Back to Journals » Drug Design, Development and Therapy » Volume 20
Efficacy and Safety of PHPV Fusion Factor Vaginal Gel (PHPV®) in Clearing Cervical Persistent High-Risk Human Papillomavirus Infection: A Randomized Controlled Clinical Trial
Authors Yan L, Yin H, Shi L, Ding B, Liu C, Wang Y, Fu C ![]()
Received 13 June 2025
Accepted for publication 9 March 2026
Published 16 March 2026 Volume 2026:20 542859
DOI https://doi.org/10.2147/DDDT.S542859
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Lei Yan,1,2 Huan Yin,1,2 Liye Shi,1,2 Bingxue Ding,1,2 Chengniang Liu,1,2 Yong Wang,3 Chun Fu1,2
1Department of Obstetrics and Gynecology, The Second Xiangya Hospital of Central South University, Changsha, Hunan, People’s Republic of China; 2Clinical Research Center for Gynecological Disease in Hunan Province, Changsha, Hunan, People’s Republic of China; 3China Academy of BioMedicine, Shenzhen, Guangdong, People’s Republic of China
Correspondence: Chun Fu, Department of Obstetrics & Gynecology, The Second Xiangya Hospital, Central South University, Changsha, 410011, People’s Republic of China, Tel +8618627315906, Email [email protected]
Purpose: To evaluate the efficacy and safety of PHPV in the treatment of persistent high-risk papillomavirus (hrHPV) infection of the cervix.
Patients and Methods: A randomized controlled trial (RCT) was conducted on patients with persistent hrHPV infection which were randomly assigned in three groups: PHPV, interferon and control. All participants were followed up at baseline, 3 months and 6 months after enrollment. The primary outcome was hrHPV clearance at 6 months post-enrollment. Secondary outcomes included effective rate, HPV E6/E7 mRNA negativity, changes in vaginal microecology and safety. The primary analysis was conducted on the modified intention-to-treat (mITT) population.
Results: Of 842 patients screened, 120 were randomly assigned to three groups and 110 were included in the mITT analyses. At 3 months, hrHPV clearance rates were higher in both the PHPV and interferon groups compared with the control group. However, after covariate adjustment, the superiority over no treatment remained robust for PHPV, whereas the interferon vs control comparison showed attenuation. At 6 months, hrHPV clearance was 66.7% in the PHPV group, 45.9% in the interferon group, and 20.6% in the control group. Adjusted analyses showed that PHPV was significantly superior to no treatment (RR 2.81, 95% CI 1.37– 5.79, P=0.005), whereas the interferon vs control comparison did not reach statistical significance (RR 2.08, 95% CI 0.98– 4.44, P=0.058). Similar patterns were observed for effective rate and HPV E6/E7 mRNA negativity, with PHPV demonstrating consistent superiority over no treatment after adjustment. Comparisons between PHPV and interferon did not reach statistical significance for clearance outcomes, although PHPV showed numerically higher efficacy. No serious adverse events were reported.
Conclusion: PHPV is an effective and safe non-invasive therapeutic option for persistent hrHPV infection.
Clinical Trial Registration: www.chictr.org.cn, ChiCTR2200063608.
Keywords: high-risk human papillomavirus, persistent infection, PHPV fusion factor, treatment, clinical trial
Introduction
Human papillomavirus (HPV) infection is the most prevalent sexually transmitted disease, with more than 10% of women infected with HPV in China.1 Statistically, HPV infection rates in the reproductive tract exceed 80% in sexually active women.2,3 Although most HPV infections cleared within 1–2 years, approximately 10% of high-risk HPV (hrHPV) infections persist,4–6 increasing the risk of cervical intraepithelial neoplasia (CIN) and invasive cervical cancer.7,8
Current preventive and therapeutic strategies, including physical therapy, surgical intervention, immunotherapy, and prophylactic vaccines, have limitations. Cervical conization is effective in eradicating CIN lesions and associated HPV infections, but residual or recurrent lesions occur in 7%–25% of cases.9,10 Antiviral or immunomodulatory agents, including interferon-based therapies, have demonstrated limited efficacy and tolerability.11–13 Prophylactic vaccines exhibit high efficacy in preventing HPV infection but have low adherence rates, and limited utility in individuals already infected.14–16 Therefore, effective therapeutic interventions to eliminate persistent hrHPV infection are urgently needed.
In recent years, biologic and topical antiviral therapies have shown great potential as non-invasive treatments for HPV infection. PHPV Fusion Factor Vaginal Gel (PHPV®) is an innovative biologic to treat HPV infection developed by Guangxi Fulaiming Biopharmaceutical. Its active component, a recombinant lactoferricin fusion protein, can bind to viral particles and inhibit their attachment to host cells. It also competes with cell surface receptors (such as heparan sulfate proteoglycans) to prevent hrHPV from attaching to and entering epithelial cells, thereby suppressing HPV replication, reducing viral load, promoting viral clearance, and preventing cervical lesions. Additional components, such as carbomer, glycerin, green tea extract,17 and triclosan (present at a very low concentration), enhance its therapeutic effects.
This study investigated the therapeutic efficacy and safety of PHPV for managing persistent hrHPV infections through clinical trials.
Material and Methods
PHPV Fusion Factor and PHPV Gel
The PHPV fusion factor is synthetic construct consisting of cell-penetrating peptide, antiviral peptide, and tissue repair peptide (Supplementary Figure S1) with the code FLM-1.x. The sequence information is registered in the NCBI GenBank (OR713750.1 and WOZ30154.1). Both the PHPV fusion factor and PHPV gel were supplied by Guangxi Fulaiming Biopharmaceutical.
Ethics
The study protocol was approved by the the Ethics Committee of the Second Xiangya Hospital of Central South University (approval number: LYG2021078), and registered in the Chinese Clinical Trial Registry website (www.chictr.org.cn, ChiCTR2200063608) on September 13, 2022. The study was conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT 2010) Guidelines18 and the principles of the Declaration of Helsinki. Written informed consent was obtained from each participant prior to the commencement of the study.
Clinical Study Design
A total of 120 gynecological outpatients were enrolled. Inclusion criteria were: (1) women aged 25–45 with an intact uterus; (2) history of persistent hrHPV infection, defined as the same-type HPV persisting >1 year.19 (3) positive hrHPV typing and HPV E6/E7 mRNA tests within 1 month; and (4) no history of drug allergies.
