Back to Journals » Clinical Ophthalmology » Volume 18
Long-Term Efficacy of Successful Excisional Goniotomy with the Kahook Dual Blade
Authors Wagner IV ![]() , Boopathiraj N
, Boopathiraj N ![]() , Lentz C, Dorairaj EA
, Lentz C, Dorairaj EA ![]() , Draper C, Kumar D, Checo L
, Draper C, Kumar D, Checo L ![]() , Miller DD
, Miller DD ![]() , Krambeer C, Dorairaj S
, Krambeer C, Dorairaj S
Received 21 November 2023
Accepted for publication 26 February 2024
Published 7 March 2024 Volume 2024:18 Pages 713—721
DOI https://doi.org/10.2147/OPTH.S451002
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Isabella V Wagner,1 Nithya Boopathiraj,1 Connor Lentz,1 Emily Aashna Dorairaj,2 Christian Draper,3 Devesh Kumar,4 Leticia Checo,1 Darby D Miller,1 Chelsey Krambeer,1 Syril Dorairaj1
1Department of Ophthalmology, Mayo Clinic, Jacksonville, FL, USA; 2Department of Medicine, Charles E. Schmidt College of Medicine, Florida Atlantic University, Boca Raton, FL, USA; 3Department of Ophthalmology, Eye Consultants, Spokane, WA, USA; 4Department of Ophthalmology, Medical College of Wisconsin, Milwaukee, WI, USA
Correspondence: Syril Dorairaj, Department of Ophthalmology, Mayo Clinic, 4500 San Pablo Road, Jacksonville, FL, USA, Tel +1 904-953-2377, Fax +1 904-953-7040, Email [email protected]
Purpose: To report clinical outcomes of successful excisional goniotomy with the Kahook Dual Blade (KDB), through 60 months.
Patients and methods: This was a noncomparative, single-surgeon, retrospective review of eyes receiving successful KDB goniotomy with or without concomitant phacoemulsification between October 2015 and January 2016 with five years of uninterrupted follow-up. Intraocular pressure (IOP), number of glaucoma medications, best corrected visual acuity (BCVA), and complications were recorded. Primary outcomes included changes from baseline in IOP, medication use, and BCVA, through five years.
Results: Fifty-two eyes of 28 patients were analyzed. Most eyes had mild primary open angle glaucoma (73%). Of the eyes analyzed, 41 underwent combined surgery and 11 underwent standalone surgery. With all eyes combined, mean (standard deviation) baseline IOP was 21.0 (4.1) mmHg and mean baseline medication use was 1.8 (1.1) medications per eye. Across time points at months 6, 12, 24, 36, 48, and 60, mean postoperative IOP ranged from 13.0 to 13.7 mmHg, representing mean reductions of 7.3– 8.0 mmHg (34.7– 38.3%; p < 0.0001 at every time point). Similarly, mean medication use ranged from 0.4 to 0.6 medications per eye, representing mean reductions of 1.2– 1.4 medications (66– 75.5%; p < 0.0001 at every time point). Mean logMAR BCVA improved from 0.321 (0.177) preoperatively to 0.015 (0.035) at month 60 (p < 0.0001).
Conclusion: In eyes not requiring secondary surgical procedures (eg, long-term surgical successes), excisional goniotomy provided clinically and statistically significant reductions in both IOP and the need for medications that were highly consistent through five years of follow-up. KDB goniotomy appears to be highly successful in Caucasian patients with open angle glaucoma on ≥ 1 IOP-lowering medications at baseline and with no history of prior ocular surgery. Successful excisional goniotomy with the KDB can be expected to improve long-term glaucoma-related visual outcomes through IOP reduction and to improve quality of life through medication reduction.
Keywords: glaucoma, goniotomy, intraocular pressure, IOP-lowering medications, phacoemulsification, minimally invasive glaucoma surgery
Introduction
As the world’s leading cause of blindness, the diagnosis and preemptive treatment of glaucoma is critical to prevent the irreversible blindness associated with disease progression.1 Typically, glaucoma is treated first by medicinal therapy and later with lasers and/or surgical interventions to promote further intraocular pressure (IOP) reduction.2 Trabeculectomy was the “gold standard” surgical procedure for many decades but is limited by significant complications such as blebitis, corneal erosion, conjunctival hemorrhage, and high reoperation rates, indicating the need for less invasive procedures performed at earlier disease stages.3–5 Minimally invasive glaucoma surgeries (MIGSs) are conjunctival sparing procedures which have minimized and/or delayed the need for traditional incisional surgeries under a favorable safety profile, albeit with a slight compromise in IOP-reducing efficacy.6 MIGS devices which target the trabecular outflow pathway, such as the Kahook Dual Blade (KDB; New World Medical), function through bypassing the majority of trabecular outflow and directing aqueous egress to the Schlemm’s canal.7
The KDB is an ab-interno trabeculotomy MIGS device that excises diseased trabecular meshwork over multiple clock hours to restore aqueous outflow to the Schlemm’s canal and its distal collector channels.8 Unlike other goniotomy-based MIGS devices, the KDB procedure involves the subsequent removal of the excised material, thus reducing the risk of scarring and probability of reoperation.7,9 KDB excisional goniotomy is indicated for use with or without phacoemulsification and across the spectrum of disease severity in patients with open angle glaucoma (OAG)7,8,10–15 but successful outcomes have been reported in patients with angle closure glaucoma,16–19 congenital glaucoma,20 and uveitis-associated ocular hypertension.21 The follow-up period of most reports on KDB ranges from 6- to 24-months, with only two studies reporting 36-month outcomes.14,15 Currently, there is an unmet need for KDB studies with long-term follow-up.
