Back to Journals » Clinical Ophthalmology » Volume 17
Comparison of Efficacy of Combined Phacoemulsification and iStent Inject versus Combined Phacoemulsification and Hydrus Microstent
Authors Chee WK, Yip VCH, Tecson IO, Chua CH, Ang BCH, Kee AR, Hu JY, Kan TCJ, Yip LWL ![]()
Received 26 January 2023
Accepted for publication 24 March 2023
Published 14 April 2023 Volume 2023:17 Pages 1151—1159
DOI https://doi.org/10.2147/OPTH.S403386
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Wai Kitt Chee,1 Vivien Cherng Hui Yip,1 Ivan O’Neill Tecson,1 Chun Hau Chua,1 Bryan Chin Hou Ang,1 Ae Ra Kee,1 Jeremy Youwei Hu,1 Tsia-Chuen John Kan,1 Leonard Wei Leon Yip1,2
1Department of Ophthalmology, National Healthcare Group Eye Institute, Tan Tock Seng Hospital, Singapore, Singapore; 2Lee Kong Chian School of Medicine, Nanyang Technological University, Singapore, Singapore
Correspondence: Vivien Cherng Hui Yip, Department of Ophthalmology, National Healthcare Group Eye Institute, Tan Tock Seng Hospital, 11 Jalan Tan Tock Seng, Singapore, 308433, Singapore, Tel +65 62566011, Email [email protected]
Aim: This study aims to compare the efficacy and safety of combined phacoemulsification with iStent inject (Phaco-iStent) and Hydrus microstent (Phaco-Hydrus).
Methods: This was a retrospective comparative study of patients who underwent Phaco-iStent from April 2019 to August 2020 and Phaco-Hydrus from August 2019 to December 2020 at a tertiary eye centre in Singapore. Sixty-nine Phaco-iStent eyes and 49 Phaco-Hydrus eyes were included in this study. Complete surgical success was defined as freedom from second glaucoma surgery, Intraocular pressure (IOP) of 18 mmHg or less, and discontinuation of all antiglaucoma medications.
Results: At 12 months, both Phaco-iStent and Phaco-Hydrus groups had comparable surgical success rate (68.1% vs 51%, p=0.061), reduction in antiglaucoma medication use (− 1.3 ± 0.1 vs − 1.4 ± 0.10, p=0.880) and intraocular pressure reduction (− 1.1 ± 0.5 mmHg vs – 1.6 ± 0.9 mmHg, p=0.323). Overall intraoperative and postoperative complications rate were similar in both groups, though hyphema was more commonly seen in early postoperative period in the Phaco-Hydrus compared to the Phaco-iStent group (8% vs 0%, p=0.028), with majority of cases resolving without any need for surgical intervention. Device obstruction was also more common in the Phaco-Hydrus group compared to the Phaco-iStent group (14% vs 4.3%, p=0.04).
Conclusion: Phaco-iStent and Phaco-Hydrus have similar surgical efficacy and safety profiles at 12 months.
Keywords: glaucoma, phacoemulsification, cataract extraction, iStent inject, Hydrus microstent
Introduction
Glaucoma is a progressive optic neuropathy where intraocular pressure (IOP) has been shown to be the main modifiable risk factor in reducing glaucoma progression.1 Hence, lowering the IOP is the main goal of treatment in patients with glaucoma. Treatment usually begins with topical antiglaucoma medication or laser therapy. Traditional glaucoma filtration surgery, such as trabeculectomy or tube shunt surgery, has been associated with higher postoperative complication with longer visual recovery, and therefore has often been reserved for refractive cases of glaucoma.2,3
With the advent of minimally invasive glaucoma surgery (MIGS), trabecular bypass procedures using implants like iStent inject (Glaukos Corporation, San Clemente, CA, USA) and Hydrus microstent (Ivantis, Inc, Irvine, CA, USA), have reported effective reduction in IOP and medication use while providing a safe alternative to traditional glaucoma surgeries given their association with low adverse events.4,5 These MIGS devices also do not preclude future filtration surgery, if necessary.