Exclusion criteria included: (1) pregnancy or lactation; (2) systemic or local treatment for cervical atypia or HPV infection within 3 months; (3) acute reproductive tract infections; (4) cervical cancer or high-grade lesions; (5) severe systemic illness; (6) antibiotic use within 3 months; (7) inability to cooperate; and (8) deemed unsuitable by the researchers, such as communication difficulties.
Randomization and Allocation Concealment
Participants were randomly assigned (1:1:1) using a computer-generated randomization scheme to one of three groups: PHPV, interferon, or control (no treatment). The randomization process was generated by an independent statistician who was not involved in participant recruitment or data analysis. Allocation concealment was maintained using sequentially numbered, opaque, sealed envelopes, which were opened only after the participant’s enrollment. This approach followed a simple randomization method, ensuring strict concealment and minimizing the risk of selection bias.
Due to the nature of the interventions, blinding of participants and treating clinicians was not feasible. However, outcome assessors and statisticians were blinded to treatment allocation. Laboratory personnel responsible for vaginal microecology assessment, HPV testing, and cytology evaluation were unaware of group assignments to minimize potential detection bias.
Interventions
The PHPV group received PHPV vaginal gel (3g/tube, Gui-MPA: 20202180247), applied every other day except during menstruation, for 3 months. The instructions for use were as follows: The package was opened, and the injector was removed. The protective cover was then taken off, and the protective tube was detached. With the patient lying on her back, the injector was carefully inserted into the vagina, reaching the deep cervix in the posterior vaginal fornix. The protective tube was used as a booster rod to facilitate the injection of the gel onto the cervix surface.
The interferon group received Xinfuning® (recombinant human interferon α-2b vaginal capsules, 80 IU/capsule, Shanghai Huaxin Biotech, NMPA: S20050075) with the same regimen. The instructions for use were as follows: After washing the vulva, the participant was instructed to lie on her back and slowly place the effervescent capsule into the posterior vaginal fornix. The participant was then advised to remain lying down for 30 minutes to allow for proper absorption.
The control group received no specific treatment. All three groups were advised to maintain a healthy lifestyle, including moderate exercise and avoiding smoking, alcohol consumption, and staying up late.
Data Collection and Follow-Up
Participants underwent vaginal microecology testing, cervical cytology examination, HPV detection, and HPV E6/E7 mRNA testing at 3 and 6 months post-enrollment. The researchers recorded patients’ baseline demographic data, treatment experiences, and adverse events using case report forms (CRFs). Abstinence was recommended during treatment, and contraception was advised during follow-up.
To facilitate regular follow-up and emergency response, the researchers provided participants with contact information. Weekly contact via WeChat was made to assess their medication usage (treatment use, adverse events, and any missed doses), sexual activity, lifestyle, and adherence. Adherence was further verified based on the consistency between follow-up attendance and self-reported treatment records.As the study drug was self-administered intravaginally at home, used gel tubes were not collected for privacy and hygiene reasons.
Test Methods
Vaginal Microecology
Vaginal microecological testing included both morphological testing and functional assessment.20 Morphological indicators evaluated bacterial density, diversity, dominant bacteria, pathogenic microorganisms, and disease scores. Functional testing assessed microbial metabolic products and enzyme activities, providing a comprehensive evaluation of vaginal microecology.
Samples were collected from the posterior vaginal fornix using sterile swabs after positioning the patient in the lithotomy position and exposing the cervix with a speculum. Samples were transported to the laboratory within 10 minutes of collection.
Vaginal microecology was analyzed using Gram-stained smears and scored according to the standardized Nugent scoring system (scores 0–3: normal; 4–6: intermediate; 7–10: bacterial vaginosis). All laboratory analyses were conducted in the same certified clinical laboratory by trained technicians blinded to group allocation. Quality control procedures were performed weekly, and inter-observer consistency was verified by duplicate assessment of 10% of randomly selected samples, yielding a Cohen’s kappa coefficient greater than 0.85.
Cervical Cytology Examination
Cervical cytology was assessed using the ThinPrep® Cytologic Test (TCT, Hologic, Marlborough, MA, USA). Results were reported according to the Bethesda System (TBS) for cervical cytology (2014).21
HPV Detection
HPV was detected using the Sansure PCR HPV test (Sansure, Hunan, China), which employs a PCR-based One-Step Fast Release technology to detect 23 HPV types, including 18 high-risk types (16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, 82) and 5 low-risk types (6, 11, 42, 43, 81). A cycle threshold (CT) value ≤30 was defined as positive, and CT>30 as negative for HPV subtype detection.
HPV E6/E7 mRNA
The APTIMA HPV assay (Hologic, Marlborough, MA, USA) was employed to detect HPV E6/E7 mRNA from 14 high-risk types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68) in Cytyc PreservCyt liquid-based cytology specimens.22
Outcomes
The primary outcome was the hrHPV clearance rate at 6 months post-enrollment. Therapy efficacy was categorized as follows: (1) Complete clearance: all HPV subtypes and HPV E6/E7 mRNA negative; (2) Effective: HPV E6/E7 mRNA or at least one HPV subtype negative; (3) Invalid: neither criterion was met.
Secondary outcomes were the clearance rate of cervical persistent hrHPV infection at 3 months, the negative rate of HPV E6/E7 mRNA at 3 and 6 months, the decreased rate of HPV viral load, the improved condition of cervical appearance (eg., cervical erosion) and cytological status (TCT), the change of vaginal microecology, and serious adverse events such as alterations in vaginal discharge (color, odor, or amount), vaginal itching or burning, dysuria, postcoital bleeding, dyspareunia and pelvic pain.
The safety population was formally defined as all randomized participants after randomization. Adverse events (AEs) were recorded throughout the study period and classified by severity (mild, moderate, or severe) and by their relationship to the study intervention (related, possibly related, or unrelated).
Sample Size and Power
The sample size was determined for the primary outcome of hrHPV clearance at 6 months. Published evidence suggests an hrHPV clearance rate of approximately 60% with intravaginal interferon after 6 months,11,12 whereas untreated hrHPV infection clears at roughly 20%.13,23 Assuming PHPV would demonstrate superior efficacy with a clearance rate over 60%, a total of 89 participants would need to be recruited to achieve 90% statistical power at a 5% significance level. Considering a 10% dropout rate and 10% loss to follow-up rate, at least 37 participants per group were recruited. The trial included two primary comparisons (PHPV vs control and interferon vs control) and used the Bonferroni-Holm adjustment to control for multiple comparisons. The PHPV vs interferon comparison was considered exploratory with no α allocation.
