Back to Journals » Therapeutics and Clinical Risk Management » Volume 20
Effectivity of Virtual Reality to Improve Balance, Motor Function, Activities of Daily Living, and Upper Limb Function in Children with Cerebral Palsy: A Systematic Review and Meta-Analysis
Authors Komariah M ![]() , Amirah S
, Amirah S ![]() , Abdurrahman MF, Handimulya MFS, Platini H
, Abdurrahman MF, Handimulya MFS, Platini H ![]() , Maulana S
, Maulana S ![]() , Nugrahani AD
, Nugrahani AD ![]() , Mulyana AM
, Mulyana AM ![]() , Qadous SG
, Qadous SG ![]() , Mediani HS
, Mediani HS ![]() , Mago A
, Mago A
Received 28 July 2023
Accepted for publication 3 February 2024
Published 14 February 2024 Volume 2024:20 Pages 95—109
DOI https://doi.org/10.2147/TCRM.S432249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Maria Komariah,1,* Shakira Amirah,2,* Muhammad Fahd Abdurrahman,2 Mohammad Farrel Shaquille Handimulya,2 Hesti Platini,3 Sidik Maulana,4 Annisa Dewi Nugrahani,5 Aep Maulid Mulyana,4 Shurouq Ghalib Qadous,6 Henny Suzana Mediani,7 Arpit Mago8
1Department of Fundamental Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, 45363, Indonesia; 2Faculty of Medicine, Universitas Indonesia, Depok, West Java, 16424 Indonesia; 3Department of Medical-Surgical Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, 45363, Indonesia; 4Master of Nursing Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia; 5Maternal Fetal Division, Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, 40161, Indonesia; 6Department of Nursing and Midwifery, Faculty of Medicine and Health Sciences, An-Najah National University, Nablus, Palestine; 7Department of Pediatric Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, 45363, Indonesia; 8Department of Clinical Medicine, Jawaharlal Nehru Medical College, Belagavi, Karnataka, 590010, India
*These authors contributed equally to this work
Correspondence: Maria Komariah, Department of Fundamental Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, 45363, Indonesia, Email [email protected]
Background: Cerebral palsy (CP) is the most common motor disorder in childhood. CP limits movement, which can interfere with children’s daily activities. As a technology that provides intensive mass practice to children, virtual reality (VR) can create an interactive and motivating environment. With the intensity set by the therapist and feedback that can be used to produce individualized therapy, VR has great potential to improve CP patients’ quality of life, especially in a safe, enjoyable, and playful environment.
Purpose: This systematic review and meta-analysis sought to determine the effectiveness of VR for children with CP.
Methods: We conducted a comprehensive literature search based on the PRISMA guidelines through PubMed, Scopus, Embase, Wiley, and ProQuest to assess the efficacy of VR in managing children with CP up to 15 September 2022. Risk assessment of bias was performed using Cochrane RoB 2.
Results: Nineteen randomized controlled trials with 467 and 427 patients with CP were included in the intervention and control groups in qualitative and quantitative analyses. Participants consisted of cerebral palsy with hemiplegia (n=7), diplegia (n=2), a combination of both (n=4), and undefined (n=13). From all studies conducted, VR showed significant results where VR could improve balance (MD: 2.71[1.95, 3.48]; p < 0.00001), motor function (MD: 3.73 [1.67, 5.79]; p = 0.0004), and activity daily living (MD: 10.05 [2.89, 17.22]. However, VR showed not effective in improving upper limb function.
Conclusion: With its advantages and excellent effectiveness, VR may improve functional mobility and the quality of life of children with CP.
Keywords: balance, cerebral palsy, children, motor function, virtual reality
Introduction
Cerebral palsy (CP) is a common underlying factor contributing to motor impairment in children. CP has frequently changed over the years. The most recent definition of CP is a collection of lasting irregularities in the development of movement and body positioning that result in activity restrictions for the affected person.1 It is a neurodevelopmental disorder that can be brought on by brain damage or developmental flaws, first manifested in early childhood or infancy.2 Population-based studies have found that the prevalence of CP globally is between 1.5 and 4 cases per 1000 live births or children of a specific age range.3 At birth, the average prevalence of CP is around 2 per 1000 live births. However, the prevalence rates may vary depending on the country, region, and ethnic group. Nevertheless, these estimates show that CP is a significant public health issue on a global scale.3
The main characteristic of CP is a delay in motor development milestones that are usually accompanied by other symptoms that commonly. The primary symptoms are disorders of behaviors, sensory, cognitive, perception, communication, etc. Patients also can have epilepsy and secondary musculoskeletal disorders CP.1,4 The secondary injuries resulting from CP include limb stiffness, skeletal abnormalities, muscular atrophy, muscle weakness, and developmental coordination problems. These limitations on movement impact the development of the child’s gross motor abilities.2 The primary aims of CP therapy are to correct incorrect posture and patterns, avoid more deformities, enhance existing abilities, learn new skills, facilitate functional use of the upper extremities, give gait training, and achieve intelligible speech.4 A thorough, all-encompassing motor therapy program specially created for each patient is key to this development.1
CP represents a group of neurological disorders that significantly affect movement coordination and muscle tone, making rehabilitation a cornerstone of effective management. Traditionally, CP rehabilitation has encompassed a range of interventions, including physical, occupational, and speech-language therapies, each targeting specific aspects of the disorder.5 However, the emergence of Virtual Reality (VR) as a rehabilitative tool has marked a paradigm shift in therapeutic approaches. VR offers a unique, immersive environment where patients can engage in interactive and stimulating activities tailored to their individual needs and abilities.6,7 Immersive VR for upper limb motor impairment home rehabilitation is easy to learn and acceptable, improves motor function, reduces the difficulty in the reproduction of therapeutic movements, is motivating and enjoyable, and improves the quality of life.6 The innovations enable a more personalized and engaging rehabilitation experience, potentially leading to better adherence and outcomes.8 This technology not only facilitates increased patient motivation through gamification but also allows for precise tracking and feedback of motor activities, making it an increasingly popular option in pediatric rehabilitation.