In fact, cataract surgery alone aids in physiological outflow and reduction of IOP.5–7 iStent inject and Hydrus microstent has the advantage of using the same clear cornea incision made during cataract surgery to implant these devices, augmenting the pressure-lowering effect of cataract surgery without the need for scleral or conjunctival manipulation.4,5
The iStent G1 is a “L”-shaped titanium device, with a single fluid inlet port and extension that is designed to extend approximately 1 mm into the Schlemm’s canal. The iStent inject is the second generation iStent which is preloaded with two stents and is roughly one third the size of the previous stent. The iStent inject has a rear flange which resides in the anterior chamber and a head that resides in the Schlemm’s canal, providing a patent bypass pathway through the trabecular meshwork. The Hydrus microstent, in contrast, bypasses the trabecular meshwork and scaffolds approximately 90 degrees of the Schlemm’s canal, providing direct access to the anterior chamber through its inlet.4,5
Thus far, the COMPARE study is the only head-to-head study comparing the differences in the surgical outcome of two iStent G1 vs Hydrus microstent. The COMPARE study has reported superior reduction of IOP and number of antiglaucoma medications in stand-alone Hydrus compared with two iStent G1 at one year.8 However, there is lacking evidence comparing the outcome of iStent inject and Hydrus microstent in Asian eyes. This is important as Asian eyes respond differently to glaucoma surgery when compared to Caucasian eyes, as Asian eyes have been associated with higher amount of pigmentation and inflammation when undergoing glaucoma filtration surgery.9
Therefore, this study aims to compare the efficacy and safety of combined phacoemulsification with iStent inject (Phaco-iStent) and combined phacoemulsification with Hydrus microstent (Phaco-Hydrus) in Asian patients with open angle glaucoma.
Methods
Study Design
This was a retrospective case notes review of consecutive eyes which underwent Phaco-iStent between April 2019 to August 2020 and Phaco-Hydrus between August 2019 and December 2020 at a tertiary eye specialist centre in Singapore.
The study was conducted in compliance with the principles of the Declaration of Helsinki and was approved by the National Healthcare Group Domain Specific Review Board (DSRB) (2021/00093). Informed consent was waived due to the retrospective nature of the study with no patient contact during the process. Patient identifiers are also removed by a third party not involved in the study before the data are analyzed.
Inclusion criteria included eyes with primary open angle glaucoma and normal tension glaucoma of any severity. Exclusion criteria included eyes with previous ocular surgery, such as cornea surgery or glaucoma filtration surgery, and secondary glaucoma. Patients who were lost to follow-up at postoperative month 12 were also excluded. Patients did not have medication washout prior to surgery.
Patient demographics including sex, age and race were collected. Preoperative data including type of glaucoma, IOP, best corrected visual acuity (BCVA), number and subclass of antiglaucoma medications, mean deviation (MD) and pattern standard deviation (PSD) of the latest Humphrey Visual Field (HVF) prior to operation were collected. Severity of glaucoma was classified as mild (MD >−6 dB), moderate (MD −6 dB to −12 dB) and severe (MD <−12 dB).
Surgical Procedure
Standard or femto-second-assisted phacoemulsification was performed. Viscoelastic device of surgeon choice was injected into the anterior chamber. Using a surgical goniolens, two iStent inject was implanted at the trabecular meshwork into Schlemm’s canal at the nasal quadrant. Whereas, for the Hydrus microstent, the tip of a preloaded injector was embedded into the trabecular meshwork and the device was advanced into the Schlemm’s canal, occupying three clock hours of the nasal quadrant.
All patients received a combination of topical antibiotics and steroid eye drops postoperatively, which was tapered over a period of 4 to 5 weeks. Antiglaucoma medications were either continued or stopped immediately after surgery depending on severity of glaucoma and surgeon discretion. Data from follow-up examination conducted on postoperative day 1, week 1, month 1, month 3, month 6, and month 12 were collected. On each visit, BCVA, IOP, number of antiglaucoma medications and any adverse events were noted.
