Back to Journals » Journal of Pain Research » Volume 18
Effects of Tissue-Bone Homeostasis Manipulation at Different Time Points on Pain and Brain Mechanisms in Patients with Knee Osteoarthritis Based on Circadian Rhythm: Study Protocol for a Randomized Controlled Trial
Authors Ma H, Ding Y, Yang K, Zhang Z, Xu H, Feng W, Jiang L ![]()
Received 28 April 2025
Accepted for publication 12 August 2025
Published 19 August 2025 Volume 2025:18 Pages 4161—4172
DOI https://doi.org/10.2147/JPR.S537328
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Alaa Abd-Elsayed
Hongli Ma,1,2,* Yuwu Ding,2,* Kun Yang,2 Zengqiao Zhang,2 Haichen Xu,2 Wei Feng,1 Liming Jiang2
1School of Rehabilitation Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2Department of Rehabilitation, Seventh People’s Hospital of Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liming Jiang, Department of Rehabilitation, Seventh People’s Hospital of Shanghai University of Traditional Chinese Medicine, 358 Datong Road, Pudong New Area, Shanghai, People’s Republic of China, Email [email protected] Wei Feng, School of Rehabilitation Medicine, Shanghai University of Traditional Chinese Medicine, 1200 Cailun Road, Pudong New Area, Shanghai, People’s Republic of China, Email [email protected]
Background: Knee osteoarthritis (KOA) is characterized by pain and dysfunction. Tissue-bone homeostasis manipulation (TBHM) has been shown to have a good effect on KOA. However, its optimal application time and related mechanism of action are still unclear. Therefore, this study will explore the efficacy and brain mechanism of TBHM at different time points in patients with KOA.
Methods: The experiment is designed as a randomized controlled single-blind study, aiming to recruit 100 patients with KOA. These patients will be divided into four groups using stratified random sampling: the TBHM group at 8 a.m. the TBHM group at 1 p.m. the TBHM group at 6 p.m. and the Joint Mobilization group. The intervention will last for 4 weeks, once a day, 5 days per week. All outcome indicators will be measured at baseline and 4 weeks after the intervention, with the efficacy indicators measured additionally during follow-up visits at the 3rd and 6th months. The efficacy results include the Visual Analog Scale, Active range of motion, SF-36, electroencephalogram (EEG) and the Hamilton Anxiety Rating Scale. The mechanism part mainly focuses on changes in melatonin content in saliva. Two-way repeated measures analysis of variance (ANOVA) will be used to measure and statistically analyze all quantitative scores, while MatLab 2022b will be utilized for the analysis of EEG data.
Discussion: This study, based on “circadian rhythm”, innovatively combines different treatment times with TBHM to treat KOA pain. It will delve into the differences in the impact of this approach on KOA pain relief at different time points and clarify its potential mechanism of action. This will not only enhance the scientific understanding of the treatment effect of this manipulation but also provide new strategies and references for clinical treatment of KOA.
Trial Registration: The study was registered in Chinese Clinical Trial Registry (No. ChiCTR2400080820). Registered on Feb. 07, 2024, https://www.chictr.org.cn/showproj.html?proj=220404.
Keywords: knee osteoarthritis, tissue-bone homeostasis manipulation, pain, circadian rhythm, brain mechanism
Introduction
Knee osteoarthritis (KOA) is a whole joint disease involving all joint tissues, including changes in infrapatellar fat pad and synovial membrane and meniscal degeneration.1,2 Its key pathological characteristics include distortion and loss of articular cartilage, sclerosis of joint border and subchondral bone, and the production of osteophytes.3 The clinical manifestations mainly include chronic joint pain, limited motor function, joint stiffness, and even deformation.4 The main risk factors include aging, obesity, joint injury, genetic predisposition, and gender.5 According to surveys, the prevalence of symptomatic KOA among middle-aged and elderly people in China is 8.1%,6 and the incidence rate increases with age. The World Health Organization (WHO) has defined KOA as the fourth leading cause of disability globally, and with the increase in average life expectancy and the progress of global aging, it has brought a heavy burden to global public health.
Pain is an important predictor of functional limitations in people with KOA,7 exhibits diverse characteristics throughout the progression of the disease.8 In the early stage of KOA, the pain is evidently predictable For instance, activities such as excessive walking or climbing stairs usually lead to a worsening of the pain. As the disease advances to the later stage, unpredictable pain gradually becomes the norm, and persistent pain frequently occurs at night, severely impairing the patients’ sleep quality. Numerous studies have also verified that sleep has become an important criterion for measuring the degree of KOA pain.9,10 There exists a close and intricate relationship between the two, interacting with each other and jointly affecting the patients’ quality of life and disease experience.
Research data show that more than half of KOA patients will suffer from continuous pain at night, which not only seriously affects their sleep quality but also often leads to insomnia and frequent awakenings. A study by Campbell et al11 found that sleep and pain can influence each other, with increased night pain affecting sleep quality and improved sleep significantly reducing the occurrence of KOA pain.12,13 Circadian rhythm is a biological rhythm within an organism that is close to a 24-hour cycle.14 It receives retinal light signals through the suprachiasmatic nucleus (SCN) of the hypothalamus and is synchronized with the earth’s rotation cycle.15 It profoundly affects everything from gene expression to overall physiological function (including inflammation and repair).16 The pathological process and symptoms of KOA have a clear circadian rhythm, especially the pain is aggravated at night and relieved during the day.17 Therefore, utilizing the principles of “circadian rhythm” to guide manual interventions for KOA becomes particularly significant.
Circadian rhythm is an intrinsic physiological cycle regulated by the biological clock, affecting various aspects including sleep-wake cycle, hormone secretion, body temperature regulation, and so on.18 It is coordinated by the SCN of the hypothalamus,19 and each internal organ also possesses its own circadian rhythm. In recent years, more and more researchers have focused on the importance of circadian rhythm to human health. Multiple studies have shown that circadian rhythm disorders can lead to the occurrence and development of many diseases,20 including neurodegenerative diseases,21 cardiovascular diseases,22 musculoskeletal diseases,23 etc. Numerous studies have proven that circadian rhythm disorders are closely related to osteoarthritis, including affecting bone density, osteoclast differentiation, and the expression of inflammatory factors.16,24 Therefore, pain caused by KOA can lead to sleep disorders, which are circadian rhythm disorders, and vice versa, circadian rhythm disorders can interfere with pain relief by affecting inflammatory factors, cell differentiation, and other aspects. Melatonin, an indole hormone secreted by the pineal gland in the brain,25 follows the circadian rhythm strictly in its synthesis and release, that is, it shows a higher level at night and a lower level during the day.26 By monitoring the release level and concentration curve of melatonin,27,28 the homeostatic state of the body’s circadian rhythm can be effectively reflected. Studies29 have shown that Melatonin lowers core body temperature to promote the drowsiness. In addition, exercise time has a regulatory effect on melatonin (exercise in the afternoon may inhibit the secretion of melatonin at night, while exercise in the morning has less negative impact on melatonin).29 Therefore, the effect of melatonin in promoting sleep may be affected by the time interval between exercise and sleep.
