Back to Journals » Drug Design, Development and Therapy » Volume 20
Efficacy and Safety of Upadacitinib for Refractory Inflammatory Bowel Disease: A Multicenter Real-World Observational Study
Authors Mao Y ![]() , Hu Y
, Hu Y ![]() , Sun S
, Sun S ![]() , Chen Y, Lyu W, Lv B, Fan Y
, Chen Y, Lyu W, Lv B, Fan Y
Received 1 December 2025
Accepted for publication 12 March 2026
Published 25 March 2026 Volume 2026:20 585709
DOI https://doi.org/10.2147/DDDT.S585709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Yuqing Mao,1,* Yibo Hu,1,* Shaopeng Sun,1 Yan Chen,2 Wen Lyu,3 Bin Lv,4 Yihong Fan4
1Department of Gastroenterology, The First Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, 310000, People’s Republic of China; 2Department of Gastroenterology, The Second Affiliated Hospital of Zhejiang University, Hangzhou, 310000, People’s Republic of China; 3Department of Gastroenterology, Hangzhou First People’s Hospital, Hangzhou, 310000, People’s Republic of China; 4Department of Gastroenterology, the First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Traditional Chinese Medicine), Hangzhou, 310000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yihong Fan, Email [email protected] Bin Lv, Email [email protected]
Background: Although Upadacitinib has proven success in inflammatory bowel diseases (IBD), there is less data on its efficacy and safety in Asian patients with refractory IBD.
Methods: This multicenter study evaluated the real-world effectiveness and safety of UPA in patients with refractory IBD. This multicenter retrospective cohort analysis included adult refractory IBD patients who received UPA therapy at three tertiary hospitals from January 2023 to March 2025. Clinical, endoscopic, and laboratory outcomes were effectiveness goals. Safety measures included AEs and and rates of discontinuation.
Results: A total of 80 eligible patients were enrolled, including 52 with CD and 28 with UC. During the induction period, for CD: steroid-free clinical remission: 59.6%; clinical response: 61.5%; endoscopic remission: 30.8%; endoscopic response: 57.7%. For UC, steroid-free clinical remission: 67.9%; clinical response: 71.4%; endoscopic remission: 46.4%; endoscopic response: 60.7%. In the maintenance phase (12 months), CD had 78.8% steroid-free clinical remission and 75.0% endoscopic remission. UC had 85.7% steroid-free clinical remission and 78.6% endoscopic remission. Inflammatory indicators and nutritional parameters improved significantly. The incidence of adverse events in CD and UC was 23.1% and 14.3%, respectively, and the discontinuation rates during the 12-month maintenance treatment period were 7.1% and 21.5%, respectively. The most common adverse reaction is acne (8.75%).
Conclusion: UPA demonstrated robust real-world effectiveness and an acceptable safety profile in Asian patients with refractory IBD.
Keywords: upadacitinib, inflammatory bowel disease, Crohn’s disease, ulcerative colitis, difficult-to-treat, real-world evidence
Introduction
Inflammatory bowel diseases (IBD), which include ulcerative colitis (UC) and Crohn’s disease (CD), are immune-mediated inflammatory diseases (IMIDs) that typically require long-term immunosuppression.1,2 Treatment targets of IBD have become more rigorous over the past two decades, advancing from symptomatic improvement to clinical remission, and subsequently to biochemical and endoscopic remission. Further goals for therapeutic targets have expanded to include histological remission in UC and transmural healing in CD.3–5
While biologics have improved IBD treatment outcomes, their limitations still restrict clinical usefulness. Most biologics achieve a 40% clinical remission rate at 52 weeks in IBD patients.6–9 Real-world studies show that 30–40% of patients with moderate to severe UC have inadequate treatment responses, and only 19–33% achieve clinical remission after biologic therapy.10–12 For CD, real-world evidence similarly indicates suboptimal outcomes: meta-analysis of anti-TNFα agents in routine clinical practice reports a 1-year clinical remission rate of 37.1%-48.6%,11 with specific biologics such as ustekinumab achieving 37.1–45.8% clinical remission at 52 weeks,12 and mirikizumab demonstrating 54.1% clinical remission in a large real-world cohort.13 Notably, 29.6% of CD patients fail to achieve meaningful response to biologic therapy in real-world settings,13 and long-term maintenance remains challenging for many. Despite more therapy options, many patients struggle to maintain remission. Thus, to standardize future research and guide treatment choices, the international Organization for the Study of Inflammatory Bowel Disease (IOIBD) held a worldwide expert consensus meeting to define difficult-to-treat (DTT) IBD in a simple, operative manner.13–16
Janus kinase inhibitors (JAKis) are innovative oral small-molecule drugs targeting the JAK-STAT signaling pathway to control pro-inflammatory cytokines involved in the pathogenesis of IBD.17–20 Upadacitinib (UPA), a second-generation selective JAK1 inhibitor, was approved for UC in June 2023, and subsequently received approval for CD in January 2024.18,19
Significant clinical data from pivotal Phase III registration trials underpin the efficacy of UPA across the spectrum of IBD. In UC, the UPA 45 mg/day regimen demonstrated significantly superior clinical remission rates versus placebo in two identical phase III induction studies (U-ACHIEVE and U-ACCOMPLISH), with this benefit being particularly evident in patients previously exposed to biologics.20 Consequently, network meta-analyses consistently rank UPA among the most effective agents for inducing remission in UC.21
The therapeutic promise of UPA extends robustly to CD, as definitively established by its dedicated phase III clinical program. The U-EXCEL and U-EXCEED induction trials collectively demonstrated that UPA 45 mg/day for 12 weeks was significantly more effective than placebo in achieving both clinical remission and endoscopic response in patients with moderate-to-severe CD.15 Patients who responded to this induction therapy were then re-randomized in the U-ENDURE maintenance trial, which confirmed the sustained efficacy of UPA. At week 52, both UPA 15 mg and 30 mg doses were significantly superior to placebo in maintaining clinical remission (48.1% and 57.9% vs. 15.2%, respectively) and endoscopic remission (27.0% and 39.7% vs. 7.3%).21 These registration trials collectively establish UPA as a leading therapeutic option for inducing and sustaining both clinical and endoscopic outcomes in moderate-to-severe CD.
Nonetheless, safety issues remain. First-generation pan-JAK inhibitors, such as tofacitinib, are associated with risks of thrombosis, severe infections, and malignancies due to extensive JAK inhibition, leading to FDA black-box warnings in 2019 and EMA limits for high-risk populations.10,15 By specifically inhibiting JAK1-dependent cytokines, UPA may reduce off-target hazards while preserving efficacy; nonetheless, long-term safety necessitates real-world validation.22
Looking beyond systemic pharmacodynamics, the next frontier in optimizing JAK inhibitor therapy involves advanced drug delivery strategies designed to enhance mucosal bioavailability and minimize systemic exposure [PMID:36356302]. The inflamed intestinal mucosa in IBD is characterized by a dysregulated microenvironment, characterized notably by overproduction of reactive oxygen species (ROS) and a concomitant diminished activity of endogenous antioxidant enzymes23. This oxidative-reductive (redox) imbalance contributes to mucosal damage and barrier dysfunction. Recent innovations in nanomedicine have exploited this pathological characteristic to engineer ROS-responsive drug delivery systems.24 Materials such as boronates, polydopamine, sulfides, and metal-based nanozymes can sense elevated ROS levels at inflammatory sites and undergo controlled degradation or activation. They release their therapeutic payload in a spatially and temporally precise manner. This approach not only directly neutralizes pathogenic ROS but also ensures high local drug concentrations where needed most, potentially improving efficacy and reducing off-target effects. Furthermore, the concept of “layered programmable delivery”—integrating ROS-responsive mechanisms with other stimuli-sensitive and targeted modalities—holds promise for overcoming the limitations of single-mechanism systems. Such multi-stage, multifunctional platforms could guide drugs more intelligently through the gastrointestinal tract to the inflamed mucosa, significantly enhancing delivery efficiency and therapeutic precision for IBD25.
UPA is the first licensed JAK1 selective inhibitor for CD and has shown efficacy in multiple phase III clinical trials, however real-world efficacy and safety evidence for DTT-IBD patients is lacking. Few studies have examined Asian DTT-IBD populations, and most have been conducted in Western countries. This multicenter trial examines UPA’s efficacy and safety for induction and maintenance therapy in China DTT-IBD.