Outcome Measures
Complete surgical success was defined as freedom from second glaucoma surgery, IOP of 18 mmHg or less and discontinuation of all antiglaucoma medications. Qualified success was defined as freedom from second glaucoma surgery and IOP of 18 mmHg or less with the use of antiglaucoma medication, irrespective of whether laser iridoplasty was performed. Surgical failure was defined as any second glaucoma surgery at any postoperative time or IOP of more than 18 mmHg for two consecutive visits despite use of antiglaucoma medications.
Statistical Analysis
A minimum number of 42 eyes in each group arm was required to detect a 2.5 mmHg difference in mean IOP reduction between groups at 6 months postoperatively, with significance level at 0.05, power of 0.80, and assuming standard deviation of reduction for both group to be 4.0 mmHg.8
Statistical analysis was performed using IBM SPSS 27.0 (IBM Corp, New York, USA) with significance level set at 5% level. Kaplan–Meier method was used to estimate the time to event (time before topical antiglaucoma medication was restarted or glaucoma surgery was needed) and log rank test was used to compare the survival time between the two interventions. Logistic regression was also performed to investigate the association of achieving IOP of 18 mmHg or less with and without medication with other demographic variables, ocular factors and surgical interventions. We used a linear mixed model to analyze the significance of IOP and medication reduction by comparing the baseline values with the each specific time point.
Results
Preoperative Characteristics
There were 69 eyes which underwent Phaco-iStent and 49 eyes which underwent Phaco-Hydrus. Demographics in both arms were similar (Table 1). The Phaco-iStent arm had a significantly higher proportion of eyes with normal tension glaucoma when compared to the Phaco-Hydrus arm (p=0.005). Eyes in the Phaco-Hydrus arm required significantly greater number of medications at baseline compared to the Phaco-iStent arm (2.0 vs 1.62 medications, p=0.006).
 |
Table 1 Baseline Demographics |
Outcomes
Surgical Success
Complete success rate at 1 year postoperatively was 68.1% (n=47) and 51% (n=25) in the Phaco-iStent and Phaco-Hydrus group respectively (p=0.061). Qualified success rate was 30% (n=21) and 45% (n=22) in the Phaco-iStent and Phaco-Hydrus group respectively (p=0.108). Surgical failure rates were 1.4% (n=1) and 4.1% (n=2) in the Phaco-iStent and Phaco-Hydrus group respectively (p=0.569). The two eyes in the Phaco-Hydrus group which had surgical failure had underlying advanced primary open angle glaucoma and IOP control remained persistently suboptimal postoperatively, requiring trabeculectomy and Ahmed tube respectively. The eye in the Phaco-iStent group which had surgical failure also had advanced primary open angle glaucoma and developed aqueous misdirection intraoperatively and IOP remained poorly controlled postoperatively. Twelve months event-free survival rate as depicted in in Figure 1, was 68.1% in the Phaco-iStent arm and 51.0% in the Phaco-Hydrus group (p=0.082, log rank test). Logistic regression was used to find possible demographic and ocular factors influencing the probability of achieving an IOP of ≤18 mmHg without glaucoma medication at postoperative month 12. The model included the treatment groups (Phaco-iStent and Phaco-Hydrus), age, type of glaucoma, number of baseline glaucoma medication as well as glaucoma severity. The treatment group, age, number of preoperative glaucoma medication, type of glaucoma and glaucoma severity had no significant influence on the probability of achieving an IOP of ≤18 mmHg with and without glaucoma medication at postoperative month 12.
 |
Figure 1 Kaplan–Meier survival curves for complete success up to month 12. No significant difference in survival distribution between treatment arms (p=0.082, log rank test). |
Intraocular Pressure and Antiglaucoma Medications
Mean IOP and mean number of antiglaucoma medication at each time point are shown in Figure 2A and B respectively. There was also no statistically significant difference in reduction of IOP at postoperative month 12 compared to baseline when comparing the Phaco-iStent group and Phaco-Hydrus group. In the Phaco-iStent group, mean IOP reduction from baseline was −1.1 ± 0.5 mmHg (p=0.149). However, in the Phaco-Hydrus group, mean IOP reduction from baseline was −1.6 ± 0.9 mmHg (p=0.384). The difference of mean IOP reduction at postoperative month 12 between the two groups was 0.7 mmHg (p=0.323).