Within this report, we evaluate five-year efficacy outcomes and success parameters of patients receiving successful KDB excisional goniotomy with or without concurrent phacoemulsification.
Methods
A retrospective, single surgeon (SD), noncomparative interventional study was conducted. The study protocol was reviewed and approved by the Mayo Clinic Institutional Review Board (IRB) in 2018 (certificate approval number: 02/28/2018). This study was conducted in accordance with the tenets of the Declaration of Helsinki.
The inclusion criteria consisted of adults aged 18 years or older diagnosed with glaucoma that underwent successful excisional KDB goniotomy, with or without concomitant phacoemulsification, between January 1, 2015, and January 31, 2016. Successful KDB goniotomy was defined as eyes which achieved an IOP ≤21 mmHg and/or ≥20% reduction from baseline and did not require secondary surgical reinterventions, through five years. Eyes were not excluded on the basis of race, surgical history, type and severity of glaucoma, or baseline IOP, medications, and best corrected visual acuity (BCVA). All consecutive eligible patients who met the criteria of successful KDB goniotomy were enrolled.
KDB excisional goniotomy was performed according to the manufacturer’s instructions for use.22 The sharp tip of the device was advanced through a clear corneal incision to the nasal angle. The device tip was used to pierce the trabecular meshwork, and the heel was seated against the Schlemm’s canal. The KDB device was then advanced for four clock hours in a clockwise or counterclockwise direction, creating two parallel incisions to excise a strip of trabecular meshwork, without damaging adjacent structures. Finally, the KDB blade was removed from the eye. A persistent opening on the goniotomy site and goniotomy opening with a wide angle can be visualized in Figures 1 and 2, respectively. In cases with combined phacoemulsification, the KDB procedure was performed following successful intraocular lens implantation.
 |
Figure 1 Gonioscopic view of a persistent opening (indicated by red arrows) on the goniotomy site (yellow outline). |
 |
Figure 2 Ultrasound biomicroscopy image of a goniotomy opening (yellow outline) with a widened iridocorneal angle (indicated by red arrow). |