VR therapy has been recently utilized to improve motor performance in children with CP. VR is a computer technology that enables the user to construct conditions and objects in a virtual environment and an exercise environment. VR technology provides spatial consistency between the quantity of movement displayed on a computer screen and in the real world. Such spatial presentation allows visual performance feedback and guidance information, both essential for motor development in CP children.2,4,9 Children with CP can benefit from active VR video games because they encourage multisensory functional activities, active muscle stretching, and motor training that tests postural stability. Other benefits of VR treatment for children with CP are that it can be enjoyable, safe, more relaxing, and less tiring for the patients.2,9 According to Y. Chen et al (2018) VR intervention treatments are more effective than other intervention methods for improving motor function in children with CP.10
Several systematic review and meta-analysis are evaluate VR on CP Outcomes. Chen et al (2018)10 concluded VR was effective in improving arm function, postural control, and ambulation. Rathinam et al (2019)11 found that VR was effective in improving hand function in children with CP. Warnier et al (2020)12 found that VR therapy had a positive effect on balance and walking in children with CP. Ren and Wu (2019)13 found that VR games had a positive effect on the gross motor skills of children with CP. Liu et al (2022)14 found that VR training had a positive effect on balance, gross motor function, and daily living ability in children with CP. The primary objectives of this study were to determine: (1) the extent to which VR improves comprehensively outcomes including motor performance, particularly to improve balance, motor function, activities of daily living, and upper limb (2) the extent sub-group analysis to evaluate VR to improve balance, motoric function, and activities daily living different types of VR, including Non-immersive, semi-immersive, and fully immersive.
Materials and Methods
Study Design
The systematic review and meta-analysis adhered to the guidelines the Cochrane Handbook for Systematic Reviews of Intervention set forth and followed the Preferred Reporting Item for Systematic Review and Meta-analysis (PRISMA) framework.15,16 By utilizing this study design, we aimed to obtain a more accurate estimate of the effectiveness of the VR intervention in children with CP and improve the precision and reliability of our findings. This study was not registered in PROSPERO.
Search Strategy
This study followed the PRISMA framework to ensure a comprehensive literature review. This study extensively searched relevant studies on several databases, including PubMed, Embase, Scopus, Wiley Library, and ProQuest. We collected data up to 15 October 2022, using the keywords “Virtual Reality” OR VR OR “active video game” OR Exergame OR AVG AND Cerebral Palsy [MeSH] OR “cerebral palsies” OR “Little disease” OR “infantile palsies” OR “spastic diplegia” OR “spastic diplegias” OR “spastic hemiplegia” OR “spastic quadriplegia”. The search strategy can be seen in Supplementary Table 1.
Eligibility Criteria
To ensure a rigorous and systematic approach in our review, we established explicit eligibility criteria for the inclusion of studies using the PICOS Framework. (1) Population: This study targeted studies involving participants diagnosed with CP. The age range was set to 0–18 years to encompass the full spectrum of childhood and adolescence, reflecting the typical age range of CP diagnosis and management. (2) Intervention: The primary interest of this study was interventions that utilized VR technology. This encompassed a wide range of VR applications, including both immersive and non-immersive systems, as well as augmented reality, provided they were used in a rehabilitative capacity for CP. (3) Comparators: Studies were eligible if they included a control group receiving standard care, no intervention, or alternative therapeutic methods. (4) Outcomes: The primary outcomes of interest for this study were improvements in balance, motor function, activities of daily living, and upper limb function. These outcomes are critical indicators of the functional impact of CP and the effectiveness of rehabilitation interventions. (5) Study Design: We included randomized controlled trials (RCTs), as they provide the highest level of evidence in intervention studies.
Exclusion criteria in this study include (1) This study is restricted to studies published in English, up to September 13, 2022. This decision was made based on our team’s linguistic capabilities and aimed at ensuring a comprehensive review within the set timeframe. (2) We excluded non-randomized studies, reviews, case reports, and studies that did not provide sufficient data on our specified outcomes. Studies that did not primarily focus on VR interventions for CP were also excluded.
Data Extraction
To organize the collected data, this study created a table that included information on the author, year of publication, study location, study population, intervention characteristics (model, methods, and type of VR), and study outcomes. VR can be immersive, semi-immersive, or non-immersive. The remaining two are called “non-immersive” because they lack fully multisensory simulation and allow users to perceive real-world information.17,18 NIVR individuals interact with a screen scenario, but they are not fully immersed because they can see the actual world as well as the digital visuals. Most of these devices can control PCs and tablets with joysticks [24]. Semi-immersive VR lets subjects engage with a screen-displayed scene through body motions. This form of simulation is prone to ambient distractions.18,19 We extracted this information using a predetermined outcome sheet and assessed the study characteristics qualitatively. Two reviewers (S.A. and M.F.A.) performed the assessment, and a third author (M.F.S.H.) rechecked the accuracy of the extracted data during statistical analysis. Furthermore, this study used EndNote X9 software to remove duplicate studies, and three independent reviewers (S.A., M.F.A., and M.F.S.H.) screened the titles and abstracts of the remaining studies for accessibility, with any disagreements resolved through discussion and consensus. When disagreements arose between the initial two reviewers regarding the inclusion of a study, we first attempted to resolve these through detailed discussion, revisiting the specific areas of discrepancy with reference to our predetermined eligibility criteria.
Quantitative Data Analysis
This study used Review Manager version 5.4 from The Cochrane Collaboration to analyze our collected data. We determined the mean differences, standard deviation, 95% confidence interval (CI), p-value for pre- and post-intervention, and the difference between intervention and control post-treatment. We used random-effect models to interpret the pooled effects. The main data we used was the mean difference between pre- and post-treatment using VR for children with CP, which we evaluated based on improvements in balance, motor function, Wee-Fim, CHAQ, and upper limb function scores. This study also used mean differences to quantify the efficacy of VR and presented these results in a forest plot using inverse variance and DerSimonian-Laird random-effects models. This study used I2 statistics to assess heterogeneity, with cut-off limits of 0%, 25%, 50%, and 75% as insignificant, low, moderate, and high heterogeneity.20 If high heterogeneity was detected, we performed a sensitivity analysis using Duval and Tweedie’s trim-and-fill method to identify any outlier studies.
Quality Assessment
The quality assessment of the included studies was conducted using the Revised Cochrane Risk of Bias Tool (RoB 2.0). This tool evaluates five domains of bias, including the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each domain was assessed in terms of low, some concerns, or high risk of bias, providing a detailed and transparent evaluation of the methodological rigor of the individual studies. Two independent reviewers performed the quality assessment for each included study. Any discrepancies or disagreements between the reviewers were resolved through discussion by consulting a third reviewer to reach a consensus.
Results
Study Selection
Initially, a total of 3307 records were identified through multiple electronic databases, including PubMed, Embase, Scopus, Wiley, and ProQuest. To streamline our search, we first removed 1477 duplicate records, resulting in 1830 unique articles for consideration. We reviewed the titles and abstracts of these 1830 records to determine their potential relevance to our research question. This led to the exclusion of 1783 records that did not meet our predefined eligibility criteria, such as those not focusing on VR interventions for CP or not reporting the outcomes of interest. The remaining 47 articles were then subjected to a full-text review for a more detailed evaluation. Of these, nine reports were not retrieved due to various reasons, such as inaccessibility or the articles being located in databases not subscribed to by our institution. Consequently, 26 full-text articles were assessed for eligibility, which involved a careful review to confirm that each study met all our inclusion criteria. Through this in-depth assessment, we excluded an additional seven studies: two because the full text was inaccessible, three that were study protocols without results, and two from which data could not be extracted. The final selection of 19 studies that were included in our study fulfilled the criteria for inclusion in our analysis.21–39 Figure 1 provides a visual summary of our search and selection methodology, ensuring transparency and replicability of the process.
