Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Effects of Proprioceptive Neuromuscular Facilitation Stretching Combined with Aerobic Training on Pulmonary Function in COPD Patients: A Randomized Controlled Trial
Authors Liu K, Yu X ![]() , Cui X, Su Y, Sun L, Yang J, Han W
, Cui X, Su Y, Sun L, Yang J, Han W ![]()
Received 22 January 2021
Accepted for publication 29 March 2021
Published 13 April 2021 Volume 2021:16 Pages 969—977
DOI https://doi.org/10.2147/COPD.S300569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Kai Liu,1,* Xinjuan Yu,2,* Xuefen Cui,2 Yi Su,2 Lixin Sun,3 Jiulong Yang,4 Wei Han2
1Department of Rehabilitation, Qingdao Municipal Hospital, Qingdao University, Qingdao, People’s Republic of China; 2Department of Respiratory and Critical Medicine, Respiratory Disease Key Laboratory of Qingdao, Qingdao Municipal Hospital, Qingdao University, Qingdao, People’s Republic of China; 3Department of Anesthesia, Qingdao Municipal Hospital, Qingdao University, Qingdao, People’s Republic of China; 4Hospital Office, Qingdao Municipal Hospital, Qingdao University, Qingdao, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Han
Department of Pulmonary and Critical Care Medicine, Qingdao Municipal Hospital, Qingdao University, No. 5 Donghaizhong Road, Qingdao, Shandong, 266071, People’s Republic of China
Tel +86 532 85937579
Email [email protected]
Jiulong Yang
Hospital Office, Qingdao Municipal Hospital, Qingdao University, No. 5 Donghaizhong Road, Qingdao, Shandong, 266071, People’s Republic of China
Tel +86 532 88905509
Email [email protected]
Background: The proprioceptive neuromuscular facilitation (PNF) stretching could improve the contractile capacity of respiratory muscles, but the effect on pulmonary function, when it is combined with aerobic training, remains unknown.
Objective: To evaluate the effect of PNF combined with aerobic training on respiratory symptoms, pulmonary function and neck/shoulder mobility in patients with COPD.
Design: Randomized controlled trial.
Participants: Fifty-five COPD patients were randomly divided into PNF group (n=28) and control group (n=27).
Intervention: On the basis of conventional treatment, the control group performed 30 min aerobic training on a treadmill, while the PNF group added 10-minute PNF stretching 3 times every training day. Both groups did their training in 5 days per week for 6 weeks.
Measures: Measures were taken before and after 6 weeks of training. COPD Assessment Test (CAT), dyspnea Visual Analog Scale (VAS), forced vital capacity (FVC), forced expiratory volume in first second (FEV1), inspiratory capacity (IC), inspiratory reserve volume (IRV), 6-minute walk test (6MWT), the range of motion (ROM) of head protraction, shoulder flexion, and the non-dominant pectoralis minor muscle (PmM) length were measured.
Results: All the indicators of both groups were significantly improved after 6 weeks of intervention except for FVC, FEV1 and PmM length. Compared to the control group, the PNF group showed significant improvement in the CAT score, dyspnea VAS score, IC, IRV, 6MWT, as well as head protraction ROM and shoulder flexion ROM. Furthermore, IC was positively correlated with the head protraction ROM and PmM length (r=0.415, 0.579, P=0.028, 0.001); IRV was positively correlated with the shoulder flexion ROM (r=0.405, P=0.032) in the PNF group.
Conclusion: PNF stretching combined with aerobic training reduces dyspnea and improves some pulmonary function measures, which is associated with neck/shoulder mobility, in COPD patients.
Keywords: chronic obstructive pulmonary disease, proprioceptive neuromuscular facilitation stretching, aerobic training, pulmonary function
Introduction
Chronic obstructive pulmonary disease (COPD) is a disease with high incidence and its importance is growing steadily. It is expected to be the third leading cause of death worldwide.1 The prevalence of COPD among people aged 40 years or older was 8.2% in 2002–2004, and 13.6% in 2014–2015, indicating that COPD has been a public health problem in China.2,3 However, as a common medical problem characterized by persistent respiratory symptoms and airflow limitation, it is worthy of developing an effective rehabilitation method to improve the pulmonary function and relieve the disability of COPD patients.
The loss of pulmonary function in COPD patients is mostly due to the remodeling of airways and pulmonary parenchyma, which leads airflow limitation, bronchoalveolar instability and air trapping, resulting in increased residual volume and end-expiratory lung volume, as well as decreased expiratory reserve volume and inspiratory volume.4 This respiratory condition not only over activates accessory respiratory muscles but also increases the burden on respiratory muscles. It reduces the contraction range of the sarcomere, decreases muscular contractility and viscoelasticity, and results in the relocation of the ribs, leading to the formation of a barrel-shaped chest.5 As the disease progresses, the stiffness of soft tissue and joint in the neck and shoulder gradually shift the patient’s positions, including head protraction, high muscular tension in the neck, enlargement of thoracic kyphosis and shoulder pronation. Moreover, these changes will lead to chest tightness, inspiratory muscle weakness, increased respiratory resistance, severe dyspnea, even affected physical activity and walking ability.6 Stretching can keep muscle and tendon tissues at optimal initial lengths, and reduce the resistance caused by viscoelasticity and stiffness.
