 1.36). Subgroup analyses revealed no meaningful differences among Wenyang Tongdu, spine-regulating Governor Vessel, and Bushen–Huoxue techniques, nor between acupuncture alone and combined modalities. These findings indicate that Governor Vessel–based acupuncture provides consistent and clinically relevant benefits for patients with LDH. However, methodological heterogeneity and the limited number of single-modality Governor Vessel trials should be considered when interpreting these findings. Nevertheless, higher-quality multicenter randomized trials are needed to validate long-term outcomes and clarify mechanistic pathways.
Keywords: lumbar disc herniation, governor vessel–oriented acupuncture, neuromodulation, inflammatory modulation, visual analogue scale, pain management
Introduction
Lumbar disc herniation (LDH) is one of the most common degenerative disorders of the spine and is a leading cause of low back and leg pain in adults. Its lifetime prevalence is estimated at 12–30%, particularly affecting working-age populations and imposing substantial socioeconomic and healthcare burdens.1 Globally, low back pain represents the leading cause of years lived with disability, and lumbar disc pathology accounts for a major proportion of clinically significant cases worldwide, making LDH a major international public health concern. The underlying pathophysiology involves mechanical compression of the nerve root, narrowing of the intervertebral foramen, and activation of local inflammatory pathways. Contemporary imaging and neurobiological evidence further highlight the contribution of inflammatory mediators—including interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and matrix metalloproteinase-3 (MMP-3)—to radicular pain, making the modulation of neuroinflammation and the spine–nerve interface key therapeutic targets.2
Conventional treatments for LDH include nonsteroidal anti-inflammatory drugs (NSAIDs), traction, epidural steroid injections, physical therapy, and, in selected cases, minimally invasive or open surgery. However, clinical management strategies differ substantially across countries: Western healthcare systems primarily emphasize pharmacological, rehabilitative, and surgical approaches, whereas acupuncture is more commonly incorporated into routine LDH management in East Asian countries as part of integrative medical models. Pharmacological treatments may provide short-term relief but are often limited by gastrointestinal or cardiovascular side effects and variable patient tolerance.3 Surgical decompression offers rapid improvement for some patients, yet concerns remain regarding recurrence, long-term outcomes, and suitability for non-severe presentations.4 These limitations have stimulated growing interest in integrating nonpharmacological therapies into modern multidisciplinary pain management.
Acupuncture has been widely used in LDH management because of its well-documented analgesic effects, regulation of neuromuscular tension, and modulation of neuroimmune activity. Experimental and clinical studies have demonstrated that acupuncture can inhibit peripheral and central sensitization, downregulate pro-inflammatory mediators (such as TNF-α, IL-1β, and IL-6), promote endogenous opioid release, and regulate spinal–supraspinal pain pathways, thereby alleviating radicular pain and functional impairment.5–7
Among acupuncture systems, Governor Vessel–based approaches, such as Tongdu therapy, Wenyang Tongluo techniques, Bushen–Huoxue methods, and spine-regulating Governor Vessel strategies have gained growing clinical interest.8–11 The Governor Vessel runs along the posterior midline of the body and anatomically overlies the spinous processes, paraspinal muscles, spinal nerves, and posterior spinal structures.12 Modern neuroanatomical and neurophysiological evidence suggests that stimulation of points along the Governor Vessel can influence spinal segmental reflexes, paraspinal muscle tone, microcirculation, and neuroimmune signaling, making it a biologically plausible and anatomically relevant therapeutic target for lumbar disc herniation.12,13
From a mechanistic perspective, needling Governor Vessel–related points may activate paraspinal muscle reflexes,14 reduce pathological muscle guarding,15 promote microcirculatory improvement,16 and enhance the release of endogenous analgesic peptides such as β-endorphin.17 Experimental studies also suggest downregulation of pro-inflammatory mediators, providing a plausible biological basis for pain reduction.6,18
In clinical practice, these techniques are often combined with traction, bloodletting-cupping, extracorporeal shockwave therapy, or massage, forming multimodal treatment strategies.1 This integrative approach is commonly adopted to enhance overall therapeutic efficacy and to address the multifactorial pathophysiology of lumbar disc herniation, including pain, inflammation, and neuromuscular dysfunction, rather than because these acupuncture techniques are ineffective when used alone. However, current evidence largely originates from small, single-center randomized trials with heterogeneous interventions, inconsistent reporting, and variable methodological rigor.19,20 Rather than excluding such studies, the present review seeks to address this limitation by explicitly incorporating them and applying predefined subgroup analyses to disentangle the effects of Governor Vessel–based acupuncture when used alone or in combination with other therapies. Consequently, important questions remain unresolved, including the comparative efficacy of different Governor Vessel–based acupuncture paradigms, the magnitude of their analgesic benefits, and whether combined interventions provide additional therapeutic value.21,22
To address these uncertainties, we conducted a systematic review and meta-analysis of randomized controlled trials evaluating Governor Vessel–based acupuncture for LDH. The analysis synthesized evidence on clinical effectiveness, pain reduction measured by the visual analogue scale (VAS), and functional improvement. Subgroup analyses were performed to compare distinct acupuncture paradigms and treatment modes. Risk-of-bias assessment, sensitivity analyses, and publication bias evaluation were incorporated to ensure the robustness of the findings. This study aims to provide comprehensive and high-quality evidence to support the clinical application, standardization, and further refinement of Governor Vessel–based acupuncture in LDH management.
Methods
Literature Search Strategy
This systematic review and meta-analysis were conducted in accordance with the PRISMA 2020 guidelines. A comprehensive search of PubMed, Web of Science, CNKI, Wanfang, VIP, CBM, Embase, AMED, and CINAHL Plus databases were performed from inception to January 2026. The search strategy combined controlled vocabulary termsand free-text keywords related to lumbar disc herniation, acupuncture and randomized controlled trials, using appropriate Boolean operators. Search strategies were adapted for each database. Full electronic search strategies are provided in Supplementary Table S1. Additional manual searches of reference lists, reviews, clinical guidelines, and grey literature were conducted to minimize omissions. All retrieved records were imported into EndNote for automatic and manual duplication. The overall search and screening procedure is shown in Figure 1.
