Back to Journals » Clinical Ophthalmology » Volume 19
Efficacy of Combined Phacoemulsification and Hydrus Microstent in Open-Angle Glaucoma Versus Combined-Mechanism/Primary Angle Closure Glaucoma
Authors Nguyen K, Chansangpetch S, Vinh MK, Tran AQH, Radhakrishnan S ![]() , Nguyen N
, Nguyen N ![]() , Iwach AG, Lin S
, Iwach AG, Lin S ![]()
Received 12 June 2025
Accepted for publication 1 September 2025
Published 11 September 2025 Volume 2025:19 Pages 3347—3356
DOI https://doi.org/10.2147/OPTH.S538439
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Kelly Nguyen,1 Sunee Chansangpetch,2– 4 Minh-Khanh Vinh,5 Alan Quang Huy Tran,6 Sunita Radhakrishnan,7,8 Ngoc Nguyen,8 Andrew G Iwach,7,9 Shan Lin7,8
1University of California, San Francisco School of Medicine, San Francisco, CA, USA; 2Center of Excellence in Glaucoma, Chulalongkorn University, Bangkok, Thailand; 3Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 4Department of Ophthalmology, King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand; 5University of California, Riverside, CA, USA; 6Southwest Medical Education Consortium, Temecula, CA, USA; 7Glaucoma Center of San Francisco, San Francisco, CA, USA; 8Glaucoma Research and Education Group, San Francisco, CA, USA; 9Department of Ophthalmology, University of California, San Francisco, CA, USA
Correspondence: Shan Lin, Glaucoma Center of San Francisco, 55 Stevenson Street, San Francisco, CA, 94105, USA, Tel +1 415 981 2020, Fax +1 415 981 2019, Email [email protected]
Purpose: To evaluate the pressure-lowering efficacy of cataract surgery combined with Hydrus microstent in mainly Asian eyes with combined-mechanism glaucoma (CMG) or primary angle closure glaucoma (PACG) versus open-angle glaucoma (OAG).
Patients and Methods: Patients with CMG, PACG, or OAG who were treated with 1 or more glaucoma medications prior to surgery were included in the study. Medical charts were reviewed for patients with CMG, PACG, or OAG undergoing cataract-Hydrus surgery. Multilevel mixed-effects linear regression models were performed to determine the efficacy of combined surgery on intraocular pressure (IOP) and number of glaucoma medications. Mixed-effects logistic regression models were used to assess post-operative 1-year success rate (IOP ≤ 18 mmHg without glaucoma medication) and percentage of medication-free patients.
Results: The post-operative IOP and medication use were compared in CMG/PACG (n = 49) and OAG (n = 29) eyes. At 1-year follow-up, IOP decreased in CMG/PACG (14.74 to 13.21 mmHg, p = 0.004) and was unchanged in OAG (14.48 to 14.84 mmHg, p = 0.56) (difference in absolute IOPs, p=0.02). IOP was significantly lower in CMG/PACG group compared to OAG group with a coefficient of − 2.1 (95% CI - 3.9 to − 0.4, p=0.02). The success rates were similar (82%, CMG/PACG; 79%, OAG, p=0.80). Both groups showed significant reductions in medications (CMG/PACG, 2.33 to 0.20, p< 0.001; OAG, 2.37 to 0.38, p< 0.001; between groups, p=0.20). 83% of patients achieved medication-free status (OAG, 83%; CMG/PACG, 84%, p=0.92). Regarding surgical complications, there was no significant difference between OAG and CMG/PACG groups for postoperative hyphema (p=0.64) and IOP spike (p=0.29).
Conclusion: In this retrospective study, the IOP-lowering efficacy of combined cataract-Hydrus surgery in CMG/PACG patients was similar or greater than in OAG patients.