Materials and Methods
Data Selection
This multicenter retrospective cohort study collected data from IBD patients treated with UPA at three tertiary hospitals in China from 1 January 2023 to 30 March 2025. Patients were diagnosed as IBD using established criteria.26 To ensure reproducibility of patient selection, data were abstracted from the standardized electronic medical records (EMR) of each center using a pre-defined, structured case report form. Two trained investigators per center independently extracted the data; a third senior reviewer cross-checked a random 20% sample, with inter-rater agreement exceeding 95%. Discrepancies were resolved by consensus. The research received approval from the Medical Ethics Committees of each hospital (Ethics Approval Numbers: 2025-KL-321-02, No. 2025-0521, 2025No. 1106-18). Patient anonymity was preserved, and informed consent was exempted due to the retrospective nature of the study. Data were acquired from electronic medical records by personnel at each center.All data were systematically acquired from the standardized electronic medical records (EMR) systems of each participating center by trained data abstractors. All methods were performed in accordance with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Patient selection aimed to include a well-defined “difficult-to-treat” (DTT) IBD cohort, based on the criteria outlined by the International Organization for the Study of IOIBD: (1) failure of at least two biologics or small molecule agents with distinct mechanisms of action, (2) recurrence following a minimum of two surgeries in adult Crohn’s disease patients (one surgery in pediatric patients), (3) combined with chronic antibiotic-refractory pouchitis, (4) combined with complex perianal disease, (5) combined with psychosocial diseases affecting disease management. Patients were identified via a systematic query of each hospital’s EMR for IBD diagnoses and Upadacitinib prescriptions within the study period, and their medical charts were individually reviewed to confirm DTT status against the IOIBD criteria. Inclusion criteria: (1) refractory IBD patients from three centers between January 2023 and March 2025; (2) Received at least 8 weeks (for UC) or 12 weeks (for CD) of UPA treatment, corresponding to the induction periods. Exclusion criteria: (1) pregnancy and breastfeeding; (2) serious infections or history of malignancy; (3) liver impairment (ALT or AST > 3 times the upper limit of normal) or kidney impairment (estimated glomerular filtration rate < 30 mL/min/1.73m2); (4) history of total colectomy for UC; (5) Patients lacking sufficient baseline or follow-up data in their medical records to adequately assess the pre-defined primary therapeutic efficacy endpoints or safety, as detailed in section 2.3 and 2.4. Such patients were excluded to ensure data completeness for the core analyses. (6) Patients receiving concomitant biological agents (eg, infliximab, vedolizumab) during upadacitinib therapy. Given the retrospective, observational nature and the specific, real-world DTT-IBD population, a formal a priori sample size calculation was not performed. The cohort size represents all eligible patients treated within the study period across the three centers.
Demographic and Clinical Data
Data Abstraction:Baseline and follow-up data were extracted from the hospital electronic medical records by two physicians at each center. One collected data using a standardized form, while the other verified it. Discrepancies were resolved through discussion to reach consensus.
The collected data include general information, clinical data, past medication history related to IBD, and surgical history related to IBD. General information includes gender, age, diagnosis (UC, CD), disease duration, and age at diagnosis. Clinical data include lesion location, disease severity score, complications, extraintestinal manifestations, inflammatory markers (CRP, FC, and ESR), nutritional parameters (25(OH) Vitamin D and ALB), and other laboratory parameters. Normal reference values for each indicator are as follows: CRP (0–8 mg/L), FC (0–50 μg/g), ESR (0–15 mm/h), 25(OH) VitD (50–125 nmol/L), ALB (40–55 g/L), WBC (3.5–9.5×109/L), Hb (115–150 g/L), PLT (125–350×109/L), ALT (7–40 U/L), AST (13–35 U/L), HDL-C (>1.04 mmol/L), TC (3.1–5.18 mmol/L), LDL-C (<3.37 mmol/L).
Disease activity in UC patients was evaluated using the adapted Mayo score, with corticosteroid-free clinical remission defined as a score ≤ 2 and a single item score ≤ 1 after stopping glucocorticoids for at least 3 months. Clinical response was defined as a ≥ 30% decrease from baseline, a score ≥ 3, and a ≥ 1 decrease in bleeding score or a score of 0–1. The endoscopic assessment was conducted using the Mayo endoscopic subscore. Endoscopic remission was defined as a Mayo endoscopic subscore of 0, and endoscopic response was defined as a reduction of >50% in Mayo score from baseline.27
Disease activity in CD patients was assessed using the Harvey-Bradshaw Index (HBI), with steroid-free clinical remission defined as an HBI ≤ 4 after discontinuation of corticosteroids for at least 3 months. Clinical response is characterized by a decrease of 3 or 50% in the HBI scores. Simple Endoscopic Score for Crohn’s Disease (SES-CD) was used for endoscopic evaluation, with scores ≤ 3 or Rutgeerts ≤ i1 indicating remission and a ≥50% decrease indicating response.
Biochemical remission was defined as fecal calprotectin (FC) <150 ug/g or C-reactive protein (CRP) < 8mg/L. Other laboratory parameters, including inflammatory markers, nutritional status, and liver and kidney function, were systematically monitored in both UC and CD patients. Adverse events were documented to evaluate treatment safety.8,28,29
Outcomes
This study is a retrospective study, all 80 patients completed at least 12 months of follow-up. Treatment followed a pragmatic real-world regimen: induction therapy consisted of upadacitinib 45 mg once daily (8 weeks for UC, 12 weeks for CD). Maintenance therapy was initiated with 15 mg once daily for both diseases. Dose escalation to 30 mg once daily during maintenance was permitted at the discretion of the treating physician, typically for patients exhibiting inadequate clinical or endoscopic response, disease flare, or persistent objective inflammation despite 15 mg therapy. This flexible dosing strategy reflects routine clinical management of refractory IBD and was documented for each patients. Record the concurrent medication usage during the treatment period.
The main outcomes assessed were steroid-free clinical remission, clinical response, endoscopic remission, and endoscopic response for both induction and maintenance therapy in UC and CD. Steroid-free clinical remission refers to a state where the patient was initially treated with steroids when starting biologic therapy, gradually tapered and discontinued steroids during subsequent follow-ups while maintaining stable condition, and achieved clinical remission without steroids after the induction period. Secondary endpoints included biochemical remission rate and incidence of adverse events (AEs) for induction and maintenance therapy. The necessity for surgery was deemed a failure of treatment concerning all endoscopic and clinical outcomes. Treatment-emerged adverse events (TEAE) were monitored including leukopaenia, elevated liver tests, infections [including tuberculosis and herpes zoster (HZ) specifically], malignancy, intestinal perforation, non-melanoma skin cancer, major adverse cardiovascular events (MACE), dyslipidaemia, hospitalization, and death. Serious adverse events were defined as intestinal perforation, cardiovascular event, hospitalization, or mortality. Clinical and endoscopic assessments were scheduled at induction completion (week 8 for UC, week 12 for CD), and at months 6 and 12 of maintenance therapy. Inflammatory and nutritional biomarkers were additionally followed up to 18 months.
Statistical Analysis
Data analysis and graph generation were conducted utilizing SPSS V.27 (IBM) and Prism V.10.1.2 (GraphPad Software, San Diego, California, USA). Categorical variables were represented as percentages. Quantitative variables were reported as mean and standard deviation (SD) or median and interquartile range (IQR), depending on the adherence to normal distribution. Because patients with missing primary efficacy or safety data were excluded according to the protocol (see section 2.2), all analyses were performed on a complete-case basis. No imputation techniques were applied for missing data. The Kruskal–Wallis test was employed for the comparison of non-parametric continuous variables. All statistical tests regarded p<0.05 as indicative of statistical significance. Given the retrospective observational design, the lack of a formal a priori power calculation, and the modest cohort size inherent to this specific DTT-IBD population, all statistical analyses should be considered exploratory. Effect estimates are presented with corresponding p-values and, where appropriate, 95% confidence intervals; however, the precision of these estimates is limited, and subgroup findings in particular require cautious interpretation. No adjustment for multiple comparisons was performed, consistent with the exploratory nature of the study.
The efficacy of UC and CD during the induction phase was assessed at weeks 8 and 12, respectively. Clinical and endoscopic data were followed up for 12 months, while inflammatory and biochemical markers were followed up for 18 months. A result was considered statistically significant when its p-value was <0.05.