Statistical Analysis
The outcomes were analyzed using generalized linear models (GLMs), with the treatment arm as the primary study variable. Risk ratios (RRs) and 95% confidence intervals (CIs) were calculated for comparisons.
For binary outcomes, GLMs with a log link were used to estimate RRs. Covariate-adjusted RRs were estimated using modified Poisson regression with robust variance estimation. Model convergence was assessed using standard diagnostic criteria, including successful model fitting and numerical stability of parameter estimates.
Both unadjusted and covariate-adjusted analyses were performed for the primary outcome and key secondary outcomes. Analyses were conducted based on the modified intention-to-treat (mITT) population. Baseline balance was assessed using standardized mean differences (SMDs) comparing the PHPV and control groups. Covariates were prespecified for adjustment based on baseline imbalance (SMD≥0.10) and clinical relevance.
Two prespecified primary confirmatory comparisons (PHPV vs control and interferon vs control) were evaluated. To account for multiplicity across these primary comparisons, the Bonferroni–Holm procedure was applied. Reported P values are unadjusted, and statistical significance for the primary comparisons was determined according to the Holm-adjusted decision rule. Secondary outcomes were analyzed as exploratory outcomes, and no formal multiplicity adjustment was applied.
Sensitivity analyses were performed in the ITT population under a conservative assumption that missing primary outcome data were classified as “not cleared”, using the same modeling framework as the primary analysis.
All statistical analyses were performed using SPSS (version 26.0, IBM, Armonk, NY, USA) and GraphPad Prism (version 8.0, La Jolla, CA, USA). A two-sided P value <0.05 was considered statistically significant unless otherwise specified by the multiplicity adjustment.
Results
Demographic and Clinical Description
Of the 842 women assessed for eligibility, 120 (14.3%) were enrolled, with 110 (91.7%) completing the study and included in the final analysis (Figure 1). At 3-month follow-up, outcome data were missing for 1 participant in the PHPV group, 3 in the interferon group, and 4 in the control group; at 6 months, missing data occurred in 1 (PHPV), 3 (interferon), and 6 (control) participants, respectively. Participants were allocated into three groups: PHPV (39 patients), interferon (37 patients), and control (34 patients). The primary reason for non-enrollment was refusal to participate (252, 34.9%), predominantly due to concerns about being assigned to the control group.
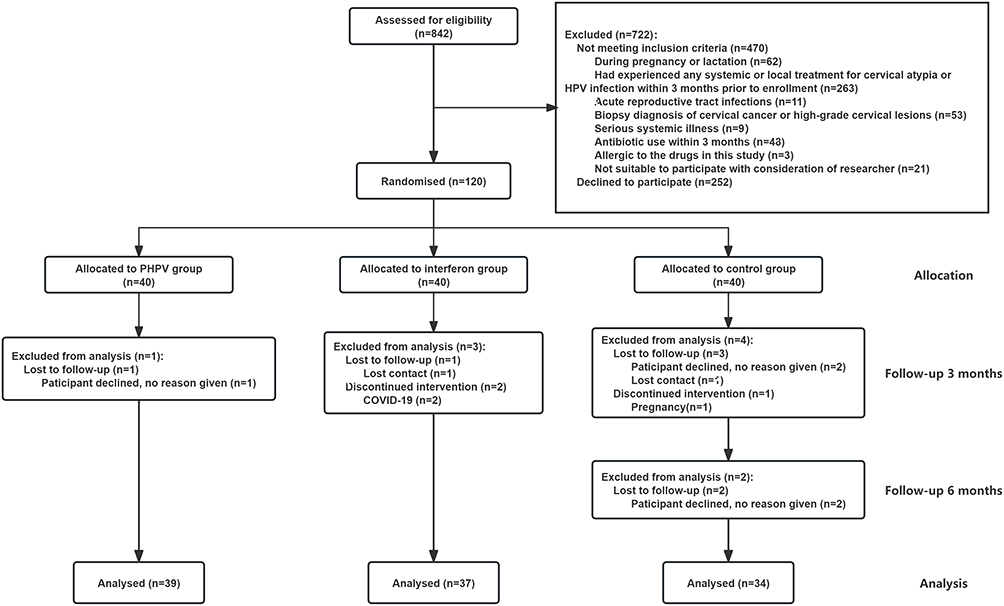 |
Figure 1 The flow diagram of clinical trial. |
Baseline demographic and clinical characteristics were generally comparable across the three study groups (Table 1). Baseline balance between the PHPV and control groups was assessed using SMDs. Covariates were prespecified for adjustment based on a combination of baseline imbalance (SMD≥0.10) and clinical relevance. Accordingly, age, residence, contraceptive method, and baseline TCT results were included in the adjusted models.