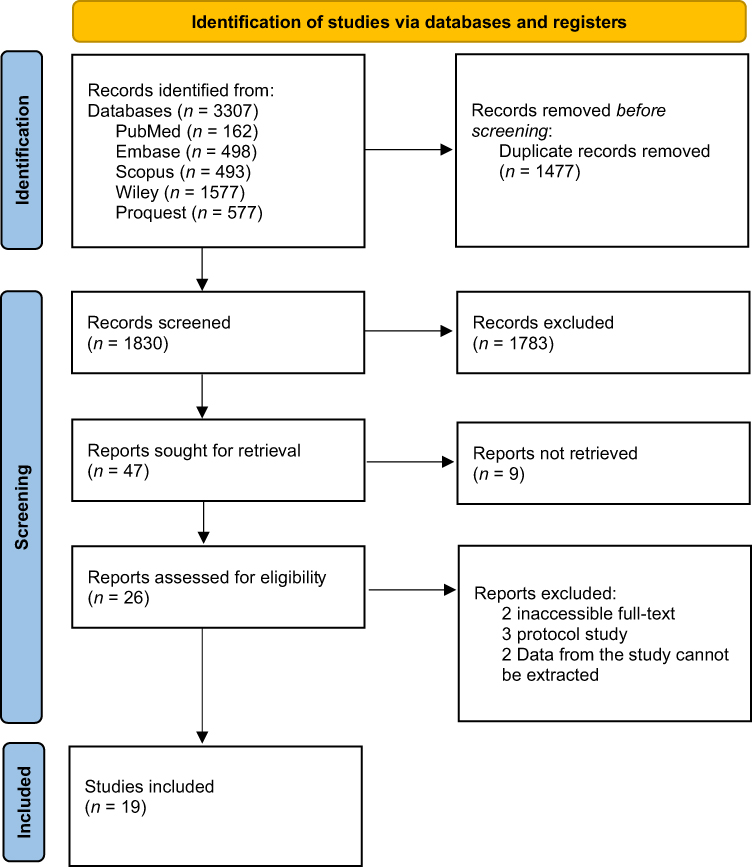 |
Figure 1 PRISMA Flow diagram. Notes: Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372:n71. |
Characteristics of Included Studies
Thirty-one RCTs yielding 467 patients in intervention groups and 427 patients in control groups, who were treated with VR, were included for quantitative and qualitative analysis. The studies were conducted in various locations (Korea, India, Turkey, England, Taiwan, Brazil, Italy, Canada, USA) and published between 2004 and 2021.21–39 The mean age of participants was between 5–16 years old, and they were further randomized to either intervention or control groups. These studies represent a similarity of research designs, predominantly parallel-group RCTs, which cater to a diverse patient demographic with conditions ranging from diplegic, hemiplegic, and dyskinetic cerebral palsy to post-operative CP cases. Participants consisted of cerebral palsy with hemiplegia (n=7), diplegia (n=2), a combination of both (n=4), and undefined (n=13). Participants’ ages spanned from 5 to 16 years, capturing a wide developmental spectrum relevant to CP intervention outcomes.
The methodologies of these trials were carefully selected to represent a breadth of VR applications, from Nintendo Wii-fit games to more specialized equipment like the RAPAEL Smart Kids devices and Xbox Kinect systems. Interventions varied significantly in terms of frequency and total duration, with some trials conducting short, intensive sessions and others opting for longer-term, home-based programs. The types of virtual reality used include non-immersive, semi-immersive, and fully immersive. (see Table 1). Balance was predominantly assessed using the Pediatric Balance Scale (PBS) and the Berg Balance Scale (BBS). Daily activities and functional independence were evaluated using the Wee-Functional Independence Measure (Wee FIM). Upper limb function was measured with tools like the Upper Limb Physician’s Rating Scale (ULPRS) and the Quality of Upper Extremity Skills Test (QUEST). For overall motor function, the Gross Motor Function Measure (GMFM) was frequently utilized. These instruments, chosen for their validated efficacy in pediatric CP assessment, reflect the specific focus of each study, capturing improvements in balance, daily activities, upper limb function, and overall motor skills among diverse CP patient populations. Detailed characteristics of the study are presented in Table 1.