Clinically, pain caused by KOA is often treated with medication,30,31 but it often leads to significant adverse reactions such as drug dependence and side effects. Therefore, there is a need for a non-pharmacological treatment method that can relieve joint pain with fewer adverse reactions. There are many non-pharmacological treatment methods for KOA, including manual therapy (MT), high-intensity laser therapy,32 and more. Among the alternative or complementary non-pharmacological treatment methods for KOA pain management, MT is widely used due to its safety, non-invasiveness, and effectiveness in reducing pain.33,34 As a form of MT, tissue-bone homeostasis manipulation (TBHM) is a treatment method developed on the basis of traditional Chinese and Western medicine theories that emphasizes the simultaneous treatment of tendons and bones. During treatment, the first step is relaxation techniques, which are conducive to the complete relaxation of the soft tissues around the knee joint and reduce tissue tension. The second step is to press the classic acupoints and Ashi points of the knee joint to increase the pain threshold and reduce the release of pain-causing substances. The third step is to use the infrapatellar fat pad release technique to completely loosen the adhesion tissue around the knee joint, especially the infrapatellar fat pad tissue. Finally, adjust the displaced patella and dislocated tibiofemoral joint, improve the movement trajectory of the patella, and restore the force line of the lower limbs, thereby promoting the recovery of joint function and pain relief in patients with KOA.35 Interestingly, time-based therapy based on circadian rhythm, which optimizes the timing of treatment, has attracted widespread attention from researchers. Although TBHM can significantly alleviate KOA pain, the optimal time for its effectiveness remains unclear.35
In summary, this study aims to optimize the treatment time of TBHM, a significant therapeutic approach for KOA, based on the “circadian rhythm” theory. The goal is to maximize its positive therapeutic effects, improve treatment efficiency, and explore related brain mechanisms.
Materials and Methods
Study Design