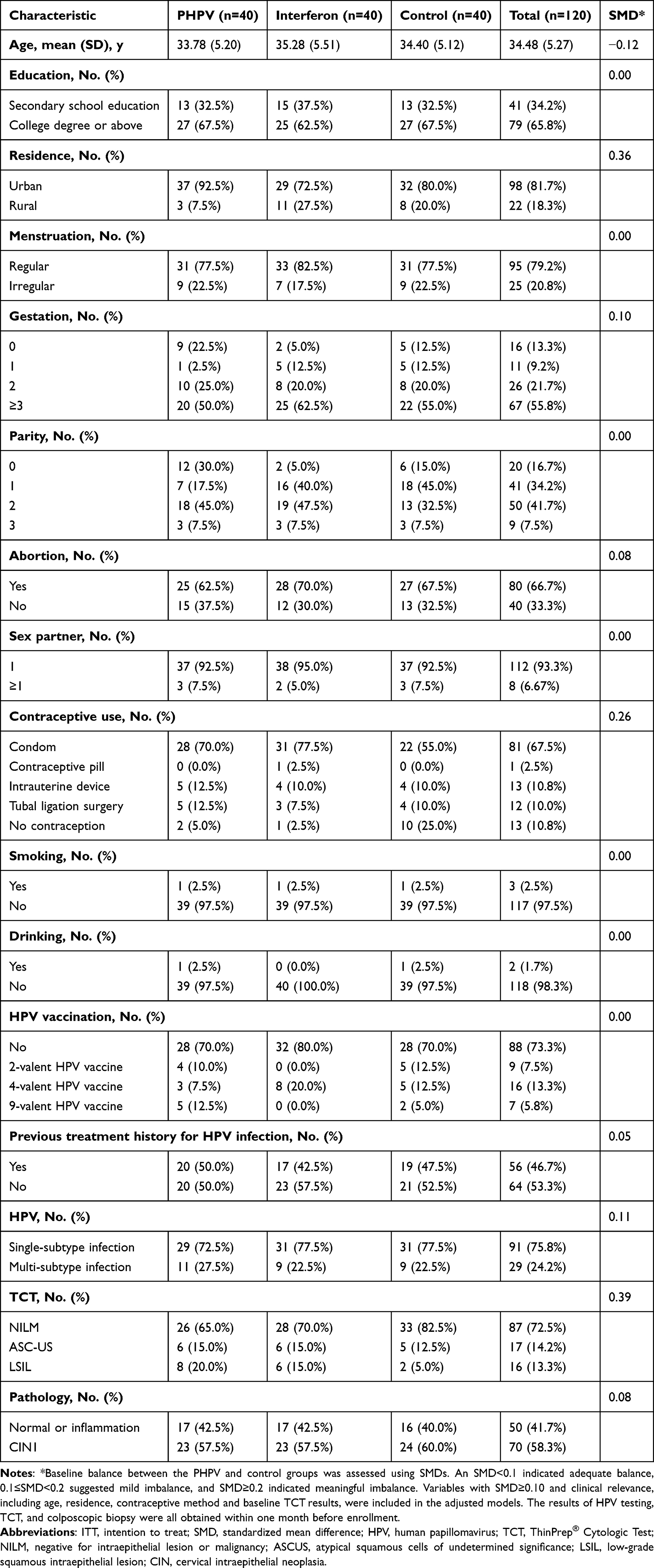 |
Table 1 Baseline Characteristics of Trial Participants |
PHPV Treatment Effectiveness in Clearing Persistent hrHPV Infection
At 3 months post-enrollment, the hrHPV clearance rates were 53.8% (21/39) in the PHPV group, 37.8% (14/37) in the interferon group and 5.6% (2/36) in the control group (Table 2). In unadjusted analyses, both PHPV and interferon demonstrated significantly higher clearance than no treatment (PHPV vs control: RR 9.69, 95% CI 2.44–38.44, P<0.001; interferon vs control: RR 6.81, 95% CI 1.67–27.86, P=0.001). After adjustment for prespecified baseline covariates, PHPV remained significantly superior to no treatment (RR 9.89, 95% CI 2.27–43.17, P=0.002), and the interferon vs control comparison remained statistically significant, although with a reduced magnitude of effect (RR 6.70, 95% CI 1.66–26.98, P=0.008). No significant difference was observed between PHPV and interferon (unadjustment: RR 1.42, 95% CI 0.86–2.36, P=0.162; after adjustment: RR 1.28, 95% CI 0.77–2.14, P=0.340).
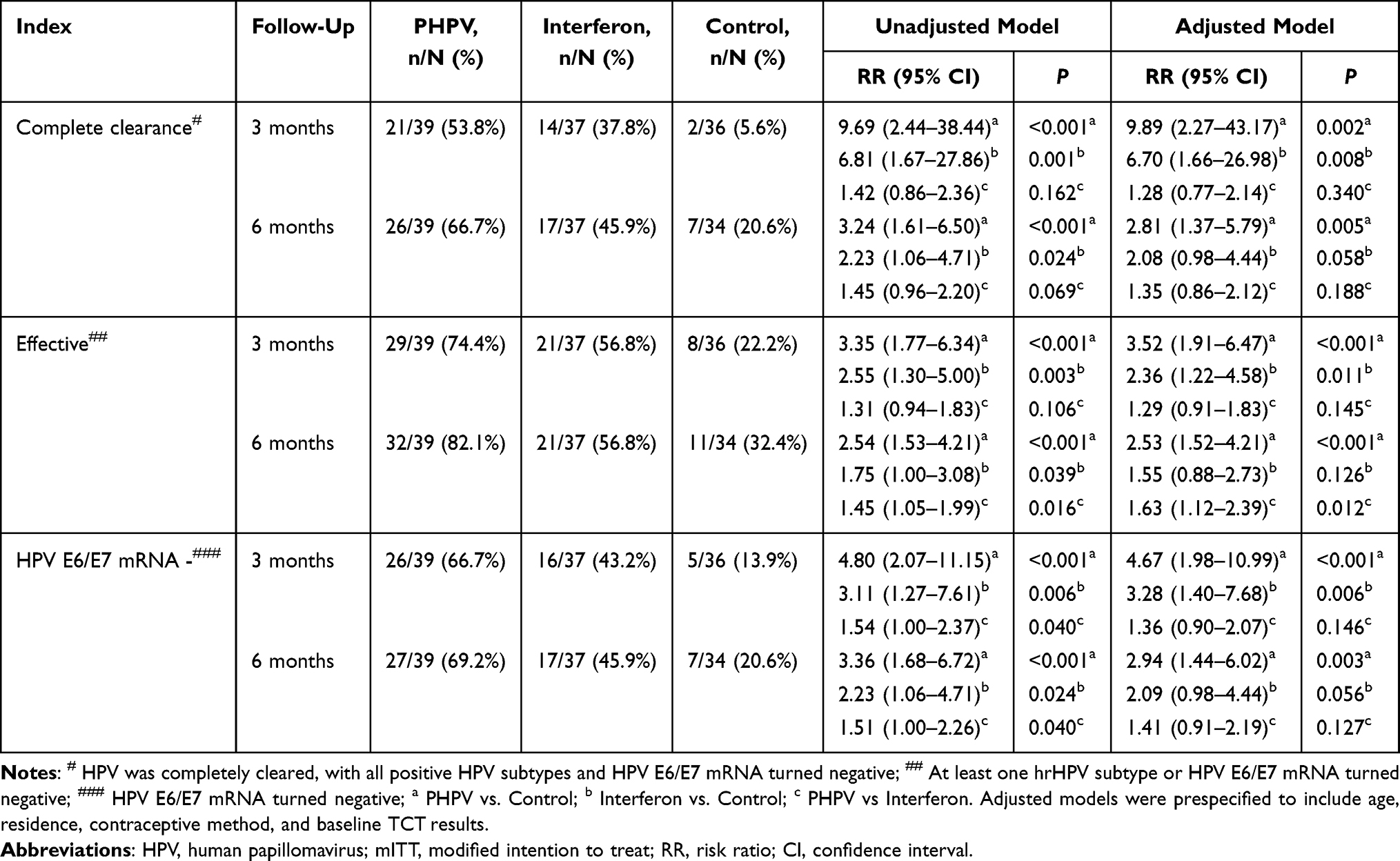 |
Table 2 Efficacy of PHPV in Clearing Cervical Persistent hrHPV Infection (mITT Population, n=110) |
At 6 months, hrHPV clearance rates increased to 66.7% (26/39) in the PHPV group, 45.9% (17/37) in the interferon group, and 20.6% (7/34) in the control group (Table 2). In unadjusted analyses, both PHPV and interferon showed higher clearance compared with the control group (PHPV vs control: RR 3.24, 95% CI 1.61–6.50, P<0.001; interferon vs control: RR 2.23, 95% CI 1.06–4.71, P=0.024). After covariate adjustment, PHPV remained significantly superior to no treatment (RR 2.81, 95% CI 1.37–5.79, P=0.005), whereas the interferon vs control comparison was attenuated and did not reach statistical significance (RR 2.08, 95% CI 0.98–4.44, P=0.058). The comparison between PHPV and interferon did not demonstrate statistical significance (unadjustment: RR 1.45, 95% CI 0.96–2.20, P=0.069; after adjustment: RR 1.35, 95% CI 0.86–2.12, P=0.188).