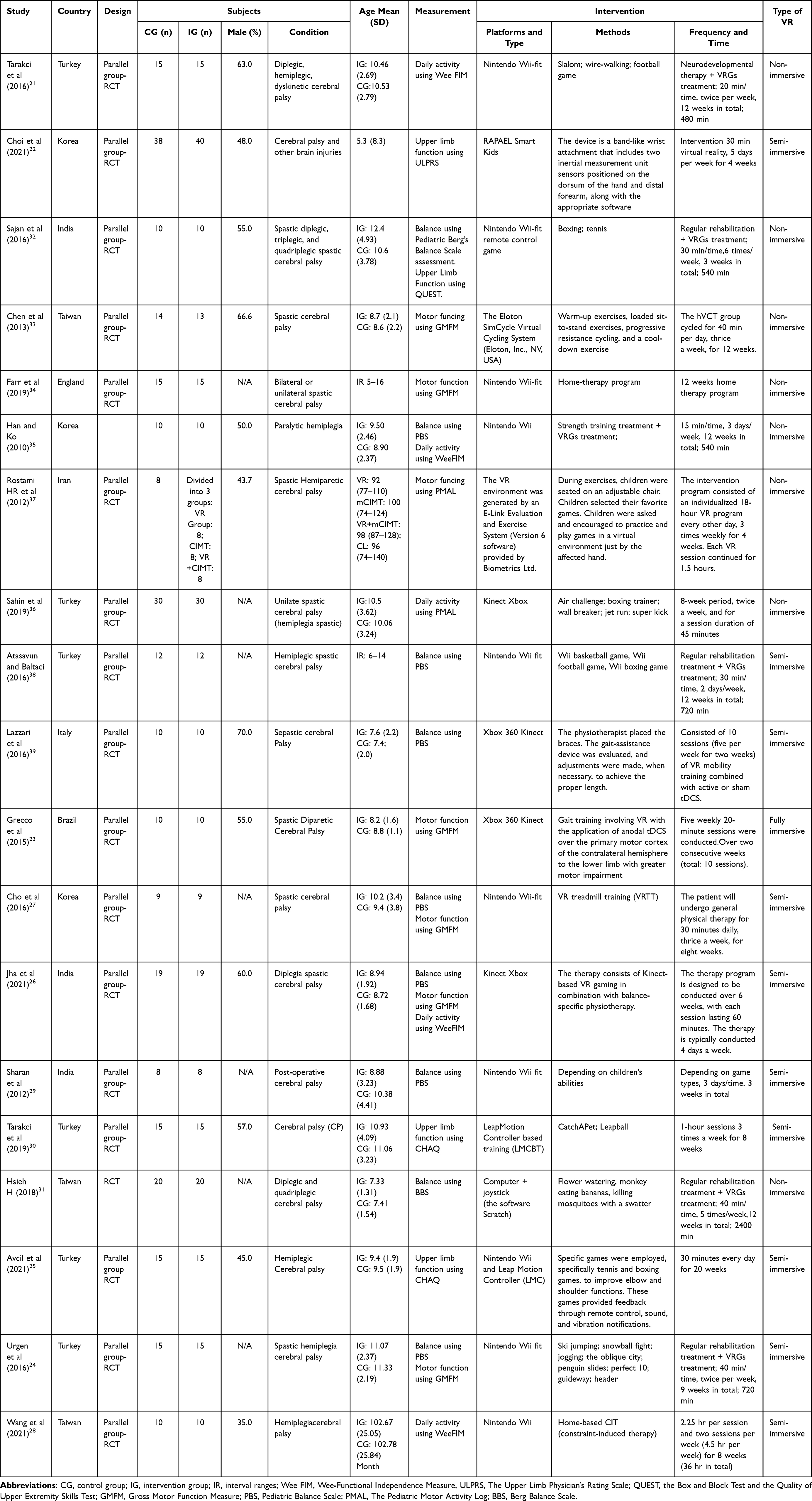 |
Table 1 Characteristics of Included Studies |
Study Outcomes
Balance
A meta-analysis was conducted to assess the outcome of VR on balanced children with CP. The questionnaires included in the meta-analysis were the Pediatric Balance Scale (PBS) and the Berg Balance Scale (BBS). VR significantly improved balance (p < 0.00001) with MD 2.71 [1.95-3.48]. Small heterogeneity was found in I2 = 35% (Figure 2). Based on sub-group analysis, non-immersive VR and semi-immersive VR both had significant effects in improving balance (MD 38.7, 95% CI 1.70–6.05, p=0.0005; MD 2.55, 95% CI 1.74–3.36, p<0.00001, respectively).
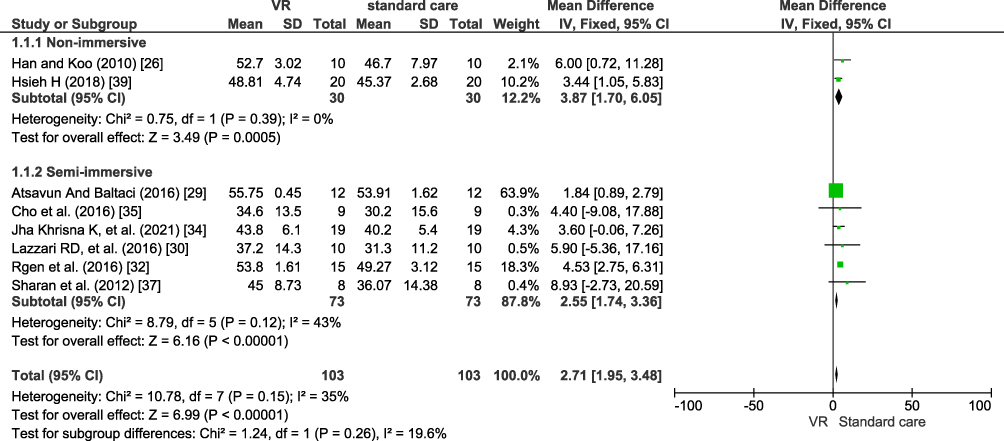 |
Figure 2 Forest plot intervention vs control effect of virtual reality in balance. |
Motor Function
Gross motor function was also assessed using the GMFM questionnaire (Figure 3). Meta-analysis also showed that VR significantly increased gross motor function (p = 0.0004) with MD 3.73 [1.67–5.79]. No heterogeneity was found (I2 = 0%). Based on sub-group analysis, semi-immersive VR had a more significant effect (MD 4.17, 95% CI 1.90–6.44, p = 0.0003) than non-immersive or fully-immersive (MD 0.008, 95% CI −5.50–5.65, p = 0.98; MD 7.00, 95% CI −3.01–17.01, p = 0.17).
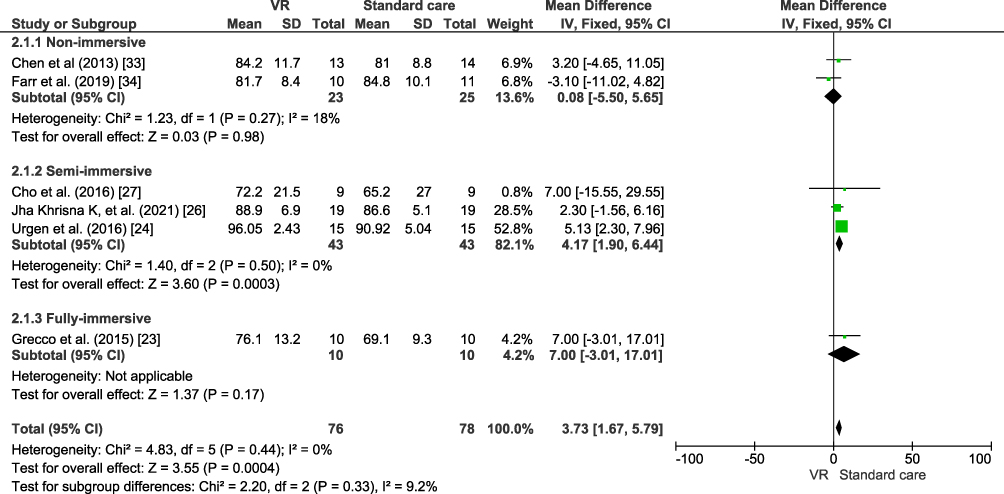 |
Figure 3 Forest plot intervention vs control effect of virtual reality in motor function. |
Activities of Daily Living
A meta-analysis was also done to assess the outcome of VR on activities of daily living children with CP (Figure 4). The questionnaire included in the meta-analysis was Wee-fim. VR significantly improved the Wee-fim score (p = 0.006) with MD 10.05 [2.89-17.22]. There is heterogeneity was found (I2 = 70%). Based on sub-group analysis, non-immersive VR had a more significant effect (MD 9.89, 95% CI 0.85–18.94, p=0.03) than semi-immersive (MD 14.85, 95% CI −10.02–39.72, p=0.24).