This research will utilize a single-blind, randomized controlled trial involving 100 qualified participants. These participants will be randomly divided into four groups: TBHM at 8 a.m., TBHM at 1 p.m., TBHM at 6 p.m., and Joint Mobilization group, with a ratio of 1:1:1:1. Stratified randomization will be used, considering factors such as gender, age, and Kellgren-Lawrence (K-L) grade. A concise flowchart of the study is depicted in Figure 1, with the schedule of activities detailed in Table 1. The study protocol was designed in strict accordance with the Standard Protocol Items: Recommendations for Interventional Trials 2013 (SPIRIT 2013) (SPIRIT Document) and was approved by the Ethics Committee of Shanghai Seventh People’s Hospital and registered with the Chinese Clinical Trial Registry (registration number: ChiCTR2400080820).
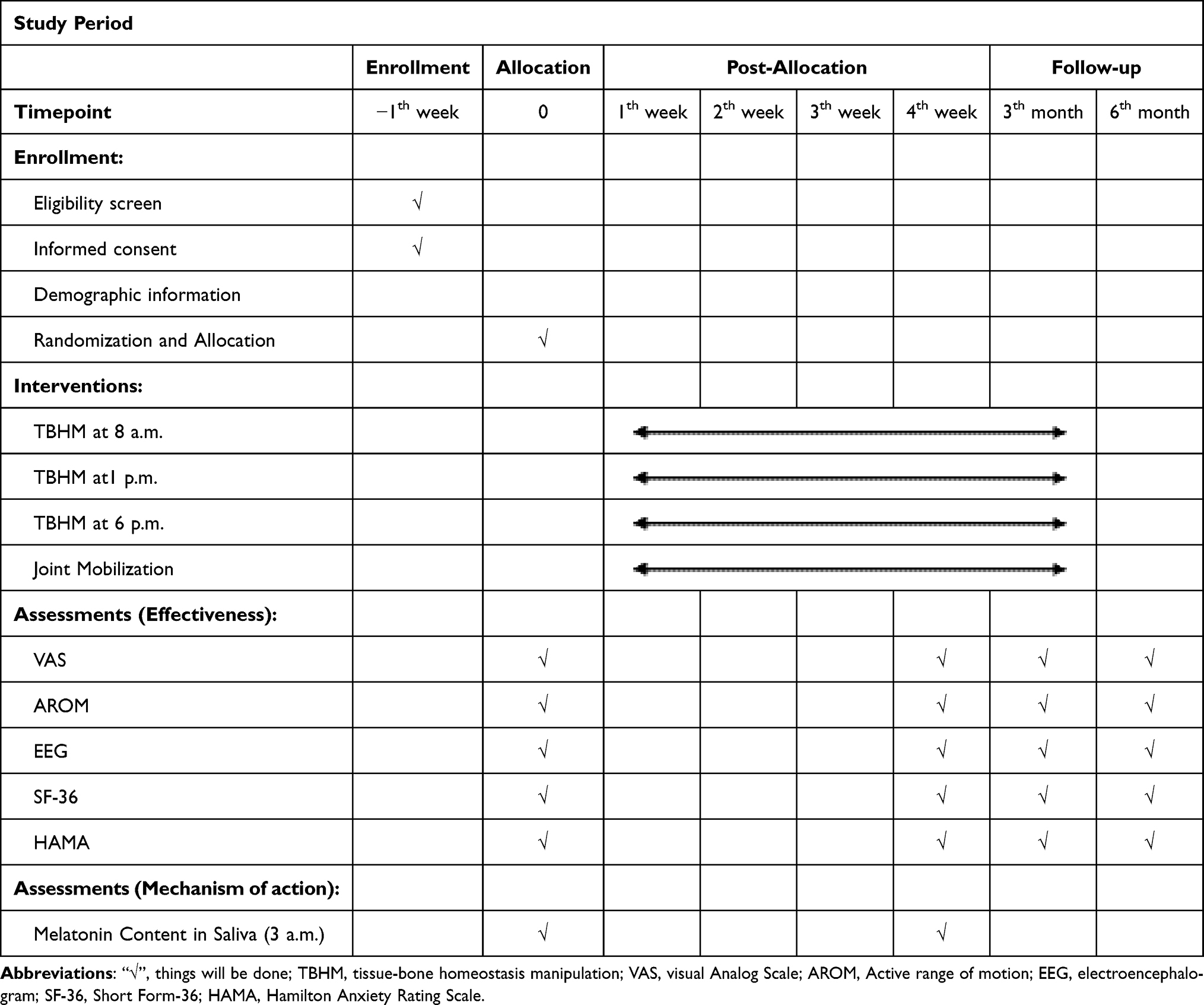 |
Table 1 Schedule of Enrolment, Intervention and Assessments |
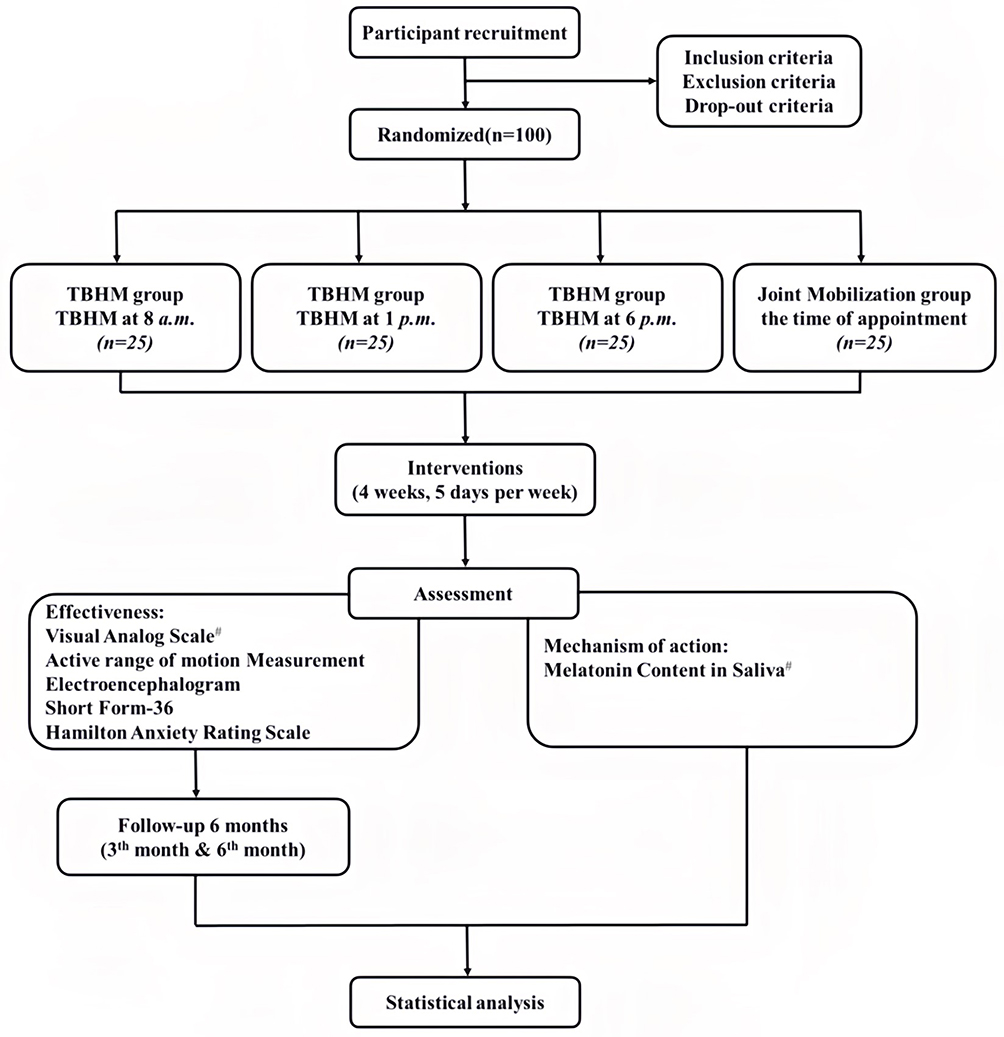 |
Figure 1 A concise flowchart of the entire study. #Primary outcomes, other indicators are secondary outcome. Abbreviation: TBHM, Tissue-bone homeostasis manipulation. |
Sample Size Calculation
In this study, we conducted an initial calculation of the sample size based on a two-way repeated measures analysis of variance (ANOVA) using G*Power software (v3.1.9.2, University Dusseldorf, Germany). The expected effect size (η² = 0.3),36 significance level (alpha = 0.05), power (1-β = 0.80), number of groups (k = 4), the number of repeated measurements per subject (n_rep = 4), and the sample size was calculated as 80. Additionally, to be conservative, we took into account a 20% dropout rate, totaling 100 subjects for the study.
Participants
Inclusion Criteria
- Fulfill the diagnostic standards for KOA according to both traditional Chinese and Western medical principles;37
- Aged between 50 and 75 years old;
- With radiological manifestations of K-L grade II–III of the disease;38
- Voluntarily participate in this trial and sign the informed consent form.
Exclusion Criteria
- Patients who have undergone knee surgery with implants;
- Patients with knee joint infection and obvious swelling;
- Patients with mental illness who are unable to communicate;
- Patients with malignant tumors and bone metastasis;
- Patients who have undergone other treatment methods for knee joints within 3 months;
- Patients who are not suitable for sleep electroencephalogram (EEG) examination include those with severe scalp injuries.
Drop-Out Criteria
- Inability to return for treatment due to any reason.
- Adverse events arising from the treatment.
- Participants who receive alternative intervention treatments for KOA or other interventions that may interfere with the results of this study (for example, employing intra-articular or oral corticosteroids; having undergone knee surgery, knee or hip replacement surgery, or tibial osteotomy; engaging in consistent physical activity).