Keywords: glaucoma, Hydrus microstent, cataract surgery, minimally invasive glaucoma surgery
Introduction
Glaucoma is one of the leading causes of blindness and vision loss.1 In most cases, decreased aqueous drainage from the anterior chamber through the trabecular meshwork causes elevated intraocular pressure (IOP) and subsequent damage to the optic nerve. Glaucoma is traditionally classified into open-angle and closed-angle forms. Open angle glaucoma (OAG) is the more prevalent form worldwide and primary open angle glaucoma (POAG) is the most common type, in which the anterior chamber angle is open and there is no secondary cause for elevated IOP or optic nerve damage. Normal tension glaucoma (NTG) is an open-angle glaucoma in which pre-treatment IOPs were not documented to be above the upper limit of the normal range (≤21 mmHg).2 Closed-angle forms of glaucoma include primary angle closure glaucoma (PACG) and combined mechanism glaucoma (CMG). POAG occurs due to increased resistance to aqueous flow across the outflow pathways even with an anatomically open angle.3 In closed-angle forms, the iris is pushed towards the trabecular meshwork and cornea—most commonly via a pupillary block mechanism—leading to restriction of aqueous flow through the trabecular meshwork.3 Cases of CMG have characteristics of both OAG and PACG, and is defined after treatment with laser peripheral iridotomy.4 Treatments for glaucoma include surgery, oral and ocular medications, and laser procedures. One group of glaucoma treatments that have been more recently developed in the last few decades are microinvasive glaucoma surgeries (MIGS), which offer a safer, albeit less effective, alternative to traditional glaucoma surgeries such as trabeculectomy.5
The Hydrus microstent, an 8-mm curved scaffold implanted into the Schlemm canal, is a MIGS device owned by Alcon Inc. (Fort Worth, TX). The proximal tip is open to the anterior chamber and serves as a conduit for direct aqueous flow into the Schlemm canal. The expansion of the canal and porous design allows for increased outflow into the collector channel ostia. The device’s composition from nitinol material allows flexibility while maintaining structural support. The Hydrus, in conjunction with cataract surgery, is effective in lowering IOP and glaucoma medication use in patients with open-angle glaucoma.6 However, few studies have been conducted in other population groups (eg Asian populations) and glaucoma types. Complications, similar to those of other MIGS procedures, have been documented and include transient hyphema, hypotony, microstent obstruction, and choroidal detachment.5
The Asian population, compared to other racial/ethnic populations, has a higher prevalence of PACG. Within the Asian groups, Chinese and Vietnamese Americans appear to have a higher prevalence of PACG compared to other Asian ethnic groups.7 In contrast to OAG, PACG can lead to a higher risk of blindness and vision loss if not treated aggressively.8
Other MIGS such as the iStent have been extensively studied in the last few decades due to their earlier availability, including with studies in other niche groups such as specific racial populations and glaucoma types besides OAG and ocular hypertension (OHTN). For example, there are a number of studies in subjects of Asian ancestry with PACG.9–11 In contrast, the Hydrus was approved relatively recently, and thus far, has a smaller number of post-approval studies (eg in other glaucoma types and in races other than Whites). In this study, we retrospectively examined the efficacy of the Hydrus microstent in reducing IOP and glaucoma medication use among Asians with PACG/CMG compared with OAG who have Hydrus microstent insertion in conjunction with cataract surgery.
Material and Methods
This retrospective comparative study of patients was conducted in the United States at the ophthalmology clinic of a single glaucoma specialist (N.N). The study was reviewed by an independent institutional review board (IRB) [Advarra, Columbia, MD], which is a committee that has reviewed this research study to help ensure that the rights and welfare of all research participants are protected and that the research study is carried out in an ethical manner. Informed consent was exempted by the IRB because the study was retrospective and subjects were not available to provide informed consent. The study subjects were a part of the existing clinic population prior to the study, and patient data confidentiality was maintained by following standard procedures for handling protected health information. Additionally, the IRB was approved for retrospective review of subjects receiving combined cataract surgery and the Hydrus implant. Although the Hydrus implant has not received FDA-approval for glaucomas other than POAG and OHTN, the treatment of CMG and PACG and secondary glaucomas usually include therapies (including other existing MIGS) which are only approved for POAG and OHTN. Similar to other MIGS which have been used in CMG and PACG cases,11 the device was only used in eyes in which the surgical area of the angle (nasal quadrant in our case) was open and visible for adequate insertion. Medical charts of patients who received cataract surgery with Hydrus implantation by a single surgeon (N.N.) between July 2020-January 2023 were reviewed. Subjects who met the following criteria were included in the initial screening process: (1) age greater than 40 years; (2) documentation of age-related cataract with best-corrected visual acuity (BCVA) of 20/40 or worse with or without glare test; (3) complete eye examination including gonioscopy; and (4) findings of glaucomatous optic neuropathy with or without corresponding visual field loss consistent with glaucoma. Glaucoma severity was classified based on Hodapp-Anderson-Parrish criteria.12 The patients were classified into open angle and closed angle groups, which were defined using criteria that we have reported in previous studies.11 Open angle was defined in eyes that had Shaffer angle grading of at least 2 for more than 180 degrees. OAG can be sub-classified as POAG and NTG, and both groups were included in our analysis as comprising OAG. PACG was defined in eyes that met the glaucoma criteria and had Shaffer angle grade 1 or less for 180 degrees or greater on gonioscopy. CMG was defined in those with initially closed angles, which was defined as Shaffer angle grading 1 or less for 180 degrees or more, and in which the angle subsequently deepened and met the open-angle definition after laser iridotomy.11 In these patients, the IOP remained elevated and/or the patient was assessed as having glaucoma at the time of laser or afterward, requiring glaucoma medications.11 Ultimately, eyes in which the angle opened after laser iridotomy and did not have peripheral anterior synechia (PAS) were classified as CMG, with both PACG and CMG eyes combined into a single group for data analysis. All patients underwent successful phacoemulsification with intraocular lens (IOL) implantation plus Hydrus implantation and completed 1-year follow-up after surgery.