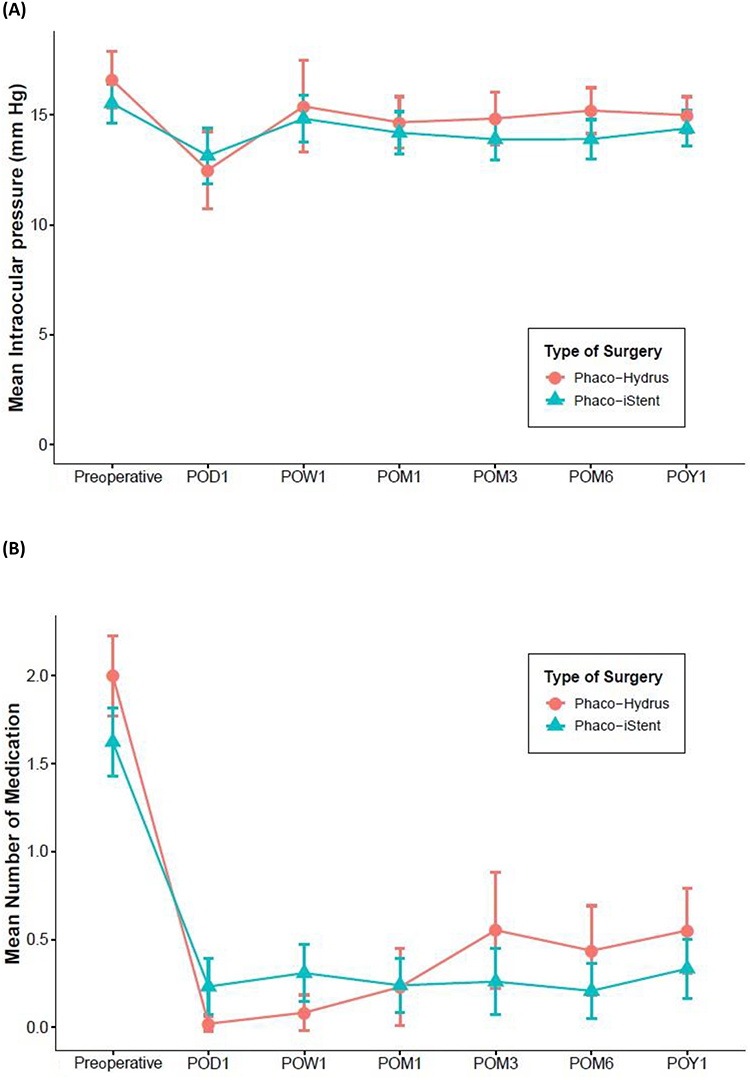 |
Figure 2 (A) Mean IOP: There was no significant difference in IOP between the Phaco-Hydrus and Phaco-iStent groups at each time point. Error bars represents 95% confidence interval. (B) Mean number of medication: There was no significant difference in the number of medication between Phaco-Hydrus and Phaco-iStent at each time point. Error bars represents 95% confidence interval. |
Preoperatively, all eyes in both groups needed one or more antiglaucoma medications. Both arms saw a significant reduction in antiglaucoma medication use after surgery, which was sustained at 12 months, although there was an upward trend seen in the Phaco-Hydrus arm (Figure 2B). There was no significant difference in mean number of medication reduction between the two groups at postoperative month 12 (−1.3 ± 0.1 for Phaco-iStent group vs −1.4 ± 0.1 for Phaco-Hydrus group).
A subgroup analysis examining eyes with primary open angle glaucoma was performed. This showed that the Phaco-Hydrus group achieved a greater mean IOP reduction compared to the Phaco-iStent group at postoperative month 12, although this difference was not statistically significant (2.2 mmHg vs 1.6 mmHg, p=0.888). Mean medication reduction in the Phaco-iStent group, howeer, was comparable to the Phaco-Hydrus group (−1.4 ± 0.1 vs −1.4 ± 0.2, p=0.345). However, it is worthy to note that the numbers in this subgroup analysis were relatively smaller, n=41 in each group.
