")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Effects of Combined Therapy of Olanzapine and Samidorphan on Safety and Metabolic Parameters in Schizophrenia Patients: A Meta-Analysis
Authors Peng Z , Jia Q, Mao J, Yi Q
Received 20 June 2023
Accepted for publication 17 October 2023
Published 26 October 2023 Volume 2023:19 Pages 2295—2308
DOI https://doi.org/10.2147/NDT.S426481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Richard J Porter
Zhenlei Peng,1,* Qiyu Jia,2,* Junxiong Mao,1 Qizhong Yi1
1The Psychological Medicine Center, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China; 2Department of Trauma Orthopedics, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qizhong Yi, The Psychological Medicine Center, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, Xinjiang, People’s Republic of China, Tel +86 13999138673, Email [email protected]
Purpose: This meta-analysis intended to evaluate the safety and metabolic effects of the combination of olanzapine (OLZ) and samidorphan (SAM) in the treatment of schizophrenia (SCZ) patients.
Patients and Methods: We searched for the English and Chinese databases for randomized controlled trials (RCTs) on the OLZ combined with SAM for SCZ. The English databases included PubMed, Web of Science, EMbase, and Cochrane Library, however, Chinese databases included Chinese Biology Medicine (CBM), VIP, Wanfang, and China National Knowledge Infrastructure (CNKI). All database searches were due by May 31, 2023. Using Review Manager 5.4 software, a meta-analysis was conducted following a literature review and data extraction.
Results: This study included five RCTs involving 1781 patients. Regarding safety, the meta-analysis revealed that the probability of weight gain was reduced in the OLZ and SAM group than in the OLZ group (RR = 0.83, 95% CI (0.69, 0.99), P < 0.05). Statistically, the incidence of severe adverse safety events, dry mouth, headache, drowsiness, death, and suicidal perception events was insignificant (P > 0.05); in terms of metabolism, compared with the OLZ group, the OLZ plus SAM group reduced total cholesterol (TC) levels (MD = − 3.58, 95% CI (− 6.81, − 0.34), P < 0.05). However, it had no significant effect on metabolic indices, including low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides, glucose, and insulin index (P > 0.05).
Conclusion: In patients with SCZ, treatment with the combination of OLZ and SAM decreased the incidence of weight gain adverse events and TC levels; nevertheless, it did not affect other adverse events or metabolic parameters. These findings provide clinicians with evidence-based guidance and support for drug selection. However, it is crucial to confirm these findings through further high-quality research.
Keywords: schizophrenia, SCZ, samidorphan, safety, metabolic parameters, meta-analysis
Introduction
Recently, samidorphan (SAM) has received much attention as a novel formulation for reducing olanzapine’s (OLZ) side effects in schizophrenia (SCZ) treatment.1–3 Despite the widespread recognition of OLZ’s efficacy in treating SCZ, its concomitant significant safety concerns of weight gain and associated metabolic disorders (eg, hyperglycemia, hypercholesterolemia, hyperlipidemia) continue to be a primary factor limiting its widespread clinical use.1,4,5 Numerous investigations have determined that OLZ has fewer adverse effects. Some researchers believe that OLZ treatment should be coupled with real-time monitoring and must be switched swiftly to other antipsychotics in case of intense adverse events.6–8 Various perspectives propose co-administering metformin, topiramate, and reboxetine to reduce weight gain is also a viable option.9,10 The new application of SAM appears to provide an additional therapeutic approach.
Promoting new treatment methods requires long-term and comprehensive scientific evidence. Czyzyk et al reported that11,12 SAM acts as a µ-opioid receptor antagonist and a partial agonist of κ- and δ-opioid receptors. The µ-, κ-, and δ-opioid receptors knockout mice have gained less body weight compared to wild mice. Furthermore, a preclinical study demonstrated13 that OLZ can increase glucose uptake in adipose tissue, whereas SAM can restore glucose utilization to normal levels and reduce olanzapine-induced weight gain. Further clinical trials14,15 revealed that compared to OLZ alone, the incidence of adverse events and metabolic effects were not significantly different when OLZ was combined with SAM. Subsequently, Srisurapanont et al conducted a meta-analysis16 to explore the impact of OLZ/SAM on short-term weight gain and cardiac metabolic changes. Four studies were included in this analysis, three of which involved patients with SCZ, and one had a healthy population. The findings did not suggest that SAM could prevent OLZ-induced weight gain and cardiac metabolic abnormalities. Another systematic review on the application of SAM in conjunction with OLZ for the treatment of SCZ and bipolar I disorder found17 that the combination therapy tended to reduce weight gain in adult patients with SCZ compared to OLZ monotherapy, however, there was no significant difference in metabolic effects. Subsequently, two studies18,19 on the treatment of SCZ with the OLZ/SAM were reported, and one randomized controlled trial (RCT) confirmed that18 OLZ/SAM treatment decreased the risk of weight gain. Briefly, higher-quality evidence regarding the specific reduction of weight gain and metabolic disturbances induced by OLZ during treatment of SCZ with OLZ/SAM is still lacking.
The transition from OLZ monotherapy to OLZ/SAM combination therapy has begun for OLZ-eligible patients due to the expansion of SAM’s clinical application. Although studies indicate a trend toward reducing adverse events related to weight gain with the use of OLZ/SAM, there is no clear consensus on whether OLZ/SAM increases the probability of other side effects or impacts metabolic processes such as glucose and lipid metabolism. In the context of comparable OLZ doses, combining the two medications increases the hepatic and renal burden and the risk of adverse events compared to a single dosing regimen. This scientific question is essential for patients, nevertheless, no studies with a higher level of evidence clarify it. When considering the potential side effects that may arise at the onset of treatment, clinicians also encounter challenges in choosing the appropriate medication. In search of more substantial evidence, we conducted our first systematic review, concentrating on the safety and metabolic effects of OLZ in combination with SAM for the treatment of SCZ. This meta-analysis seeks to determine whether OLZ/SAM is safer and has a negligible impact on metabolic levels in treating SCZ. This study aims to provide valuable insights into managing SCZ and enhancing patient medication acceptance and adherence.