Absolute treatment effects at 6 months were further quantified using absolute risk differences (ARDs) and the corresponding number needed to treat (NNT) (Supplementary Table S1). Compared with the control group, PHPV demonstrated an ARD of 46.1% (95% CI: 26.0%-66.2%), corresponding to an NNT of 2.2. Interferon demonstrated an ARD of 25.4% (95% CI 4.3%-46.4%; NNT 3.9). When PHPV was compared directly with interferon, the ARD was 20.7% (95% CI: −1.1%-42.6%), with the 95% CI including zero, indicating uncertainty in the magnitude of this difference.
Treatment effectiveness, defined as HPV E6/E7 mRNA or at least one hrHPV subtype becoming negative, showed similar patterns. At 3 months, effective rates were higher in both treatment groups compared with the control group (PHPV vs control: RR 3.35, 95% CI 1.77–6.34, P<0.001; interferon vs control: RR 2.55, 95% CI 1.30–5.00, P=0.003). After adjustment, PHPV remained significantly superior to no treatment (RR 3.52, 95% CI 1.91–6.47, P<0.001), while interferon also remained statistically superior (RR 2.36, 95% CI 1.22–4.58, P=0.011). At 6 months, effective rates were 82.1% (32/39) for PHPV, 56.8% (21/37) for interferon, and 32.4% (11/34) for the control (PHPV vs control: RR 2.54, 95% CI 1.53–4.21, P<0.001; interferon vs control: RR 1.75, 95% CI 1.00–3.08, P=0.039; PHPV vs interferon: RR 1.45, 95% CI 1.05–1.99, P=0.016). Adjusted analyses demonstrated that PHPV remained significantly superior to no treatment (RR 2.53, 95% CI 1.52–4.21, P<0.001), whereas the interferon vs control comparison did not remain statistically significant after adjustment (RR 1.55, 95% CI 0.88–2.73, P=0.126). PHPV showed significantly higher effective rates than interferon after adjustment (RR 1.63, 95% CI 1.12–2.39, P=0.012).
Both unadjusted and covariate-adjusted treatment effect estimates are presented in Table 2. The treatment effects across the primary and key secondary outcomes are summarized in a forest plot (Figure 2). Overall, adjusted analyses consistently supported the superiority of PHPV over no treatment across outcomes, whereas interferon vs control comparisons were less stable after covariate adjustment. Comparisons between PHPV and interferon did not demonstrate statistically significant differences for clearance outcomes.
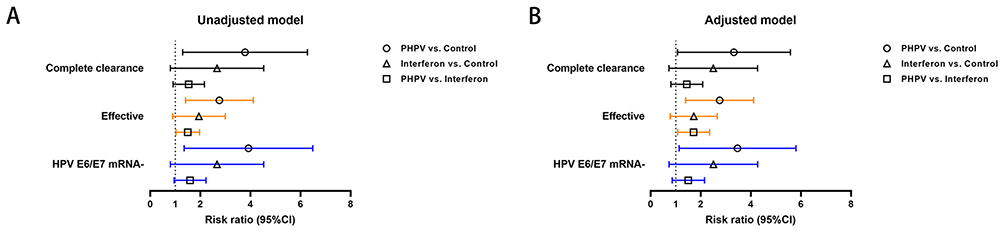 |
Figure 2 Forest plot summarizing treatment effects. The forest plots presents unadjusted (A) and covariate-adjusted (B) RRs with 95% CIs for the primary outcome (hrHPV complete clearance at 6 months) and selected key secondary outcomes (effective rate and HPV E6/E7 mRNA negativity at 6 months). Estimates were derived from GLM in the mITT population. Covariate-adjusted models included age, residence, contraceptive method, and baseline TCT results. The forest plots are intended as descriptive summaries of treatment effect patterns and do not introduce inferential claims beyond those presented in the main analyses. |
Sensitivity Analysis
In the sensitivity analysis, aligned with the prespecified primary estimand based on the ITT population (n=120), we applied a conservative assumption that all participants with missing hrHPV clearance outcomes at 3 and 6 months were classified as “not cleared”. The same covariate-adjusted modeling framework as the primary mITT analysis was applied. Under this approach, PHPV continued to demonstrate significantly higher hrHPV clearance and effective rates compared with the control group (Supplementary Table S2).
When compared with interferon, PHPV showed numerically higher hrHPV clearance and effective rates; however, these differences did not reach statistical significance in the adjusted sensitivity analyses.
PHPV Treatment Suppresses the HPV E6 and E7 Expression
At 3 months post-enrollment, 66.7% (26/39) of patients in the PHPV group, 43.2% (16/37) in the interferon group, and 13.9% (5/36) in the control group tested negative for HPV E6/E7 mRNA (Table 2). At 6 months, the corresponding rates were 69.2% (27/39), 45.9% (17/37), and 20.6% (7/34), respectively.