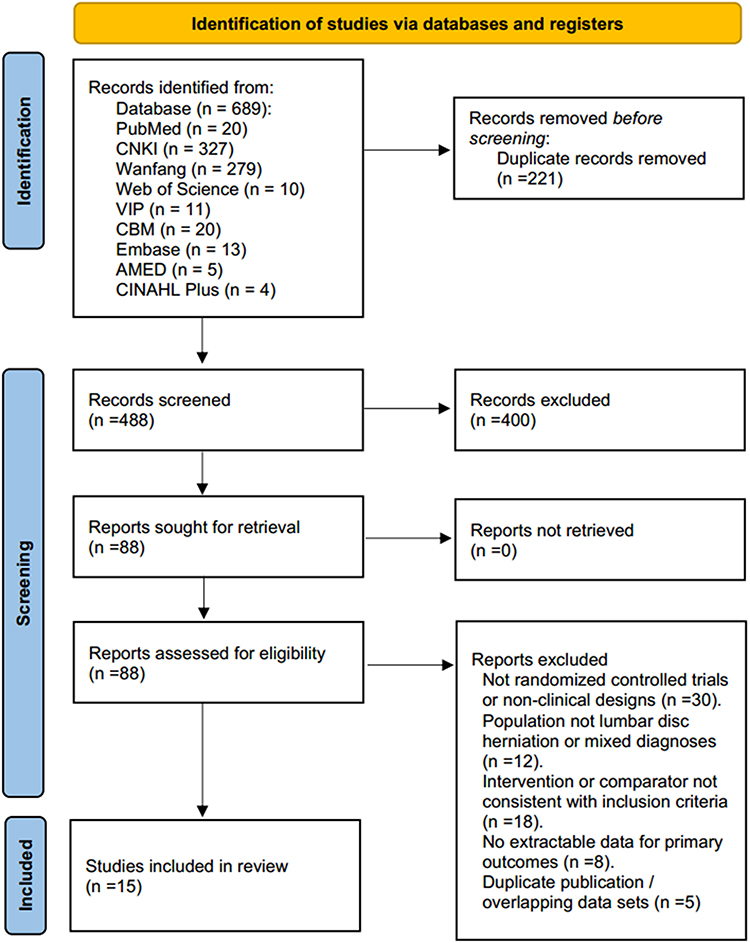 |
Figure 1 PRISMA flow diagram. Flow diagram summarizing the identification, screening, eligibility assessment, and final inclusion of randomized controlled trials. A total of 689 records were retrieved; 15 studies met eligibility criteria and were included in the meta-analysis. |
Inclusion and Exclusion Criteria
Studies were included if they met all the following conditions:
(1) Study design: randomized controlled trials (RCTs); (2) Participants: patients diagnosed with lumbar disc herniation based on clearly defined clinical or radiological criteria; (3) Interventions: experimental groups treated with Governor Vessel–based acupuncture techniques, including Wenyang Tongluo acupuncture, Bushen–Huoxue acupuncture, spine-regulating Governor Vessel therapy, Tongdu-based analgesic techniques, or related systems, administered alone or combined with adjunctive therapies such as traction, cupping, shockwave therapy, acupoint massage, or topical herbal applications. Combined-intervention trials were included to reflect real-world practice and to enable predefined subgroup analyses (acupuncture alone vs combined therapy; (4) Comparators: conventional acupuncture, routine acupuncture, physiotherapy, NSAIDs, standard Western medical treatment, traction, or any other recognized control intervention; (5) Outcomes: reporting at least one core endpoint, including overall clinical effectiveness or visual analogue scale (VAS) pain scores; (6) Data availability: studies reporting extractable quantitative data for at least one prespecified outcome, including sample size and effect estimates (eg, means and standard deviations), either directly reported or obtainable through standard data extraction or conversion methods.
Studies were excluded if any of the following conditions applied:
(1) Reviews, case reports, expert opinions, or experience-based articles; (2) mixed or poorly defined interventions where the independent effect of Governor Vessel–based acupuncture could not be determined; (3) absence of core outcome data or inability to extract effect-size information; (4) duplicate publications or studies with overlapping datasets; (5) studies irrelevant to the clinical question or not involving Governor Vessel–related acupuncture modalities.
Study Selection and Data Extraction
Two reviewers independently screened titles, abstracts, and full texts against predefined criteria, resolving disagreements through discussion with a third reviewer. Extracted data included author, year of publication, sample size, age, disease duration, intervention and control details, treatment frequency and duration, study design characteristics, and primary outcomes. When outcome data were incomplete, values were inferred from graphs or tables, or attempts were made to contact the original authors. Ultimately, a total of 15 randomized controlled trials23–37 were included in the final quantitative synthesis. (Figure 1)
Risk-of-Bias Assessment
Risk of bias was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool for randomized trials. Each included study was evaluated across five domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. Two reviewers independently performed the assessment, and disagreements were resolved through discussion.
Using the RoB 2 tool, most included studies were judged to have a low risk of bias across several domains; however, some concerns were identified in specific domains, particularly related to the randomization process and selective reporting. One study was rated as having a high risk of bias in the randomization process due to insufficient reporting of random sequence generation. Overall, most studies were judged to have a low overall risk of bias, with one study classified as high risk (Figure 2).
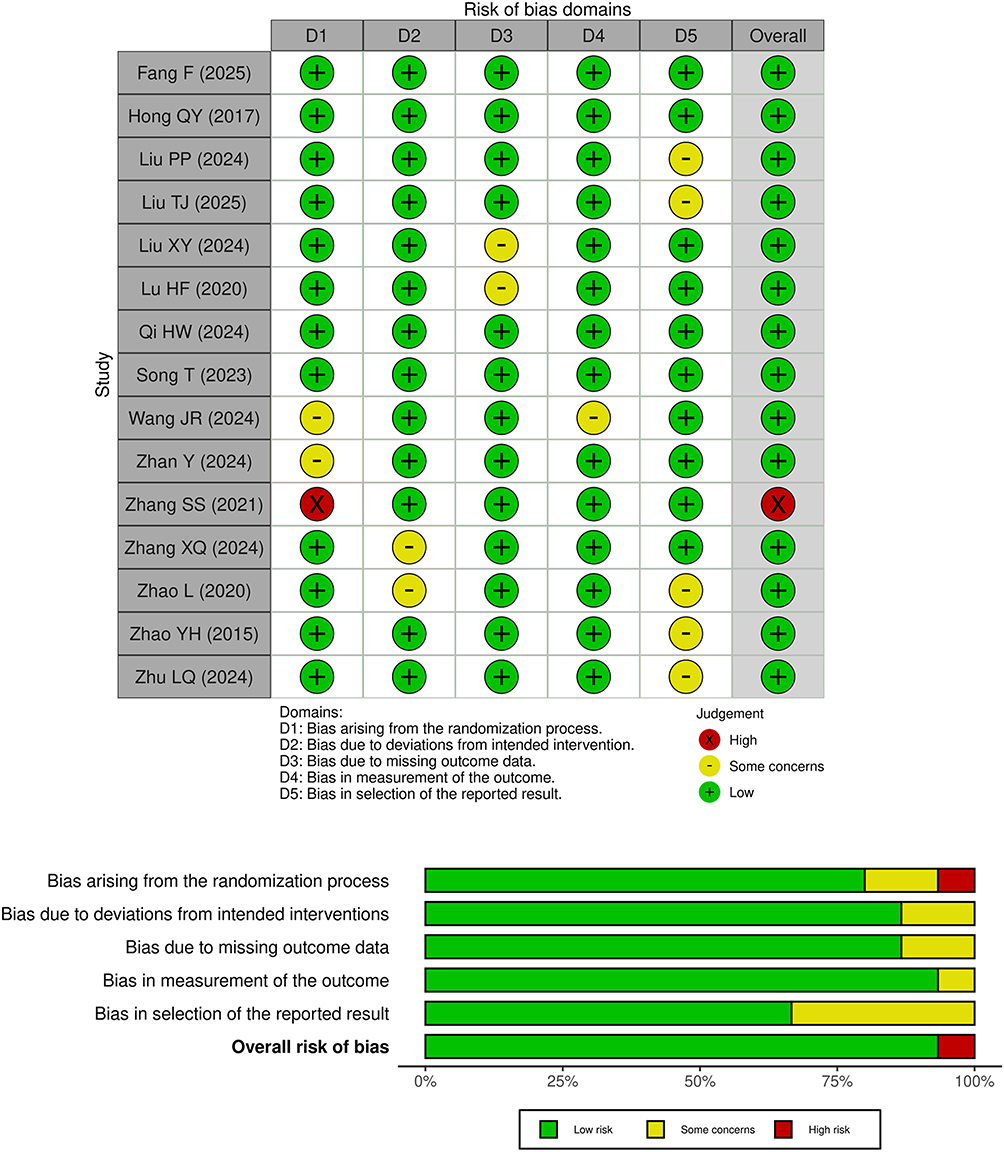 |
Figure 2 Risk-of-bias assessment of included studies. Risk of bias of the included randomized controlled trials was assessed using the Cochrane Risk of Bias 2 (RoB 2) tool across five domains: (D1) bias arising from the randomization process; (D2) bias due to deviations from intended interventions; (D3) bias due to missing outcome data; (D4) bias in measurement of the outcome; and (D5) bias in selection of the reported result. The upper panel presents the traffic light plot showing domain-level judgments for each individual study, while the lower panel summarizes the overall distribution of risk of bias judgments across studies. Green indicates low risk of bias, yellow indicates some concerns, and red indicates high risk of bias. |
Evidence Quality Assessment
The certainty of evidence for key outcomes was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. Evidence was evaluated across five domains, including risk of bias, inconsistency, indirectness, imprecision, and other considerations. The GRADEpro GDT online tool (https://gradepro.org/) was used to generate a structured Summary of Findings table Overall clinical effectiveness and pain intensity measured by the visual analogue scale (VAS) were prespecified as critical outcomes.