Materials and Methods
Data Sources and Search Strategy
This meta-analysis adheres to the Preferred Reporting for Systematic Reviews and Meta-AnalysIs (PRISMA) Statement.20 After two researchers independently screened the search results based solely on eligibility criteria, it was registered in the PROSPERO database (registration number: CRD420234325). We searched Wanfang, China National Knowledge Infrastructure (CNKI), VIP, Chinese Biology Medicine (CBM), PubMed, Cochrane Library, Embase, and Web of Science for articles written in English or Chinese. RCTs were conducted to investigate the efficacy of OLZ and SAM in treating SCZ patients. The research was conducted on all publications until May 31, 2023, without restrictions on countries or article categories. Additionally, a manual search of references from reviews, systematic reviews, meta-analyses, and trials to identify additional relevant literature and enhance accessibility to the relevant research. The search strategy was subtly modified for different databases. The terms used in the search were olanzapine, samidorphan, Lybalvi, 3-carboxamido-4-hydroxynaltrexone, schizophrenia*/schizophrenic Disorder*and schizophrenic. A flowchart of the literature screening process and results is shown in Figure 1. The search details are provided in Supplementary Table 1.
 |
Figure 1 Flow diagram of the literature screening process and results. |
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: 1) Patients diagnosed with SCZ by the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV or DSM-V),21,22 regardless of race, nationality, gender, or duration of illness; 2) The trial method was an RCT; 3) The intervention group was treated with OLZ combined with SAM, while the control group received OLZ alone; 4) Outcome indicators included both safety and metabolic indicators; safety indicators in this study refer to the number of adverse reactions with an incidence rate of ≥ 5% during the medication treatment process, that include death, somnolence, headache, weight gain (≥ 7% change from baseline), dry mouth, and other adverse events. Metabolic indicators, however, included alterations in total cholesterol (TC), triglycerides, high-density lipoprotein (HDL), low-density lipoprotein (LDL), glucose, and insulin. The following were the criteria for exclusion:1) Literature in languages other than Chinese and English; 2) Unavailability of the full text; 3) Absence of or insufficient data for key outcome indexes; 4) Reviews, commentaries, and conference abstracts, among others, are excluded categories of literature.
Screening and Data Extraction
Two researchers independently reviewed the titles and abstracts, assessed the full-text publications, selected the trials, extracted the data, and evaluated the trial quality. The process was carried out per the Cochrane Systematic Evaluation Manual criteria.23 A third researcher would intervene and summarize the discussion in the case of a disagreement. The screening of published articles begins with an initial review of the article’s title and abstract. After eliminating irrelevant literature, we examined the content of the remaining literature to determine if it met the criteria. The data was then extracted using a predesigned table. The subsequent information was extracted from each study: first author, year of publication, country, diagnostic criteria, sample size, study design, sample characteristics, intervention and control group treatments, duration of intervention, and outcome indicators (see Table 1). If there were inadequate or missing data, we contacted the authors to request the raw data.
 |
Table 1 Characteristics of Included Trails |
Assessment of the Risk of Bias
Two authors independently evaluated the included trials’ methodological quality using the Cochrane risk of bias (ROB) tool.26 The contents of the evaluation tool comprised sequence generation, allocation sequence concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and others that could introduce various sources of bias (see Figure 2a/b). If there were divergent viewpoints, a third party was consulted to determine the outcome.
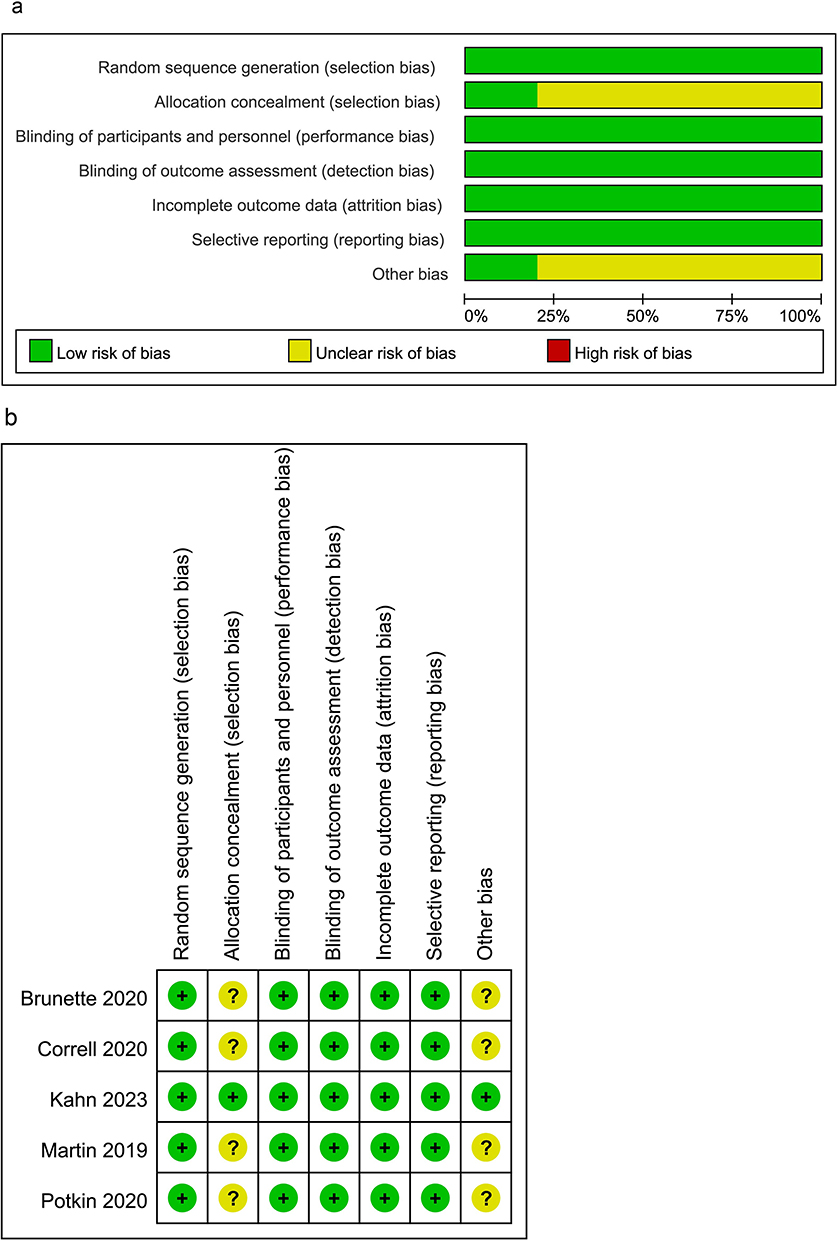 |
Figure 2 Risk of bias graph. Notes: (a) Review authors’ judgements about each risk of bias item presented as percentages across all included studies. (b) Review authors’ judgements about each risk of bias item for each included study. |
Statistical Analysis
The meta-analysis was conducted using RevMan version 5.4 Software. We tabulated the characteristics of the study interventions and compared them against the control groups for each synthesis. Additionally, we analyzed safety indicators and metabolic indicators from the relevant literature. The dichotomous outcomes were presented as pooled relative risks (RRs) with 95% confidence intervals (CIs); however, the continuous outcomes were presented as mean differences (MDs) with 95% CIs. Additionally, heterogeneity between studies was analyzed using the Cochran Q test and the I2 statistic. If the Q test result was P > 0.1 and I2 < 50%, the fixed effects model (FEM) was used to calculate the pooled RRs. Otherwise, the random effects model (REM) was employed. Furthermore, we conducted sensitivity analysis or subgroup analysis to explore the stability of the model and further eliminate potential sources of heterogeneity. The reporting bias was estimated using funnel diagrams (See Supplementary Figures 1–14). Due to the limited number of trials (less than ten), we did not conduct a statistical test to measure publication bias.26 We will present the results in graphs and tables. When data was insufficient, we inquired to the authors for additional information. We eliminated that study from the meta-analysis if data could not be obtained.