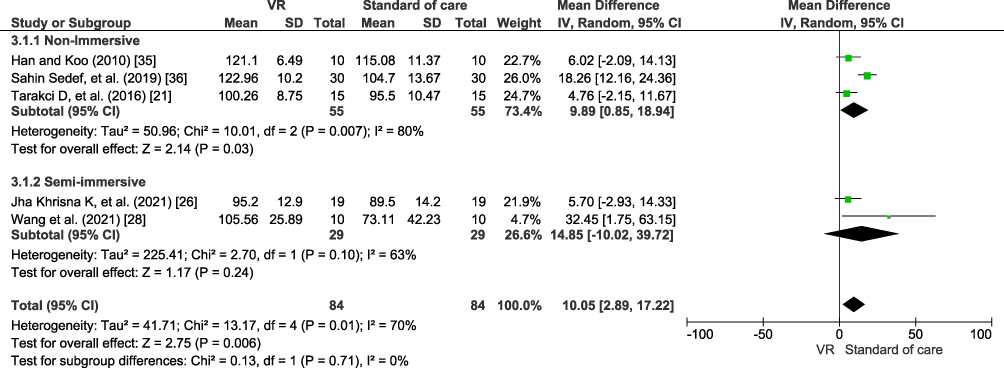 |
Figure 4 Forest plot intervention vs control effect of virtual reality in activities of daily living. |
Upper Limb Function
Upper limb function was asses using the CHAQ questionnaire (Figure 5). Meta-analysis showed that VR significantly increased upper limb function among children with standard care (p = 0.002). No heterogeneity was found (I2 = 0%). Additionally, Upper limb function was also asses using the upper limb function rating scale (ULPRS) and pediatric motor activity log (PMAL). There is only one study conducted by Choi et al was evaluated using ULPRS and two studies conducted by Rostami et al and Wang et al used PMAL. However, the UPLRS outcome did not generate to meta-analysis because only asses in one study and PMAL conducted by Rostami et al and Wang et al did not generate a meta-analysis because they used different sub-scale. Choi et al showed there is an enhanced ULPRS score after participants received the VR intervention compared to before the intervention (p< 0.001). However, there is no statistically significant effective compared between the intervention and control group (p= 0.99). Rostami et al showed VR was significantly enhanced quality of movement, despite Wang et al showed VR was not statistically significant to enhance amount of arm use.
 |
Figure 5 Forest plot intervention vs control effect of virtual reality in upper limb function. |
Quality Assessment and Publication Bias
The quality of each study was also evaluated using the Cochrane Revised Risk of Bias (ROB 2.0) for randomized controlled trials. This assessment tool examines five domains, which encompass the evaluation of potential biases. These domains include randomization bias resulting from deviations from the intended intervention, handling of missing outcome data, appropriateness of outcome measures, and bias in reporting outcomes. In terms of quality, a study is classified as good quality if the research meets the requirements of good research converted through the AHRQ standard. Although there are 4 studies with some concerns and 1 study with a high risk of bias, most of the studies have a low quality of bias in the overall results (Figure 6).
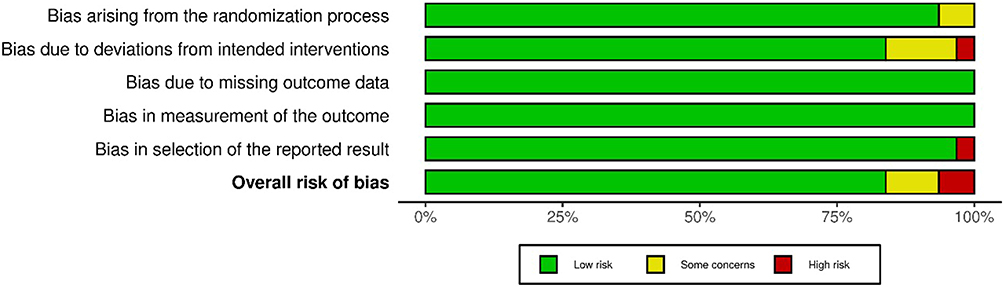 |
Figure 6 Summary risk of bias. |
Discussion
Principal Findings
VR is the creation of an immersive simulation environment using the software. With VR, users can feel that they are really in a different environment. In addition to its use of a new environment, VR is also a method that is a safe, enjoyable, and playful environment.38 Our study is the first to assess VR’s effectiveness on multiple functions in children with CP. This study found that VR gives significant results in increasing balance, motor function, and daily activity living. Moreover, VR has no statistically significant effect on enhancing upper limb function. However, qualitatively VR effective enhances upper limb function.
This study reveals significant insights into the effectiveness of VR interventions in children with CP, aligning with and expanding upon findings from previous studies. These were concluded that VR is effective to enhance upper and limb function, gross motoric skill, and ambulatory. For instance, this finding resonates with the large effect of VR on arm function (as a part of upper limb function) and postural control (as a part of lower limb function) reported by Chen et al (2018).10 This study demonstrated a large effect size (d = 0.861) for VR compared with other interventions, underscoring the substantial impact of VR in rehabilitation settings. Similarly, our analysis also revealed improvements in ambulation, aligning with the medium effect size (d = 0.755) observed by Chen et al. However, our study advances this understanding by differentiating the effects of various VR types, noting that immersive are more effective than non-immersive, a distinction not extensively explored in prior research. Furthermore, the categorization of outcome variables based on the International Classification of Functioning, Disability and Health (ICF) model in our study provides a more nuanced perspective. Our study also addresses the heterogeneity observed in previous studies, such as the large variability reported by Chen et al. By conducting a thorough sub-group analysis, we provide clarity on how different types of VR, intervention durations, and intensity levels contribute to this heterogeneity, thereby offering valuable insights for future research and practice.
VR can produce neuroplastic changes attached to the sensory-motor cortex. These changes are also associated with increased motor skills in the affected patient’s limbs. VR can provide significant results on motor skill function by increasing cortical reorganization and changes in neuroplasticity.40 In our study, most RCTs we took were VR-using games. The use of VR by playing games involves actions, such as screaming, laughing, or doing hand or foot movements that can increase bioelectric signals in the brain. The use of VR also provides somatic experiences.41 In this regard, duration, intensity, and repetition play an important role in motor function improvement in children with CP. In children with CP, the spatial presentation offered by VR can provide crucial visual feedback and guidance information, which can significantly contribute to their motor learning.40
A study conducted by Pottle J (2019). VR systems usually only consist of a combination of headsets and laptops, both of which are commercially available, so their use is intended for the convenience and safety of users. In addition, VR can provide psychological security and fun, and its gamification potential can encourage children and users from various other circles to do autonomous learning.42 Another study showed that as long as appropriate hardware and software are used and patient selection is carefully made under the guidance of Certified Child Life Specialists, VR is considered safe for pediatric patients. Side effects are rare, and even if they occur, they are self-limited, likewise in another study of VR in critically ill patients. All patients in the study completed their sessions almost daily. None of the committed sessions were terminated due to security issues. The study’s results also showed that the exercises performed with VR could improve attention and working memory and cause no side effects.43,44
Research on VR and technological developments is increasing from year to year. In rehabilitation, using VR coupled with assistive technologies has shown positive results. One example is the robot-assisted upper limb therapy associated with VR providing significant results with users being able to train wheelchair navigation skills in dangerous situations. In addition, research on VR with several other medical conditions, such as psychiatric disorders, pain management, and other clinical conditions, also gave positive results.45 From several meta-analyses on VR for children with CP, VR has effectively enhanced various aspects of function in children with CP, including upper limb motor skills, gross motor skills, postural control, and balance.46,47 Our study and several others show that VR has enormous benefits for treating children with CP and other medical conditions related to visual and cognitive problems or lack of spasticity.