Statistical Analysis
Meta-analyses were performed using Review Manager 5.4 and R version 4.3.1 (meta and metafor packages). For dichotomous outcomes such as overall clinical effectiveness, risk ratios (RRs) with 95% confidence intervals (CIs) were calculated. For continuous outcomes such as VAS scores, standardized mean differences (SMDs) were applied due to variations in measurement scales across studies. Heterogeneity was assessed using Cochran’s Q test and the Higgins I2 statistic, with fixed-effects models used when I2 ≤ 50% and random-effects models applied when I2 > 50%. Predefined subgroup analyses examined differences across acupuncture paradigms and treatment modes (acupuncture alone vs combined therapy). Sensitivity analysis was conducted using a leave-one-out approach, and publication bias was assessed using funnel plots. Statistical significance was defined as a two-sided P value < 0.05.
Results
Balanced Baseline Profiles
A total of 15 randomized controlled trials involving 670 patients with lumbar disc herniation were included (Figure 1). Across studies, sample size, intervention characteristics, and outcome measures demonstrated good overall comparability. Participants were predominantly middle-aged adults, with mean ages ranging from approximately 41 to 53 years across treatment and control groups. Disease duration was moderately consistent, spanning 2 to 6 weeks in most trials, with only one study reporting a 1-month course.
Interventions were categorized into three major Governor Vessel–related acupuncture systems—GV-warming–Yang/Tongluo, spine-regulating GV, and tonifying-kidney/activating-blood techniques—either applied alone or combined with adjunctive therapies such as bloodletting-cupping, radial shockwave therapy, lumbar traction, acupoint massage, or herbal plaster. Comparator groups primarily received conventional acupuncture, routine conservative care, NSAIDs, lumbar traction, or meloxicam with epidural block. Among the included studies, only four trials employed single-modality Governor Vessel–based acupuncture, whereas the majority applied combined interventions. Accordingly, comparisons between integrated and independent strategies were exploratory in nature, and the limited number of single-modality studies may restrict the precision of efficacy estimates (Table 1).
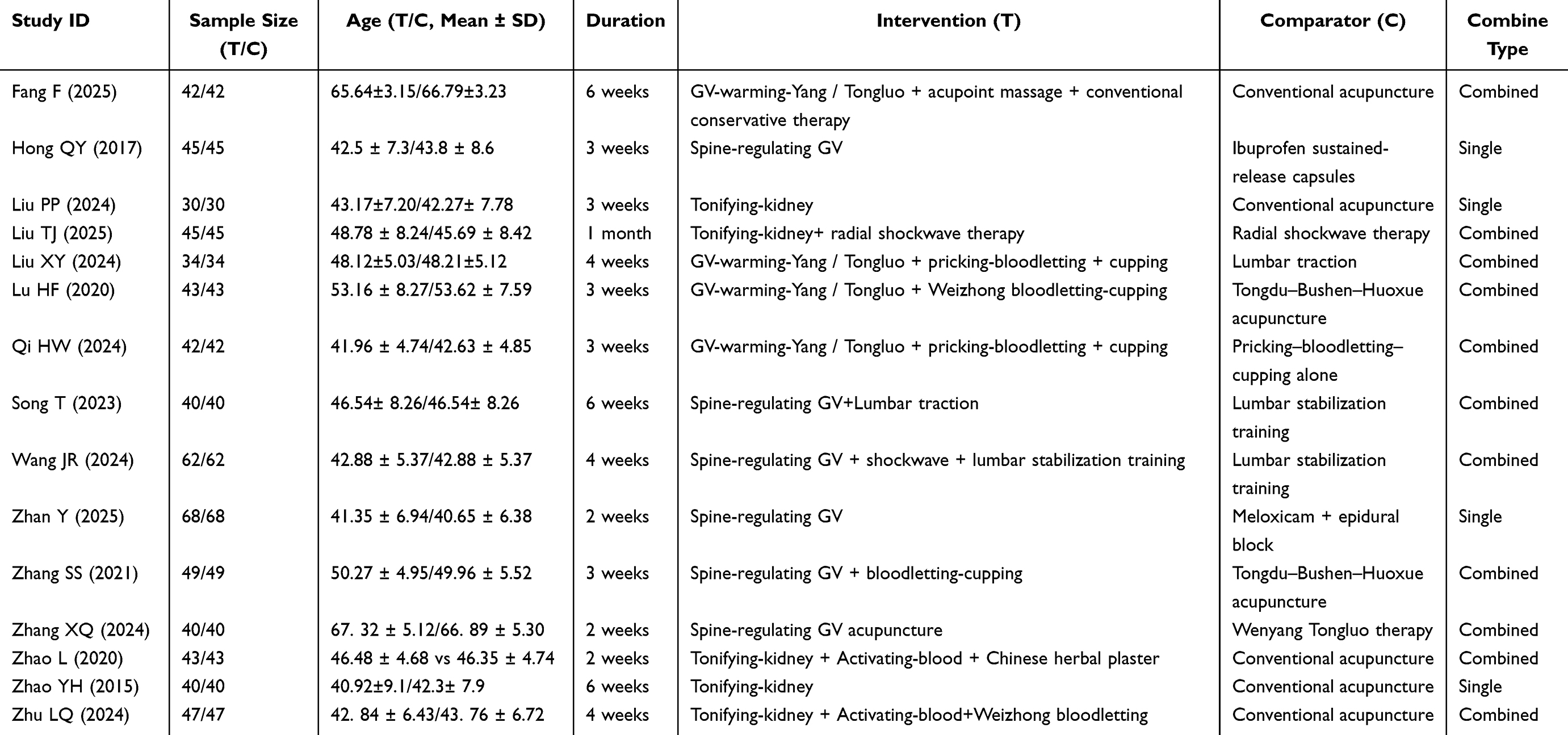 |
Table 1 Baseline Characteristics and Treatment Profiles Included Randomized Controlled Trials |
Reporting of allocation concealment and blinding was limited; however, risk-of-bias assessment (Figure 2) indicated that most studies presented low risk in selective reporting and incomplete outcome data. Random sequence generation was generally rated as low to moderate risk. Taken together, the baseline characteristics across studies were broadly balanced between groups, and the methodological quality of the included trials was acceptable for quantitative synthesis.