Results
Screening and Selection of Studies
Figure 1 represents a flowchart of the literature selection approach. Initial electronic database searches yielded 237 retrieved studies (one from CNKI, two from Wanfang, two from VIP, two from CBM, 66 from Web of Science, 42 from PubMed, 70 from EMbase, and 52 from Cochrane Library). During the preliminary assessment of the title and abstract, 163 duplicate and 55 irrelevant studies were removed. Furthermore, after excluding 14 studies by further reading their full texts, only five studies14,15,18,24,25 were included in this meta-analysis, all from the English literature.
Study Characteristics and Quality Assessment
Table 1 summarizes the primary characteristics of the suitable studies, whose outcome indicators included safety indicators (such as the incidence of weight gain, headache, and dry mouth) and metabolic indicators (such as TC, triglycerides, and glucose). Five studies14,15,18,24,25 with 1781 patients were included in our meta-analysis, with 965 in the OLZ/SAM group and 816 in the OLZ group. Figure 2a and b illustrate the results of the risk of bias evaluation of the included studies. All five trials14,15,18,24,25 included in this study were multicenter, double-blind trials and described the randomization method; one trial18 specified the method of allocation concealment, The remaining four trials were missing a precise description of allocation concealment and were therefore rated as having an unclear risk. Five experimental studies were conducted with Alkermes, Inc.’s participation, and only one trial18 indicated that the company was unaware of the entire trial procedure. Contrarily, the remaining four trials failed to specify whether or not the company intervened, resulting in an unclear risk rating. We believe that the aggregate quality of the included studies is low-risk.
Meta-Analysis of Safety
All five studies14,15,18,24,25 reported any adverse events and serious adverse events. These studies had no significant heterogeneity (I2 = 0%, P = 0.67; I2 = 25%, P = 0.25. Figure 3a/b); therefore, a FEM was used for analysis. The meta-analysis showed no statistically significant difference between the two groups (RR = 0.96, 95% CI (0.89, 1.02), P = 0.19; RR = 0.77, 95% CI (0.45, 1.33), P = 0.34. Figure 3a/b). Five of these studies14,15,18,24,25 reported weight gain (RR = 0.83, 95% CI (0.69, 0.99), P = 0.04; I2 = 33%, P = 0.20. Figure 3c), treatment with OLZ in combination with SAM reduced the incidence of weight gain events in patients with SCZ compared to OLZ. Furthermore, for subgroup analysis, we divided studies into two groups, including a long follow-up time group with a follow-up time of ≥ 12 weeks and a short follow-up time group with a follow-up time of < 12 weeks. The results demonstrated that in the long follow-up time group, OLZ in combination with SAM still reduced the rate of weight-gaining events in SCZ’s patients (RR = 0.78, 95% CI (0.64, 0.94), P = 0.43; I2 = 0%, P = 0.01. Figure 3c), and there was no significant difference between the two groups in the short follow-up time group (RR = 1.31, 95% CI (0.76, 2.25), P = 0.34. Figure 3c). Additionally, four studies14,15,18,24 reported somnolence (RR = 1.23, 95% CI (0.95, 1.60), P = 0.12; I2 = 5%, P = 0.37. Figure 3d), four14,15,18,24,25 reported headache (RR = 0.95, 95% CI (0.57, 1.60), P = 0.85; I2 = 0%, P = 0.39. Figure 3e), four14,18,24,25 reported death (RR = 1.72, 95% CI (0.23, 12.99), P = 0.60; I2 = 0%, P = 0.62. Figure 3f), three14,15,24 reported dry mouth (RR =1.47, 95% CI (0.97, 2.22), P = 0.07; I2 = 0%, P = 0.78. Figure 3g), and three18,24,25 reported suicide perception (RR = 0.51, 95% CI (0.15, 1.68), P = 0.27; I2 = 13%, P = 0.32. Figure 3h). There was no statistically significant difference between the two groups on these adverse events.
