Back to Journals » Journal of Pain Research » Volume 16
Bibliometric Analysis of Publications in Clinical Trials on Knee Osteoarthritis Between 2001 and 2022
Authors Gu JY, Han F, Chen SY, Zhang Q
Received 16 October 2022
Accepted for publication 3 April 2023
Published 12 June 2023 Volume 2023:16 Pages 1961—1977
DOI https://doi.org/10.2147/JPR.S392840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Jin Yu Gu,1 Fei Han,2 Si-Yu Chen,2 Qing Zhang1
1Department of Orthopaedic, The Hospital of Wang Jing, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China; 2Department of Orthopaedic, The Hospital of Guang An Men, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China
Correspondence: Qing Zhang, Department of Orthopaedic, The Hospital of Wang Jing, China Academy of Chinese Medical Sciences, Huajiadi Street, Chao Yang District, Beijing, 100102, People’s Republic of China, Tel +86-13911570607, Email [email protected]
Purpose: Clinical treatment of knee osteoarthritis has gained great interest, and numerous clinical studies have been reported. Few studies have described the detailed characterizations of clinical trials on knee osteoarthritis. This study is to identify, visualize, and characterize the clinical trials in knee osteoarthritis research.
Design and Methods: Articles published in recent two decades were extracted from the Web of Science core collection database using a query based on MeSH terms and topics of knee osteoarthritis and clinical trial. Basic characteristics of publications were analyzed based on the publication year, authors, institutions, counties, and keywords covered in the article. CiteSpace and VOS viewer were used for data visualization. The data were retrieved on May 28, 2022.
Results: A total of 1972 trials on knee osteoarthritis were identified. The number of publications has experienced rapid growth in the past two decades. America, England, and China had strong contributions in publication. Osteoarthritis and Cartilage, Annals of the Rheumatic Diseases and American Journal of Sports Medicine were highly cited and bellwether journals. Clustering mapping of the collaborative network, co-citation, and co-occurrence analyses showed that the research hotspots are mainly focused on disease-modifying medications, intra-articular injections, physical therapy for symptom control, lifestyle intervention, Chinese medicine treatment, and knee replacement.
Conclusion: Clinical treatments of knee OA are evolving. Pharmacologic therapy, intra-articular therapy, nonpharmacologic therapy including exercise or diet, self-management programs, Chinese medicine treatment, and knee replacement were highly represented in clinical trials of knee OA. Adjustment of combination therapy may be the next study focus in the future.
Keywords: knee osteoarthritis, treatment, clinical trial, bibliometric analysis, public health
Introduction
Osteoarthritis (OA) is the most common type of arthritis. Its pathological changes include synovial inflammation to varying degrees, degeneration of articular cartilage, formation of osteophytes, thickening of subchondral bone, degeneration of ligaments and meniscus of knee joint, and hypertrophy of joint capsule, affecting the entire joint structure.1 The World Health Organization calls OA “the first disabling disease”, current medical means can only reduce the symptoms and signs of patients to a certain extent, delay the progress of the disease, it is difficult to treat the disease fundamentally.2 The causes of OA involve inflammation, oxidative stress, joint damage, age and many other factors, and health care costs for OA reach $303 billion a year.3
Osteoarthritis of the knee (knee OA) is the most common cause of articular pain in the elderly and features cartilage loss, synovial hypertrophy, osteophytes, and meniscal damage.4 Knee OA is a chronic aging disorder in the whole joint, increasing in incidence year on year due to the aging population. Symptoms of knee OA often involve joint pain, reduced functional motion, swelling, and stiffness.5 Many basic and clinical studies focusing on radiology,6 cytology,7 risk factors,8 medications,9,10 behavioral therapy,11 and surgery12 have been devoted to understanding the physiological and pathophysiological processes of knee OA and seeking effective treatments.13–15 However, there are still no effective therapeutic strategies that have been proven to cure or delay symptom deterioration even with the huge economic cost to both individuals and society.16 However, this does not mean the researchers and clinicians would stop their steps to explore the best therapies for knee osteoarthritis. Targeted medical research is the key to achieving this goal.
Clinical trial, also commonly called randomized controlled trial (RCT) is a scientific research activity used to determine the safety and efficacy of therapies or drugs for use in patients. Clinical trial is characterized by rigorous study design, high levels of evidence, and more reliable results. Ever since clinical discovery of the treatment difficulty of knee osteoarthritis, more than 3000 clinical trials in this domain have already appeared in the scientific literature. Published articles covered a wide range of therapies, including but not limited to, physical therapy, pharmacological therapy, intra-articular injections, knee replacement, and combined treatment. Concurrently, these articles also revealed a wide range of dominant countries, journals, institutions, and authors that have made certain contributions in this field. Given the broad range of interests covered in these published works, it is of great necessity for scientific investigators to determine the precise study direction and relative challenges. Characterization of clinical trials for treating knee OA can aid researchers to tailor their study orientations and pursuit of associated interests.
Bibliometric analysis takes the publication system and characteristics as the research object, adopts mathematical and statistical methods to study the distribution structure, quantitative relationship and research topics of literature data, which can aid researchers to evaluate the publication trend and hotspots in a specific domain.17 Up to now, no bibliometric studies of clinical trials on knee OA have been conducted. Here, we aimed to identify the clinical trials focusing on the treatment of and to characterize these articles.
Materials and Methods
Articles Search and Selection
On May 28, 2022, we generated a series of published clinical trial studies related to the treatment of knee OA by utilizing the Web of Science Core Collection database. Here, we selected the Science Citation Index Expanded (SCI-EXPANDED), and Social Sciences Citation Index (SSCI) as the editions. Medical Subject Headings (MeSH) from the America National Library of Medicine was used to standardize the search terms due to the lack of subject term database in the Web of Science. Based on this, we used the following search terms and topics to retrieve publications in the database: (TS=(“Knee osteoarthr*”)) AND TS=(“Randomized Controlled Trial” OR “Randomised Controlled Trial” OR “clinical trial”). Next, we selected “Articles” for the file type and the publication period from January 1, 2001 to May 28, 2022, for the search and obtained 1972 original articles. All articles were published in English language. Through this flow, we finalized the clinical trial studies related to the treatment of knee OA for nearly two decades.
A clinical trial article related to the treatment of knee OA was defined as any research primarily focusing on surgical or nonsurgical treatment, drug or cell therapy, and combined management. Articles unrelated to our interests were excluded. Two reviewers (Jin-Yu Gu and Fei Han) performed independent article searching, identification, and analysis. The third senior reviewer (Qing Zhang) reassessed the fuzzy articles and discussed them until a consensus was reached.
Bibliometric Analysis
The basic characteristics of publications were described by using the intrinsic function of the Web of Science. Every article was reviewed for retrieval of the publication year, authors, institutions, counties, H-index, publication journal, journal citation reports (JCR), and keywords covered in the article. The H-index, widely considered a valuable measure of assessing academic productivity, has been studied in various medical and surgical specialties and has shown strong associations between higher h-indices and academic promotion, as well as with National Institutes of Health (NIH) awards.18
Data Visualization
Microsoft Office Excel and GraphPad Prism (8.3.0 version) were utilized to store data and visualize annual publications, institutional publications, and funding weightings, respectively. CiteSpace (version 6.1.R2) and VOS viewer (Leiden University, The Netherlands, version 1.6.18) were used for visualization of co-authorship, co-citation, and co-occurrence analysis. CiteSpace, a visual analysis software developed by Chaomei Chen, is most commonly used in bibliometric analysis. It analyses specific clusters of literature from multiple perspectives to explore and visualize research hotspots and trends in a particular field.19
Co-authorship analysis can be used to assess collaboration among countries, institutions and authors. Co-cited references (journals, authors) are two (or more) references (journals, authors) cited by one or more articles simultaneously.17,20 The centrality (betweenness centrality) of a node can present the significance of the position of the node in an interactive network.19,21 Its essence is a graph-theoretical property. The dual-map overlay of journals can well show the distribution of journals and the relationship between journals and cited journals (the color path represents the cited relationship).22 Clustering analysis of the co-authorship and co-citation results can indicate the research categories and directions of every study cluster. In addition, we used co-occurrence analysis (also known as keyword analysis) to cluster keywords from different studies to represent and predict research hotspots in the field.20
Results
A total of 1972 original clinical trials on the treatment of knee OA were determined for further analysis. The number of annual publications for clinical trials on knee OA from 2001 to 2022 is shown in Figure 1. The number curve can be divided into three periods according to the increasing trend: slow growth period (P1, 2001–2010), accelerating growth period (P2, 2011–2018), and plateau period (P3, 2018–2021). The number of published clinical trials on the treatment of knee OA increased relatively rapidly after 2010, reaching a peak in 2018 with more than 200 publications per year, and then entered a plateau period. The top 15 study categories and funding of the total number of publications were also visualized in Figures 2 and 3, respectively. The research category with the highest number of publications was orthopedics, and the funding with the largest number of publications was United States Department of Health Human Services.