Safety
There was no statistically significant difference in the intraoperative and postoperative complications between the two groups other than postoperative hyphema (Table 2). There were 8.2% (n=4) of Phaco-Hydrus eyes which had hyphema, compared to none in the Phaco-iStent group (p=0.028). The four eyes had hyphema on postoperative day 1, of which three of them showed resolution at postoperative week 1, whereas the remaining one developed eight-ball hyphema requiring anterior chamber washout at week 1. In the Phaco-iStent group, one eye developed aqueous misdirection intraoperatively which resolved with Chandler’s procedure. This patient had advanced primary open angle glaucoma, and subsequently suffered a loss of BCVA >2 lines postoperatively. This is likely due to glaucoma progression as this patient has advanced disease.
 |
Table 2 Proportion of Eyes Achieving ≤18 mmHg and 0 Medication |
Device Obstruction
Device obstruction was defined as iris adhesion to the iStent lumen or the Hydrus microstent inlet on gonioscopy. Device obstruction was more common in the Phaco-Hydrus arm (14%, n=8) compared to the Phaco-iStent arm (4.3%, n=3) (p=0.04). For the Phaco-Hydrus group, the highest blockage rate occurred at post-operative month 1 (37.5%, n=3) and postoperative month 3 (37.5%, n=3), while the remaining (25%, n=2) occurred at postoperative month 6. Two of the three eyes with blocked Hydrus at postoperative month 1 were associated with adverse events postoperatively. One eye required anterior chamber washout for total hyphema while the other required anterior chamber paracentesis for high IOP and hyphema. Of the eight eyes which had blocked Hydrus, seven underwent iridoplasty whilst the remaining one eye did not undergo iridoplasty and antiglaucoma medication was started. Of these seven eyes, five did not require drops or further surgical intervention. Two eyes were subsequently started on antiglaucoma medication, of which one eye subsequently underwent trabeculectomy. Another two eyes also underwent prophylactic iridoplasty for impending blockage of implant in the Phaco-Hydrus group. Of these two eyes, one did not require additional antiglaucoma drops or surgery, while the other eye was started on antiglaucoma drops at the next follow up visit. In the Phaco-iStent group, three eyes were noted to have blocked iStents (both iStents being blocked in two of the eyes, and only one iStent being blocked in the remaining one eye) at postoperative month 3. All three underwent focal iridoplasty. Two eyes did not require additional antiglaucoma medication or surgery postiridoplasty while one eye was started on antiglaucoma medication at the next follow-up visit.
Discussion
This study suggests at 12 months, both Phaco-iStent and Phaco-Hydrus have comparable surgical success rates (68.1% vs 51%, p=0.061). Phaco-Hydrus achieved greater IOP reduction compared to Phaco-iStent at postoperative month 12, although this difference was not statistically significant (1.6 vs 1.1 mmHg, p=0.323). There was also no significant difference between both groups at 1 year in terms of mean reduction in number of antiglaucoma medication. This is in contrast to previous comparative studies, which showed that standalone Hydrus achieved greater reduction in number of antiglaucoma medication as well as surgical success when compared with standalone iStent.8 This difference could be due to the differences in study protocol and design, namely that of our study being a retrospective study, including glaucoma of varying severity and having had no washout of antiglaucoma medication performed preoperatively. It is also worthy to note that the COMPARE study was comparing iStent G1 versus iStent inject in our study, although the number of stents implanted were similar. In contrast to the COMPARE study which looked at standalone Hydrus and iStent, our study evaluated patients who underwent combined phacoemulsification with Hydrus and iStent, which closely mimics real-world clinical practice where MIGS are commonly performed in the same sitting as phacoemulsification. The exact mechanism of IOP lowering in open angle glaucoma from cataract surgery is still unclear. However, there are hypotheses which suggest trabecular endothelium remodeling as a result of stress induced from ultrasound energy during phacoemulsification.10 Another theory proposed that cataract extraction dislodges the zonules over the ciliary body by moving the posterior capsule backwards, resulting in widening of the Schelmm’s canal and thus improving aqueous drainage.11 The mean age of the patients in this study was 72 years of age. Asian eyes have a higher degree of pigmentation and thicker irises. Perhaps earlier cataract surgery combined with MIGS could be considered in Asian eyes, where less phacoemulsification energy is required and thus less inflammation induced. This has been shown to be very successful in decreasing medication burden and maintaining lower IOP among Black patients.12
Success rate was defined based on achieving an IOP of 18 mmHg or less rather than 15 mmHg as suggested by the World Glaucoma Association.13 This is because the baseline preoperative IOP in our study is above 15 mmHg. These patients were regarded to have stable glaucoma and cataracts, for which they were listed for cataract extraction and MIGS in the hope of reducing medication burden. Therefore, we do not expect the IOP to be significantly lower than the preoperative IOP. We did further subgroup analysis was done to evaluate the ability of Phaco-iStent and Phaco-Hydrus in achieving IOP <15 mmHg, which showed that 98.6% of Phaco-iStent and 51% of Phaco-Hydrus group obtained IOP <15 mmHg with or without medication/intervention postoperatively. Of note, our study included a high proportion of patients with advance glaucoma, and hence they often require drops to achieve their target IOP.