Tongdu-Related Acupuncture Significantly Improved Overall Clinical Effectiveness
All trials demonstrated higher clinical effectiveness rates in the Governor Vessel–based acupuncture group compared with controls. The fixed-effects model showed a statistically significant improvement in overall effectiveness (RR = 1.21, 95% CI 1.15–1.27; P < 0.0001) with negligible heterogeneity (I2 = 0%) (Figure 3). The prediction interval (1.15–1.28) further suggests that this therapeutic benefit is likely to persist across future studies. These findings indicate a consistent short-term symptomatic improvement associated with Tongdu-based acupuncture therapies.
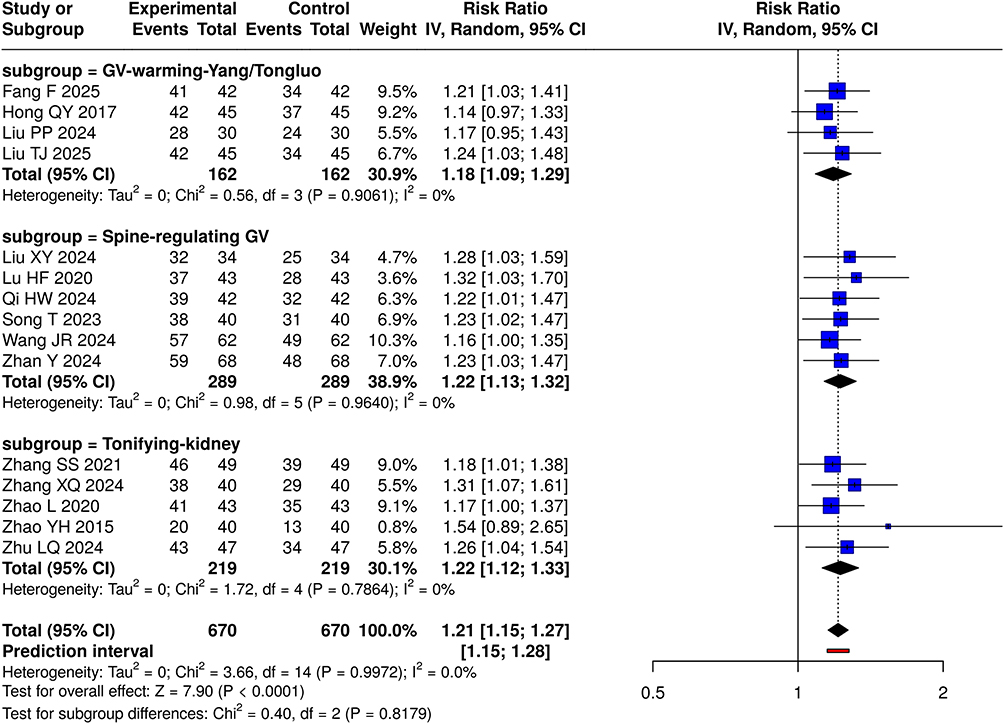 |
Figure 3 Overall and subgroup meta-analysis of clinical effectiveness. Forest plot comparing overall clinical effectiveness between Governor Vessel–based acupuncture and control interventions. Subgroup analyses stratified by GV-warming–Yang/Tongluo, spine-regulating GV, and tonifying-kidney/activating-blood techniques showed consistently favorable effects across all systems. RRs are presented with 95% CIs. Squares represent individual study estimates, with the size of the square proportional to study weight. Horizontal lines indicate 95% CIs. Diamonds represent pooled effect estimates. The vertical solid line indicates no effect (RR = 1). Bold values indicate pooled results. Prediction interval is shown in red. |
Comparable Effectiveness Across Different Tongdu-Based Acupuncture Systems
Based on underlying theoretical principles, trials were categorized into GV-warming–Yang/Tongluo, spine-regulating GV, and tonifying-kidney with activating-blood systems. All subgroups demonstrated significant therapeutic advantage over controls. Between-group differences were not statistically significant (P = 0.8038) (Figure 3), indicating that despite variations in manipulation techniques and conceptual frameworks, different Tongdu-related acupuncture systems achieve largely consistent clinical outcomes. This suggests a shared therapeutic mechanism grounded in spinal functional regulation and meridian modulation.
Combination Therapies Showed a Tendency Toward Enhanced Benefit but without Significant Superiority
Some trials used acupuncture alone, whereas others integrated traction, bloodletting, shock-wave therapy, or manual manipulation. Subgroup analysis showed slightly larger effect sizes in combined-therapy trials (RR = 1.22) compared with single-technique acupuncture (RR = 1.18), although the difference was not significant (P = 0.6112) (Figure 4). These findings suggest that while multimodal strategies may reinforce therapeutic effects, standalone Tongdu acupuncture already provides a substantial clinical benefit, and current evidence does not establish the superiority of combined interventions.
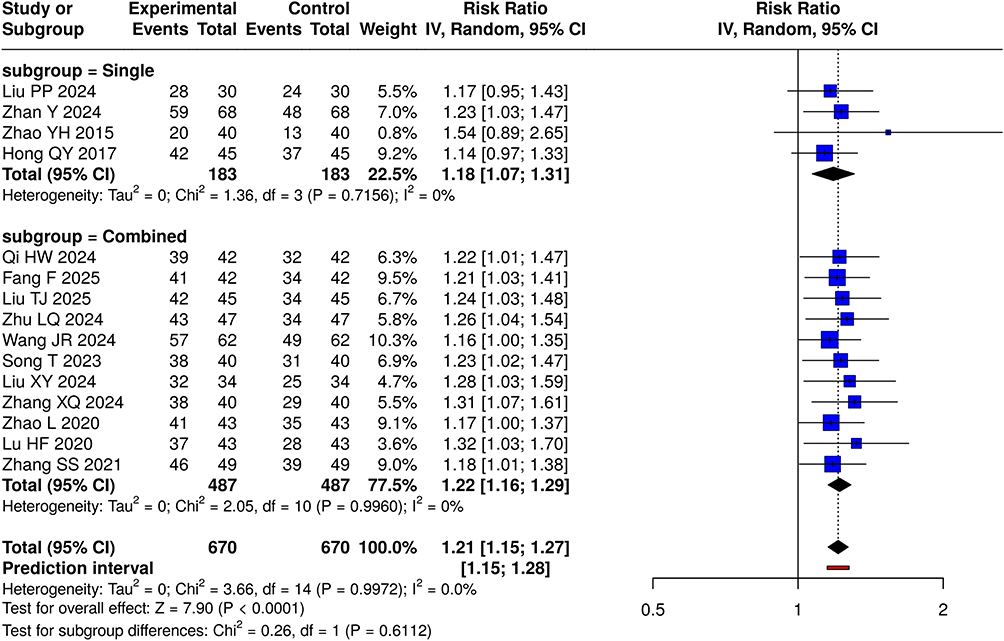 |
Figure 4 Meta-analysis of clinical effectiveness by treatment mode. Forest plot comparing acupuncture alone versus combined therapy (eg, traction, shockwave, bloodletting-cupping). RRs with 95% CIs are shown. Squares represent individual studies and diamonds indicate pooled estimates. The vertical solid line denotes no treatment effect (RR = 1). Bold values indicate pooled results. Both groups demonstrated improved clinical effectiveness without significant differences between treatment modes. |
Tongdu-Based Acupuncture Produced Significant Reductions in Pain Intensity (VAS)
Fourteen trials reported changes in VAS scores. Pooled results demonstrated a significant reduction in pain in the acupuncture group (SMD = –1.77, 95% CI –2.18 to –1.36; P < 0.0001) (Figure 5). Despite substantial heterogeneity (I2 = 88.1%), all individual studies favored acupuncture over control interventions. Differences in treatment duration, baseline pain severity, and auxiliary modalities likely contributed to heterogeneity but did not affect the overall trend toward pain alleviation.