Result
Comparison of Baseline Characteristics
As shown in Table 1, A total of 80 patients were included in this study, divided into two groups based on diagnosis (Group 0, N=28; Group 1, N=52). Baseline characteristics analysis showed that there were statistically significant differences between the two groups in age (51 [38, 60] years vs. 34 [29, 42] years, P<0.001) and age at diagnosis (43 [35, 50] years vs. 26 [19, 36] years, P<0.001), with Group 1 patients being younger. In terms of disease-related characteristics, the proportion of patients in Group 1 who had previously received immunosuppressive therapy was significantly higher than that in Group 0 (51.9% vs. 25.0%, P=0.020), and the proportion of patients using corticosteroids at baseline was lower (38.5% vs. 64.3%, P=0.027). Analysis of medication history revealed significant differences between the two groups in the use of anti-integrins (82.1% vs. 19.2%, P<0.001) and IL-12/23 and IL-23 inhibitors (32.1% vs. 75.0%, P<0.001), reflecting different treatment pathways. Additionally, the proportion of patients with a history of surgery in Group 1 was much higher than that in Group 0 (63.5% vs. 10.7%, P<0.001). However, there were no significant differences between the two groups in terms of gender, disease duration, time of first use of Upadacitinib, and the proportion of use of most biologics (such as anti-TNF drugs). At various time points during the treatment period (0, 8/12, 26, 52, and 78 weeks), there were no statistically significant differences between the two groups in biochemical remission rates of fecal calprotectin (FC) and C-reaction protein (CRP), endoscopic remission and response rates, clinical remission and response rates, as well as adverse reactions and discontinuation rates, indicating that the two groups of patients exhibited similar short-term and long-term efficacy indicators and safety profiles after Upadacitinib treatment.
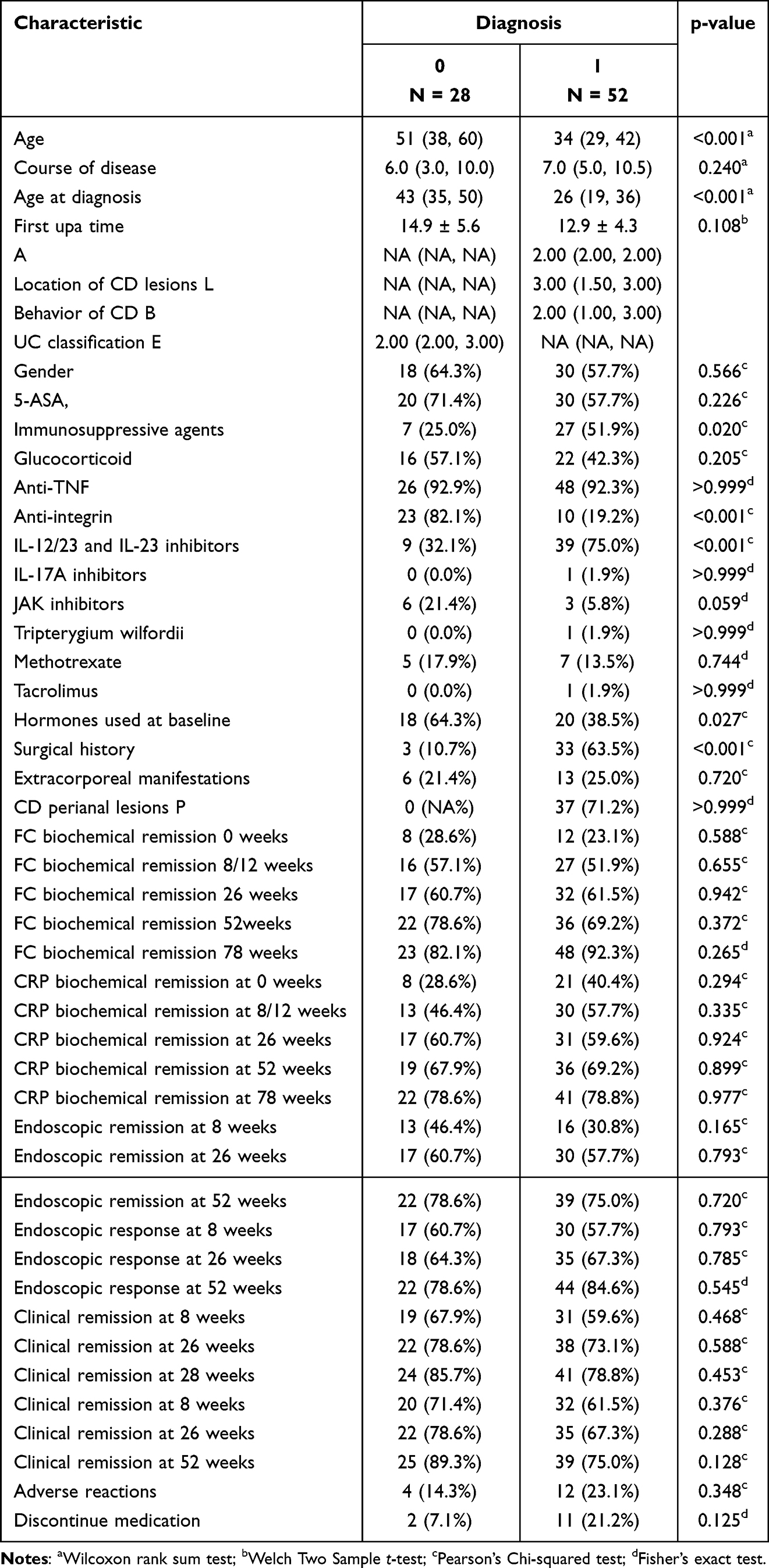 |
Table 1 Patient Demographics and Baseline Characteristics |
The Efficacy and Safety of Upadacitinib in the Treatment of Refractory Inflammatory Bowel Disease
In this study, the elastic net regularization regression method with 10-fold cross-validation was used for variable selection (Figure 1A). The following four variables were considered relatively important: age, anti-integrin, IL.12.23, and IL.23, and the history of inhibitor surgery (Figure 1B). Due to the limitation of the sample size, the Boruta random forest algorithm was further used to evaluate the importance of these variables. The Boruta analysis (Figure 2) showed that 4 variables were determined to be important, including age, anti-integrin, IL.12.23, and IL.23, and the history of inhibitor surgery. The specific importance indicators of each variable are presented in Supplementary Table 1.
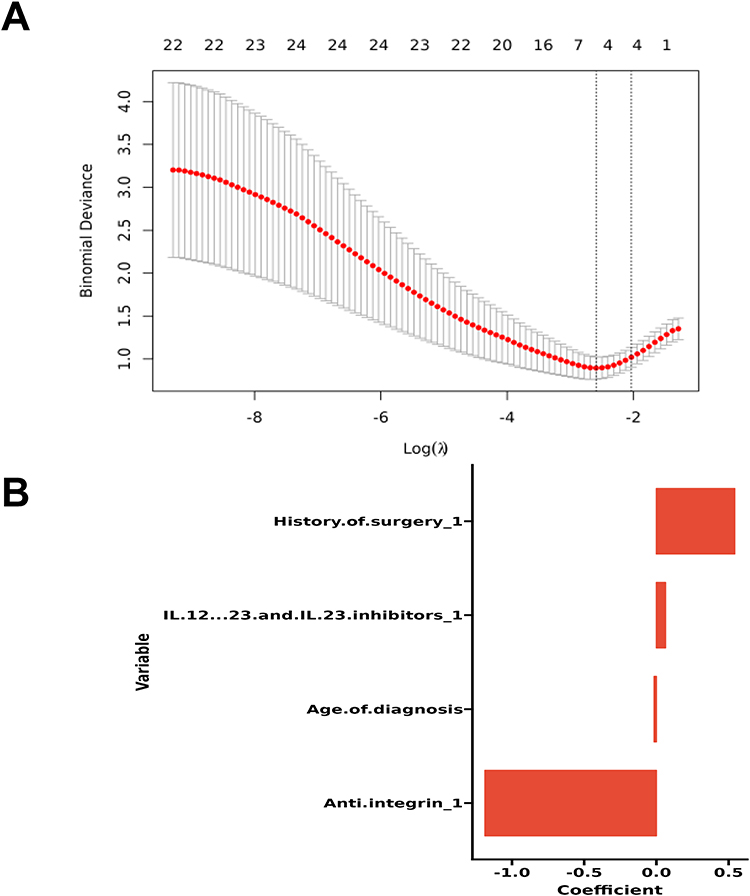 |
Figure 1 Lasso regression screening variables. (A) Elastic net regression model and 10-fold cross-validation to select the most appropriate features (λ = 0.130900498904221); (B) Predictors and corresponding coefficients of elastic network selection. Only variables with non-zero coefficients after elastic network selection were displayed. All variables were included and collinearity interference was excluded. |
 |
Figure 2 Boruta method for variable selection. The variables screened by Lasso were further constructed into a random forest to obtain the importance ranking of the variables. Green, important; yellow, tentative; red, unimportant, blue, shadow. The vertical axis lists the name of each variable, and the horizontal axis is the Z value. |
To evaluate the impact of upatiden on the efficacy of treating refractory inflammatory bowel disease, we established a multivariate logistic regression model based on the results of variable screening (Table 2), and combined the ROC curve to analyze the model for predicting efficacy (Figure 3). This indicates that including IL-12/23 and IL-23 inhibitors, confirmed age, and anti-integrin has better effects in predicting the efficacy of upatiden in treating refractory inflammatory bowel disease.