This study did not show statistically significant reduction in IOP at 12 months when compared to baseline for both Phaco-Hydrus and Phaco-iStent as they were not subjected to medication washout. Hence, the IOP lowering effect of both Phaco-Hydrus and Phaco-iStent was demonstrated in the reduction of antiglaucoma medication. However, the mean IOP at 1 year for both groups were consistent with previous published studies.14–18 Mean IOP at 1 year was 15.0 ± 2.9mmHg in the Phaco-Hydrus group and 14.4 ± 3.4 mmHg in the Phaco-iStent group. This is consistent with Phaco-Hydrus for primary open angle glaucoma studies, which reported 1 year mean IOP of 13–17 mmHg14,15 and 12–16 mmHg for Phaco-iStent.16,17 Contrary to a previous comparative study8 which suggested that reduction of number of medications was greater in Hydrus when compared to 2-iStent, our study showed that both Phaco-Hydrus and Phaco-iStent reduce medication use equally at 1 year.
Our study also compared the safety of Phaco-Hydrus and Phaco-iStent groups. There was no significant statistical difference between the two groups in their surgical complications except for postoperative hyphema (Phaco-Hydrus 8.2% vs Phaco-iStent 0%, p=0.028). Variable rates of hyphema post-Hydrus implantation were reported in the literature ranging from 1–19%.18,19 In patients on anticoagulant, they should be seated with the head elevated above the waist for 4 days to reduce episcleral venous pressure and back flow of blood from the aqueous veins and prevent the need for evacuation of hyphema.
We also noted that 14% of eyes in the Phaco-Hydrus group had blocked device inlet at various time points during the follow-up, most commonly at postoperative months 1 and 3. This is in comparison to 4.3% of eyes in the Phaco-iStent group. Such device obstructions was reported in other studies, and they can be due to focal iris adhesion, which has been reported in iStent studies, and peripheral anterior synechiae, which were more commonly reported in Hydrus studies.8 For such cases, we performed iridoplasty by applying argon lasers to contract the iris anterior to the stent, pulling it away from the stent. Our rate of Hydrus obstruction was marginally higher than reported in the literature, which reported device obstruction rate of 8–13.9%8,9,14 in Hydrus and 1–13.2%5,8,17 in iStent. The higher incidence of Hydrus device obstruction in our study could be attributed to thicker iris in Asian eyes20,21, which may increase the propensity to be drawn toward the device inlet. We also observed that early Hydrus obstruction could be related to postoperative intervention, where two of the eight patients with blocked Hydrus had anterior chamber paracentesis for retained viscoelastic and anterior chamber washout for hyphema. Iris pigment release and inflammation postoperatively, perpetuated by further postoperative interventions, could increase the risk of stent obstruction from peripheral anterior synechiae, especially in Asian brown irides.9,20 Despite this, the Phaco-Hydrus group still achieved similar IOP reduction when compared to the Phaco-iStent group in our study.