The presence of PAS was not an exclusion for the CMG or the PACG groups; however, eyes that had significant PAS at the nasal angle were excluded from the study due to inability to adequately access the Schlemm canal. Exclusion criteria included the following: (1) any ocular or systemic condition (besides cataract) that could affect vision and/or visual field interpretation; (2) any ocular or systemic condition that could affect IOP or preclude accurate tonometry (eg corneal pathology, previous refractive surgery, concurrent use of systemic steroid); (3) previous intraocular surgery including filtering surgery, glaucoma drainage device implantation, and retina surgery; (4) history of ocular trauma; and (5) complicated cataract surgery such as posterior capsule rupture, vitreous loss, intraoperative zonular instability, and dropped nucleus. Prior laser trabeculoplasty and intraoperative floppy iris syndrome were not excluded.
Surgical Technique
Patients received standard phacoemulsification with the divide-and-conquer technique, through a temporal clear corneal incision. All patients underwent monitored anesthesia care (MAC) during the procedure and were given preservative-free 0.5% Xylocaine. An acrylic foldable IOL was successfully implanted in all cases. The Hydrus was implanted after IOL implantation. After the anterior chamber was filled with Viscoat, the viscoelastic, an anterior chamber paracentesis at the 1 o’clock position was made in the left eye and at the 7 o’clock position was made in the right eye. After tilting of the microscope and repositioning of the patient’s head, the Hill surgical gonioprism (Ocular Instrument Inc, Bellevue, WA, USA) was placed over the cornea to visualize the nasal angle. Once the TM was identified, the Hydrus inserter was directed through the paracentesis site and the Hydrus was implanted in the infero-nasal quadrant of the left eye or supero-nasal quadrant in the right eye, by sliding the leading edge through the TM into the Schlemm canal. The Lester hook was used to push on the trailing end of the Hydrus edge to ensure two-thirds of the distal end (between the last “window” and the trailing tip) of the Hydrus was covered by TM. The viscoelastic was not removed to act as a tamponade for bleeding from the angle. The wound was closed by irrigating the wound with balanced salt solution. A suture (10–0 nylon) was placed in the main wound depending on the presence of a floppy iris. All patients were given acetazolamide 500 mg sequels BID post-operation on the operative day.
Postoperative Follow up
All patients were prescribed a fluorometholone drop 4 times daily for 5 weeks and adjusted to a lower dose depending on the anterior chamber inflammation and the IOP in the early follow up period; a 0.3% nepafenac drop once a day for 5 weeks; and a fluoroquinolone antibiotic drop 4 times a day for 1 week and then 2 times a day for one week. Postoperative data was recorded at day 1, week 1 (7–10 days post-operation), week 5–6, month 3, month 6, and year 1 post-operation. Although participants may have had additional clinic visits outside these specified time points in our study, the other time points were variable among the subjects and may not be representative of the overall study population and therefore they were not included in the analysis. Anti-glaucoma medications were discontinued, restarted, or adjusted based on the IOP at each follow-up visit at the discretion of the surgeon (N.N).
Data Collection and Outcomes
Preoperative clinical information including BCVA, IOP measured by Goldmann applanation tonometry, pachymetry, gonioscopy, number of glaucoma medications, vertical cup-to-disc (C/D) ratio, and visual field mean deviation obtained from automated perimetry (24–2 Swedish interactive threshold algorithm [SITA] standard on Humphrey Field Analyzer-2; Carl Zeiss Meditec, Dublin, CA, USA), and optic nerve and retinal fiber layer analysis using optical coherence tomography (OCT) (Cirrus OCT, CarlZeiss Meditec, Dublin, CA, USA) were reviewed and recorded. The visual acuity, applanation IOP, and number of medications were recorded at week 1; at months 1, 3, 6; and at 1 year. Any laser or glaucoma surgery such as trabeculectomy, tube shunt or cyclo-destructive procedure were recorded. Any adverse events or complications such as postoperative hyphema, infections, or IOP spike (IOP>35 mm Hg) were recorded. The outcome measures were: (1) the success rate, which was defined as the proportion of subjects that had IOP ≤ 18 mm Hg without glaucoma medications; (2) the absolute postoperative IOP; and (3) the number of glaucoma medications, at one-year post-surgery.
Statistical Analysis
For continuous variables, the data were summarized using the mean and median as appropriate. Categorical variables were analyzed using the chi-square test or Fisher’s exact test. Paired t-tests or Wilcoxon tests were used to compare continuous variables between baseline and follow-up measurements within each group, while comparisons between the two groups were made using Student’s t-test.
To analyze the longitudinal data while accounting for the correlation of repeated measurements within the same subjects over time, repeated-measure models were utilized. For continuous outcomes, including IOP, number of medications, and visual acuity, multilevel mixed-effects linear regression models were employed. For binary outcomes, including the success rate and the percentage of medication-free patients, mixed-effects logistic regression models were used. The models were constructed to include interactions with time to assess changes in each outcome over the follow-up period. All analyses were conducted using STATA 16.0 (Stata Corp, College Station, TX), with a significance level set at p<0.05.