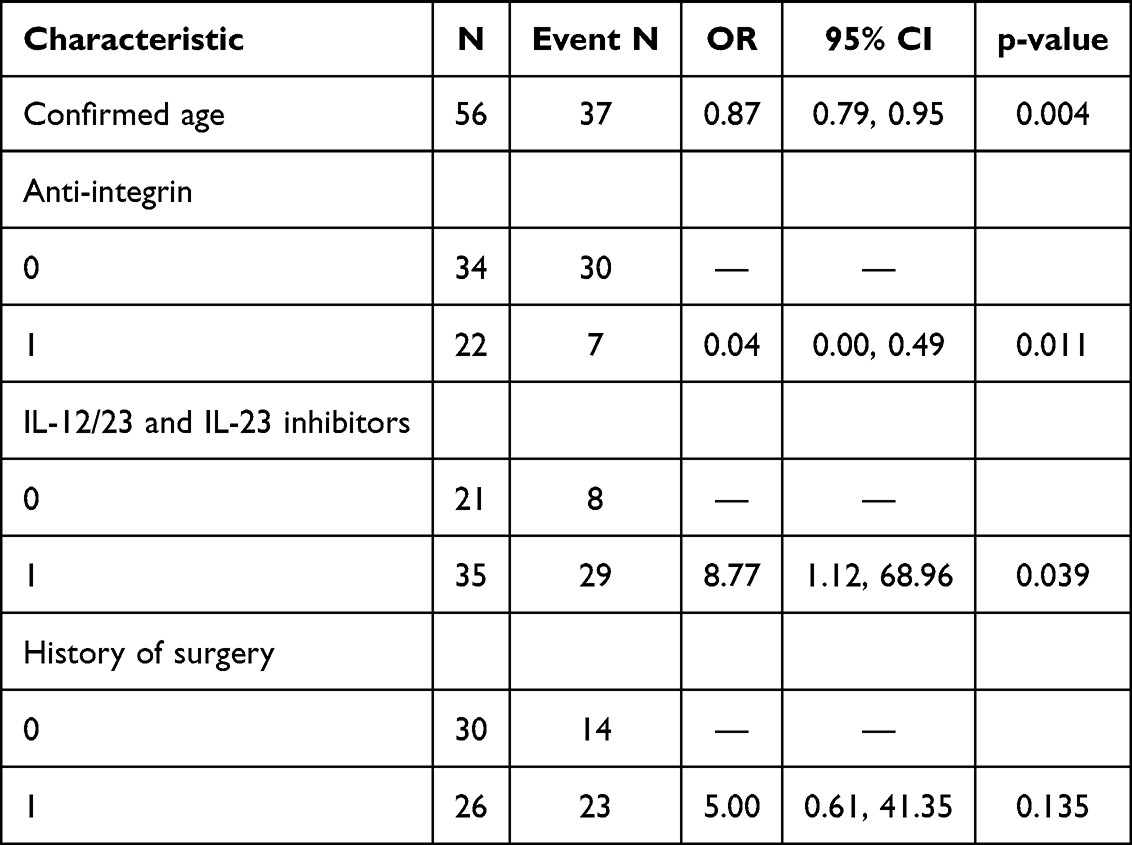 |
Table 2 Multivariate Logistic Regression for Training Cohort |
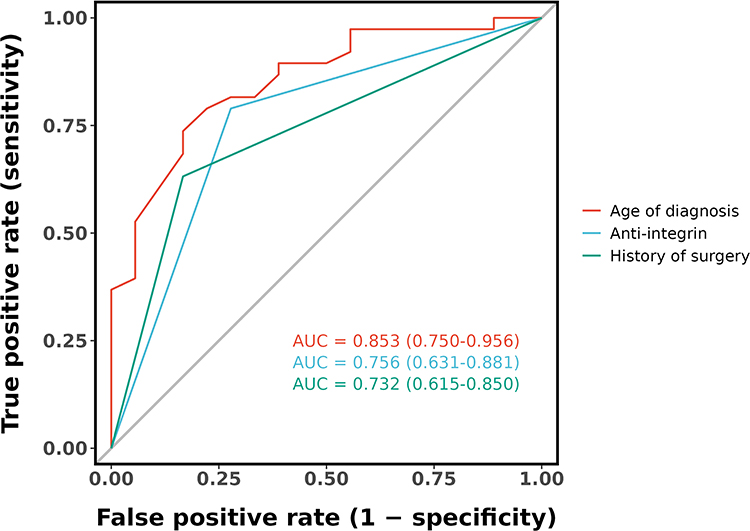 |
Figure 3 ROC curve and AUC of multivariate model. |
Patient Population
We evaluated the efficacy of UPA in 122 patients with UC or CD from both inpatient and outpatient settings. During the study period, 8 patients were excluded for failing to meet the definition of refractory IBD. Additionally, 1 patient was excluded due to being under 18 years of age. Furthermore, 23 patients were excluded due to incomplete baseline or follow-up data.Moreover, 2 patients were excluded for receiving concomitant biological agents (infliximab or vedolizumab) during upadacitinib therapy. Lastly, 10 patients were excluded for other reasons, culminating in a total of 80 eligible patients included in the study (52 CD and 28 UC). The overall process is illustrated in Figure 4.
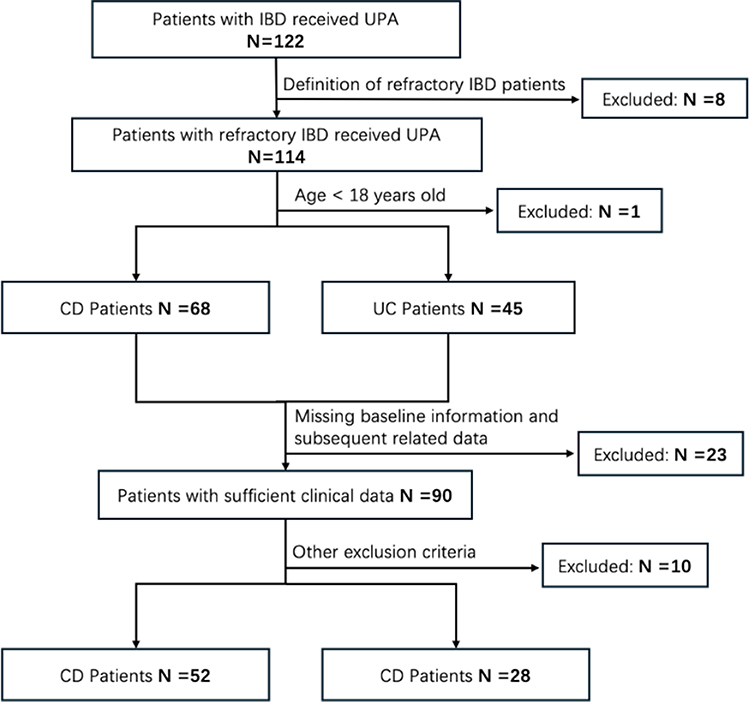 |
Figure 4 Patient selection flow chart. |
The median age of CD patients was 34 years (IQR: 29–41.8), with a median disease duration of 7 years (IQR: 5–10.8 years). The Montreal classification indicates that the age of disease onset was A1 in 17.3%, A2 in 61.5%, and A3 in 21.2%. Disease localization was observed as follows: ileal (L1) in 23.1%, colonic (L2) in 21.2%, ileocolonic (L3) in 51.9%, and upper gastrointestinal tract involvement in 3.8%. Disease behavior exhibited an inflammatory phenotype (B1) in 26.9% of cases, stricturing (B2) in 44.2%, penetrating (B3) in 28.8%, and perianal disease was observed in 71.2% of patients.
The average age of UC patients was 49.9 years (SD: 14.2), with a median disease duration of 6 years (IQR: 3–10 years). The disease location was categorized based on the Montreal classification: 42.9% exhibited E3 (extensive colitis), 35.7% demonstrated E2 (left-sided colitis), and 21.4% presented with E1 (proctitis). Other specific information is in Table 3.