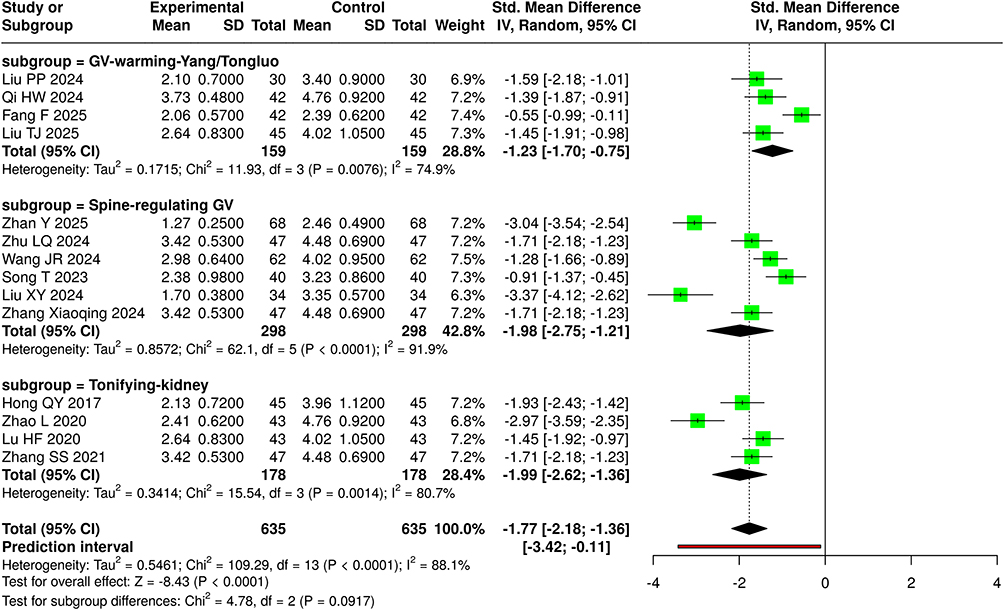 |
Figure 5 Meta-analysis of pain intensity (VAS). Forest plot presenting standardized meaning differences in VAS reduction between acupuncture and control groups. Tongdu-related acupuncture produced significant pain alleviation across included studies. Squares represent individual study effect sizes and horizontal lines indicate 95% CIs. Diamonds represent pooled estimates. The vertical solid line indicates no effect (SMD = 0). Negative values indicate pain reduction in the acupuncture group. Bold values indicate pooled results. Prediction interval is shown in red. |
Analgesic Effects of Governor Vessel Based Acupuncture Alone or in Combination for Lumbar Disc Herniation
Subgroup analysis showed that both single acupuncture and acupuncture combined with other therapies significantly reduced pain compared with control treatments. The overall pooled effect favored Governor Vessel–based acupuncture (SMD = −1.77, 95% CI −2.18 to −1.36, P < 0.001) (Figure 6), with substantial heterogeneity (I2 = 88.1%). No significant difference was observed between the two subgroups (P = 0.27).
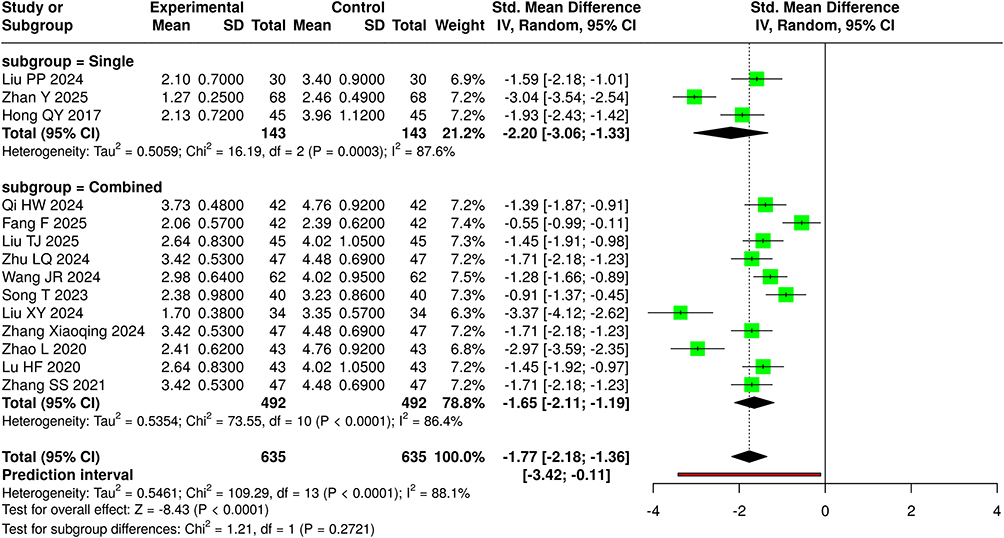 |
Figure 6 Subgroup meta-analysis of VAS reduction. Forest plot showing VAS improvement across three acupuncture paradigms: GV-warming–Yang/Tongluo, spine-regulating GV, and tonifying-kidney approaches. SMDs with CIs are shown. Squares represent individual studies and diamonds indicate pooled subgroup estimates. The vertical solid line represents no effect (SMD = 0). Negative values indicate pain reduction. Bold values indicate pooled results. All subtypes yielded significant pain reduction with no significant subgroup differences. |
Certainty of Evidence According to the GRADE Approach
The certainty of evidence for the key outcomes was assessed using the GRADE approach (Table 2). The evidence for both overall clinical effectiveness and pain intensity measured by VAS was rated as low, mainly due to methodological limitations and heterogeneity across the included randomized controlled trials. Both outcomes were considered critical for clinical decision-making.
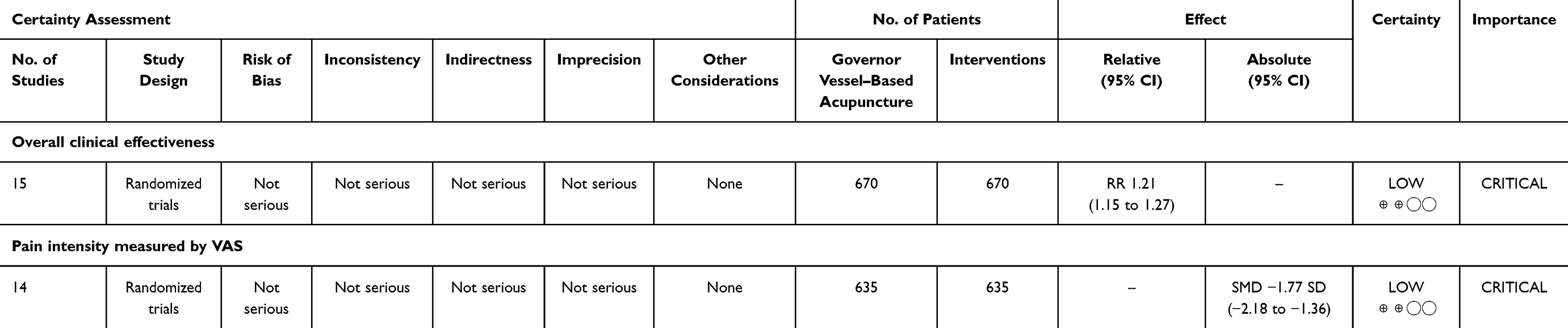 |
Table 2 GRADE Summary of Findings for Governor Vessel–Based Acupuncture in Lumbar Disc Herniation |
Publication Bias Assessment Suggested Stable and Reliable Results
The funnel plot demonstrated an overall symmetrical distribution with only mild right-sided deviation (Figure 7), indicating minimal risk of small-study effects. The primary findings are therefore unlikely to be materially influenced by publication bias.