Our study is not without its limitations. This was a retrospective study with a small sample size and a short follow-up duration of 1 year. Furthermore, there were some baseline differences in ocular characteristics of eyes in the Phaco-Hydrus and the Phaco-iStent group. Firstly, there was a higher proportion of normal tension glaucoma eyes in the Phaco-iStent than in the Phaco-Hydrus group. We acknowledge that this may confound the mean IOP reduction from baseline and medication reduction, hence a two-way ANCOVA was used adjusting for the type of glaucoma. Secondly, though the mean preoperative IOP was similar in both groups, eyes in the Phaco-Hydrus group were on greater number of antiglaucoma medication preoperatively. There was also no washout period prior to surgery in both groups.
In conclusion, our study showed that Phaco-Hydrus and Phaco-iStent have similar success rates and safety profile for both primary open angle glaucoma and normal tension glaucoma in Asian eyes. Due to the limitations of our study as mentioned above, further large-scale head-to-head prospective comparative studies are needed to evaluate if both devices are indeed equally effective. Future studies looking at patient reported outcome measures, differences in diurnal variation of IOP will also be helpful in deciding which minimally invasive glaucoma implants to choose.
Disclosure
Dr Bryan Chin Hou Ang receives research support, speaker’s honorarium, and travel reimbursement from Glaukos Corporation and speaker’s honorarium and travel from Alcon, Inc., outside the submitted work. Dr Leonard Wei Leon Yip is a speaker for Glaukos Singapore. The authors report no other conflicts of interest in this work.
References
1. The Advanced Glaucoma Intervention Study (AGIS). 7. The relationship between control of intraocular pressure and visual field deterioration. The AGIS Investigators. Am J Ophthalmol. 2000;130:4290–4440.
2. SooHoo JR, Seibold LK, Radcliffe NM, Kahook MY. Minimally invasive Glaucoma Surgery: current Implants and Future Innovations. Canadian J Ophthalmol. 2014;49(6):528–533. doi:10.1016/j.jcjo.2014.09.002
3. Jablonska J, Lewczuk K, Koponiska J, Mariak Z, Rekas M. Microinvasive Glaucoma Surgery: a Review and Classification of Implant- dependent Procedures and Techniques. Acta Ophthalmol. 2022;100(2):e327–e338. doi:10.1111/aos.14906
4. Laspas P, Pfeiffer N. Hydrus Microstent. In: Sng CCA, Barton K, editors. Minimally Invasive Glaucoma Surgery. Singapore: Springer; 2021.
5. Le K, Saheb H. iStent trabecular micro-bypass stent for open-angle glaucoma. Clin Ophthalmol. 2014;8:1397–1945.
6. Young CE, Seibold LK, Kahook MY. Cataract Surgery and Intraocular Pressure in Glaucoma. Current Opinion in Ophthalmolog. 2020;31(1):15–22. doi:10.1097/ICU.0000000000000623
7. Mansberger SL, Gordon MO, Jampel H, et al. Reduction in intraocular pressure after cataract extraction. Ocular Hypertension Treatment Study Ophthalmol. 2012;119(9):1826–1831. doi:10.1016/j.ophtha.2012.02.050
8. Ahmed I, Fea A, Au L, et al. A prospective Randomized Trial Comparing Hydrus and iStent Microinvasive Glaucoma Surgery Implants for Standalone Treatment of Open-Angle Glaucoma- The COMPARE Study. Ophthalmology. 2020;127:52–61. doi:10.1016/j.ophtha.2019.04.034
9. Corbett MC, Hingorani M, Boulton JE, Shilling JS. Factors predisposing to postoperative intraocular inflammation. Eur J Ophthalmol. 1995;5(1):40–47. doi:10.1177/112067219500500107
10. Wang N, Chintala SK, Fini ME, Schuman JS. Ultrasound activates the TM ELAM-1/IL-1/NF-κB response: a potential mechanism for intraocular pressure reduction after phacoemulsification. Invest Ophthalmol Vis Sci. 2003;44(5):1977–1981. doi:10.1167/iovs.02-0631
11. Poley BJ, Lindstrom RL, Samuelson TW, Schulze R. Intraocular pressure reduction after phacoemulsification with intraocular lens implantation in glaucomatous and nonglaucomatous eyes: evaluation of a causal relationship between the natural lens and open-angle glaucoma. J Cataract Refract Surg. 2009;35:1946–1955. doi:10.1016/j.jcrs.2009.05.061
12. Laroche D, Oseni J, Nkrumah G, Ng C. Clear Lensectomy with Hydrus Stent in Black and AfroLatino Patients: a 1-Year Retrospective Study. J Ophthalmol. 2022;2022:8011745. doi:10.1155/2022/8011745
13. Shaarawy T, Grehn F, Sherwood M. WGA Guidelines on Design and Reporting of Glaucoma Surgical Trials. The Hague: Kugler Publications; 2009.