Figure 3 Continued. Figure 3 Forest plot: safety indicators. Abbreviations: OLZ/SAM, A combination of olanzapine and samidorphan group; OLZ, Olanzapine group. Notes: (a) Forest plot: the incidence of any adverse events. (b) Forest plot: the incidence of serious adverse events. (c) Forest plot: the incidence of weight gain. (d) Forest plot: the incidence of somnolence. (e) Forest plot: the incidence of headache. (f) Forest plot: the incidence of death. (g) Forest plot: the incidence of dry mouth. (h) Forest plot: the incidence of suicide perception.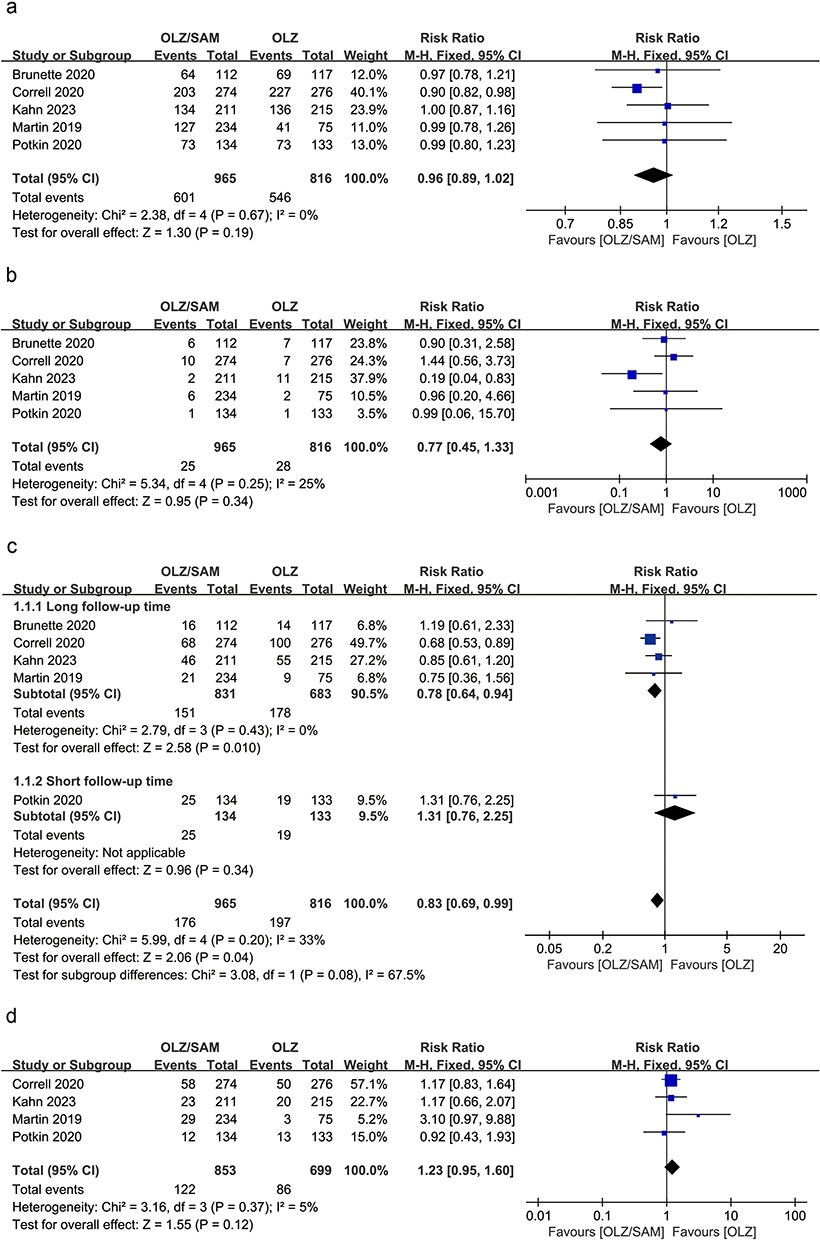

Meta-Analysis of Metabolic Parameters
Regarding metabolic parameters, three studies were included.14,15,18 Among them, there was insignificant heterogeneity in these studies at the level of TC (I2 = 0%, P = 0.40. Figure 4a), LDL (I2 = 0%, P = 0.46. Figure 4b), triglycerides (I2 = 0%, P = 1.00. Figure 4c), glucose (I2 = 0%, P = 0.73. Figure 4d), and insulin (I2 = 0%, P = 0.68. Figure 4e) indicators; thus, a FEM was used for the analysis. Conversely, there was heterogeneity in the studies at the HDL indicators level (I2 = 64%, P = 0.06. Figure 4f), hence, a REM analysis was used. Among them, OLZ combined with SAM can reduce TC levels (MD = −3.58, 95% CI (−6.81, −0.34), P = 0.03. Figure 4a). However, the meta-analysis showed no statistically significant differences between the two groups in LDL (MD = −1.76, 95% CI (−4.56, 1.04), P = 0.22. Figure 4b), triglycerides (MD = −3.04, 95% CI (−11.09, 5.02), P = 0.46. Figure 4c), glucose (MD = 1.40, 95% CI (−0.34, 3.13), P = 0.11. Figure 4d), or insulin (MD = −0.31, 95% CI (−3.01, 2.38), P = 0.82. Figure 4e), HDL (MD = −0.70, 95% CI (−2.89, 1.48), P = 0.53. Figure 4f).