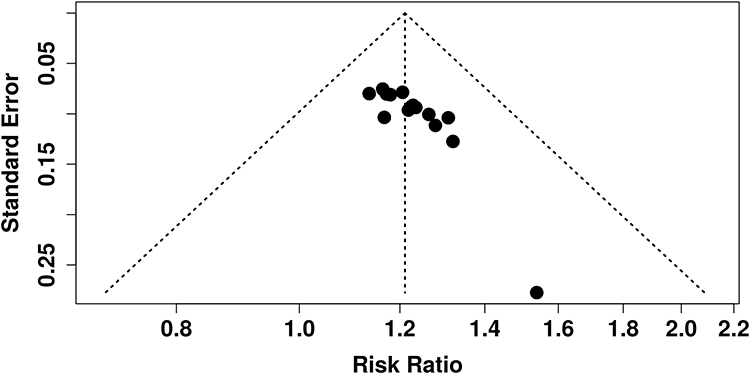 |
Figure 7 Funnel plot for publication bias assessment. Funnel plot evaluating small-study effects for clinical effectiveness outcomes. The distribution was generally symmetrical, suggesting minimal publication bias. |
Discussion
This systematic review synthesizes current evidence regarding the use of Governor Vessel–related acupuncture therapies for acute-stage LDH and demonstrates overall favorable therapeutic outcomes across major clinical outcomes, including overall effectiveness and pain reduction.38–40 The meta-analysis revealed that these techniques significantly improved clinical efficacy and produced moderate-to-large effect sizes in pain relief, with remarkably consistent results across different Governor Vessel–based acupuncture systems.41,42 This suggests that whether the therapeutic rationale emphasizes warming and activating the Yang meridians, regulating the spine and paraspinal muscles, or tonifying the kidney and promoting blood circulation, these modalities may converge on similar therapeutic pathways targeting the spinal axis, periarticular tissues, and myofascial tension modulation.3,40
The stable analgesic effect observed in this review carries substantial clinical implications. Patients with acute LDH typically experience a combination of nerve root inflammation, protective paraspinal muscle spasm, and mechanical compression. Although NSAIDs remain the standard first-line therapy, their clinical utility is often limited by gastrointestinal or cardiovascular intolerance, and some patients respond inadequately. By stimulating Governor Vessel–related acupoints along the midline and paraspinal regions, acupuncture may exert dual mechanisms: regulating deep stabilizing muscles such as the multifidus to reduce mechanical irritation around the nerve root and modulating segmental neural activity to enhance endogenous analgesic signaling (eg, β-endorphin release), thereby reducing central sensitization.43,44 These multimodal actions align well with contemporary pain management strategies, making Governor Vessel acupuncture a potentially valuable intervention during the acute symptomatic phase.45
The therapeutic consistency observed across different acupuncture systems suggests that Governor Vessel–based interventions possess a relatively “platform-like” efficacy mechanism. Despite theoretical distinctions, most techniques focus on the lumbar Governor Vessel pathway and adjacent paraspinal structures, producing overlapping biomechanical and neuroregulatory effects.39,42,45 Clinically, this means that practitioners may select among these acupuncture systems according to patient constitution, pain characteristics, and operational feasibility without concern for major differences in treatment effectiveness.42,46
Although combined interventions, such as acupuncture with traction, bloodletting, shockwave therapy, or manual therapies showed slightly stronger effect sizes, subgroup comparisons did not demonstrate statistically significant differences47 This indicates that Governor Vessel acupuncture alone provides substantial therapeutic value, while combination strategies may enhance patient experience or provide complementary mechanisms rather than representing the primary driver of treatment efficacy.48 For acute LDH, such flexibility allows individualized integration of multimodal therapies within a safe and controllable therapeutic framework.49
Nevertheless, the therapeutic efficacy of acupuncture remains a subject of ongoing debate. Several high-quality randomized controlled trials and systematic reviews in musculoskeletal pain have reported that the benefits of acupuncture may not consistently exceed those of sham acupuncture, suggesting that observed effects may partly reflect placebo responses, contextual healing factors, or nonspecific neurophysiological stimulation.50–52 These findings highlight the potential contribution of expectancy, patient and practitioner interaction, and treatment ritual to clinical outcomes.53 Accordingly, although our meta-analysis demonstrates favorable outcomes associated with Governor Vessel–based acupuncture, these results should be interpreted with caution, as limited blinding, heterogeneous control conditions, and variable methodological rigor across trials may have influenced effect estimates.
Overall, the present findings support the consideration of Governor Vessel acupuncture as an important treatment option for acute LDH, especially for patients seeking rapid pain relief while minimizing medication exposure.40 Acupuncture provides a repeatable, relatively low-risk intervention that does not disrupt daily activity and adds a valuable modality to multidisciplinary pain management.3 Despite the robustness of the pooled results, several limitations must be acknowledged. First, the relatively small number of trials using single-modality Governor Vessel–based acupuncture limited the precision of comparisons between independent and combined strategies. Reporting randomization and blinding procedures was generally insufficient, raising concerns regarding potential methodological bias.39,54 Follow-up durations in most studies were short, preventing conclusions on long-term outcomes or recurrence rates.48 Moreover, procedural heterogeneity—such as variations in needle retention time, stimulation intensity, and treatment frequency likely contributed to residual heterogeneity in the quantitative synthesis.55 Future research should prioritize rigorously designed multicenter randomized trials with appropriate sham controls and standardized intervention protocols to further clarify the specific versus nonspecific effects of Governor Vessel acupuncture, to identify optimized treatment strategies for different patient subgroups.
Conclusion
This systematic review and meta-analysis suggest that Governor Vessel–based acupuncture is associated with significant short-term improvements in pain and overall clinical effectiveness in acute lumbar disc herniation. Consistent benefits were observed across different Governor Vessel–related paradigms, supporting the clinical relevance of targeting the spinal midline and paraspinal axis. By integrating current randomized evidence, this study provides a structured synthesis supporting the role of Governor Vessel–based acupuncture as a potential nonpharmacological option within contemporary pain management for acute LDH. However, well-designed, sham-controlled, multicenter trials are required to confirm specific efficacy, clarify mechanisms, and determine long-term outcomes.
Data Sharing Statement
All data supporting the findings of this study are included within the article and its supplementary materials. No new data was generated. Extracted data and analytical methods are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Ethical approval and informed consent were not required for this study. The study did not involve any new experiments on human participants or animals, nor did it include the collection of individual-level patient data. All included studies were conducted in accordance with their respective institutional ethical standards.
Consent for Publication
Not applicable. This manuscript does not contain any individual person’s data, images, videos, recordings, or other potentially identifiable information. Therefore, consent for publication was not required.
Acknowledgments
Shuai Yang and Qngfeng Guo are co-first authors for this study. The authors would like to thank all investigators and participants of the original studies included in this meta-analysis.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or non-profit sectors.