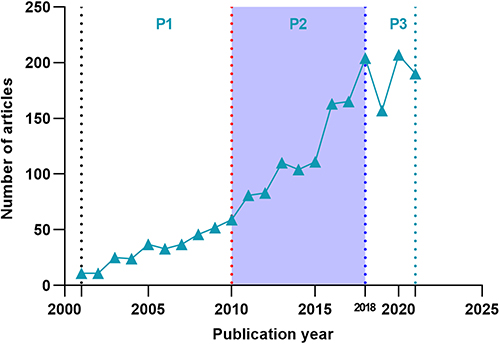 |
Figure 1 The number of annual publications during the past 22 years. |
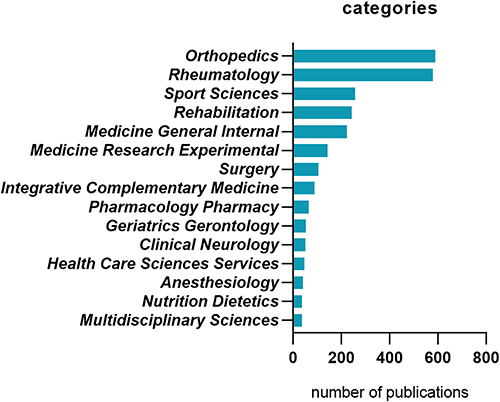 |
Figure 2 The top 15 study categories related to the clinical trials on knee osteoarthritis. |
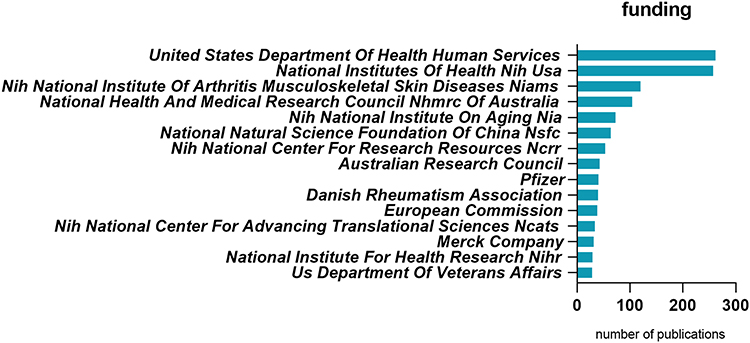 |
Figure 3 The top 15 study fundings related to the clinical trials on knee osteoarthritis. |
Countries, Institutions and Authors
The articles covered 87 countries or regions, 2923 institutions, and 8967 authors. The majority of the publications were contributed by the United States (n = 631), distantly followed by Australia (n=240), China (n=218), England (n=170), and Canada (n=143) (Table 1). The top five countries mentioned above contributed 71% of the total publications. Considering the number of total citations and average citations (citation/publication ratio), the United States had 27,333 citations (43 average citations), far more than all other countries. The number of publications in England was relatively low, but its citation/publication ratio (44) was the highest among the 10 countries. China had many publications but a relatively fewer citation/publication ratio (26). Collaboration network analysis of countries visualized in Figure 4 shows that the US, England, China and Australia had relatively higher volume of outputs and closely cooperation networks with each other.
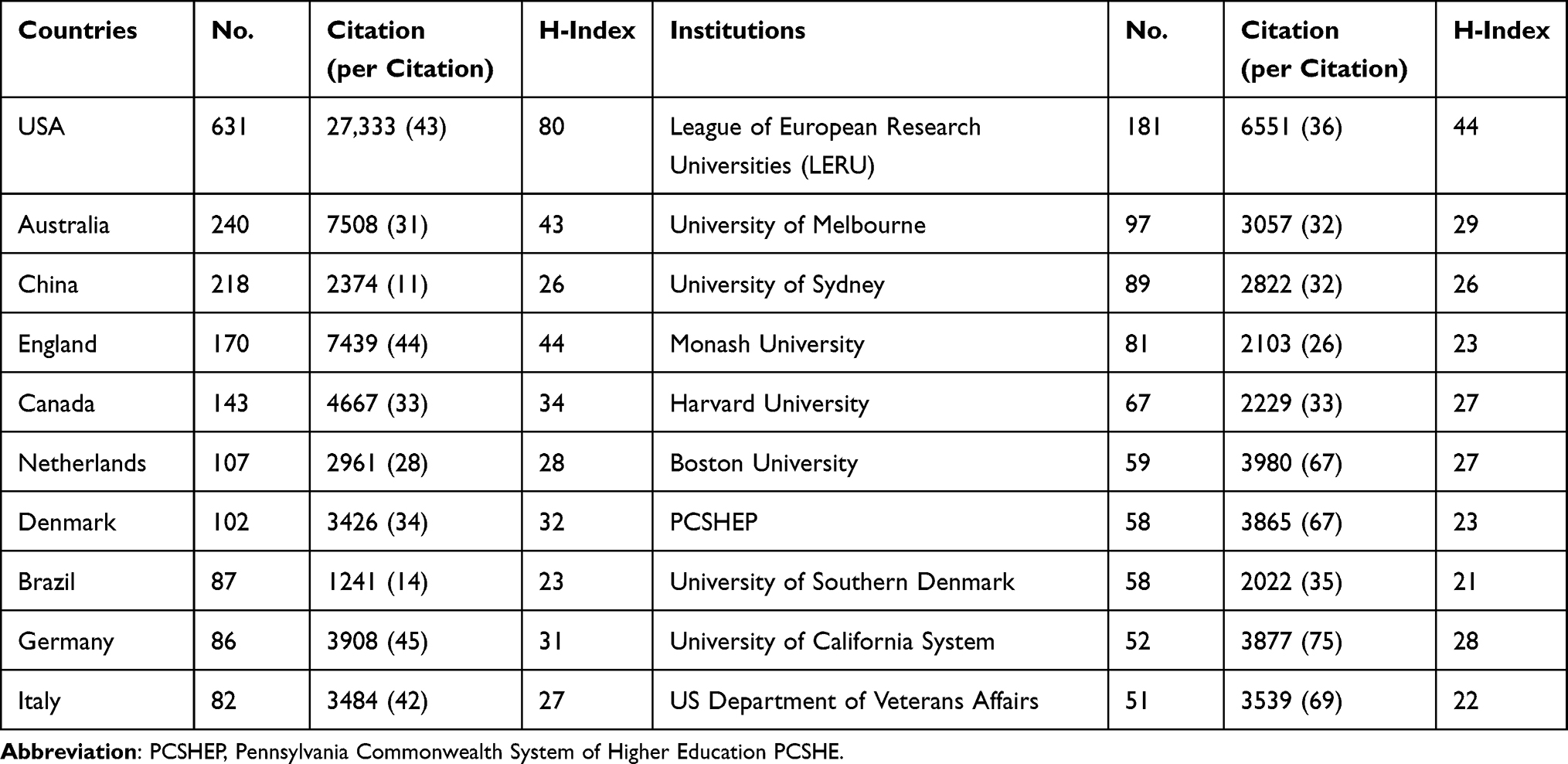 |
Table 1 Top 10 Productive Countries and Institutions in the Clinical Trial on Knee Osteoarthritis Research |
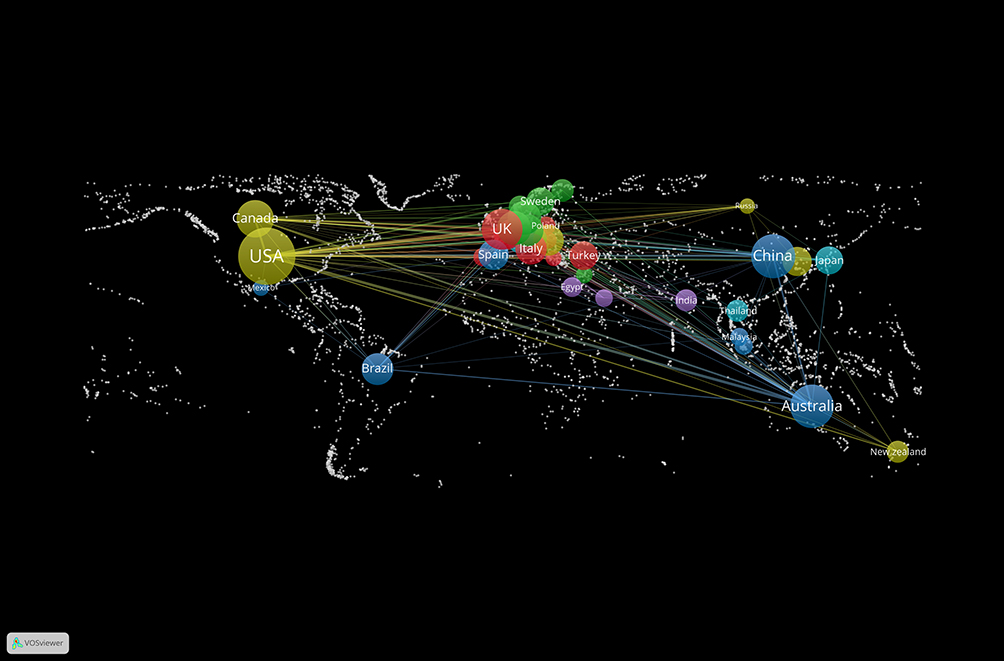 |
Figure 4 Collaboration network analysis of countries associated with the clinical trials on knee osteoarthritis. |
The top 10 institutions of the total number of publications are presented in Table 1. League of European Research Universities (LERU) published most clinical trials (n=181) with citation/publication ratio of 36, followed by the University of Melbourne (97 articles, 32 average citations), and the University of Sydney (89 articles, 32 average citations). Here, we specifically explored the collaborative networks and research direction clustering among institutions. As shown in Figure 5, institutions participating in the publication of clinical trials on the treatment of knee OA were divided into nine clusters that respectively focused on different research orientations, such as Beijing University Chinese Medicine and its collaborative institutions (mainly focusing on manual acupuncture study), University of Ottawa and its collaborative institutions (mainly focusing on the efficacy of Hylan G-F injection).