Proprioceptive receptors in myofibers and tendon are responsible for perceiving joint angle, muscle length and muscle tension. Proprioceptive neuromuscular facilitation (PNF) is the most common exercise in the field of muscle rehabilitation, but rare in pulmonary rehabilitation.7,8 PNF stretching plays roles in increasing muscle length and joint range of motion (ROM) via inhibiting myotatic reflex.9 A double-blinded cross-over study conducted by Putt et al10 revealed that COPD patients received 2 days PNF stretching on pectoralis major have improved in shoulder motion range and vital capacity with carryover effects. However, this study was limited because it only involved a stretching group, had no control group.
In this study, we assessed the effects of the PNF stretching on the respiratory symptoms, pulmonary function and neck/shoulder mobility in COPD patients in a randomized controlled trial. Meanwhile, the correlation between pulmonary function and neck/shoulder mobility was evaluated.
Methods
Design
This trial was conducted at the Qingdao Municipal Hospital, Qingdao, and registered with the Chinese Clinical Trial Registry (ChiCTR1800018413). The study was approved by the Ethics Committee of Qingdao Municipal Hospital (Approval number: 2018-031). All patients signed on informed consent before the enrollment of this study.
Randomization
Randomization was performed using Microsoft Excel. The procedure was designed by one investigator who was not involved in the other aspects of the protocol. The group allocations were performed using numbered, sealed, opaque envelopes that had been previously prepared for all participants.11
Participants
Adult subjects with moderate-to–severe COPD were recruited between Sep. 2018 and Apr. 2019, in accordance with criteria of Global Initiative for Chronic Obstructive Lung Disease (GOLD) (GOLD II–III). Inclusion criteria were as follows: 1) ratio of forced expiratory volume in first second and forced vital capacity (FEV1/FVC) <0.7, 30% ≤ FEV1% <80%; 2) age >40 years old; 3) BMI: 18–36 kg/m2; 4) stable clinical conditions without any change after medication in 1 month. Exclusion criteria were as follows: 1) acute onset with change after medication in 1 month; 2) serious conditions which require auxiliary supply of oxygen or ventilatory support devices; 3) inability to follow the pulmonary rehabilitation program; 4) cognitive disorders with definite medical history; 5) severe complications, such as previous cardiothoracic surgery. Patients continued to take their own medication, which could include a LAMA, a LABA, or an inhaled glucocorticoid alone or in combination, during the study. All patients who met the eligibility criteria were randomly divided into PNF group and control group.
Pulmonary Rehabilitation Program
All patients underwent a conventional pulmonary rehabilitation program comprising controlled breathing techniques, expectoration training, and a personalized aerobic exercise schedule 30 minutes per day for 6 weeks (5 days per week). The patients of PNF group received 10-minute PNF stretching 3 times per training day in addition. Two physical therapists assisted the training, and the other two physical therapists evaluated the training effect independently.