Participants were evaluated preoperatively, intraoperatively, and at 6, 12, 24, and 36, 48, and 60 months postoperatively. Pre- and postoperative data included IOP (assessed with Goldmann applanation tonometry), number of glaucoma medications used, and BCVA (assessed using a Snellen eye chart at 20 feet). Slit lamp and fundus examinations were used to visualize and evaluate the anterior and posterior segments of each eye. Glaucoma severity was classified based upon the International Classification of Diseases 10 definition.23
Standard descriptive statistics were used to report demographics and baseline characteristics, with means and standard deviations used for continuous variables, and percentages used for categorical variables. Data analysis was conducted using the SPSS program 22.0 (SPSS Inc., Chicago, IL). The primary outcome measures of the study were changes from baseline in IOP, glaucoma medication burdens, and BCVA at each postoperative time point, assessed using 2-tailed paired t-tests with P <0.007 as the level of significance (adjusted using the Bonferroni correction). Primary outcomes were reported as means (standard deviations) and were calculated from the total number eyes at each follow-up visit. Sample size remained consistent through the study duration as all patients were present at each follow-up.
Results
Fifty-two eyes of 28 patients underwent KDB excisional goniotomy and were followed for up to 60 months. Demographic and preoperative glaucoma status data can be found in Table 1. The mean (SD) age of all patients was 67.8 (9.3) years, and most were Caucasian (75%) and female (61%). All eyes were surgically naïve and had various forms of OAG, ranging from a mild to severe severity. The study’s retention rate was 100%.
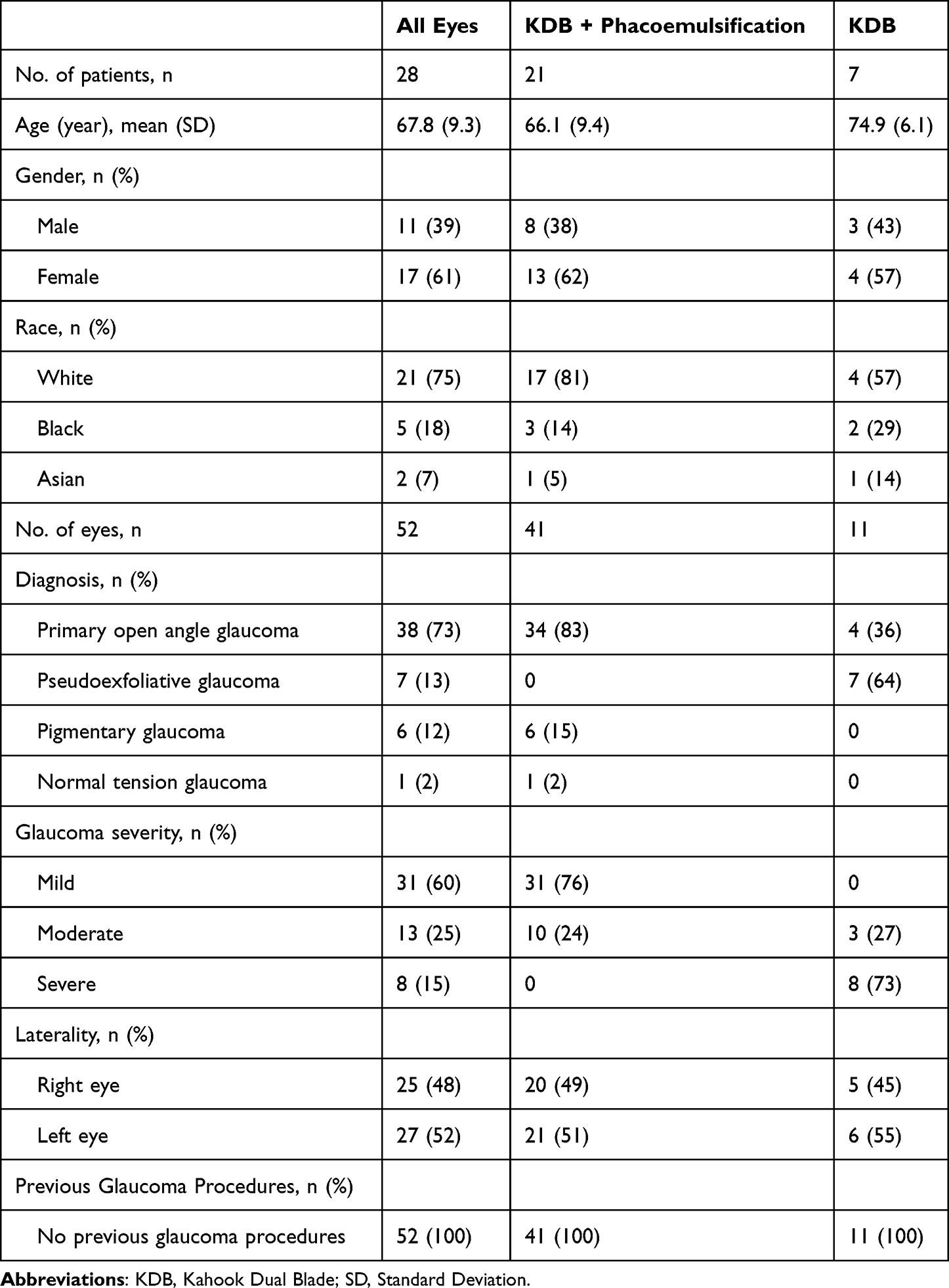 |
Table 1 Demographic and Preoperative Glaucoma Status of Study Participants |
Mean IOP at baseline and each postoperative visit for all eyes can be found in Table 2. The mean (SD) baseline IOP was 21.0 (4.1) mmHg and through up to 60 months of follow-up ranged consistently from 13.0 (2.1) to 13.7 (2.1) mmHg (P <0.0001 for every time point compared to baseline) with mean percent IOP reductions from 34.7% to 38.3% (Figure 3). At 60 months, all eyes achieved an IOP ≤21 mmHg, and 81% achieved an IOP reduction of ≥20% from baseline.
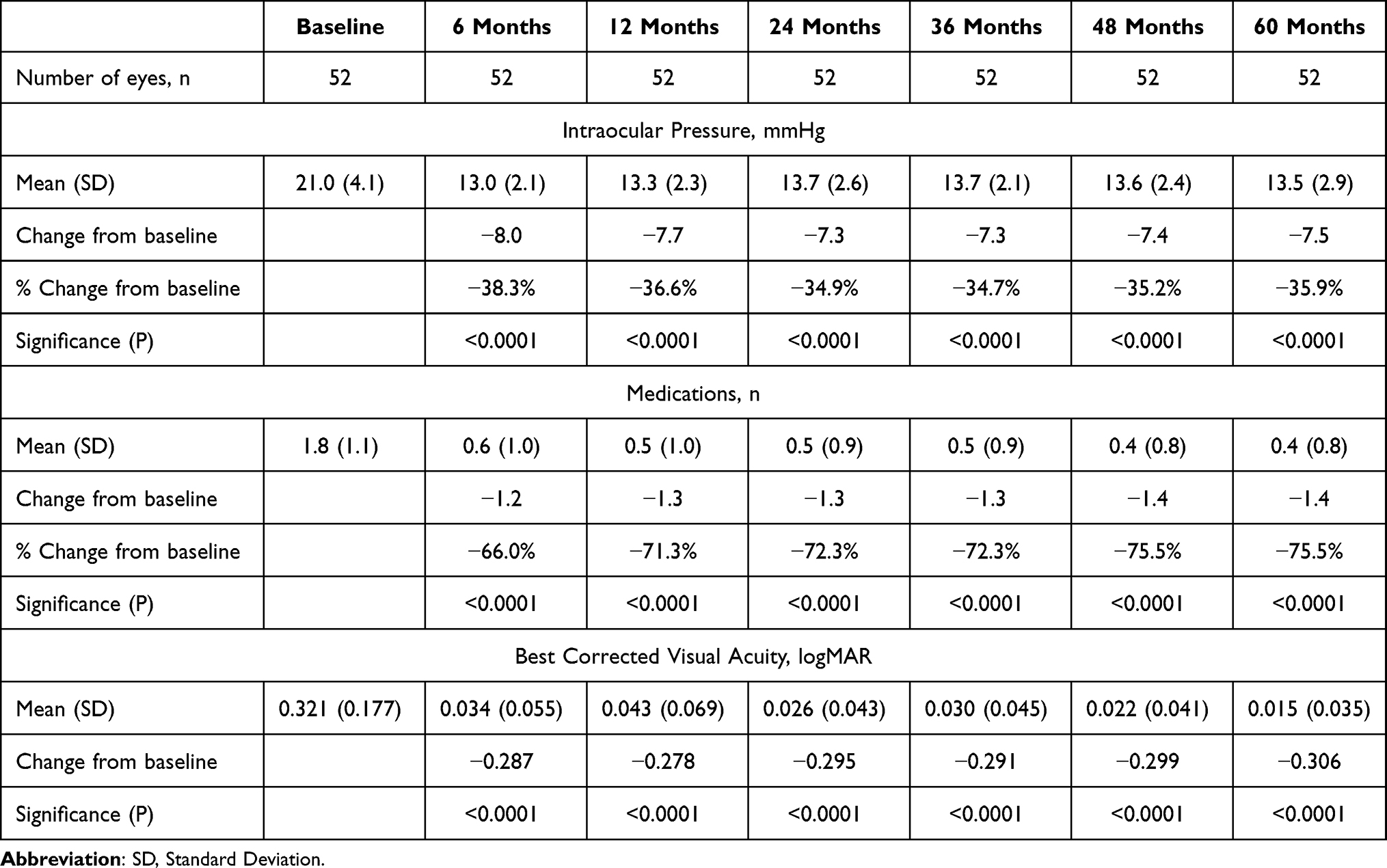 |
Table 2 Mean Intraocular Pressure, Medication Use, and Best Corrected Visual Acuity at Each Study Visit in All Eyes |
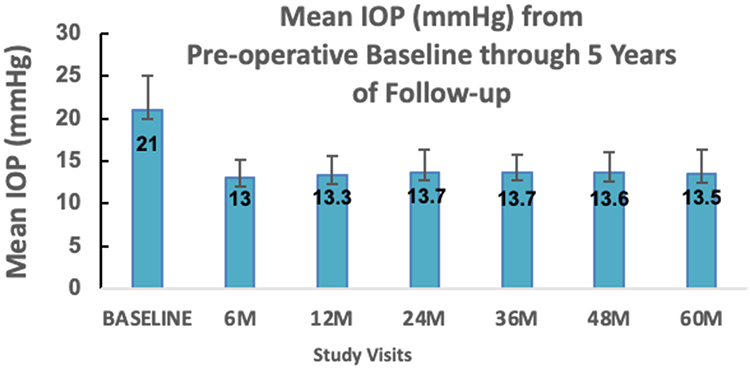 |
Figure 3 Mean IOP over time in the study cohort. Error bars represent standard deviation. Reductions from baseline were significant (p < 0.0001) at every time point. |