Results
A total of 78 eyes from 78 patients, who met the inclusion/exclusion criteria, were included in the study, comprising 29 patients with OAG (12 NTG and 17 POAG) and 49 patients with CMG/PACG (44 CMG and 5 PACG). Patients can be further classified as having mild (OAG, n=21; CMG/PACG, n=33), moderate (OAG, n=4; CMG/PACG, n=14), or advanced glaucoma (OAG, n=2; CMG/PACG n=1), with no difference in severity found between the groups (p=0.22). The majority of patients were Chinese or Vietnamese (96%). The demographic and baseline characteristics are described in Table 1. There was no significant difference in baseline characteristics. Maximum IOP, defined as the highest IOP recorded before surgery, was similar in both groups. However, three patients in the OAG group were on IOP lowering medical therapy when maximum IOP was recorded, whereas none of the patients in the CMG/PACG group were on medications at the time when maximum IOP was recorded. In terms of IOP outcome, the OAG group showed similar IOP between baseline and 12 months (from 14.48 ± 3.02 to 14.84 ± 2.91 mmHg, p=0.56 for change), whereas the CMG/PACG group experienced a significant decrease (from 14.74 ± 2.99 to 13.21 ± 3.13 mmHg, p=0.004 for change). Although the baseline IOPs in medicated eyes were similar (p=0.71), the difference in the absolute IOPs at 12 months was statistically significant (p=0.02), lower in the CMG/PACG group. Repeated measures analysis also showed significantly lower IOP in the CMG/PACG group compared to the OAG group with a coefficient of −2.1 (95% CI −3.9 to −0.4, p=0.02).
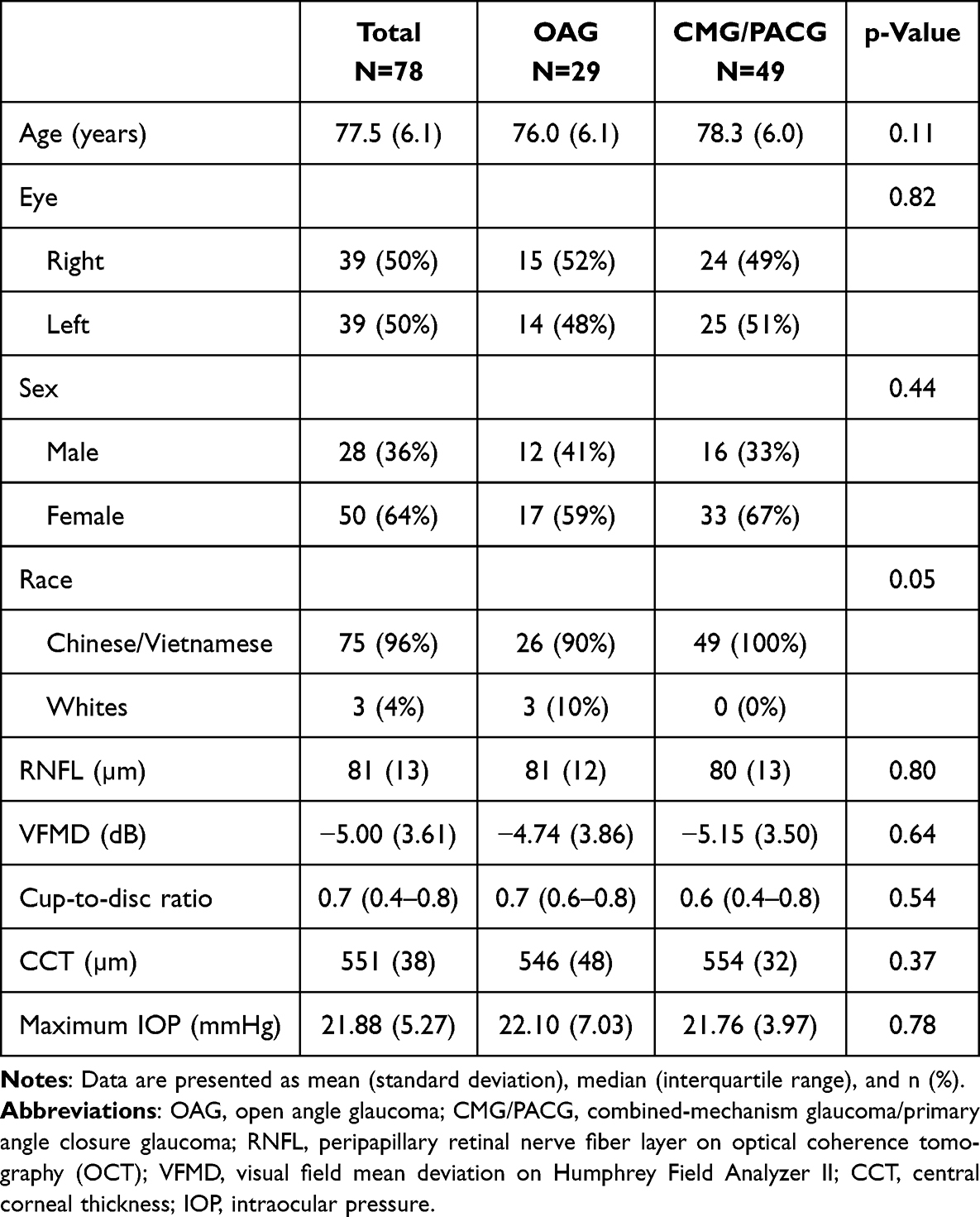 |
Table 1 Baseline Demographic and Clinical Characteristics |
Medication Use and Visual Acuity
There was a significant reduction in the number of medications from baseline to 12 months (OAG, baseline 2.37 (1.27) to 12-months 0.38 (0.98), p<0.001; CMG/PACG, baseline 2.33 (0.99) to 12-months 0.20 (0.54), p<0.001). Visual acuity without correction (measured in decimal unit) improved significantly in both groups, with a median improvement between 0.3 to 0.4 (OAG, p=0.001; CMG/PACG, p<0.001). The difference between the groups was not significant for both number of and change in medications as well as visual acuity (all p>0.05).