Stretching Method
Stretching was applied to scalenus, sternocleidomastoid, trapezius muscle, pectoralis major, pectoralis minor, internal intercostal muscles, anterior serratus muscle and musculus rectus abdominis for 10 minutes, 3 times per day (Table 1). The specific method was the hold-relax method of PNF stretching. The therapist first stretched the muscles to the maximum length the patient could tolerate. The muscles had 3 s isometric contraction against resistance, and then relaxed. The therapist then applied 15 s stretching on the muscles. All the muscles were stretched in turn. These procedures were repeated three times.12
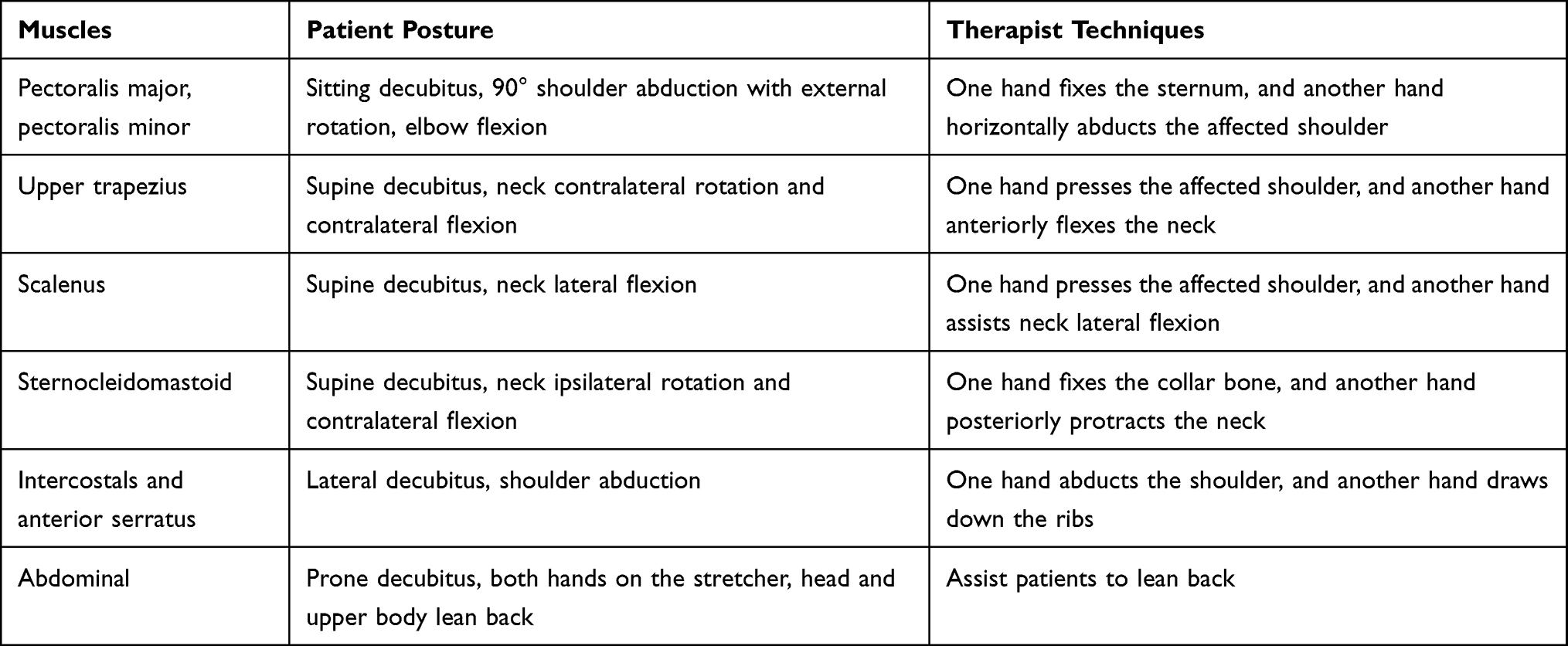 |
Table 1 Stretching Methods for Different Muscles |
Aerobic Training
Aerobic training was performed on a treadmill for 30 minutes beginning at 60% and reaching up to 85% of the average speed achieved during the 6-minute walk test (6MWT). The intensity was gradually enhanced and was associated with a perception effort between 4 and 7 points on the modified Borg scale.11
Measurements
The following items were recorded before and after rehabilitation training.
Pulmonary Function Test
On the basis of the guidelines of the American Thoracic Society/European Respiratory Society guidelines, all patients underwent post-bronchodilator pulmonary function testing (CHESTGRAPH HI-101, OMRON, Japan), containing spirometry assessments. Test started at the time of 20 minutes after subjects inhaling 400 μg of salbutamol. The following variables were assessed: FVC, FEV1, inspiratory capacity (IC), and inspiratory reserve volume (IRV).
After 1 hour of relaxation, the 6MWT was performed in the corridor of our department. Subjects were asked to walk with their top speed. Oxygen saturation and heart rate were monitoring all the way.13
CAT14 and dyspnea VAS15 were used for patients’ self-evaluation. Scores range of CAT and dyspnea VAS are from 0 to 40, and from 0 to 10, respectively. Lower scores indicate less symptoms. For dyspnea VAS, patients mark a 10-cm line at the point that they feel represents their current state on a sheet (0=no dyspnea and 10=the most severe).
Neck/Shoulder Mobility
After 30 minutes of relaxation, neck/shoulder mobility, including head protraction ROM, shoulder flexion ROM and non-dominant PmM length as follows were evaluated.
Measurement of head protraction ROM: subject stood upright in front of the posture assessment chart with the feet placing on the cross marks drawn on the ground. A tripod-mounted digital camera was placed 1.5 m away from the chart on the extension of subjects’ vertical plane. A marker was fixed (using double-sided tape) on the C7 spinous process, and the angle between the horizontal line and the line from the marker to the tragus were recorded. Subjects stared at a fixed point right ahead, and then they were asked to make maximum head protraction and retraction. Both angles were recorded. The head protraction ROM equals the latter minus the former (Supplementary Figure 1A and B).16
Measurement of shoulder flexion ROM: the shoulders of the subject were placed in maximum anterior flexion. The angle between the line from external epicondyle of humerus to the glenohumeral joint central and the midaxillary line was recorded (Supplementary Figure 1C).16
Measurement of the non-dominant pectoralis minor muscle (PmM) length: subjects stood with arms alongside the trunk. The distance between the coracoid process to the inferior margin of the fourth rib was recorded. This method is of high reliability and validity (Supplementary Figure 1D).16,17
Statistical Analyses
Sample Size Calculation
The number of subjects is based on the differences in 6MWT between PNF group and the control group after intervention. According to an earlier study, the difference was reported to be 56 with a standard deviation of 71.18 The target sample size was 27 patients per group with 80% power and a=0.05. To account for dropout and lost data, we recruited a total of 60 subjects.