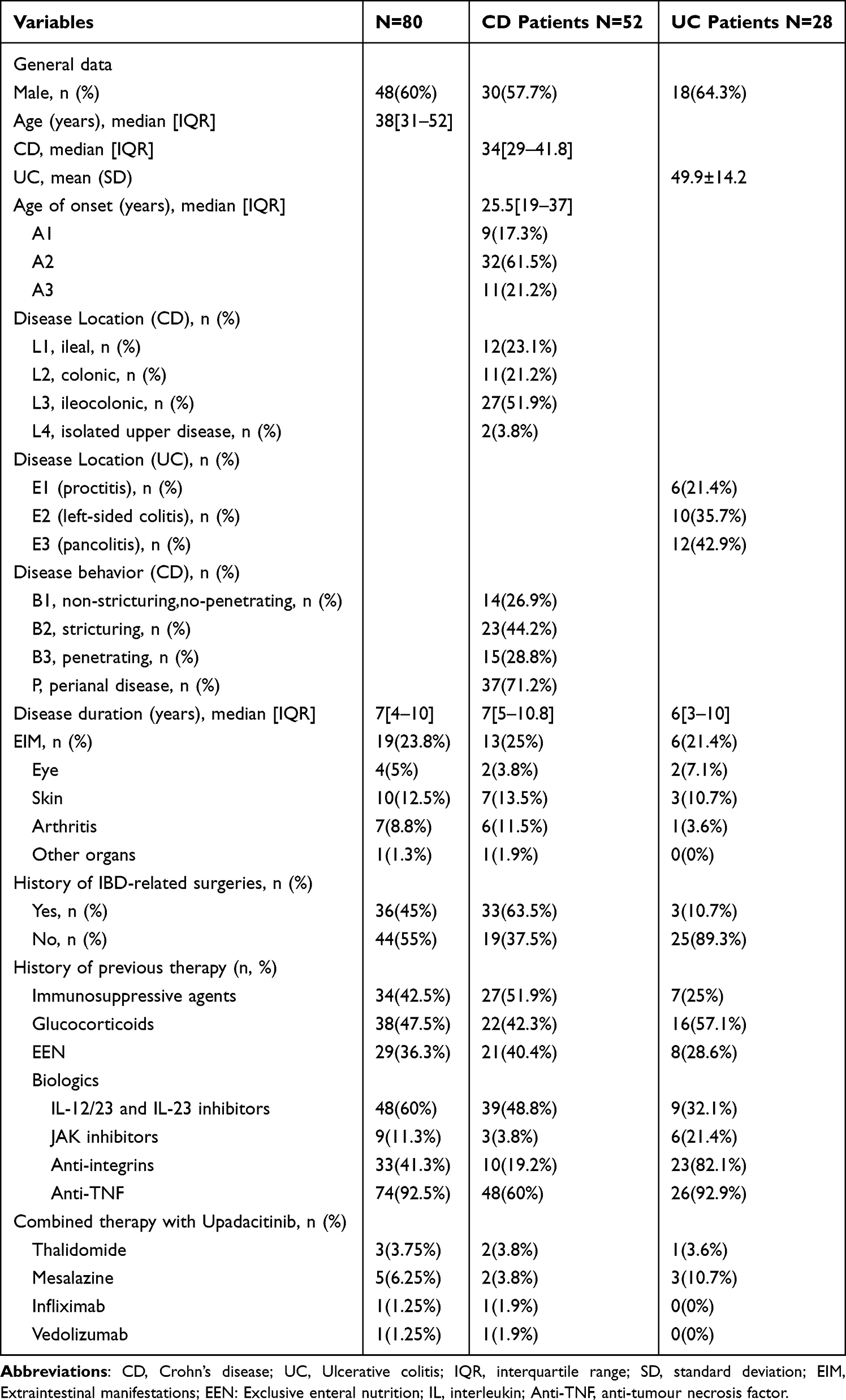 |
Table 3 Baseline Characteristics |
Combination therapy during upadacitinib treatment: Among 80 IBD patients, a total of 10 patients (6 CD, 4 UC) had combination therapy during upadacitinib treatment, including 3 patients with thalidomide, 5 patients with mesalamine, 1 patient with infliximab, and 1 patient with vedolizumab.
Clinical Outcomes and Subgroup Analysis
In patients with UC, the rates of steroid-free clinical remission at months 2, 6, and 12 were 67.9% (19/28), 78.6% (22/28), and 85.7% (24/28), respectively, while the clinical response rates were 71.4% (20/28), 78.6% (22/28), and 89.3% (25/28) (Figure 5A and B). The mean modified Mayo score significantly declined from 6.95 ± 1.78 at baseline to 1.18 ± 0.67 after 12 months of UPA treatment (p < 0.001). In patients with CD, the rates of steroid-free clinical remission at 3, 6, and 12 months were 59.6% (31/52), 73.1% (38/52), and 78.8% (41/52), respectively. The clinical response rates were 61.5% (32/52), 67.3% (35/52), and 75.0% (39/52) (Figure 5A and B). The mean HBI score dramatically lowered from 4.6 ± 1.6 at baseline to 2.0 ± 0.5 after 12 months of UPA treatment (p < 0.01). The steroid-free clinical remission rates at 2/3, 6, and 12 months were 62.5% (50/80), 75.0% (60/80), and 81.3% (65/80), respectively, while the overall clinical response rates were 65.0% (52/80), 71.3% (57/80), and 80.0% (64/80) (p = 0.001). Subgroup analysis revealed no significant difference in steroid-free clinical remission and response between patients with UC and CD (p > 0.05).
 |
Figure 5 (A) Clinical remission rates in UC and CD patients during the induction period and maintenance therapy. (B) Clinical response rates. (C) Endoscopic remission rates. (D) Endoscopic response rates. (E) CRP Normalization. (F) FC Normalization. |
Endoscopic Outcomes and Subgroup Analysis
Endoscopic findings indicated improvement in patients with both UC and CD. The endoscopic remission rates for UC patients following UPA treatment were 46.4% (13/28) at 2 months, 60.7% (17/28) at 6 months, and 78.6% (22/28) at 12 months (p = 0.020). The endoscopic response rates were 60.7% (17/28), 64.3% (18/28), and 78.6% (22/28) (p =0.166), respectively. (Figure 5C and D). The Mayo endoscopic subscore improved significantly from 4.0 ± 3.7 at baseline to 1.9 ± 1.1 after 12 months of UPA treatment. (p < 0.001). In patients with CD, the endoscopic remission rates following UPA treatment were 30.8% (16/52) at 3 months, 57.7% (30/52) at 6 months, and 75.0% (39/52) at 12 months (p <0.01). The endoscopic response rates were 57.7% (30/52), 67.3% (35/52), and 84.6% (44/52) (p =0.002). (Figure 5C and D). The median SES-CD decreased from 17 (7.1–13.0) to 2.6 (1.7–3.2) (p < 0.01). The endoscopic remission rate for IBD patients during the induction period was 36.3%, increasing to 58.8% at 6 months and 76.3% at 12 months. (p < 0.01). The endoscopic response rate during the induction period was 58.8%, increasing to 66.3% at 6 months and 82.5% at 12 months. (p =0.002). Sub-group analysis revealed no significant difference in endoscopic remission and response between patients with UC and those with CD (p>0.05).
Inflammatory Markers
Inflammatory markers demonstrated improvement, as evidenced by normal CRP levels and a consistent increase in normal FC rates among patients with UC and CD. In patients with UC, the normal CRP rates at baseline, 2, 6, 12, and 18 months were 28.6% (8/28), 46.4% (13/28), 60.7% (17/28), 67.9% (19/28), and 78.6% (22/28) (p<0.001). In patients with CD, the normal C-reactive protein (CRP) rates at baseline and 3, 6, 12, and 18 months were 40.4% (21/52), 57.7% (30/52), 59.6% (31/52), 69.2% (36/52), and 78.6% (41/52), respectively (p<0.001). The initial normal CRP rate was 36.3%, rising to 53.8% during the induction period and subsequently reaching 78.8% after 18 months of maintenance therapy. (Figure 5E).
In UC patients, the baseline normal FC rates at 2, 6, 12, and 18 months were 28.6% (8/28), 57.1% (16/28), 60.7% (17/28), 78.6% (22/28), and 82.1% (23/28), respectively (p<0.0001). In patients with CD, the normal FC rate at baseline, 3, 6, 12, and 18 months was 23.1% (12/52), 51.9% (27/52), 61.5% (32/52), 69.2% (36/52), and 92.3% (48/52) (p<0.0001). The baseline FC normal rate was 25%. Following induction therapy and 18 months of maintenance therapy, the rates increased to 53.8% and 88.8%, respectively. (Figure 5F). The baseline average level of FC was 834.6 µg/g, which decreased to 233.9 µg/g following induction therapy, and further declined to 187.1 µg/g after 18 months of maintenance therapy. (Figure 6A). Sub-group analysis revealed no significant difference in biochemical remission between patients with UC and those with CD (p>0.05). The baseline average CRP level was 5.3 mg/L, which decreased to 1.1 mg/L following induction therapy. The levels fluctuated and increased during subsequent maintenance therapy, yet remained within the normal range, reaching 3.0 mg/L at 18 months. (Figure 6B).
 |
Figure 6 (A) Baseline and post-treatment trends of total FC levels. (B) Baseline and post-treatment trends of total CRP levels. (C) Baseline and post-treatment trends of total ESR levels. (D) Baseline and post-treatment trends of total FC levels. (E) Baseline and post-treatment trends of total FC levels. |
The baseline average ESR level was 19.8 mm/h, which decreased to 10.3 mm/h following induction therapy. Despite fluctuations during subsequent treatment, the values consistently remained within the normal range, peaking at 11.3 mm/h at 18 months. (Figure 6C). Sub-group analysis revealed no significant difference in biochemical remission between patients with UC and those with CD (p>0.05).