 |
Figure 5 Collaboration network analysis of institutions associated with the clinical trials on knee osteoarthritis. |
The top 10 authors of the total number of publications and the top 10 co-cited authors are presented in Table 2. Bennell KL published the most trials (n=73), but the Messier SP had the highest citation/publication ratio (88), which indicated the high quality of his articles. Among the top 10 co-cited authors, Bellamy N had the highest number of citations (n=901). Correspondingly, visualization of collaborative networks and research direction clustering among authors is presented in Figure 6. Here, we found that all authors can be classified into eight clusters according to their research networks. Details can be found in Figure 6.
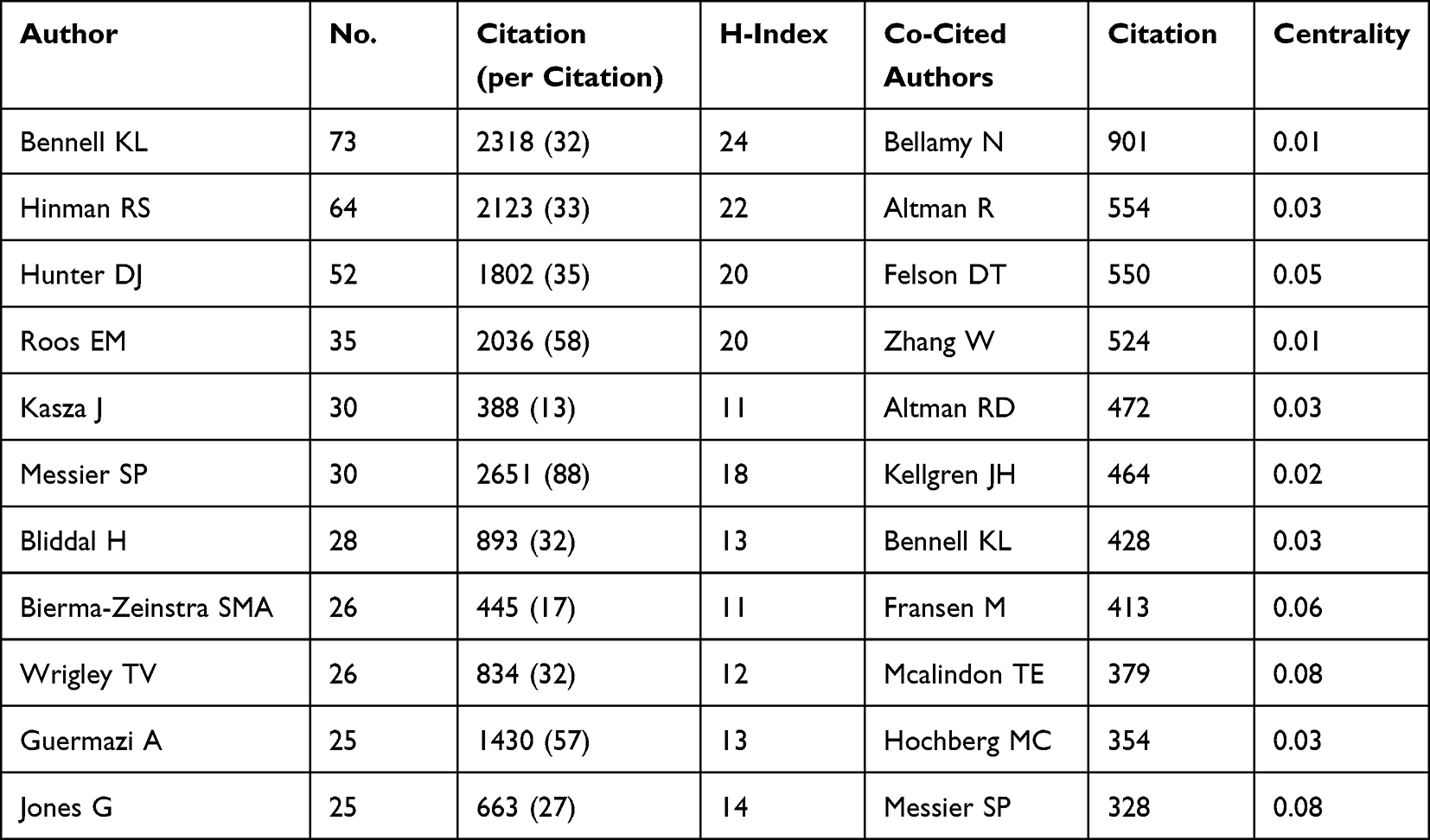 |
Table 2 Top 10 Productive Authors and Co-Cited Authors Related to Clinical Trial on Knee Osteoarthritis |
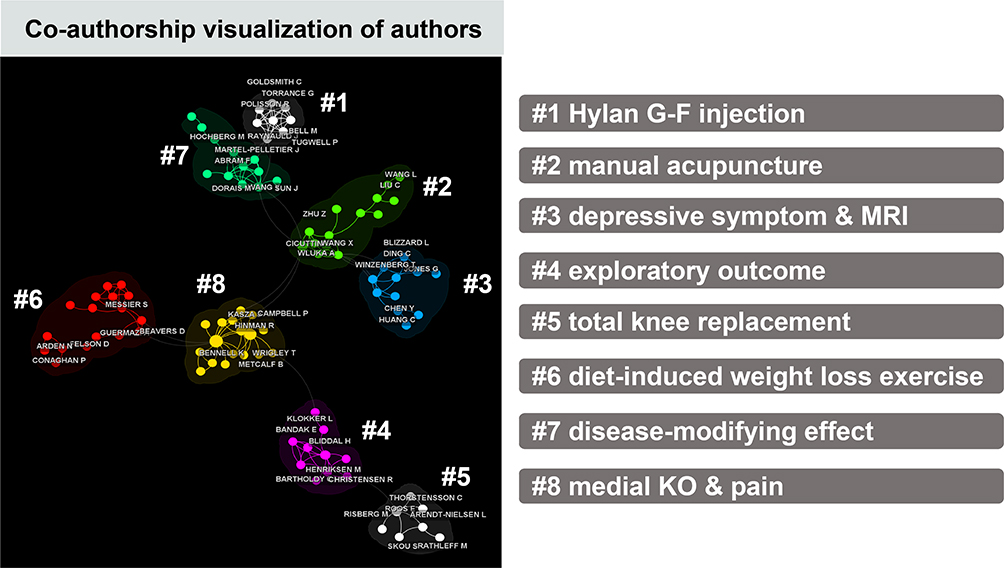 |
Figure 6 Collaboration network analysis of authors associated with the clinical trials on knee osteoarthritis. |
Journals and References
All of the clinical trials were published in 449 journals. The majority of the publications were contributed by BMC Musculoskeletal Disorders (147 articles, 15 average citations), followed by Osteoarthritis and Cartilage (240 articles, 32 average citations), Trials (73 articles, 7 average citations) (Table 3). It is worth noting that even though the American Journal of Sports Medicine (43 articles, 70 average citations) and Annals of the Rheumatic Diseases (40 articles, 77 average citations) did not have many published trials, they had a high citation/publication ratio. The highly cited articles were published in co-cited journals, led by Osteoarthritis and Cartilage (5175 citations) and Annals of the Rheumatic Diseases (3712 citations). The impact factors and JCR category of journals and co-cited journals are also summarized in Table 3. Visualization of co-cited analysis of journals and corresponding clusters based on research direction is presented in Figure 7. All of these cited journals were divided into 14 categories with research preferences that covered diverse treatment options used in the clinical setting. Furthermore, we also used the journal burst analysis in CiteSpace to detect emerging journals in a specific period to determine the advancement of research in this domain. The top 30 cited journals with the strongest citation bursts (burst intensity) are presented in Figure 8.