Data Analyses
All statistical analyses were performed by the SPSS 22.0 software. The normality of the data was tested using the Shapiro–Wilks test and all continuous variables were normally distributed. The data were presented as mean ± standard deviation. Intragroup differences before and after the treatment were tested by paired t test. Intergroup differences before treatment were tested by the independent sample t test. Intergroup differences after treatment were tested by the analysis of covariance with the pre-treatment data as covariate. Pearson correlation analysis was employed to evaluate the association between neck/shoulder mobility and pulmonary function. P < 0.05 was considered significant.
Results
A total of 165 clinical records were reviewed. Sixty met the inclusion/exclusion criteria, and were randomly assigned to either the PNF group (n=30) or the control group (n=30). However, five subjects dropped out (2 in the PNF group and 3 in the control group) either through non-attendance or through incomplete assessments. Therefore, a total of 55 subjects with COPD were the study sample, of whom 28 subjects comprised the PNF group, and 27 subjects comprised the control group. Subject flow through the study is outlined in Figure 1. There was no significant difference in the baseline characteristics between the two groups (P > 0.05) (Table 2).
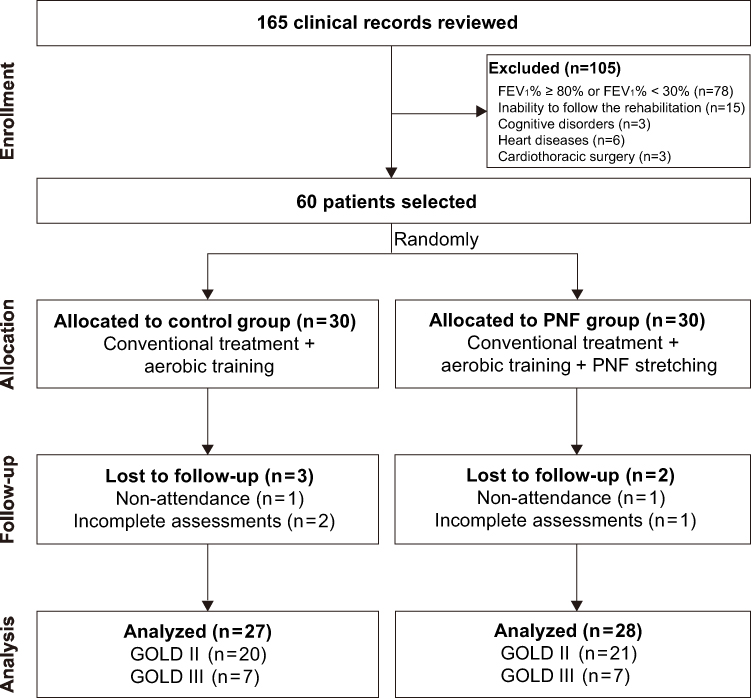 |
Figure 1 Study flow diagram. Abbreviations: FEV1, forced expiratory volume in the first second; PNF, proprioceptive neuromuscular facilitation; GOLD, Global Initiative for Chronic Obstructive Pulmonary Disease. |
 |
Table 2 Baseline Characteristics of the Study Patients |
Respiratory Symptoms
Rehabilitation training resulted in improvements of CAT and dyspnea VAS in both groups (both P < 0.05). However, scores of CAT and dyspnea VAS in PNF group were significantly lower than those of the control group after rehabilitation training (both P < 0.05), as shown in Figures 2A and B. These results suggested that PNF stretching combined with aerobic training significantly reduced the dyspnea symptom.