In unadjusted analyses, both PHPV and interferon demonstrated significantly higher HPV E6/E7 mRNA negativity compared with the control group. After adjustment for prespecified baseline covariates, PHPV remained significantly superior to no treatment at both time points (3 months: RR 4.67, 95% CI 1.98–10.99, P<0.001; 6 months: RR 2.94, 95% CI 1.44–6.02, P=0.003), whereas the interferon vs control comparison was attenuated at 6 months and did not reach statistical significance (3 months: RR 3.28, 95% CI 1.40–7.68, P=0.006; 6 months: RR 2.09, 95% CI 0.98–4.44, P=0.056). Comparisons between PHPV and interferon did not demonstrate statistically significant differences after adjustment.
Exploratory Western blot analysis showed reduced expression of HPV E6/E7 proteins following PHPV treatment (Supplementary Figure S2).
Together, these findings suggested that PHPV treatment is associated with suppression of HPV E6/E7 expression, providing supportive biological evidence consistent with its observed therapeutic effects.
Additional Exploratory Findings of PHPV Treatment in hrHPV Infection
PHPV treatment significantly reduced HPV viral load in 82.1% of participants, compared to 70.3% in the interferon group and 44.1% in the control group (RR 1.86, 95% CI 1.24–2.79, P=0.001, PHPV vs control; RR 1.59, 95% CI 1.03–2.46, P=0.026, interferon vs control; RR 1.17, 95% CI 0.90–1.51, P=0.227, PHPV vs interferon; Supplementary Table S3). However, no significant improvements were observed in cervical appearance or TCT outcomes.
Exploratory analyses further suggested a potential influence of PHPV on vaginal microecology. After 3 months of treatment, the normal/abnormal ratio of vaginal microecology increased 3.94-fold (from 8/27 to 21/18, P=0.007), with enhanced bacterial community diversity observed 6 months post-treatment (P=0.003; Supplementary Table S4).
In addition, an exploratory observation was made in a small subset of five participants who had failed a single course of interferon therapy. Following subsequent PHPV treatment, three of these participants achieved hrHPV negativity (Supplementary Table S5).
Taken together, these exploratory findings indicate that PHPV treatment is associated with favorable changes in HPV viral load and vaginal microbiota, providing supportive biological evidence consistent with the observed clinical effects.
Adverse Reactions
Safety analyses were conducted in the predefined safety population (Table 3). Only two participants in the interferon group experienced AEs, both reporting mild vaginal pruritus.No AEs were reported in the PHPV or control groups. All reported AEs were mild and transient, and were judged to be possibly related to the study intervention. No moderate or severe AEs were observed during the study period.
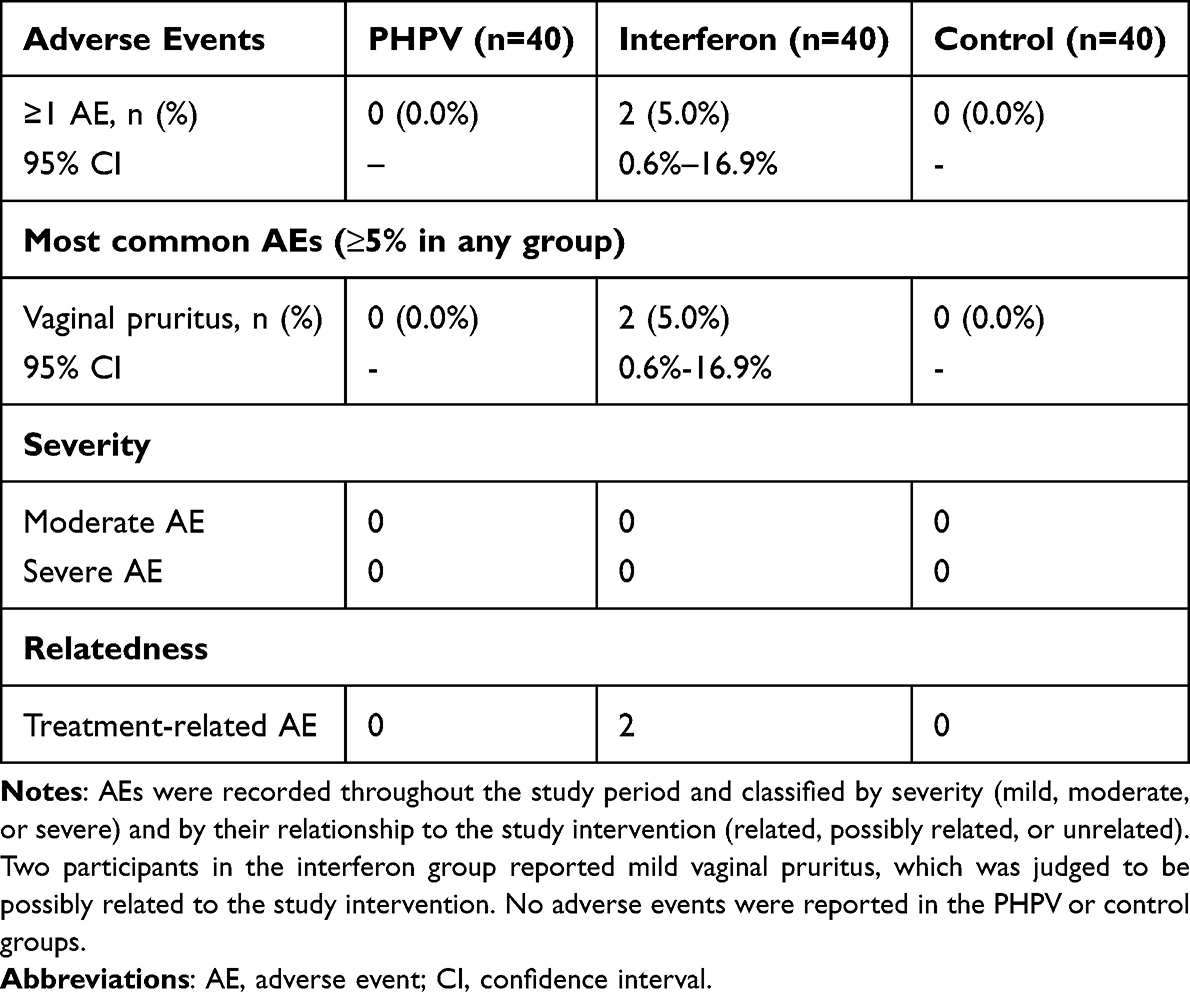 |
Table 3 Summary of Adverse Events by Treatment Group |
Discussion
This study provides clinical evidence supporting the efficacy and safety of PHPV in the management of persistent hrHPV infection. Compared with no treatment, PHPV significantly improved hrHPV clearance and related biological outcomes across multiple endpoints. Although interferon also demonstrated higher clearance rates than no treatment in unadjusted analyses, covariate-adjusted analyses showed attenuation of these effects at 6 months, whereas PHPV maintained consistent superiority. These findings position PHPV as a promising non-invasive therapeutic option for persistent hrHPV infection.