There are not only the potential benefits but also the inherent limitations and challenges associated with this technology. While numerous studies, including those analyzed in our review, demonstrate positive outcomes in improving balance, motor function, activities of daily living, and upper limb function, the results are not uniformly positive across all research. Some studies report mixed or inconclusive results, highlighting the variability in effectiveness of VR interventions. There are practical challenges and limitations in the application of VR therapy. These include the accessibility and cost of VR technology, which may limit its widespread adoption in clinical and home settings.8,48 Technical issues, such as the need for specialized equipment and trained personnel, and the potential for VR-induced symptoms like motion sickness or discomfort, also pose significant challenges.48,49 Additionally, long-term effects and sustainability of improvements gained through VR therapy remain under-researched, warranting further investigation.48,49 Despite these challenges, VR interventions have shown promise in improving balance function in children with CP.48 However, the effectiveness of VR interventions can vary depending on several factors, including differences in VR technology (non-immersive vs semi-immersive vs fully immersive), variability in program design and implementation, as well as differences in participant characteristics such as age, severity of CP, and individual responsiveness to VR therapy.
Implication to Practice
Of the various advantages of VR as a therapy, several challenges are a concern in the use of VR. First, prolonged exposure within a few centimeters of the eye can cause eye strain or headaches. Then cybersickness that can cause nausea is one of the most frequently reported side effects. Last but not least, its implementation requires influential factors and conditions. Therapists play an important role in optimizing VR therapy for these various challenges. With the therapist’s guidance, the hardware and software selection can be adjusted to the patient’s age to reduce side effects such as cybersickness. The therapist can change the patient’s duration, intensity, and repetitions to avoid eye strain and headaches due to prolonged exposure to the screen. In the future, VR-based therapy can be implemented in hospitals and at home so that the treatment can adjust to the conditions and influential factors needed. This VR-based therapy will also provide reduced costs, increased efficiency, and the system’s convenience tailored to its users’ comfort. Children with CP might benefit from VR therapy targeted at the lower extremities because it allows kids to have fun while exercising, which improves patient compliance. The safety of the therapist and patient has been described in various studies, so this VR-based therapy is effective for children with CP and other necessary needs.
Moreover, the research landscape in VR therapy for CP is continuously evolving, with emerging studies exploring new applications and methodologies. It is imperative that future research not only replicates and expands upon studies showing positive outcomes but also rigorously investigates instances where VR therapy may have limited or no therapeutic benefits. Such comprehensive exploration is vital for developing a complete understanding of VR therapy’s role in CP rehabilitation, ensuring that its application is guided by evidence that is both robust and nuanced.
Strength and Limitations
As far as we know, this systematic review is the first to explore the impact of VR on balance, motor function, activities of daily living, and upper limb function outcomes in children with CP. However, we have some limitations to our study. First, this study only extracted data from published English-language papers; the data from the extraction table are pretty varied, including the variety of subject characteristics and the type and degree of severity of CP, and unpublished studies were not included. While our review provides comprehensive insights from English-language studies, this selection bias might have led to the exclusion of relevant studies conducted in other languages, possibly affecting the overall conclusions regarding the effectiveness of VR in CP treatment. Hence, future systematic reviews on this topic could aim to include studies published in multiple languages to ensure a more comprehensive and inclusive analysis, are needed. This systematic review is unregistered in the PROSPERO because they no longer accept published papers. The spectrum of cerebral palsy (CP) encompasses a range of heterogeneous subtypes, each presenting with varying degrees of severity and clinical manifestations. While this review initially aims to explore the effectiveness of VR in a broad CP population, we acknowledge the distinct characteristics and therapeutic needs of specific subtypes, such as unilateral cerebral palsy. Future research could benefit from a concentrated focus on these subtypes to yield more precise insights into the efficacy of VR interventions.
Moreover, the duration of VR intervention and the period for measuring its therapeutic effects may not have been sufficient to capture long-term changes and the sustainability of the benefits of VR. Future research could extend the observation period to evaluate the long-term impact and sustainability of improvements obtained through VR therapy, providing a more comprehensive picture of its benefits for CP patients. This study is limited in examining the influence of comorbid conditions, such as epilepsy, on the effectiveness of VR. Further studies are needed that specifically explore how these comorbid conditions affect the response to VR therapy and identify therapy adaptation methods that can enhance safety and effectiveness for this population. Lastly, the potential side effects, particularly the risk of triggering epileptic seizures in susceptible patients, need to be further investigated. Future research should systematically record and analyze incidences of side effects, including the possibility of VR-induced epileptic seizures, to ensure that VR therapy is not only effective but also safe for all CP patients.r.
Conclusion
The findings of this study highlight the significant potential of VR as an effective therapeutic modality for children with CP. The diverse advantages of VR, ranging from its engaging nature to its ability to simulate real-life scenarios in a controlled environment, make it a promising tool in pediatric rehabilitation. Furthermore, ongoing advancements in VR technology continue to enhance its applicability and effectiveness, not only for children with CP but also for patients with various other medical conditions that could benefit from VR-based therapy. This study highlights how VR therapy can specifically address the unique challenges faced by children with CP. By improving balance, motor function, and activities of daily living, VR therapy can significantly enhance the quality of life for these children, potentially offering advantages over traditional therapeutic approaches. These improvements are not just limited to physical aspects but also extend to psychological and social benefits, contributing to a more holistic approach to CP management.