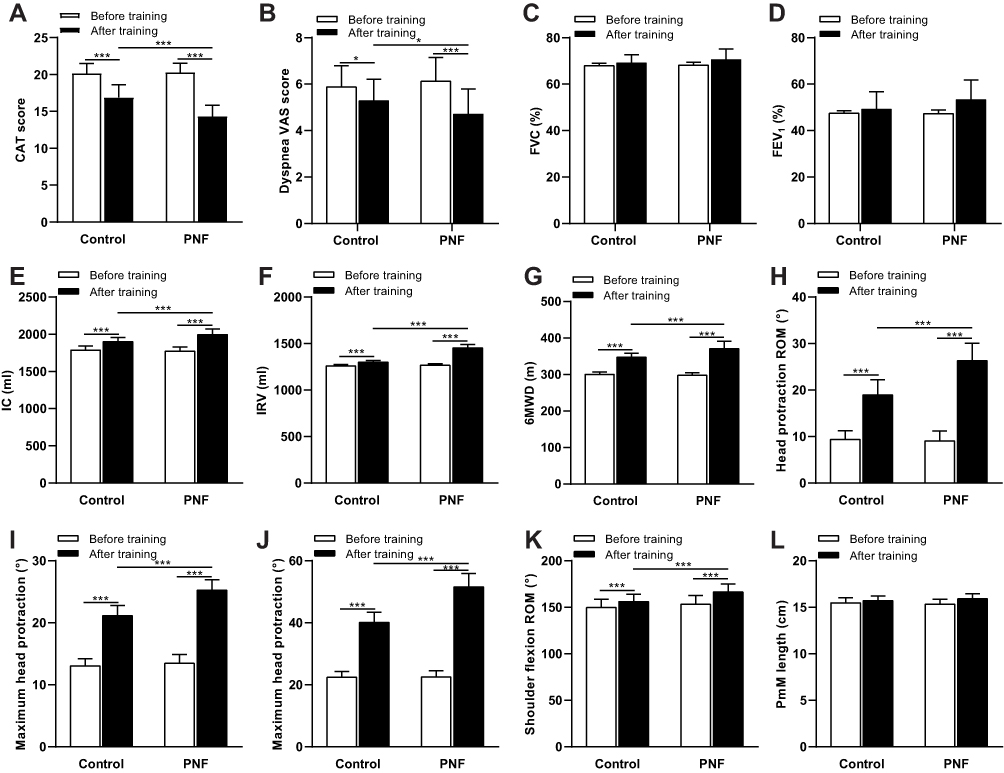 |
Figure 2 Comparison of respiratory symptoms, pulmonary function and muscular movement before and after rehabilitation training in different groups. (A) CAT score; (B) dyspnea VAS score; (C) FVC% predicted; (D) FEV1% predicted; (E) IC; (F) IRV; (G) 6MWT; (H) head protraction ROM; (I) maximum head protraction; (J) maximum head retraction; (K) shoulder flexion ROM; (L) PmM length. *P < 0.05, ***P < 0.001. Abbreviations: PNF, proprioceptive neuromuscular facilitation; BMI, body mass index; CAT, COPD Assessment Test; VAS, Visual Analogue Scale; FVC, forced vital capacity; FEV1, forced expiratory volume in the first second; IC, inspiratory capacity; IRV, inspiratory reserve volume; 6MWT, 6-minute walking distance test; ROM, range of motion. |
Pulmonary Function
Pulmonary function (IC and IRV) and 6MWT have been improved after the rehabilitation training (all P < 0.05), but FVC and FEV1 did not increase significantly (both P > 0.05), although FEV1 and FVC increased by 3.4% and 12.8% in PNF group, respectively. IC, IRV and 6MWT in PNF group were much better than those of the control group after rehabilitation training (all P < 0.05). There was no significant difference in FVC and FEV1 in two groups after rehabilitation training (both P > 0.05). Results showed in Figures 2C–G, suggesting that PNF stretching combined with aerobic training improved some pulmonary function measures.
Neck/Shoulder Mobility
Neck/shoulder mobility (head protraction ROM, maximum head protraction, maximum head retraction and shoulder flexion ROM) of both groups has been significantly improved after the training (all P < 0.05). These indicators in PNF group were much better than those of the control group after training (all P < 0.05) (Figure 2H–K). The non-dominant PmM length was slightly increased, but there was no significant difference between before and after training and between the two groups (P > 0.05) (Figure 2L). These results revealed that PNF stretching combined with aerobic training resulted in significant improvements in neck/shoulder mobility.
Association Between Neck/Shoulder Mobility and Pulmonary Function
Finally, a number of secondary, but notable, observations for the correlation between neck/shoulder mobility and lung function were made in our study by Pearson correlation analyses. IC was found to be positively correlated with the head protraction ROM and non–dominant PmM length (r=0.415, 0.579, P=0.028, 0.001) (Figure 3A and B); IRV was positively correlated with shoulder flexion ROM (r=0.405, P=0.032) in the PNF group (Figure 3C). However, there were no significant associations between neck/shoulder mobility and FVC or FEV1.