Success Rates
The OAG and CMG/PACG groups showed similar success rates following Hydrus microstent implantation. The overall success rate (IOP ≤ 18 mmHg on no medications) was similar between the two groups, with 79% of OAG patients and 82% of CMG/PACG patients achieving success at 12 months (p=0.80 for the difference). At the start of the study, all patients in the cohort used at least one medication. At 12 months, 83% of patients achieved medication-free status, with no significant difference between the two groups (OAG, 83%; CMG/PACG, 84%, p=0.92). However, the mixed-effect model showed that the OAG group tended to have a greater proportion of medication-free patients during the postoperative period than the CMG/PACG group, with coefficient of variation of –9.3 −17.6 to −0.9, p=0.03) (Figure 1). Additionally, of the eyes that did not meet the success criteria at 12 months, 1 of 6 eyes in the OAG group and no eyes in the CMG/PACG group increased in the number of medications. Some patients whose eyes did not meet the success criteria also underwent additional transscleral cyclophotocoagulation (TSCP) surgery (OAG, n=1) or had a change in medications (OAG, n=3; CMG/PACG, n=6), with no eyes requiring additional incisional surgery.
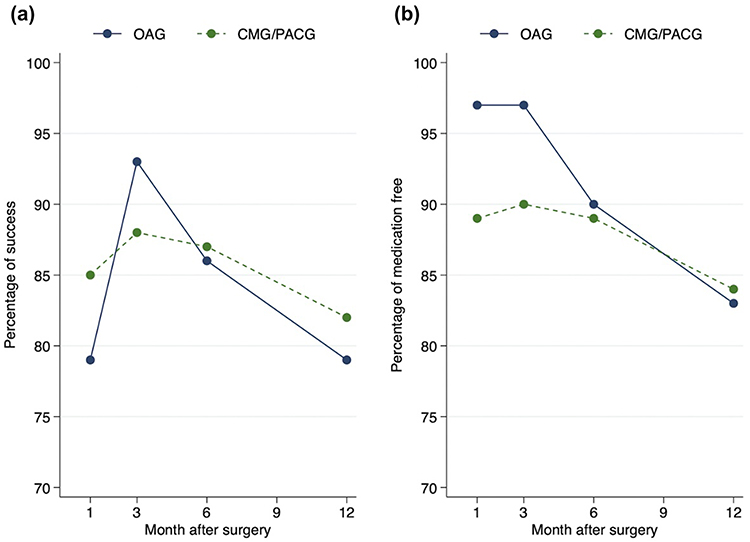 |
Figure 1 Success (a) and Medication-Free Rates (b) Over 12 Months Following Surgery; The open angle glaucoma (OAG) group is represented by solid lines; The combined mechanism glaucoma/primary angle closure glaucoma (CMG/PACG) group is represented by dashed lines. |
Table 2 compares the outcomes for the OAG and CMG/PACG groups. The success rate, percentage of medication-free patients, IOP, and number of medications over the 12-month follow-up period are shown in Figures 1 and 2. Regarding the complication rates, postoperative hyphema occurred in 4 patients (8.2%) in the CMG/PACG group and 1 patient (3.5%) in the OAG group (p=0.64). A postoperative IOP spike (IOP > 35 mmHg) was noted in 3 patients (6.1%) in the CMG/PACG group and in none of the patients in the OAG group, although there was no significant difference between the groups (p=0.29). Among these cases, patients experienced corneal edema and inflammation (n=1) and sensitivity to steroids (n=2) causing an IOP rise at 1-week follow up.