There is a clear need for more high-quality standards of randomized RCTs that are specifically designed to evaluate the effectiveness of VR in managing CP in children. The futher studies should aim to explore various aspects of VR therapy, including the identification of the most effective types of VR applications (eg, non-immersive, semi-immersive, fully immersive) and their respective impacts on different symptoms of CP. Additionally, these future studies should also aim to understand the long-term effects of VR therapy and its sustainability in routine clinical practice. Furthermore, alongside clinical research, there is a necessity for developing comprehensive guidelines that encompass hardware and software requirements, standard operating procedures, and best practices for implementing VR therapy in clinical settings. These guidelines would aid clinicians and therapists in effectively integrating VR into their treatment protocols, ensuring that the therapy is delivered safely, efficiently, and in a manner that maximizes patient outcomes.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Sadowska M, Sarecka-Hujar B, Kopyta I. Cerebral palsy: current opinions on definition, epidemiology, risk factors, classification and treatment options. Neuropsychiatr Dis Treat. 2020;16:1505–1518. doi:10.2147/NDT.S235165
2. Wu J, Loprinzi PD, Ren Z. The rehabilitative effects of virtual reality games on balance performance among children with cerebral palsy: a meta-analysis of randomized controlled trials. Int J Environ Res Public Health. 2019;16(21):4161. doi:10.3390/ijerph16214161
3. Stavsky M, Mor O, Mastrolia SA, Greenbaum S, Than NG, Erez O. Cerebral palsy-trends in epidemiology and recent development in prenatal mechanisms of disease, treatment, and prevention. Front Pediatr. 2017;5:21. doi:10.3389/fped.2017.00021
4. Metin Ökmen B, Doğan Aslan M, Nakipoğlu Yüzer GF, Özgirgin N. Effect of virtual reality therapy on functional development in children with cerebral palsy: a single-blind, prospective, randomized-controlled study. Turkish J Phys Med Rehabil. 2019;65(4):371–378. doi:10.5606/tftrd.2019.2388
5. Anaby D, Korner-Bitensky N, Steven E, et al. Current rehabilitation practices for children with cerebral palsy: focus and gaps. Phys Occup Ther Pediatr. 2016;37(1):1–15. doi:10.3109/01942638.2015.1126880
6. Phelan I, Carrion-Plaza A, Furness PJ, Dimitri P. Home-based immersive virtual reality physical rehabilitation in paediatric patients for upper limb motor impairment: a feasibility study. Virtual Real. 2023;27(4):3505–3520. doi:10.1007/s10055-023-00747-6
7. Fregna G, Schincaglia N, Baroni A, Straudi S, Casile A. A novel immersive virtual reality environment for the motor rehabilitation of stroke patients: a feasibility study. Front Robot AI. 2022;9:1–12. doi:10.3389/frobt.2022.906424
8. Kouijzer MMTE, Kip H, Bouman YHA, Kelders SM. Implementation of virtual reality in healthcare: a scoping review on the implementation process of virtual reality in various healthcare settings. Implement Sci Commun. 2023;4(1):67. doi:10.1186/s43058-023-00442-2
9. Liu W, Hu Y, Li J, Chang J. Effect of virtual reality on balance function in children with cerebral palsy: a systematic review and meta-analysis. Front Public Health. 2022;10:865474. doi:10.3389/fpubh.2022.865474
10. Chen Y, Fanchiang HD, Howard A. Effectiveness of virtual reality in children with cerebral palsy: a systematic review and meta-analysis of randomized controlled trials. Phys Ther. 2018;98(1):63–77. doi:10.1093/ptj/pzx107
11. Rathinam C, Mohan V, Peirson J, Skinner J, Nethaji KS, Kuhn I. Effectiveness of virtual reality in the treatment of hand function in children with cerebral palsy: a systematic review. J Hand Ther off J Am Soc Hand Ther. 2019;32(4):426–434.e1. doi:10.1016/j.jht.2018.01.006
12. Warnier N, Lambregts S, Port I. Effect of virtual reality therapy on balance and walking in children with cerebral palsy: a systematic review. Dev Neurorehabil. 2020;23(8):502–518. doi:10.1080/17518423.2019.1683907
13. Ren Z, Wu J. The effect of virtual reality games on the gross motor skills of children with cerebral palsy: a meta-analysis of randomized controlled trials. Int J Environ Res Public Health. 2019;16(20). doi:10.3390/ijerph16203885
14. Liu C, Wang X, Chen R, Zhang J. The effects of virtual reality training on balance, gross motor function, and daily living ability in children with cerebral palsy: systematic review and meta-analysis. JMIR Serious Games. 2022;10(4):e38972. doi:10.2196/38972
15. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:372. doi:10.1136/bmj.n71
16. Riley RD, Moons KGM, Snell KIE, et al. A guide to systematic review and meta-analysis of prognostic factor studies. BMJ. 2019;364. doi:10.1136/BMJ.K4597
17. Matijević V, Secić A, Masić V, Sunić M, Kolak Z, Znika M. Virtual reality in rehabilitation and therapy. Acta Clin Croat. 2013;52(4):453–457.
18. García-López H, Obrero-Gaitán E, Castro-Sánchez AM, Lara-Palomo IC, Nieto-Escamez FA, Cortés-Pérez I. Non-immersive virtual reality to improve balance and reduce risk of falls in people diagnosed with parkinson’s disease: a systematic review. Brain Sci. 2021;11(11):1435. doi:10.3390/brainsci11111435
19. Basso Moro S, Bisconti S, Muthalib M, et al. A semi-immersive virtual reality incremental swing balance task activates prefrontal cortex: a functional near-infrared spectroscopy study. Neuroimage. 2014;85(Pt 1):451–460. doi:10.1016/j.neuroimage.2013.05.031
20. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/BMJ.327.7414.557
21. Tarakci D, Huseyinsinoglu BE, Tarakci E, Ozdinçler AR. The effects of Nintendo Wii-Fit video games on balance in children with mild cerebral palsy. Pediatr Int. 2016;58(10):1042–1050. doi:10.1111/ped.12942
22. Choi JY, Yi SH, Ao L, et al. Virtual reality rehabilitation in children with brain injury: a randomized controlled trial. Dev Med Child Neurol. 2021;63(4):480–487. doi:10.1111/dmcn.14762
23. Grecco LAC, Duarte N, Mendonça ME, Galli M, Fregni F, Oliveira CS. Effects of anodal transcranial direct current stimulation combined with virtual reality for improving gait in children with spastic diparetic cerebral palsy: a pilot, randomized, controlled, double-blind, clinical trial. Clin Rehabil. 2015. doi:10.1177/0269215514566997