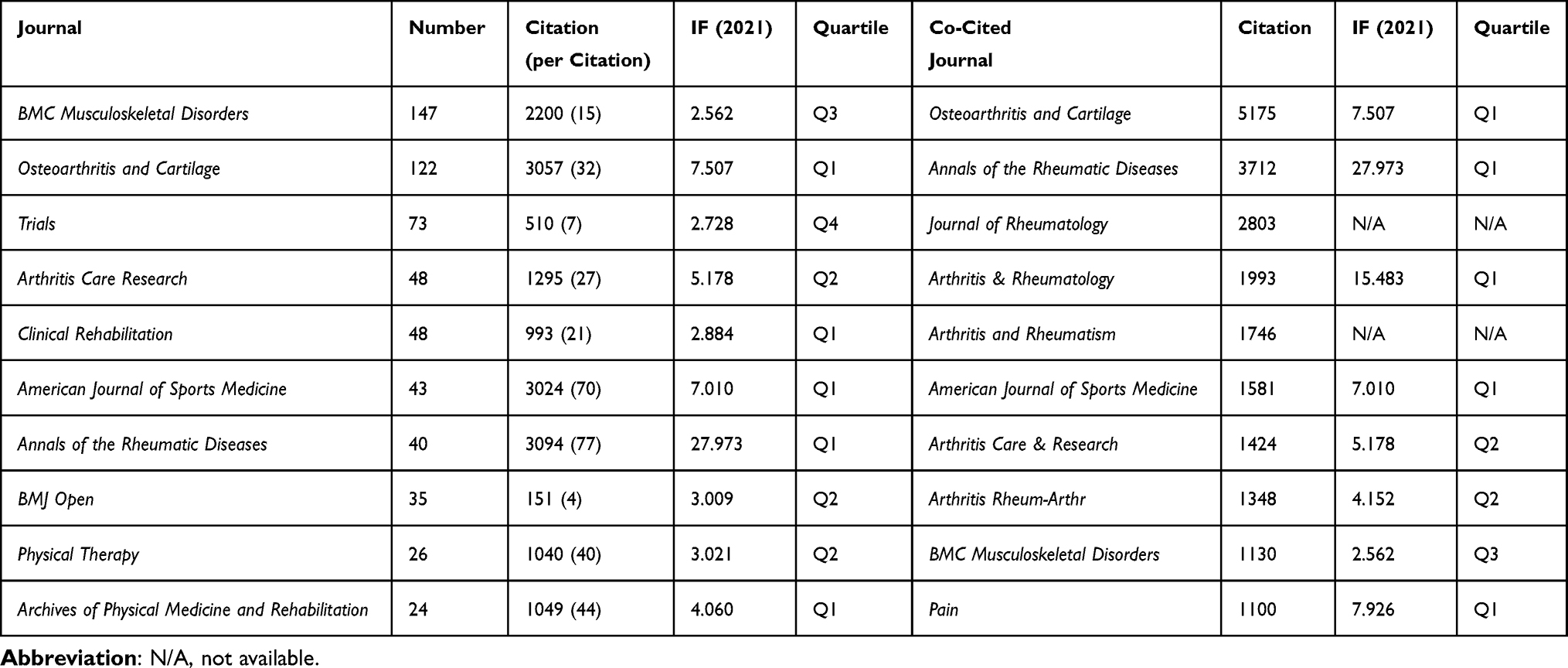 |
Table 3 Top 10 Productive Journals and Co-Cited Journals Related to Clinical Trials on Knee Osteoarthritis |
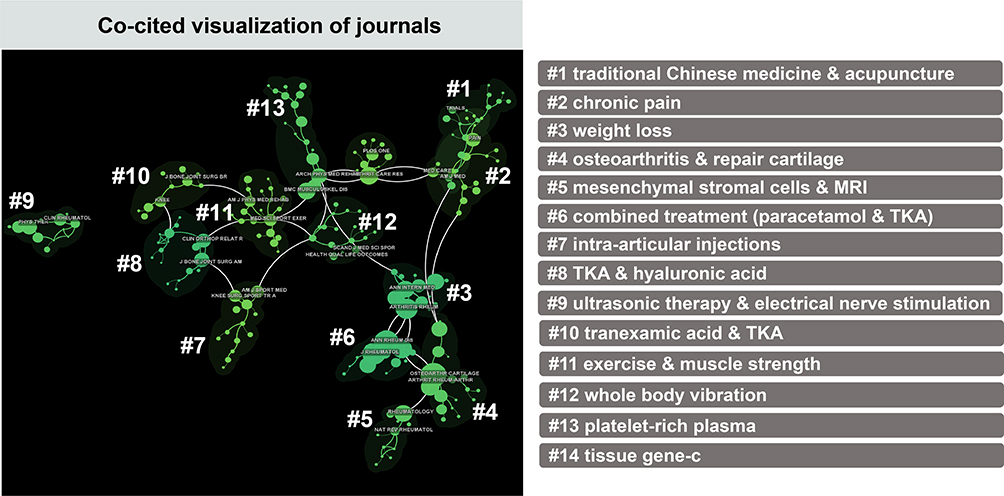 |
Figure 7 A cluster diagram of co-cited analysis of journals associated with the clinical trials on knee osteoarthritis. |
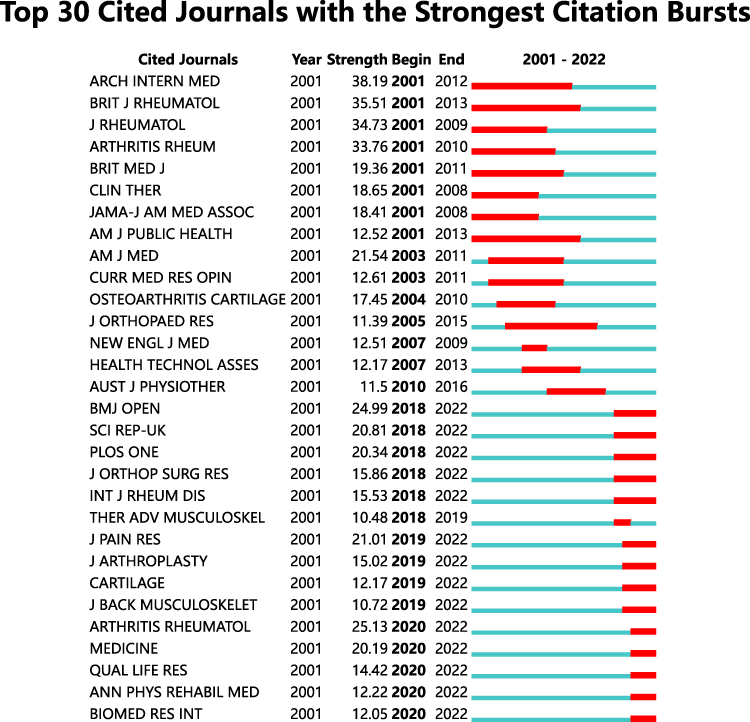 |
Figure 8 The top 30 journal with the most burstiness related to clinical trials on knee osteoarthritis. Years in blue indicate that the journal is less influential, and years in red indicate that the journal is more influential. |
Dual-map overlay of journals identified two main colored reference pathways in Figure 9 indicating that articles published in Molecular, Biology, Genetics, Health, Nursing, Medicine, and Sports, Rehabilitation, Sport journals were often cited in articles published in Medicine, Medical, Clinical and Neurology, Sports, Ophthalmology journals.