Disclosure
The authors declare that they have no known competing financial or non-financial interests that could have appeared to influence the work reported in this paper.
References
1. Zhong X, Liu J, Wang Y, Zhang L, Zhang H. Which of the acupuncture treatment regimen for lumbar disc herniation is more effective and safer: a protocol for systematic review and network meta-analysis. Medicine. 2021;100(12):e25199. doi:10.1097/MD.0000000000025199
2. Cunha C, Silva AJ, Pereira P, Vaz R, Goncalves RM, Barbosa MA. The inflammatory response in the regression of lumbar disc herniation. Arthritis Res Ther. 2018;20(1):251. doi:10.1186/s13075-018-1743-4
3. Wu Y, Sun Y, Zhang J, Li Y, Wang C. Clinical research of mild and moderate lumbar disc herniation of blood stagnation syndrome treated with qi-conducting needling technique at the governor vessel acupoints combined with electroacupuncture. Zhongguo Zhen Jiu. 2017;37(5):467–15. doi:10.13703/j.0255-2930.2017.05.004
4. Ha-Na K, Jun-Yeon K, Kyeong-Ju P, et al. An economic evaluation of thread embedding acupuncture for the treatment of lumbar herniated intervertebral disc in a randomized controlled clinical trial. J Acupuncture Res. 2021;38(4):312–319. doi:10.13045/jar.2021.00199
5. Torres-Rosas R, Yehia G, Pena G, et al. Dopamine mediates vagal modulation of the immune system by electroacupuncture. Nat Med. 2014;20(3):291–295. doi:10.1038/nm.3479
6. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/ALN.0000000000000101
7. Li T, Wang S, Zhang S, et al. Evaluation of clinical efficacy of silver-needle warm acupuncture in treating adults with acute low back pain due to lumbosacral disc herniation: study protocol for a randomized controlled trial. Trials. 2019;20(1):470. doi:10.1186/s13063-019-3566-2
8. Wang P, Wang Z, Li ZX, et al. Efficacy and safety of Tongdutiaoshen acupuncture on insomnia in maintenance hemodialysis patients: a randomized clinical trial protocol. Contemp Clin Trials Commun. 2023;35:101196. doi:10.1016/j.conctc.2023.101196
9. Xi Mali LC, Paoqiu W, Wei L, Longze T. Effect of Wenyang Tongluo acupuncture and moxibustion on spastic state of upper limb muscle group, limb motor function and EEG power in children with spastic cerebral palsy. Chin Pediatrics Integr Trad Western Med. 2023;15(4):347–351. doi:10.3969/j.issn.1674-3865.2023.04.016
10. Zhu H, Zhang T, Li R, Ren D, Xu J, Xiao L. Bushen Huoxue acupuncture ameliorates Alzheimer’s disease by upregulating MARCHF3 to induce NLRP3 ubiquitination and inhibit caspase-1-dependent pyroptosis. Metab Brain Dis. 2024;40(1):11. doi:10.1007/s11011-024-01459-9
11. Mo YP, Yao HJ, Lv W, et al. Effects of electroacupuncture at governor vessel acupoints on Neurotrophin-3 in rats with experimental spinal cord injury. Neural Plast. 2016;2016:2371875. doi:10.1155/2016/2371875
12. Dorsher PT, da Silva MAH. Acupuncture’s neuroanatomic and neurophysiologic basis. Longhua Chin Med. 2021;5. doi:10.21037/lcm-21-48
13. Mo Z, Li D, Zhang R, Chang M, Yang B, Tang S. Comparisons of the effectiveness and safety of tuina, acupuncture, traction, and Chinese herbs for lumbar disc herniation: a systematic review and network meta-analysis. Evid Based Complement Alternat Med. 2019;2019:6821310. doi:10.1155/2019/6821310
14. Lim TK, Ma Y, Berger F, Litscher G. Acupuncture and neural mechanism in the management of low back pain-an update. Medicines. 2018;5(3). doi:10.3390/medicines5030063
15. Li HL, Zhang Y, Zhou JW. Acupuncture for radicular pain: a review of analgesic mechanism. Front Mol Neurosci. 2024;17:1332876. doi:10.3389/fnmol.2024.1332876
16. Min S, Lee H, Kim SY, et al. Local changes in microcirculation and the analgesic effects of acupuncture: a laser Doppler perfusion imaging study. J Altern Complement Med. 2015;21(1):46–52. doi:10.1089/acm.2013.0442
17. Ahsin S, Saleem S, Bhatti AM, Iles RK, Aslam M. Clinical and endocrinological changes after electro-acupuncture treatment in patients with osteoarthritis of the knee. Pain. 2009;147(1–3):60–66. doi:10.1016/j.pain.2009.08.004
18. Lin JG, Chen WL. Acupuncture analgesia: a review of its mechanisms of actions. Am J Chin Med. 2008;36(4):635–645. doi:10.1142/S0192415X08006107
19. Shi F, Wen H, Liu Y, et al. Comparative clinical efficacy of acupuncture combined with manipulation and other non-pharmacological interventions in the treatment of lumbar disc herniation: a prospective, multi-arm, randomized, open-label, blinded endpoint trial. Front Med Lausanne. 2024;11:1507115. doi:10.3389/fmed.2024.1507115
20. Yang Y, Liu L, Yuan L, et al. A randomized, sham-controlled trial on the efficacy and safety of electroacupuncture for lumbar disc herniation with radiculopathy: rationale and study protocol. J Pain Res. 2025;18:2307–2319. doi:10.2147/JPR.S512711
21. Chen M, Chen R, Xiong J, Yi F, Chi Z, Zhang B. Effectiveness of heat-sensitive moxibustion in the treatment of lumbar disc herniation: study protocol for a randomized controlled trial. Trials. 2011;12(1):226. doi:10.1186/1745-6215-12-226
22. Brotis AG, Kalogeras A, Spiliotopoulos T, Fountas KN, Demetriades AK. Physical therapies after surgery for lumbar disc herniation- evidence synthesis from 55 randomized controlled trials (RCTs) and a total of 4311 patients. Brain Spine. 2025;5:104238. doi:10.1016/j.bas.2025.104238
23. Fang F, Chen W, Zhang L. Observation on the curative effect of Wenyang Tongluo acupuncture combined with acupoint massage on elderly lumbar disc herniation of cold-damp obstruction type. Zhejiang J Trad Chin Med. 2024;59(2):189–192.
24. Hong Q, Wang G, Wang S, Liu X, Mao X, Zhao J. Clinical study of Tongdu Bushen Huoxue acupuncture for acute lumbar disc herniation. Beijing J Trad Chinese Med. 2017;49(8):54–56.
25. Liu P. Clinical Observation of Tongdu Wenyang Analgesic Acupuncture Method in the Treatment of Cold-Damp Type Lumbar Disc Herniation. Heilongjiang University of Traditional Chinese Medicine; 2024.
26. Liu T, Wang L. Tongdu Wenyang acupuncture combined with radial shock wave therapy for lumbar disc herniation with cold-dampness obstruction pattern. Inform Trad Chin Med. 2025;42(10):64–68. doi:10.19656/j.cnki.1002-2406.20251012
27. Liu X. Clinical observation of Tiaodu Lijin acupuncture as an adjunctive treatment for lumbar disc herniation. J Pract Trad Chin Med. 2024;40(3):472–473.