Recruitment, Enrollment and Randomization Procedures
All patients with KOA who participate will be recruited from the Orthopedics or Rehabilitation Departments of Shanghai Seventh People’s Hospital, as well as from the surrounding communities. Recruitment methods will encompass bedside briefings by doctors, the posting of posters, online advertisements, and the distribution of flyers. We will discuss the study details and considerations with potential participants. After patients voluntarily sign the informed consent form, they will be invited to join the research. Recruitment is set to begin on July 1, 2025, with an expected enrollment of 100 participants by that time.
In this study, we will adopt a stratified randomization strategy based on gender, age, and K-L grade to evenly allocate 100 eligible participants into four experimental groups in a 1:1:1:1 ratio. The specific stratified random sampling process is as follows: Firstly, participants will be divided into male and female groups according to their gender. Secondly, within the male and female groups, we will further categorize them into two age groups: those under 60 years old (≤60 ages) and those 60 years old and above (>60 ages). Subsequently, these two age groups, divided by gender, will be further subdivided into four subgroups based on K-L grade (Grade II and Grade III), resulting in a total of eight subgroups. Participants within these subgroups will then be randomly assigned to four TBHM groups at different time points (8 a.m., 1 p.m., 6 p.m.) and a joint mobilization group. To ensure the fairness and accuracy of the final results, we will also rearrange all participants into four new experimental groups, minimizing potential biases. The entire randomization process will be conducted by an independent research assistant who has no direct contact with the participants and has not participated in data collection. This assistant will use sealed opaque envelopes to hide the serial numbers to ensure the fairness and accuracy of the random allocation.
Allocation Concealment and Blinding
In implementing the allocation concealment in the study, we adopted sealed opaque envelopes to hide the serial numbers, ensuring the fairness of the allocation process. After all participants complete the baseline assessment, independent researchers will follow the established order to open the envelopes one by one, effectively preventing the occurrence of selective bias. Given the intuitive nature of the TBHM and joint mobilization interventions, owing to the nature of the intervention, it is inevitable that both therapists and patients will be aware of the allocation of the treatment. However, to maintain the objectivity of the study, we have adopted a blinding strategy, ensuring that the evaluators and statisticians responsible for data collection and final statistical analysis remain blind to the intervention allocation. This approach aims to eliminate implementation bias and measurement bias, ensuring the accuracy of the study results. Importantly, these evaluators and statisticians will not be involved in the recruitment process of participants, ensuring that they maintain an objective and neutral attitude throughout the study.
Interventions
TBHM35
1) Muscle relaxation: The patient lies on the back and relaxes. The therapist applies the rolling, kneading and pressing techniques to the muscles on the medial and lateral sides of the thigh as well as the posterior muscles of the calf, lasting for approximately 5 minutes. 2) Acupoint pressing: Select acupoints such as “Liangqiu” (RN23), “Xuehai” (SP10), “Neixiyan”, “Waixiyan”, “Yanglingquan” (GB34), “Zusanli” (ST36) and “Ashi” points for pressing, with the duration of about 5 minutes. The pressing force should be within the tolerable range of each patient, avoiding causing pain, and it is advisable to produce a sensation of soreness and the so-called “deqi” feeling. 3) Release of the infrapatellar fat pad: The patient lies on the back and relaxes. The therapist first slightly bends the affected knee joint of the patient, places both thumbs on the midpoint of the patellar tendon, and the remaining four fingers on the back of the knee joint. Subsequently, the therapist lifts the heel of the affected side, presses firmly with both thumbs towards the femoral condyles, and simultaneously lifts the affected leg to the knee extension position. 4) Manipulation of the patella: The patient lies on the back and relaxes. The therapist places one thumb on the outer side of the patella to slightly fix it inwards. The palm of the other hand is placed on the upper and lower edges of the patella and pushes it along its natural movement direction to the maximum displacement. After maintaining for a few seconds, it returns to its original position, repeating the movement three times. 5) Rotation of the tibia: The patient lies on the back and slightly flexes the knee joint. The therapist places the affected thigh of the subject on the edge of the bed, places both thumbs on the inner and outer knee eyes, and the remaining four fingers on the back of the popliteal fossa. Then, the tibia is rotated inward and outward to the maximum extent, maintained for a few seconds and then relaxed. This manipulation is repeated three times.
Previous studies have shown that different exercise time points have different effects on melatonin secretion, mainly in the morning and afternoon.29 In addition, from the perspective of subject compliance, this study set the intervention time points of TBHM to three nodes: 8 am, 1 pm, and 6 pm.
These techniques are performed once a day, 5 days per week, with each session lasting 20 minutes, and the whole treatment period is 4 weeks. During the process of manual intervention, communicate with the patients and adjust the strength of the techniques in a timely manner.
Joint Mobilization
1) Long-axis Traction: The patient takes a sitting position with the affected knee flexed and the lower leg naturally hanging over the edge of the bed. The therapist grasps the ankle joint of the affected side and pulls the lower leg in the direction towards the foot. Each traction lasts for about 15 seconds and is repeated 5 times. 2) Anterior-Posterior Glide: The patient takes a sitting position and flexes the affected leg to the maximum extent. The therapist uses his own bilateral calves to firmly clamp and fix the patient’s lower leg in this position. The therapist places both hands on the front of the proximal tibia. By leaning the upper body forward to transfer force while keeping the hands stationary, the therapist uses the strength of the upper body to push the proximal tibia posteriorly. Each glide lasts for about 15 seconds and is repeated 5 times. 3) Posterior-Anterior Glide: The patient takes a supine position and keeps the affected hip and knee flexed. The therapist sits on the affected side of the bed, places the thumb on the proximal tibia and the remaining four fingers in the popliteal fossa. After the hands are properly fixed, the therapist leans backward, using the strength of the upper body to push the tibia anteriorly. Each glide lasts for about 15 seconds and is repeated 5 times.