 |
Figure 9 The dual map overlay of journals associated with the clinical trials on knee osteoarthritis. The cited journals are located on the right, and the citing journals are located on the left. The colored path represents cited association. |
The top five most frequently co-cited references involved Mcalindon TE (2014),10 Hochberg MC (2012),23 Bannuru RR (2019),24 Zhang W (2010),25 and Zhang W (2018).26 Clustering analysis based on research directions and detailed characterizations of co-cited references were summarized in Figure 10. The top 30 references with the strongest citation bursts (burst intensity) are presented in Figure 11.9,10,16,23–49
 |
Figure 10 A cluster diagram of co-cited references associated with the clinical trials on knee osteoarthritis. |
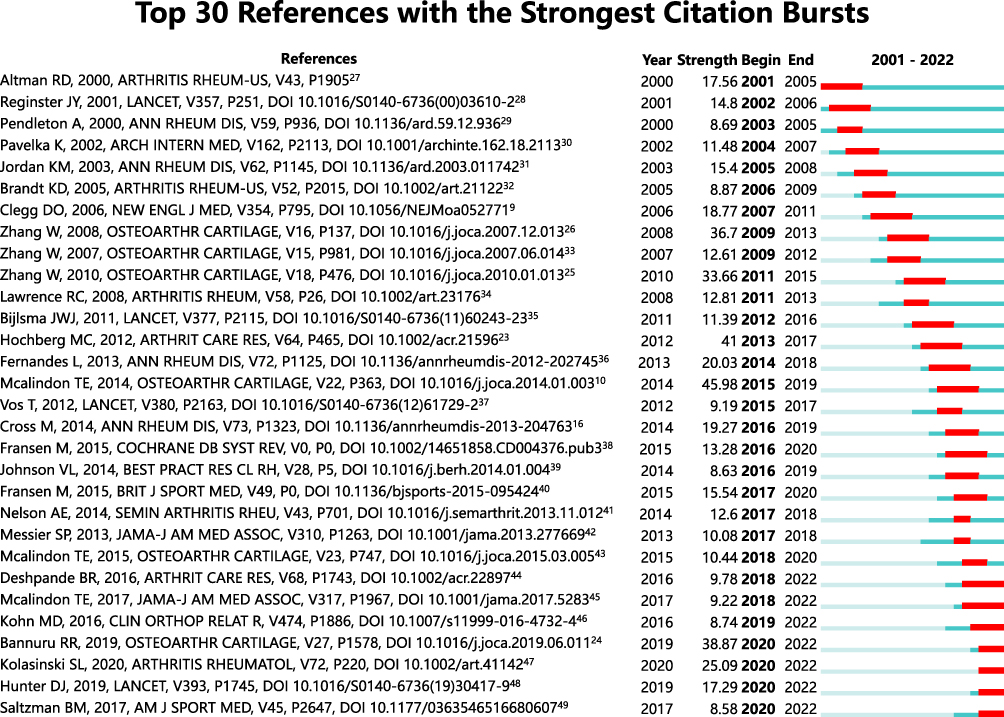 |
Figure 11 The top 30 co-cited references with the most burstiness related to clinical trials on knee osteoarthritis. The bolded type in the graph represents the point in time when the number of citations to an article increases significantly, indicating that the relevant research direction receives progressively more attention after that point in time. |
Keywords
In total, 5429 keywords were extracted from all of the clinical trials and were classified into 11 clusters (Figure 12) based on co-occurrence analysis in CiteSpace: structure-modifying drug, platelet-rich plasma injection, bone marrow, total knee arthroplasty, sham acupuncture, exercise therapy, behavioral management, strengthening muscles, multicenter, anterior cruciate ligament reconstruction, and medial compartment osteoarthritis studies. The larger the circle in the graph, the more frequently the keyword appears. Furthermore, we visualized the keywords based on the timeline of their occurrence, as detailed in Figure 13. The position where the circle appears represents the time of the first appearance of the keyword, and the size of the circle represents the cumulative number of appearances. In addition, the top 30 keywords with the strongest citation bursts (burst intensity) are presented in Figure 14.
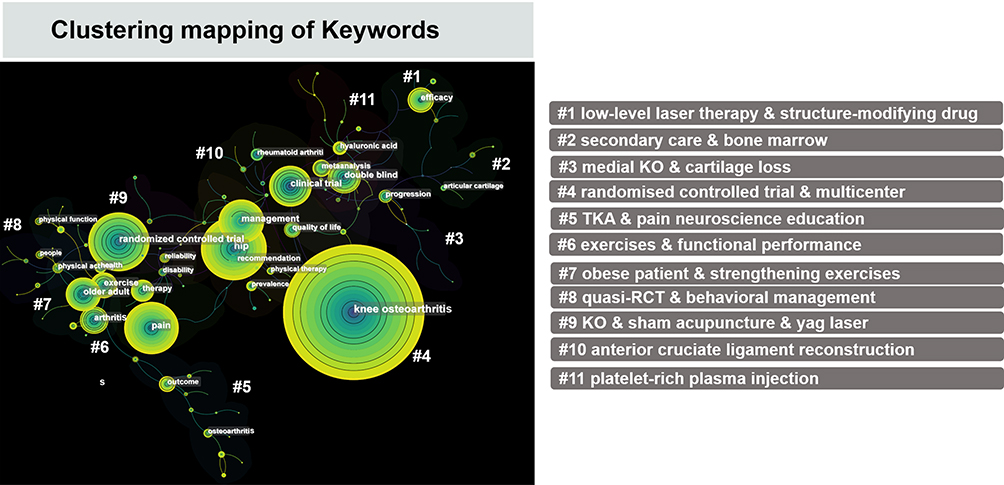 |
Figure 12 Mapping of keyword clusters associated with the clinical trials on knee osteoarthritis. |
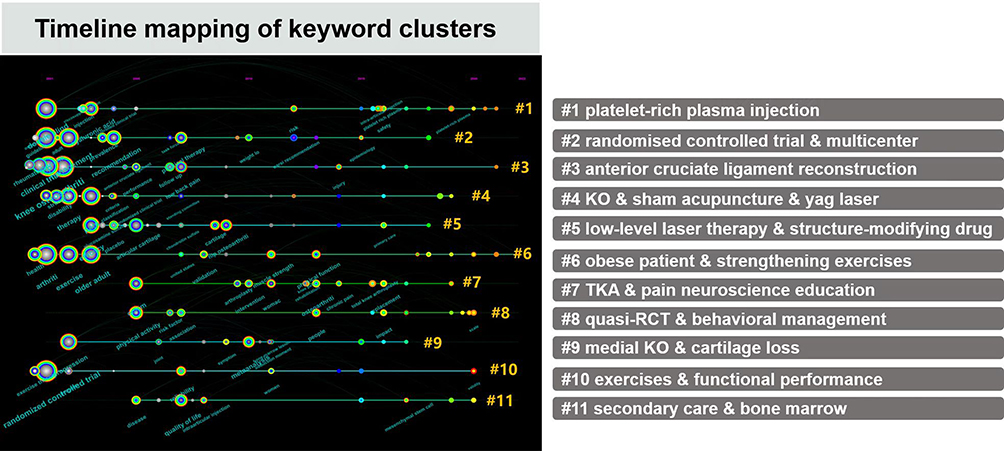 |
Figure 13 Keyword cluster analysis on timeline distribution associated with the clinical trials on knee osteoarthritis. |
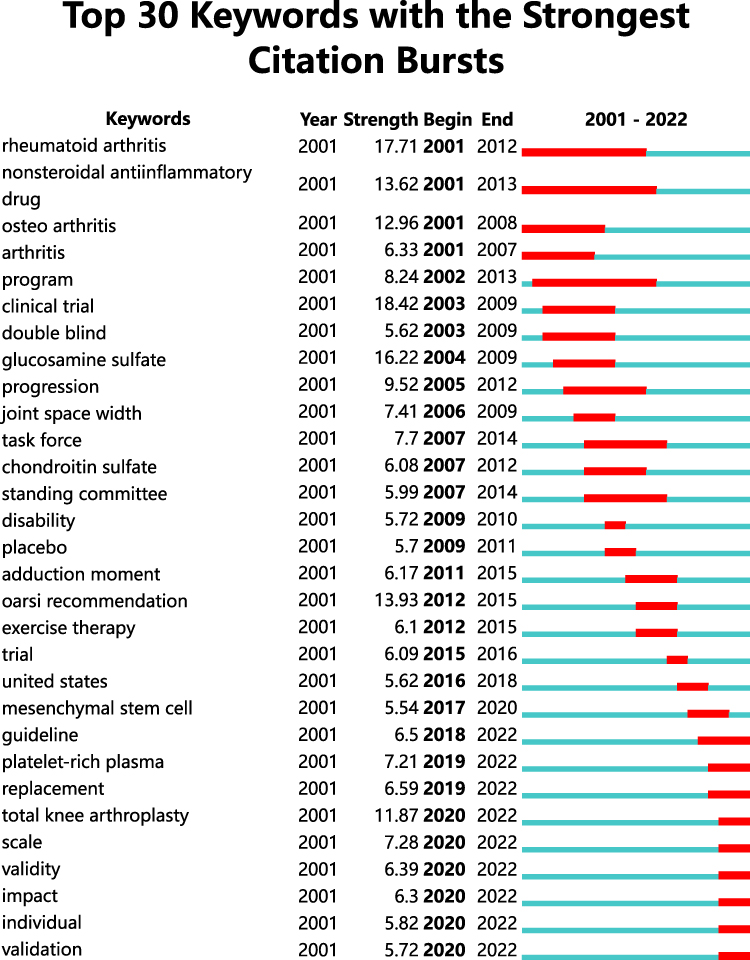 |
Figure 14 The top 30 keywords with the largest bursts related to clinical trials on knee osteoarthritis. The bolded type in the graph represents the point in time when the number of citations to an article increases significantly, indicating that the relevant research direction receives progressively more attention after that point in time. |
Highly Cited Clinical Trials
Publications with a high number of citations are considered central in a specific domain.50 We also characterized the influential clinical trials with the most total citations related to the treatment of knee OA. The number of subjects, intervention measures, delivery methods, duration, primary outcome measures, and National Clinical Trial (NCT) number are summarized in Table 4. Medications such as glucosamine sulphate and behavioral intervention such as diet for losing weight, depression care and exercise treatments were previously evaluated in randomized controlled trials, and then investigators began to focus on the intra-articular injection therapies such as mesenchymal stem cells and platelet-rich plasma. Primary clinical measures of the majority of these clinical trials were the extent of pain decrease and physical performance of the knee. Although these treatments did not achieve joint complete pain relief and function, the results of these influential clinical trials were encouraging and published in international top journals. A combination of multiple interventions may be more effective. Large and long-term clinical trials are ongoing.