Nutritional Status
The baseline mean 25(OH)VitD level was 40.3 nmol/L, which significantly increased to 46.6 nmol/L following UPA induction therapy. Although fluctuations occurred during maintenance therapy, the level reached 55.2 nmol/L at 18 months. (Figure 6D). The percentage of patients exhibiting normal levels of 25(OH)VitD increased from 77.5% (62/80) to 88.8% (71/80) (p=0.029).
Nutritional parameters, specifically 25(OH) Vitamin D and ALB, demonstrated significant overall improvement. The baseline average level of ALB was 41.1 g/L, increasing to 42.5 g/L and 44.2 g/L (p<0.0001) following the induction period and after 18 months of maintenance therapy, respectively. (Figure 6E). The percentage of patients exhibiting normal ALB increased from 75.0% (60/80) to 92.5% (74/80) (p=0.002).
Other Laboratory Parameters
In the 18-month follow-up, the baseline mean WBC was 6.5*109/L, decreasing to 6.1*109/L post-induction therapy (p=0.9461), and further declining to 4.9*109/L after 18 months of UPA treatment (p<0.0001). The baseline mean hemoglobin (HGB) was 122.4 g/L, decreasing to 119.3 g/L following induction therapy (p=0.9592), and further declining to 117.8 g/L after 18 months of UPA treatment (p=0.0005). The baseline mean PLT was 296.3 U/L, which decreased to 288.7 U/L following induction therapy (p>0.9999), and further declined to 233 U/L after 18 months of UPA treatment (p<0.0001). This suggests that UPA exerts long-term effects on the hematopoietic system. The baseline mean value of the liver function indicator ALT was 14.8 U/L, increasing to 18 U/L following induction therapy (p<0.0001), and subsequently decreasing to 16.5 U/L after 18 months of UPA maintenance therapy (p=0.7455). The baseline mean value of AST was 18.2 U/L, increasing to 23 U/L following induction therapy (p<0.0001), and was sustained at 24.4 U/L after 18 months of UPA maintenance therapy (p<0.0001).
Lipid indicators comprise the High-Density Lipoprotein (HDL) to Total Cholesterol (TC) ratio and Low-Density Lipoprotein Cholesterol (LDL-C). The baseline mean of HDL-C/TC was 0.3 mmol/L, increasing to 0.32 mmol/L following induction therapy (p=0.2290), and further rising to 0.38 mmol/L after 18 months of UPA maintenance therapy (p<0.0001). The baseline mean of LDL-C was 2.3 mmol/L, increasing to 2.4 mmol/L following induction therapy (p=0.6574), fluctuating to 2.6 mmol/L at the 6-month mark (p=0.0002), and subsequently decreasing to 2.3 mmol/L after 18 months of UPA maintenance therapy (p=0.9197). (Figure 7).
 |
Figure 7 Baseline and post-treatment trends of other laboratory outcomes. (A) WBC. (B) Hb. (C) PLT. (D) ALT. (E) AST. (F) HDL-C/TC. (G) LDL-C. |
Drug Safety Analysis
UPA was safe for refractory IBD patients throughout treatment. Adverse events occurred at 21.3% in CD and 14.3% in UC, totaling 20.0%. In UC, maintenance therapy discontinuation rates were 7.1% compared to 21.5% in CD, indicating better tolerability. (Figure 8). Acne (8.75%) was the most common adverse effect, followed by newly developed anemia (5.0%), neutropenia (3.75%), and infection (3.75%). In addition, the incidence of creatine kinase abnormalities and dyslipidemia was 1.25% and 11.25%, respectively. (Table 4). Most adverse effects were modest and did not stop treatment. No thromboembolic or malignant events occurred during the study. Subgroup analysis showed no significant differences in adverse event rates (p=0.355) or discontinuation rates (p=0.108) between UC and CD patients.
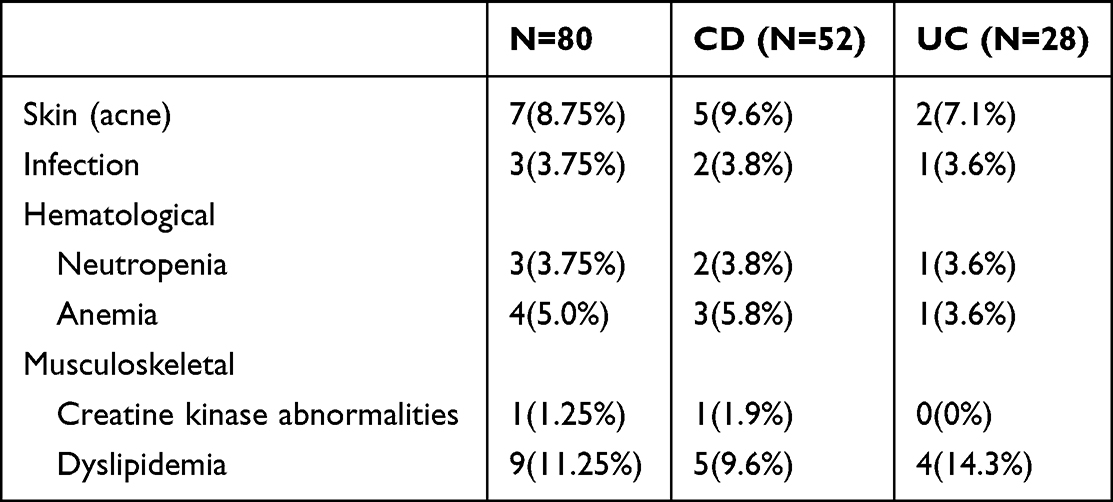 |
Table 4 Comparison of the Incidence of Adverse Event Types |
 |
Figure 8 Discontinuation rates and adverse events in UC and CD patients. |
Discussion
This real-world study demonstrates UPA’s effectiveness in achieving rapid and sustained remission in a therapy-refractory Asian IBD population with prior biologic failure. The steroid-free clinical remission rates (78.8% in CD, 85.0% in UC) and endoscopic remission rates (75.0% in CD, 78.6% in UC) at 12 months are numerically higher than those reported in pivotal trials of UPA and other biologics, these comparisons are indirect, confounded by differences in study design, patient selection, and outcome definitions, and should not be interpreted as evidence of superiority, potentially due to UPA’s high JAK1 selectivity.22
The endoscopic remission rate of 78.6% in refractory UC at 12 months in our cohort substantially exceeds the 30–40% rates observed in the U-ACHIEVE and U-ACCOMPLISH trials at week 8.30 The pronounced reduction in Mayo Endoscopic subscores corroborates UPA’s efficacy in promoting mucosal healing, consistent with Sandborn et al’s long-term findings.31 In CD, endoscopic remission rates increased from 30.8% post-induction to 75.0% during maintenance, paralleling outcomes from U-EXCEED/U-EXCEL but suggesting enhanced treatment persistence in Asian populations.27
It is worth noting that a recent multi-centre real-world study on pediatric Crohn’s Disease also indicated that upadacitinib achieved a clinical remission rate of 56% after 8 weeks of induction therapy in refractory children who had previously failed biological agents treatment, and the overall safety was acceptable.32 Several factors may contribute to these superior response rates: concomitant medication use in 10 IBD patients, maintenance therapy with 30 mg qd in 4 patients, and the relatively younger age of our cohort (only 9 patients >60 years). When contextualized with Western real-world evidence, our findings align with emerging data suggesting potentially enhanced UPA responsiveness in Asian populations, though direct cross-regional comparisons remain limited by demographic and treatment practice variations.Furthermore, genetic differences between Asian and Western IBD populations may contribute to these observed therapeutic variations. A systematic review and meta-analysis of IBD genetics in Asia revealed distinct susceptibility genes and mutations compared to Caucasians, including variations in NOD2, IL-23R, and TNF superfamily genes.33 A recent large-scale genetic study across ancestral populations further confirms that although the genetic effects of IBD are generally consistent, the genetic background of Crohn’s Disease is more ancestry-dependent than that of Ulcerative Colitis, which may lead to differences in treatment responses among different populations.34 These genetic disparities could influence disease behavior, treatment response, and safety profiles, underscoring the importance of region-specific real-world evidence.