These operations are performed once a day, 5 days per week. The complete treatment session lasts for 20 minutes each time and the manipulation force is about grade 3 to 4, with the specific force adjusted according to the patient’s tolerance. The whole treatment period lasts for 4 weeks. It should be noted that, unlike the TBHM group, the treatment time of the joint mobilization group is determined according to each participant’s appointment time. The reason for choosing joint mobilization as a routine control intervention is that previous studies have shown that joint mobilization has been widely used in the clinical rehabilitation treatment of KOA and has become a routine and mature rehabilitation treatment method. However, there are differences between joint mobilization and TBHM. The treatment of TBHM focuses on the coordination of muscles and bones, loosening the muscles first and then adjusting the bones; while the treatment of joint mobilization focuses on the adjustment of bones and then taking into account the loosening of muscles. Moreover, it has been found in past studies that the treatment effect of joint mobilization does not vary significantly due to differences in treatment time.39
Outcome Measurements
The participants will be blindly assessed by other physical therapists according to the different evaluations shown in Table 1 at different time points. In addition, baseline information including age, gender, symptoms, disease severity, duration, prior treatments, and medication will be recorded using a questionnaire (at Week 0). All assessment scales in Table 1 will also be recorded at Week 0, along with EEG and saliva sample collection. The saliva samples will be collected at 3 a.m. The primary endpoint is at Week 4, with the same assessment and collection time points as Week 0. Furthermore, we plan to conduct follow-up visits at the 3rd and 6th months after the completion of the intervention measures to continuously monitor efficacy indicators such as VAS, ensuring that the time and location of assessment remain consistent with the 0th week. All adverse effects will be documented in real-time throughout the study.
Effectiveness
Primary Outcomes
Visual Analog Scale (VAS)
The VAS will be used as the primary outcome measure for evaluating the improvement of knee joint pain.40 In the context of musculoskeletal disorders, the VAS has proven to be reliable and valid.40 To evaluate the clinical significance of VAS score variations, the Minimal Clinically Important Difference (MCID) will be utilized, and it has been set at 1.16 according to existing research.41 Participants will be evaluated according to the assessment schedule of the experimental protocol and indicate their pain level on a number line ranging from 0 to 10.
Secondary Outcomes
Active Range of Motion Measurement (AROM)
Active range of motion will be employed to assess pain relief and restoration of motor function.42 Under healthy conditions, joints possess a normal range of motion. However, the pain induced by KOA frequently leads to abnormal movement patterns and consequently an abnormal range of joint motion. Therefore, in this experiment, the change in the range of joint motion will be measured as an evaluation criterion.
Short Form-36 (SF-36)
The SF-36 scale consists of 8 aspects and 35 items.42 The score of this scale is positively correlated with the quality of life. That is to say, the higher the score is, the better the quality of life will be. With the help of the SF-36 scale, the changes in the health level of subjects before, during and after the intervention can be evaluated comprehensively and objectively.
Electroencephalogram (EEG)
The wireless portable electroencephalogram (EEG) acquisition device will be used to record the EEG data of subjects before and after the intervention.43,44 Neural oscillations are endogenous rhythmic electrophysiological activities in the brain and a characteristic of the brain state. According to their frequency ranges, they can be mainly divided into delta oscillations (1–4 Hz), theta oscillations (4–8 Hz), alpha oscillations (8–12 Hz), beta oscillations (15–30 Hz) and gamma oscillations (30–100 Hz).45 Among them, the theta and beta frequency bands are related to KOA pain, and the alpha frequency band is related to sleep.46 Chronic pain can also disrupt normal brain electrical activity. Studies have shown that patients with greater pain intensity and more severe KOA symptoms exhibit higher beta power and lower theta activity in the frontal central area. In contrast, subjects with lower KOA severity and less pain show higher theta oscillation ability.47 By monitoring and analyzing the percentage of energy occupied by each frequency band of the EEG, pain degree of the subjects can be evaluated in a more objective manner. In the experiment, during the data analysis process, the focus will be placed on the changes in power spectral density (PSD) of different frequency bands and the functional connections between different brain regions.
Hamilton Anxiety Rating Scale (HAMA)
The HAMA scale is a crucial tool for assessing the severity of anxiety, encompassing 14 items that cover both psychic and somatic anxiety.48 This study utilizes the HAMA to evaluate patients’ anxiety levels before and after treatment with TBHM, aiming to explore its effectiveness in relieving pain and improving anxiety symptoms.49
Mechanism of Action
Primary Outcomes
Melatonin Content in Saliva
Melatonin plays a crucial role in regulating the sleep-wake cycle of the human body. Saliva samples can be used to evaluate the changes in melatonin levels.29 Since the secretion of melatonin is inversely proportional to the intensity of light and the timing of exercise has a significant impact on the secretion of melatonin, and its secretion reaches a peak between 3 a.m. and 4 a.m. Therefore, saliva samples are collected from participants at 3 a.m., and measuring the melatonin levels therein can help us understand the subjects’ melatonin secretion patterns and further reveal their sleep-wake cycles. The saliva sampling method of the subjects was uniformly trained by professional laboratory physicians for researchers or their immediate family members. When the subjects were inpatients, the researchers collected the samples, and when they were outpatients, their immediate family members collected the samples. The subjects were awakened by researchers or their immediate family members at 03:00 in the morning of the next day and the samples were collected in a low-light environment (roughly the time for the peak of melatonin secretion detection), and the saliva was collected into a sterile 10 mL polypropylene conical tube by passive drip method, and then the samples were frozen at −80°C for subsequent analysis of the melatonin concentration in the saliva.29 Salivary melatonin concentrations were measured by enzyme-linked immunosorbent assay (ELISA) (Jiancheng Nanjing). Melatonin was extracted as per manufacturer protocol (Jiancheng Nanjing).
Safety and Adverse Events
During the study, the safety officer was responsible for documenting all adverse events that occurred in detail and promptly reporting them to relevant departments. At the same time, we fully disclosed to all participants the potential risks that might exist in the study and listed these risks in detail in the informed consent form to ensure that each participant could make decisions based on a full understanding of the risks.
Statistical Analysis
Statistical analysis will be conducted using IBM SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). The results will be analyzed using intention-to-treat (ITT) analysis, which interpolates using the last observation carried forward in case of missing data. For normally distributed data, continuous variables will be described as mean ± standard deviation, or for non-normal distributions, continuous variables will be described as median and interquartile range, while categorical variables will be described as frequencies. For continuous variables that satisfy the assumptions of normal distribution and homogeneity of variance, we will use two-way repeated measures analysis of variance (ANOVA); if not, we will use the Wilcoxon test. Categorical variables will be analyzed using the chi-square test. In addition, the correlation between the primary and secondary outcomes with salivary melatonin levels was evaluated by Pearson correlation coefficient, and the correlation coefficient was graded as follows: low correlation (r < 0.30), moderate correlation (0.30 < r < 0.60), and high correlation (r > 0.60).50 Results will be considered statistically significant when the p-value is less than 0.05. Furthermore, the preprocessing and analysis of EEG data will be performed using MATLAB 2022b software. The results of the statistical analysis will be processed through IBM SPSS Statistics 25, and the final data visualization will be achieved using the EEGLAB toolbox to facilitate our intuitive understanding and analysis of the data.