Mean glaucoma medication use and BCVA at baseline at each postoperative visit for all eyes can also be found in Table 2. The mean (SD) number of medications was 1.8 (1.1) and through up to 60 months of follow-up ranged from 0.4 (0.8) to 0.6 (1.0) medications (P <0.0001 for every time point against baseline) with a trend for decreased medication use over time (Figure 4). Mean medication reductions across all follow-up visits ranged from 66% to 75.5%. At 60 months, 98% of all eyes were using ≥1 fewer glaucoma medications than at baseline, with 67.3% being medication-free. No eyes experienced an increase in medication dependence. Mean logMAR BCVA improved from 0.321 (0.177) at baseline to 0.015 (0.035) at month 60 (P < 0.0001). At last follow-up (60 months), all eyes had a visual acuity of 20/20 (n = 44; 84.6%) or 20/25 (n = 8; 15.4%).
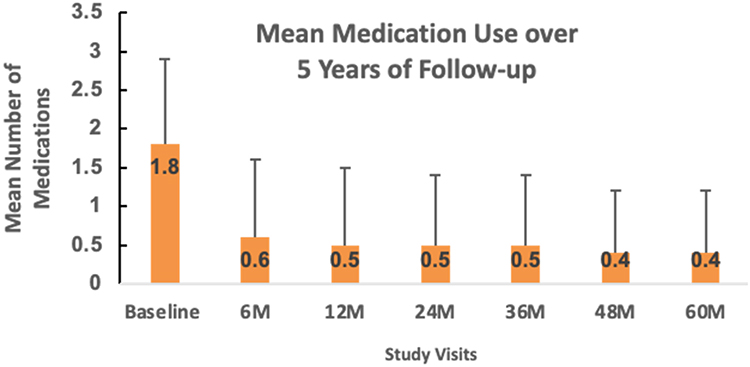 |
Figure 4 Mean medication use over time in the study cohort. Error bars represent standard deviation. Reductions from baseline were significant (p < 0.0001) at every time point. |
Separate analyses for eyes receiving KDB goniotomy with phacoemulsification and standalone KDB can be found in Tables 3 and 4, respectively. In the combined group, the mean (SD) baseline IOP was 20.5 (3.5) mmHg and ranged from 13.3 (2.9) to 13.8 (2.8) mmHg over 60 months of follow-up, representing mean percent reductions from 32.9% to 35.3%. Mean number of medications was 1.3 (0.7) at baseline and ranged consistently from 0.1 (0.4) to 0.2 (0.5) medications at each follow-up visit, characterizing mean percent reductions by 83.6–89.1%. Mean logMAR BCVA was 0.400 (0.096) at baseline and ranged from 0.010 (0.026) to 0.030 (0.061) over 60 months. Changes from baseline in IOP, medication use, and BCVA within the combined group were significant at every time point (P < 0.0001). Within the standalone cohort, the mean (SD) baseline IOP was 22.8 (5.8) mmHg and ranged from 11.4 (2.6) to 14.5 (1.4) mmHg over 60 months of follow-up, representing mean percent reductions by 36.7–50.2%. The mean number of medications was 3.5 (0.5) and ranged from 1.5 (0.9) to 2.2 (1.0) medications, characterizing mean percent reductions from 38.5% to 56.4%. Mean logMAR BCVA was 0.030 (0.045) at baseline and ranged from 0.040 (0.051) to 0.080 (0.087) over 60 months. Changes from baseline in IOP and medication use within the standalone group were significant for every time point (P < 0.0001), but changes in BCVA did not reach statistical significance.