 |
Table 4 Influential Published Clinical Trials Investigating the Safety and Efficacy of Diverse Treatment Measures for Knee Osteoarthritis |
Discussion
Here, we first utilized bibliometric analysis in an attempt to characterize the clinical trials on the clinical management of knee OA. Results of randomized controlled trials have a decisive impact on clinical treatment. Since the industry noticed the difficulties in the therapy of knee OA, clinical trials of diverse therapeutic measures have flourished. Identification and understanding of the publication trend and hotspots of these clinical trials are of great interest to scientific researchers, clinicians, and the public. First, scientific researchers would find clear study orientations and current challenges that they must face thereby effectively adjusting interventions. They also can determine the influential institutions or authors that specialize in one subspecialty and cooperate with them. Furthermore, with the aid of the information that our study provides, clinicians can guide patients with knee OA to manage their distressing symptoms reasonably. Third, the public also can capture some specific information such as topics covered in clinical trials, which might be helpful for compliance with informed clinical and daily prevention treatments.
Characterizations of Published Trials
The number of publications related to the clinical treatment of knee OA has experienced rapid growth in the past two decades (nearly 20-fold since 2001). Three different increased periods clarified the quantity and clinical importance of scientific research related to the clinical trials on knee OA. Clinical efficacy observations and understanding of knee OA before 2009 contributed to the burst research activity of the clinical trials during 2010–2018.51,52 There was a decrease in clinical trial studies in 2019, which may be due to COVID-19. COVID-19 lockdown has a significant impact on end-stage knee OA patients in many ways, such as physical activity and function, joint function, pain, etc.53
International collaborative network analysis revealed the majority of clinical trials were conducted in developed countries such as America, England, Australia, and their domestic influential institutions. The dominant position of publications of China in developing countries is firmly established (Table 1 and Figure 4). This trend demonstrates that more effective interventions are urgently needed in these areas. In this study, we also explored in particular the directions of collaboration and research frontiers of different institutions and authors (Figures 5 and 6). Visualization results showed that the therapeutic measures or research hotspots in this field are mainly focused on manual acupuncture, intra-articular injection such as Hylan G-F injection, physical therapy, medications for disease-modifying such as chondroitin sulfate, lifestyle intervention such as diet, knee replacement, and pain management.
The journal BMC Musculoskeletal Disorders and Osteoarthritis and Cartilage published the majority of clinical trials on the treatment of knee OA, while the highly cited journals focusing on the cartilage, rheumatic diseases, and rehabilitation mainly include the journals Osteoarthritis and Cartilage, Annals of the Rheumatic Diseases, and American Journal of Sports Medicine (Table 3). These journals are bellwether in the domain of orthopedics, rheumatology, and sports sciences. The co-citation visualization (Figure 7) and top-cited trials illustrated that Mcalindon TE, Hochberg MC, Bannuru RR, and Zhang W were the game changers on the current concept of the clinical treatment of knee OA. Their future research may have a substantial impact on the development in this field and should be closely monitored to grasp the latest advancement. The same therapeutic focuses obtained in the cooperative network clustering analysis were roughly found in the co-cited visualization of references and journals. Noteworthy, finer research subcategories yielded in the co-cited visualization of references and journals demonstrated that there is a growing consensus among clinicians on the management concept of a thorough understanding of the treatment mechanism and precise control of symptoms.
The high-frequency keywords involving osteoarthritis, clinical trial, pain, management, exercise, older adult, and hip in the clinical trials on the treatment of knee OA were classified into 11 clusters (Figure 12). This indicates that clinical trials in this area are becoming more mature and precise in treatment. We were also able to clarify from the analysis the main current research directions and clinical strategies. Furthermore, the TimeLine mapping of these clusters (Figure 13) illustrated that these studies have been carried out for almost 20 years and are still ongoing. Burst detection analysis of top keywords showed that clinical trial, rheumatoid arthritis, nonsteroidal anti-inflammatory, OA, glucosamine sulfate, oral recommendation, and total knee arthroplasty attracted relatively higher attention from researchers and clinicians during the past two decades (Figure 14). Additionally, mesenchymal stem cell, platelet-rich plasma, total knee arthroplasty, individual therapy, and treatment validation were among the new emerging since 2017. Therefore, the research foci in the clinical medication treatment of knee OA seem to have shifted from nonsteroidal anti-inflammatory drugs to intra-articular injection therapy. Arthroplasty is gradually becoming more acceptable to patients. In general, researchers are placing more emphasis on clinical efficacy and pursuing individualized precision medicine.
Treatment Findings and Areas of Uncertainty
In the past two decades, there has been a shift from pharmacologic treatment to nonpharmacologic therapy due to the limited efficacy of symptom relief and daily activity of the former.54 Choice of effective medications for the base treatment of knee OA is uncertain. Pharmacological treatment is also gradually shifting from non-steroidal anti-inflammatory drugs (NSAIDs) to intra-articular injection therapy, especially mesenchymal stem cells.55 Nonpharmacologic treatments mainly include exercise, diet therapy, self-efficacy and self-management program, Chinese medicine treatment such as manual acupuncture, and surgery. Clinical trials have proved that therapeutic exercise in patients with knee OA can significantly alleviate pain and improve joint function and quality of life.51,56,57 However, how to achieve reasonable physical exercise is still unclear. In overweight or obese patients, weight loss is urgently needed.11 Clinicians could add exercise therapy as needed.51 Self-management programs include education, pain management, practice, and behavioral control such as fear, depression, and anxiety.11,58 In patients with advanced knee OA and uncontrolled pain with other nonsurgical therapies, knee arthroplasty should be considered.59 More clinical data on the performance comparison between monotherapy and combination therapy are still needed. Large clinical trials are ongoing.
Limitations
Compared with reviews that cannot analyze massive heterogeneous articles, the present study based on bibliometric and visualized analyses provides a deep insight into the global status and trends of studies about the treatment of knee OA. However, our study has limitations. First, database bias. We searched only the Web of Science database that might differ from other databases such as PubMed, Scopus, and Embase to determine the relative studies. Second, the abbreviated forms and the plural forms of the same author, institution, country, and keywords might need to be merged during the analysis making the process cumbersome. Finally, we used the Medical Subject Headings (MeSH) that Web of Science does not have to standardize the search formula, which may lead to incomplete retrieval of publications.