The primary outcome, hrHPV clearance at 6 months post-enrollment, demonstrated PHPV’s superior efficacy (66.7%) compared to interferon (45.9%) and the control group (20.6%). Reported spontaneous hrHPV clearance rates range around 20%,13,23 while interferon treatment achieves 25%-61% clearance,11–13 consistent with our findings. PHPV also showed higher effective rates, defined as HPV E6/E7 mRNA or at least one hrHPV type becoming negative, at both 3 and 6 months. While interferon demonstrated efficacy over the control in unadjusted analyses, adjusted analyses indicated less stable effects, whereas PHPV maintained consistent superiority over no treatment.
Exploratory biological analyses provided supportive evidence for the observed clinical effects. PHPV treatment was associated with reduced HPV E6/E7 oncogene expression, as indicated by exploratory Western blot analyses demonstrating lower E6/E7 protein levels following treatment. Suppression of E6/E7 expression may contribute to restoration of tumor suppressor pathways such as p53 and Rb.24,25 In addition, PHPV (82.1%) was associated with a reduction in HPV viral load in a greater proportion of participants compared with interferon (70.3%) and no treatment (44.1%). Exploratory analyses also suggested favorable changes in vaginal microecology, including improved bacterial diversity and normalization of microecological status, which may help reduce reinfection risk and support cervical health.26,27 These biological findings should be interpreted cautiously, as the corresponding analyses were exploratory and not powered for confirmatory inference.
PHPV was well-tolerated, with no adverse reactions reported during treatment or follow-up, unlike interferon, which caused mild vaginal itching in two participants. The absence of adverse events suggests that PHPV is a safe therapeutic option for long-term management of hrHPV infections.
Although PHPV demonstrated higher hrHPV clearance rates than interferon, the differences did not reach statistical significance in covariate-adjusted analyses at either 3 or 6 months. This may reflect limited statistical power for this comparison, as the study was primarily designed to compare active treatment with no treatment rather than to detect moderate differences between active interventions. Larger, adequately powered trials are therefore warranted to further evaluate the comparative efficacy of PHPV and interferon.
Beyond initial viral clearance, durable clearance and prevention of progression to high-grade cervical lesions (CIN2+) represent clinically meaningful long-term goals of hrHPV treatment. Given the 6-month follow-up duration of the present study, further studies with longer follow-up and larger sample sizes are required to assess the sustained efficacy of PHPV and its potential role in preventing disease progression.
Although baseline characteristics were generally balanced across groups, prespecified covariate-adjusted analyses were performed to improve the precision of treatment effect estimates. Adjustment for age, residence, contraceptive method, and baseline TCT results modestly influenced treatment effect estimates but did not change the overall interpretation of the primary mITT analysis, supporting the robustness of the PHPV findings.
Despite the use of randomization and allocation concealment to minimize selection bias, the open-label design may have introduced behavioral or assessment biases. Participants in the control group, who received no active treatment, may have differed in adherence or reporting behavior compared with treated participants. Future multicenter, double-blind studies may further reduce these potential sources of bias.
Current therapeutic options, including surgical interventions and interferon, have limitations such as high recurrence rates and incomplete efficacy.9,28 While prophylactic HPV vaccines are effective in preventing new infections, they have limited efficacy in individuals already infected.14,15 In this context, PHPV represents a non-invasive therapeutic approach targeting persistent hrHPV infection, with favorable efficacy and safety profiles.
In conclusion, PHPV demonstrated significant efficacy and good safety in treating persistent hrHPV infection. Despite limitations related to sample size, follow-up duration, and potential biases, PHPV offers a promising, well-tolerated, and non-invasive therapeutic option. Further large-scale, long-term, multicenter studies are needed to confirm its sustained clinical benefits and elucidate its underlying mechanisms.
Conclusion
PHPV is an effective and safe therapeutic option for persistent cervical hrHPV infection and demonstrated clear efficacy compared with no treatment. Compared with interferon, PHPV showed numerically higher clearance rates, although adjusted analyses did not demonstrate statistically significant differences. Its ability to reduce viral replication, suppress oncogene expression, and promote vaginal health suggests a promising role in preventing cervical precancerous lesions (CIN2+) and warrants further clinical development and broader application.
Data Sharing Statement
The individual participant data underlying this article were subject to ethical approval and cannot be shared publicly. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors wish to thank Guangxi Fulaiming Biopharmaceutical Co., Ltd. for providing the drug, and Sansure and Hologic for their support of HPV detection technology. The authors thank the patients who participated in this clinical trial, without whom the trial would not have been possible.