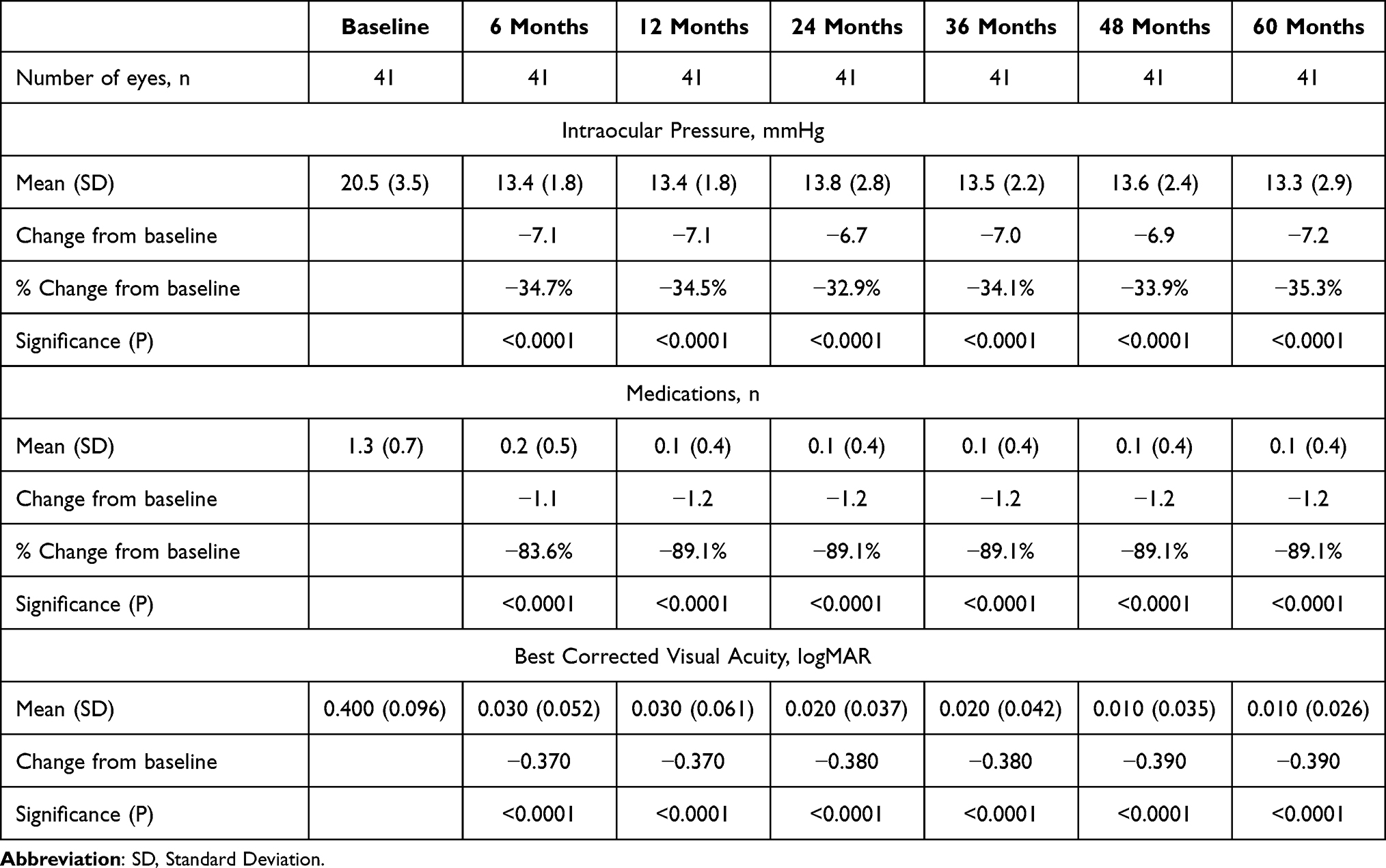 |
Table 3 Mean Intraocular Pressure, Medication Use, and Best Corrected Visual Acuity at Each Study Visit in Eyes Receiving Kahook Dual Blade Goniotomy Combined with Phacoemulsification |
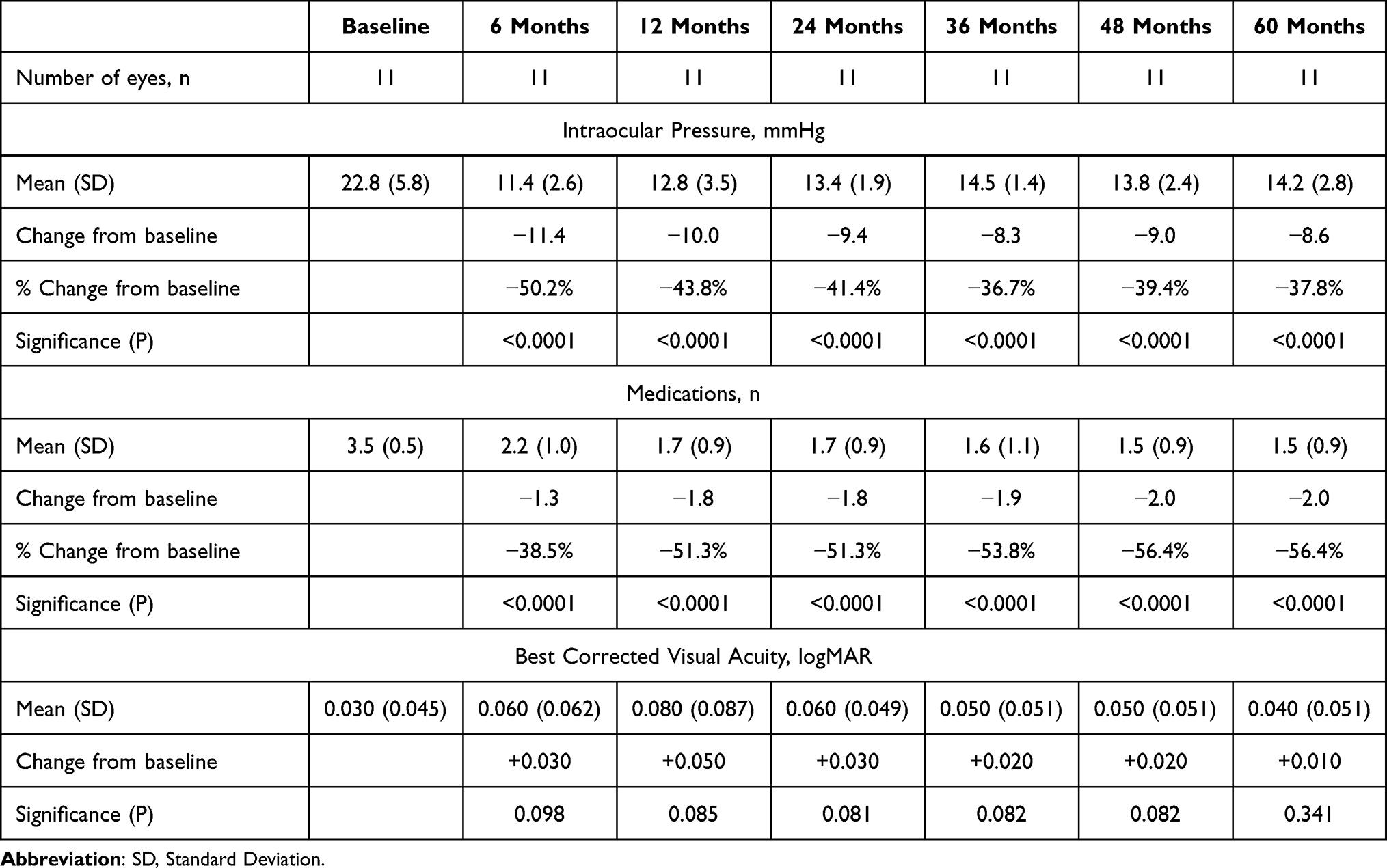 |
Table 4 Mean Intraocular Pressure, Medication Use, and Best Corrected Visual Acuity at Each Study Visit in Eye Receiving Standalone Kahook Dual Blade Goniotomy |
Common complications observed include intraoperative heme reflux (n = 10; 19.2%) which resolved within week 1 of follow-up, and IOP spikes within the first postoperative month which did not persist beyond 6 months. No serious adverse device-related events were observed in any eye, through 60 months. Additionally, no patient complaints or visual field changes were observed.
Discussion
In this analysis of our five-year experience with successful KDB goniotomy, clinically and statistically significant reductions in both IOP and the use of IOP-lowering medications were observed in all eyes through up to 60 months of follow-up. The procedure’s safety profile was excellent, with minimal intraoperative and early post-operative complications observed.
It is unclear as to what led to the long-term success of this study cohort. All eyes within this study cohort were surgically naïve, with no previous glaucoma surgeries or laser therapies performed. This could have possibly led to a higher probability of surgical success than seen in previously operated eyes, but there is inconclusive evidence within the literature to support this assertion. For instance, one study compared outcomes of Trabectome surgery (NeoMedix) in surgically naïve eyes to previously operated eyes and observed a higher surgical success rate (defined as IOP ≤21 mmHg with ≥20% reduction from baseline and no glaucoma surgical reinterventions) in surgically naïve eyes (78% vs 65%; P < 0.01) at 36 months, but its findings are limited by the inclusion of prior vitreoretinal surgery, vitrectomy, and corneal transplantation in the surgery-naïve group.24 Another study concluded that prior failed tube shunt implantation did not decrease the IOP-reducing efficacy of trabectome surgery but was ineffective at reducing glaucoma medication burdens in these patients.25