 |
Table 2 Comparison of Cataract Surgery Plus Hydrus Implant Outcomes |
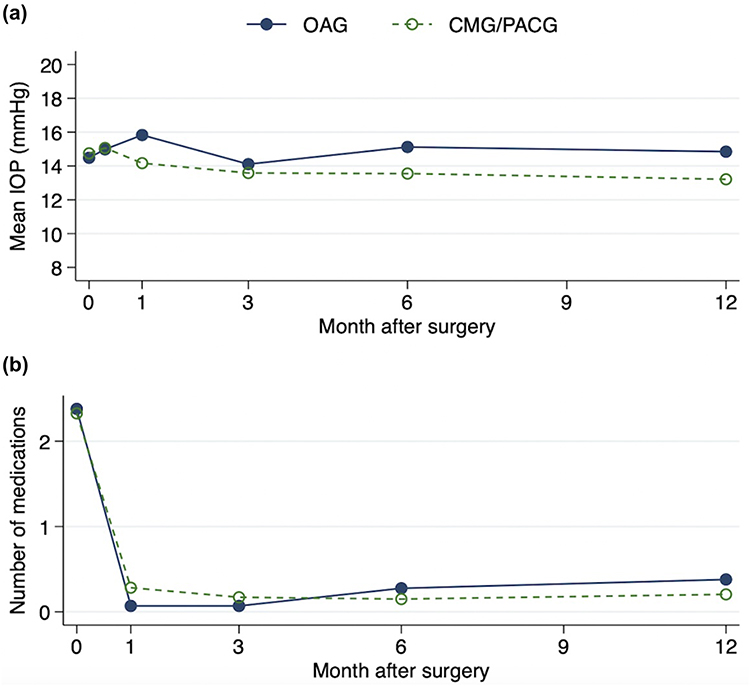 |
Figure 2 Mean Intraocular Pressure (a) and Number of Medications (b) Over 12 Months Following Surgery; The open angle glaucoma (OAG) group is represented by solid circles and lines; The combined mechanism glaucoma/primary angle closure glaucoma (CMG/PACG) group is represented by open circles and dashed lines. |
Discussion
In this retrospective study, we found that the postoperative IOP was lower in the CMG/PACG group compared to the OAG group. Although statistically significant, the absolute difference in postoperative IOP between groups is similar. However, the reduction in medication use was similar in both groups and the success rates were equivalent. Complication rates related to the Hydrus implant were low and not significantly different between the groups.
There may be various reasons to explain the effectiveness of combined cataract surgery with the Hydrus microstent in the CMG/PACG group. First, previous literature has consistently demonstrated that patients with angle closure and narrow angles tend to exhibit greater IOP reduction following cataract surgery.13,14 Similarly, prior studies have shown trends in greater IOP reduction in PACG compared to OAG eyes undergoing combined cataract surgery and other glaucoma surgery such as trabeculectomy.15,16 This phenomenon may explain the lower postoperative IOP in the CMG/PACG group in our study. However, our study did not include patients undergoing simple cataract surgery as control groups for both OAG and CMG/PACG. Additionally, the lower IOP reduction in the OAG group may be explained by the high proportion of NTG eyes (41.4%), which have demonstrated a more modest IOP-lowering effect due to lower preoperative IOPs.17 Likewise, another study demonstrated modest reductions in IOP after combined cataract-Hydrus treatment on mild to moderate OAG, NTG, and OHTN with lower baseline IOPs.18 Our findings indicate that POAG and CMG/PACG groups showed greater success rates one-year post operation with Hydrus implantation (79% and 82%, respectively) than those reported in a previous study using iStent implantation for POAG and CMG groups (33.3% and 43.7%, respectively).11 For comparison, in the iStent study the IOP reduction in CMG eyes was 14.69 (3.39) at baseline to 14.58 (2.46) at 12 months, suggesting that the addition of Hydrus confers additional IOP-lowering benefit.11 Additionally, the POAG and CMG groups showed similar efficacy with the iStent intervention when comparing success rate and number of medications.11 However, future research with cataract surgery alone as controls would provide valuable insights as to specific benefits and downsides of adjunctive Hydrus implantation. Second, the slightly higher percentage of medication-free patients observed in the OAG group could suggest that our OAG cohort was more likely to discontinue medications and/or at an earlier time point compared to the CMG/PACG group. It is likely that the treating clinician was more comfortable stepping off medications for OAG patients, possibly due to the proven efficacy of the Hydrus stent in OAG patients.19–21 Furthermore, the target IOPs may have been different among the subjects within each cohort, eg those with angle-closure glaucoma tend to have more aggressive disease requiring lower pressures7 and thus may require more medication use. Moreover, eyes with PACG experience intermittent or acute elevations in IOP compared to a more gradual progression in POAG,7 which can cause greater optic nerve damage and benefit from greater medication use.
In our study, the percentage of medication-free patients at 12 months was high compared to previously reported rates.19–21 This could be due to the less severe glaucoma in our cohort, as our study included patients predominantly in the mild to moderate stage, many of whom were on few medications prior to surgery. This predisposition is supported by previous studies which have suggested that trabecular MIGS, such as the iStent, might be less effective in eyes with more advanced glaucoma, possibly due to irreversible pathology in the collector channels in such eyes.22 Given the mostly mild stage of glaucoma in our study, the post-Schlemm canal pathway might be more viable, resulting in a favorable response in terms of IOP control and a higher percentage of medication-free patients. Moreover, another cohort who underwent combined canaloplasty-Hydrus demonstrated a similar proportion of medication-free patients at 6 months (87.5%) with minimal complications,23 thus supporting Hydrus as an effective addition to phacoemulsification for mild to moderate POAG.