Patient and Public Involvement
The research concept was developed by the research team. The proposal was prepared with contributions from patients with KOA, physiotherapists, orthopedic doctors, and experts from the Shanghai Rehabilitation Medicine Society, all of whom participated through face-to-face interviews. Additionally, based on feedback from the research protocol, any completely unresolved concerns that were not addressed in the initially proposed draft will be revised and enhanced to guarantee the intervention’s safety and suitability. Additionally, the dissemination of the standardized protocol, technical procedures, and clinical applications will occur through peer-reviewed journals and the Shanghai Rehabilitation Medicine Society.
Discussion
KOA is a common chronic degenerative disease that severely affects the patient’s quality of life due to pain.51 Currently, anti-inflammatory and analgesic drugs (including glucocorticoids and opioids52 as well as surgical interventions are widely used in clinical practice, but these methods are often accompanied by problems such as drug addiction, drug tolerance, and additional surgical risks. Traditional rehabilitation methods have limited efficacy in treating pain, depression, and sleep disorders caused by KOA.53 It is worth noting that our team’s previous experiment has shown that TBHM has superior therapeutic effects compared to conventional rehabilitation therapy.35
Since KOA pain is the main cause of motor dysfunction,54 and pain is significantly influenced by sleep and circadian rhythm,55 it is of great significance to explore the correlation between circadian rhythm and the treatment of KOA. Circadian rhythm type is one of the main methods to assess individual circadian rhythm, and there are many ways to reflect circadian rhythm to a certain extent, such as melatonin content in saliva: melatonin is secreted by the pineal gland, and its secretion shows an obvious circadian rhythm, with the secretion amount at night being significantly higher than that in the daytime. It plays a crucial role in regulating the sleep-wake cycle, etc.,56,57 The change in the content of melatonin in saliva is closely related to the body’s biological clock.58,59 When the circadian rhythm is disrupted, the secretion pattern of salivary melatonin will also change accordingly.60 Through the detection and analysis of relevant indicators such as salivary melatonin, it is helpful to gain an in-depth understanding of the changes in the circadian rhythm of KOA patients, and then provide new ideas and bases for the treatment of KOA. For example, personalized treatment plans can be formulated according to the characteristics of the circadian rhythm. When the test results show that after TBHM intervention in the morning, the patient’s nocturnal melatonin secretion is the highest, it indicates that the best time to arrange treatment in the morning. When other results are obtained, a similar mechanism can be used to reasonably arrange the best treatment time, thereby better relieving pain, improving motor dysfunction, and improving patients’ quality of life, and providing a reference for future KOA clinical guidelines.
This study aims to apply “circadian rhythm” as a guideline to select different times for administering TBHM. We will utilize a comprehensive approach including EEG and measurement of melatonin levels in saliva to reveal the optimal timing for implementing this technique, providing further guidance for clinical applications. Additionally, based on this theory, we will also delve into the relevant brain mechanisms of TBHM in treating KOA.
While this study will provide valuable preliminary evidence, future research still needs to investigate the impact of treatment at different time points on other biomarkers such as inflammatory factors and stress hormones, which will help us gain a more comprehensive understanding of the mechanism of how circadian rhythm affects the treatment effect of KOA. Additionally, long-term follow-up studies are also required to evaluate the long-term effectiveness of this time-optimized treatment strategy and the sustained improvement in patients’ quality of life.
Ethics Approval and Informed Consent
Ethical approval for this study has been granted by the Ethics Committee of Shanghai Seventh People’s Hospital (2024-7th-HIRB-007) and registered in the Chinese Clinical Trial Registry (ChiCTR2400080820). All participants are required to provide signed informed consent prior to the commencement of the study. Furthermore, all procedures will be executed in compliance with the Declaration of Helsinki.
Generative AI Statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Acknowledgments
The author wishes to extend sincere thanks to the rehabilitation physicians and therapists at Shanghai Seventh People’s Hospital. Your contributions as members of the patient public involvement group, along with those of many others, are greatly appreciated.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is supported by the General Project of Shanghai Pudong New Area Science and Economy Commission (PKJ2023-Y61) and The Young Medical Talents Training Program of Shanghai Pudong New Area Health Commission (PWRq2024-36).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Favero M, El-Hadi H, Belluzzi E, et al. Infrapatellar fat pad features in osteoarthritis: a histopathological and molecular study. Rheumatology. 2017;56(10):1784–1793. doi:10.1093/rheumatology/kex287