Other studies have analyzed success predictors of KDB goniotomy. Sieck et al analyzed 12-month outcomes of KDB goniotomy with or without phacoemulsification and found no significant association between surgical success (defined as ≥20% IOP reduction and/or ≥1 medication reduction) and age, sex, baseline IOP, or baseline number of medications.26 Similarly, Pratte et al evaluated surgical success of combined phacoemulsification and KDB goniotomy (defined as ≥20% IOP reduction or ≥1 medication reduction with an IOP <18 mmHg at each follow-up visit) and found that prior laser trabeculoplasty, ethnicity, age, glaucoma type or severity, and preoperative IOP were not significant predictors of surgical success in a cohort of 132 eyes.27 However, these authors concluded that a higher number of IOP-lowering medications at baseline correlated with a greater probability of surgical success, with a higher percentage of patients on >1 medication meeting success criteria compared to those on 0–1 medications (68.3% vs 56.5%; P = 0.037) at 6 months.27 This may account for the success seen within our study cohort, as all patients were on ≥1 IOP-lowering medications at baseline. Conversely, Ibrahim et al also evaluated 6-month surgical success outcomes (defined as ≥20% IOP reduction and/or ≥1 medication reduction if postoperative IOP was +2 mmHg from baseline) of combined phacoemulsification and KDB goniotomy and did not find the baseline number of glaucoma medications to be a significant success predictor (OR, 1.73; P = 0.166); however, the authors established that a higher baseline IOP was associated with greater surgical success (OR, 2.01; P = 0.016);.10 When stratifying our study cohort by baseline IOP, pressures ranged from 14 to 21 mmHg in 63.5% of eyes (Group 1) and 22–34 mmHg in 36.5% of eyes (Group 2). At 60 months, IOP decreased to 13.5 mmHg in both groups, therefore it is unlikely that baseline IOP was a significant success predictor within our study.