Funding
This work was supported by the National Natural Science Foundation of China (grant number 82271674, C.F.), Hunan Provincial Innovation Foundation for Postgraduate (grant number QL20230060, L.Y.), and Postgraduate Innovative Project of Central South University (grant number 2022XQLH151, L.Y.).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yang X, Li Y, Tang Y. et al. Cervical HPV infection in Guangzhou, China: an epidemiological study of 198,111 women from 2015 to 2021. Emerg Microbes Infect. 2023;12(1):e2176009. doi:10.1080/22221751.2023.2176009
2. Monk BJ, Tewari KS. The spectrum and clinical sequelae of human papillomavirus infection. Gynecol Oncol. 2007;107(Suppl 1):S6–13. doi:10.1016/j.ygyno.2007.07.076
3. Chesson HW, Dunne EF, Hariri S, Markowitz LE. The estimated lifetime probability of acquiring human papillomavirus in the United States. Sex Transm Dis. 2014;41(11):660–664. doi:10.1097/OLQ.0000000000000193
4. Moscicki AB, Shiboski S, Hills NK, et al. Regression of low-grade squamous intra-epithelial lesions in young women. Lancet. 2004;364(9446):1678–1683. doi:10.1016/S0140-6736(04)17354-6
5. Bulkmans NW, Berkhof J, Bulk S, et al. High-risk HPV type-specific clearance rates in cervical screening. Br J Cancer. 2007;96(9):1419–1424. doi:10.1038/sj.bjc.6603653
6. de Sanjose S, Brotons M, Pavon MA. The natural history of human papillomavirus infection. Best Pract Res Clin Obstet Gynaecol. 2018;47:2–13. doi:10.1016/j.bpobgyn.2017.08.015
7. Day PM, Schelhaas M. Concepts of papillomavirus entry into host cells. Curr Opin Virol. 2014;4:24–31. doi:10.1016/j.coviro.2013.11.002
8. Yuan Y, Cai X, Shen F, Ma F. HPV post-infection microenvironment and cervical cancer. Cancer Lett. 2021;497:243–254. doi:10.1016/j.canlet.2020.10.034
9. Fan A, Wang C, Han C, Wang Y, Xue F, Zhang L. Factors affecting residual/recurrent cervical intraepithelial neoplasia after cervical conization with negative margins. J Med Virol. 2018;90(9):1541–1548. doi:10.1002/jmv.25208
10. So KA, Lee IH, Kim TJ, Lee KH. Risk factors of persistent HPV infection after treatment for high-grade squamous intraepithelial lesion. Arch Gynecol Obstet. 2019;299(1):223–227. doi:10.1007/s00404-018-4936-9
11. Xiong Y, Cui L, Bian C, Zhao X, Wang X. Clearance of human papillomavirus infection in patients with cervical intraepithelial neoplasia: a systemic review and meta-analysis. Medicine. 2020;99(46):e23155. doi:10.1097/MD.0000000000023155
12. Yang Y, Hu T, Ming X, Yang E, Min W, Li Z. REBACIN(R) is an optional intervention for persistent high-risk human papillomavirus infection: a retrospective analysis of 364 patients. Int J Gynaecol Obstet. 2021;152(1):82–87. doi:10.1002/ijgo.13385
13. Zhou SG, Wu DF, Yao H, et al. REBACIN((R)) inhibits E6/E7 oncogenes in clearance of human papillomavirus infection. Front Oncol. 2022;12:1047222. doi:10.3389/fonc.2022.1047222
14. Simms KT, Steinberg J, Caruana M, et al. Impact of scaled up human papillomavirus vaccination and cervical screening and the potential for global elimination of cervical cancer in 181 countries, 2020-99: a modelling study. Lancet Oncol. 2019;20(3):394–407. doi:10.1016/S1470-2045(18)30836-2
15. Bruni L, Saura-Lazaro A, Montoliu A, et al. HPV vaccination introduction worldwide and WHO and UNICEF estimates of national HPV immunization coverage 2010–2019. Prev Med. 2021;144:106399. doi:10.1016/j.ypmed.2020.106399
16. Rahangdale L, Mungo C, O’Connor S, Chibwesha CJ, Brewer NT. Human papillomavirus vaccination and cervical cancer risk. BMJ. 2022;379:e070115. doi:10.1136/bmj-2022-070115
17. Zhao T, Li C, Wang S, Song X. Green Tea (Camellia sinensis): a Review of Its Phytochemistry, Pharmacology, and Toxicology. Molecules. 2022;27(12):3909.
18. CONSORT Group, Schulz KF, Altman DG, Moher D. Statement: updated guidelines for reporting parallel group randomised trials. Trials. 2010;11(1):32. doi:10.1186/1745-6215-11-32
19. Stensen S, Kjaer SK, Jensen SM, et al. Factors associated with type-specific persistence of high-risk human papillomavirus infection: a population-based study. Int J Cancer. 2016;138(2):361–368. doi:10.1002/ijc.29719
20. Zhang QQ, Zhang L, Liu Y, et al. Effect of ozonated water on normal vaginal microecology and Lactobacillus. Chin Med J. 2019;132(9):1125–1127. doi:10.1097/CM9.0000000000000216
21. Nayar R, Wilbur DC. The Pap test and Bethesda 2014. Cancer Cytopathol. 2015;123(5):271–281. doi:10.1002/cncy.21521
22. Getman D, Aiyer A, Dockter J, Giachetti C, Zhang F, Ginocchio CC. Efficiency of the APTIMA HPV Assay for detection of HPV RNA and DNA targets. J Clin Virol. 2009;45(1):S49–54. doi:10.1016/S1386-6532(09)70008-3
23. Chen F, Zhang GN, Lei W, et al. Effectiveness and safety of REBACIN as a non-invasive intervention for persistent high-risk human papillomavirus infection: a real-world prospective multicenter cohort study. Gynecol Oncol. 2023;178:8–13. doi:10.1016/j.ygyno.2023.09.004
24. Narisawa-Saito M, Kiyono T. Basic mechanisms of high-risk human papillomavirus-induced carcinogenesis: roles of E6 and E7 proteins. Cancer Sci. 2007;98(10):1505–1511. doi:10.1111/j.1349-7006.2007.00546.x
25. Hoppe-Seyler K, Bossler F, Braun JA, Herrmann AL, Hoppe-Seyler F. The HPVE6/E7Oncogenes: key Factors for Viral Carcinogenesis and Therapeutic Targets. Trends Microbiol. 2018;26(2):158–168. doi:10.1016/j.tim.2017.07.007
26. Liang Y, Chen M, Qin L, Wan B, Wang H. A meta-analysis of the relationship between vaginal microecology, human papillomavirus infection and cervical intraepithelial neoplasia. Infect Agent Cancer. 2019;14:29. doi:10.1186/s13027-019-0243-8
27. Zhang Z, Ma Q, Zhang L, et al. Human papillomavirus and cervical cancer in the microbial world: exploring the vaginal microecology. Front Cell Infect Microbiol. 2024;14:1325500. doi:10.3389/fcimb.2024.1325500
28. Hoffman SR, Le T, Lockhart A, et al. Patterns of persistent HPV infection after treatment for cervical intraepithelial neoplasia (CIN): a systematic review. Int J Cancer. 2017;141(1):8–23. doi:10.1002/ijc.30623
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bibliometric Analysis of Publications in Clinical Trials on Knee Osteoarthritis Between 2001 and 2022
Gu JY, Han F, Chen SY, Zhang Q
Journal of Pain Research 2023, 16:1961-1977
Published Date: 12 June 2023