2. Battistelli M, Favero M, Burini D, et al. Morphological and ultrastructural analysis of normal, injured and osteoarthritic human knee menisci. Eur J Histochem. 2019;63(1):2998. doi:10.4081/ejh.2019.2998
3. Roos EM, Arden NK. Strategies for the prevention of knee osteoarthritis. Nat Rev Rheumatol. 2016;12(2):92–101. doi:10.1038/nrrheum.2015.135
4. Belluzzi E, El Hadi H, Granzotto M, et al. Systemic and local adipose tissue in knee osteoarthritis. J Cell Physiol. 2017;232(8):1971–1978. doi:10.1002/jcp.25716
5. Li M, Xia Q, Nie Q, Ding L, Huang Z, Jiang Z. Burden of knee osteoarthritis in China and globally: 1990–2045. BMC Musculoskelet Disord. 2025;26(1):582. doi:10.1186/s12891-025-08858-8
6. Zeng L, Zhou G, Yang W, Liu J. Guidelines for the diagnosis and treatment of knee osteoarthritis with integrative medicine based on traditional Chinese medicine. Front Med. 2023;10:1260943. doi:10.3389/fmed.2023.1260943
7. Timo-Iaria C, Negrao N, Schmidek WR, Hoshino K, Lobato de Menezes CE, Leme da Rocha T. Phases and states of sleep in the rat. Physiol Behav. 1970;5(9):1057–1062. doi:10.1016/0031-9384(70)90162-9
8. Ahn H, Galle K, Mathis KB, et al. Feasibility and efficacy of remotely supervised cranial electrical stimulation for pain in older adults with knee osteoarthritis: a randomized controlled pilot study. J Clin Neurosci. 2020;77:128–133. doi:10.1016/j.jocn.2020.05.003
9. Taylor-Gjevre RM, Gjevre JA, Nair B, Skomro R, Lim HJ. Components of sleep quality and sleep fragmentation in rheumatoid arthritis and osteoarthritis. Musculoskeletal Care. 2011;9(3):152–159. doi:10.1002/msc.208
10. Ohayon MM. Relationship between chronic painful physical condition and insomnia. J Psychiatr Res. 2005;39(2):151–159. doi:10.1016/j.jpsychires.2004.07.001
11. Salwen JK, Smith MT, Finan PH. Mid-treatment sleep duration predicts clinically significant knee osteoarthritis pain reduction at 6 months: effects from a behavioral sleep medicine clinical trial. Sleep. 2017;40(2):zsw064. doi:10.1093/sleep/zsw064
12. Vitiello MV, McCurry SM, Shortreed SM, et al. Short-term improvement in insomnia symptoms predicts long-term improvements in sleep, pain, and fatigue in older adults with comorbid osteoarthritis and insomnia. Pain. 2014;155(8):1547–1554. doi:10.1016/j.pain.2014.04.032
13. Koffel E, Kroenke K, Bair MJ, Leverty D, Polusny MA, Krebs EE. The bidirectional relationship between sleep complaints and pain: analysis of data from a randomized trial. Health Psychol. 2016;35(1):41–49. doi:10.1037/hea0000245
14. Logan RW, McClung CA. Rhythms of life: circadian disruption and brain disorders across the lifespan. Nat Rev Neurosci. 2019;20(1):49–65. doi:10.1038/s41583-018-0088-y
15. Bhaskar R, Narayanan KB, Singh KK, Han SS. Mapping the connection between circadian rhythms, metabolism, and neurodegeneration: exploring therapeutic strategies. Curr Alzheimer Res. 2025. doi:10.2174/0115672050381989250626071304
16. Du Z, You X, Wu D, Huang S, Zhou Z. Rhythm disturbance in osteoarthritis. Cell Commun Signal. 2022;20(1):70. doi:10.1186/s12964-022-00891-7
17. Bellamy N, Sothern RB, Campbell J. Rhythmic variations in pain perception in osteoarthritis of the knee. J Rheumatol. 1990;17(3):364–372.
18. Patke A, Young MW, Axelrod S. Molecular mechanisms and physiological importance of circadian rhythms. Nat Rev Mol Cell Biol. 2020;21(2):67–84. doi:10.1038/s41580-019-0179-2
19. Dibner C, Schibler U, Albrecht U. The mammalian circadian timing system: organization and coordination of central and peripheral clocks. Annu Rev Physiol. 2010;72:517–549. doi:10.1146/annurev-physiol-021909-135821
20. Bishehsari F, Voigt RM, Keshavarzian A. Circadian rhythms and the gut microbiota: from the metabolic syndrome to cancer. Nat Rev Endocrinol. 2020;16(12):731–739. doi:10.1038/s41574-020-00427-4
21. Swanson CM, Shea SA, Wolfe P, et al. Bone turnover markers after sleep restriction and circadian disruption: a mechanism for sleep-related bone loss in humans. J Clin Endocrinol Metab. 2017;102(10):3722–3730. doi:10.1210/jc.2017-01147
22. Song C, Wang J, Kim B, et al. Insights into the role of circadian rhythms in bone metabolism: a promising intervention target? Biomed Res Int. 2018;2018:9156478. doi:10.1155/2018/9156478
23. Guo B, Yang N, Borysiewicz E, et al. Catabolic cytokines disrupt the circadian clock and the expression of clock-controlled genes in cartilage via an NFsmall ka, CyrillicB-dependent pathway. Osteoarthritis Cartilage. 2015;23(11):1981–1988. doi:10.1016/j.joca.2015.02.020
24. Song X, Ma T, Hu H, et al. Chronic circadian rhythm disturbance accelerates knee cartilage degeneration in rats accompanied by the activation of the canonical Wnt/beta-catenin signaling pathway. Front Pharmacol. 2021;12:760988. doi:10.3389/fphar.2021.760988
25. Miranda-Riestra A, Estrada-Reyes R, Torres-Sanchez ED, Carreno-Garcia S, Ortiz GG, Benitez-King G. Melatonin: a neurotrophic factor? Molecules. 2022;27(22):7742. doi:10.3390/molecules27227742
26. Reiter RJ. Melatonin: clinical relevance. Best Pract Res Clin Endocrinol Metab. 2003;17(2):273–285. doi:10.1016/s1521-690x(03)00016-2
27. Goh VH, Tong TY, Lim CL, Low EC, Lee LK. Effects of one night of sleep deprivation on hormone profiles and performance efficiency. Mil Med. 2001;166(5):427–431.