The rapid onset of action observed has significant clinical implications, with 67.0% of UC patients achieving remission by week 8—surpassing tofacitinib’s 34% remission rate in the OCTAVE trials.35 This accelerated response aligns with Danese et al’s proposition that UPA’s JAK1 specificity expedites symptom control in biologically experienced patients.This result also resonates with a recent editorial perspective on the individualized selection of JAK inhibitors, which emphasizes that upadacitinib can be an effective second-line option in the treatment of ulcerative colitis, based on the patient’s refractory status and previous treatment history36. Similarly, the 3-month clinical remission rate in CD (59.6%) exceeded the 12-week outcomes with ustekinumab in IM-UNITI (35%),27 underscoring UPA’s efficacy in managing complex phenotypes including penetrating disease and perianal involvement.In addition, in a real-world head-to-head comparative study in Japan, upadacitinib showed a significantly higher clinical remission rate than nemolizumab and tofacitinib in patients with refractory ulcerative colitis who had previously received various biologics or other JAK inhibitors, demonstrating its advantages in multiple refractory patients.37
UPA significantly improved inflammatory biomarkers in refractory IBD patients. By week 8, 57.7% and 53.8% achieved complete biochemical remission, with sustained rates of 78% and 88.8% at 1.5 years, indicating durable anti-inflammatory activity. The prompt normalization of inflammatory markers suggests UPA’s targeted JAK1 inhibition may resolve mucosal inflammation more rapidly than biologic agents—a particular advantage for DTT-IBD patients who often exhibit persistent inflammation despite conventional therapy.
Nutritional parameters improved substantially following UPA initiation, with significant vitamin D elevation after induction therapy and increased albumin levels after 1.5 years of maintenance treatment. These improvements suggest UPA may confer metabolic benefits beyond direct inflammatory suppression, though the precise mechanisms warrant further investigation.
Safety monitoring revealed expected class effects of JAK inhibition. Hematologic analyses showed reductions in leukocyte and platelet counts with minimal hemoglobin impact, consistent with JAK inhibition’s myelosuppressive properties but within clinically acceptable ranges. The inhibition of JAK1/JAK2 may reduce myeloid differentiation and platelet integrin (GPIIb/IIIa) expression, potentially affecting fibrinogen binding.38 UPA metabolism via hepatic cytochrome P450 enzymes (CYP3A4 and partially CYP2D6) necessitates ongoing hepatic monitoring, though no significant hepatotoxicity was observed. Lipid metabolism alterations manifested as increased HDL-C/TC ratios without significant LDL-C changes during induction or maintenance therapy, possibly mediated through IL-6/JAK1-STAT3 pathway modulation or leptin signaling interference.39 Most parameter fluctuations were transient and clinically manageable.Importantly, similar to anti-TNF therapy, JAK inhibitors including UPA have been shown to impair immune responses to vaccines, leading to reduced formation of neutralizing antibodies. This may elevate the risk of vaccine-preventable infections during outbreaks of influenza, COVID-19, or other communicable diseases, a consideration particularly relevant for patients on long-term immunosuppression.40,41
The overall adverse event rate was 20%, lower than the 30–40% reported in global Phase III trials.35 Treatment discontinuation occurred in 4 UC (7.1%) and 8 CD (21.5%) patients due to inefficacy or surgery, with overall maintenance therapy discontinuation of 16.3%, indicating improved tolerability in UC patients. Notably, no thromboembolic events or malignancies occurred during the study—a reassuring finding given JAK inhibitor boxed warnings. Infection rates, including herpes zoster recurrence, aligned with previous reports but were comparatively lower in our Asian cohort, potentially reflecting stringent patient selection or ethnic variations in susceptibility.
Our study has several limitations. First, as a retrospective observational study, it carries the risk of selection bias and information bias. Second, the sample size is relatively small, especially for UC patients. Third, to ensure clarity in attributing efficacy to upadacitinib monotherapy, we excluded patients receiving concomitant biological agents, which may limit the generalizability of our findings to real-world settings where combination therapy is sometimes used. Fourth, although longer than most clinical trials, the follow-up period of 18 months may be insufficient to fully assess long-term safety. These limitations highlight the need for larger, prospective, long-term investigations to validate our findings.
Conclusion
This is the first multicenter real-world study from China evaluating upadacitinib in rigorously defined refractory IBD. In this retrospective cohort with limited sample size, UPA demonstrated encouraging effectiveness and a tolerable safety profile over 12–18 months. However, given the exploratory nature of the data, the absence of a control group, and the inherent biases of observational design, these findings do not support definitive conclusions regarding UPA’s comparative efficacy or long-term safety. The observed effect sizes, while numerically high, require confirmation in adequately powered, prospective, controlled studies. We propose a concrete framework for such validation. Until then, generalizability to broader refractory IBD populations should be considered cautiously.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
This study was approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang Chinese Medical University (Ethics Approval Number: 2025-KL-321-02).
Acknowledgment
This has been uploaded to Research Square as a preprint: Observation of the Efficacy and Safety of Upadacitinib for Refractory Inflammatory Bowel Disease: A Multicenter Real-World Study | Research Square.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no competing interests associated with this study.
References
1. Pfeffel F, Stiglbauer W, Depisch D, Oberhuber G, Raderer M, Scheithauer W. Coincidence of Crohn’s disease and a high-risk gastrointestinal stromal tumor of the terminal ileum. Digestion. 1999;60(4):363–19. doi:10.1159/000007684
2. Olendzki BC, Silverstein TD, Persuitte GM, Ma Y, Baldwin KR, Cave D. An anti-inflammatory diet as treatment for inflammatory bowel disease: a case series report. Nutr J. 2014;13(1):5. doi:10.1186/1475-2891-13-5
3. Bryant RV, Burger DC, Delo J, et al. Beyond endoscopic mucosal healing in UC: histological remission better predicts corticosteroid use and hospitalisation over 6 years of follow-up. Gut. 2016;65(3):408–414. doi:10.1136/gutjnl-2015-309598
4. Colombel J-F, Keir ME, Scherl A, et al. Discrepancies between patient-reported outcomes, and endoscopic and histological appearance in UC. Gut. 2017;66(12):2063–2068. doi:10.1136/gutjnl-2016-312307
5. Geyl S, Guillo L, Laurent V, D’Amico F, Danese S, Peyrin-Biroulet L. Transmural healing as a therapeutic goal in Crohn’s disease: a systematic review. Lancet Gastroenterol Hepatol. 2021;6(8):659–667. doi:10.1016/S2468-1253(21)00096-0
6. Peyrin-Biroulet L, Lémann M. Review article: remission rates achievable by current therapies for inflammatory bowel disease: review: remission rates in IBD. Aliment Pharmacol Ther. 2011;33(8):870–879. doi:10.1111/j.1365-2036.2011.04599.x
7. Sandborn WJ, Gasink C, Gao -L-L, et al. Ustekinumab induction and maintenance therapy in refractory Crohn’s disease. N Engl J Med. 2012;367(16):1519–1528. doi:10.1056/NEJMoa1203572
8. Ma C, Panaccione R, Xiao Y, et al. REMIT-UC: real-world effectiveness and safety of tofacitinib for moderate-to-severely active ulcerative colitis. Am J Gastroenterol. 2023;118(5):861–871. doi:10.14309/ajg.0000000000002129
9. Feagan BG, Rutgeerts P, Sands BE, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2013;369(8):699–710. doi:10.1056/NEJMoa1215734
10. Napolitano M, D’Amico F, Ragaini E, Peyrin-Biroulet L, Danese S. Evaluating upadacitinib in the treatment of moderate-to-severe active ulcerative colitis: design, development, and potential position in therapy. Drug Des Devel Ther. 2022;16:1897–1913. doi:10.2147/DDDT.S340459