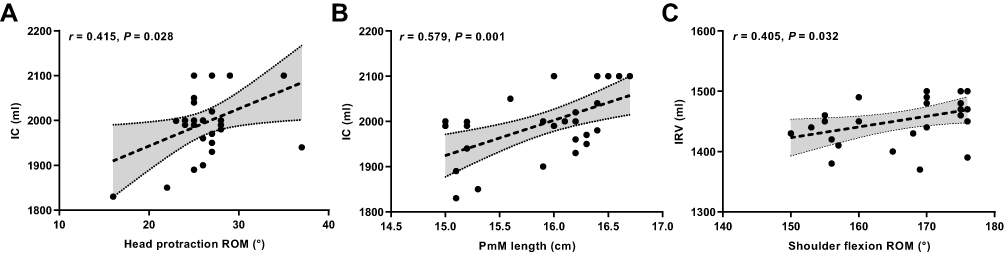 |
Figure 3 Correlation between neck/shoulder mobility and lung function in the PNF group. (A) Head protraction ROM and IC; (B) PmM length and IC; (C) shoulder flexion ROM and IRV. Abbreviations: PNF, proprioceptive neuromuscular facilitation; ROM, range of motion; IC, inspiratory capacity; IRV, inspiratory reserve volume; PmM, pectoralis minor muscle. |
Discussion
Our results showed that PNF stretching combined with aerobic training effectively reduced the symptom of dyspnea and improved some pulmonary function measures and neck/shoulder mobility in COPD patients.
Repeated stretching of respiratory muscles is beneficial to the increase in joint range of motion and pulmonary function of COPD patients.11,19–21 It has been evidenced that PNF stretching is more effective in enhancing muscle activation and improving motor coordination compared with static stretching.22–24 As early as 1988, PNF has been used to efficiently stretch respiratory muscles and fascia to improve patients’ pulmonary function and dyspnea.25 PNF stretching is effective at increasing the pulmonary function of normal adults and patients with pontine bleed, chronic low back pain and chronic stoke.8,26–28 COPD patients received 2 days PNF stretching on pectoralis major have improved in shoulder motion range and vital capacity.10 Improvements in thoracic wall muscles, thoracic cage, spine, shoulder range of motion and PNF of the thoracic wall muscles are also recommended as a part of the comprehensive respiratory rehabilitation plan.29 In addition, it was found that PNF stretching had a cumulative effect. Therefore, prolonged and frequent treatment is recommended to achieve better clinical effect.30
In our study, PNF technology was used to stretch respiratory muscle, and the dyspnea symptom and some pulmonary function measures of COPD patients were improved effectively after 6 weeks of training. Compared with the control group, the CAT score, dyspnea VAS score, IC, IRV, and 6MWT were all improved, which suggests that the strength training of respiratory muscles was helpful to the improvement of respiratory symptoms and pulmonary function, so as to enhance the quality of life. Consistent with this, Wada et al11 also reported that respiratory muscle stretching combined with aerobic training improved the 6MWT and respiratory muscle activity of COPD patients. Therefore, PNF stretching of respiratory muscles could be used as routine lung rehabilitation training.
Morais et al16 demonstrated that pulmonary function was correlated with respiratory muscle strength, as well as neck/shoulder mobility, including the head protraction ROM, shoulder flexion, cervical vertebrae, angle of thoracic kyphosis, and the length of PmM. In this study, we use the indicators of neck/shoulder flexibility to indicate the function improvement of respiratory muscle by PNF stretching. As an accessory inspiratory muscle, the non-dominant PmM could play its full role when its length was improved.31 The improvement in head protraction angle helps patients keep the flexibility of the neck and shoulder, and the improvement in shoulder flexion angle elevated upper limbs higher, and then facilitated the function of accessory inspiratory muscles, suggesting that adaptive change in COPD patients’ position and mobility had an association with their pulmonary function. In our study, the change in head protraction ROM, shoulder flexion ROM and the PmM length had correlation with the change in the patient’s lung function, which may throw light on the rehabilitation intervention.
PNF stretching improves muscle length and joint range of motion via the mechanism of autogenic inhibition. There are Golgi tendon organs in tendons which respond to muscle tension. Muscle contraction activated Ib afferent nerve fibers, and the nerve impulse transmitted to spinal cord by afferent fibers activated inhibitory interneurons. The inhibitory signal transmitted to α motor neurons by interneurons in turn decreased their nerve excitability and muscle tension.32 When muscles were stretched again, the overlap of actin and myosin filaments decreased with increased myofiber length, improved muscle viscoelasticity, more efficient muscle contraction, decreased motor nerve excitability, and decreased energy consumption.33 In addition, for all these, information will finally be transmitted to the central nervous system; therefore, stretching is beneficial to proprioception and motor control of central nervous system.20
Certain limitations in this study should be mentioned. First, the sample size is relatively small, which might lead to false-positive and false-negative results. Second, the follow-up time is shorter, long-term effect of PNF stretching needs further follow-up observation in large samples. Third, the PNF stretching proposal is not involved diaphragm, which is the most important structure determining pulmonary function. Adding diaphragm training on the PNF stretching of respiratory muscle is expected to exert more positive effects on the lung function. Further studies will design more comprehensive training.