28. Kennaway DJ. Measuring melatonin by immunoassay. J Pineal Res. 2020;69(1):e12657. doi:10.1111/jpi.12657
29. Carlson LA, Pobocik KM, Lawrence MA, Brazeau DA, Koch AJ. Influence of exercise time of day on salivary melatonin responses. Int J Sports Physiol Perform. 2019;14(3):351–353. doi:10.1123/ijspp.2018-0073
30. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, Hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27(11):1578–1589. doi:10.1016/j.joca.2019.06.011
31. Peng H, Ou A, Huang X, et al. Osteotomy around the knee: the surgical treatment of osteoarthritis. Orthop Surg. 2021;13(5):1465–1473. doi:10.1111/os.13021
32. Poenaru D, Sandulescu MI, Potcovaru CG, Cinteza D. High-Intensity Laser Therapy in Pain Management of Knee Osteoarthritis. Biomedicines. 2024;12(8):1679. doi:10.3390/biomedicines12081679
33. Silvernail JL, Deyle GD, Jensen GM, et al. Orthopaedic manual physical therapy: a modern definition and description. Phys Ther. 2024;104(6):pzae036. doi:10.1093/ptj/pzae036
34. Pehlivan S, Karadakovan A. Effects of aromatherapy massage on pain, functional state, and quality of life in an elderly individual with knee osteoarthritis. Jpn J Nurs Sci. 2019;16(4):450–458. doi:10.1111/jjns.12254
35. Zhang ZQ, Ding YW, Tao Y, et al. Efficacy of tissue-bone homeostasis manipulation on the gait and knee function for the patients with knee osteoarthritis: a randomized controlled trial. BMC Musculoskelet Disord. 2024;25(1):794. doi:10.1186/s12891-024-07896-y
36. Cheung DST, Yeung WF, Suen LK, et al. Self-administered acupressure for knee osteoarthritis in middle-aged and older adults: a pilot randomized controlled trial. Acupunct Med. 2020;38(2):75–85. doi:10.1177/0964528419883269
37. Altman RD. Classification of disease: osteoarthritis. Semin Arthritis Rheum. 1991;20(6 Suppl 2):40–47. doi:10.1016/0049-0172(91)90026-v
38. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502. doi:10.1136/ard.16.4.494
39. Yacks CA, Kacmarcik CMY, Archambeau CA, Barrios JA. Effect duration of a self-applied talocrural joint mobilization on restricted dorsiflexion: a repeated measures design. J Man Manip Ther. 2025;33(1):54–62. doi:10.1080/10669817.2024.2424545
40. Wewers ME, Lowe NK. A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health. 1990;13(4):227–236. doi:10.1002/nur.4770130405
41. Lai MH, Xu HC, Ding YW, Yang K, Xu XP, Jiang LM. Effectiveness and mechanism of action of rTMS combined with quadriceps strength training in individuals with knee osteoarthritis: study protocol for a randomized controlled trial. BMC Musculoskelet Disord. 2024;25(1):37. doi:10.1186/s12891-023-07146-7
42. Svensson M, Lind V, Löfgren Harringe M. Measurement of knee joint range of motion with a digital goniometer: a reliability study. Physiother Res Int. 2019;24(2):e1765. doi:10.1002/pri.1765
43. Olmo Arroyo J, De Sanctis L, Sidhoum L, et al. Quality of poly(somno)graphy recordings in children. J Sleep Res. 2021;30(4):e13241. doi:10.1111/jsr.13241
44. Durka PJ, Klekowicz H, Blinowska KJ, Szelenberger W, Niemcewicz S. A simple system for detection of EEG artifacts in polysomnographic recordings. IEEE Trans Biomed Eng. 2003;50(4):526–528. doi:10.1109/TBME.2003.809476
45. Buzsaki G, Draguhn A. Neuronal oscillations in cortical networks. Science. 2004;304(5679):1926–1929. doi:10.1126/science.1099745
46. Wu R, Ma H, Hu J, et al. Electroacupuncture stimulation to modulate neural oscillations in promoting neurological rehabilitation. Brain Res. 2024;1822:148642. doi:10.1016/j.brainres.2023.148642
47. Simis M, Imamura M, Pacheco-Barrios K, et al. EEG theta and beta bands as brain oscillations for different knee osteoarthritis phenotypes according to disease severity. Sci Rep. 2022;12(1):1480. doi:10.1038/s41598-022-04957-x
48. Thompson E. Hamilton Rating Scale for Anxiety (HAM-A). Occup Med. 2015;65(7):601. doi:10.1093/occmed/kqv054
49. Xu H, Zhao C, Guo G, et al. The effectiveness of tuina in relieving pain, negative emotions, and disability in knee osteoarthritis: a randomized controlled trial. Pain Med. 2023;24(3):244–257. doi:10.1093/pm/pnac127
50. Monticone M, Capone A, Frigau L, et al. Development of the Italian version of the High-Activity Arthroplasty Score (HAAS-I) following Hip and knee total arthroplasty: cross-cultural adaptation, reliability, validity and sensitivity to change. J Orthop Surg Res. 2018;13(1):81. doi:10.1186/s13018-018-0782-5
51. Chen N, Wang J, Mucelli A, Zhang X, Wang C. Electro-acupuncture is beneficial for knee osteoarthritis: the evidence from meta-analysis of randomized controlled trials. Am J Chin Med. 2017;45(5):965–985. doi:10.1142/s0192415x17500513
52. Resmini G, Ratti C, Canton G, Murena L, Moretti A, Iolascon G. Treatment of complex regional pain syndrome. Clin Cases Miner Bone Metab. 2015;12(Suppl 1):26–30. doi:10.11138/ccmbm/2015.12.3s.026
53. Plavoukou T, Iosifidis M, Papagiannis G, Stasinopoulos D, Georgoudis G. The effectiveness of telerehabilitation in managing pain, strength, and balance in adult patients with knee osteoarthritis: systematic review. JMIR Rehabil Assist Technol. 2025;12:e72466. doi:10.2196/72466
54. Ma Y, Chen YS, Liu B, Sima L. Ultrasound-guided radiofrequency ablation for chronic osteoarthritis knee pain in the elderly: a randomized controlled trial. Pain Physician. 2024;27(3):121–128.
55. Crodelle J, Vanty C, Booth V. Modeling homeostatic and circadian modulation of human pain sensitivity. Front Neurosci. 2023;17:1166203. doi:10.3389/fnins.2023.1166203
56. Tan DX, Xu B, Zhou X, Reiter RJ. Pineal calcification, melatonin production, aging, associated health consequences and rejuvenation of the pineal gland. Molecules. 2018;23(2):301. doi:10.3390/molecules23020301
57. Fowler S, Hoedt EC, Talley NJ, Keely S, Burns GL. Circadian rhythms and melatonin metabolism in patients with disorders of gut-brain interactions. Front Neurosci. 2022;16:825246. doi:10.3389/fnins.2022.825246
58. Pundir M, De Rosa MC, Lobanova L, et al. Structural properties and binding mechanism of DNA aptamers sensing saliva melatonin for diagnosis and monitoring of circadian clock and sleep disorders. Anal Chim Acta. 2023;1251:340971. doi:10.1016/j.aca.2023.340971
59. Arendt J. Melatonin and human rhythms. Chronobiol Int. 2006;23(1–2):21–37. doi:10.1080/07420520500464361
60. Carpi M, Fernandes M, Risino I, et al. Alteration of circadian sleep-wake rhythm and salivary melatonin secretion in idiopathic/isolated REM sleep behavior disorder: preliminary evidence. Sleep Med. 2024;119:135–138. doi:10.1016/j.sleep.2024.04.020
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.