Figure 4 Continued. Figure 4 Forest plot: metabolic parameters. Abbreviations: OLZ/SAM, A combination of olanzapine and samidorphan group; OLZ, Olanzapine group. Notes: (a) Forest plot: Total Cholesterol (mg/dL). (b) Forest plot: Low Density Lipoprotein (mg/dL). (c) Forest plot: Triglycerides (mg/dL). (d) Forest plot: Glucose (mg/dL). (e) Forest plot: Insulin (mIU/dL). (f) Forest plot: High Density Lipoprotein (mg/dL). (g) Forest plot: High density lipoprotein (mg/dL) sensitivity analysis.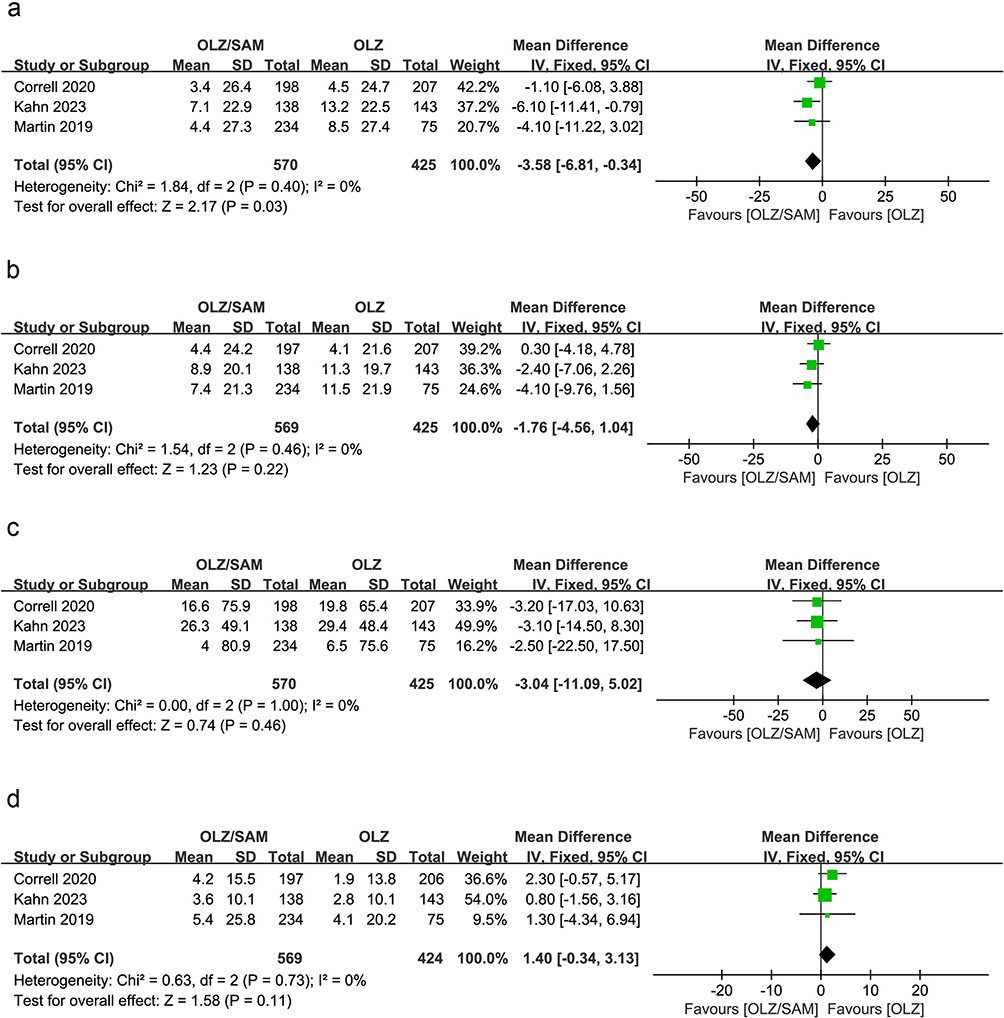

Sensitivity Analysis
Using a FEM, the results of modifying the combined model for HDL metabolic indicators were (I2 = 64%, P = 0.06). Figure 4g demonstrates that the difference in HDL levels between the two groups was not statistically significant (MD = −0.99, 95% CI (−2.27, 0.3), P = 0.13). In Figure 4g, the combined results of the two models were consistent, indicating that the results were reliable and that the model was robust.
Discussion
While OLZ/SAM (LYBALVI™) has received FDA approval27 as an effective new combination for treating SCZ, academic opinion has not been unanimous, and widespread controversy persists regarding the safety and effects of SAM on metabolic parameters. Regarding efficacy, the study by Potkin et al indicated24 significant differences between OLZ/SAM and monotherapy with OLZ or placebo relative to the Positive and Negative Syndrome Scale (PANSS) scores after four weeks of treatment. Moreover, at 1214 and 2415 weeks of treatment, the total PANSS scores of both groups improved similarly relative to baseline. Furthermore, a 52-week study of SCZ patients treated with OLZ/SAM revealed28 a decrease in PANSS total scores from baseline, with 93.5% of patients retaining stable mental symptoms and no significant relapses. Although relevant meta-analyses16 and systematic reviews17 have been conducted on weight gain and metabolic changes in individuals treated with OLZ/SAM, they have not focused solely on SCZ patients. Additionally, it has not been considered to investigate other adverse safety events caused by OLZ/SAM in patients. Given the paucity of high-quality evidence on the safety and impact of metabolic indicators of OLZ combined with SAM for treating SCZ patients, the drug’s safety should be considered first in a composite event for patients. A total of 1781 patients from five studies were included in this study.14,15,18,24,25 In terms of adverse events related to weight gain, we included one trial24 with a duration of 4 weeks and four trials14,15,18,25 with follow-up periods exceeding 12 weeks. Subgroup analysis was conducted based on the duration of follow-up. After excluding the negative results from the study24 by Potkin et al, the incidence of adverse events in the OLZ/SAM group was further reduced compared to the OLZ group, and the between-group difference became more significant. Regarding the metabolic parameter of TC, all included studies14,15,18 showed a decreasing trend in TC levels with OLZ/SAM compared to OLZ monotherapy. These early metabolic changes suggest that29 they may be a direct effect of OLZ rather than a consequence of weight gain associated with antipsychotic medications, and SAM appears to attenuate this metabolic risk. The results demonstrated in the meta-analysis that compared with the control group, in terms of safety, the incidence of weight gain was significantly lower in patients with SCZ treated with a combination of OLZ and SAM. In contrast, the incidence of any adverse events and the incidence of adverse events such as dry mouth, headache, somnolence, suicide perception, and death were significantly indifferent. Regarding metabolic indicators, the intervention group reduced TC levels in SCZ’s patients, while there were no significant differences in triglyceride, LDL, HDL, glucose, and insulin levels, which differed from the previous meta-analysis.16
While many antipsychotic medications can cause weight gain, OLZ is considered high-risk.30–32 Indeed, the higher the dose of OLZ, the greater the observed weight gain. In the first six weeks of OLZ treatment, high doses were associated with an average weight gain of +3.2kg, while moderate doses were associated with an average weight gain of +1.9kg, according to a study.33 Nevertheless, co-administration of SAM can mitigate this problem. Specifically, previous studies have shown that11,12,34 SAM played a vital role as a μ-opioid receptor antagonist and a partial agonist of κ- and δ-opioid receptors mainly in regulating feeding behavior. Preclinical studies reported that the knockdown of μ-, κ-, and δ-opioid receptors prevented obesity and impaired glucose tolerance in transgenic mice fed a high-energy diet.11,12 Additionally, studies have demonstrated that SAM can attenuate weight gain by restoring the increased glucose absorption caused by OLZ.13 SAM has a bioavailability of 69% and a half-life of 7–10 h compared to OLZ’s 35–52 h, making it an appropriate companion for OLZ when taken as a combination tablet.35 Therefore, adding SAM to antipsychotics known to induce weight gain (such as OLZ) would reduce weight gain associated with OLZ use and enhance patient adherence to long-term treatment. Due to the presence of opioid receptors in the central nervous system and the periphery (eg, pancreas, muscle, and liver), the opioid system is a potential therapeutic target for addressing antipsychotic-associated weight gain, as shown by the significantly lower incidence of weight gain in the intervention group compared to the control group.36,37 SAM can counteract the weight gain associated with OLZ administration by inhibiting fat and glucose uptake and resisting insulin resistance caused by OLZ.38 This therapeutic benefit supports the idea that OLZ/SAM would be a better treatment option for long-term use than OLZ monotherapy.