14. Samuelson TW, Chang DF, Marquis R, et al. A Schlemm canal microstent for intraocular pressure reduction in primary open-angle glaucoma and cataract: the HORIZON study. Ophthalmology. 2018;126(1):29–37. doi:10.1016/j.ophtha.2018.05.012
15. PfeiNer N, Garcia-Feijoo J, et al. A randomized trial of a Schlemm’s canal microstent with phacoemulsification for reducing intraocular pressure in open-angle glaucoma. Ophthalmology. 2015;122(7):1283–1293. doi:10.1016/j.ophtha.2015.03.031
16. Dorairaj S, Kahook MY, Williamson BK, et al. Comparison of Goniotomy versus Trabecular Bypass Device Implantation in Glaucoma Patients Undergoing Cataract Extraction. Clin Ophthalmology. 2018;12:791. doi:10.2147/OPTH.S158403
17. Tan SZ, Au L. Manchester iStent Study: 3-year results and cost analysis. Eye. 2016;30:1365–1370. doi:10.1038/eye.2016.139
18. Fea AM, Rekas M, Au L. Evaluation of a Schlemm Canal Scaffold microstent combined with Phacoemulsification in Routine Clinical Practice: two-year Multicentre Study. J Cataract Refract Surg. 2017;4397:886–891. doi:10.1016/j.jcrs.2017.04.039
19. Ganofi SA, Ungaro N, Ghirardini S, Tardini MG, Mora P. Comparison of Surgical Outcomes between Canaloplasty and Schlemm’s Canal Scaffold at 24 months’ follow up. J Ophthalmol. 2016;2016:3410469. doi:10.1155/2016/3410469
20. Lowe RF. Clinical types of primary angle closure glaucoma, Aust NZ. J Ophthalmol. 1988;16:245–250.
21. Wang D, He M, Weu L, Yaplee S, Singh K, Lin S. Differences in iris structural measurements among American Caucasians, American Chinese and mainland Chinese. Clin Exp Ophthalmol. 2012;40(2):162–169. doi:10.1111/j.1442-9071.2011.02658.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Spotlight on Schlemm’s Canal MicroStent Injection in Patients with Glaucoma
Wagner IV, Ang B, Checo L, Simsek D, Draper C, Dorairaj S
Clinical Ophthalmology 2023, 17:1557-1564
Published Date: 2 June 2023
Comparing Outcomes of Phacoemulsification and Endocyclophotocoagulation with Either Dual Blade Goniotomy (PEcK) or Two Trabecular Stents (ICE2)
El Helwe H, Oberfeld B, Golsoorat Pahlaviani F, Falah H, Trzcinski J, Solá-Del Valle D
Clinical Ophthalmology 2023, 17:2879-2888
Published Date: 3 October 2023
Long-Term Efficacy of Successful Excisional Goniotomy with the Kahook Dual Blade
Wagner IV, Boopathiraj N, Lentz C, Dorairaj EA, Draper C, Kumar D, Checo L, Miller DD, Krambeer C, Dorairaj S
Clinical Ophthalmology 2024, 18:713-721
Published Date: 7 March 2024
Six-Month Outcomes of Goniotomy Performed with a Trapezoidal Dual Blade in Combination with Cataract Surgery
Meyer AD, Huggins D, Nwokeji I, Provencher LM
Clinical Ophthalmology 2024, 18:2619-2625
Published Date: 19 September 2024