28. Lu H. Clinical observation of Tongdu Bushen Huoxue acupuncture combined with Weizhong bloodletting cupping in the treatment of acute lumbar disc herniation. Chin J Ethnomedicine Ethnopharm. 2020;29(19):93–95.
29. Qi H, Qi Y, Chen J, Gao L. Efficacy of Wenyang Tongluo acupuncture combined with pricking and cupping on lumbar disc herniation and its influence on lumbar range of motion, plasma β-endorphin, and inflammatory factors. Shaanxi J Trad Chin Med. 2024;45(10):140–145. doi:10.3969/j.issn.1000-7369.2024.10.028
30. Song T. Clinical study on Tiaoji Tongdu acupuncture combined with lumbar traction for lumbar disc herniation. New Chin Med. 2023;55(21):152–156. doi:10.13457/j.cnki.jncm.2023.21.028
31. Wang J, Hu L, Liu M. Clinical observation of Tiaoji Tongdu acupuncture combined with Cobamamide intramuscular injection in treatment of lumbar disc herniation. J Guangzhou Univer Trad Chin Med. 2024;41(11):2961–2967. doi:10.13359/j.cnki.gzxbtcm.2024.11.021
32. Zhan Y, Wang L, Jiang J. Clinical efficacy of Tiaoji Tongdu acupuncture on acute lumbar disc herniation and its effects on lumbar function and inflammatory factors. J Liaoning Univ Trad Chin Med. 2025.
33. Zhang S. Clinical observation on Tongdu Bushen Huoxue acupuncture combined with bloodletting cupping for acute lumbar disc herniation. J Pract Trad Chin Med. 2021;37(8):1426–1428.
34. Zhang X. Clinical efficacy of Tiaodu Lijin acupuncture combined with four-finger pushing spine adjustment in treatment of patients with lumbar disc herniation. Liaoning J Trad Chin Med. 2024;51(5):168–172. doi:10.13192/j.issn.1000-1719.2024.05.045
35. Zhao L, Zhao Y, Hu J, Chen S, Shao Q. Observation on the efficacy of Chinese herbal mud therapy combined with Tongdu Bushen Huoxue acupuncture in the treatment of acute phase lumbar disc herniation. Pract Clin J Integr Trad Chin Western Med. 2020;20(10):52–55. doi:10.13638/j.issn.1671-4040.2020.10.009
36. Zhao Y, Zhang J. Experience of Yang Jun in treating lumbar disc herniation with Bushen Huoxue acupuncture method. J Trad Chin Med. 2015;56(3):120–124. doi:10.3969/j.issn.2095-7246.2015.03.016
37. Zhu L, Wang D, Gao J, Shen J. Clinical study of Tiaoji Tongdu acupuncture combined with wrist-ankle acupuncture in treatment of lumbar disc herniation. J Clin Acupuncture Moxibustion. 2024;40(8):63–73. doi:10.19917/j.cnki.1005-0779.024152
38. Zhang S-N. Effect of dredging meridian and governor vessel manipulation on patients with lumbar intervertebral disc herniation. 2012.
39. Zhang K, Shen M, Zhang H, Ding L, Li C, Huang B. Research status and prospects of traditional chinese medicine in the treatment of lumbar intervertebral disc herniation. J Contemporary Med Pract. 2024. doi:10.53469/jcmp.2024.06(07).23
40. Zhan Y, Xia Y. Study on rehabilitation treatment of patients with lumbar disc herniation by acupuncture and massage. Highlights Sci Engineer Technol. 2023;45:329–333. doi:10.54097/hset.v45i.7485
41. Yan L, Zhang J, Wang X, et al. Efficacy of acupuncture for lumbar disc herniation: changes in paravertebral muscle and fat infiltration. Front Endocrinol. 2024;15. doi:10.3389/fendo.2024.1467769
42. Xue K, Wang X, Xiao C-H, et al. Clinical efficacy and safety of a modified moxibustion therapy for low back pain in lumbar disc herniation. J Pain Res. 2024;Volume 17:1853–1865. doi:10.2147/JPR.S457724
43. Wang Y-H, Zhou Y, Xie Y-Z, et al. The effect of ultrasound-guided acupotomy and Juanbi decoction on lumbar disc herniation: a randomized controlled trial. Medicine. 2023;102(1):e32622. doi:10.1097/MD.0000000000032622
44. Shi F, Wen H, Liu Y, et al. Comparative clinical efficacy of acupuncture combined with manipulation and other non-pharmacological interventions in the treatment of lumbar disc herniation. Front Med. 2025;11:1507115. doi:10.3389/fmed.2024.1507115
45. Y-x L, Xiong J, Zhang Z, et al. Research trends of the research and development of acupuncture and moxibustion therapy on lumbar disc herniation: a bibliometric analysis. J Pain Res. 2023;16:1835–1853. doi:10.2147/JPR.S400362
46. Zhong X-W, Liu J, Wang Y, Zhang L-Z, Zhang H. Which of the acupuncture treatment regimen for lumbar disc herniation is more effective and safer. Medicine. 2021;100(12):e25199. doi:10.1097/MD.0000000000025199
47. Li C, Li T, Ma X, Ni C, Wei X-Y, Zhang S. A randomized clinical study on acupuncture therapy for relieving sciatica caused by lumbar disc herniation. Indian J Pharm Sci. 2021;83:5–9. doi:10.36468/pharmaceutical-sciences.spl.284
48. Inoue M, Kitakoji H, Yano T, Ishizaki N, Itoi M, Katsumi Y. Acupuncture treatment for low back pain and lower limb symptoms—the relation between acupuncture or electroacupuncture stimulation and sciatic nerve blood flow. Evid Based Complement Alternat Med. 2007;5(2):133–143. doi:10.1093/ecam/nem050
49. Lee J, Shin JS, Lee YJ, et al. Effects of Shinbaro pharmacopuncture in sciatic pain patients with lumbar disc herniation: study protocol for a randomized controlled trial. Trials. 2015;16(1):455. doi:10.1186/s13063-015-0993-6
50. Yuan QL, Wang P, Liu L, et al. Acupuncture for musculoskeletal pain: a meta-analysis and meta-regression of sham-controlled randomized clinical trials. Sci Rep. 2016;6(1):30675. doi:10.1038/srep30675
51. Yu C, Zhang R, Shen B, et al. Effects of sham acupuncture for chronic musculoskeletal pain syndrome: a systematic review and network meta-analysis of randomized controlled trials. Medicine. 2023;102(46):e35275. doi:10.1097/MD.0000000000035275
52. Hinman RS, McCrory P, Pirotta M, et al. Acupuncture for chronic knee pain: a randomized clinical trial. JAMA. 2014;312(13):1313–1322. doi:10.1001/jama.2014.12660
53. Wasan AD, Kong J, Pham LD, Kaptchuk TJ, Edwards R, Gollub RL. The impact of placebo, psychopathology, and expectations on the response to acupuncture needling in patients with chronic low back pain. J Pain. 2010;11(6):555–563. doi:10.1016/j.jpain.2009.09.013
54. He SH, Tan HS, Huang Y, et al. Study on the clinical effect of Meridian massage in the treatment of lumbar disc herniation. Zhongguo Gu Shang. 2024;37(10):991–996. doi:10.12200/j.issn.1003-0034.20240311
55. Cai C, Gong Y, Dong D, et al. Combined therapies of modified taiyi miraculous moxa roll and cupping for patients with lumbar intervertebral disc herniation. Evid Based Complement Alternat Med. 2018;2018(1). doi:10.1155/2018/6754730
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.