In addition to preventing weight gain, SAM also plays a role in metabolism.11,12,34 When using atypical antipsychotics, such as OLZ, to enhance the prognosis of patients with SCZ, the metabolic syndrome is equally as concerning as weight gain. A recent meta-analysis revealed a stronger association between OLZ use and elevated levels of TC, low-density lipoprotein, and triglycerides.39 It has been established that OLZ increases the susceptibility to cardiovascular and endocrine disorders by inducing metabolic alterations.40 Considering the metabolic effects of the second-generation antipsychotics, such as OLZ, can be enhanced. In this case, metabolic diseases, including diabetes, hyperlipidemia, and hypertension can be prevented, and the therapeutic effect can be substantially enhanced.41 This study compared two treatment regimens and found that SAM had a positive effect on reducing serum TC levels, but had no significant impact on metabolic parameters such as triglycerides, blood glucose, and serum insulin. Hypercholesterolemia is a risk factor independent of atherosclerosis.42 Increasing evidence indicates that43,44 OLZ treatment can result in severe cardiac metabolic disturbances, such as abnormal cholesterol levels, exacerbating the cardiac burden in SCZ patients and decreasing their lifespan. Unknown is the mechanism by which SAM may reduce the increase in TC caused by OLZ. Previous research indicates that45 morphine, a member of the same class of κ- and δ-opioid receptor agonists as SAM, may inhibit hepatic cholesterol secretion by stimulating the Oddi sphincter. Recent studies have shown that42 κ-opioid receptor agonists can normalize endothelial ultrastructure and function in hyperlipidemic states by activating the PI3K/Akt signaling pathway and downregulating endothelial NO synthase expression/activity. Future research should characterize the mechanisms by which SAM affects lipid metabolism. Further validation of the reduced cardiovascular risks associated with OLZ/SAM treatment versus OLZ monotherapy in patients with SCZ will necessitate longer-term comparative trials and retrospective observational studies. This phenomenon prompted us to consider that any potential metabolic effects of the OLZ/SAM combination to reduce weight gain may have been neglected. The patients included in this study, except for those in Kahn et al’s study18 who were young individuals in the early stages of the disease, were individuals who had been suffering from SCZ for many years and were in a stable phase.14,15,24,25 These samples may represent a relatively unique subgroup of patients with SCZ who may not be particularly sensitive to the metabolic effects of antipsychotic drugs. Therefore, it may be necessary to observe the metabolic benefit of reduced weight gain with OLZ/SAM in patients with first-episode of SCZ or in extended follow-up experimental studies, where future experimental research should be conducted.
This meta-analysis was based on the safety and metabolic indices in SCZ patients treated with OLZ/SAM. After extensive analysis, we determined that the combination of OLZ and SAM may decrease the incidence of weight gain and positively affect serum TC. The incidence of other indicators such as somnolence, dry mouth, and other metabolic indicators such as triglycerides and glucose did not differ between the OLZ and control group. Results demonstrated that OLZ/SAM is safer than other treatment options because it is administered as a single tablet, thereby mainly avoiding the adverse effects and drug interactions associated with additional medications and prescription pills.46 The finding gives clinicians some evidence to support and point guidance in drug use. Furthermore, clinicians can provide more precise and individualized treatment plans based on the patient’s condition. Meanwhile, a significant element is the optimal timing of using OLZ in combination with SAM, whether it must be used only when metabolic effects develop or as a first-line treatment. Moreover, it is essential to ascertain the additional hepatorenal toxicity and other adverse outcomes that may develop after long-term (5 or 10 years) administration of OLZ/SAM. These points require clarification in future research.
Limitations
This study has some limitations that must be mentioned. First, it is important to note that the number of articles included in this study was limited, and there were variations in the results of the original studies. Therefore, the uncertainties related to these findings should be further investigated in future high-quality research. Second, some of the included literature does not describe the randomization and allocation concealment methods, which creates the potential for implementation and measurement bias. Third, the study’s slightly different intervention protocols, with varying concentrations of OLZ combined with SAM treatment and durations of follow-up, may have influenced the results. At last, the duration of the included trials may have been insufficient for determining the maximal efficacy of SAM in preventing weight gain and metabolic index.
Conclusion
The current study found that treatment with OLZ in combination with SAM decreased the incidence of weight gain and TC levels in patients with SCZ relative to the OLZ group, nevertheless, it did not affect other adverse events or metabolic parameters. Compared to OLZ monotherapy, the advantages of OLZ/SAM regarding weight and serum TC offer empirical support for promoting OLZ/SAM in the personalized treatment of psychotic patients. Given the long-term medication requirements of patients, it remains necessary to dynamically monitor whether OLZ/SAM will cause additional hepatorenal toxicity and other adverse effects. To validate them, further high-quality clinical trials and long-term follow-ups are required.