Conclusion
In summary, our results provide evidence for the application of PNF stretching in the pulmonary rehabilitation of COPD patients. PNF stretching combined with aerobic training as a simple, practicable and widely applicable rehabilitation method can improve the pulmonary function and relieve their symptoms by enhancing neck/shoulder mobility of patients.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author (Dr Wei Han) in response to reasonable requests.
Ethics Approval and Consent to Participate
The studied protocol was approved by the Ethics Committee of Qingdao Municipal Hospital (Approval number: 2018-031). Written informed consent was obtained from all patients before the enrollment of this study in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
Thanks for the support of Beijing DAO Research Technology Ltd in research design, data processing, statistical analysis and report. The trial was registered with the Chinese Clinical Trial Registry (ChiCTR1800018413).
Funding
The study was supported by the Qingdao Science and Technology Fund (project number 17-3-3-16-nsh).
Disclosure
The authors report no conflict of interest in this work. The abstract of this paper was presented at the Chest Congress 2019 as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Chest: https://journal.chestnet.org/article/S0012-3692(19)30463-5/fulltext.
References
1. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
2. Fang L, Gao P, Bao H, et al. Chronic obstructive pulmonary disease in China: a nationwide prevalence study. Lancet Respir Med. 2018;6(6):421–430. doi:10.1016/s2213-2600(18)30103-6
3. Zhong N, Wang C, Yao W, et al. Prevalence of chronic obstructive pulmonary disease in China: a large, population-based survey. Am J Respir Crit Care Med. 2007;176(8):753–760. doi:10.1164/rccm.200612-1749OC
4. Zhao HM, Wang C. Pulmonary rehabilitation of chronic obstructive pulmonary disease: evaluation and implementation. Zhonghua Jie He He Hu Xi Za Zhi. 2018;41(7):561–566. doi:10.3760/cma.j.issn.1001-0939.2018.07.013
5. Guo BP, Zhou LL, Guan LL. Recent advance in impacts of pulmonary rehabilitation on inflammation and oxidative stress in chronic obstructive pulmonary disease. Zhonghua Jie He He Hu Xi Za Zhi. 2017;40(12):936–938. doi:10.3760/cma.j.issn.1001-0939.2017.12.014
6. Make BJ, Yawn BP. Breathing life into COPD management: ongoing monitoring, pulmonary rehabilitation, and individualized care. Chest. 2018;154(4):980–981. doi:10.1016/j.chest.2018.08.1023
7. Wanderley D, Lemos A, Moretti E, Barros MMMB, Valença MM, de Oliveira DA. Efficacy of proprioceptive neuromuscular facilitation compared to other stretching modalities in range of motion gain in young healthy adults: a systematic review. Physiother Theory Pract. 2019;35(2):109–129. doi:10.1080/09593985.2018.1440677
8. Slupska L, Halski T, Żytkiewicz M, et al. Proprioceptive neuromuscular facilitation for accessory respiratory muscles training in patients after ischemic stroke. Adv Exp Med Biol. 2019;1160:81–91. doi:10.1007/5584_2018_325
9. González-Ravé JM, Sánchez-Gómez A, Santos-García DJ. Efficacy of two different stretch training programs (passive vs. proprioceptive neuromuscular facilitation) on shoulder and hip range of motion in older people. J Strength Cond Res. 2012;26(4):1045–1051. doi:10.1519/JSC.0b013e31822dd4dd
10. Putt MT, Watson M, Seale H, Paratz JD. Muscle stretching technique increases vital capacity and range of motion in patients with chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2008;89(6):1103–1107. doi:10.1016/j.apmr.2007.11.033
11. Wada JT, Borges-Santos E, Porras DC, et al. Effects of aerobic training combined with respiratory muscle stretching on the functional exercise capacity and thoracoabdominal kinematics in patients with COPD: a randomized and controlled trial. Int J Chron Obstruct Pulmon Dis. 2016;11:2691–2700. doi:10.2147/copd.S114548
12. Cruz-Montecinos C, Godoy-Olave D, Contreras-Briceño FA, et al. The immediate effect of soft tissue manual therapy intervention on lung function in severe chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2017;12:691–696. doi:10.2147/copd.S127742
13. Polkey MI, Spruit MA, Edwards LD, et al. Six-minute-walk test in chronic obstructive pulmonary disease: minimal clinically important difference for death or hospitalization. Am J Respir Crit Care Med. 2013;187(4):382–386. doi:10.1164/rccm.201209-1596OC
14. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
15. Ozoglu Aytac S, Kilic SP, Ovayolu N. Effect of inhaler drug education on fatigue, dyspnea severity, and respiratory function tests in patients with COPD. Patient Educ Couns. 2020;103(4):709–716. doi:10.1016/j.pec.2019.11.003
16. Morais N, Cruz J, Marques A. Posture and mobility of the upper body quadrant and pulmonary function in COPD: an exploratory study. Braz J Phys Ther. 2016;20(4):345–354. doi:10.1590/bjpt-rbf.2014.0162
17. Rondeau MW, Padua DA, Thigpen CA, Harrington SE. Precision and validity of a clinical method for pectoral minor length assessment in overhead-throwing athletes. Athl Train Sports Health Care. 2012;4(2):67–72. doi:10.3928/19425864-20110630-01
18. López-García A, Souto-Camba S, Blanco-Aparicio M, González-Doniz L, Saleta JL, Verea-Hernando H. Effects of a muscular training program on chronic obstructive pulmonary disease patients with moderate or severe exacerbation antecedents. Eur J Phys Rehabil Med. 2016;52(2):169–175.