Conclusion
Clinical trials on knee OA have flourished and matured after over 20 years of research. Bibliometric visualization in our study identified and characterized the publication trends and hotspots in this domain. Pharmacologic therapy including oral NSAIDs, glucosamine or chondroitin sulfate, intra-articular therapy including glucocorticoid and mesenchymal stem cells injections, nonpharmacologic therapy including exercise or diet, self-management programs and pain-coping skills training, Chinese medicine treatment such as manual acupuncture, and knee replacement were highly represented in the clinical trials on the clinical treatments of knee OA. Relevant results have been published in influential journals. Combination therapy may be the study foci in the future. The trends concluded from this cohort of articles furnish substantial confidence for future therapeutics for knee OA.
Abbreviations
Knee OA, osteoarthritis of the knee; RCT, randomized controlled trial; NCT, National Clinical Trial.
Data Sharing Statement
Data yielded in our study will be made available by the corresponding author to any qualified researchers.
Acknowledgments
We would like to thank data collectors and funding supporter for their invaluable support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Technology Innovation Project of China Academy of Chinese Medical Sciences (Grant No. CI2021A02003) and the Capital Health Development Research Project (First issue 2018-2-4162).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Loeser RF, Goldring SR, Scanzello CR, Goldring MB. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum. 2012;64:1697–1707. doi:10.1002/art.34453
2. Chen H, Chen L. An integrated analysis of the competing endogenous RNA network and co-expression network revealed seven hub long non-coding RNAs in osteoarthritis. Bone Joint Res. 2020;9:90–98. doi:10.1302/2046-3758.93
3. Murphy LB, Cisternas MG, Pasta DJ, Helmick CG, Yelin EH. Medical expenditures and earnings losses among US adults with arthritis in 2013. Arthrit Care Res. 2018;70:869–876. doi:10.1002/acr.23425
4. Sharma L, Solomon CG. Osteoarthritis of the Knee. N Engl J Med. 2021;384:51–59. doi:10.1056/NEJMcp1903768
5. Deng P, Liang H, Xie K, et al. Study on the molecular mechanism of Guizhi Jia Shaoyao decoction for the treatment of knee osteoarthritis by utilizing network pharmacology and molecular docking technology. Allergologia Et Immunopathologia. 2021;49:16–30. doi:10.15586/aei.v49i6.484
6. Guermazi A, Roemer FW, Haugen IK, Crema MD, Hayashi D. MRI-based semiquantitative scoring of joint pathology in osteoarthritis. Nat Rev Rheumatol. 2013;9:236–251. doi:10.1038/nrrheum.2012.223
7. Zacharjasz J, Mleczko AM, Bąkowski P, Piontek T, Bąkowska-żywicka K. Small Noncoding RNAs in knee osteoarthritis: the role of microRNAs and tRNA-derived fragments. Int J Mol Sci. 2021;22:5711. doi:10.3390/ijms22115711
8. Øiestad BE, Holm I, Gunderson R, Myklebust G, Risberg MA. Quadriceps muscle weakness after anterior cruciate ligament reconstruction: a risk factor for knee osteoarthritis? Arthrit Care Res. 2010;62:1706–1714. doi:10.1002/acr.20299
9. Clegg DO, Reda DJ, Harris CL, et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N Engl J Med. 2006;354:795–808. doi:10.1056/NEJMoa052771
10. McAlindon TE, Bannuru RR, Sullivan MC, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarth Cart. 2014;22:363–388. doi:10.1016/j.joca.2014.01.003
11. Thomas KS, Muir KR, Doherty M, et al. Home based exercise programme for knee pain and knee osteoarthritis: randomised controlled trial. BMJ. 2002;325:752. doi:10.1136/bmj.325.7367.752
12. Kwoh CK, Guehring H, Aydemir A, et al. Predicting knee replacement in participants eligible for disease-modifying osteoarthritis drug treatment with structural endpoints. Osteoarth Cart. 2020;28:782–791. doi:10.1016/j.joca.2020.03.012
13. Dantas LO, Salvini T, McAlindon TE. Knee osteoarthritis: key treatments and implications for physical therapy. Brazil J Physical Therap. 2021;25:135–146. doi:10.1016/j.bjpt.2020.08.004
14. Luetzner J, Kasten P, Guenther K-P, Kirschner S. Surgical options for patients with osteoarthritis of the knee. Nat Rev Rheumatol. 2009;5:309–316. doi:10.1038/nrrheum.2009.88
15. Zhang Y, Zeng Y. Curcumin reduces inflammation in knee osteoarthritis rats through blocking TLR4/MyD88/NF-kappa B signal pathway. Drug Dev Res. 2019;80:353–359. doi:10.1002/ddr.21509
16. Cross M, Smith E, Hoy D, et al. The global burden of Hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73:1323–1330. doi:10.1136/annrheumdis-2013-204763
17. Tang F, Dai W-B, Li X-L, et al. Publication trends and hot spots in femoroacetabular impingement research: a 20-year bibliometric analysis. J Arthroplasty. 2021;36:2698–2707. doi:10.1016/j.arth.2021.03.019
18. Bastian S, Ippolito JA, Lopez SA, Eloy JA, Beebe KS. The use of the h-index in academic orthopaedic surgery. J Bone Joint Surg. 2017;99:e14. doi:10.2106/jbjs.15.01354
19. Chen C, Song M. Visualizing a field of research: a methodology of systematic scientometric reviews. PLoS One. 2019;14:e0223994. doi:10.1371/journal.pone.0223994
20. Wang K, Xing D, Dong S, Lin J. The global state of research in nonsurgical treatment of knee osteoarthritis: a bibliometric and visualized study. BMC Musculoskelet Disord. 2019;20:407. doi:10.1186/s12891-019-2804-9
21. Ma L, Ma J, Teng M, Li Y. Visual analysis of colorectal cancer immunotherapy: a bibliometric analysis from 2012 to 2021. Front Immunol. 2022;13:843106. doi:10.3389/fimmu.2022.843106
22. Miao L, Zhang J, Zhang Z, et al. A bibliometric and knowledge-map analysis of CAR-T cells from 2009 to 2021. Front Immunol. 2022;13:840956. doi:10.3389/fimmu.2022.840956
23. Hochberg MC, Altman RD, April KT, et al. American college of rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, Hip, and knee. Arthrit Care Res. 2012;64:465–474. doi:10.1002/acr.21596
24. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, Hip, and polyarticular osteoarthritis. Osteoarth Cart. 2019;27:1578–1589. doi:10.1016/j.joca.2019.06.011
25. Zhang W, Nuki G, Moskowitz RW, et al. OARSI recommendations for the management of Hip and knee osteoarthritis: part III: changes in evidence following systematic cumulative update of research published through January 2009. Osteoarth Cart. 2010;18:476–499. doi:10.1016/j.joca.2010.01.013
26. Zhang W, Moskowitz RW, Nuki G, et al. OARSI recommendations for the management of Hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarth Cart. 2008;16:137–162. doi:10.1016/j.joca.2007.12.013
27. Altman RD. Intra-articular sodium hyaluronate in osteoarthritis of the knee. Semin Arthritis Rheum. 2000;30:11–18. doi:10.1053/sarh.2000.0248
28. Reginster JY, Deroisy R, Rovati LC, et al. Long-term effects of glucosamine sulphate on osteoarthritis progression: a randomised, placebo-controlled clinical trial. Lancet. 2001;357:251–256. doi:10.1016/s0140-6736(00)03610-2
29. Pendleton A, Arden N, Dougados M, et al. EULAR recommendations for the management of knee osteoarthritis: report of a task force of the standing committee for international clinical studies including therapeutic trials (ESCISIT). Ann Rheum Dis. 2000;59:936–944. doi:10.1136/ard.59.12.936
30. Pavelká K, Gatterová J, Olejarová M, et al. Glucosamine sulfate use and delay of progression of knee osteoarthritis: a 3-year, randomized, placebo-controlled, double-blind study. Arch Intern Med. 2002;162:2113–2123. doi:10.1001/archinte.162.18.2113
31. Jordan KM, Arden N, Doherty M, Dougados M. EULAR recommendations 2003: an evidence based approach to the management of knee osteoarthritis: report of a task force of the standing committee for international clinical studies including therapeutic trials (ESCISIT). Ann Rheum Dis. 2003;62:1145–1155. doi:10.1136/ard.2003.011742