24. Urgen, MS, Akbayrak T, Gunel M, Cankaya O, Guchan Z, Turkyilmaz E. Investigation of the effects of the NintendoWii-Fit training on balance and advanced motor performance in children with spastic hemiplegic cerebral palsy: a randomized controlled trial. Int J Ther Rehabil Res. 2016;5(4):146. doi:10.5455/ijtrr.000000157
25. Avcil E, Tarakci D, Arman N, Tarakci E. Upper extremity rehabilitation using video games in cerebral palsy: a randomized clinical trial. Acta Neurol Belg. 2021;121(4):1053–1060. doi:10.1007/s13760-020-01400-8
26. Jha KK, Karunanithi GB, Sahana A, Karthikbabu S. Randomised trial of virtual reality gaming and physiotherapy on balance, gross motor performance and daily functions among children with bilateral spastic cerebral palsy. Somatosens Mot Res. 2021;38(2):117–126. doi:10.1080/08990220.2021.1876016
27. Cho C, Hwang W, Hwang S, Chung Y. Treadmill training with virtual reality improves gait, balance, and muscle strength in children with cerebral palsy. Tohoku J Exper Med. 2016:213–218. doi:10.1620/tjem.238.213.Correspondence
28. Wang TN, Chen YL, Shieh JY, Chen HL. Commercial exergaming in home-based pediatric constraint-induced therapy: a randomized trial. OTJR. 2021;41(2):90–100. doi:10.1177/1539449220984110
29. Sharan D, Ps A, Rameshkumar R, Mathankumar M, Manjula M. Virtual reality based therapy for post operative rehabilitation of children with cerebral palsy. Work. 2012;41:3612–3615. doi:10.3233/WOR-2012-0667-3612
30. Tarakci E, Arman N, Tarakci D, Kasapcopur O. Leap Motion Controller e based training for upper extremity rehabilitation in children and adolescents with physical disabilities: a randomized controlled trial. J Hand Ther. 2019;32(1):1–9. doi:10.1016/j.jht.2019.03.012
31. Hsieh HC. Effects of a gaming platform on balance training for children with cerebral palsy. Pediatr Phy Ther. 2018;30(4):303–308. doi:10.1097/PEP.0000000000000521
32. Sajan JE, John JA, Grace P, et al. Wii-based interactive video games as a supplement to conventional therapy for rehabilitation of children with cerebral palsy: a pilot, randomized controlled trial rehabilitation of children with cerebral palsy: a pilot, randomized controlled trial. Dev Neurorehabil. 2016:1–7. doi:10.1080/17518423.2016.1252970
33. Chen CL, Chen CY, Liaw MY, Chung CY, Wang CJ, Hong WH. Efficacy of home-based virtual cycling training on bone mineral density in ambulatory children with cerebral palsy. Osteopo Int. 2013;24(4):1399–1406. doi:10.1007/s00198-012-2137-0
34. Farr WJ, Green D, Bremner S, et al. Feasibility of a randomised controlled trial to evaluate home-based virtual reality therapy in children with cerebral palsy. Disabil Rehabil. 2019;43(1):85–97. doi:10.1080/09638288.2019.1618400
35. Han JH, Ko JY. Evaluation of balance and activities of daily living in children with spastic cerebral palsy using virtual reality program with electronic games. J Korea Contents Assoc. 2010;10(6):480–488. doi:10.5392/jkca.2010.10.6.480
36. Sahin S, Aran OT, Bahadir Z, Kayihan H. The effects of virtual reality on motor functions and daily life activities in unilateral spastic cerebral palsy: a single-blind randomized controlled trial. Antioxidants. 2019;8(6). doi:10.1089/g4h.2019.0020
37. Rostami HR, Arastoo AA, Nejad SJ, Mahany MK, Malamiri RA, Goharpey S. Effects of modified constraint-induced movement therapy in virtual environment on upper-limb function in children with spastic hemiparetic cerebral palsy: a randomised controlled trial. NeuroRehabilitation. 2012;31(4):357–365. doi:10.3233/NRE-2012-00804
38. Atasavun Uysal S, Baltaci G. Effects of Nintendo Wii TM training on occupational performance, balance, and daily living activities in children with spastic hemiplegic cerebral palsy: a single-blind and randomized trial. Games Health J. 2016;5(5):311–317. doi:10.1089/g4h.2015.0102
39. Lazzari RD, Politti F, Belina SF, et al. Effect of transcranial direct current stimulation combined with virtual reality training on balance in children with cerebral palsy: a randomized, controlled, double-blind, clinical trial. J Motor Behav. 2016:2895. doi:10.1080/00222895.2016.1204266
40. You SH, Jang SH, Kim YH, Kwon YH, Barrow I, Hallett M. Cortical reorganization induced by virtual reality therapy in a child with hemiparetic cerebral palsy. Dev Med Child Neurol. 2005;47(9):628–635. doi:10.1017/S0012162205001234
41. Shin JW, Song GB, Hwangbo G. Effects of conventional neurological treatment and a virtual reality training program on eye-hand coordination in children with cerebral palsy. J Phys Ther Sci. 2015;27(7):2151–2154. doi:10.1589/jpts.27.2151
42. Pottle J. Virtual reality and the transformation of medical education. Futur Healthc J. 2019;6(3):181–185. doi:10.7861/fhj.2019-0036
43. Caruso TJ, O’Connell C, Qian JJ, et al. Retrospective review of the safety and efficacy of virtual reality in a pediatric hospital. Pediatr Qual Saf. 2020;5(2):e293. doi:10.1097/pq9.0000000000000293
44. Son H, Ross A, Mendoza-Tirado E, Lee LJ. Virtual reality in clinical practice and research: viewpoint on novel applications for nursing. JMIR Nurs. 2022;5(1):e34036. doi:10.2196/34036
45. Garrett B, Taverner T, Gromala D, Tao G, Cordingley E, Sun C. Virtual reality clinical research: promises and challenges. JMIR Serious Games. 2018;6(4):e10839. doi:10.2196/10839
46. Chen YP, Lee SY, Howard AM. Effect of virtual reality on upper extremity function in children with cerebral palsy: a meta-analysis. Pediatr Phys Ther off Publ Sect Pediatr Am Phys Ther Assoc. 2014;26(3):289–300. doi:10.1097/PEP.0000000000000046
47. Pin TW. Effectiveness of interactive computer play on balance and postural control for children with cerebral palsy: a systematic review. Gait Posture. 2019;73:126–139. doi:10.1016/j.gaitpost.2019.07.122
48. Cullen AJ, Dowling NL, Segrave R, Morrow J, Carter A, Yücel M. Considerations and practical protocols for using virtual reality in psychological research and practice, as evidenced through exposure-based therapy. Behav Res Methods. 2021;53(6):2725–2742. doi:10.3758/s13428-021-01543-3
49. Naro A, Calabrò RS. What do we know about the use of virtual reality in the rehabilitation field? A brief overview. Electronics. 2021;10(9):1042. doi:10.3390/electronics10091042
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fracture Rates in Children with Cerebral Palsy: A Danish, Nationwide Register-Based Study
Granild-Jensen JB, Pedersen AB, Kristiansen EB, Langdahl B, Møller-Madsen B, Søndergaard C, Farholt S, Vestergaard ET, Rackauskaite G
Clinical Epidemiology 2022, 14:1405-1414
Published Date: 22 November 2022