Abbreviations
RCTs, randomized controlled trials; CBM, Chinese Biology Medicine; CNKI, China National Knowledge Infrastructure; RevMan, Review Manager 5.4 software; TC, total cholesterol; LDL, low density lipoprotein; HDL, high density lipoprotein; SCZ, schizophrenia; SAM, samidorphan; OLZ, olanzapine; PRISMA, the Preferred Reporting for Systematic Reviews and Meta-analysis Statement; DSM-IV/V, Diagnostic and Statistical Manual of Mental Disorders; BMI, body mass index; ROB, risk of bias; RRs, relative risks; Cis, confidence intervals; MDs, mean differences; FEM, the fixed effects model; REM, the random effects model; OLZ/SAM, A combination of olanzapine and samidorphan; LYBALVI™, A combination of olanzapine and samidorphan; PANSS, Positive and Negative Syndrome Scale.
Acknowledgments
The authors thank all the other members of the team for their contributions to this study. We also thank Home for Researchers editorial team (www.home-for-researchers.com) for language editing service.
Funding
This study was supported by the Natural Science Foundation of Xinjiang Uygur Autonomous Region (Grant No. 2022D01D64).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Lieberman JA, Stroup TS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209–1223. doi:10.1056/NEJMoa051688
2. Treuer T, Anders M, Bitter I, et al. Effectiveness and tolerability of schizophrenia treatment in Central and Eastern Europe: results after 1 year from a prospective, observational study (IC-SOHO). Int J Psychiatry Clin Pract. 2006;10(2):78–90. doi:10.1080/13651500500409663
3. Komossa K, Rummel-Kluge C, Hunger H, et al. Olanzapine versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst Rev. 2010;3:CD006654. doi:10.1002/14651858.CD006654.pub2
4. De Hert M, Detraux J, van Winkel R, Yu W, Correll CU. Metabolic and cardiovascular adverse effects associated with antipsychotic drugs. Nat Rev Endocrinol. 2011;8(2):114–126. doi:10.1038/nrendo.2011.156
5. Schneider-Thoma J, Chalkou K, Dorries C, et al. Comparative efficacy and tolerability of 32 oral and long-acting injectable antipsychotics for the maintenance treatment of adults with schizophrenia: a systematic review and network meta-analysis. Lancet. 2022;399(10327):824–836. doi:10.1016/S0140-6736(21)01997-8
6. Siskind D, Gallagher E, Winckel K, et al. Does switching antipsychotics ameliorate weight gain in patients with severe mental illness? A systematic review and meta-analysis. Schizophr Bull. 2021;47(4):948–958. doi:10.1093/schbul/sbaa191
7. Ostuzzi G, Vita G, Bertolini F, et al. Continuing, reducing, switching, or stopping antipsychotics in individuals with schizophrenia-spectrum disorders who are clinically stable: a systematic review and network meta-analysis. Lancet Psychiatry. 2022;9(8):614–624. doi:10.1016/S2215-0366(22)00158-4
8. Speyer H, Westergaard C, Albert N, et al. Reversibility of antipsychotic-induced weight gain: a systematic review and meta-analysis. Front Endocrinol. 2021;12:577919. doi:10.3389/fendo.2021.577919
9. Maayan L, Vakhrusheva J, Correll CU. Effectiveness of medications used to attenuate antipsychotic-related weight gain and metabolic abnormalities: a systematic review and meta-analysis. Neuropsychopharmacology. 2010;35(7):1520–1530. doi:10.1038/npp.2010.21
10. Meftah AM, Deckler E, Citrome L, Kantrowitz JT. New discoveries for an old drug: a review of recent olanzapine research. Postgrad Med. 2020;132(1):80–90. doi:10.1080/00325481.2019.1701823
11. Tabarin A, Diz-Chaves Y, Carmona Mdel C, et al. Resistance to diet-induced obesity in mu-opioid receptor-deficient mice: evidence for a “thrifty gene”. Diabetes. 2005;54(12):3510–3516. doi:10.2337/diabetes.54.12.3510
12. Czyzyk TA, Romero-Pico A, Pintar J, et al. Mice lacking delta-opioid receptors resist the development of diet-induced obesity. FASEB J. 2012;26(8):3483–3492. doi:10.1096/fj.12-208041
13. Cunningham JI, Eyerman DJ, Todtenkopf MS, et al. Samidorphan mitigates olanzapine-induced weight gain and metabolic dysfunction in rats and non-human primates. J Psychopharmacol. 2019;33(10):1303–1316. doi:10.1177/0269881119856850
14. Martin WF, Correll CU, Weiden PJ, et al. Mitigation of olanzapine-induced weight gain with samidorphan, an opioid antagonist: a randomized double-blind Phase 2 study in patients with schizophrenia. Am J Psychiatry. 2019;176(6):457–467. doi:10.1176/appi.ajp.2018.18030280
15. Correll CU, Newcomer JW, Silverman B, et al. Effects of olanzapine combined with samidorphan on weight gain in schizophrenia: a 24-week Phase 3 study. Am J Psychiatry. 2020;177(12):1168–1178. doi:10.1176/appi.ajp.2020.19121279
16. Srisurapanont M, Suttajit S, Likhitsathian S, Maneeton B, Maneeton N. A meta-analysis comparing short-term weight and cardiometabolic changes between olanzapine/samidorphan and olanzapine. Sci Rep. 2021;11(1):7583. doi:10.1038/s41598-021-87285-w
17. Jawad MY, Alnefeesi Y, Lui LMW, et al. Olanzapine and samidorphan combination treatment: a systematic review. J Affect Disord. 2022;301:99–106. doi:10.1016/j.jad.2022.01.004
18. Kahn RS, Kane JM, Correll CU, et al. Olanzapine/samidorphan in young adults with schizophrenia, schizophreniform disorder, or bipolar I disorder who are early in their illness: results of the randomized, controlled ENLIGHTEN-early study. J Clin Psychiatry. 2023;84(3). doi:10.4088/JCP.22m14674
19. Correll CU, Stein E, Graham C, et al. Reduction in multiple cardiometabolic risk factors with combined olanzapine/samidorphan compared with olanzapine: post hoc analyses from a 24-week Phase 3 study. Schizophr Bull. 2023;49(2):454–463. doi:10.1093/schbul/sbac144
20. Page MJ, McKenzie JE, Bossuyt PM, et al. Declaracion PRISMA 2020: una guia actualizada para la publicacion de revisiones sistematicas [The PRISMA 2020 statement: an updated guideline for reporting systematic reviews]. Rev Esp Cardiol. 2021;74(9):790–799. doi:10.1016/j.rec.2021.07.010
21. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59 Suppl 20:22–33;quiz 34–57.