This study has potential limitations. For example, the study relies on data from a single ophthalmology clinic and a single glaucoma-trained specialist, although this setting may also lessen the variability across varying sites and surgeons. Also, the small sample size increases the variability of the data and introduces potential bias to the results. Moreover, the retrospective nature of the study can lead to selection bias in this convenience sample which may not be representative of the general population. Additionally, the study has a sample predominantly composed of Asian patients due to the clinic’s Vietnamese/Chinese patient demographic. Consequently, the study outcomes cannot be generalized to ethnic groups outside of Asians, or even necessarily to those who are not of predominantly Vietnamese or Chinese origin. Lastly, the Hydrus implant currently has FDA approval only for POAG and OHTN. However, it was selected for CMG and PACG cases because of its safety profile and potential to reduce IOP and medication use. Although there can be ethical issues of using medications or surgeries for CMG and PACG that are not specifically approved for those indications, it is common in clinical practice since almost all glaucoma medications and surgeries have approval only for OAG and OHTN. In addition, the Hydrus was only performed in eyes which had open angles in the surgical area (nasal quadrant). Future studies should explore the efficacy of the Hydrus implant on other and more diverse patient populations, since there may be different mechanisms that can influence the efficacy of the MIGS device.
Conclusion
In summary, this study provides early evidence about the efficacy of the Hydrus implant in mainly Asian eyes with CMG/PACG (compared to OAG), when performed in conjunction with cataract surgery. Prior studies have demonstrated the effectiveness of the Hydrus implant in OAG, but studies have yet to show comparable data for other types of glaucoma.19,20 Given the high prevalence of PACG in Asian populations, our study provides early evidence to support this therapy for angle-closure eyes which are often at greater risk of blindness than open-angle subtypes of glaucoma.7 Our study suggests that the success rate among patients undergoing cataract surgery together with the Hydrus implant is comparable between OAG and CMG/PACG groups. It is interesting to note that there is no significant difference in the mean IOP between preoperative and postoperative for the OAG group. However, the significant reduction in glaucoma medication use in both groups indicates that there is potential for the Hydrus to improve the quality of life for patients with mild/moderate glaucoma. Future studies can help to assess the impact of the Hydrus implant on different glaucoma types or in patients with more severe glaucoma beyond 1-year follow up and when compared to cataract surgery alone.
Funding
Grant support received from Glaucoma Research Foundation, San Francisco, CA.
Disclosure
Shan C. Lin is a consultant for Santen, IRIDEX, Bausch & Lomb, and iSTAR and a speaker for Santen and Bausch & Lomb. Sunita Radhakrishnan is a consultant for Netra Systems Inc. Andrew G. Iwach is a consultant and advisor for Alcon Laboratories, Inc., public equity and stockholder for Eyenovia, public equity and stockholder for Eli Lilly & Company, and board member for Ophthalmic Mutual Insurance Company. The authors report no other conflicts of interest in this work.
References
1. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262–267.
2. Esporcatte BL, Tavares IM. Normal-tension glaucoma: an update. Arq Bras Oftalmol. 2016;79(4):270–276. doi:10.5935/0004-2749.20160077. PMID: 27626157.
3. Dietze J, Blair K, Havens SJ. Glaucoma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024. Available from https://www.ncbi.nlm.nih.gov/books/NBK538217/.
4. Peng PH, Manivanh R, Nguyen N, Weinreb RN, Lin SC. Glaucoma and clinical characteristics in Vietnamese Americans. Curr Eye Res. 2011;36(8):733–738. doi:10.3109/02713683.2011.584009
5. Ansari E. An update on implants for minimally invasive glaucoma surgery (MIGS). Ophthalmol Ther. 2017;6(2):233–241. doi:10.1007/s40123-017-0098-2
6. Ahmed IIK, Francesco TD, Rhee D, et al. Long-term outcomes from the horizon randomized trial for a schlemm’s canal microstent in combination cataract and glaucoma surgery. Ophthalmology. 2022;129(7):742–751. doi:10.1016/j.ophtha.2022.02.021
7. George R, Panda S, Vijaya L. Blindness in glaucoma: primary open-angle glaucoma versus primary angle-closure glaucoma—a meta-analysis. Eye. 2022;36(11):2099–2105. doi:10.1038/s41433-021-01802-9
8. Stein JD, Kim DS, Niziol LM, et al. Differences in Rates of Glaucoma Among Asian Americans Compared With Other Races and Among Individuals of Different Asian Ethnicities. Ophthalmology. 2011;118(6):1031–1037. doi:10.1016/j.ophtha.2010.10.024