This study’s results fulfill an unmet need for clinical outcome data of KDB goniotomy with a long-term follow-up. Advantages of our study include its complete follow-up and enrollment of all eligible eyes. The main limitation of our study is its retrospective nature. Additionally, the results from this study do not represent real-world outcomes, as it exclusively evaluates long-term surgical successes.
Conclusions
Excisional goniotomy using the KDB, with or without concomitant phacoemulsification, appears to be a safe and efficacious treatment modality in surgically naïve eyes with OAG on ≥1 IOP-lowering medications at baseline, through five years. When evaluating device outcomes in long-term surgical successes, KDB goniotomy was demonstrated to improve long-term visual outcomes by significantly reducing both IOP and medication burdens. Patients with self-limited bleeding and no complications had successful outcomes.
Data Sharing Statement
The author’s institution (Mayo Clinic Florida) does not authorize data sharing. Queries and requests should be handled by the corresponding author (SD).
Consent for Publication
This retrospective study was performed in accordance with the tenets of the Declaration of Helsinki. Patient consent was waived by the Mayo Clinic IRB. All data and images have been deidentified.
Acknowledgments
The authors acknowledge Ms. Joyce Baker for her generous contribution to the Mayo Clinic Ophthalmology Department. Without her, the publication of this article would not have been possible.
Author Contributions
All listed authors made a significant contribution to this work in multiple areas including conception, study design, execution, data acquisition, analysis, interpretation, drafting, and/or critical review. All authors gave final approval of the version to be published, agreed on the journal of submission, and agreed to be accountable for all aspects of the work.
Funding
No grant support was obtained.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Soh Z, Yu M, Betzler BK, et al. The global extent of undetected glaucoma in adults: a systematic review and meta-analysis. Ophthalmology. 2021;128(10):1393–1404. PMID: 33865875. doi:10.1016/j.ophtha.2021.04.009
2. Wagner IV, Stewart MW, Dorairaj SK. Updates on the diagnosis and management of glaucoma. Mayo Clin Proc Innov Qual Outcomes. 2022;6(6):618–635. PMID: 36405987; PMCID: PMC9673042. doi:10.1016/j.mayocpiqo.2022.09.007
3. Pantalon A, Feraru C, Tarcoveanu F, Chiselita D. Success of primary trabeculectomy in advanced open angle glaucoma. Clin Ophthalmol. 2021;15:2219–2229. PMID: 34079219; PMCID: PMC816681. doi:10.2147/OPTH.S308228
4. Jampel HD, Solus JF, Tracey PA, et al. Outcomes and bleb-related complications of trabeculectomy. Ophthalmology. 2012;119(4):712–722. PMID: 22244944. doi:10.1016/j.ophtha.2011.09.049
5. Craven ER, Singh IP, Yu TM, Rhoten S, Sadruddin OR, Sheybani A. Reoperation rates and disease costs for primary open-angle glaucoma patients in the United States treated with incisional glaucoma surgery. Ophthalmol Glaucoma. 2022;5(3):297–305. PMID: 34715397. doi:10.1016/j.ogla.2021.10.011
6. Gurnani B, Tripathy K. Minimally Invasive Glaucoma Surgery. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023. PMID: 35881761.
7. Barkander A, Economou MA, Jóhannesson G. Kahook dual-blade goniotomy with and without phacoemulsification in medically uncontrolled glaucoma. Clin Ophthalmol. 2023;17:1385–1394. PMID: 37204995; PMCID: PMC10187655. doi:10.2147/OPTH.S409375
8. Laroche D, Nkrumah G, Ugoh P, Ng C. Real world outcomes of kahook dual blade goniotomy in black and afro-latinx adult patients with glaucoma: a 6-month retrospective study. J Natl Med Assoc. 2021;113(2):230–236. PMID: 33158570. doi:10.1016/j.jnma.2020.09.147
9. Seibold LK, Soohoo JR, Ammar DA, Kahook MY. Preclinical investigation of ab interno trabeculectomy using a novel dual-blade device. Am J Ophthalmol. 2013;155(3):524–529.e2. PMID: 23218696. doi:10.1016/j.ajo.2012.09.023
10. Ibrahim LF, Pereira AFR, Terenzi LAO, et al. Phacoemulsification with kahook dual blade goniotomy in eyes with medically treated glaucoma: analysis of surgical outcomes and success predictors. Arq Bras Oftalmol. 2021;85(4):359–363. PMID: 34586247. doi:10.5935/0004-2749.20220046
11. Hirabayashi MT, King JT, Lee D, An JA. Outcome of phacoemulsification combined with excisional goniotomy using the kahook dual blade in severe glaucoma patients at 6 months. Clin Ophthalmol. 2019;13:715–721. PMID: 31114149; PMCID: PMC648816. doi:10.2147/OPTH.S196105