19. Apostolopoulos N, Metsios GS, Flouris AD, Koutedakis Y, Wyon MA. The relevance of stretch intensity and position-a systematic review. Front Psychol. 2015;6:1128. doi:10.3389/fpsyg.2015.01128
20. Abdel-aziem AA, Draz AH, Mosaad DM, Abdelraouf OR. Effect of body position and type of stretching on hamstring flexibility. Int J Med Res Health Sci. 2013;2(3):399–406. doi:10.5958/j.2319-5886.2.3.070
21. Wang JS. Effect of joint mobilization and stretching on respiratory function and spinal movement in very severe COPD with thoracic kyphosis. J Phys Ther Sci. 2015;27(10):3329–3331. doi:10.1589/jpts.27.3329
22. Yıldırım MS, Ozyurek S, Tosun O, Uzer S, Gelecek N. Comparison of effects of static, proprioceptive neuromuscular facilitation and Mulligan stretching on hip flexion range of motion: a randomized controlled trial. Biol Sport. 2016;33(1):89–94. doi:10.5604/20831862.1194126
23. Minshull C, Eston R, Bailey A, Rees D, Gleeson N. The differential effects of PNF versus passive stretch conditioning on neuromuscular performance. Eur J Sport Sci. 2014;14(3):233–241. doi:10.1080/17461391.2013.799716
24. Reznik JE, Biros E, Bartur G. An electromyographic investigation of the pattern of overflow facilitated by manual resistive proprioceptive neuromuscular facilitation in young healthy individuals: a preliminary study. Physiother Theory Pract. 2015;31(8):582–586. doi:10.3109/09593985.2015.1061627
25. Ries AL, Ellis B, Hawkins RW. Upper extremity exercise training in chronic obstructive pulmonary disease. Chest. 1988;93(4):688–692. doi:10.1378/chest.93.4.688
26. Seo K, Cho M. The effects on the pulmonary function of normal adults proprioceptive neuromuscular facilitation respiration pattern exercise. J Phys Ther Sci. 2014;26(10):1579–1582. doi:10.1589/jpts.26.1579
27. Dubey L, Karthikbabu S. Trunk proprioceptive neuromuscular facilitation influences pulmonary function and respiratory muscle strength in a patient with pontine bleed. Neurol India. 2017;65(1):183–184. doi:10.4103/0028-3886.198193
28. Kim BR, Lee HJ. Effects of proprioceptive neuromuscular facilitation-based abdominal muscle strengthening training on pulmonary function, pain, and functional disability index in chronic low back pain patients. J Exerc Rehabil. 2017;13(4):486–490. doi:10.12965/jer.1735030.515
29. Rochester CL, Vogiatzis I, Holland AE, et al. An Official American Thoracic Society/European Respiratory Society Policy Statement: enhancing Implementation, Use, and Delivery of Pulmonary Rehabilitation. Am J Respir Crit Care Med. 2015;192(11):1373–1386. doi:10.1164/rccm.201510-1966ST
30. Wang RY. Effect of proprioceptive neuromuscular facilitation on the gait of patients with hemiplegia of long and short duration. Phys Ther. 1994;74(12):1108–1115. doi:10.1093/ptj/74.12.1108
31. Courtney R. The functions of breathing and its dysfunctions and their relationship to breathing therapy. Int J Osteopath Med. 2009;12(3):78–85. doi:10.1016/j.ijosm.2009.04.002
32. Sharman MJ, Cresswell AG, Riek S. Proprioceptive neuromuscular facilitation stretching: mechanisms and clinical implications. Sports Med. 2006;36(11):929–939. doi:10.2165/00007256-200636110-00002
33. Hindle KB, Whitcomb TJ, Briggs WO, Hong J. Proprioceptive neuromuscular facilitation (PNF): its mechanisms and effects on range of motion and muscular function. J Hum Kinet. 2012;31:105–113. doi:10.2478/v10078-012-0011-y
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.