9. Seider MI, Pekmezci M, Han Y, et al. High prevalence of narrow angles among Chinese-American glaucoma and glaucoma suspect patients. J Glaucoma. 2009;18(8):578–581. doi:10.1097/IJG.0b013e3181996f19
10. Nguyen N, Mora JS, Gaffney MM, et al. A high prevalence of occludable angles in a Vietnamese population. Ophthalmology. 1996;103(9):1426–1431. doi:10.1016/S0161-6420(96)30488-0
11. Chansangpetch S, Lau K, Perez CI, Nguyen N, Porco TC, Lin SC. Efficacy of cataract surgery with trabecular microbypass stent implantation in combined-mechanism angle closure glaucoma patients. Am J Ophthalmol. 2018;195:191–198. doi:10.1016/j.ajo.2018.08.003
12. Ng M, Sample PA, Pascual JP, et al. Comparison of visual field severity classification systems for glaucoma. J Glaucoma. 2012;21(8):551–561. doi:10.1097/IJG.0b013e31821dac66
13. Yoon JY, Hong YJ, Kim CY. Cataract surgery in patients with acute primary angle-closure glaucoma. Korean J Ophthalmol. 2003;17(2):122–126. doi:10.3341/kjo.2003.17.2.122
14. Brown RH, Zhong L, Whitman AL, Lynch MG, Kilgo PD, Hovis KL. Reduced intraocular pressure after cataract surgery in patients with narrow angles and chronic angle-closure glaucoma. J Cataract Refract Surg. 2014;40(10):1610–1614. doi:10.1016/j.jcrs.2014.01.038
15. Lai J, Tham C, Chan J, et al. Phacotrabeculectomy in Treatment of Primary Angle-closure Glaucoma and Primary Open-angle Glaucoma. Jpn J Ophthalmol. 2004;48(4):408–411. doi:10.1007/s10384-003-0075-2
16. Poon LYC, Lai C, Lee JJ, Tsai JC, Lin PW, Teng MC. Comparison of surgical outcomes after phacotrabeculectomy in primary angle-closure glaucoma versus primary open-angle glaucoma. Taiwan J Ophthalmol. 2015;5(1):28–32. doi:10.1016/j.tjo.2015.01.001
17. Ang BCH, Chen EJ, Chee WK, et al. Combined Phacoemulsification and Hydrus Microstent Implantation in Asian Eyes With Moderate-to- Severe Normal Tension Glaucoma-12-Month Outcomes. J Glaucoma. 2024;33(11):855–861. doi:10.1097/IJG.0000000000002475. Epub 2024 Aug 1. PMID: 39083013.
18. Holmes DP, Clement CI, Nguyen V, et al. Comparative study of 2‐year outcomes for Hydrus or iStent inject microinvasive glaucoma surgery implants with cataract surgery. Clin Exp Ophthalmol. 2022;50(3):303–311. doi:10.1111/ceo.14048
19. Ahmed IIK, Fea A, Au L, Ang RE, Harasymowycz P, Jampel HD, COMPARE Investigators. A prospective randomized trial comparing Hydrus and iStent microinvasive glaucoma surgery implants for standalone treatment of open-angle glaucoma: the COMPARE study. Ophthalmology. 2020;127(1):52–61. doi:10.1016/j.ophtha.2019.04.034
20. Fea AM, Ahmed IIK, Lavia C, et al. Hydrus microstent compared to selective laser trabeculoplasty in primary open angle glaucoma: one year results. Clin Exp Ophthalmol. 2017;45(2):120–127. doi:10.1111/ceo.12805
21. Samuelson TW, Chang DF, Marquis R, et al. A Schlemm canal microstent for intraocular pressure reduction in primary open-angle glaucoma and cataract: the HORIZON study. Ophthalmology. 2019;126(1):29–37. doi:10.1016/j.ophtha.2018.05.012
22. Chansangpetch S, Ittarat M, Yang S, et al. Comparison of 1-year effectiveness of trabecular microbypass stent implantation (istent) in conjunction with phacoemulsification among mild, moderate, and severe primary open-angle glaucoma patients. J Glaucoma. 2020;29(7):542–549. doi:10.1097/IJG.0000000000001542
23. Dickinson A, Leidy L, Nusair O, et al. Short-term outcomes of hydrus microstent with and without additional canaloplasty during cataract surgery. J Glaucoma. 2023;32(9):769–776. doi:10.1097/IJG.0000000000002245
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Efficacy of Combined Phacoemulsification and iStent Inject versus Combined Phacoemulsification and Hydrus Microstent
Chee WK, Yip VCH, Tecson IO, Chua CH, Ang BCH, Kee AR, Hu JY, Kan TCJ, Yip LWL
Clinical Ophthalmology 2023, 17:1151-1159
Published Date: 14 April 2023
Spotlight on Schlemm’s Canal MicroStent Injection in Patients with Glaucoma
Wagner IV, Ang B, Checo L, Simsek D, Draper C, Dorairaj S
Clinical Ophthalmology 2023, 17:1557-1564
Published Date: 2 June 2023
Long-Term Efficacy of Successful Excisional Goniotomy with the Kahook Dual Blade
Wagner IV, Boopathiraj N, Lentz C, Dorairaj EA, Draper C, Kumar D, Checo L, Miller DD, Krambeer C, Dorairaj S
Clinical Ophthalmology 2024, 18:713-721
Published Date: 7 March 2024
Outcomes and Complications of Minimally Invasive Glaucoma Surgeries (MIGS) in Primary Angle Closure and Primary Angle Closure Glaucoma: A Systematic Review and Meta-Analysis
Paik B, Chua CH, Yip LW, Yip VC
Clinical Ophthalmology 2025, 19:483-506
Published Date: 11 February 2025
Early Real-World Safety and Short-Term Outcomes of Combined iStent Infinite and Intracameral Travoprost Implant (iDose TR) with or without Cataract Surgery
Yadgarov A
Clinical Ophthalmology 2026, 20:597257
Published Date: 20 May 2026