11. Alipour O, Gualti A, Shao L, Zhang B. Systematic review and meta-analysis: real-world data rates of deep remission with anti-TNFα in inflammatory bowel disease. BMC Gastroenterol. 2021;21(1):312. doi:10.1186/s12876-021-01883-6
12. Johnson AM, Barsky M, Ahmed W, et al. The real-world effectiveness and safety of ustekinumab in the treatment of Crohn’s Disease: Results From The SUCCESS Consortium. Am J Gastroenterol. 2023;118(2):317–328. doi:10.14309/ajg.0000000000002047
13. Ferrante M, D’Haens G, Jairath V, et al. Efficacy and safety of mirikizumab in patients with moderately-to-severely active Crohn’s disease: a Phase 3, multicentre, randomised, double-blind, placebo-controlled and active-controlled, treat-through study. Lancet. 2024;404(10470):2423–2436. doi:10.1016/S0140-6736(24)01762-8
14. Dalal RS, Kallumkal G, Cabral HJ, Bachour S, Barnes EL, Allegretti JR. Clinical and endoscopic outcomes after upadacitinib induction for ulcerative colitis: a multicenter retrospective cohort study. Inflammat Bowel Dis. 2024;30(7):1207–1210. doi:10.1093/ibd/izad155
15. Honap S, Agorogianni A, Colwill MJ, et al. JAK inhibitors for inflammatory bowel disease: recent advances. Front Gastroenterol. 2024;15(1):59–69. doi:10.1136/flgastro-2023-102400
16. AlAmeel T, AlMutairdi A, Al-Bawardy B. Emerging therapies for ulcerative colitis: updates from recent clinical trials. Clin Exper Gastroenterol. 2023;16:147–167. doi:10.2147/CEG.S375969
17. Boland BS, Sandborn WJ, Chang JT. Update on Janus kinase antagonists in inflammatory bowel disease. Gastroenterol Clin North Am. 2014;43(3):603–617. doi:10.1016/j.gtc.2014.05.011
18. Irani M, Fan C, Glassner K, Abraham BP. Clinical evaluation of upadacitinib in the treatment of adults with moderately to severely active Ulcerative Colitis (UC): patient selection and reported outcomes. Clin Exper Gastroenterol. 2023;16:21–28. doi:10.2147/CEG.S367086
19. Zhang J, Li R, Chen L, et al. Effectiveness and safety of upadacitinib in acute severe ulcerative colitis patients from single Chinese IBD Center: a monocentric study. Clin Exp Med. 2024;24(1):233. doi:10.1007/s10238-024-01468-z
20. Lasa JS, Olivera PA, Danese S, Peyrin-Biroulet L. Efficacy and safety of biologics and small molecule drugs for patients with moderate-to-severe ulcerative colitis: a systematic review and network meta-analysis. Lancet Gastroenterol Hepatol. 2022;7(2):161–170. doi:10.1016/S2468-1253(21)00377-0
21. Loftus EV, Panés J, Lacerda AP, et al. Upadacitinib Induction and maintenance therapy for Crohn’s disease. New Engl J Med. 2023;388(21):1966–1980. doi:10.1056/NEJMoa2212728
22. Bonelli M, Kerschbaumer A, Kastrati K, et al. Selectivity, efficacy and safety of JAKinibs: new evidence for a still evolving story. Ann Rheumatic Dis. 2024;83(2):139–160. doi:10.1136/ard-2023-223850
23. Hsu NY, Nayar S, Gettler K, et al. NOX1 is essential for TNFα-induced intestinal epithelial ROS secretion and inhibits M cell signatures. Gut. 2023;72(4):654–662. doi:10.1136/gutjnl-2021-326305
24. Liu J, Wu Z, Liu Y, et al. ROS-responsive liposomes as an inhaled drug delivery nanoplatform for idiopathic pulmonary fibrosis treatment via Nrf2 signaling. J Nanobiotechnol. 2022;20(1):213. doi:10.1186/s12951-022-01435-4
25. Wan X, Zhang C, Lei P, et al. Precision therapeutics for inflammatory bowel disease: advancing ROS-responsive nanoparticles for targeted and multifunctional drug delivery. J Mat Chem B. 2025;13(10):3245–3269. doi:10.1039/d4tb02868f
26. Maaser C, Sturm A, Vavricka SR, et al. ECCO-ESGAR guideline for diagnostic assessment in IBD part 1: initial diagnosis, monitoring of known IBD, detection of complications. J Crohn’s Colitis. 2019;13:144–164. doi:10.1093/ecco-jcc/jjy113
27. Dickerson A, Huang JS, Bauman LE. Upadacitinib as salvage therapy in adolescents with acute severe ulcerative colitis refractory to conventional treatments. JPGN Rep. 2024;5(4):447–453. doi:10.1002/jpr3.12124
28. Daperno M, D’Haens G, Van Assche G, et al. Development and validation of a new, simplified endoscopic activity score for Crohn’s disease: the SES-CD. Gastrointest Endosc. 2004;60(4):505–512. doi:10.1016/s0016-5107(04)01878-4
29. Harvey RF, Bradshaw JM. A simple index of Crohn’s-disease activity. Lancet. 1980;1(8167):514. doi:10.1016/s0140-6736(80)92767-1
30. pencer EA, Bergstein S, Dolinger M, et al. Single-center experience with upadacitinib for adolescents with refractory inflammatory bowel disease. Inflammat Bowel Dis. 2024;30(11):2057–2063. doi:10.1093/ibd/izad300
31. Nakase H. Understanding the efficacy of individual Janus kinase inhibitors in the treatment of ulcerative colitis for future positioning in inflammatory bowel disease treatment. Immunol Med. 2023;46(3):121–130. doi:10.1080/25785826.2023.2195522
32. Cohen S, Spencer EA, Dolinger MT, et al. Upadacitinib for induction of remission in paediatric Crohn’s disease: an international multicentre retrospective stud. Aliment Pharmacol Ther. 2025;61(8):1372–1380. doi:10.1111/apt.70016
33. Ng SC, Tsoi KK, Kamm MA, et al. Genetics of inflammatory bowel disease in Asia: systematic review and meta-analysis. Inflammat Bowel Dis. 2012;18(6):1164–1176. doi:10.1002/ibd.21845
34. Liu Z, Liu R, Gao H, et al. Genetic architecture of the inflammatory bowel diseases across East Asian and European ancestries. Nature Genet. 2023;55(5):796–806. doi:10.1038/s41588-023-01384-0
35. Gilmore R, Tan WL, Fernandes R, An Y-K, Begun J. Upadacitinib salvage therapy for infliximab-experienced patients with acute severe ulcerative colitis. J Crohn’s Colitis. 2023;17(12):2033–2036. doi:10.1093/ecco-jcc/jjad115
36. Woelfel S, Brand S. Editorial: individualising JAK inhibitor selection for patients with ulcerative colitis. Aliment Pharmacol Ther. 2025;61(4):735–736. doi:10.1111/apt.18476
37. Akiyama S, Shimizu H, Tamura A, et al. Comparative efficacy and safety of three janus kinase inhibitors in ulcerative colitis: a real-world multicentre study in Japan. Aliment Pharmacol Ther. 2025;61(3):524–537. doi:10.1111/apt.18406
38. Dignass A, Esters P, Flauaus C. Upadacitinib in Crohn’s disease. Expert Opinion Pharmacother. 2024;25(4):359–370. doi:10.1080/14656566.2024.2333964
39. Wang S, Wang X, Ding J, et al. Disproportionality analysis of upadacitinib-related adverse events in inflammatory bowel disease using the FDA adverse event reporting system. Front Pharmacol. 2025;16:1436183. doi:10.3389/fphar.2025.1436183
40. Woelfel S, Dütschler J, Junker D, et al. Systemic and mucosal immunogenicity of monovalent XBB.1.5-adapted COVID-19 mRNA vaccines in patients with inflammatory bowel disease. Vaccines. 2024;12(7):774. doi:10.3390/vaccines12070774
41. Woelfel S, Dütschler J, Junker D, et al. XBB.1.5-adapted COVID-19 mRNA vaccines but not infections with previous omicron variants boost neutralisation against the SARS-CoV-2 JN.1 variant in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2025;61(2):299–312. doi:10.1111/apt.18349
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Biosimilars in Pediatric IBD: Updated Considerations for Disease Management
Dipasquale V, Cucinotta U, Romano C
Biologics: Targets and Therapy 2022, 16:57-66
Published Date: 13 June 2022
Atypical Forms of Pyoderma Gangrenosum in Inflammatory Bowel Disease: Report of Four Cases and Literature Review
Martinelli VF, Martinelli Barbosa P, Dantas de Oliveira LS, Melo LALV, Casa Nova JM, Brito CAA
International Medical Case Reports Journal 2022, 15:449-456
Published Date: 26 August 2022
A Review on Inflammatory Bowel Diseases: Recent Molecular Pathophysiology Advances
Abdulla M, Mohammed N
Biologics: Targets and Therapy 2022, 16:129-140
Published Date: 12 September 2022
The Association Between Inflammatory Bowel Disease and Exposure to Tobacco Smoking: A Case-Control Study in Qatar
Abdallah B, Arif M, Al-Malki M, Hourani R, Al-Maadeed T, Khodr N, Al-Kuwari G, Al-Siddiqi M, Kane T, Chivese T
International Journal of General Medicine 2023, 16:233-242
Published Date: 21 January 2023
Clinical Characteristics and Treatment of Middle-Aged and Elderly Patients with IBD in Shanghai, China
Mi L, Wang K, Yao J, Ma J, Chen YW, Zeng Q, Liu K
International Journal of General Medicine 2024, 17:6053-6064
Published Date: 11 December 2024