32. Brandt KD, Mazzuca SA, Katz BP, et al. Effects of doxycycline on progression of osteoarthritis: results of a randomized, placebo-controlled, double-blind trial. Arthritis Rheum. 2005;52:2015–2025. doi:10.1002/art.21122
33. Zhang W, Moskowitz RW, Nuki G, et al. OARSI recommendations for the management of Hip and knee osteoarthritis, part I: critical appraisal of existing treatment guidelines and systematic review of current research evidence. Osteoarth Cart. 2007;15:981–1000. doi:10.1016/j.joca.2007.06.014
34. Lawrence RC, Felson DT, Helmick CG, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008;58:26–35. doi:10.1002/art.23176
35. Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: an update with relevance for clinical practice. Lancet. 2011;377:2115–2126. doi:10.1016/s0140-6736(11)60243-2
36. Fernandes L, Hagen KB, Bijlsma JWJ, et al. EULAR recommendations for the non-pharmacological core management of Hip and knee osteoarthritis. Ann Rheum Dis. 2013;72:1125–1135. doi:10.1136/annrheumdis-2012-202745
37. Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380:2163–2196. doi:10.1016/s0140-6736(12)61729-2
38. Fransen M, McConnell S, Harmer AR, et al. Exercise for osteoarthritis of the knee. Cochrane Database Syst Rev. 2015;1:Cd004376. doi:10.1002/14651858.CD004376.pub3
39. Johnson VL, Hunter DJ. The epidemiology of osteoarthritis. Best practice & research. Clin Rheumatol. 2014;28:5–15. doi:10.1016/j.berh.2014.01.004
40. Fransen M, McConnell S, Harmer AR, et al. Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med. 2015;49:1554–1557. doi:10.1136/bjsports-2015-095424
41. Nelson AE, Allen KD, Golightly YM, Goode AP, Jordan JM. A systematic review of recommendations and guidelines for the management of osteoarthritis: the chronic osteoarthritis management initiative of the U.S. bone and joint initiative. Semin Arthritis Rheum. 2014;43:701–712. doi:10.1016/j.semarthrit.2013.11.012
42. Messier SP, Mihalko SL, Legault C, et al. Effects of intensive diet and exercise on knee joint loads, inflammation, and clinical outcomes among overweight and obese adults with knee osteoarthritis: the IDEA randomized clinical trial. JAMA. 2013;310:1263–1273. doi:10.1001/jama.2013.277669
43. McAlindon TE, Driban JB, Henrotin Y, et al. OARSI clinical trials recommendations: design, conduct, and reporting of clinical trials for knee osteoarthritis. Osteoarth Cart. 2015;23:747–760. doi:10.1016/j.joca.2015.03.005
44. Deshpande BR, Katz JN, Solomon DH, et al. Number of persons with symptomatic knee osteoarthritis in the US: impact of race and ethnicity, age, sex, and obesity. Arthrit Care Res. 2016;68:1743–1750. doi:10.1002/acr.22897
45. McAlindon TE, LaValley MP, Harvey WF, et al. Effect of intra-articular triamcinolone vs saline on knee cartilage volume and pain in patients with knee osteoarthritis: a randomized clinical trial. JAMA. 2017;317:1967–1975. doi:10.1001/jama.2017.5283
46. Kohn MD, Sassoon AA, Fernando ND. Classifications in brief: Kellgren-Lawrence classification of osteoarthritis. Clin Orthop Relat Res. 2016;474:1886–1893. doi:10.1007/s11999-016-4732-4
47. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthrit Rheumatol. 2020;72:220–233. doi:10.1002/art.41142
48. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393:1745–1759. doi:10.1016/s0140-6736(19)30417-9
49. Saltzman BM, Leroux T, Meyer MA, et al. The therapeutic effect of intra-articular normal saline injections for knee osteoarthritis: a meta-analysis of evidence level 1 studies. Am J Sports Med. 2017;45:2647–2653. doi:10.1177/0363546516680607
50. Eyre-Walker A, Stoletzki N. The assessment of science: the relative merits of post-publication review, the impact factor, and the number of citations. PLoS Biol. 2013;11:e1001675. doi:10.1371/journal.pbio.1001675
51. Villareal DT, Chode S, Parimi N, et al. Weight loss, exercise, or both and physical function in obese older adults. N Engl J Med. 2011;364:1218–1229. doi:10.1056/NEJMoa1008234
52. Krebs EE, Gravely A, Nugent S, et al. Effect of opioid vs nonopioid medications on pain-related function in patients with chronic back pain or hip or knee osteoarthritis pain: the SPACE randomized clinical trial. JAMA. 2018;319:872–882. doi:10.1001/jama.2018.0899
53. Endstrasser F, Braito M, Linser M, et al. The negative impact of the COVID-19 lockdown on pain and physical function in patients with end-stage Hip or knee osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2020;28:2435–2443. doi:10.1007/s00167-020-06104-3
54. Nalamachu SR, Robinson RL, Viktrup L, et al. Multimodal treatment patterns for osteoarthritis and their relationship to patient-reported pain severity: a cross-sectional survey in the United States. J Pain Res. 2020;13:3415–3425. doi:10.2147/jpr.S285124
55. Pers YM, Rackwitz L, Ferreira R, et al. Adipose mesenchymal stromal cell-based therapy for severe osteoarthritis of the knee: a phase I dose-escalation trial. Stem Cells Transl Med. 2016;5:847–856. doi:10.5966/sctm.2015-0245
56. Messier SP, Loeser RF, Miller GD, et al. Exercise and dietary weight loss in overweight and obese older adults with knee osteoarthritis: the arthritis, diet, and activity promotion trial. Arthritis Rheum. 2004;50:1501–1510. doi:10.1002/art.20256
57. Roddy E, Zhang W, Doherty M, et al. Evidence-based recommendations for the role of exercise in the management of osteoarthritis of the Hip or knee--The MOVE consensus. Rheumatology. 2005;44:67–73. doi:10.1093/rheumatology/keh399
58. Lin EH, Katon W, Von Korff M, et al. Effect of improving depression care on pain and functional outcomes among older adults with arthritis: a randomized controlled trial. JAMA. 2003;290:2428–2429. doi:10.1001/jama.290.18.2428
59. Rueckl K, Runer A, Jungwirth-Weinberger A, et al. Severity of valgus knee osteoarthritis has no effect on clinical outcomes after total knee arthroplasty. Arch Orthop Trauma Surg. 2021;141:1385–1391. doi:10.1007/s00402-021-03785-4
60. Pahor M, Guralnik JM, Ambrosius WT, et al. Effect of structured physical activity on prevention of major mobility disability in older adults: the LIFE study randomized clinical trial. JAMA. 2014;311:2387–2396. doi:10.1001/jama.2014.5616
61. Jo CH, Lee YG, Shin WH, et al. Intra-articular injection of mesenchymal stem cells for the treatment of osteoarthritis of the knee: a proof-of-concept clinical trial. Stem Cells. 2014;32:1254–1266. doi:10.1002/stem.1634
62. Patel S, Dhillon MS, Aggarwal S, Marwaha N, Jain A. Treatment with platelet-rich plasma is more effective than placebo for knee osteoarthritis: a prospective, double-blind, randomized trial. Am J Sports Med. 2013;41:356–364. doi:10.1177/0363546512471299
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Bibliometric and Scientific Knowledge Map Study of Migraine Treatment from 2013 to 2022
Wang T, Li Y, Miao S, Yang C, Xie W, Yuan H, Bai W, Xiao H, Yu S
Journal of Pain Research 2023, 16:3169-3184
Published Date: 15 September 2023
Bibliometric Analysis of the Knowledge Landscape of Periodontal Disease in Pregnancy: A Noteworthy Multidisciplinary Issue
Liu Z, Li Z, Wang L, Gu Z, Ma L
Journal of Multidisciplinary Healthcare 2023, 16:3941-3957
Published Date: 8 December 2023
Inflammation in Obstructive Sleep Apnea: A Global Bibliometric Perspective
Fan H, Niu H, Zhao B, Gao X
Nature and Science of Sleep 2025, 17:2275-2295
Published Date: 22 September 2025
Current Trends and Future Insights on Rosacea Treatment: A Bibliometric Analysis
Wang D, Zhang J, Wang B, Gao J, Zhang G
Clinical, Cosmetic and Investigational Dermatology 2025, 18:3397-3412
Published Date: 13 December 2025
Efficacy and Safety of PHPV Fusion Factor Vaginal Gel (PHPV®) in Clearing Cervical Persistent High-Risk Human Papillomavirus Infection: A Randomized Controlled Clinical Trial
Yan L, Yin H, Shi L, Ding B, Liu C, Wang Y, Fu C
Drug Design, Development and Therapy 2026, 20:542859
Published Date: 16 March 2026