22. Association AP. Diagnostic and Statistical Manual of Mental Disorders.
23. Tarsilla M. Cochrane Handbook for systematic reviews of interventions. J Multidis Evaluat. 2008;6:142–148.
24. Potkin SG, Kunovac J, Silverman BL, et al. Efficacy and safety of a combination of olanzapine and samidorphan in adult patients with an acute exacerbation of schizophrenia: outcomes from the randomized, Phase 3 ENLIGHTEN-1 study. J Clin Psychiatry. 2020;81(2). doi:10.4088/JCP.19m12769
25. Brunette MF, Correll CU, O’Malley SS, et al. Olanzapine plus samidorphan (ALKS 3831) in Schizophrenia and comorbid alcohol use disorder: a phase 2, randomized clinical trial. J Clin Psychiatry. 2020;81(2). doi:10.4088/JCP.19m12786
26. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Wiley-Blackwell; 2008.
27. Alkermes. Alkermes announces FDA approval of LYBALVI™ for the treatment of schizophrenia and bipolar I disorder [media release]; June 1, 2021. Available from: https://investor.alkermes.com/.
28. Kahn RS, Silverman BL, DiPetrillo L, et al. A phase 3, multicenter study to assess the 1-year safety and tolerability of a combination of olanzapine and samidorphan in patients with schizophrenia: results from the ENLIGHTEN-2 long-term extension. Schizophr Res. 2021;232:45–53. doi:10.1016/j.schres.2021.04.009
29. Goh KK, Chen CY, Wu TH, Chen CH, Lu ML. Crosstalk between Schizophrenia and metabolic syndrome: the role of oxytocinergic dysfunction. Int J Mol Sci. 2022;23(13):7092. doi:10.3390/ijms23137092
30. Bai Z, Wang G, Cai S, et al. Efficacy, acceptability and tolerability of 8 atypical antipsychotics in Chinese patients with acute schizophrenia: a network meta-analysis. Schizophr Res. 2017;185:73–79. doi:10.1016/j.schres.2017.01.002
31. Meyer JM, Simmons A, Jiang Y, Graham C, Yagoda S, McDonnell D. Olanzapine/samidorphan combination consistently mitigates weight gain across various subgroups of patients. CNS Spectr. 2022;1–4. doi:10.1017/S1092852922000967
32. Wu H, Siafis S, Hamza T, et al. Antipsychotic-induced weight gain: dose-response meta-analysis of randomized controlled trials. Schizophr Bull. 2022;48(3):643–654. doi:10.1093/schbul/sbac001
33. Bazo-Alvarez JC, Morris TP, Carpenter JR, Hayes JF, Petersen I. Effects of long-term antipsychotics treatment on body weight: a population-based cohort study. J Psychopharmacol. 2020;34(1):79–85. doi:10.1177/0269881119885918
34. Shram MJ, Silverman B, Ehrich E, Sellers EM, Turncliff R. Use of remifentanil in a novel clinical paradigm to characterize onset and duration of opioid blockade by samidorphan, a potent mu-receptor antagonist. J Clin Psychopharmacol. 2015;35(3):242–249. doi:10.1097/JCP.0000000000000320
35. Sun L, McDonnell D, von Moltke L. Pharmacokinetics and short-term safety of ALKS 3831, a fixed-dose combination of olanzapine and samidorphan, in adult subjects with Schizophrenia. Clin Ther. 2018;40(11):1845–1854 e2. doi:10.1016/j.clinthera.2018.09.002
36. Cheng KC, Asakawa A, Li YX, et al. Opioid μ-receptors as new target for insulin resistance. Pharmacol Ther. 2013;139(3):334–340. doi:10.1016/j.pharmthera.2013.05.002
37. Sehgal N, Smith HS, Manchikanti L. Peripherally acting opioids and clinical implications for pain control. Pain Physician. 2011;14(3):249–258. doi:10.36076/ppj.2011/14/249
38. Rehan ST, Siddiqui AH, Khan Z, et al. Samidorphan/olanzapine combination therapy for schizophrenia: efficacy, tolerance and adverse outcomes of regimen, evidence-based review of clinical trials. Ann Med Surg. 2022;79:104115. doi:10.1016/j.amsu.2022.104115
39. Pillinger T, McCutcheon RA, Vano L, et al. Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta-analysis. Lancet Psychiatry. 2020;7(1):64–77. doi:10.1016/S2215-0366(19)30416-X
40. Casey DE, Haupt DW, Newcomer JW, et al. Antipsychotic-induced weight gain and metabolic abnormalities: implications for increased mortality in patients with schizophrenia. J Clin Psychiatry. 2004;65 Suppl 7:4–18; quiz 19–20.
41. Velligan DI, Weiden PJ, Sajatovic M, et al. The expert consensus guideline series: adherence problems in patients with serious and persistent mental illness. J Clin Psychiatry. 2009;70 Suppl 4:1–46; quiz 47–8.
42. Tian F, Zheng XY, Li J, et al. kappa-opioid receptor stimulation improves endothelial function via Akt-stimulated NO production in hyperlipidemic rats. Sci Rep. 2016;6:26807. doi:10.1038/srep26807
43. Li R, Zhang Y, Zhu W, et al. Effects of olanzapine treatment on lipid profiles in patients with schizophrenia: a systematic review and meta-analysis. Sci Rep. 2020;10(1):17028. doi:10.1038/s41598-020-73983-4
44. Zhu Z, Gu Y, Zeng C, et al. Olanzapine-induced lipid disturbances: a potential mechanism through the gut microbiota-brain axis. Front Pharmacol. 2022;13:897926. doi:10.3389/fphar.2022.897926
45. Bryant HU, Story JA, Yim GK. Morphine-induced alterations in plasma and tissue cholesterol levels. Life Sci. 1987;41(5):545–554. doi:10.1016/0024-3205(87)90406-1
46. Citrome L, Graham C, Simmons A, et al. An evidence-based review of OLZ/SAM for treatment of adults with Schizophrenia or Bipolar I disorder. Neuropsychiatr Dis Treat. 2021;17:2885–2904. doi:10.2147/NDT.S313840
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.