12. Wakil SM, Birnbaum F, Vu DM, McBurney-Lin S, ElMallah MK, Tseng H. Efficacy and safety of a single-use dual blade goniotomy: 18-month results. J Cataract Refract Surg. 2020;46(10):1408–1415. PMID: 32483073. doi:10.1097/j.jcrs.0000000000000263
13. Dorairaj SK, Seibold LK, Radcliffe NM, et al. 12-month outcomes of goniotomy performed using the kahook dual blade combined with cataract surgery in eyes with medically treated glaucoma. Adv Ther. 2018;35(9):1460–1469. PMID: 30078175; PMCID: PMC6133141. doi:10.1007/s12325-018-0755-4
14. Iwasaki K, Kakimoto H, Orii Y, Arimura S, Takamura Y, Inatani M. Long-term outcomes of a kahook dual blade procedure combined with phacoemulsification in Japanese patients with open-angle glaucoma. J Clin Med. 2022;11(5):1354. PMID: 35268445; PMCID: PMC8910915. doi:10.3390/jcm11051354
15. Albuainain A, Al Habash A. Three-year clinical outcomes of phacoemulsification combined with excisional goniotomy using the kahook dual blade for cataract and open-angle glaucoma in Saudi Arabia. Saudi J Ophthalmol. 2022;36(2):213–217. PMID: 36211318; PMCID: PMC9535918. doi:10.4103/sjopt.sjopt_182_21
16. Dorairaj S, Tam MD, Balasubramani GK. Twelve-month outcomes of excisional goniotomy using the Kahook Dual Blade® in eyes with angle-closure glaucoma. Clin Ophthalmol. 2019;13:1779–1785. PMID: 31571816; PMCID: PMC6750200. doi:10.2147/OPTH.S221299
17. Dorairaj S, Tam MD. Kahook dual blade excisional goniotomy and goniosynechialysis combined with phacoemulsification for angle-closure glaucoma: 6-month results. J Glaucoma. 2019;28(7):643–646. PMID: 30950968. doi:10.1097/IJG.0000000000001256
18. Dorairaj S, Tam MD, Balasubramani GK. Two-year clinical outcomes of combined phacoemulsification, goniosynechialysis, and excisional goniotomy for angle-closure glaucoma. Asia Pac J Ophthalmol (Phila). 2020;10(2):183–187. PMID: 33031110. doi:10.1097/APO.0000000000000321
19. Al Habash A, Albuainain A. Long term outcome of combined phacoemulsification and excisional goniotomy with the Kahook Dual Blade in different subtypes of glaucoma. Sci Rep. 2021;11(1):10660. PMID: 34021228; PMCID: PMC8140085. doi:10.1038/s41598-021-90223-5
20. Harvey MM, Schmitz JW. Use of ab interno Kahook Dual Blade trabeculectomy for treatment of primary congenital glaucoma. Eur J Ophthalmol. 2020;30(1):NP16–NP20. Epub 2018 Oct 14. PMID: 30318913. doi:10.1177/1120672118805873
21. Miller VJ, Patnaik JL, Young CEC, et al. Outcomes of kahook dual blade goniotomy for uveitis associated open angle glaucoma or ocular hypertension. J Glaucoma. 2022;31(11):903–908. PMID: 35980845. doi:10.1097/IJG.0000000000002099
22. New World Medical, Inc. Kahook Dual Blade: the Reliable Choice. Labtician Ophthalmics, Inc; 2020. Available from: https://www.labtician.com/wp-content/uploads/2020/07/55-0018-SurgicalStepsKDB-MM.pdf.
23. American Academy of Ophthalmology. ICD-10-CM Quick Reference Guide for Glaucoma. San Francisco: American Academy of Ophthalmology; 2015.
24. Mosaed M. Comprehensive trabectome outcomes in surgery-naïve versus previously operated eyes. Eur Ophthalmol Rev. 2018;12(1):50–55. doi:10.17925/EOR.2018.12.1.50
25. Mosaed S, Chak G, Haider A, Lin KY, Minckler DS. Results of trabectome surgery following failed glaucoma tube shunt implantation: cohort study. Medicine. 2015;94(30):e1045. PMID: 26222842; PMCID: PMC4554133. doi:10.1097/MD.0000000000001045
26. Sieck EG, Epstein RS, Kennedy JB, et al. Outcomes of kahook dual blade goniotomy with and without phacoemulsification cataract extraction. Ophthalmol Glaucoma. 2018;1(1):75–81. PMID: 32672636. doi:10.1016/j.ogla.2018.06.006
27. Pratte EL, Cho J, Landreneau JR, Hirabayashi MT, An JA. Predictive factors of outcomes in kahook dual blade excisional goniotomy combined with phacoemulsification. J Curr Glaucoma Pract. 2022;16(1):47–52. PMID: 36060044; PMCID: PMC9385392. doi:10.5005/jp-journals-10078-1313
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension
Matsuo M, Matsuoka Y, Tanito M
Clinical Ophthalmology 2022, 16:1261-1279
Published Date: 26 April 2022
Interim Analysis of STREAMLINE® Surgical System Clinical Outcomes in Eyes with Glaucoma
Lazcano-Gomez G, Garg SJ, Yeu E, Kahook MY
Clinical Ophthalmology 2022, 16:1313-1320
Published Date: 27 April 2022
24-Month Outcomes of Ahmed ClearPath® Glaucoma Drainage Device for Refractory Glaucoma
Dorairaj S, Checo LA, Wagner IV, Ten Hulzen RD, Ahuja AS
Clinical Ophthalmology 2022, 16:2255-2262
Published Date: 13 July 2022
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Six-Month Outcomes of Goniotomy Performed with a Trapezoidal Dual Blade in Combination with Cataract Surgery
Meyer AD, Huggins D, Nwokeji I, Provencher LM
Clinical Ophthalmology 2024, 18:2619-2625
Published Date: 19 September 2024